Embed Size (px)
Citation preview
Gut 1996; 38: 296-298
CASE REPORTS
Langerhan's cell histiocytosis complicating smallbowel Crohn's disease
C Lee-Elliott, J Alexander, A Gould, R Talbot, J A Snook
AbstractLangerhan's cell histiocytosis is a rareinfiltrative disorder ofunknown aetiology.A variety of tissues may be affected, butclinically evident intestinal involvement isunusual. An adult patient is describedwith Crohn's disease ofthe terminal ileumwho subsequently developed Langerhan'scell histiocytosis with extensive infiltra-tion ofthe small bowel.(Gut 1996; 38: 296-298)
Keywords: Langerhan's cell histiocytosis, Crohn'sdisease.
Langerhan's cell histiocytosis (LCH), pre-viously known as histiocytosis X, is a disorderresulting from tissue infiltration with character-istic cells of monocyte/macrophage lineage.'These cells have immunohistochemical andmorphological similarities to Langerhan's cells,specialised histiocytes normally found in theskin and squamous mucosae, which have sur-face membrane expression of CD 1 a and char-acteristic cytoplasmic organelles of unknownfunction (Birbeck granules) on electron micro-scopy.' 2 The definitive diagnosis of LCHrequires the finding of CD 1 a expression orBirbeck granules in lesional cells.2LCH may present at any age, though most
cases occur in childhood.' The manifestationsare protean, though overt intestinal involve-ment is rare. The aetiology of LCH remains tobe established: the capacity of less aggressivevariants ofLCH to remit spontaneously mightimply a reactive process, though the finding ofmonoclonality suggests that LCH may result
