Embed Size (px)
Citation preview

This article was downloaded by: [University Federal Do Parana]On: 21 February 2013, At: 08:58Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office:Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Sports SciencesPublication details, including instructions for authors and subscriptioninformation:http://www.tandfonline.com/loi/rjsp20
The Conconi test is not valid for estimation ofthe lactate turnpoint in runnersAndrew M. Jones & Jonathan H. DoustVersion of record first published: 26 Nov 2010.
To cite this article: Andrew M. Jones & Jonathan H. Doust (1997): The Conconi test is not valid for estimationof the lactate turnpoint in runners, Journal of Sports Sciences, 15:4, 385-394
To link to this article: http://dx.doi.org/10.1080/026404197367173
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Any substantialor systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that thecontents will be complete or accurate or up to date. The accuracy of any instructions, formulae, anddrug doses should be independently verified with primary sources. The publisher shall not be liablefor any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoevercaused arising directly or indirectly in connection with or arising out of the use of this material.

The Conconi test is not valid for estimation of the
lactate turnpoint in runners
ANDREW M. JONES* and JONATHAN H. DOUST
Human Performance Laboratory, Chelsea School Research Centre, University of B r ighton, Eastbourne B N20 7SP,
UK
Accepted 16 October 1996
Conconi et al. (1982) reported that an observed deviation from linearity in the heart rate-running velocity
relationship determined during a ® eld test in runners coincided with the `lactate threshold’ . The aim of this
study was to assess the validity of the original Conconi test using conventional incremental and constant-load
laboratory protocols. Fourteen trained male distance runners (mean 6 s: age 22.6 6 3.4 years; body mass
67.6 6 4.8 kg; peak ÇVO2 66.3 6 4.7 ml kg- 1 min- 1) performed a standard multi-stage test for determination of
lactate turnpoint and a Conconi test on a motorized treadmill. A deviation from linearity in heart rate was
observed in nine subjects. Signi® cant differences were found to exist between running velocity at the lactate
turnpoint (4.39 6 0.20 m s- 1) and at deviation from linear heart rate (5.08 6 0.25 m s- 1) (P < 0.01), and
between heart rate at the lactate turnpoint (172 6 10 beats min- 1) and at deviation from linearity (186 6 9
beats min- 1) (P < 0.01). When deviation of heart rate from linearity was evident, it occurred at a systematically
higher intensity than the lactate turnpoint and at approximately 95% of maximum heart rate. These results
were con® rmed by the physiological responses of seven subjects, who performed two constant-velocity
treadmill runs at 0.14 m s- 1 below the running velocity at the lactate turnpoint and that at which the heart rate
deviated from linearity. For the lactate turnpoint trial, the prescribed 30 min exercise period was completed by
all runners (terminal blood lactate concentration of 2.4 6 0.5 mM ), while the duration attained in the trial for
which heart rate deviated from linearity was 15.9 6 6.7 min (terminal blood lactate concentration of 8.1 6 1.8
mM ). We concluded that the Conconi test is invalid for the non-invasive determination of the lactate turnpoint
and that the deviation of heart rate from linearity represents the start of the plateau at maximal heart rate, the
expression of which is dependent upon the speci® cs of the Conconi test protocol.
Keywords : Conconi test, lactate turnpoint, running intensity.
Introduction
The `anaerobic threshold’ , de® ned as the exercise ÇVO2
above which anaerobic high-energy phosphate produc-
tion supplements aerobic high-energy phosphate pro-
duction (Wasserman et al., 1994), has long been
recognized as an important determinant of endurance
exercise performance (Davies and Thompson, 1979;
Sjodin and Jacobs, 1981; Tanaka et al., 1986). The
determination of the anaerobic threshold has tradition-
ally required laboratory exercise and blood sampling
procedures for the assessment of the exercise intensity
above which lactate starts to accumulate in the blood
(lactate threshold), or sophisticated gas analysis appa-
ratus if the anaerobic threshold is de® ned by non-inva-
sive gas exchange methods (Wasserman et al., 1973).
Conconi et al. (1982) reported the development of a
non-invasive ® eld test of the anaerobic threshold after
hypothesizing that anaerobic energy production would
`spare’ aerobic demand and result in a reduced rate of
increase in ÇVO2 (and heart rate) above the anaerobic
threshold. This test, which was to become known as the
`Conconi test’ , was simply based upon the relationship
*Address all correspondence to Andrew M. Jones, Department of
Exercise and Sport Science, the Manchester Metropolitan Univer-
sity, Crewe + Alsager Faculty, Hassall Road, Alsager, Cheshire ST7
2HL, UK.
0264-0414/97 © 1997 E & FN Spon
Journal of Sports Sciences, 1997, 15, 385-394
Dow
nloa
ded
by [
Uni
vers
ity F
eder
al D
o Pa
rana
] at
08:
58 2
1 Fe
brua
ry 2
013

between heart rate and running velocity in runners per-
forming an incremental exercise protocol. Conconi et
al. (1982) reported that beyond a certain submaximal
running velocity, the previously linear relationship
between heart rate and running velocity was lost, such
that the increase in running velocity exceeded the
increase in heart rate. The Conconi group validated this
point of deviation in heart rate against measurements
of blood lactate obtained during an unconventional
protocol in the ® eld, and reported coincidence between
running velocity at which heart rate deviated from lin-
earity and that at the `lactate threshold’ (Conconi et al.,
1982). The Conconi method was later supported in a
number of other activities (Droghetti et al., 1985; Cel-
lini et al., 1986; Droghetti, 1986) and population
groups (Maffulli et al., 1987; Ballarin et al., 1989; Bar-
aldi et al., 1989) using Conconi’s original techniques.
