Embed Size (px)
Citation preview

La Farmacogenetica in
oncologia
Dott.ssa Marzia Del Re
Prof. Romano Danesi
Dipartimento di Medicina Clinica e Sperimentale
Università di Pisa UOC Farmacologia clinica
Azienda Ospedaliero-Universitaria Pisana

SNPs may occur at any position in the gene
2

Introduction
Circula(ng Tumor Cells (CTCs)
• CTCs play a cri,cal role in the metasta,c spread of carcinomas and their detec,on is associated with prognosis in many human cancers, while their enumera,on has been cleared by the FDA for follow up of breast, colon, and prostate cancer pa,ents with verified metastasis. • CTCs represent a promising new diagnos,c tool, especially for advanced-‐stage cancer pa,ents where they can be used as a “liquid biopsy,” allowing physicians to follow cancer changes over ,me and tailor treatment accordingly. • However, it is quite clear now that simple enumera,on of CTCs is not enough.
• CTC molecular characteriza,on is very important since it can play a crucial role in understanding the biology of metastasis and in selec,ng pa,ents for targeted therapy.
3

Cell free DNA (cfDNA)
• cfDNA circulates in plasma of pa,ents with cancer at increased concentra,ons.
• Many teams have focused on the development of assays that allow the specific detec,on of small amounts of tumor specific cfDNA in the peripheral blood of pa,ents with cancer.
• The detec,on of tumor specific DNA altera,ons such as muta,ons and methyla,on in cfDNA provides a less invasive, more easily accessible source of DNA for gene,c analysis than tumor biopsies.
Introduction
4

DNARNA
IntracellularProtein
Membraneprotein
ApoptosisProliferation
Apoptotic Bodies/Debris &Protein/DNA/RNA Complexes
Plasma
Circula(ng Cellular Debris Contains Fingerprints of Tumor Cells
5

20 mL Peripheral blood
Ficoll gradient
PBMCs
Cell count
Positive selection (EpCAM)
Apply magnet
DNA extraction From CTCs
CTCs isolation
CellFreeDNA isolation
Plasma
Methodology
Outline of the extraction of cell free DNA and CTCs. 6

Concordance in detected mutations between paired FFPE tumors and cpDNA.
Perkins G, Yap TA, Pope L, Cassidy AM, et al. (2012) Mul,-‐Purpose U,lity of Circula,ng Plasma DNA Tes,ng in Pa,ents with Advanced Cancers. PLoS ONE 7(11): e47020. doi:10.1371/journal.pone.0047020 hZp://www.plosone.org/ar,cle/info:doi/10.1371/journal.pone.0047020
7

DNA concentrations classified by tumor types
Perkins G, Yap TA, Pope L, Cassidy AM, et al. (2012) Mul,-‐Purpose U,lity of Circula,ng Plasma DNA Tes,ng in Pa,ents with Advanced Cancers. PLoS ONE 7(11): e47020. doi:10.1371/journal.pone.0047020 hZp://www.plosone.org/ar,cle/info:doi/10.1371/journal.pone.0047020 8

Relationship between cpDNA concentration and survival
Perkins G, Yap TA, Pope L, Cassidy AM, et al. (2012) Mul,-‐Purpose U,lity of Circula,ng Plasma DNA Tes,ng in Pa,ents with Advanced Cancers. PLoS ONE 7(11): e47020. doi:10.1371/journal.pone.0047020 hZp://www.plosone.org/ar,cle/info:doi/10.1371/journal.pone.0047020
9

Relationship between cpDNA concentration and RMH prognostic score.
Perkins G, Yap TA, Pope L, Cassidy AM, et al. (2012) Mul,-‐Purpose U,lity of Circula,ng Plasma DNA Tes,ng in Pa,ents with Advanced Cancers. PLoS ONE 7(11): e47020. doi:10.1371/journal.pone.0047020 hZp://www.plosone.org/ar,cle/info:doi/10.1371/journal.pone.0047020
10

!
!!
G12A
Control
Control
Emergence of a KRAS muta,on in a pa,ent resistant to EGFR/TKI
11