from neoplastic proliferation.3 An intriguinglink relates more aggressive forms of LCH tovarious haematological malignancies.2
Case reportA 76 year old woman presented in November1993 with a six month history of low gradewatery diarrhoea, right iliac fossa discomfort,weight loss, and malaise. She had a history ofrecurrent unexplained iron deficiency duringthe 1980s, and of erythema nodosum in 1987.
Physical examination including sigmoi-doscopy was unremarkable. Basic blood testsshowed a low serum albumin concentration(32 g/l) and modestly raised inflammatorymarkers (erythrocyte sedimentation rate, 61mm in first hour; C reactive protein, 14 mgll).A small bowel barium study showed narrowingof the terminal ileum, with disorganisation ofthe mucosal pattern. At colonoscopy the colonlooked normal, but examination of theterminal ileum showed patchy hyperaemia
Departments ofGastroenterologyC Lee-ElliottA GouldR TalbotJ A Snook
and HistopathologyJ Alexander
Poole Hospital NHSTrust, Poole, Dorset
Correspondence to:Dr J A Snook, Departmentof Gastroenterology, PooleHospital NHS Trust,Longfleet Road, Poole,Dorset BH15 2JB.Accepted for publication24 July 1995
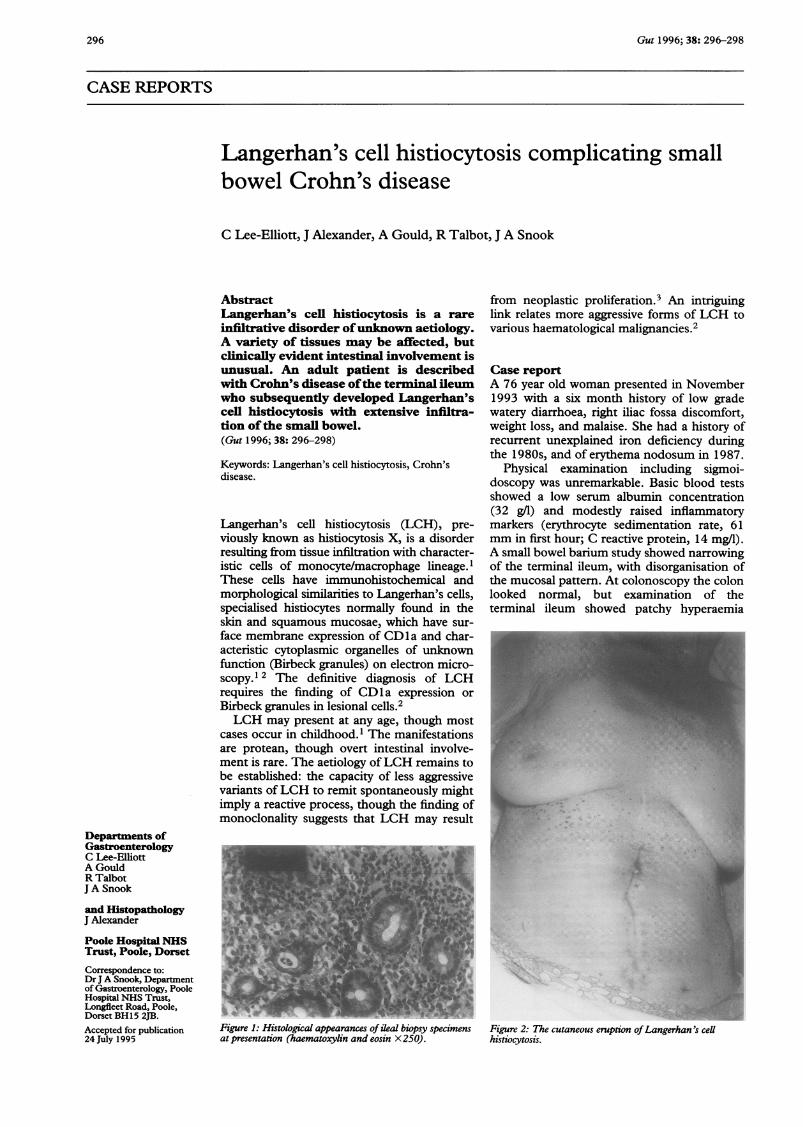
Figure 1: Histological appearances of ileal biopsy specimensat presentation (haematoxylin and eosin X 250).
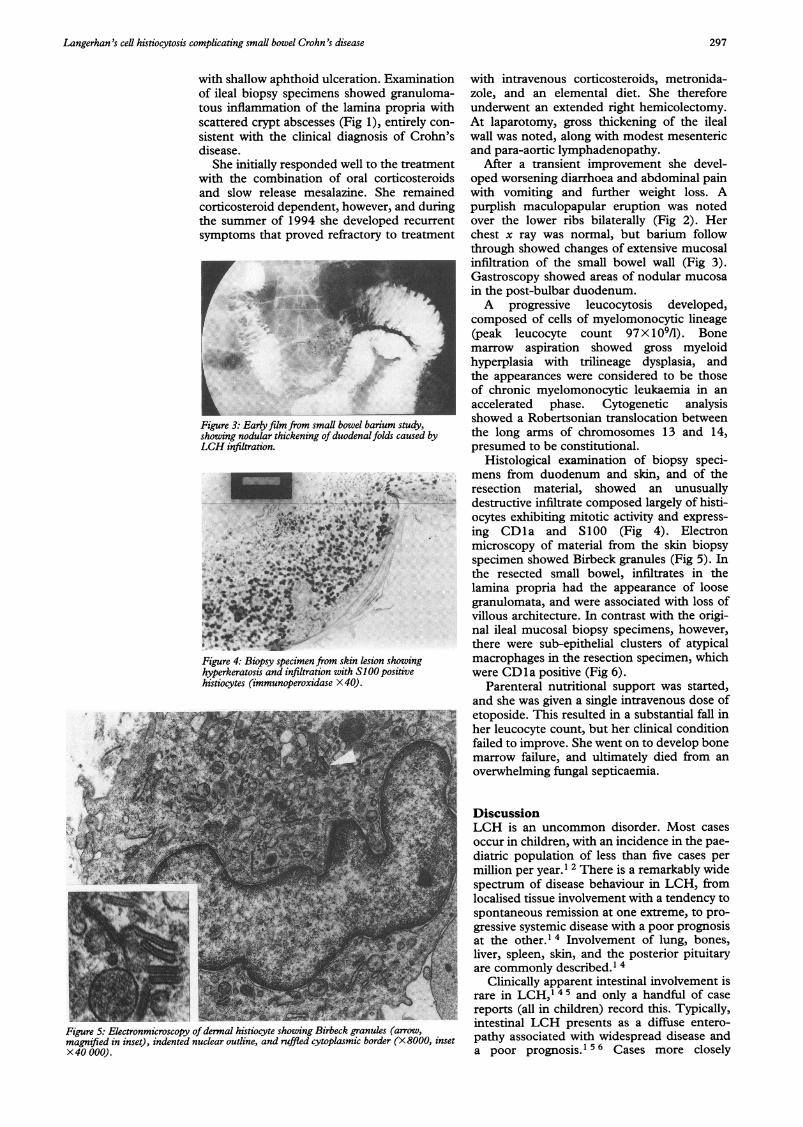
Figure 2: The cutaneous eruption ofLangerhan 's cellhistiocytosis.
