Embed Size (px)
Citation preview
Max Mak Clinical Pharmacist Yan Chai Hospital
18th May 2015
Joint Pharmacist-Nurse Round in Medical Extended Care Unit to
Reduce Polypharmacy – Physicians’ Acceptance Rate and
Clinical Significance of Interventions
Hospital Authority Convention 2015
1. Introduction Medication-related problems in older adults are common,
costly, and lead to poor outcomes.1
However, these events are often preventable.1
Most preventable adverse drug events (ADEs) occur at ordering & monitoring stages of care2,3
Older adults are at increased risk of harm from medication use4
Experience adverse drug reactions (ADRs) at twice the frequency of younger adults
1. The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society Updated Beers Criteria for Potentially
Inappropriate Medication Use in Older Adults. J Am Geriatr Soc 2012;60(4):616-31. doi: 10.1111/j.1532-5415.2012.03923.x. 2. Gurwitz JH, Field TS, Harrold LR, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA
2003;289:1107–1116. 3. Gurwitz JH, Field TS, Judge J, et al. The incidence of adverse drug events in two large academic long-term care facilities. Am J Med 2005;118:251– 258. 4. Budnitz DS, Pollock DA, Weidenbach KN, et al. National surveillance of emergency department visits for outpatient adverse drug events. JAMA.
2006;296:1858–1866.
Avoiding the use of inappropriate & high-risk drugs is an important, simple, & effective strategy in reducing medication-related problems & ADEs in older adults.
