Embed Size (px)
Citation preview
RESEARCH LETTER
Keppen–Lubinsky Syndrome: Expandingthe PhenotypeLina Basel-Vanagaite,1,2* Lisa Shaffer,3 and David Chitayat4,5
1Schneider Children’s Medical Center of Israel, Raphael Recanati Genetics Institute, Rabin Medical Center, Beilinson Hospital,
Petah Tikva, Israel2Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel3Signature Genomic Laboratories, Spokane, Washington4Divisions of Clinical and Metabolic Genetics, The Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada5The Prenatal Diagnosis and Medical Genetics Program, Department of Obstetrics and Gynecology, Mount Sinai Hospital,
University of Toronto, Toronto, Ontario, Canada
Received 1 March 2009; Accepted 9 May 2009
TO THE EDITOR:
Keppen–Lubinsky syndrome is a rare condition characterized by
severely reduced facial adipose tissue and thin facial skin combined
with severe developmental delay and hypertonia [Gorlin et al.,
2001]. The pathogenesis of this syndrome is unknown. Since the
description of the original case in 2001, only one additional report
has been published on a child with a similar phenotype [De Brasi
et al., 2003]. We report on a third case of Keppen–Lubinsky
syndrome presenting with previously undescribed clinical features.
The propositus, a boy, was the second child born to non-
consanguineous Jewish parents of Yemenite origin. The 22-year-
old mother and 21-year-old father are both healthy. The couple has
two healthy sons and one healthy daughter, but also had three
previous miscarriages each at 2 months gestation. The pregnancy
with the propositus was uncomplicated. Maternal serum screen was
performed in the second trimester and did not show an increased
risk for trisomy 21, trisomy 18 or open neural tube defect; detailed
fetal ultrasounds at 15 and 22 weeks gestation were normal. The
propositus was born at 40 weeks gestation with a birth weight of
3,300 g (50th centile). At birth he was noted to have facial
dysmorphism. The mother also recalled that he had an unusual
face, but no specific information is available.
At the age of 2 weeks he was noted to have an opisthotonic
posture in addition to breathing difficulties with upper airway
obstruction due to narrow nares. During the first year of life he was
noted to have severe developmental delay, and at 1.5 years of age he
underwent reconstruction of the nasal cartilage in order to improve
his breathing. He then started self-mutilating and chewed on his
tongue and lips, as a result of which, at 2 years of age, protective
plastic plates were put on his teeth. Between the ages of 2 and 4 years
he had many episodes of febrile seizures.
On physical examination at the age of 6 years 9 months
his head circumference was 48.5 cm (2nd centile), height 108 cm
(3rd centile), and weight 17 kg (3rd centile). He had substantially
reduced facial subcutaneous fat with tightly adherent facial skin,
frontal hair upsweep, large and prominent eyes, long eyelashes,
loose periorbital skin, pinched nose with hypoplastic alae nasi, short
philtrum, tented upper lip, open mouth and high-arched palate,
and prominent chin (Fig. 1A–E). He had a mask face with minimal
facial movements when crying or smiling. The body subcutaneous
tissue was normal. He had severe developmental delay, had no
purposeful movements and was only able to follow objects and
smile. He was able to recognize only his parents and siblings. He was
jittery, and even minimal external stimuli triggered abrupt stretch-
ing of the limbs, body arching and opisthotonic posture. There were
no signs of autonomic dysfunction or insensitivity to pain and he
had neither corneal erosions nor ulcers. Neurological examination
showed that he was able to follow objects with his eyes, but he did
not move his head in response to voices or other stimuli. He had
increased muscle tone in all four limbs, increased deep tendon
reflexes, flexor plantar responses and cogwheel rigidity of his hands.
*Correspondence to:
Lina Basel-Vanagaite, M.D., Ph.D., Raphael Recanati Genetics Institute,
Rabin Medical Center, Beilinson Hospital, Petah Tikva 49100, Israel.
E-mail: [email protected]
Published online 16 July 2009 in Wiley InterScience
(www.interscience.wiley.com)
DOI 10.1002/ajmg.a.32975
How to Cite this Article:Basel-Vanagaite L, Shaffer L, Chitayat D.
2009. Keppen–Lubinsky syndrome:
Expanding the phenotype.