In Europe, the Conconi test is now widely used to
assess endurance capacity and to guide training pre-
scription.
Recently, a number of studies have independently
assessed the validity of the Conconi test, but these have
produced contradictory results. Some studies have
demonstrated disparity between the exercise intensities
corresponding to a deviation in heart rate from linearity
and to the anaerobic threshold (Kuipers et al., 1988;
Tokmakidis and Leger, 1988, 1992; Francis et al.,
1989; Zacharogiannis and Farrally, 1993), whereas
others have con® rmed the validity of the method (Hof-
mann et al., 1994; Bunc et al., 1995). However, the
blood lactate or gas exchange criteria used to de ® ne the
anaerobic threshold have differed between studies, with
some authors using the second lactate threshold or lac-
tate turnpoint in their comparisons (Hofmann et al.,
1994; Bunc et al., 1995; Pokan et al., 1995). In addi-
tion, the methods used to compare the Conconi test
with these criteria are at times open to criticism. Con-
coni et al. (1982) used an incremental protocol of ® xed
distance (and thus a reducing stage duration) to facili-
tate ® eld testing, but others (Ribeiro et al., 1985; Kuip-
ers et al., 1988; Francis et al., 1989; Zacharogiannis
and Farrally, 1993; Hofmann et al., 1994; Bunc et al.,
1995; Pokan et al., 1995) have used modi® cations of
the original Conconi test protocol. Only two studies
(Heck and Hollmann, 1992; Hofmann et al., 1994),
both of which used cycle ergometry, have attempted to
examine the physiological responses of subjects to con-
tinuous exercise at or close to the point at which heart
rate deviates from linearity. Evaluation of the physio-
logical responses to constant-load exercise is useful in
determining the effectiveness of training prescriptions
based on the results of incremental tests. This lack of
data makes it dif® cult to evaluate the validity of the
Conconi test.
The aim of this study was to assess the validity of the
Conconi test as originally reported (Conconi et al.,
1982) using conventional incremental and constant-
load laboratory protocols in well-trained distance
runners.
Methods
Subjects
Fourteen male distance runners provided written
informed consent once the possible risks and bene® ts
of the experimental procedures were fully explained to
them. The study was approved by the Chelsea School
Ethics Committee. All subjects were well-trained and
experienced in laboratory exercise testing procedures.
Their mean ( 6 s) age, height, body mass, sum of four
skinfolds (Durnin and Womersley, 1974), ÇVO2 peak
and maximal heart rate (determined during the lactate
turnpoint test, see below) were 22 6 3 years, 176 6 5
cm, 67.6 6 4.8 kg, 25.4 6 4.6 mm, 66.3 6 4.7 ml kg-1
min-1 and 195 6 10 beats min-1 , respectively. The sub-
jects were instructed to arrive at the laboratory for test-
ing in a rested and fully hydrated state. The exercise
tests took place at least 4 h after eating and at the same
time of day to minimize the effects of diurnal biological
variability (Reilly et al., 1984). The detailed training
records kept by the subjects over the course of the
study con® rmed that the laboratory visits were pre-
ceded by a day or two of rest or very light training.
General procedures
All exercise tests were undertaken on a motorized
Woodway ELG2 treadmill (CadioKinetics, Salford,
UK) set at 1% grade to compensate for the lack of air
resistance during treadmill running such that the ener-
getic cost was equivalent to running outdoors (Jones
and Doust, 1996). The subjects performed a consistent
individual warm-up before each treadmill test, and
wore the same running shoes and lightweight running
apparel on each occasion. During all tests, heart rate
was recorded every 5 s with an ECG-calibrated Polar
Sport Tester heart rate monitor (Polar Electro, Kem-
pele, Finland).
Study 1: Determination of the point at which heart rate
deviates from linearity and of the lactate turnpoint
The aim of this ® rst study was to assess the validity of
the deviation in heart rate from linearity in the non-
invasive identi® cation of the work intensity correspond-
ing to the lactate turnpoint derived from a conventional
386 Jones and Doust
Dow
nloa
ded
by [
Uni
vers
ity F
eder
al D
o Pa
rana
] at
08:
58 2
1 Fe
brua
ry 2
013

multi-stage laboratory protocol. The Conconi test and
the lactate turnpoint test were presented in random
order separated by 3-8 days.
For the Conconi test, subjects began running at a
submaximal velocity of 3.33 m s- 1, reached over a
period of 1-2 min. Running velocity was then increased
by 0.14 m s- 1 at the completion of each consecutive
200 m according to the speci® cations of Conconi et al.
(1982). Increments in running velocity were attained
within 5 s. The heart rates recorded at the completion
of each 200 m stage were used in the subsequent gen-
eration of individual heart rate-running velocity plots
(Conconi et al., 1982).
For the assessment of the lactate turnpoint, the sub-
jects completed ® ve to seven exercise stages of 4 min
duration at a submaximal running velocity estimated to
require 60-90% of individual peak ÇVO2. This protocol
was similar to that recently validated by Weltman et al.