However, many of our geriatric patients have the problem of polypharmacy
• Definition: the use of multiple medications or the use of more medications than are medically necessary
• 50% of older adults have polypharmacy5
• Hong Kong: 65% to 73% 6,7
5. Maher RL, Hanlon J, Hajjar ER. Clincial consequences of polypharmacy in elderly. Expert Opin. Drug Saf. 2013: DOI 10.1517/14740338.2013.827660. 6. Lam DPY, Mak CF, Chan SMC, Yao RWY, Leung SSY, You JHS. Polypharmacy and inappropriate prescribing in elderly Hong Kong Chinese Patients. Journal
of American Geriatrics Society 2010;58(1):203-204. 7. Liu BC, Leung DS, Chi I. Social functioning, polypharmacy and depression in older Chinese primary care patients. Aging & Mental Health 2011;15(6):732-
741.
1. Introduction
Negative consequences associated with polypharmacy:5
Increase healthcare cost Increase risk of ADEs Increase risk of drug interactions Decrease medication adherence Decrease functional status Increase cognitive impairment Increase fall risks Increase urinary incontinence Malnutrition
1. Introduction
5. Maher RL, Hanlon J, Hajjar ER. Clincial consequences of polypharmacy in elderly. Expert Opin. Drug Saf. 2013: DOI 10.1517/14740338.2013.827660.
Multidisciplinary Approach to Tackle Polypharmacy:
Establish weekly Joint Pharmacist-nurse Round including clinical pharmacists, senior nurses & ± physicians
