Embed Size (px)
Citation preview

KHA-CARI Autosomal Dominant Polycystic Kidney Disease Guideline:
Management of Renal Stone DiseaseAndrew Mallett, MB BS, MMed, AFRACMA, FRACP,*,† Manish Patel, MB BS, MMed, PhD, FRACS,‡
David J. Tunnicliffe, MIPH,§,II and Gopala K. Rangan, MB BS, PhD, FRACP¶,#
*KB
†C
‡D
§K
IIS
¶D
#C
Se
GUIDELINE RECOMMENDATIONS*
a. We recommend that unenhanced computed tomog-
raphy is the preferred imaging modality for the
diagnosis of suspected nephrolithiasis in autosomal
dominant polycystic kidney disease (1B).
b. We recommend that patients with autosomal-
dominant polycystic kidney disease complicated
by nephrolithiasis should be investigated for pre-
disposing urinary metabolic abnormalities (1C) and
we suggest receive corrective therapy if an abnor-
mality is identified (2D).
idnrienandResQuiscUrDisHAdreydnAuepSydenMe
mi
ey Hsbantre fC
eareensiplinologtric-CAn’seystralartmneytre fdica
nars
*Criteria used for recommendations and levels ofevidence (1,2;A-D) are described in more detail in Tables
1 and 2 of Rangan G, Savige J. Introduction to the KHA-CARI Guidelines on ADPKD. Semin Nephrol.2015;35:521-3in this issue.UNGRADED SUGGESTIONS FOR CLINICAL CARE
�
Financial support: KHA-CARI Guidelines is supported by KidneyHealth Australia, the Australian and New Zealand Society of
We suggest that in the patients with autosomal-dominant polycystic kidney disease (ADPKD) inwhom a diagnosis of nephrolithiasis is considered,that the diagnostic performance of the imagingmodality needs to be balanced against the relativerisks of these different diagnostic tests, as doeswhether or not a contrast-enhanced computed
0270-& 201http://
NepGui
ManisSan
ConflAdvticKDIADPfromboa
ealth Service and Conjoint Kidney Research Laboratory, Royale and Women’s Hospital, Brisbane, Queensland, Australia.or Kidney Disease Research, Centre for Chronic DiseaseKD, School of Medicine and Centre for Rare Diseasesch, Institute for Molecular Bioscience, The University ofland, Brisbane, Queensland, Australia.e of Surgery, University of Sydney and Department ofy, Westmead Hospital, Western Sydney Local Healtht, Westmead, Sydney, Australia.RI Guidelines, Centre for Kidney Research, The Chil-Hospital at Westmead, Westmead, Sydney, Australia.School of Public Health, University of Sydney, Sydney,ia.ent of Renal Medicine, Westmead Hospital, WesternLocal Health District, Sydney, Australia.or Transplant and Renal Research, Westmead Institute forl Research, University of Sydney, Westmead, Sydney, Australia.
AddreAFRBuiHermal
in Nephrology, Vol 35, No 6, November 2015, pp 603–606
tomography scan is required for other differentialdiagnoses or clinical indications.
�
We suggest that in the early stages of cystic renaldisease, screening for nephrolithiasis with ultra-sound may be more useful.�
We suggest that the medical management of anacute presentation with suspected nephrolithiasisin a patient with ADPKD as well as the preven-tion of recurrent stone formation should followgeneral principles recommended for the generalpopulation, with the exception that:○ A superimposed urinary tract infection shouldbe considered in the acute presentation.○ The differential diagnosis of the acute presentationshould include ruling out other causes of acuteloin pain (eg, cyst infection or hemorrhage); and
○ Screening for underlying urinary metabolicabnormalities should be considered in ADPKDpatients presenting with their first stone.
