Embed Size (px)
Citation preview
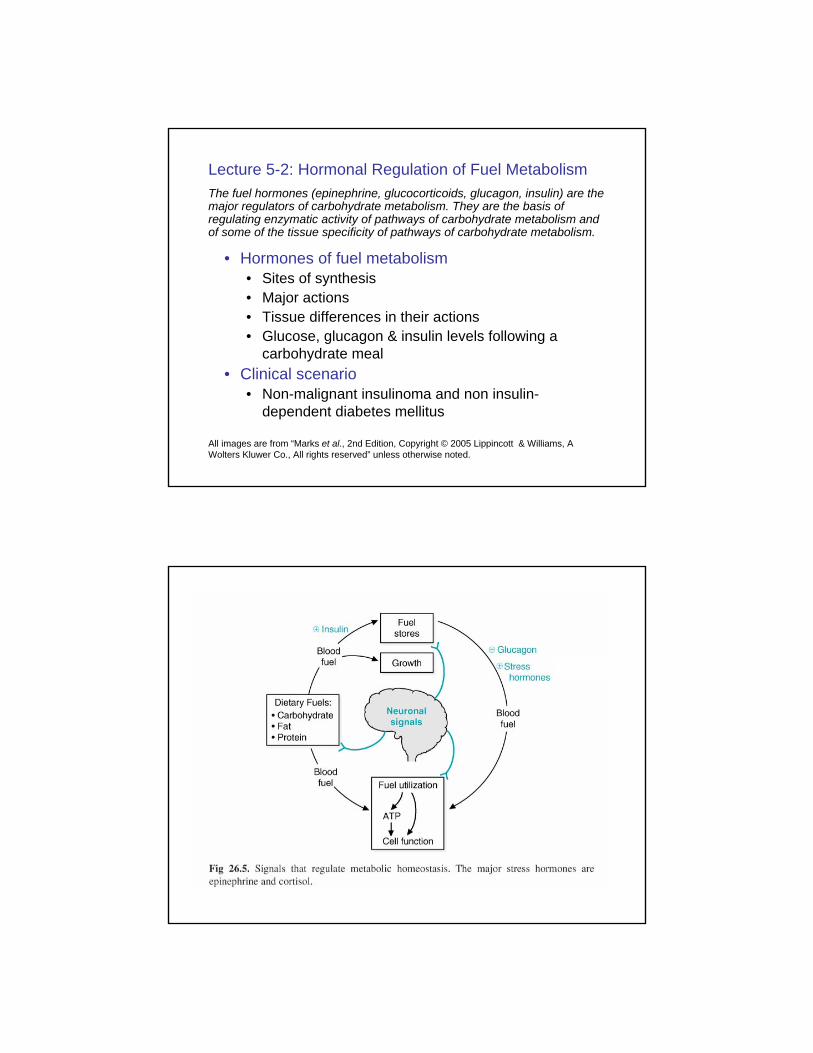
Lecture 5-2: Hormonal Regulation of Fuel MetabolismThe fuel hormones (epinephrine, glucocorticoids, glucagon, insulin) are the major regulators of carbohydrate metabolism. They are the basis of regulating enzymatic activity of pathways of carbohydrate metabolism and of some of the tissue specificity of pathways of carbohydrate metabolism.
• Hormones of fuel metabolism• Sites of synthesis• Major actions• Tissue differences in their actions• Glucose, glucagon & insulin levels following a
carbohydrate meal• Clinical scenario
• Non-malignant insulinoma and non insulin-dependent diabetes mellitus
All images are from “Marks et al., 2nd Edition, Copyright © 2005 Lippincott & Williams, A Wolters Kluwer Co., All rights reserved” unless otherwise noted.