Make recommendations to physicians by attaching standardized intervention forms to patients’ drug charts
1. Introduction
Multidisciplinary Approach to Tackle Polypharmacy:
Aims: To formulate the BEST treatment plan through teamwork To reduce polypharmacy To enhance patient safety by identifying potentially
inappropriate medications (PIMs) To provide drug-related problem support to physicians &
nurses
1. Introduction
Multidisciplinary Approach to Tackle Polypharmacy:
Setting: Extended Care Unit (ECU) 2 rehabilitation wards(75 beds) & 1 infirmary ward(38 beds) ECU patients usually received less intensive care on drug
regimens
1. Introduction
Multidisciplinary Approach to Tackle Polypharmacy:
Target Patients: Newly admitted patients to the ECU(< 7 days) Selected patients, who have problems in polypharmacy,
poor drug compliance, &/or poor drug tolerance, referred by other healthcare professions
1. Introduction
Multidisciplinary Approach to Tackle Polypharmacy:
Physicians High daily workload for physicians in ECU Each physician takes charge of >35 patients in each ward
Clinical Pharmacists Specialized in streamlining complicated drug regimens
1. Introduction
Multidisciplinary Approach to Tackle Polypharmacy:
Nurses Better understanding on patients’ need & complaint Provide the most valuable information on patients’ drug
response
Direct interaction with Patients
1. Introduction
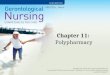
Service Work Flow:
2. Service Details