(1990). The tests began at 3.61-4.17 m s- 1 depending
on the ability of the subject, and running velocity was
increased by 0.28 m s- 1 at the completion of each stage.
Serial collections of expired air into Douglas bags were
made during the last minute of each stage for subse-
quent calculation of respiratory gas exchange variables
by standard formulae. The concentration of O2 and
CO2 in the expired air was determined by sampling
through a paramagnetic transducer (Servomex Series
100, Crowborough, UK) and an infrared analyser (Ser-
vomex Model 1490), respectively. The gas analysers
were calibrated before and after each test using certi-
® ed standard gases. Volumes were determined using a
dry gas meter (Harvard Instruments, Edenbridge,
UK), previously calibrated against a Tissot spirometer.
On completion of each exercise stage, running was
brie¯ y interrupted to allow the collection of ® ngertip
capillary blood samples. The ® ngertip was cleaned with
an alcohol swab, dried and punctured with an auto-
mated lancet before 30 m l of blood were collected in a
capillary tube containing a ¯ uoride/heparin/nitrite mix-
ture. In general, the interruptions in exercise did not
exceed 20 s. It has been demonstrated that blood lac-
tate concentrations are not altered signi® cantly when
30 s breaks are taken between exercise stages of 4 min
duration (Gullstrand et al., 1994). Following mixing,
the blood was assayed in duplicate for whole blood lac-
tate concentration (Analox GM7, UK).
The lactate turnpoint test was also used for the
determination of peak ÇVO2 . After completion of the
® nal submaximal stage, the treadmill grade was
increased to 5% to elicit a supramaximal workload. The
subjects were encouraged to run for as long as possible
for this ® nal stage, during which expired air was col-
lected every 30 s. Volitional exhaustion was normally
reached in 3-4 min. The highest ÇVO2 recorded in any
30 s period was taken as the peak ÇVO2 value.
The data were plotted, coded and presented blindly
to two experienced physiologists who were asked to
identify: (1) the running velocity at which heart rate
began to increase less rapidly with increments in run-
ning velocity during the Conconi test (i.e. the ® rst clear
departure from linearity in the heart rate-running
velocity plots), and (2) the running velocity at which
the second `sudden and sustained’ increase in blood
lactate occurred (Davis et al., 1983; Hofmann et al.,
1994; Bunc et al., 1995). The lactate turnpoint occurs
at an appreciably higher metabolic rate than the `® rst’
lactate threshold described in the early literature, which
referred to a clear increase in arterial blood lactate
above baseline (Wasserman et al., 1973). In well-
trained runners, the lactate turnpoint typically occurs
at 75-85% ÇVO2 max, and lies between a blood lactate
concentration of 2.5 and 4.0 mM when whole blood is
assayed (Jones and Doust, 1994). When the two
reviewers were unable to agree in the determination of
the lactate turnpoint or the point at which heart rate
deviated from linearity (approximately 10% of cases), a
third reviewer acted as arbitrator. Running velocity at a
blood lactate concentration of 4 mM was determined by
interpolation (Heck et al., 1985).
Study 2: Performance at running intensities corresponding
to the point at which heart rate deviates from linearity
and at the lactate turnpoint
To assess the physiological responses to training pre-
scriptions made from determination of the lactate turn-
point and the point at which heart rate deviates from
linearity, seven of the nine subjects who demonstrated
such a deviation in linearity in Study 1 agreed to per-
form constant-velocity treadmill runs at 0.14 m s- 1
below the running velocity at the lactate turnpoint and
the point at which heart rate deviates from linearity.
These runs were performed by all subjects within 2
weeks of the completion of Study 1, were presented in
random order and were separated by 2-5 days. It was
hypothesized that if these two conditions provided good
estimates of the maximal lactate steady-state for con-
tinuous constant-load exercise, then subjects should be
capable of sustaining work at these running velocities
for 30 min without any appreciable accumulation of
blood lactate. The runs were performed at 0.14 m s- 1
below the lactate turnpoint and below the point at
which the heart deviates from linearity because 0.14 m
s- 1 represented the minimum possible error in the
determination of the latter condition. For both runs,
the prescribed running velocity was reached over a
The Conconi test and the lactate turnpoint 387
Dow
nloa
ded
by [
Uni
vers
ity F
eder
al D
o Pa
rana
] at
08:
58 2
1 Fe
brua
ry 2
013

period of 2 min, and the subjects then ran for 30 min or
to exhaustion if this occurred before 30 min had
elapsed. Heart rate was recorded throughout the runs,
and blood lactate determinations were made every 5
min throughout the runs and at exhaustion, as descri-
bed above.
Statistical analysis
The signi® cance of differences between data sets were
analysed by one-way analysis of variance with paired t-
tests where appropriate. Pearson product-moment cor-
relation coef® cients were used to test for relationships
between variables. Simple linear regression analysis was
used to create individual regression equations of the
form ÇVO2 = mv + c, where v = running velocity. While
we appreciate that the kinetics of ÇVO2 are considerably
more complex above the anaerobic threshold (Barstow
and Mole, 1991), this approach was used simply to
provide an estimate of the ÇVO2 required at the devia-
tion of heart rate from linearity. The 5% level was cho-
sen a priori to represent statistical signi® cance.