Fuel Homeostasis
• Fuel availability and tissue needs must be balanced
• This balance is achieved by three types of messages
Blood level of nutrientsHormone levelsNerve impulse
Glucose is a special fuel
• Tissues that depend upon glycolysis for energy include red blood cells, the lens of the eye and the kidney medulla• Uninterrupted access to glucose is required
to sustain high level of ATP utilization• Normal homeostatic concentration of
glucose in the blood is 80 – 100 mg/dL (~ 5 mM)
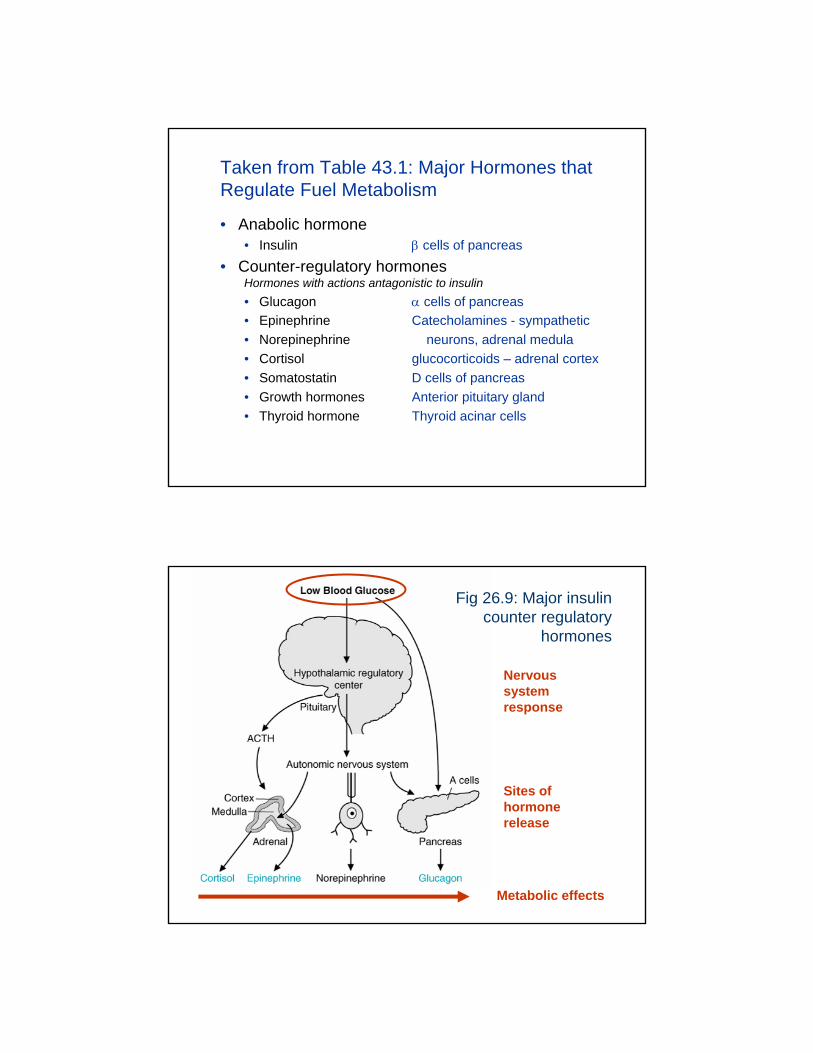
Taken from Table 43.1: Major Hormones that Regulate Fuel Metabolism
• Anabolic hormone• Insulin β cells of pancreas
• Counter-regulatory hormonesHormones with actions antagonistic to insulin• Glucagon α cells of pancreas• Epinephrine Catecholamines - sympathetic• Norepinephrine neurons, adrenal medula• Cortisol glucocorticoids – adrenal cortex• Somatostatin D cells of pancreas• Growth hormones Anterior pituitary gland• Thyroid hormone Thyroid acinar cells
Nervous system response
Sites of hormone release
Metabolic effects
Fig 26.9: Major insulin counter regulatory
hormones
Hormones of fuel metabolism
• What are the… • …major roles of the hormones?• …tissue differences in their effects?
• Insulin versus glucagon• These hormones have opposite effects on
metabolism.• What are the fasting levels of these hormones?• What are the post absorptive levels of these
hormones?
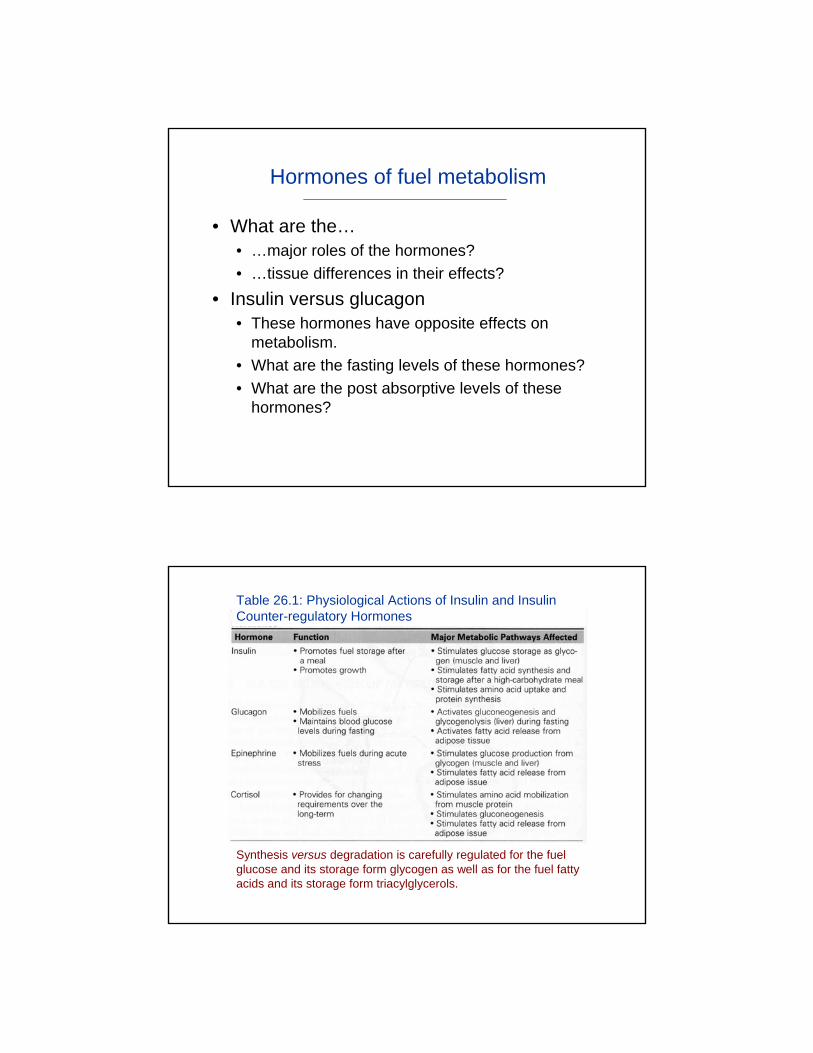
Synthesis versus degradation is carefully regulated for the fuel glucose and its storage form glycogen as well as for the fuel fatty acids and its storage form triacylglycerols.