9295 Edx.
hrodelih Pofi
ictisorGooGOKDG
rd mssACldinstonlett
�
We suggest that the indications for urologicalintervention for stone removal in ADPKD dependon the clinical circumstances. If required, percuta-neous nephrolithotomy, extracorporeal shock-wave lithotripsy, or ureteroscopy with laserlithotripsy may be considered.5/ - see front matterlsevier Inc. All rights reserved.doi.org/10.1016/j.semnephrol.2015.10.012
logy, Amgen Australia, and Shire Australia Pty Ltd.ne members were not remunerated for their work.atel received an honorarium from GSK, Janssen, Astellas,and Abbvie as an advisory board member.
of interest statement: Gopala Rangan is a member of they Committee on the Safety of Medical Devices, Therapeu-ds Administration and received financial support fromto attend the KDIGO Controversies Conference onin January 2014. Manish Patel received an honorarium
SK, Janssen, Astellas, Sanofi and Abbvie as an advisoryember.reprint requests to Andrew Mallett, MB BS, MMed,MA, FRACP, Kidney Health Service, Level 9, Ned Hanlong, Royal Brisbane and Women’s Hospital, Butterfield St,, Brisbane, QLD, 4029 Australia. E-mail: [email protected]
603
A. Mallett et al.604
IMPLEMENTATION AND AUDIT
Patients with ADPKD with nephrolithiasis should bereferred to urology services to receive further assess-ment and management. This might be consideredfor implementation as part of a multidisciplinaryclinic service. Further study and clinical audit isrequired of those with ADPKD complicated by neph-rolithiasis, specifically with regards to interventionsutilized, complications and adverse events, and clin-ical outcomes.
BACKGROUND
Nephrolithiasis does commonly complicate ADPKD.When it occurs in ADPKD it poses additional clinicalchallenges that are not present in the non-ADPKDpopulation. These include the superimposition ofcomplicated urinary tract infection, difficulties withthe diagnosis (eg, differentiating acute flank pain dueto stone formation from acute cyst infection or hem-orrhage), and choice of the surgical intervention.1
Accordingly, heightened awareness and potential mod-ification of the standard clinical approach is requiredcompared to patients presenting with nephrolithiasiswho do not have ADPKD.2,3
The prevalence of nephrolithiasis in ADPKD maybe 5 to 10 times higher compared to the generalpopulation.4 This increased risk is probably due toreduced urinary flow (and stasis) in renal tubules andcalyces due to compression from expanding renal cystsas well as underlying urinary metabolic abnormalities.5
In a large cohort of 751 patients with ADPKD, renalstone disease occurred in 20.1% of subjects over a 10-year period.6 However, only a minority of patients withADPKD with nephrolithiasis report clinical symptoms(ie, either recall having passed a renal stone or requiredsurgical intervention) and the vast majority are asymp-tomatic with abnormalities (renal stones or calcifica-tions) noted on imaging.7 Patients with ADPKD withnephrolithiasis have greater morbidity burden includ-ing flank pain and urinary tract infections compared tothose that have not developed stones.7 There may alsobe a relationship between nephrolithiasis and anincreased number and size of renal cysts in ADPKDpatients.8 Further, such patients have been observed tohave lower levels of renal function, suggesting thatprogression of ADPKD with resultant intrarenal ana-tomic obstruction is associated with a predisposition tonephrolithiasis.8
In contrast to the general population (wherecalcium-containing stones are most prevalent), renalstones in ADPKD are most commonly composed ofurate (56%-47%), and to a lesser degree, calciumoxalate.6,9 The most common urine metabolic abnor-malities predisposing to stone formation in ADPKD
are hypocitraturia, aciduria and hypomagesuria, as wellas low urine volume.6,8 In the ADPKD subgroup withpreserved renal function, other risk factors predispos-ing to nephrolithiasis include hyperuricosuria, hyper-oxaluria, and hypercalcuria.6 Given the latter, emphasisshould be placed not just on treating nephrolithiasis,but also its predisposing metabolic and structuralfactors.10 This presents challenges and opportunitiesamong those affected by both ADPKD and nephroli-thiasis, with heightened emphasis on metabolic evalu-ation and resultant correction.11 The surgicalmanagement of nephrolithiasis in ADPKD is notthought to differ from that utilized in those withoutADPKD,2 apart from additional considerationsrequired due to the presence of multiple renal cysts,such as extracorporeal shockwave therapy (ESWL)beam targeting (or avoidance of this technique) tominimize the risk of cyst hemorrhage.