Results
Study 1: Comparison of the point at which heart rate
deviates from linearity and the lactate turnpoint
For the Conconi test, a deviation in heart rate from
linearity was noted in nine subjects with the remaining
® ve subjects demonstrating linear relationships between
heart rate and running velocity (Table 1 and Fig. 1).
On average, the running velocity at which heart rate
deviated from linearity was 13% higher than that at the
lactate turnpoint (P < 0.01), and 8% higher than at a
blood lactate concentration of 4 mM (P < 0.01) (Table
1 and Fig. 2). A signi® cant difference was also noted
between the running velocity at the lactate turnpoint
and that at a blood lactate concentration of 4 mM
(P < 0.01). Signi® cant correlations (P < 0.05) existed
between the running velocities at which heart rate
deviated from linearity and at the lactate turnpoint
(r = 0.73), those at which heart rate deviated from lin-
earity and at a blood lactate concentration of 4 mM
(r = 0.74), and those at the lactate turnpoint and at a
blood lactate concentration of 4 mM (r = 0.87).
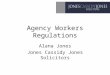
Figure 1 Representative demonstration of a linear relationship between heart rate and running velocity (subject C.R.) and the
existence of the heart rate deviation point (subject T.A.).
388 Jones and Doust
Dow
nloa
ded
by [
Uni
vers
ity F
eder
al D
o Pa
rana
] at
08:
58 2
1 Fe
brua
ry 2
013

Signi® cant differences were noted between heart rate
at the lactate turnpoint and at deviation from linearity
(P < 0.01), and between heart rate at the lactate turn-
point and at a blood lactate concentration of 4 mM
(P < 0.01) (Table 1). There was a signi® cant difference
between heart rate at a blood lactate concentration of 4
mM and at deviation from linearity (P < 0.05). Signi® -
cant correlations (P < 0.05) were found to exist
between heart rate at the lactate turnpoint and at devia-
tion from linearity (r = 0.89), between heart rate at a
blood lactate concentration of 4 mM and at deviation
from linearity (r = 0.74), and between heart rate at the
lactate turnpoint and at a blood lactate concentration
of 4 mM (r = 0.87)
Extrapolation of individual regression equations ofÇVO2 on running velocity, calculated from data collected
during the lactate turnpoint test, indicated that the
running velocity at the point at which heart rate devia-
ted from linearity would require 93.0 6 8.3% of peakÇVO2. This was signi® cantly higher than the percentage
of peak ÇVO2 used at the lactate turnpoint
(80.8 6 3.4%) (P < 0.01).
Table 1 Running velocity (RV) and heart rate (HR) at the lactate turnpoint (LTP), at a blood
lactate concentration of 4 mM and at the Concini test heart rate deviation point (HRd ev)
LTP 4 mM HRd ev
Subject
RV
(m s- 1)
HR
(beats min- 1)
RV
(m s- 1)
HR
(beats min- 1)
RV
(m s- 1)
HR
(beats min- 1)
T.A. 4.72 168 5.25 183 5.14 177
R.H. 4.31 163 4.33 165 5.00 184
S.W. 4.17 176 4.22 179 4.58 180
D.L. 4.44 183 4.58 188 5.00 190
D.R. 4.44 163 4.94 174 5.42 177
G.B. 4.31 178 4.33 182 5.00 191
A.V. 4.58 165 4.78 175 5.14 177
R.M. 4.31 180 4.75 189 5.00 191
S.O. 4.72 194 5.00 200 5.42 204
I.G. 4.17 178 4.31 183 N.D. N .D.
C.S. 4.03 170 4.06 172 N.D. N .D.
C.R. 4.31 173 4.67 187 N.D. N .D.
D.J. 4.44 156 4.83 175 N.D. N .D.
S.B. 4.44 156 4.64 160 N.D. N .D.
Mean 4.39 172 4.62 179 5.08 186
s 0.2 10 0.34 10 0.25 9
N .D. 5 no heart rate deviation point observed.
Table 2 Physiological responses to constant-velocity running at 0.5 km h- 1 below the lactate turnpoint (LTP) and
0.5 km h- 1 below the heart rate deviation point (HRd ev)
Subject
RV-LTP
(m s- 1)
Time
(min)
BLa
(mM )
HR
(beats min- 1)
RV-HRd ev
(m s- 1)
Time
(min)
BLa
(mM )
HR
(beats min- 1)
T.A. 4.58 30 3 175 5 30 4.9 187
R.H. 4.17 30 2.4 164 4.86 18 10 191
D.L. 4.31 30 2.8 177 4.86 13 9.5 194
D.R. 4.31 30 1.5 159 5.28 10 9.3 178
G.B. 4.17 30 2.5 175 4.86 15 8.7 191
A.V. 4.44 30 2.6 156 5 14 7.9 188
R.M. 4.17 30 2.2 175 4.86 11.5 6.5 189
Mean 4.31 30 2.4 169 4.97 15.9 8.1 188
s 0.39 0 0.5 9 0.39 6.7 1.8 5
Abbreviations: RV-LTP, running velocity at the lactate turnpoint; RV-HRd e v, running velocity at HRd ev ; BLa, blood lactate concentra-
tion.
