Embed Size (px)
Citation preview
Laboratory for Immunohistochemistry and Immunopathology (LIIPAT), Department of Pathology,
Oslo University Hospital Rikshospitalet, Norway
Mucosal immunization:relevance to protection against
tuberculosis
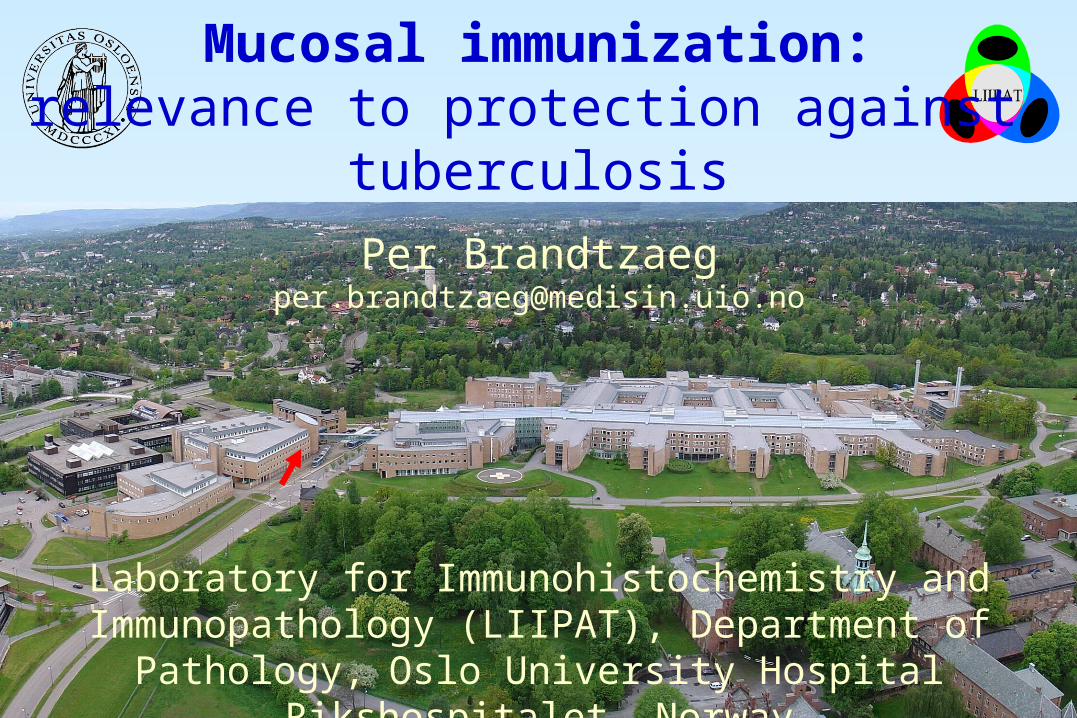
The mucosae are an enormous battlefieldMucosal effector sites provide secretory IgA (SIgA) antibodies
Section through skin
Airways and oral cavity
Gastrointestinal mucosa
Hornified layerEpithelial cells
Mucus and cilia
GlandsPlasma cells
Surface epithelium
Glands (crypts)
Plasma cells
Epithelial cells
IgAIgGNormal human colon
Plasma cellsH&E
IgA
80% of all plasma cells arelocated in gut mucosa
An adult exports 3 g of SIgA to the gut lumen per day
At the border of hell!
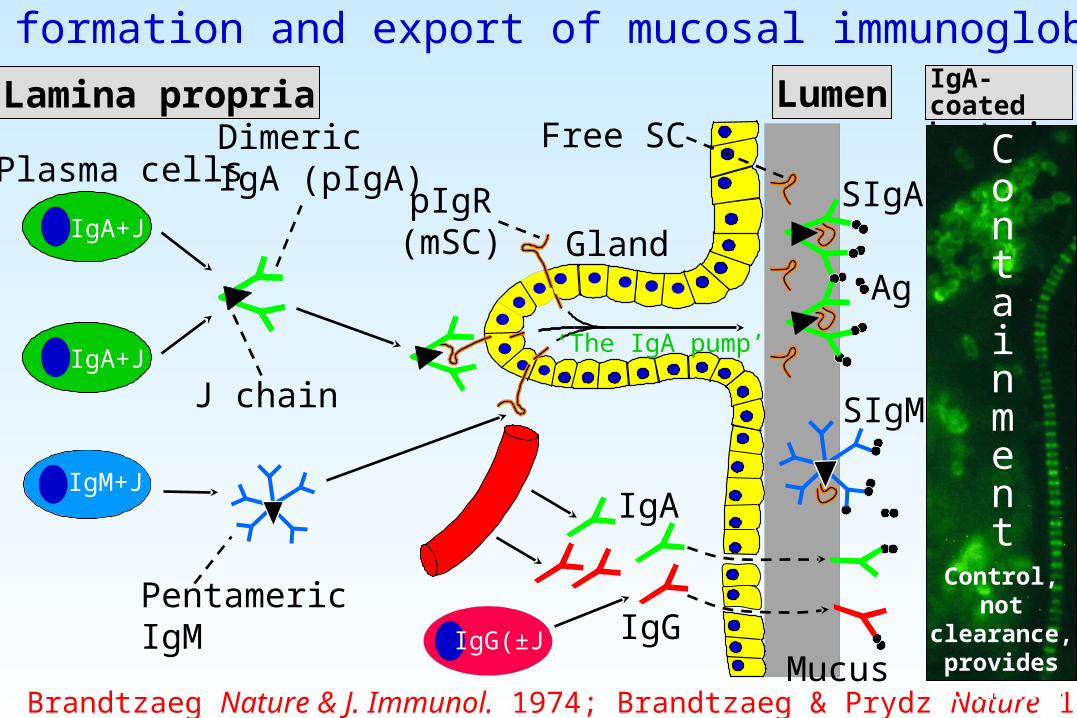
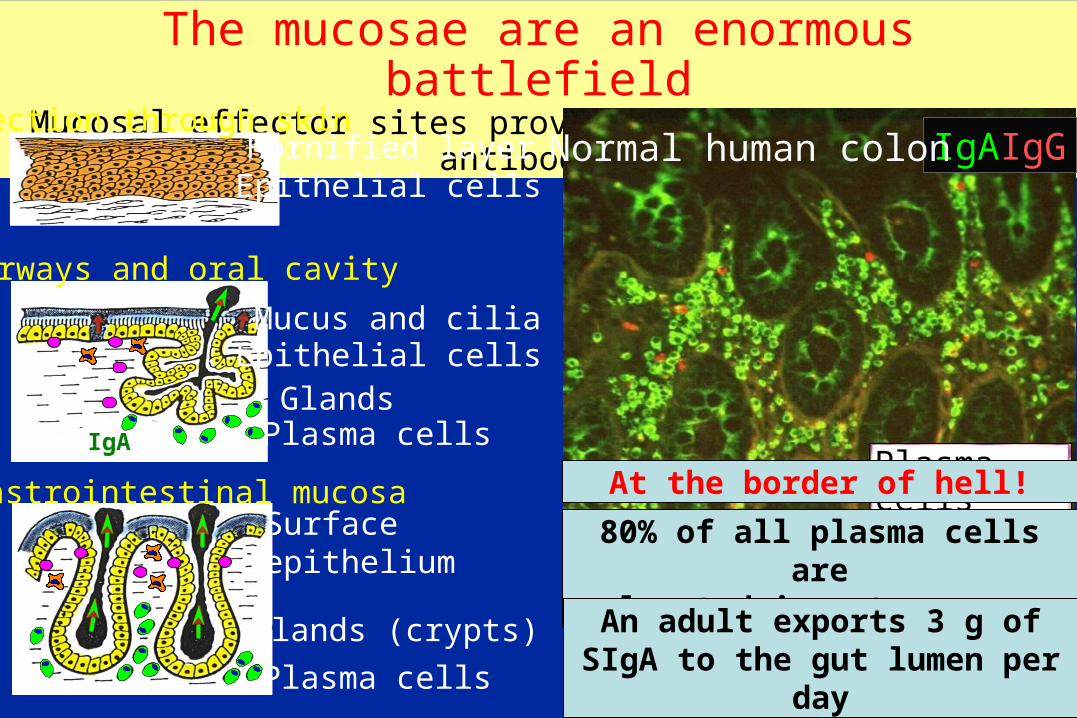
Local formation and export of mucosal immunoglobulins