Table 26.1: Physiological Actions of Insulin and Insulin Counter-regulatory Hormones
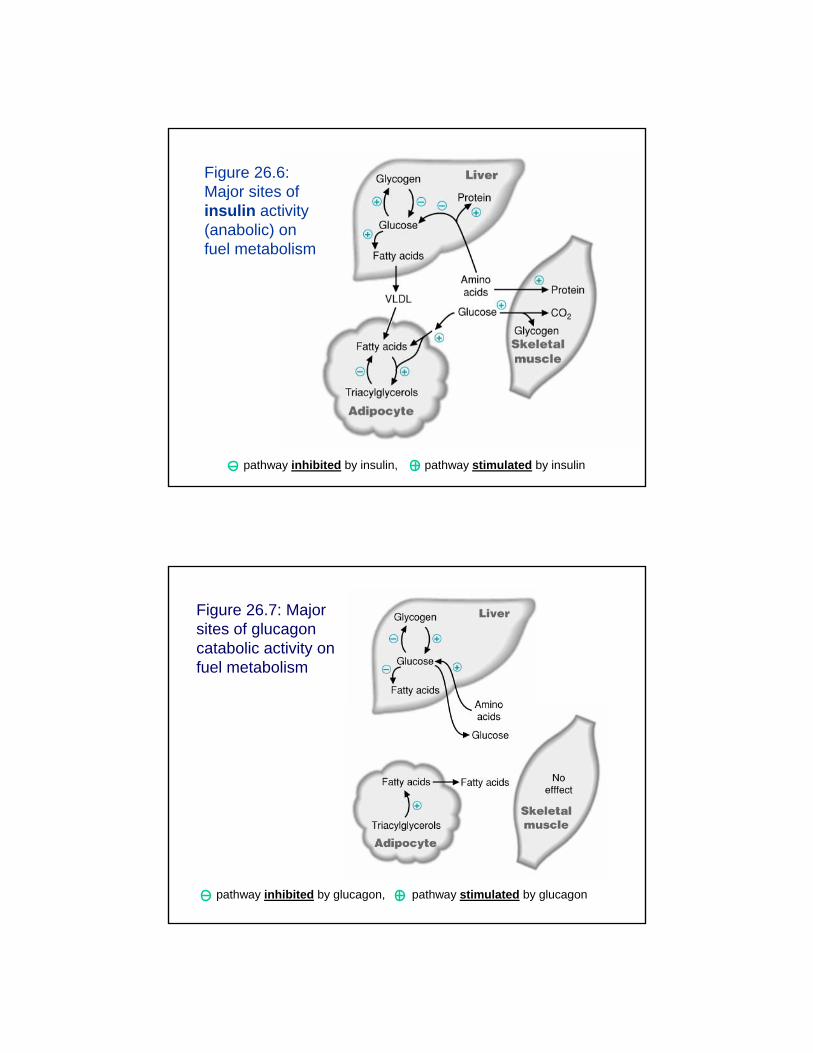
Figure 26.6: Major sites of insulin activity (anabolic) on fuel metabolism
pathway inhibited by insulin, pathway stimulated by insulin
Figure 26.7: Major sites of glucagon catabolic activity on fuel metabolism
pathway inhibited by glucagon, pathway stimulated by glucagon
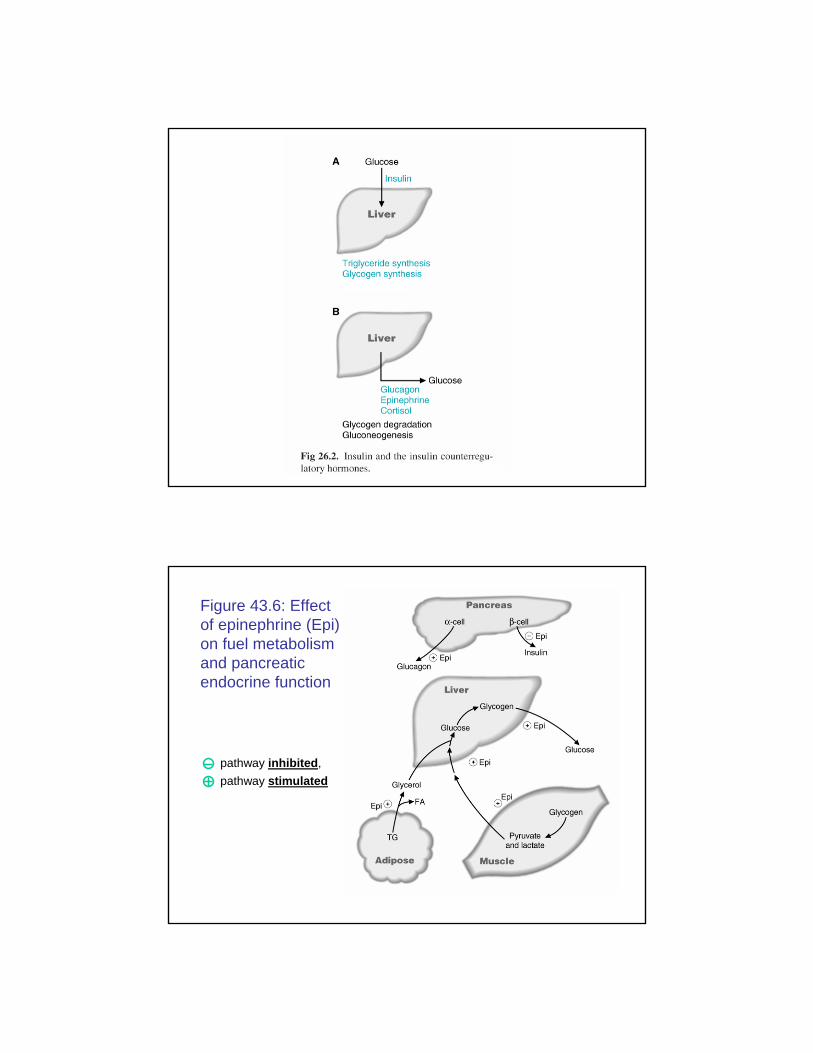
pathway inhibited, pathway stimulated
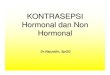