Le fluoropirimidine sono i farmaci antitumorali maggiormente utilizzati in
clinica
1ChemSpider 2D Image | 5-fluoro-1-(tetrahydrofuran-2-yl)pyrimidine-2,4(1H,3H)-dione - pyrimidine-2...
September 22, 2012 1:08:14 PMhttp://www.chemspider.com/ImageView.aspx?id=94558
Show 2D Show 3D
1ChemSpider 2D Image | Capecitabine | C15H22FN3O6
September 22, 2012 1:07:39 PMhttp://www.chemspider.com/ImageView.aspx?id=54916
Show 2D Show 3D 3
1ChemSpider 2D Image | Fluorouracil | C4H3FN2O2
September 22, 2012 1:00:12 PMhttp://www.chemspider.com/ImageView.aspx?id=3268&mode=2d
Show 2D Show 3D
5-Fluorouracile
Capecitabina
Tegafur/uracile (UFT)
12

Meccanismo di azione delle fluoropirimidine: metabolismo attivante
13

Metabolismo inattivante del 5-fluorouracile: metaboliti privi di effetto antitumorale
1ChemSpider 2D Image | 2-Fluoroalanine | C3H6FNO2
September 22, 2012 4:27:05 PMhttp://www.chemspider.com/ImageView.aspx?id=11659864
Show 2D Show 3D 5-Fluoroalanina
1ChemSpider 2D Image | 5-Fluorodihydropyrimidine-2,4(1H,3H)-dione | C4H5FN2O2
September 22, 2012 4:21:58 PMhttp://www.chemspider.com/ImageView.aspx?id=108825
Show 2D Show 3D
1ChemSpider 2D Image | Fluorouracil | C4H3FN2O2
September 22, 2012 1:00:12 PMhttp://www.chemspider.com/ImageView.aspx?id=3268&mode=2d
Show 2D Show 3D
5-Fluorouracile 5-Fluorodiidrouracile
1ChemSpider 2D Image | 3-(Carbamoylamino)-2-fluoropropanoic acid | C4H7FN2O3
September 22, 2012 4:24:47 PMhttp://www.chemspider.com/ImageView.aspx?id=133299
Show 2D Show 3D Acido 5-Fluoroureidopropionico
DPD Diidropirimidinasi
β-Ureidopropionasi
!14

La diidropirimidina deidrogenasi
• La DPD (diidropirimidina deidrogenasi) è il primo enzima della via catabolica delle basi pirimidiniche (uracile e timina) ed è caratterizzato da minore attività enzimatica rispetto alle successive tappe enzimatiche.
• L’incapacità di inattivare le fluoropirimidine determina aumento di concentrazione dei farmaci attivi e grave tossicità neurologica, emopoietica e gastrointestinale che può essere mortale.
• Circa il 31% dei pazienti con carcinoma del colon-retto metastatico che vengono trattati con fluoropirimidine possono manifestare tossicità ematologica e gastrointestinale di grado 3/4.
15

IVS14+1G>A è la variante associata a grave alterazione funzionale di DPD
Transizione G>A nella sequenza consenso del sito di splicing nell’esone 14
L’esone 14 è deleto e viene prodotto un enzima inattivo
Esone 13! Esone 14! Esone 15!
AG! GT! AG! GT! AG! GT!
3% Eterozigoti!Mut: A! 97% Omozigoti WT!
WT: G!Esone 13! Esone 15!
Proteina non funzionale!
Tossicità grave da!fluoropirimidine!
Esone 13! Esone 14! Esone 15!
Proteina funzionale!
Normale tollerabilità da!fluoropirimidine!
16

Varianti genetiche DPD
61C>T 62G>A 74A>G 85T>C
257C>T 295-298delTCAT
100delA
496A>G 601A>C 632A>G
703C>T
812delT
Introne
5’
Esone 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
3’
1003G>T 1039delTG 1108A>G
1156G>T
1475 C>T
1601G>A 1627A>G 1679T>G 1714C>G
1896T>C 1897delC
IVS14+1G>A
2194G>A
2657G>A
2846A>T
2933A>G 2983G>T
Del Re M et al. EPMA Journal 2011
17

Attività enzimatica della DPD e tossicità delle fluoropirimidine (5-FU)
DPD
5-FdUMP
TS
Tossicità tollerabile
5-FDHU
5-FdUMP
TS
Tossicità grave/
mortale
5-FU
Deficit (allele IVS14+1G>A)
5-FDHU
5-FU
Normale
Del Re M et al. EPMA Journal 2011
18