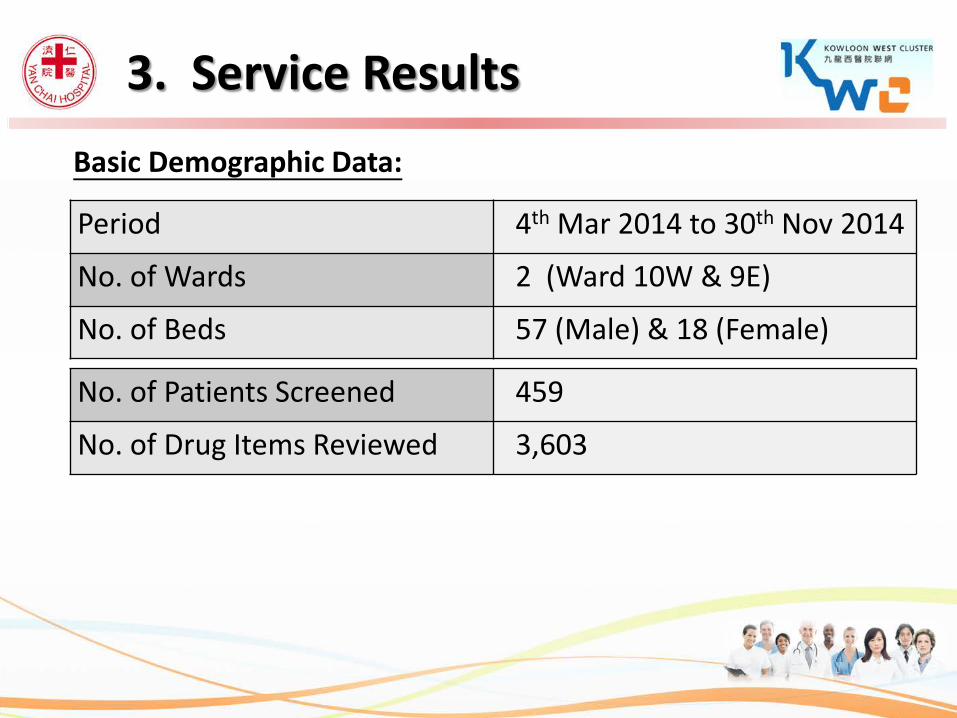
Basic Demographic Data:
Period 4th Mar 2014 to 30th Nov 2014
No. of Wards 2 (Ward 10W & 9E)
No. of Beds 57 (Male) & 18 (Female)
No. of Patients Screened 459
No. of Drug Items Reviewed 3,603
3. Service Results
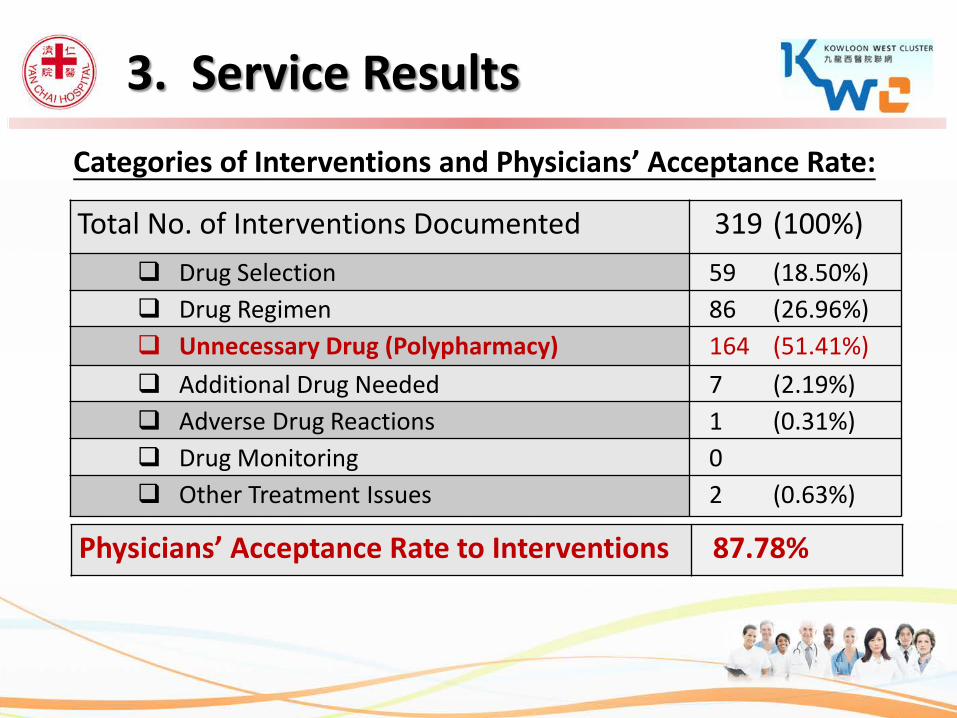
Categories of Interventions and Physicians’ Acceptance Rate:
Total No. of Interventions Documented 319 (100%) Drug Selection 59 (18.50%) Drug Regimen 86 (26.96%) Unnecessary Drug (Polypharmacy) 164 (51.41%) Additional Drug Needed 7 (2.19%) Adverse Drug Reactions 1 (0.31%) Drug Monitoring 0 Other Treatment Issues 2 (0.63%)
Physicians’ Acceptance Rate to Interventions 87.78%
3. Service Results
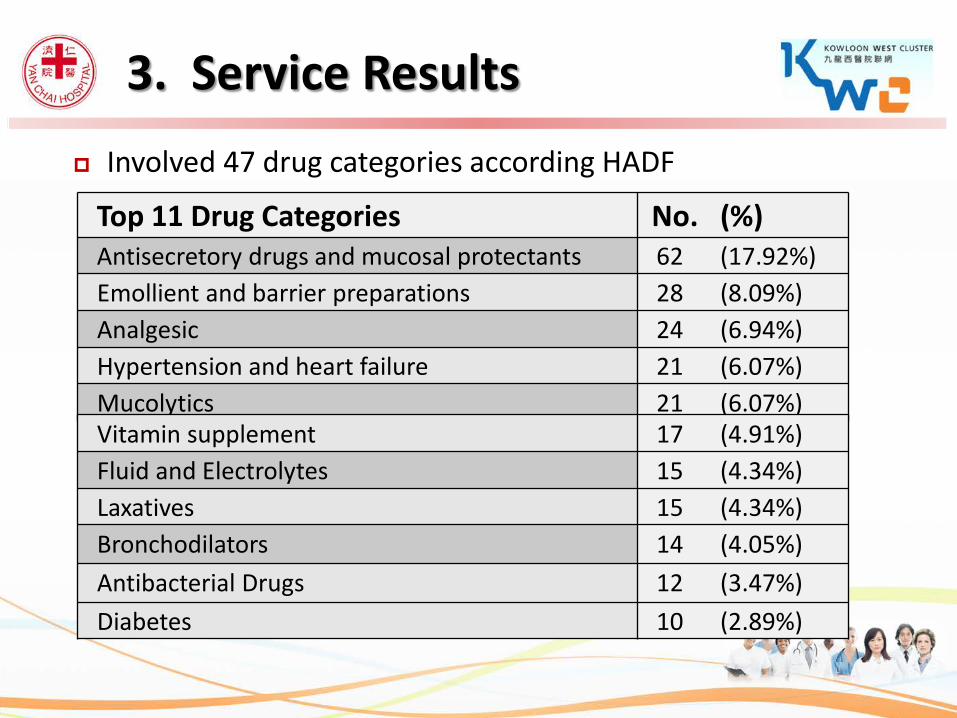
Involved 47 drug categories according HADF
Top 11 Drug Categories No. (%) Antisecretory drugs and mucosal protectants 62 (17.92%) Emollient and barrier preparations 28 (8.09%) Analgesic 24 (6.94%) Hypertension and heart failure 21 (6.07%) Mucolytics 21 (6.07%) Vitamin supplement 17 (4.91%) Fluid and Electrolytes 15 (4.34%) Laxatives 15 (4.34%) Bronchodilators 14 (4.05%) Antibacterial Drugs 12 (3.47%) Diabetes 10 (2.89%)
3. Service Results
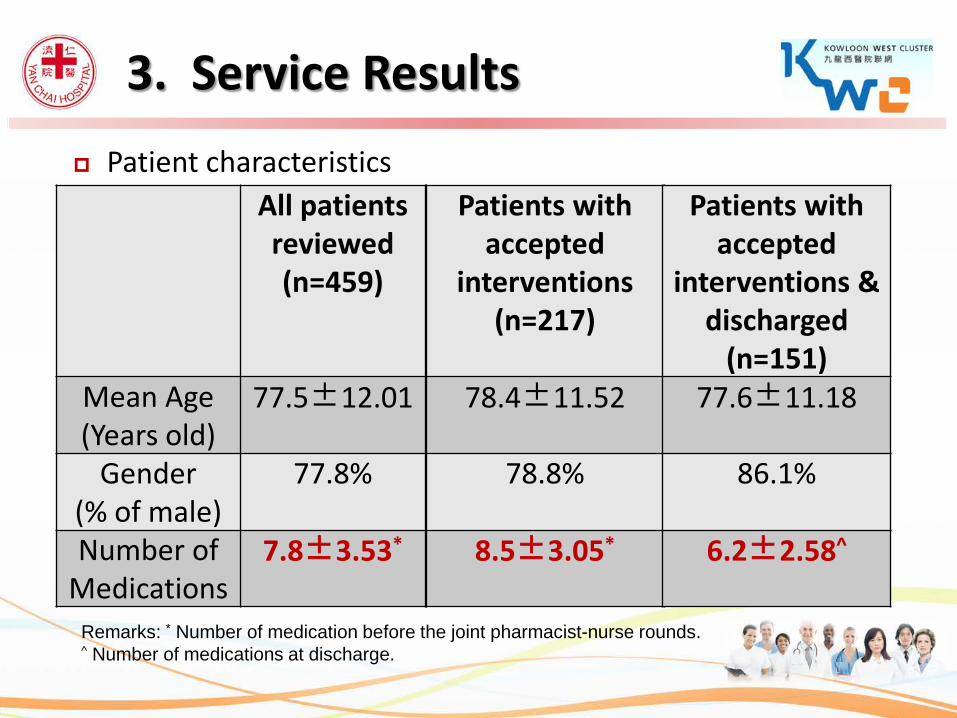
Patient characteristics
All patients reviewed (n=459)
Mean Age (Years old)
77.5±12.01
Gender (% of male)
77.8%
Number of Medications
7.8±3.53*
Remarks: * Number of medication before the joint pharmacist-nurse rounds. ^ Number of medications at discharge.