Dimeric IgA (pIgA)
J chain
Mucus
Gland
IgA+J
SIgM
SIgA
IgM+J
LumenLamina propria
IgG
pIgR(mSC)
PentamericIgM IgG(±J)
Free SC
IgA+J
Plasma cells
IgA
IgA-coated bacteria
Brandtzaeg Nature & J. Immunol. 1974; Brandtzaeg & Prydz Nature 1984
Ag
‘The IgA pump’
Containment
Control, not clearance, provides
mutualism
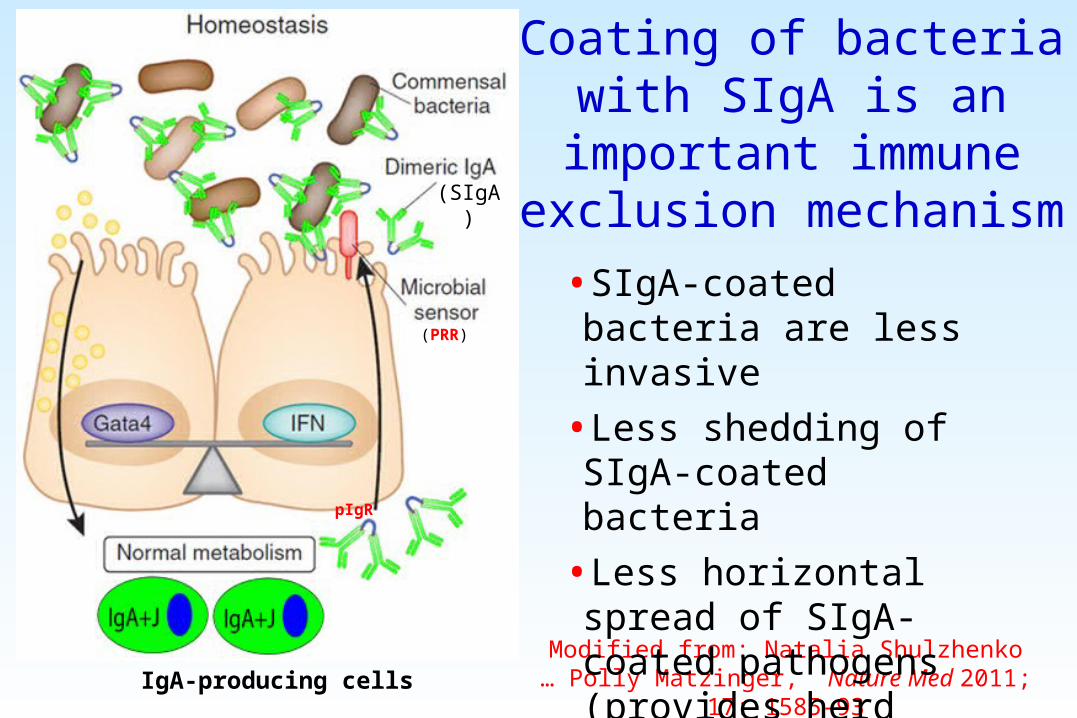
Coating of bacteria with SIgA is an important immune exclusion
mechanism
IgA-producing cellsModified from: Natalia Shulzhenko … Polly Matzinger, Nature Med 2011; 17: 1585-93
(PRR)
pIgR
•SIgA-coated bacteria are less invasive
•Less shedding of SIgA-coated bacteria
•Less horizontal spread of SIgA-coated pathogens (provides herd protection)
(SIgA)
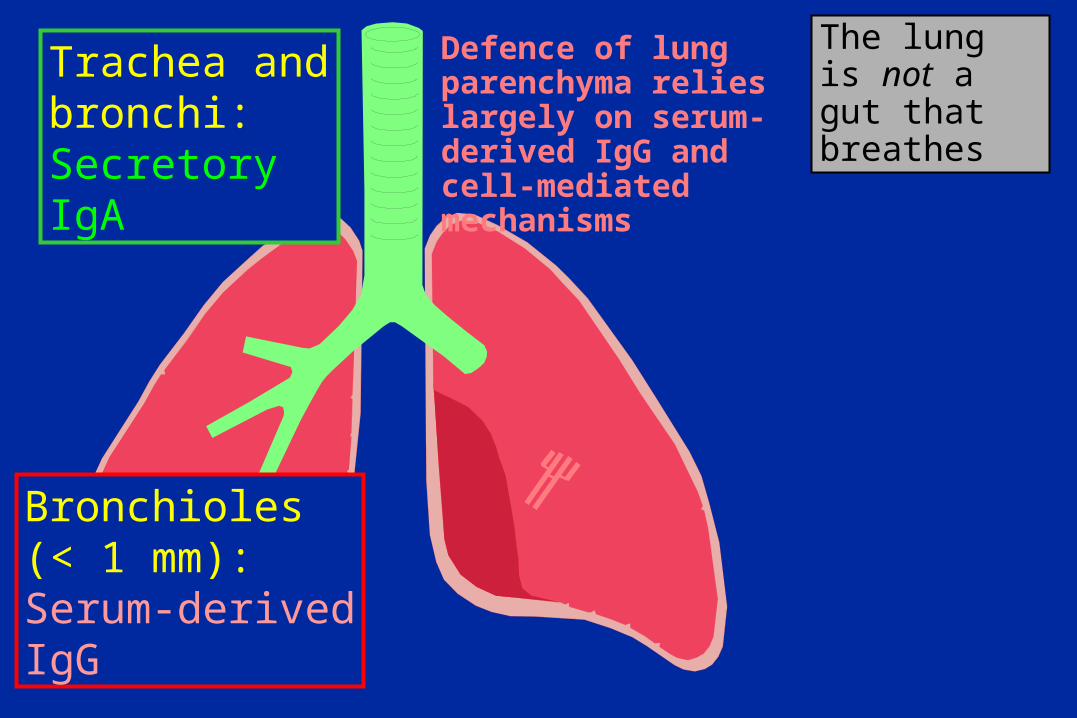
Bronchioles(< 1 mm):Serum-derivedIgG
Trachea andbronchi:Secretory IgA
