Embed Size (px)
Citation preview

Laparoscopic Intraperitoneal OnlayInguinal Herniorrhaphy
Darra Kingsley, MD, Diana M. Vogt, MD, M. Timothy Nelson, MD, Myriam J. Curet, MD,David E. Pitcher, MD, Albuquerque, New Mexico
BACKGROUND: This study presents intermediatefollow-up data on a randomized prospective se-ries of patients undergoing either a modifiedlaparoscopic intraperitoneal onlay mesh hernior-rhaphy (IPOM) or conventional anterior inguinalherniorrhaphy (CH).
METHODS: All patients from two university affili-ated hospitals with primary or recurrent inguinalhernias were recruited for randomization to ei-ther the IPOM technique utilizing a meshed ex-panded polytetrafluorethylene (ePTFE) soft tissuepatch or CH. Follow-up data were gathered frompostoperative clinic visits and telephone andmail surveys.
RESULTS: Previously reported early recurrenceand complication rates at a mean follow-up of 8months were 1 of 30 (3%) and 5 of 30 (17%) forIPOM, and 2 of 28 (7%) and 5 of 28 (18%) for CH.Intermediate follow-up with 50 (23 IPOM and 27CH) of the original 58 patients (86%) at a meanof 41 months reveals a recurrence rate of 10 of23 (43%) for the IPOM group and 4 of 27 (15%)for the CH group (P 5 0.053). Five delayed com-plications occurred in 4 IPOM patients (port sitehernia 4, painful neuroma 1), while 2 delayedcomplications (unilateral testicular atrophy 2) oc-curred in 2 patients in the CH group. One IPOMversus 5 CH patients subsequently developedpreviously unrecognized contralateral hernias.There was 1 death unrelated to previous hernior-rhaphy in each group.
CONCLUSIONS: IPOM recurrence rates (43%) at amean follow-up of 41 months are excessivelyhigh when compared with CH (15%) or with pre-liminary results of IPOM at 8 months of follow-up(3%). Despite reduced perioperative pain anddisability and promising preliminary results in theIPOM group, these intermediate follow-up datastrongly suggest that the IPOM technique shouldnot be used for repair of inguinal hernias.
Am J Surg. 1998;176:548–553. © 1998 by Ex-cerpta Medica, Inc.
The laparoscopic era in general surgery has beencharacterized by the development of numerous in-novative minimally invasive surgical procedures.
The reduced incision-related morbidity in combinationwith equivalent or superior surgical outcomes has resultedin widespread acceptance of many laparoscopic proceduressuch as laparoscopic cholecystectomy and laparoscopicNissen fundoplication. Other procedures such as laparo-scopic colon resections for malignant disease, laparoscopicappendectomy, and laparoscopic inguinal herniorrhaphyhave not gained similar widespread enthusiastic acceptancebecause of a lack of long-term efficacy data, unfavorable orunclear cost-benefit ratios, or the inability of many sur-geons to gain the necessary training and experience.
Multiple investigators have reported favorable prelimi-nary results utilizing several different laparoscopic inguinalherniorrhaphy techniques.1–4 Results from most early se-ries are consistent in finding reduced postoperative painand discomfort, quicker return to usual activities, and su-perior patient satisfaction with the laparoscopic tech-niques. However, many initial trials suffer from a lack ofrandomization or from limited follow-up.5
Our group previously published favorable preliminary re-sults after a mean of 8 months’ follow-up from a random-ized prospective trial comparing a modified laparoscopicintraperitoneal onlay mesh herniorrhaphy technique(IPOM) with conventional inguinal herniorrhaphy (CH)utilizing either a Bassini or McVay technique.4 We reportnow on this same group of patients with a mean follow-upof 41 months.
MATERIALS AND METHODSThe details of the randomization process, operative tech-
nique, and follow-up have been previously published.4 Inbrief, Human Research Committee approval was obtainedfrom the University of New Mexico School of Medicineand the Veterans Affairs Medical Center in Albuquerque.All patients seen by the general surgery services withprimary or recurrent inguinal hernias at each institutionwere recruited for randomization. The only exclusion cri-teria was the inability to provide informed consent.