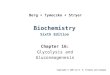
Figure 43.6: Effect of epinephrine (Epi) on fuel metabolism and pancreatic endocrine function
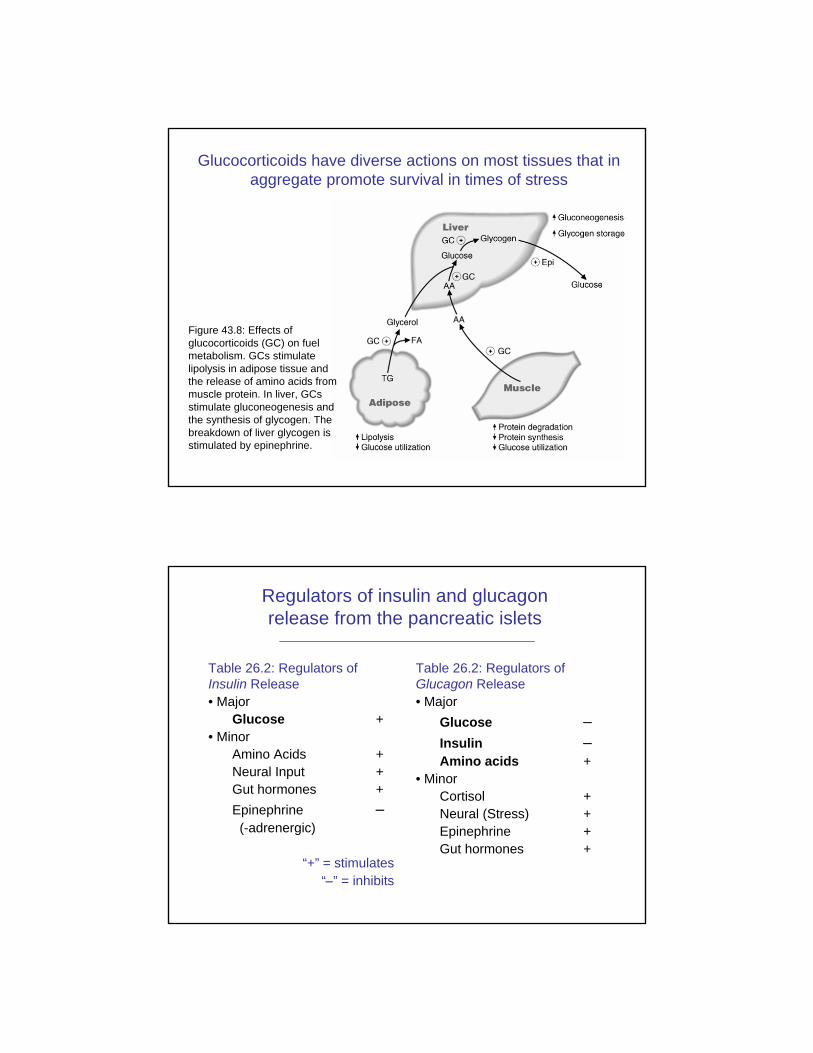
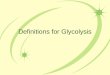
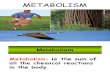
Figure 43.8: Effects of glucocorticoids (GC) on fuel metabolism. GCs stimulate lipolysis in adipose tissue and the release of amino acids from muscle protein. In liver, GCs stimulate gluconeogenesis and the synthesis of glycogen. The breakdown of liver glycogen is stimulated by epinephrine.