Defence of lung parenchyma relies largely on serum-derived IgG and cell-mediated mechanisms
The lung is not a gut that breathes
Bronchioles(< 1 mm):Serum-derivedIgG
Trachea andbronchi:Secretory IgA
Defence of lung parenchyma relies largely on serum-derived IgG and cell-mediated mechanisms
The lung is not a gut that breathes
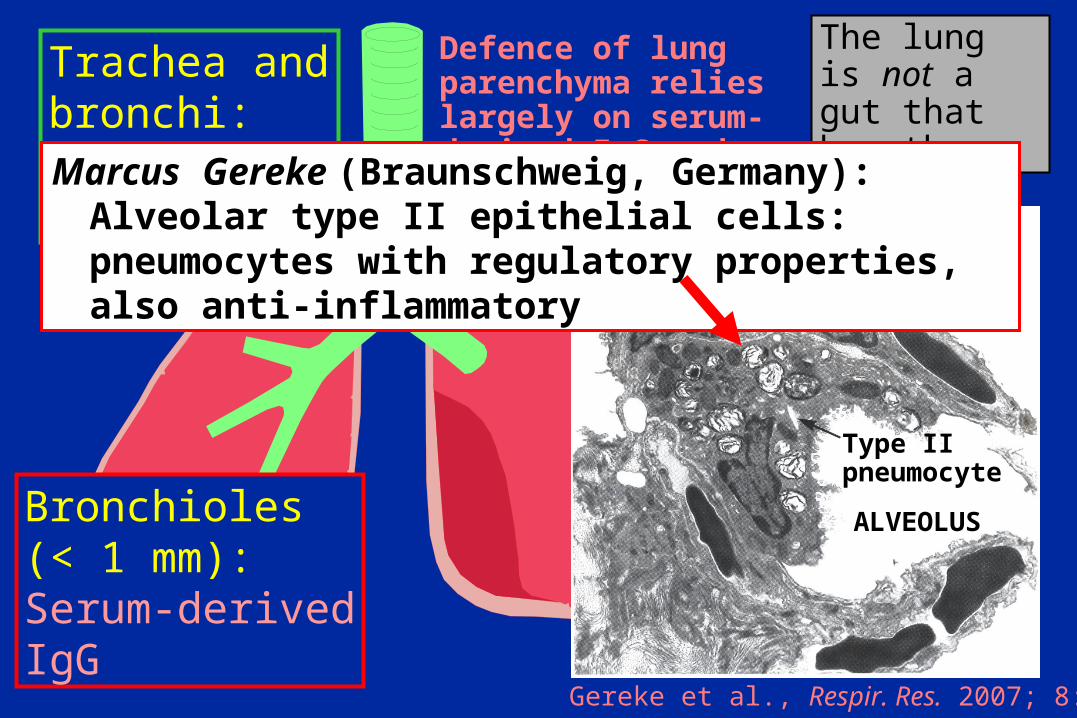
Gereke et al., Respir. Res. 2007; 8: 47
Type IIpneumocyte
ALVEOLUS
Marcus Gereke (Braunschweig, Germany):Alveolar type II epithelial cells: pneumocytes with regulatory properties, also anti-inflammatory
Homeostatic function ofmucosal vaccines
• The goal of mucosal vaccines is to stop the pathogen at the portal of entry
• This can best be achieved by induction of secretory IgA (SIgA) antibodies
• Protection against invasive mucosal pathogens requires, in addition, systemic immunity (IgG antibodies and cytotoxic T cells)