The Conconi test and the lactate turnpoint 389
Dow
nloa
ded
by [
Uni
vers
ity F
eder
al D
o Pa
rana
] at
08:
58 2
1 Fe
brua
ry 2
013

Study 2: Physiolog ical responses at running intensities
corresponding to the point at which heart rate deviates
from linearity and at the lactate turnpoint
All seven subjects completed 30 min of running at 0.14
m s- 1 below the running velocity at the lactate turn-
point (Table 2). Heart rate increased slightly (by about
5-10 beats min- 1) over the 30 min period to reach
169 6 9 beats min-1 . Blood lactate was stable over the
30 min (on average there was a 0.1 mM increase in
blood lactate from 10 to 30 min) (Fig. 3). The mean
blood lactate concentration at the completion of the 30
min run (2.4 6 0.5 mM ) did not differ signi® cantly
from the mean blood lactate concentration at the lac-
tate turnpoint.
Only one subject was able to complete the 30 min
run at 0.14 m s- 1 below the running velocity at which
heart rate deviated from linearity. All other subjects ter-
minated exercise before 30 min had elapsed due to gen-
eral fatigue. For the group as a whole, mean exercise
duration at this intensity was 15.9 6 6.7 min (range
10-30 min) (Fig. 3). Blood lactate did not attain a
steady-state at this running velocity in any subject;
rather, blood lactate rose continuously until exercise
was terminated. The mean blood lactate concentration
measured at termination of exercise was 8.1 6 1.8 mM
(range 4.9-10.0 mM ). Mean heart rate at the termina-
tion of exercise was 188 6 5 beats min-1, equal to 99%
of maximal heart rate.
Discussion
The Conconi test was originally designed for the non-
invasive determination of the anaerobic threshold in the
® eld. Although our experiments were laboratory-based,
we contend that if the point at which heart rate deviates
from linearity is a viable physiological phenomenon,
then it should be equally demonstrable using identical
procedures under controlled conditions in the labora-
tory.
Using the Conconi protocol under laboratory condi-
tions, 9 of 14 subjects tested demonstrated a deviation
in heart rate linearity. The remaining ® ve subjects
exhibited a linear relationship between heart rate and
running velocity. This failure to observe reliably in all
Figure 2 Location of the lactate turnpoint (LTP), 4 mM blood lactate concentration and heart rate deviation point (HRd ev) in
a typical subject (A.V.).
390 Jones and Doust
Dow
nloa
ded
by [
Uni
vers
ity F
eder
al D
o Pa
rana
] at
08:
58 2
1 Fe
brua
ry 2
013

subjects a deviation in heart rate from linearity has
been reported previously and has been recognized as a
limitation to the Conconi test (Ribeiro et al., 1985;
Kuipers et al., 1988; Tokmakidis and Leger, 1988;
Heck and Hollmann, 1992; Jones and Doust, 1995).
The running velocity at which heart rate deviates
from linearity, measured using the Conconi test proto-
col, was found to be signi® cantly higher than that at the
lactate turnpoint and at a blood lactate concentration
of 4 mM , measured during a conventional multi-stage
protocol. These results con® rm those of Tokmakidis
and Leger (1992), who, using similar methods, repor-
ted a signi® cant difference between running velocity at
the point at which heart rate deviates from linearity and
that at the lactate threshold in 17 athletes of compara-
ble physiological status to the subjects in the present
study. This difference persisted even when more objec-
tive mathematical techniques were used (Tokmakidis
and Leger, 1992). These results suggest that the devia-
tion in heart rate from linearity is not valid for the indi-
rect estimation of the lactate turnpoint, and that the
two are subserved by different physiological mecha-
nisms. It is possible that the coincidence between the
lactate threshold and the point at which heart rate devi-
ates from linearity, reported by Conconi et al. (1982), is
the result of inadvertent methodological and mathe-
matical bias in the original validation procedure, with
these elements conspiring to produce an arti® cially ele-
vated `lactate threshold’ . Conconi et al. (1982) had
their subjects perform six 1200 m runs, three above
and three below the predetermined heart rate deviation
point, and sampled blood for lactate analysis 5 min
after the completion of each run. Their de® nition of
`lactate threshold’ was the intersection of two straight
lines drawn through the three lactate points below and
through the three lactate points above the point at
which heart rate deviates from linearity. The use of
such a procedure is likely to result in close agreement
between the lactate threshold, so de® ned, and the heart
rate deviation point (Leger and Tokmakidis, 1988).
The physiological responses of our subjects to two
constant-velocity runs, performed just below the run-
ning velocities at the lactate turnpoint and at the point
at which heart rate deviates from linearity, substanti-
ated the ® ndings of our ® rst study. All subjects (n = 7)
were able to complete 30 min of running at 0.14 m s- 1
Figure 3 Individual blood lactate responses to continuous running at 0.14 m s- 1 below the running velocity at the heart rate
deviation point (n = 7). The mean response of the individuals to running at 0.14 m s- 1 below the running velocity at the lactate
turnpoint (RV-LTP) is shown for comparison.
The Conconi test and the lactate turnpoint 391
Dow
nloa
ded
by [
Uni
vers
ity F
eder
al D
o Pa
rana
] at
08:
58 2
1 Fe
brua
ry 2
013

below the running velocity at the lactate turnpoint and
showed no symptoms of fatigue, whereas they could
only continue running for 15.9 6 6.7 min at 0.14 m s-1
below the running velocity at the heart rate deviation
point before reaching volitional exhaustion. This is the
® rst study to demonstrate that work at intensities close
to the heart rate deviation point cannot be sustained
without appreciable accumulation of blood lactate and
early fatigue during running. The large standard devia-
tion in the latter condition was due to one subject who
was able to complete the 30 min exercise period,
despite recording maximum heart rate at the end of his
test and reporting exhaustion at this point.