Patients with accepted
interventions (n=217)
78.4±11.52
78.8%
8.5±3.05*
Patients with accepted
interventions & discharged
(n=151) 77.6±11.18
86.1%
6.2±2.58^
3. Service Results
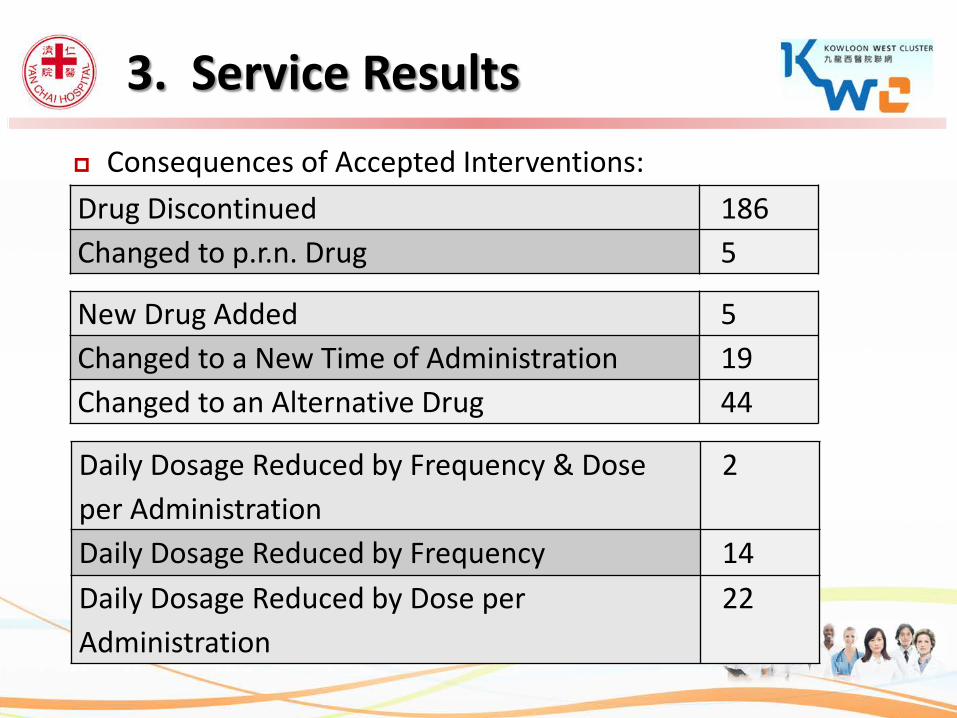
Consequences of Accepted Interventions:
Drug Discontinued 186 Changed to p.r.n. Drug 5
Daily Dosage Reduced by Frequency & Dose per Administration
2
Daily Dosage Reduced by Frequency 14 Daily Dosage Reduced by Dose per Administration
22
3. Service Results
New Drug Added 5 Changed to a New Time of Administration 19 Changed to an Alternative Drug 44
Consequences of Accepted Interventions:
3. Service Results
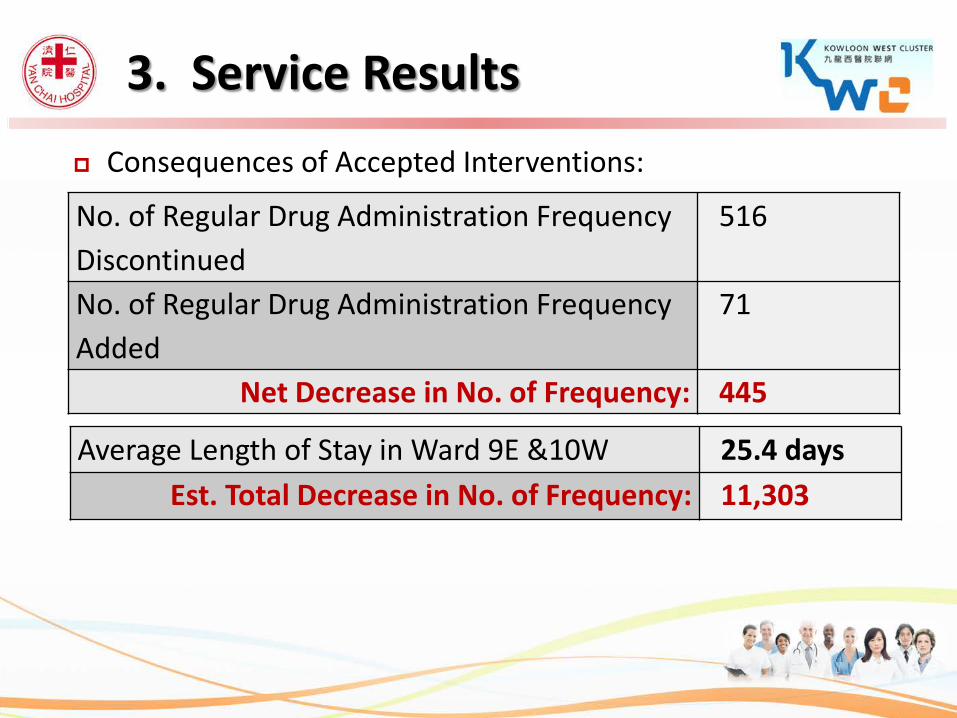
No. of Regular Drug Administration Frequency Discontinued
516
No. of Regular Drug Administration Frequency Added
71
Net Decrease in No. of Frequency: 445
Average Length of Stay in Ward 9E &10W 25.4 days Est. Total Decrease in No. of Frequency: 11,303
Hatoum Scale: Score system used in many previous trials to evaluate clinical significance of interventions8-13
Each accepted intervention was reviewed by an expert panel using Hatoum Scale: 1 senior geriatrician 1 nursing professor 2 pharmacy lecturers
All panel members were independent to our hospital & none of them were involved in any of the intervention