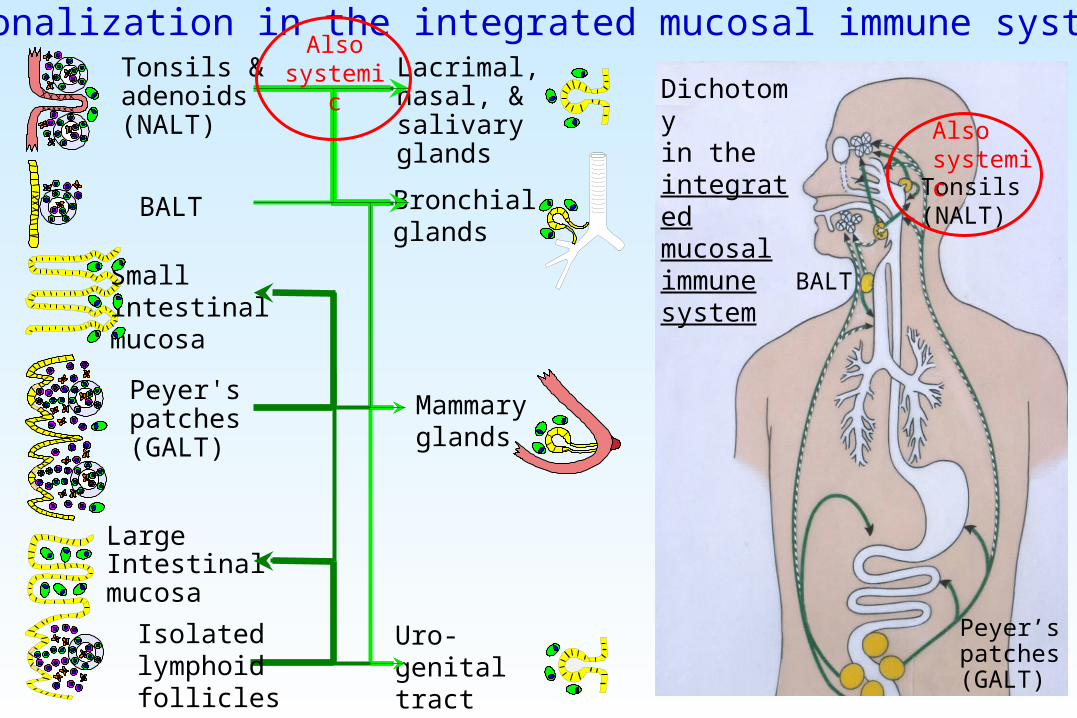
Small intestinalmucosa
Large Intestinal mucosa
Peyer'spatches(GALT)
Uro-genitaltract
Mammaryglands
Lacrimal,nasal, &salivary glands
Bronchial glands
Regionalization in the integrated mucosal immune systemTonsils &adenoids(NALT)
BALT
Dichotomy in the integrated mucosal immune system
Tonsils(NALT)
BALT
Peyer’spatches(GALT)
Isolated lymphoid follicles (GALT)
Also systemic
Also systemic
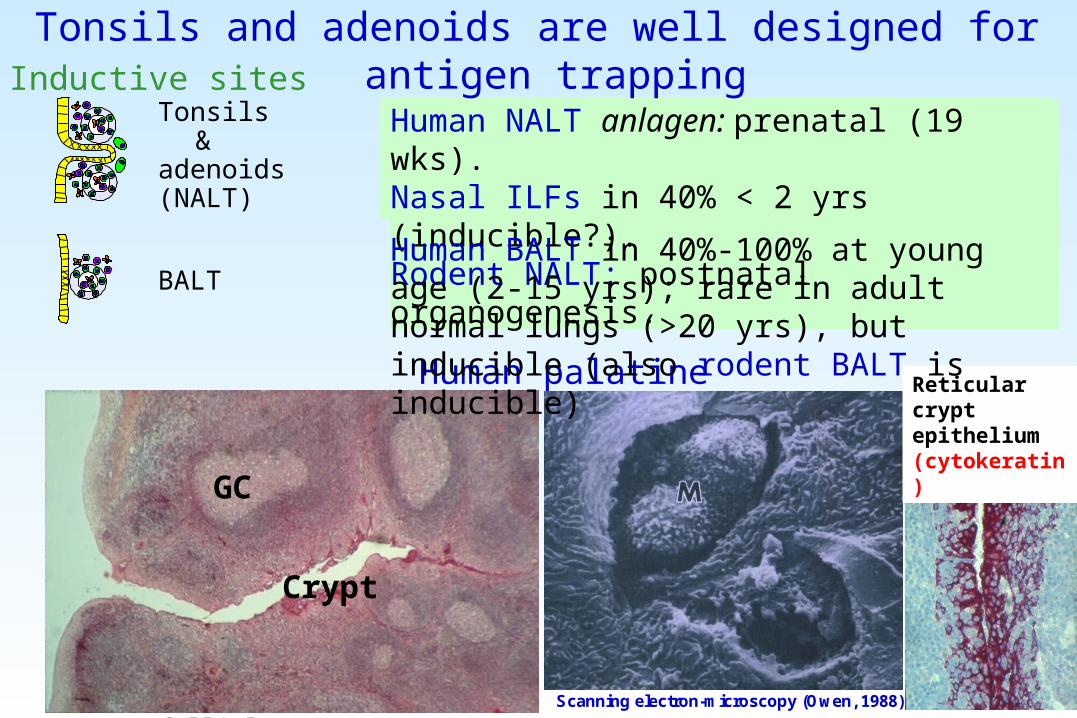
Human palatine tonsil
Human NALT anlagen: prenatal (19 wks).Nasal ILFs in 40% < 2 yrs (inducible?).Rodent NALT: postnatal organogenesis.
Tonsils and adenoids are well designed for antigen trappingInductive sites
BALT
Peyer'spatches,appendixand solitary intestinal lymphoid follicles (GALT)
Tonsils &adenoids(NALT)
GC
Crypt
Scanning electron-microscopy (Owen, 1988)
Reticular cryptepithelium(cytokeratin)