It should be pointed out that the constant-velocity
runs were performed at a velocity of only 3% below
that at the heart rate deviation point. The day-to-day
variability in the determination of this deviation point is
not known. It is therefore possible that, during the runs
designed to be at a running velocity that would elicit a
heart rate below that at which the heart rate deviated
from linearity, some subjects may have exceeded this
heart rate. However, there is growing evidence to sug-
gest that when the lactate turnpoint is determined
using multi-stage exercise tests with stage durations of
2-4 min and small intensity increments (as in the pres-
ent study), it provides a valid approximation of the
maximal lactate steady-state for continuous constant-
load exercise (Weltman et al., 1990; Aunola and Rusko,
1992; Jones, 1994). This would suggest that the run-
ning velocity at which heart rate deviates from linearity
is signi® cantly higher than that at the maximal lactate
steady-state. In support of this, Heck and Hollmann
(1992) reported that only 6 of 22 cyclists were able to
maintain work at 90-100% of the work intensity at the
heart rate deviation point for 30 min; the others were
forced to stop prematurely owing to fatigue. In con-
trast, Hofmann et al. (1994) concluded that the max-
imal steady-state lay within 6 10% of the power output
at the heart rate deviation point in a study of 16
untrained female students. It is possible that training
status is important when the validity of the Conconi
test is being considered. However, our results indicate
that, in well-trained distance runners, the Conconi test
will overestimate the running velocity at maximal lac-
tate steady-state and lead to high-intensity training pre-
scriptions in the majority of individuals.
In well-trained distance runners, a continuous max-
imal run of about 16 min duration (as for our subjects
when running at 0.14 m s-1 below the velocity at which
heart rate deviates from linearity in Study 2) would
require approximately 95% ÇVO2 max (Davies and
Thompson, 1979; Leger et al., 1986). This is in keeping
with the estimated ÇVO2 required to run at the velocity
at which heart deviates from linearity (93% peak ÇVO2),
calculated using the individual regression equations of
ÇVO2 on running velocity derived from the lactate turn-
point test. Our calculations are similar to those of Leger
and Tokmakidis (1988), who estimated that the run-
ning velocity at the heart rate deviation point was
equivalent to approximately 96% ÇVO2 max. It is inter-
esting that it is at this relative intensity (95% ÇVO2 max)
that heart rate characteristically begins to plateau at its
maximum value, with a widening of the arterial-venous
oxygen difference and an increase in cardiac output
being responsible for the further increase in ÇVO2 up to
the attainment of ÇVO2 max (Davies, 1968). The strong
correlation between the lactate turnpoint (or anaerobic
threshold) and the deviation in heart rate from linearity
found in this study and others (Ribeiro et al., 1985;
Heck and Hollmann, 1992; Zacharogiannis and Far-
rally, 1993), may be explained if the heart rate devia-
tion point is related to the approach to, and the
expression of, maximal heart rate, as has been sugges-
ted previously (Jones and Doust, 1995). The nature of
the Conconi test protocol ( ® xed-distance stages) dic-
tates that heart rate is recorded more frequently at high
running velocities, leading to the production of a curvi-
linear relationship between heart rate and running
velocity as the maximal heart rate is attained (Jones and
Doust, 1992). Strong correlations between physiolog-
ical parameters such as the anaerobic threshold andÇVO2 max are well established (Davies et al., 1976;
Rusko et al., 1980). In the present study, the maximum
heart rate and the heart rate at deviation from linearity
were closely related (r = 0.93), as were the maximum
heart rate and the heart rate at the lactate turnpoint
(r = 0.94).
The physiological mechanisms underpinning the
deviation of heart rate from linearity are currently in
dispute (Bunc et al., 1995; Pokan et al., 1995). Pokan et
al. (1993) used radionuclide ventricular scintigraphy to
study myocardial function during high-intensity exer-
cise and concluded that the existence of such a devia-
tion point is dependent upon an increase in the left
ventricular ejection fraction. Pokan et al. (1995) could
not demonstrate a signi® cant relationship between the
existence of the heart rate deviation point and individ-
ual patterns of increase in plasma catecholamines or
blood lactate. There would appear to be no obvious
physiological rationale to link alterations in myocardial
function with the onset of blood lactate accumulation
during submaximal exercise. In addition, Hansen et al.
(1988) used 15, 30 and 60 W min-1 ramp exercise tests
and showed that there was no reduction in the slope ofÇVO2 on power output for exercise above, compared
with exercise below, the anaerobic threshold for any
test. The results of Hansen et al. (1988) are inconsistent
with the theoretical basis to the Conconi test.
In summary, the present study has shown that the
Conconi test, as originally described (Conconi et al.,
392 Jones and Doust
Dow
nloa
ded
by [
Uni
vers
ity F
eder
al D
o Pa
rana
] at
08:
58 2
1 Fe
brua
ry 2
013

1982), is invalid for the non-invasive estimation of the
lactate turnpoint, since the running velocity and heart
rate at which the latter deviates from linearity were
found to be signi® cantly higher than the values at the
lactate turnpoint determined with a standard multi-
stage laboratory protocol.