Glucocorticoids have diverse actions on most tissues that in aggregate promote survival in times of stress
Table 26.2: Regulators of Glucagon Release• Major
Glucose −Insulin −Amino acids +
• MinorCortisol +Neural (Stress) +Epinephrine +Gut hormones +
Table 26.2: Regulators of Insulin Release• Major
Glucose +• Minor
Amino Acids +Neural Input +Gut hormones +Epinephrine −(-adrenergic)
“+” = stimulates“−” = inhibits
Regulators of insulin and glucagon release from the pancreatic islets
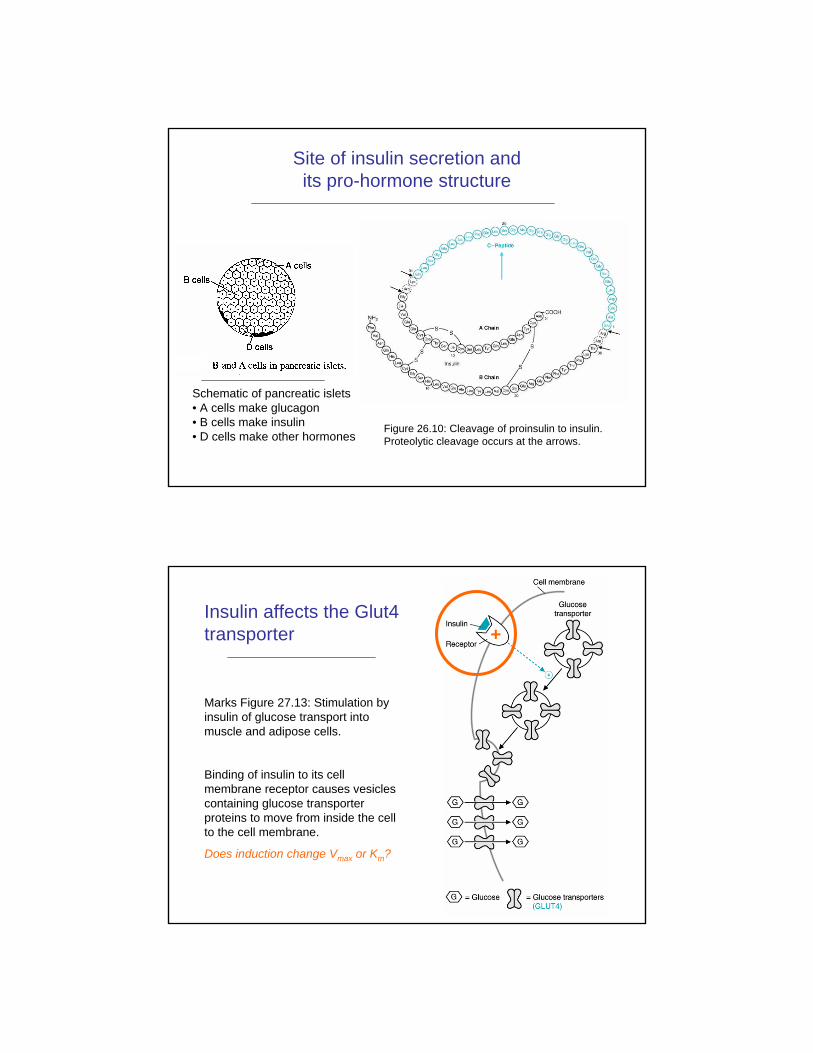
Figure 26.10: Cleavage of proinsulin to insulin. Proteolytic cleavage occurs at the arrows.