Reticular crypt epithelium (cytokeratin)
BALTHuman BALT in 40%-100% at young age (2-15 yrs); rare in adult normal lungs (>20 yrs), but inducible (also rodent BALT is inducible)
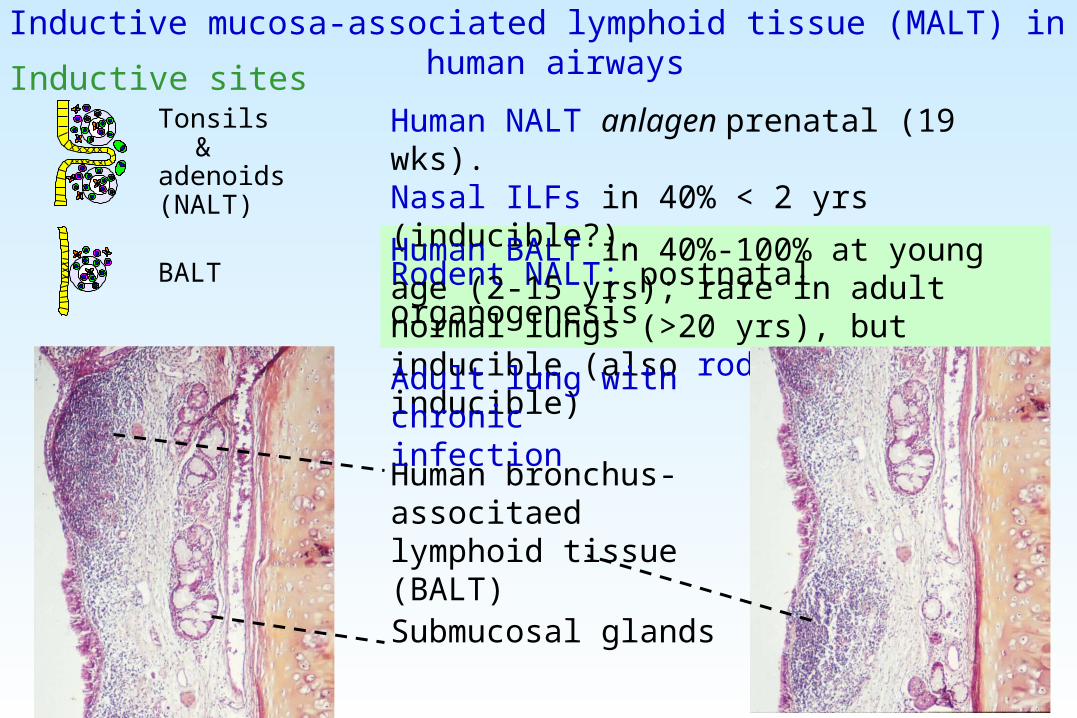
Inductive sites
BALT
Tonsils &adenoids(NALT)
Human NALT anlagen prenatal (19 wks).Nasal ILFs in 40% < 2 yrs (inducible?).Rodent NALT: postnatal organogenesis
Human BALT in 40%-100% at young age (2-15 yrs); rare in adult normal lungs (>20 yrs), but inducible (also rodent BALT is inducible)
Human bronchus-associtaed lymphoid tissue (BALT)
Submucosal glands
Adult lung with chronic infection
Inductive mucosa-associated lymphoid tissue (MALT) in human airways
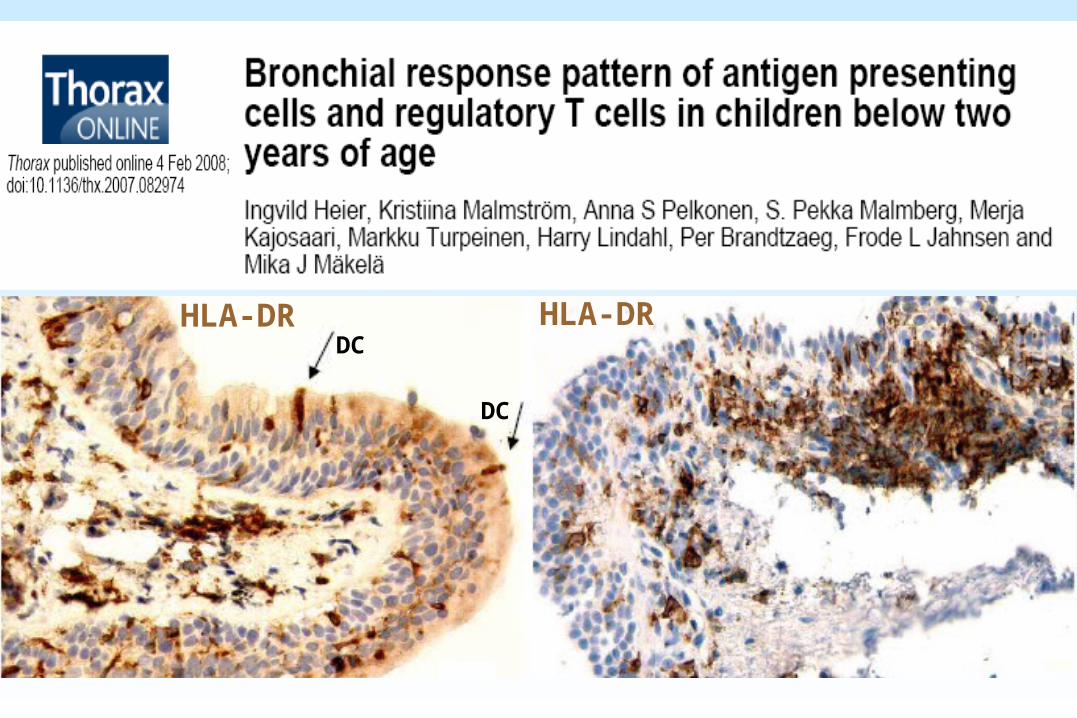
HLA-DR HLA-DR
DC
DC
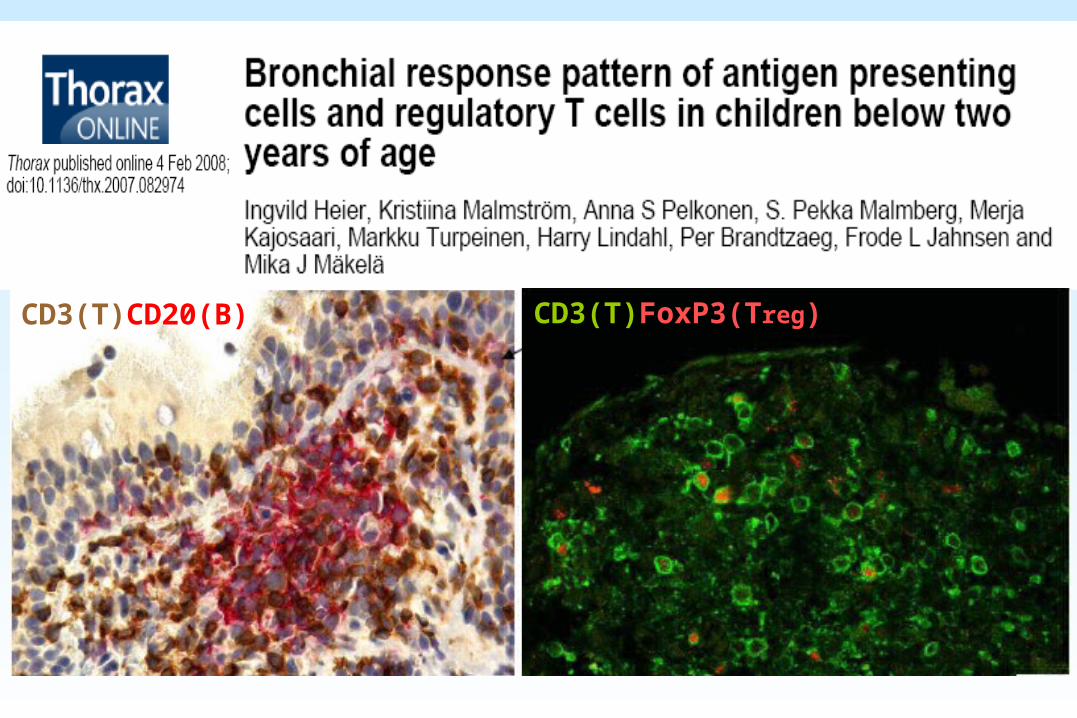
CD3(T)FoxP3(Treg)CD3(T)CD20(B)
Adenoids
Middle turbinate
Oral cavity
Tounge
Epiglottis