Caso clinico - paziente 1
85T>C
496AG
Introne
5’
Esone 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
3’
1601G>A 1627A>G
1801G>C 1896T>C IVS14+1G>A
2194GA
DIARREA 4 STOMATITE 4 DERMATITE 3 ALOPECIA 2 LEUCOPENIA 3 NEUTROP 4 HFS 2
OXALIPLATINO – CAPECITABINA
19

85T>C 496AG
Introne
5’
Esone 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
3’
1601G>A
1627AG
1801G>C 1896T>C IVS14+1G>A
2194GA
Caso clinico - paziente 2
1° ciclo CISPLATINO 100 mg/mq g 1 5-‐FU 1000 mg/mq i.c. 24 ore per 5 gg
DIARREA 3 STOMATITE 3 LEUCOPENIA 3 NEUTROPENIA 4 ANEMIA 3 HFS 2
20

85T>C 496A>G
Introne
5’
Esone 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
3’
1601G>A
1627GG
1801G>C 1896T>C IVS14+1G>A
2194G>A
Caso clinico - paziente 3
FOLFOX-‐4 (Ciclo 5°)
NAUSEA/VOMITO 3 DIARREA 4 STOMATITE 3 DERMATITE 2 LEUCOPENIA 4 NEUTROPENIA 4 NEUTROPENIA FEB si HFS 2
21

85T>C 496A>G
Introne
5’
Esone 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
3’
1601G>A 1627A>G
1801G>C 1896T>C IVS14+1GA
2194G>A
Caso clinico - paziente 4
DIARREA 4 NAUSEA/VOMITO 3 STOMATITE 3 NEUTROPENIA 3 PIASTRINOPENIA 2
FOLFOX-‐4
22

85T>C 496A>G
Introne
5’
Esone 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
3’
1601G>A 1627A>G
1801G>C 1896T>C IVS14+1AA
2194G>A
Caso clinico - paziente 5
DIARREA 3 HFS 3 ALOPECIA COMPLETA MUCOSITE 3 NEUTROPENIA (febbrile) 4
5-‐FU DOSE TEST: 250 mg/m2 bolo senza folato
23

85T>C 496A>G
Introne
5’
Esone 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
3’
1601G>A 1627A>G
1801G>C 1896T>C IVS14+1G>A
2194G>A
Caso clinico - paziente 6
DIARREA 3 ALOPECIA 2 MUCOSITE 3 NEUTROPENIA (febbrile) 4
FOLFIRI
UGT1A1 7/7!
24

Proposed algorhithm for DPD evaluation in patients
Patient never treated with fluoropyrimidines
Screening for IVS14+1G>A
If negative
Treat with standard dose
If toxicity occurs
If homozygous for IVS14+1G>A
No treatment
If heterozygous
5-FU test dose or measure DPD activity
Adjust therapeutic dose based on clearance values or DPD activity
If hetero- or homozygous
Empirical adjustment of dose or – if available –
Screen for additional polymorphisms
Patient with fluoropyrimidine-induced toxicity
Screening for multiple variants
If heterozygous for IVS14+1G>A or hetero- or homozygous for
other variants
Continue treatment
If no toxicity
25

Metabolism of irinotecan
26

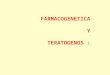
Nomenclatura delle ripetizioni TA in UGT1A1
J U L Y 2 0 0 6 • W W W . M A Y O R E F E R E N C E S E R V I C E S . O R G / C O M M U N I Q U E / • P A G E 5
Figure 2. UGT1A1 gene showing the polymorphic variation in TA repeat numbers.
demonstrate roughly a 2-fold to 4-fold decrease in glucuronidation of SN-38,14
resulting in a 50% higher risk of developingserious neutropenia (<1.0 x 10
9neutrophils/L).
Heterozygous UGT1A1*28 TA6/7 patients havea 25% reduction in UGT1A1 activity, but stillexperience a higher risk of toxicity, comparedwith homozygous UGT1A1*1 TA6/6 patients.15
Because patients homozygous for the UGT1A1*28 allele are at increased risk foririnotecan toxicity, reducing the dosage forthese patients could significantly decrease thenumber of cases of irinotecan toxicity byupwards of 50%.14 Determination of thepatient’s genotype can help the physiciandetermine the most appropriate therapy forindividual patients, thereby optimizing drugefficacy and avoiding adverse side effects.
The FDA and Camptosar Labeling
The Food and Drug Administration (FDA) is working to develop standards for theutilization of genomic data to influence safetyand efficacy of new drugs. The FDA has issued guidance requiring the submission ofpharmacogenetic data when there is evidencethat the disposition of a test compound isinfluenced by a protein encoded by apolymorphic gene. The current focus is onproven biomarkers such as UGT1A1. In 2005, the FDA required that irinotecan packagelabeling be changed to include lower dosing for homozygous UGT1A1*28 individuals(Figure 4).
—Continued next page
27