SEARCH STRATEGY
Databases Searched
Medical subject headings and text words forADPKD were combined with medical subject head-ings terms and text words relating to the assessmentand management of nephrolithiasis and renal stonedisease. The search was carried out in Ovid MED-LINE (1946 to June 2014), Embase (1974 to May 23,2014), PsycINFO (1806 to June 2014), and theCochrane Database of Systematic Reviews and theCochrane Registry of Clinical Trials (inception toJune 2014).Date of search: June 2014.
WHAT IS THE EVIDENCE?
Supplementary evidence Tables are available online.
Imaging
There are few studies specifically examining theoptimal imaging modality for renal stone diseaseamong those with ADPKD.
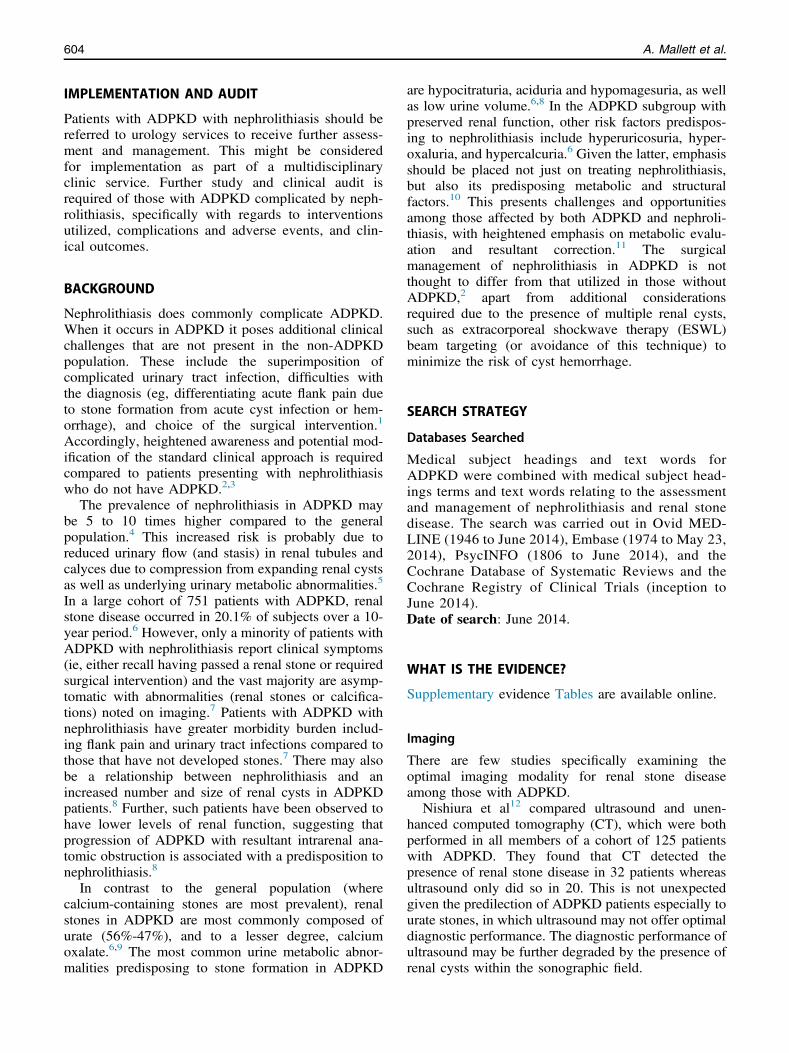
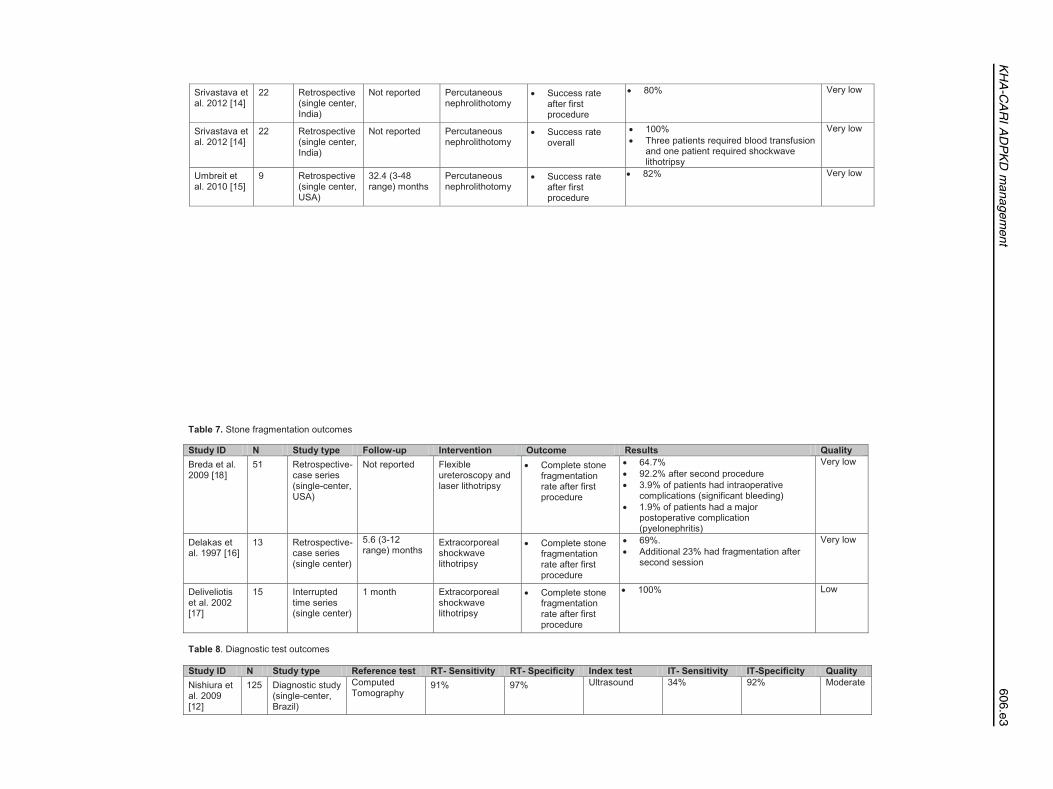
Nishiura et al12 compared ultrasound and unen-hanced computed tomography (CT), which were bothperformed in all members of a cohort of 125 patientswith ADPKD. They found that CT detected thepresence of renal stone disease in 32 patients whereasultrasound only did so in 20. This is not unexpectedgiven the predilection of ADPKD patients especially tourate stones, in which ultrasound may not offer optimaldiagnostic performance. The diagnostic performance ofultrasound may be further degraded by the presence ofrenal cysts within the sonographic field.

KHA-CARI ADPKD management 605
Urinary Metabolic Therapy
While evaluation and treatment for predisposing uri-nary metabolic circumstances is frequently recom-mended given their increased prevalence in patientswith ADPKD complicated by nephrolithiasis,1,6,8 thereis no clearly reported evidence of the clinical outcomeswhen such urinary metabolic predisposition iscorrected.