296
Langerhan 's cell histiocytosis complicating small bowel Crohn 's disease
with shallow aphthoid ulceration. Examinationof ileal biopsy specimens showed granuloma-tous inflammation of the lamina propria withscattered crypt abscesses (Fig 1), entirely con-sistent with the clinical diagnosis of Crohn'sdisease.
She initially responded well to the treatmentwith the combination of oral corticosteroidsand slow release mesalazine. She remainedcorticosteroid dependent, however, and duringthe summer of 1994 she developed recurrentsymptoms that proved refractory to treatment
Figure 3: Early film from small bowel barium study,showing nodular thickening of duodenal folds caused byLCH infiltration.
Figure 4: Biopsy specimen from skin lesion showinghyperkeratosis and infiltration with SlOO positivehistiocytes (immunoperoxidase X 40).
Figure 5: Electronmicroscopy ofdermal histiocyte showing Birbeck granules (arrow,magnified in inset), indented nuclear outline, and ruffled cytoplasmic border (X 8000, insetX40 000).
with intravenous corticosteroids, metronida-zole, and an elemental diet. She thereforeunderwent an extended right hemicolectomy.At laparotomy, gross thickening of the ilealwall was noted, along with modest mesentericand para-aortic lymphadenopathy.
After a transient improvement she devel-oped worsening diarrhoea and abdominal painwith vomiting and further weight loss. Apurplish maculopapular eruption was notedover the lower ribs bilaterally (Fig 2). Herchest x ray was normal, but barium followthrough showed changes of extensive mucosalinfiltration of the small bowel wall (Fig 3).Gastroscopy showed areas of nodular mucosain the post-bulbar duodenum.A progressive leucocytosis developed,
composed of cells of myelomonocytic lineage(peak leucocyte count 97 X 109/1). Bonemarrow aspiration showed gross myeloidhyperplasia with trilineage dysplasia, andthe appearances were considered to be thoseof chronic myelomonocytic leukaemia in anaccelerated phase. Cytogenetic analysisshowed a Robertsonian translocation betweenthe long arms of chromosomes 13 and 14,presumed to be constitutional.
Histological examination of biopsy speci-mens from duodenum and skin, and of theresection material, showed an unusuallydestructive infiltrate composed largely of histi-ocytes exhibiting mitotic activity and express-ing CD1a and S100 (Fig 4). Electronmicroscopy of material from the skin biopsyspecimen showed Birbeck granules (Fig 5). Inthe resected small bowel, infiltrates in thelamina propria had the appearance of loosegranulomata, and were associated with loss ofvillous architecture. In contrast with the origi-nal ileal mucosal biopsy specimens, however,there were sub-epithelial clusters of atypicalmacrophages in the resection specimen, whichwere CD la positive (Fig 6).
Parenteral nutritional support was started,and she was given a single intravenous dose ofetoposide. This resulted in a substantial fall inher leucocyte count, but her clinical conditionfailed to improve. She went on to develop bonemarrow failure, and ultimately died from anoverwhelming fungal septicaemia.
DiscussionLCH is an uncommon disorder. Most casesoccur in children, with an incidence in the pae-diatric population of less than five cases permillion per year.' 2 There is a remarkably widespectrum of disease behaviour in LCH, fromlocalised tissue involvement with a tendency tospontaneous remission at one extreme, to pro-gressive systemic disease with a poor prognosisat the other.' 4 Involvement of lung, bones,liver, spleen, skin, and the posterior pituitaryare commonly described.' 4
Clinically apparent intestinal involvement israre in LCH,1 4 5 and only a handful of casereports (all in children) record this. Typically,intestinal LCH presents as a diffuse entero-pathy associated with widespread disease anda poor prognosis.' 5 6 Cases more closely
297

298 Lee-Elliott, Alexander, Gould, Talbot, Snook
A e.
dutr of CDJ poxsitive .~'~¼ .Figure 6. eal mucosa from resection specimen showingclusters fCDla positivehistiocytes in the lamina propria(immunoperoxidase X 250).