Am J Med Genet Part A 149A:1827–1829.
� 2009 Wiley-Liss, Inc. 1827
The gag reflex was normal. There was no nystagmus and examina-
tion of the fundi was normal.
Laboratory investigations including CBC, peripheral blood
smear, liver function tests, urea, creatinine, cholesterol, trigly-
cerides, blood amino acids, blood lactate/pyruvate ratio, VLCFA,
homocysteine, CK, and acylcarnitines were all normal. Serum
transferrin glycosylation analysis to exclude congenital disorders
of glycosylation (CDG) was normal. Urinary uric acid, organic
acids, purines and pyrimidines as well as creatine/creatinine ratio
were all normal. CSF amino acids, pterins, folates, and neurotrans-
mitter metabolites were normal. Brain stem auditory evoked
potentials, electroretinogram, visual evoked potentials and EEG
were normal. Brain MRI was normal except for mild lateral
ventriculomegaly and increased subarachnoid spaces.
Chromosome analysis revealed a normal male karyotype (46,
XY). Maternal X inactivation studies at the androgen receptor (AR)
gene locus performed in order to exclude skewed X inactivation in
mutation carriers, a characteristic feature of a number of X-linked
mental retardation-causing genes, demonstrated non-random
X inactivation (39%:61%). Microarray analysis of 1,543 loci using
an oligonucleotide array, which includes the subtelomeres,
pericentromeric regions and known genetic syndromes performed
by Signature Genomic Laboratories� detected no abnormalities in
the DNA of this patient.
In the 4th edition of ‘‘Syndromes of the Head and Neck’’ [Gorlin
et al., 2001], a 5-year-old boy who was reported as a personal
communication had severe developmental delay, facial lipodys-
trophy, deep-set eyes, a small nose with hypoplasia of the alae nasi, a
large mouth and a tented upper lip. The author named this
condition Keppen–Lubinsky syndrome. A second patient with this
disorder was reported by De Brasi et al. in 2003; this child had
striking similarities to the first patient including normal
weight, length, and OFC at birth, failure to thrive, unique
facial appearance with almost no subcutaneous fat, generalized
paucity of subcutaneous fat, and severe psychomotor retardation.
Minimal clinical diagnostic criteria were suggested including
normal growth parameters at birth, postnatal growth failure,
characteristic facial dysmorphism with tight facial skin adherent
to the facial bones, generalized lipodystrophy, and developmental
delay.
Crisponi [1996] reported an autosomal recessive condition in
which the patients had abnormal, paroxysmal muscular contrac-
tions resembling neonatal tetanus, a large face, broad nose, ante-
verted nares, camptodactyly, hyperthermia, and sudden death.
They also had an exaggerated response to noise and tactile stimuli,
with spasmodic contractions of the face, jaw, and neck muscles and
opisthotonus, as was the case with our patient. However, unlike
the patients reported by Crisponi [1996], our patient and the one
reported by De Brasi et al. [2003], as Keppen–Lubinsky did not have
hyperthermia or contractures and had different facial features.
Several types of genetic lipodystrophies have been reported
[Garg, 2004], but severe psychomotor retardation is usually not
a feature of these conditions.
Our patient had strikingly similar features to the two patients
previously reported with Keppen–Lubinsky syndrome. However,
our patient’s lipodystrophy was restricted to the face and was milder
than in the patients described previously, with the body adipose
tissue and skin being normal. Furthermore, the blood triglyceride
levels in our patient were normal. Our patient also showed novel
clinical features including severe hyperexcitability with stretching
of the whole body in response to any stimulus and self-mutilation
causing shortening and scarring of the tongue.