Percutaneous Nephrolithotomy
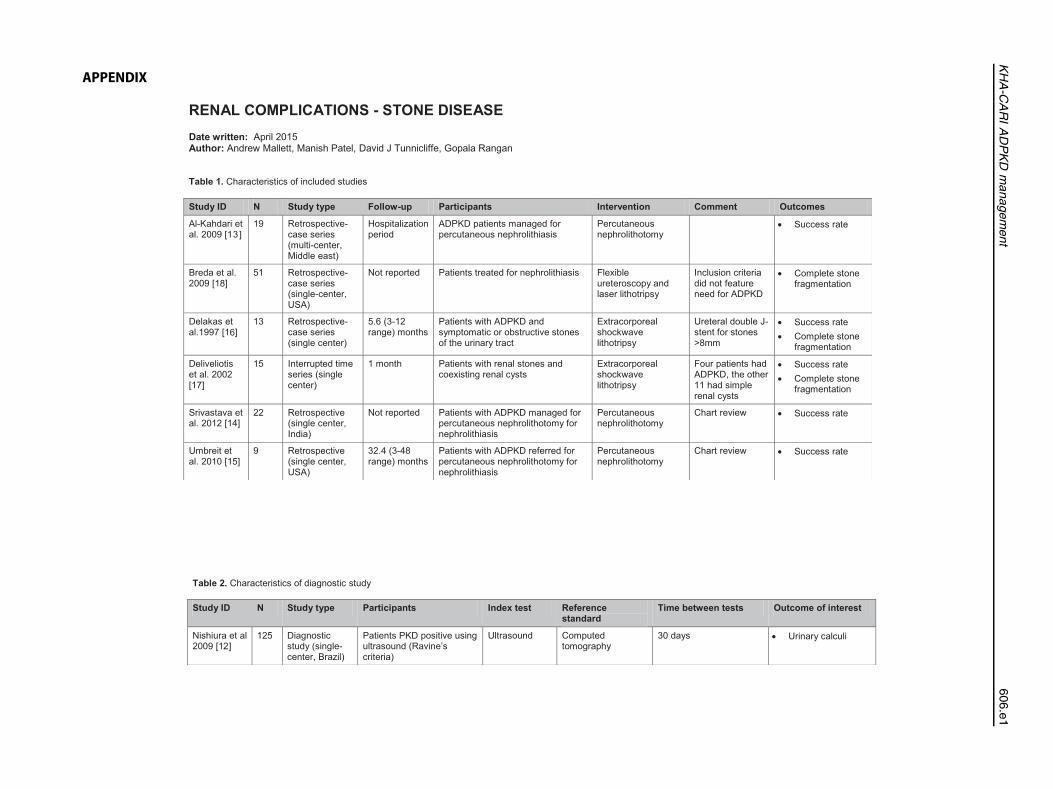
In a case series of 19 patients with ADPKD and upper-tract nephrolithiasis greater than 2 cm in largestdiameter, including one with bilateral renal stonedisease, percutaneous nephrolithotomy (PCNL)achieved stone clearance in 89.4%, with a meanhospital stay of 3 days, no patient deaths, improvementin renal function in all who had acute kidney injury,and three complications.13 Another case series of 25such patients achieved stone clearance in 88%,improvement in renal function, and seven complica-tions, although the mean hospital stay was not knownand two and one patient, respectively, required arepeat PCNL and ESWL.14 A third case series of nineADPKD patients with upper-tract nephrolithiasisgreater than 2 cm in largest diameter achieved 82%stone clearance without any postoperative complica-tions and no recurrence at 2.7 years of follow-up.15
Extracorporeal Shockwave Lithotripsy
There is only one case series exclusively reportingon the use of ESWL for nephrolithiasis in patientswith ADPKD. In 13 patients a stone-free rate of85% was achieved at 3 months, with two patientsrequiring repeated treatments in this time.16 Themean stone size was 15.2 mm (range, 7-35 mm).Complete stone fragmentation was achieved for69% of patients with one session. No complicationswere reported.
Another case series of 15 patients with nephroli-thiasis in the setting of renal cysts demonstrated a 60%stone-free rate at 1 month.17 One of four patients withADPKD in the cohort was stone-free at 1 month;however, complete stone fragmentation was achievedin all patients in the cohort.
Ureteroscopy With Laser Lithotripsy
There was one case series that reported on the use ofureteroscopy with laser lithotripsy (ULL) amongpatients with ADPKD complicated by nephrolithiasis.18
Among 51 such patients with a mean stone size of 6.6� 3 mm per patient, stone-free rates of 64.7% and92.2% were achieved with one and two procedures,respectively. Complications occurred in 13.6% of
patients (intraoperative bleeding, ureteral perforation,pyelonephritis), the majority of which (7.8%) wereuncomplicated urinary tract infections.
SUMMARY OF THE EVIDENCE
Nephrolithiasis is more common among those withADPKD, and commonly has an underlying urinarymetabolic predisposition. Given a predilection to form-ing urate stones, unenhanced CT has a better diagnosticperformance in comparison to ultrasound.