resembling Crohn's disease on clinical orradiological grounds, or both have beendescribed, and the histological similarities havebeen highlighted.5 For example, Sutphen andFechner have reported a child with segmentalileal narrowing,7 while Grapin et al havedescribed a case with complex anal fistulae.8There is no evidence in these cases, however,that LCH developed as a complication of pre-existing Crohn's disease.Did out patient have low grade Crohn's
disease subsequently complicated by LCH, orcould she have had LCH all along? We favourthe first explanation for two reasons. Firstly, itfits better with her history of recurrent iron defi-ciency anaemia and erythema nodosum.Secondly, her ileal tissue macrophages wereCD1a negative at initial presentation butstrikingly positive later, implying that LCH infil-tration occurred after the initial samples weretaken. Although LCH has not to our knowledgebeen previously described as a complication ofCrohn's disease, there is a well recognisedincreased incidence of (other) myeloprolifera-tive and lymphoproliferative disorders inpatients with inflammatory bowel disease.9 ei
Active inflammatory bowel disease is knownto enhance mucosal recruitment of circulatingcells of monocyte/macrophage lineage. ki Overtintestinal involvement with LCH does not nor-mally occur without evidence of major tissueinfitration elsewhere, so the predominance ofintestinal involvement in our patient mightperhaps be accounted for by pre-existing(Crohn's) disease facilitating the accumulationof LCH cells. An alterative explanation forthis distribution of disease, however, may lie in
the aberrant expression of cellular adhesionmolecules, which has recently been shown inLCH,12 resulting in abnormal homing proper-ties of the affected cells.The attractive explanation for the develop-
ment of chronic myelomonocytic leukaemia inour patient is that the leukaemic cells are pre-cursors of the infiltrating Langerhan's cells.There may, however, be a more complexexplanation, because a wide range of (other)myeloproliferative and lymphoproliferative dis-orders have been reported in association withLCH.2 13 While the treatment given for LCHmay be the cause in some instances,2 themalignancy pre-dates treatment in a substan-tial proportion of cases13 and so presumablyreflects an as yet undefined oncogenic factorassociated with LCH.
In conclusion this case illustrates the devel-opment of intestinal LCH as a complication ofileal Crohn's disease. LCH should be consid-ered in the differential diagnosis of Crohn'sdisease that becomes refractory to medicaltreatment, particularly if there is evidence of anaccompanying multisystem disorder.
1 Broadbent V, Egeler RM, Nesbit ME. Langerhan's cell his-tiocytosis - clinical and epidemiological aspects. Br JfCancer 1994; 70: S11-6.
2 Jenney MEM. Langerhan's cell histiocytosis: where do wego from here? Lancet 1994; 344: 1717-8.
3 Willman CL, Busque L, Griffith BB, Favara BE, McLainKL, Duncan MH, et al. Langerhan's cell histiocytosis(histiocytosis X) - a clonal proliferative disease. N EnglJMed 1994; 331: 154-60.
4 Leavey P, Varughese M, Breatnach F, O'Meara A.Langerhan's cell histiocytosis - a 31 year review. IrJ MedSci 1991; 160: 271-4.
5 Egeler RM, Schipper MEI, Heymans HSA. Gastrointestinalinvolvement in Langerhan's cell histiocytosis: a clinicalreport of three cases. EurJf Pediatr 1990; 149: 325-9.
6 Patel BJ, Chippindale AJ, Gupta SC. Small bowel histiocy-tosis X. Clin Radiol 1991; 44: 62-3.
7 Sutphen JL, Fechner RE. Chronic gastroenteritis in apatient with histiocytosis X. Jf Pediatr Gastroenterol Nutr1986; 5: 324-8.
8 Grapin C, Audry G, Josset P, Patte C, Sorrel Dejerine E,Gruner M. Histiocytosis X revealed by complex anal fis-tula. EurJ Pediatr Surg 1994; 4: 184-5.
9 Mir-Madjlessi SH, Farmer RG, Weick JL. Inflammatorybowel disease and leukaemia. Dig Dis Sci 1986; 31:1025-31.
10 Greenstein AJ, Gennuso R, Sachar DB, Heimann T, SmithH, Janowitz HD, et al. Extraintestinal cancers in inflam-matory bowel disease. Cancer 1986; 56: 2914-21.
11 Meuret G, Bitzi A, Hammer B. Macrophage turnover inCrohn's disease and ulcerative colitis. Gastroenterology1978; 74: 501-3.
12 de Graaf JH, Tamminga RY, Kamps WA, Timens W.Langerhan's cell histiocytosis: expression of leucocyte cel-lular adhesion molecules suggests abnormal homing anddifferentiation. Am Jf Pathol 1994; 144: 466-72.
13 Egeler RM, Neglia JP, Puccetti DM, Brennan CA, NesbitME. Association of Langerhan's cell histiocytosis withmalignant neoplasms. Cancer 1993; 71: 865-73.





