Schematic of pancreatic islets• A cells make glucagon• B cells make insulin• D cells make other hormones
Site of insulin secretion and its pro-hormone structure
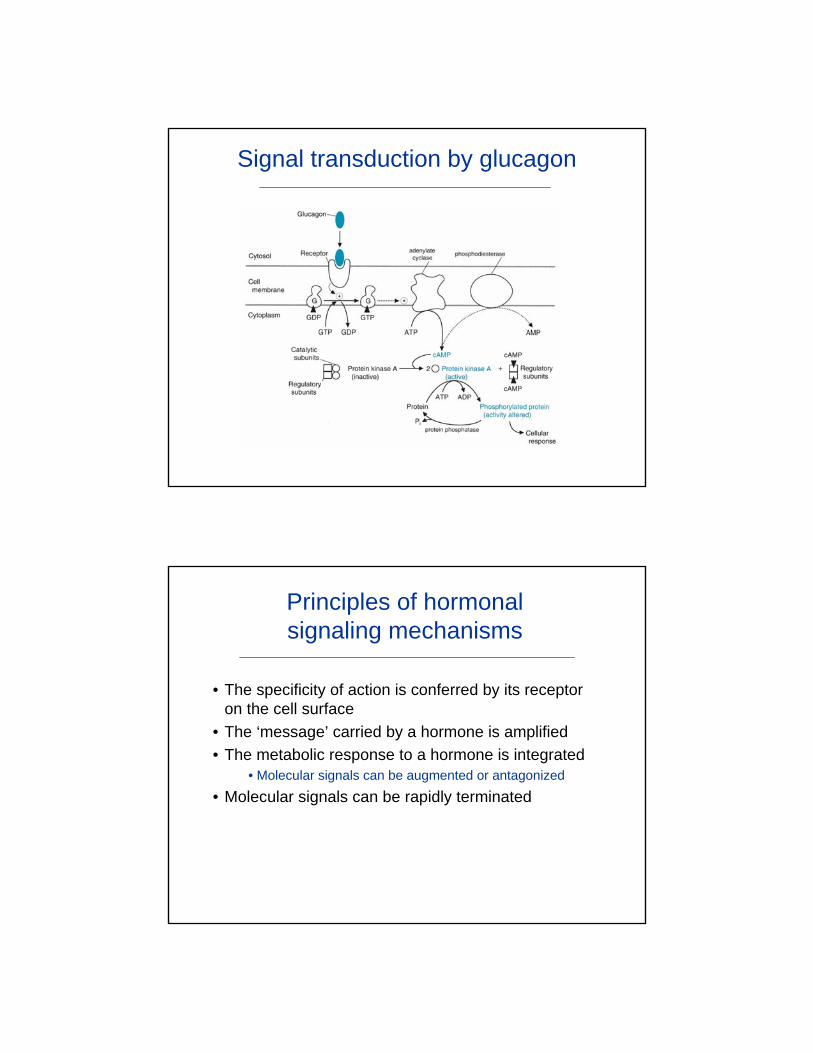
+Insulin affects the Glut4 transporter
Marks Figure 27.13: Stimulation by insulin of glucose transport into muscle and adipose cells.
Binding of insulin to its cell membrane receptor causes vesicles containing glucose transporter proteins to move from inside the cell to the cell membrane.
Does induction change Vmax or Km?
Signal transduction by glucagon
Principles of hormonal signaling mechanisms
• The specificity of action is conferred by its receptor on the cell surface
• The ‘message’ carried by a hormone is amplified• The metabolic response to a hormone is integrated
• Molecular signals can be augmented or antagonized
• Molecular signals can be rapidly terminated
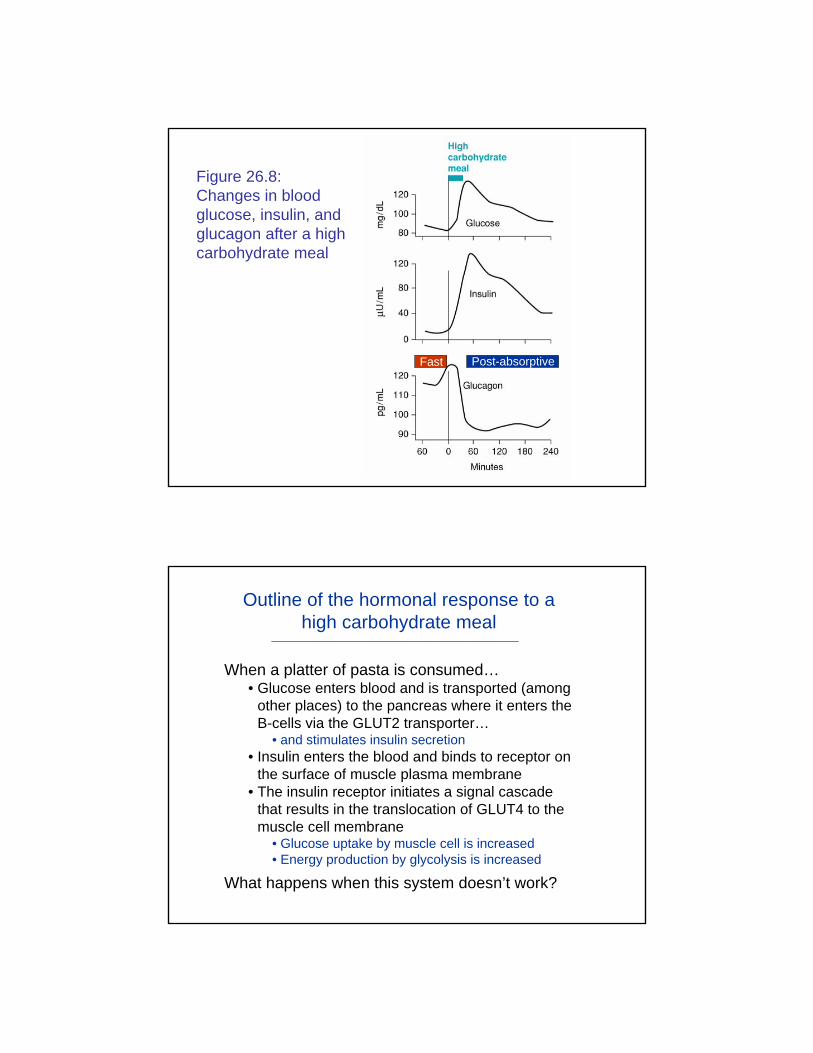
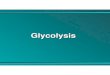
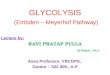
Figure 26.8: Changes in blood glucose, insulin, and glucagon after a high carbohydrate meal
Post-absorptiveFast
Outline of the hormonal response to a high carbohydrate meal
When a platter of pasta is consumed…• Glucose enters blood and is transported (among
other places) to the pancreas where it enters the B-cells via the GLUT2 transporter…
• and stimulates insulin secretion• Insulin enters the blood and binds to receptor on
the surface of muscle plasma membrane• The insulin receptor initiates a signal cascade
that results in the translocation of GLUT4 to the muscle cell membrane
• Glucose uptake by muscle cell is increased• Energy production by glycolysis is increased
What happens when this system doesn’t work?
Clinical scenario: Insulinoma induced hypoglycemia