8. Harrison JJ, Wang J, Cervenko J, Jackson L, Munyal D, Hamandi B, et al. Pilot study of a pharmaceutical care intervention in an outpatient lung transplant clinic. Clin Transplant 2012:26:E149–E157. 9. Nerich V, Limat S, Demarchi M, Borq C, Rohrlich PS, Deconinck, et al. Computerized physician order entry of injectable antineoplastic drugs: An epidemiologic study of prescribing medication errors. International Journal of Medical Informatics 2010;79(10):699-706. 10. Fernández-Llamazares CM, Calleja-Hernandez MA, Manrique-Rodriguez S, Pérez-Sanz C, Duran-García E, Sanjurjo-Saez M. Impact of clinical pharmacist interventions inreducing paediatric prescribing errors. Arch Dis Child 2012;97:564–568. 11. Wang HY, Chan ALF, Chen MT, Liao CH, Tian YF. Effects of Pharmaceutical Care Intervention by Clinical Pharmacists in Renal Transplant Clinics. Transplantation Proceedings 2008;40(7):2319–2323. 12. Bosma L, Jansman FGA, Franken AM, Harting JW, Van den PMLA. Evaluation of pharmacist clinical interventions in a Dutch hospital setting. Pharmacy World and Science 2008;30(1):31-38. 13. Hick HL, Deady PE, Wright DJ, Silcock J. The impact of the pharmacist on an elective general surgery pre‐admission clinic. Pharmacy World and Science 2001;23(2):65-69.
3. Service Results
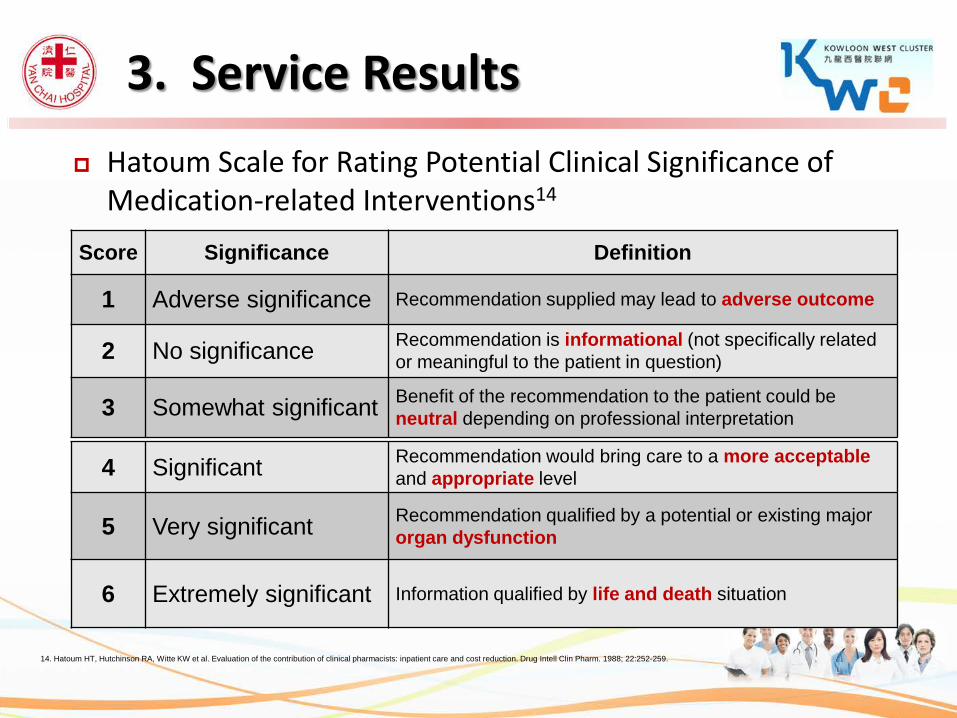
Hatoum Scale for Rating Potential Clinical Significance of Medication-related Interventions14
14. Hatoum HT, Hutchinson RA, Witte KW et al. Evaluation of the contribution of clinical pharmacists: inpatient care and cost reduction. Drug Intell Clin Pharm. 1988; 22:252-259.