After agreeing to participate, patients were randomized toeither CH or laparoscopic (IPOM) inguinal herniorrhaphy.Conventional herniorrhaphy techniques utilized includedBassini repairs, and McVay repairs. The laparoscopic repairutilized a prototype 10 3 15 cm 3 1 mm expanded poly-tetrafluorethylene soft tissue patch (ePTFE; W.L. Gore andAssociates, Flagstaff, Arizona), which was fenestrated uti-lizing a standard skin expander using a 1:1.5 template.
From the Departments of Surgery, University of New MexicoSchool of Medicine and Albuquerque Veterans Affairs MedicalCenter, Albuquerque, New Mexico.
Requests for reprints should be addressed to David E. Pitcher,MD, Department of Surgery, ACC-2, University of New MexicoSchool of Medicine, 2211 Lomas Boulevard, NE, Albuquerque,New Mexico 87131.
Presented at the 50th Annual Meeting of the SouthwesternSurgical Congress, San Antonio, Texas, April 19–22, 1998.
548 © 1998 by Excerpta Medica, Inc. 0002-9610/98/$19.00All rights reserved. PII S0002-9610(98)00274-8

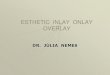
Cooper’s ligament was exposed through a small opening inthe peritoneum. The mesh was secured to Cooper’s liga-ment, the iliopubic tract, and the transversus abdominusarch utilizing an endoscopic hernia stapler (EMS HerniaStapler; Ethicon Endosurgery, Cincinnati, Ohio; Figure 1.
All patients were then seen in routine clinic postopera-tive visits and had intermittent telephone follow-up as wellto determine recovery times, early and delayed complica-tions, and recurrence rates. Patients were also asked to ranktheir degree of satisfaction with their operative repair andpostoperative outcome on a scale of 1 to 10, with 1 beingextremely dissatisfied, and 10 being extremely satisfied.
Hernia recurrence and complication rates were analyzedby chi-squared analysis for P value with 95% confidenceinterval by comparison of proportions. Ordinal data (sat-isfaction survey) were analyzed by the Mann-Whitney ranksum test.
RESULTSSixty-one patients agreed to randomization (30 IPOM
and 31 CH). Three patients in the CH group dropped outfollowing randomization and received IPOM off of proto-col. The mean age of patients was 56 years in the IPOMgroup versus 55 years in the CH group. All but 1 patientwas male. The mean operating time was 63 minutes (range35 to 115) in the IPOM group versus 81 minutes (range 45to 150) in the CH group.
IPOM patients required a mean of 5 (range 1 to 20) dosesof oral narcotic analgesic postoperatively, while CH pa-tients reported using a mean of 16 (range 6 to 28) doses.Return to normal nonstrenuous activity occurred at a meanof 7.5 (range 1 to 16) days in the IPOM group versus 18.5(range 3 to 30) days in the CH group.
Intermediate follow-up was possible with 50 (23 IPOMand 27 CH) of the original 58 patients (86%). Previouslyreported early recurrence and complication rates at a meanfollow-up of 8 months were 1 of 30 (3%) and 5 of 30(17%), respectively, for IPOM and 2 of 28 (7%) and 5 of28 (18%), respectively, for CH (not statistically different).At a mean follow-up of 41 months (range 27 to 49), therecurrence rate is 10 of 23 (43%) for the IPOM group and4 of 27 (15%) for the CH group (P 5 0.053; 95%confidence interval 3.7% to 53.6%; (Figures 2 and 3). Fivesurgeons were responsible for the 10 IPOM recurrences(one surgeon with 3, three surgeons with 2 each, and onesurgeon with 1 recurrence). Four surgeons were responsiblefor 1 recurrence each in the CH group. The delayed com-plication rate is 5 of 23 (22%) in the IPOM group and 2 of28 (7%) in the CH group (P 5 0.0272; 95% confidenceinterval 24.4% to 33.6%). Five delayed complicationsoccurred in 4 IPOM patients (port site hernia in 4, painfulneuroma in 1), and 2 delayed complications (unilateraltesticular atrophy) occurred in 2 patients in the CH group.One IPOM versus 5 CH patients subsequently developed
Figure 1. A completed intraperitoneal onlay mesh inguinal herniorrhaphy. Reprinted from Vogt et al.4
LAPAROSCOPIC INTRAPERITONEAL ONLAY INGUINAL HERNIORRHAPHY/KINGSLEY ET AL
THE AMERICAN JOURNAL OF SURGERY® VOLUME 176 DECEMBER 1998 549

previously unrecognized contralateral hernias. There was 1death unrelated to previous herniorrhaphy in each group.