Furthermore, this study is the ® rst to demonstrate
that continuous constant-velocity running close to the
heart rate deviation point leads to signi ® cant accumula-
tion of blood lactate and the rapid development of
fatigue in well-trained runners.
References
Aunola, S. and Rusko, H. (1992). Does anaerobic threshold
correlate with maximal lactate steady-state? Journal of
Sports Science s, 10, 309-323.
Ballarin, E., Borsetto, C., Cellini, M., Patracchini, M.,
Vitiello, P., Ziglio, P.G. and Conconi, F. (1989). Adapta-
tion of the Conconi test to children and adolescents. Inter-
national Journal of Sports M edicine, 10, 334-338.
Baraldi, E., Zanconato, S., Santuz, P.A. and Zacchello, F.
(1989). A comparison of two non-invasive methods in the
determination of the anaerobic threshold in children.
International Journal of Sports Medicine, 10, 132-134.
Barstow, T.J. and Mole, P. (1991). Linear and nonlinear char-
acteristics of oxygen uptake kinetics of heavy exercise.
Journal of Applied Physiology, 71, 2099-2106.
Bunc, V., Hofmann, P., Leitner, H. and Gaisl, G. (1995).
Veri ® cation of the heart rate threshold. European Jour nal of
Applied Physiology, 70, 263-269.
Cellini, M., Vitiello, P., Nagliati, A., Ziglio, P.G., Martinelli,
S., Ballarin, E. and Conconi, F. (1986). Noninvasive
determination of the anaerobic threshold in swimming.
International Journal of Sports Medicine, 7, 347-351.
Conconi, F., Ferrari, M., Ziglio, P.G., Droghetti, P. and
Codeca, L. (1982). Determination of the anaerobic
threshold by a noninvasive ® eld test in runners. Journal of
Applied Physiology, 52, 869-873.
Davies, C.T.M. (1968). Limitations to the prediction of max-
imum oxygen intake from cardiac frequency measure-
ments. Journal of Applied Physiology, 24, 700-706.
Davies, C.T.M. and Thompson, M.W. (1979). Aerobic per-
formance of female marathon and male ultramarathon
athletes. European Journal of Applied Physiology, 41,
233-245.
Davis, H.A., Bassett, J., Hughes, P. and Gass, G.C. (1983).
Anaerobic threshold and lactate turnpoint. European Jour-
nal of Applied Physiology, 50, 383-392.
Davis, J.A., Vodak, P., Wilmore, J.H., Vodak, J. and Kurtz, P.
(1976). Anaerobic threshold and maximal aerobic power
for three modes of exercise. Journal of Applied Physiology,
41, 544-550.
Droghetti, P. (1986). Determination of the anaerobic thresh-
old on a rowing ergometer by the relationship between
work output and heart rate. Scandinavian Journal of Sports
Science, 8, 59-62.
Droghetti, P., Borsetto, C., Casoni, I., Cellini, M., Ferrari,
M., Pauolini, A.R., Ziglio, P.G. and Conconi, F. (1985).
Non-invasive determination of the anaerobic threshold in
canoeing, cross-country skiing, cycling, roller and iceskat-
ing, rowing and walking. European Journal of Applied Physi-
ology, 53, 299-303.
Durnin, J.V.G.A. and Womersley, J. (1974). Body fat assessed
from total body density and its estimation from skinfold
thickness: Measurements on 481 men and women aged
from 16 to 72 years. B ritish Journal of Nutr ition, 32,
77-97.
Francis, K.T., McClatchey, P.R., Sumison, J.R. and Hansen,
D.E. (1989). The relationship between anaerobic thresh-
old and heart rate linearity during cycle ergometry. Euro-
pean Journal of Applied Physiology, 59, 273-277.
Gullstrand, L., Sjodin, B. and Svedenhag, J. (1994). Blood
sampling during continuous running and 30-second inter-
vals on a treadmill: Effects on the lactate threshold results?
Scandinavian Journal of M edicine and Science in Sports, 4,
239-242.
Hansen, J.E., Casaburi, R., Cooper, D.M. and Wasserman,
K. (1988). Oxygen uptake as related to work rate incre-
ment during cycle ergometer exercise. European Journal of
Applied Physiology, 57, 140-145.
Heck, H. and Hollmann, W. (1992). Identi® cation, objectiv-
ity and validity of Conconi threshold by cycle stress tests.
Osler Journal Sportsmedizin, 22, 35-53.
Heck, H., Mader, A., Hess, G., Mucke, S., Muller, R. and
Hollmann, W. (1985). Justi® cation of the 4 mmol/l lactate
threshold. International Journal of Sports M edicine, 6,
117-130.
Hofmann, P., Bunc, V., Leinter, H., Pokan, R. and Gaisl, P.
(1994). Heart rate threshold related to lactate turnpoint
and steady-state exercise on a cycle ergometer. European
Journal of Applied Physiology, 69, 132-139.
Jones, A.M. (1994). The assessment of endurance capacity in
competitive runners. Unpublished doctoral thesis, Univer-
sity of Brighton.
Jones, A.M. and Doust, J.H. (1992). Conconi’s heart rate
deviation is an artefact of ® xed distance protocol. Journal
of Sports Sciences, 10, 559.