• The patient is a 46-year old woman who reports the following symptoms• Six months ago, fatigue and
confusion sometimes followed pre-breakfast jogs - anxiety, pallor and sweating also reported
• Blurred vision and an ‘unusually urgent’ hunger sometimes experienced
• Eating relieved all of the symptoms within 25 – 30 min
• The patient exercises before breakfast when glucose and insulin levels are low and glucagon is high• Fatigue suggests a lack of fuel• Confusion, blurred vision and
‘urgent’ hunger suggest lack of glucose
• The fact that eating relieves the symptoms suggests that the enzymology necessary to metabolize food is functional and points to a regulatory deficiency…
Clinical scenario: Insulinoma induced hypoglycemia
• The episodes now recur more frequently during the day with increasing daily frequency• The frequency of the episodes
is diminished by snacking between meals
• The extra calories ingested by snacking have resulted in a weight gain of 8 pounds
• The patient’s serum glucose is 46 mg/dL (80 –100 is normal) during the initial late afternoon consultation
• The problem is progressive• Again, the relief gained by
eating suggests that the metabolic pathways are functional and that the problem is one of regulation
• The conversion of calories to weight gain indicates suggests stimulation of the anabolicpathways
• The patient is hypoglycemic (low blood sugar) even though she has been eating (presumably) during the day
Clinical scenario: Insulinoma induced hypoglycemia
• The physician ordered • a test of fasting serum
glucose levels and• requested that the
patient keep a daily symptoms diary
• The diagnosis is ‘fasting’ hypoglycemia where glucose stores are not mobilized in the absence of available fuel
• What is the source of this disorder?