Two of 4 recurrences in the CH group occurred in pa-tients who had a previous failed repair. All of the CHrecurrences occurred following repair of direct defects.Seven of the 10 recurrences in the IPOM group occurred inpatients undergoing primary hernia repair of 4 direct and 3indirect defects. The other 3 IPOM recurrences occurred inpatients with direct hernias from previously failed conven-tional hernia repairs. Of those patients who have devel-oped recurrences (4 CH and 10 IPOM), 9 have undergonea subsequent repair. Eight have chosen conventional Lich-tenstein-type mesh repairs, while 1 patient chose to un-dergo a second attempt at IPOM repair. This repair alsoresulted in recurrence, which was then repaired conven-tionally.
The mean satisfaction score at a mean follow-up of 41months is 6.7 (range 1 to 10) of patients undergoing IPOMversus 7.8 (range 1 to 10) in the CH group (P 5 0.363).
COMMENTSLaparoscopic inguinal herniorrhaphy was first described
by Ger et al6 in 1982 but did not gain significant noticeuntil the early 1990s. Since the early 1990s, laparoscopicequipment and instrumentation have improved substan-tially with the growing utilization of laparoscopic chole-cystectomy. As a result of the increasing utilization oflaparoscopic techniques, greater numbers of general sur-geons have attempted various innovative methods of lapa-roscopic inguinal hernia repair. Among the described re-
pairs are the plug and patch technique, transabdominalpreperitoneal repair (TAPP), intraperitoneal onlay meshrepair (IPOM), and the totally extraperitoneal repair(TEP).
Early repairs such as the plug and patch technique werequickly abandoned due to unacceptable early recurrencerates of 5.4% to 15%.7,8 Other repairs such as the TAPPand TEP repairs were developed based on the concepts ofhigh ligation of the sac and tension-free reinforcement ofthe inguinal floor with mesh as advocated by Stoppa andNyhus.9–15 Both the TAPP and TEP repairs require dis-section of the preperitoneal space with the potential fordissection-related morbidity.
The IPOM repair was conceived as a procedure thatwould reduce or eliminate the dissection related morbidityof the preperitoneal approach while maintaining the con-cepts of tension-free mesh reinforcement of the inguinalfloor utilizing a laparoscopic approach.16 Another per-ceived advantage of the IPOM repair is the simplicity ofthe repair and relative speed with which it can be per-formed. Since ePTFE elicits less tissue reaction and adhe-sion formation, this material was thought to be well suitedto intraperitoneal placement.16
Our group began utilizing the modified IPOM repair in1992. Initial patient acceptance and enthusiasm in combi-nation with minimal morbidity or early recurrenceprompted the institution of a randomized prospective studycomparing the modified IPOM technique to conventionalinguinal herniorrhaphy techniques that were in current usein our department at the time. Favorable preliminary re-sults from that study were reported in early 1995.4 With amean follow-up of 8 months, IPOM patients were noted torequire fewer doses of narcotic analgesic, had a quickerreturn to normal nonstrenuous activity, and had a lower(although not statistically different) early recurrence rate(3% versus 7%) when compared with the conventionalherniorrhaphy group. Complication rates were similar foreach group, and operative times were shorter for the IPOMgroup. Our conclusion based on preliminary data was thatthe modified IPOM method, although investigational, ap-peared promising as an alternative herniorrhaphy tech-nique.
However, the recurrence rate of 43% and the delayedcomplication rate of 22% in the IPOM group at a meanfollow-up of 41 months is clearly unacceptable. Many pa-tients in this study live long distances from Albuquerqueand some were lost to follow-up, so not all patients wereavailable for follow-up physical examination. Thus, the
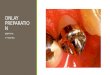
Figure 2. Outcome for primary direct and indirect inguinal hernia repairs in both the conventional herniorrhaphy (CH) group and theintraperitoneal onlay mesh (IPOM) inguinal herniorrhaphy groups.