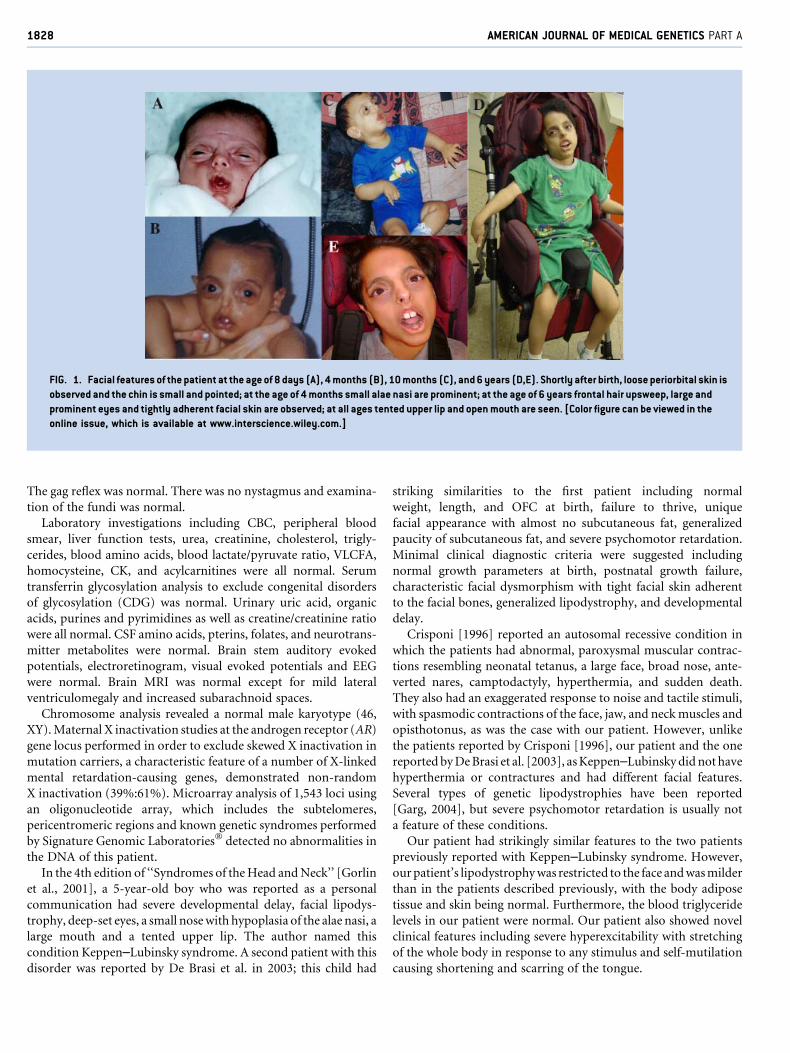
FIG. 1. Facial features of the patient at the age of 8 days (A), 4 months (B), 10 months (C), and 6 years (D,E). Shortly after birth, loose periorbital skin is
observed and the chin is small and pointed; at the age of 4 months small alae nasi are prominent; at the age of 6 years frontal hair upsweep, large and
prominent eyes and tightly adherent facial skin are observed; at all ages tented upper lip and open mouth are seen. [Color figure can be viewed in the
online issue, which is available at www.interscience.wiley.com.]
1828 AMERICAN JOURNAL OF MEDICAL GENETICS PART A

The etiology and inheritance of Keppen–Lubinsky syndrome is
unknown and the number of reported patients is too small to draw
any conclusions regarding the pattern of inheritance. So far, all
three patients reported have been males and born to non-
consanguineous parents and there were no recurrences. Of note,
no abnormalities were noted prenatally and the birth growth
parameters were normal. Thus, at this point in time, we have no
means of diagnosing the condition prenatally in a couple at risk.
Additional cases are required to further delineate the etiology and
pathogenesis of this condition.
ACKNOWLEDGMENTS
We thank Dr. Gabrielle J. Halpern for editing the manuscript and
Prof. Raoul Hennekam for stimulating scientific discussions.
REFERENCES
Crisponi G. 1996. Autosomal recessive disorder with muscle contractionsresembling neonatal tetanus, characteristic face, camptodactyly, hyper-thermia, and sudden death: A new syndrome? Am J Med Genet 62:365–371.
De Brasi D, Brunetti-Pierri N, Di Micco P, Andria G, Sebastio G. 2003. Newsyndrome with generalized lipodystrophy and a distinctive facial appear-ance: Confirmation of Keppen-Lubinski syndrome? Am J Med GenetPart A 117A:194–195.
Garg A. 2004. Acquired and inherited lipodystrophies. N Engl J Med350:1220–1234.
Gorlin RJ, Cohen MM, Hennekam RCM, editors. 2001. Keppen-Lubinskisyndrome. In: Syndromes of the head and neck, 4th edition. New York:Oxford University Press. p 1179.
BASEL-VANAGAITE ET AL. 1829