Score Significance Definition
1 Adverse significance Recommendation supplied may lead to adverse outcome
2 No significance Recommendation is informational (not specifically related or meaningful to the patient in question)
3 Somewhat significant Benefit of the recommendation to the patient could be neutral depending on professional interpretation
4 Significant Recommendation would bring care to a more acceptable and appropriate level
5 Very significant Recommendation qualified by a potential or existing major organ dysfunction
6 Extremely significant Information qualified by life and death situation
3. Service Results
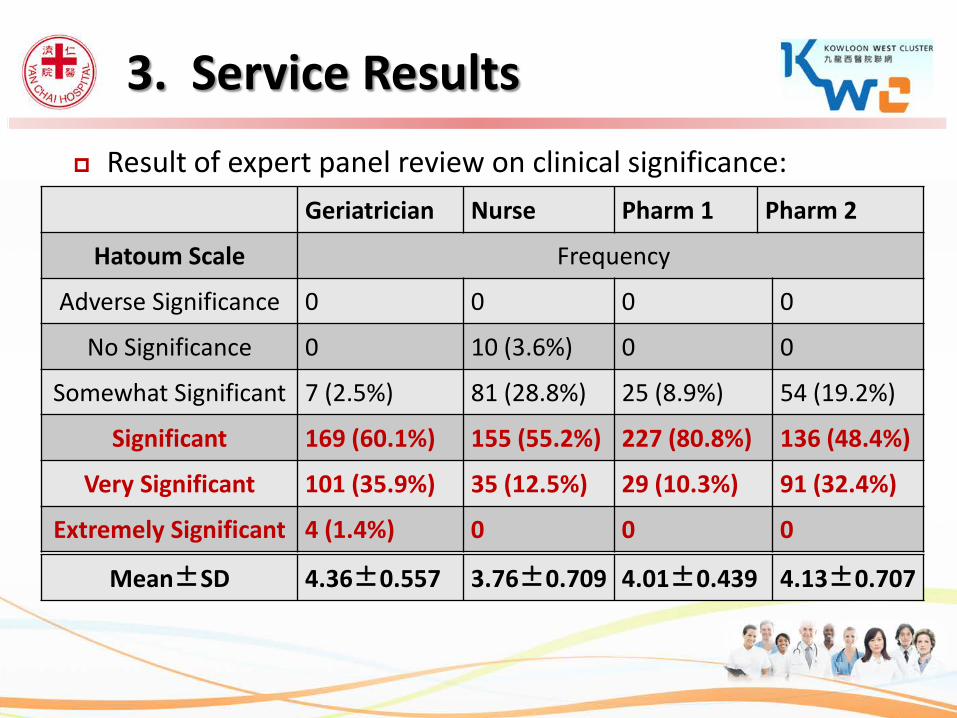
Result of expert panel review on clinical significance: Geriatrician Nurse Pharm 1 Pharm 2
Hatoum Scale Frequency
Adverse Significance 0 0 0 0
No Significance 0 10 (3.6%) 0 0
Somewhat Significant 7 (2.5%) 81 (28.8%) 25 (8.9%) 54 (19.2%)
Significant 169 (60.1%) 155 (55.2%) 227 (80.8%) 136 (48.4%)
Very Significant 101 (35.9%) 35 (12.5%) 29 (10.3%) 91 (32.4%)
Extremely Significant 4 (1.4%) 0 0 0
Mean±SD 4.36±0.557 3.76±0.709 4.01±0.439 4.13±0.707
3. Service Results