Jones, A.M. and Doust, J.H. (1994). Disparity between exer-
cise intensity at lactate threshold and at the 4 mM blood
lactate reference value increases with maximal aerobic
power in runners. Journal of Sports Sciences, 12, 141.
Jones, A.M. and Doust, J.H. (1995). Lack of reliability in
Conconi’s heart rate de¯ ection point. International Journal
of Sports M edicine, 16, 541-544.
Jones, A.M. and Doust, J.H. (1996). A 1% treadmill grade
most accurately re¯ ects the energetic cost of outdoor run-
ning. Jour nal of Sports Sciences, 14, 321-327.
Kuipers, H., Keizer, H.A., De Vries, T., van Rijthoven, P. and
Wijts, M. (1988). Comparison of heart rate as a non-inva-
sive determinant of anaerobic threshold with the lactate
threshold when cycling. European Journal of Applied Physi-
ology, 58, 303-306.
The Conconi test and the lactate turnpoint 393
Dow
nloa
ded
by [
Uni
vers
ity F
eder
al D
o Pa
rana
] at
08:
58 2
1 Fe
brua
ry 2
013

Leger, L. and Tokmakidis, S. (1988). Use of the heart rate
de¯ ection point to assess the anaerobic threshold (letter).
Journal of Applied Physiology, 64, 1758-1759.
Leger, L.M., Mercier, D. and Gauvin, L. (1986). The rela-
tionship between % ÇVO2 max and running performance
time. In Sport and Elite Performers (edited by D.M. Land-
ers), pp. 113-119. Champaign, IL: Human Kinetics.
Maffulli, N., Sjodin, B. and Ekblom, B. (1987). A laboratory
method for non-invasive anaerobic threshold determina-
tion. Journal of Sports Medicine, 27, 419-423.
Pokan, R., Hofmann, P., Preidler, K., Leitner, H., Dusleag,
J., Eber, B., Schwaberger, G., Fuger, G.F. and Klein, W.
(1993). Correlation between in¯ ection of heart rate/work
performance curve and myocardial function in exhausting
cycle ergometer exercise. European Journal of Applied Phys-
iology, 67, 385-388.
Pokan, R., Hofmann, P., Lehmann, M., Leitner, H., Eber,
B., Gasser, R., Schwaberger, G., Schmid, P., Keul, J. and
Klein, W. (1995). Heart rate de¯ ection related to lactate
performance curve and plasma catecholamine response
during incremental cycle ergometer exercise. European
Jour nal of Applied Physiology, 70, 175-179.
Reilly, T., Robinson, G. and Minors, G.S. (1984). Some cir-
culatory responses to exercise at different times of the day.
Medicine and Science in Sports and Exercise, 16, 471-478.
Ribeiro, J.P., Fielding, R.A., Hughes, V., Black, A., Bochese,
M.A. and Knuttgen, H.G. (1985). Heart rate breakpoint
may coincide with the anaerobic and not the aerobic
threshold. International Journal of Sports Medicine, 6,
224-234.
Rusko, H., Rahkila, P. and Karvinen, B. (1980). Anaerobic
threshold, skeletal muscle enzymes and ® ber composition
in young female cross-country skiers. Acta Physiologica
Scandinavica, 108, 263-268.
Sjodin, B. and Jacobs, I. (1981). Onset of blood lactate accu-
mulation and marathon running performance. Inter na-
tional Journal of Sports M edicine, 2, 23-26.
Tanaka, K., Watanabe, H., Konishi, Y., Mitsuzono, R., Siu-
mida, S., Tanaka, S., Fukuda, T. and Nakadomo, G.
(1986). Longitudinal associations between anaerobic
threshold and distance running performance. European
Journal of Applied Physiology, 55, 248-252.
Tokmakidis, S.P. and Leger, L. (1988). External validity of
the Conconi heart rate anaerobic threshold as compared
to the lactate threshold. In Exercise Physiology: Current
Selected Research, Vol. 3 (edited by C.D. Dotson and J.H.
Humphrey), pp. 43-58. New York: AMS Press.
Tokmakidis, S.P. and Leger, L. (1992). Comparison of math-
ematically determined blood lactate and heart rate ̀ thresh-
old’ points and relationship with performance. European
Journal of Applied Physiology, 641, 309-317.
Wasserman, K., Whipp, B.J., Koyal, S.N. and Beaver, W.L.
(1973). Anaerobic threshold and respiratory gas exchange
during exercise. Journal of Applied Physiology, 35,
236-243.
Wasserman, K., Hansen, J.E., Sue, D.Y., Whipp, B.J. and
Casaburi, R. (1994). Principles of Exercise Testing and Inter-
pretation. Philadelphia, PA: Lea and Febiger.
Weltman, A., Snead, D., Steim, P., Seip, R., Rutt, R. and
Weltman, J. (1990). Reliability and validity of a continu-
ous incremental protocol for the determination of lactate
threshold, ® xed blood lactate concentrations, and ÇVO2
max. International Journal of Sports Medicine, 11, 26-32.
Zacharogiannis, E. and Farrally, M. (1993). Ventilatory
threshold, heart rate de¯ ection point and middle distance
running performance. Journal of Sports M edicine and Phys-
ical Fitness, 33, 337-347.
394 Jones and Doust
Dow
nloa
ded
by [
Uni
vers
ity F
eder
al D
o Pa
rana
] at
08:
58 2
1 Fe
brua
ry 2
013