Inferior turbinate
Olfactory region
Tubal tonsil
Palatine tonsil
Lingual tonsil
Skin
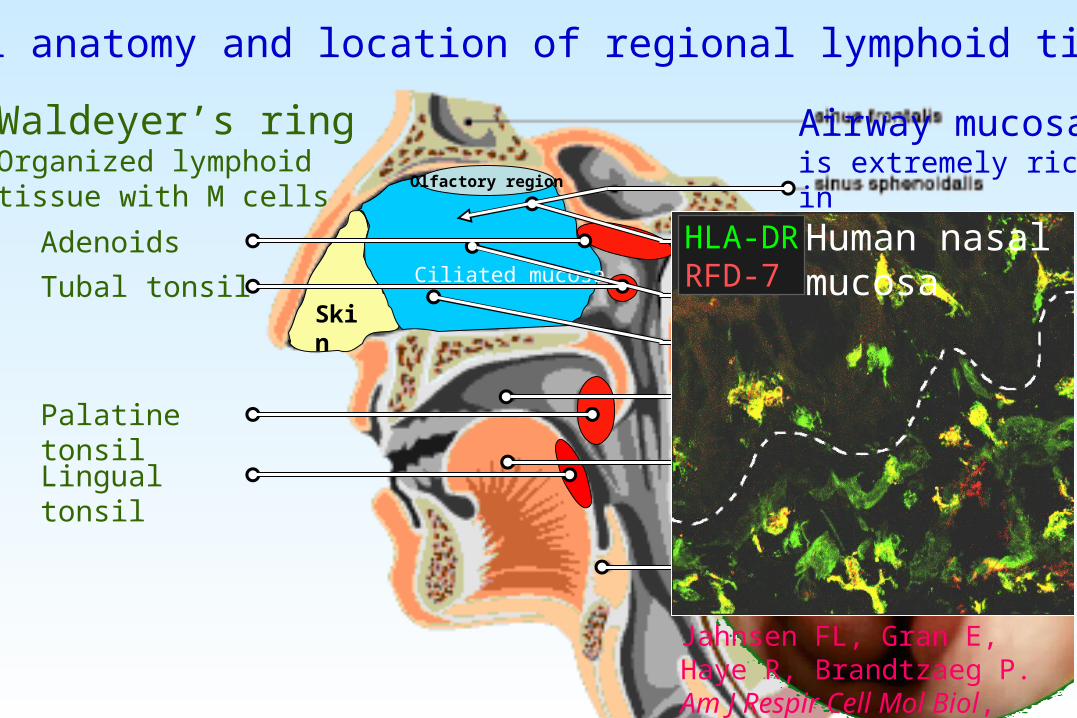
Waldeyer’s ringOrganized lymphoid tissue with M cells
Nasal anatomy and location of regional lymphoid tissue
Olfactory region
Ciliated mucosa
Airway mucosais extremely rich in dendritic cells
150-200 cm2
Jahnsen FL, Gran E, Haye R, Brandtzaeg P. Am J Respir Cell Mol Biol, 2004; 30:31-37
HLA-DRRFD-7
Human nasal mucosa

Mesentericlymph nodes
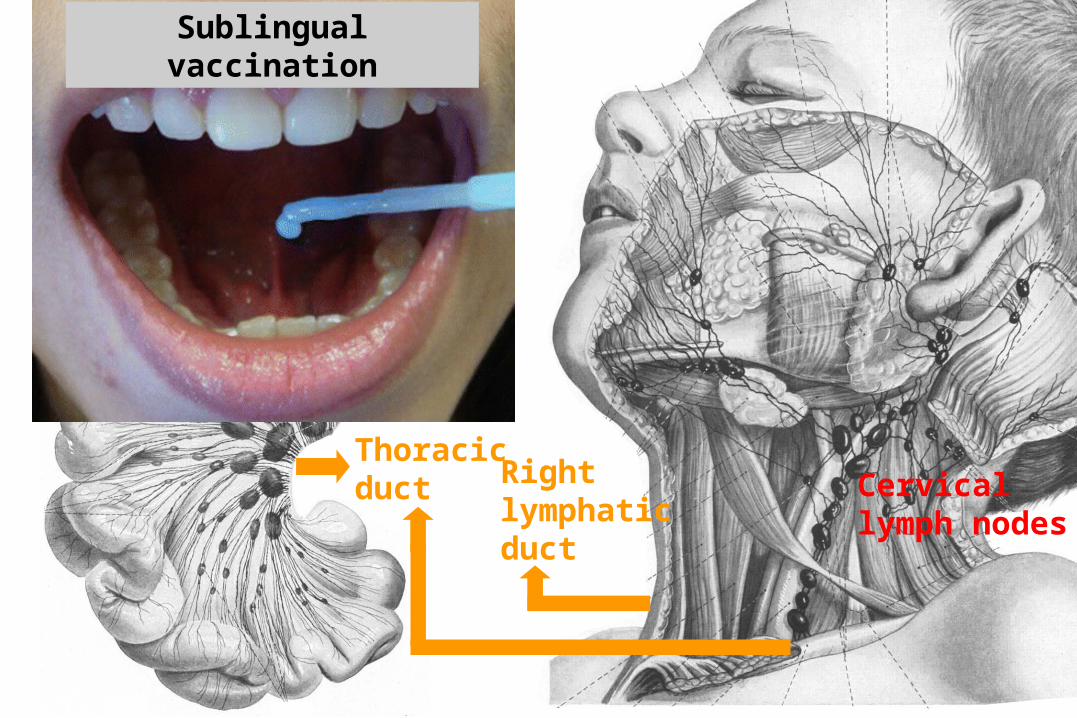
Thoracicduct Cervical
lymph nodes
Right lymphaticduct
Regional lymph drainage through mesenteric and cervical lymph nodes
Mesentericlymph nodes
Thoracicduct Cervical
lymph nodes
Right lymphaticduct
Regional lymph drainage through mesenteric and cervical lymph nodes
Sublingual vaccination
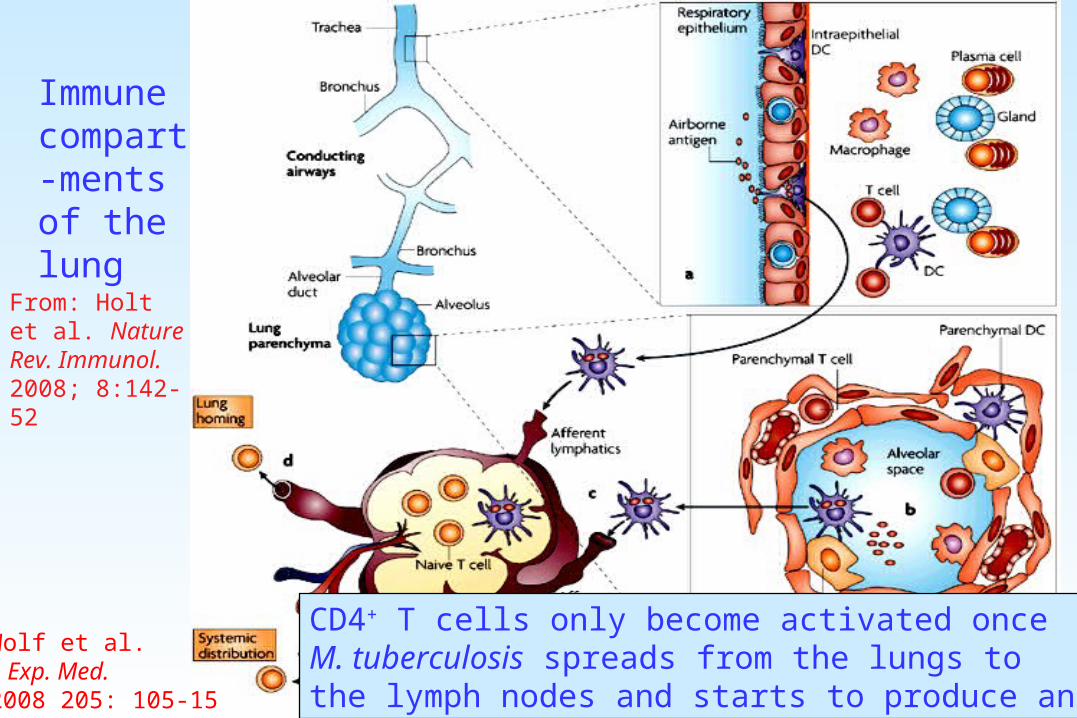
Immune compart-ments of the lung