The % of accepted interventions being rated as significant, very significant, & extremely significant: Senior geriatrician: 97.4% Nursing professor: 67.5% 2 pharmacy lecturers: 91.1% and 80.8%
The Intraclass Correlation Coefficient: 0.693
3. Service Results
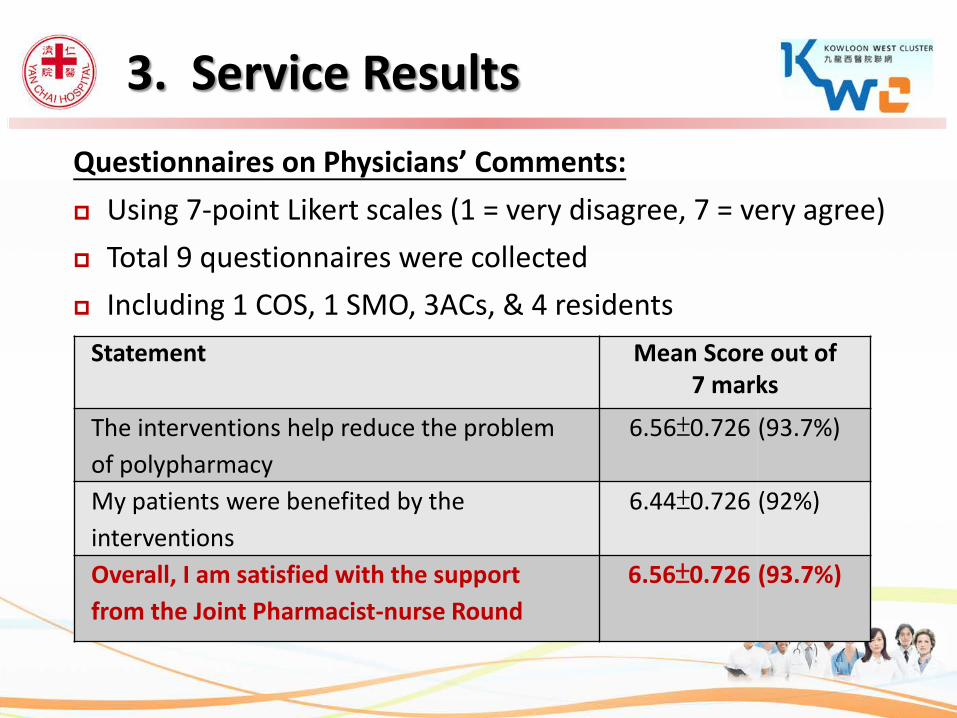
Questionnaires on Physicians’ Comments: Using 7-point Likert scales (1 = very disagree, 7 = very agree) Total 9 questionnaires were collected Including 1 COS, 1 SMO, 3ACs, & 4 residents
Statement Mean Score out of 7 marks
The interventions help reduce the problem of polypharmacy
6.56±0.726 (93.7%)
My patients were benefited by the interventions
6.44±0.726 (92%)
Overall, I am satisfied with the support from the Joint Pharmacist-nurse Round
6.56±0.726 (93.7%)
3. Service Results
Tackling medication-related problems in geriatric patients by a multidisciplinary approach was well accepted by physicians and nurses.
Provide better patient care through professional teamwork Significant decrease in numbers of unnecessary drugs and
administration frequencies were achieved. Should be further developed to enhance medication safety &
quality of life of our patients.
4. Conclusion
Thank You!
Q & A