There is no specific evidence that the standardmedical management to prevent recurrent stone for-mation should differ from the general population.19
In the setting that urological intervention is required,PCNL for upper renal tract stones greater than 2 cm inmaximal diameter among those with ADPKD is effec-tive and safe in limited published case series. Similarly,ESWL is effective in the same circumstances for stonesthat generally are smaller, although up to a 3.5-cmmaximal diameter. The choice of intervention (and itsurgency) depends on the location of the renal stonewithin the urinary tract, the clinical presentation, othercomplicating co-existing or intercurrent factors, therenal stone composition, the degree of renal cystburden, and the clinical opinion of the treating urolo-gist. However, current urological practice is evolvingand ULL is being increasingly utilized and favored.
WHAT DO THE OTHER GUIDELINES SAY?
Kidney Disease Outcomes Quality Initiative: Norecommendation.UK Renal Association: No recommendation.Canadian Society of Nephrology: No recommen-dation.European Best Practice Guidelines: No recom-mendation.International Guidelines: No recommendation.
Spanish Guidelines20:
Diagnosis
i)
CT scanning should be used in uncertain cases orin those with suspicion of associated renal diseasesuch as stones or tumor (D).Lithiasis
i)
Renal lithiasis may benefit from potassium citratewhen hypocitraturia is present, as well as fromurine alkalinization (D).ii)
Percutaneous nephrolithotomy and extracorpor-eal shock wave lithotripsy can be used in anindividualized setting (D).
A. Mallett et al.606
SUGGESTIONS FOR FUTURE RESEARCH
Further research is required into the outcomes ofcorrecting predisposing urinary metabolic circumstancesfor nephrolithiasis in those with ADPKD. Audit, com-parison, and description of the treatment (PCNL, ESWL,ULL) and clinical outcomes in cohorts with ADPKDcomplicated by nephrolithiasis is required to furtherdelineate and inform future clinical decision making.
APPENDIX A. SUPPLEMENTARY INFORMATION
Supplementary data associated with this article can befound in the online version at http://dx.doi.org/10.1016/j.semnephrol.2015.10.012.
REFERENCES1. Amar AD, Das S, Egan RM. Management of urinary calculous
disease in patients with renal cysts: review of 12 years ofexperience in 18 patients. J Urol. 1981;125:153-6.
2. Torres VE, Wilson DM, Hattery RR, Segura JW. Renal stonedisease in autosomal dominant polycystic kidney disease. Am JKidney Dis. 1993;22:513-9.
3. Tan YK, Cha DY, Gupta M. Management of stones inabnormal situations. Urol Clin North Am. 2013;40:79-97.
4. Delaney VB, Adler S, Bruns FJ, Licinia M, Segel DP, FraleyDS. Autosomal dominant polycystic kidney disease: presenta-tion, complications, and prognosis. Am J Kidney Dis.1985;5:104-11.
5. Mufti UB, Nalagatla SK. Nephrolithiasis in autosomal domi-nant polycystic kidney disease. J Endourol. 2010;24:1557-61.
6. Torres VE, Erickson SB, Smith LH, Wilson DM, Hattery RR,Segura JW. The association of nephrolithiasis and autosomaldominant polycystic kidney disease. Am J Kidney Dis.1988;11:318-25.
7. Levine E, Grantham JJ. Calcified renal stones and cystcalcifications in autosomal dominant polycystic kidney disease:clinical and CT study in 84 patients. AJR Am J Roentgenol.1992;159:77-81.
8. Grampsas SA, Chandhoke PS, Fan J, Glass MA, Townsend R,Johnson AM, et al. Anatomic and metabolic risk factors for
nephrolithiasis in patients with autosomal dominant polycystickidney disease. Am J Kidney Dis. 2000;36:53-7.
9. Idrizi A, Barbullushi M, Petrela E, Kodra S, Koroshi A,Thereska N. The influence of renal manifestations to theprogression of autosomal dominant polycystic kidney disease.Hippokratia. 2009;13:161-4.