From: Holt et al. Nature Rev. Immunol. 2008; 8:142-52
CD4+ T cells only become activated onceM. tuberculosis spreads from the lungs tothe lymph nodes and starts to produce antigen
Wolf et al.J. Exp. Med.2008 205: 105-15
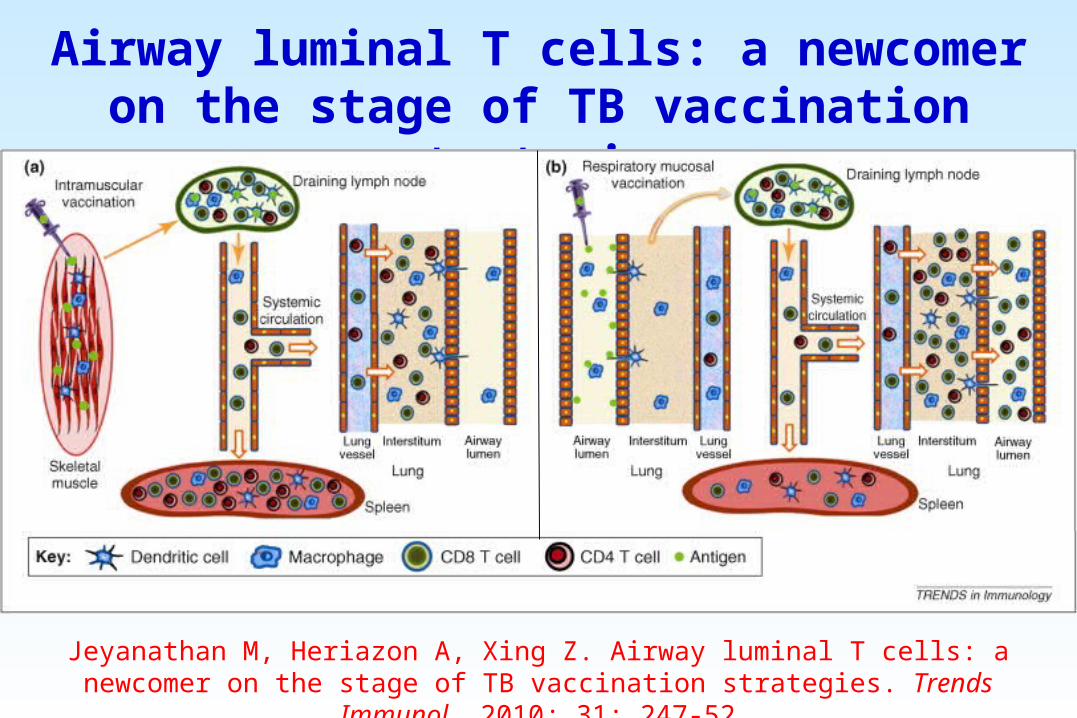
Airway luminal T cells: a newcomer on the stage of TB vaccination strategies
Jeyanathan M, Heriazon A, Xing Z. Airway luminal T cells: a newcomer on the stage of TB vaccination strategies. Trends Immunol. 2010; 31: 247-52
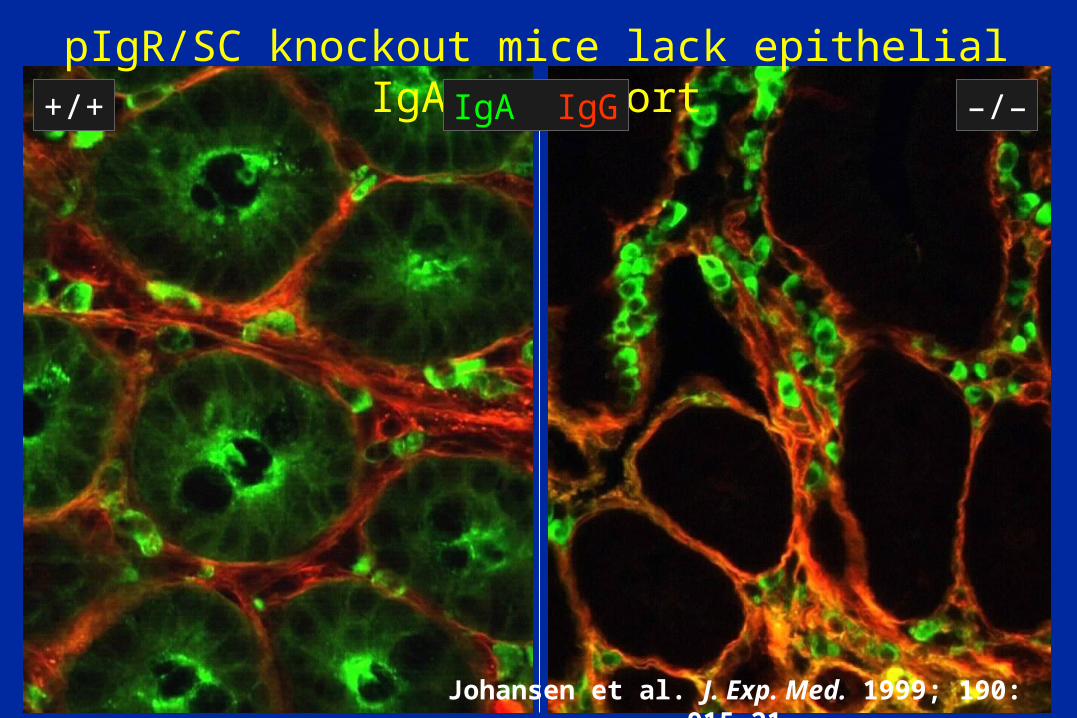
pIgR/SC knockout mice lack epithelial IgA transportIgA IgG+/+ –/–
Johansen et al. J. Exp. Med. 1999; 190: 915-21
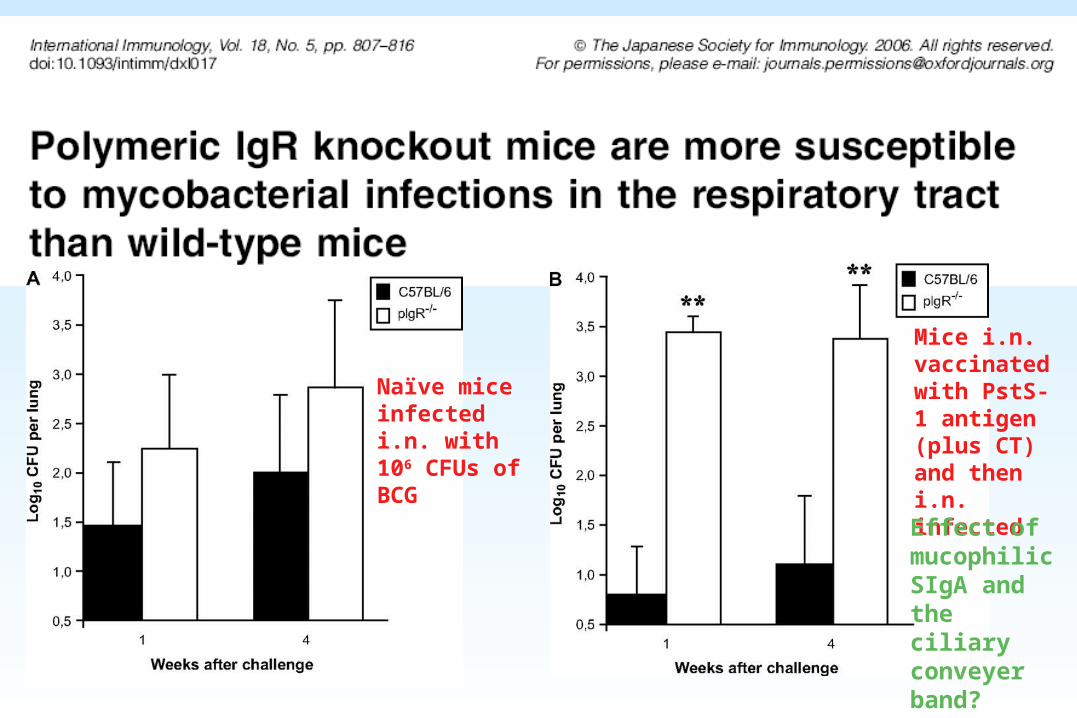
Mice i.n. vaccinated with PstS-1 antigen (plus CT) and then i.n. infected
Naïve mice infected i.n. with 106 CFUs of BCG
Effect of mucophilic SIgA and the ciliary conveyer band?