Frequenze alleliche di UGT
P A G E 4 • W W W . M A Y O R E F E R E N C E S E R V I C E S . O R G / C O M M U N I Q U E / • J U L Y 2 0 0 6
Table 1. UGT1A1 allele and genotype alleles, nomenclature, frequencies, and ethnicity information.
28

Effetto funzionale delle varianti alleliche di UGT1A1
P A G E 4 • W W W . M A Y O R E F E R E N C E S E R V I C E S . O R G / C O M M U N I Q U E / • J U L Y 2 0 0 6
Table 1. UGT1A1 allele and genotype alleles, nomenclature, frequencies, and ethnicity information.
29

Innocenti F et al. J Clin Oncol 2004
8000
2000
1500
1000
500
Genotipo TA
Correlazione tra genotipo UGT1A1 e tossicità di irinotecano
Numero
di g
ranu
lociti
neutro
fili
circolan
ti
5/6 6/6 6/7 6/8 7/7
30

Induttori ed inibitori di UGT1A1
J U L Y 2 0 0 6 • W W W . M A Y O R E F E R E N C E S E R V I C E S . O R G / C O M M U N I Q U E / • P A G E 7
At Mayo Clinic, prospective phase I and II trials are under way to ascertain safe, clinically effectiveirinotecan dosages for each UGT1A1 genotype.17,18
Factors under investigation to determine theoptimal drug regimen for each genotype are dosage, timing and frequency of drugadministration, and effective combination withother drugs.
Summary
Health care has barely begun to explore theimplications of genetic testing, but UGT1A1genotyping is a new important tool for identifyingpatients at risk for irinotecan toxicity. The FDArecognizes that UGT1A1 testing offers the potential
to reduce mortality and improve patient outcomes,and recommends lower dosages for individualswho are homozygous for the variant associatedwith reduced clearance of the drug. By utilizinggenotype testing for patients facing irinotecantherapy, physicians can weigh the risks andbenefits of therapy and tailor their patient’s careoptions.
Mayo’s exclusive license for this test includes theright to sublicense this test. MML will activelypursue agreements with other academic medicalcenters, laboratories, diagnostic test companies, andpharmaceutical companies to ensure that patientseverywhere have access to this important screeningtest. For more information, contact Mayo LabInquiry at 800-533-1710.
Table 2. Common UGT1A1-drug substrates, inhibitors, and inducers.
acetaminophenatazanaviratorvastatinbropiriminebuprenorphinecarvedilolcerivastatinclofibratecotinineethinylestradioletoposideezetimibefisetinflavopiridolgalangingemfibrozilgenisteinnalorphinenaltrexonenaringeninnicotinesimvastatinSN-38telmisartantroglitazone
diclofenacketoconazoleprobenecidsilibinintacrolimus
chrysindexamethasonephenobarbitalphenytoinrifampinritonavirSt. John’s Wort
apigenin
Substrates Inhibitors
Inducers
Inducer and Substrate
31

Metabolismo della gemcitabina
32

Caso clinico
Ipertrasaminasemia AST 575 -‐ ALT 860 Tossicità midollare Piastrinopenia: 73000/μl Anemia: 8,8 g/dl Hb Leucopenia: 1790/μl Neutropenia: 910/μl
CDBCA/GEM (dose somministrata carbopla(no 340 mg, gemcitabina 1700 mg)
CDA 79CC (omozigote mutato)
33

Major limitations of current studies on pharmacogenetics
• Insufficiently powered to detect a difference among gene,c variants
• Choice of gene,c polymorphism oken unclear
• Issue of germline vs. soma,c variants not addressed
• Standard clinical endpoints may not be suitable
• Clinical trial design -‐ retrospec,ve vs. prospec,ve data collec,on • Ethnic issue oken not taken into account • Predic,vity of drug effect confused with prognos,c value
34