10. Muldoon LD, Resnick MI. Secondary urolithiasis. EndocrinolMetab Clin North Am. 1990;19:909-18.
11. Gambaro G, Fabris A, Puliatta D, Lupo A. Lithiasis in cystickidney disease and malformations of the urinary tract. Urol Res.2006;34:102-7.
12. Nishiura JL, Neves RFCA, Eloi SRM, Cintra SMLF, Ajzen SA,Heilberg IP. Evaluation of nephrolithiasis in autosomal domi-nant polycystic kidney disease patients. Clin J Am SocNephrol. 2009;4:838-44.
13. Al-Kandari AM, Shoma AM, Eraky I, El-Kenawy MR, Al-EeziH, El-Kappany HA. Percutaneous nephrolithotomy for manage-ment of upper urinary tract calculi in patients with auto-somal dominant polycystic kidney disease. Urology. 2009;74:273-7.
14. Srivastava A, Bansal R, Srivastava A, Chaturvedi S, Ranjan P,Ansari MS, et al. Percutaneous nephrolithotomy in polycystickidney disease: is it safe and effective? Int Urol Nephrol.2012;44:725-30.
15. Umbreit EC, Childs MA, Patterson DE, Torres VE, LeRoy AJ,Gettman MT. Percutaneous nephrolithotomy for large or multi-ple upper tract calculi and autosomal dominant polycystickidney disease. J Urol. 2010;183:183-7.
16. Delakas D, Daskalopoulos G, Cranidis A. Extracorporealshockwave lithotripsy for urinary calculi in autosomal domi-nant polycystic kidney disease. J Endourol. 1997;11:167-70.
17. Deliveliotis C, Argiropoulos V, Varkarakis J, Albanis S,Skolarikos A. Extracorporeal shock wave lithotripsy producesa lower stone-free rate in patients with stones and renal cysts.Int J Urol. 2002;9:11-4.
18. Breda A, Ogunyemi O, Leppert JT, Schulam PG. Flexibleureteroscopy and laser lithotripsy for multiple unilateral intra-renal stones. Eur Urol. 2009;55:1190-6.
19. Thomas M, Becker G, Kairaitis L, Hughes P, Richmond J.KHA-CARI guidelines kidney stones. Nephrology. 2007;12:S1-36.
20. Ars E, Bernis C, Fraga G, Martínez V, Martins J, Ortiz A, et al.Spanish guidelines for the management of autosomal dominantpolycystic kidney disease. Nephrol Dial Transplant. 2014;29(iv):95-105.
APPENDIX
RENAL COMPLICATIONS - STONE DISEASE Date written: Author:
Table 1.
Study ID N Study type Follow-up Participants Intervention Comment Outcomes
8
6
7
4
5
Table 2.
Study ID N Study type Participants Index test Reference standard
Time between tests Outcome of interest
KHA-C
ARIADPKD
management
606.e1
Table 3. Study ID Independent
Intervention Shape of intervention pre-specified
Intervention unlikely to affect data collection
Blind outcome assessment
Incomplete data
Selective reporting
Other risks of bias
Quality
Table 4.
Study ID Patient selection Index test Reference standard Flow and timing Quality
Table 5.
Study ID Comments Quality
Table 6.
Study ID N Study type Follow-up Intervention Outcome Results Quality
8
5
7
A.Mallettetal.
606.e2
4
4
5
Table 7. Study ID N Study type Follow-up Intervention Outcome Results Quality
Table 8 Study ID N Study type Reference test RT- Sensitivity RT- Specificity Index test IT- Sensitivity IT-Specificity Quality
6
7
KHA-C
ARIADPKD
management
606.e3






















![Clinical manifestations of autosomal recessive polycystic kidney ... · viduals to survive the perinatal period [ 8, 10]. Pulmonaryhypoplasia,aserio uscomplicationthatgenerally occurs](https://img.pdfslide.net/doc/110x75/5f09f6827e708231d4295907/clinical-manifestations-of-autosomal-recessive-polycystic-kidney-viduals-to.jpg)