Proceedings
Passive administration of purified secretory IgA from human colostrum induces protection against Mycobacterium tuberculosis in a murine model of progressive pulmonary infection
Nadine Alvarez1
, Oscar Otero1
, Frank Camacho1
, Reinier Borrero1
, Yanely Tirado1
, Alina Puig1
, Alicia Aguilar1
, Cesar Rivas2
, Axel Cervantes2
, Gustavo Falero-Díaz1
, Armando Cádiz3
, María E Sarmiento1, Mohd Nor Norazmi4,5
, Rogelio Hernández-Pando2 and Armando Acosta1*
•
* Corresponding author: Armando Acosta [email protected] Author Affiliations
1 Department of Molecular Biology. Finlay Institute. Center of Research – Producction of Vaccines. Ave. 27 No. 19805, La Lisa. Ciudad de la Habana, Cuba. AP. 16017, CP 11600 2 Experimental Pathology Section, Department of Pathology, National Institute of Medical Sciences and Nutrition “Salvador Zubiràn”, D.F. Mexico. CP 14 000 3 Enterprise of Production of Serum and Hemoderivates “Adalberto Pesant González”. Ave 51 No.33 235 km 19 medio ½. Arroyo Arenas, La Lisa. Ciudad de la Habana, Cuba. CP 13400 4 School of Health Sciences, Universiti Sains Malaysia, 16150 Kubang Kerian, Malaysia 5 Institute for Research in Molecular Medicine, Universiti Sains Malaysia, 16150 Kubang Kerian, Malaysia For all author emails, please log on. BMC Immunology 2013, 14(Suppl 1):S3 doi:10.1186/1471-2172-14-S1-S3
Authors from Cuba, Mexico and Malaysia
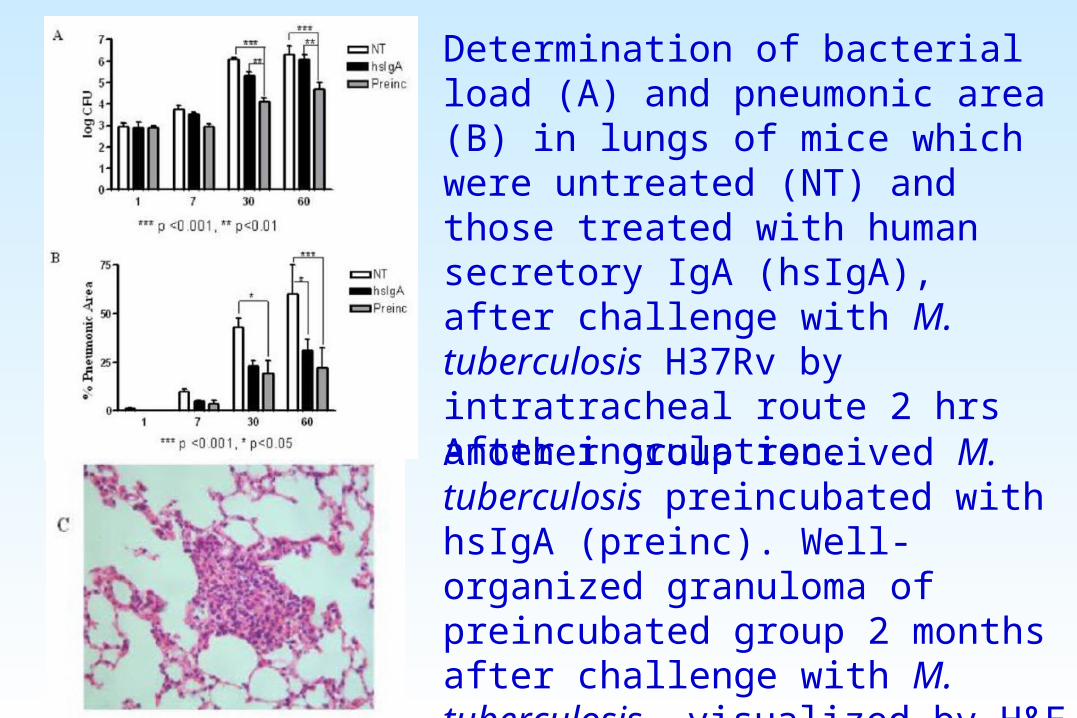
Determination of bacterial load (A) and pneumonic area (B) in lungs of mice which were untreated (NT) and those treated with human secretory IgA (hsIgA), after challenge with M. tuberculosis H37Rv by intratracheal route 2 hrs after inoculation.
Another group received M. tuberculosis preincubated with hsIgA (preinc). Well-organized granuloma of preincubated group 2 months after challenge with M. tuberculosis, visualized by H&E staining (25x) (C).
• Such vaccine administration elicits both regional mucosal and systemic immunity
• Future strategy: prime-boost approach, e.g. BCG (prime) followed by mucosal boost, or vice versa
Acknowledgements
Laboratory for Immunohistochemistry and Immunopathology (LIIPAT) is part of Centre for Vaccinology and
Immunotherapy (CEVI, 2001) and Centre of Excellence for Immune Regulation (CIR, 2007), funded by the Research Council of Norway, University of Oslo and Rikshospitalet
University Hospital