• The patient’s fasting serum glucose level is below normal
• The symptoms track with fasting
• The fatigue, confusion and blurred vision (neuroglycopeicsymptoms) result from the brain’s lack of glucose
• The anxiety, pallor and sweating are due to release of epinephrine in response to the stress of hypoglycemia
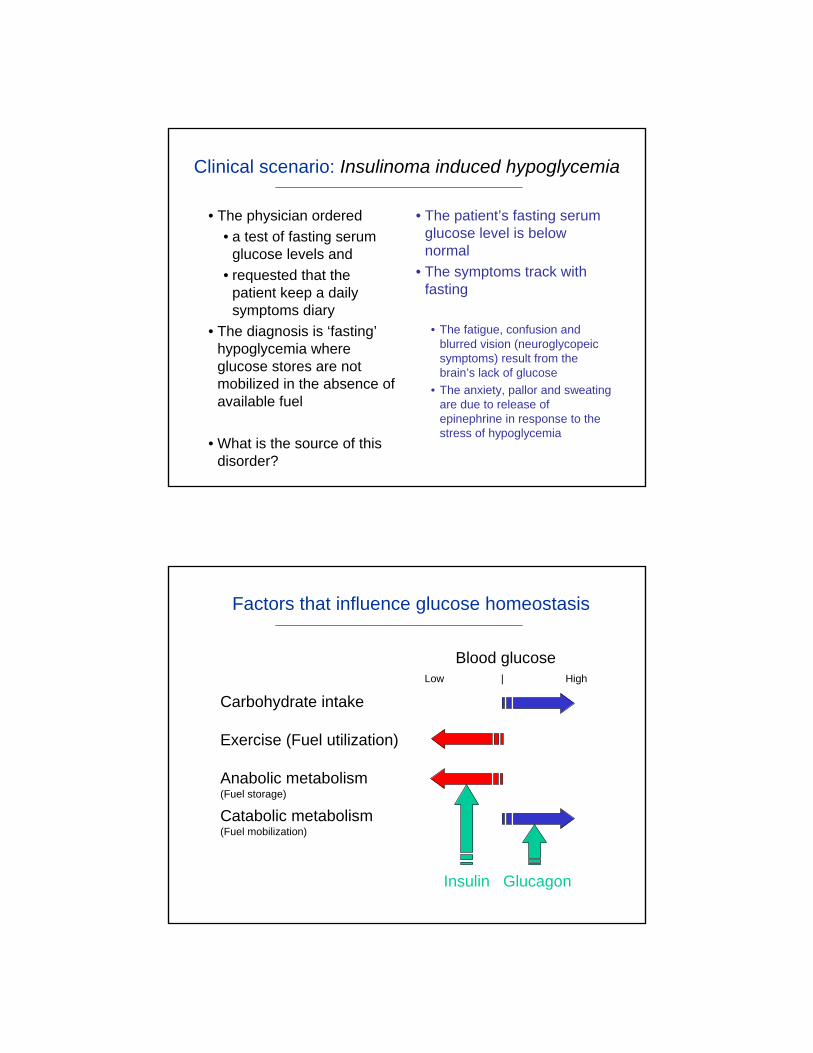
Factors that influence glucose homeostasis
Carbohydrate intake
Exercise (Fuel utilization)
Anabolic metabolism(Fuel storage)
Catabolic metabolism(Fuel mobilization)
Blood glucoseLow | High
Insulin Glucagon
Clinical scenario: Insulinoma induced hypoglycemia
• Is the disorder the result of autonomous (unregulated) hormone secretion?
• Unregulated hormone secretion disrupts the homeostatic balance of anabolic and catabolic reactions.
• Why is autonomous hypersecretion of insulin suspected?• Insulin stimulates anabolic
reactions• Constitutive insulin release will
stimulate glucose uptake from the blood even when glucose concentrations are low…
Clinical scenario: Insulinoma induced hypoglycemia
• The test of the proposed diagnosis is to simultaneously measure blood glucose and insulin when the patient is symptomatic
• The low blood glucose (45 mg/dL) measured earlier is confirmed
• A high insulin to glucagon ratio was measured• Quantification of the insulin
concentration is accomplished my measurement of the concentration of the C-peptide present in the blood produced by the conversion of proinsulinto insulin.
• Note: Epinephrine secretion is unaffected by insulin hyper-secretion resulting the patient’s ‘stress response’.
Clinical scenario: Resolution of the problem
• An ultrasound of the patient’s abdomen revealed a mass within the pancreas• Insulin is secreted by the
pancreas
• A nonmalignant mass consisting of insulin rich B cells (an ‘insulinoma’) was surgically removed
• After recovering from the surgery, the patient• no longer experienced the
symptoms of hypoglycemia• had normal levels of blood
glucose• lost the weight gained prior
to surgery• Homeostasis is restored…
• New York Times articles - 2006
Lecture Summary
• The regulation of glucose metabolism is dominated by the insulin : glucagon ratio. • High values of this ratio stimulates glucose uptake and storage
as glycogen and fatty acids and amino acid uptake and protein synthesis (anabolic reactions)
• Low levels of this ratio stimulate gluconeogenesis and glycogenolysis to release glucose into the blood (catabolic reactions)
• Hormones modulate fuel metabolism through multi-step branching signal transduction pathways. Modulations include• Allosteric regulation• Post-translational modification• Regulation of gene transcription
• Hypoglycemia and hyperglycemia have serious clinical consequences. Homeostasis is to be maintained…