Figure 3. Outcome for recurrent direct inguinal hernia repairs inboth the conventional herniorrhaphy (CH) and the intraperitonealonlay mesh (IPOM) inguinal herniorrhaphy groups.
LAPAROSCOPIC INTRAPERITONEAL ONLAY INGUINAL HERNIORRHAPHY/KINGSLEY ET AL
550 THE AMERICAN JOURNAL OF SURGERY® VOLUME 176 DECEMBER 1998

true recurrence and complication rates may be higher sincesome recurrences and complications can be presumed to beasymptomatic.
The actual time from initial repair to the development ofrecurrence can not be determined adequately from our datasince many patients were followed up by phone or mailsurvey and not examined routinely after the immediateperioperative period. Several patients report symptoms sug-gesting early recurrence within the first 6 months in boththe IPOM and conventional herniorrhaphy groups. How-ever, none of these patients reported the symptoms or wasexamined for recurrence until at least 1 year postopera-tively when the recurrences were discovered. The onlyobservation regarding time to recurrence we can make withcertainty is that the preliminary recurrence rates for bothIPOM and CH at a mean of 8 months follow-up are insharp contrast to the results seen at a mean follow-up of 41months. The early results may have shown a higher recur-rence rate had each patient been examined more fre-quently during the first 2 years postoperatively. Some au-thors have reported that early recurrences within the firstyear represent 25% to 50% of the long-term rate, whileothers report a consistent rise in recurrence percentagesover long periods of time.17,18 Either way, the disparity inrecurrence rates seen in this study underscore the impor-tance of and need for long-term follow-up.
No significant relationship was observed between recur-rence and operating surgeon or surgeon experience/level oftraining. This is in contrast to the findings of Liem et al19
in which a majority of recurrences could be attributed tosurgeons with limited experience with laparoscopic ingui-nal herniorrhaphy. This trial was undertaken with experi-enced laparoscopic surgeons, and only after initial resultswith nonrandomized patients appeared promising. How-ever, given the small numbers of patients and surgeonsinvolved in this study, no conclusions can be drawn re-garding the role of experience or the learning curve incontributing to or preventing recurrence.
Although no clear pattern has emerged, recurrences inthe IPOM group seem to be due to either mesh dislodge-ment from Cooper’s ligament or mesh migration due toinadequate fixation. This is similar to the findings of Sal-erno et al20 and the findings from a multi-institutional trialin which two types of technical errors (undersized meshand inadequate mesh fixation) were responsible for mostearly recurrences.21 Recurrences in the IPOM group oc-curred with both indirect and direct hernia repairs.
Our impression is that the cause of inadequate fixationand mesh migration with the modified IPOM repair isprobably multifactorial in origin. It was originally thoughtthat the thin peritoneal membrane did not represent asignificant barrier to adequate staple fixation to underlyingstructures (Cooper’s ligament, iliopubic tract, and thetransversus abdominus arch). However, early in our expe-rience, we modified our approach and used minimal sharpand blunt dissection to expose Cooper’s ligament to insuregood staple fixation to this important structure. Althoughthis may have solved the problem of medial dislodgement,it did not reduce the incidence of later mesh migration andhernia recurrence. It may be that the thickness of theperitoneum in combination with preperitoneal tissues pre-
vent adequate mesh fixation to the iliopubic tract andtransversus abdominus arch. Both animal studies and ourown experience with repeat laparoscopy in patients with aprevious IPOM repair have revealed mesh incorporationwith peritoneum, so lack of incorporation does not seem tobe a major factor in mesh migration.22 Thus, althoughmany factors may contribute to inadequate fixation andmesh migration, we cannot identify a specific cause. It isstill clear, however, that the modified IPOM techniqueresults in an unacceptably high recurrence rate.
Recurrences in the conventional herniorrhaphy groupwere most likely due to suture line tension. At the time ofthis study, conventional mesh repairs were not used rou-tinely at either institution, except for complex recurrentinguinal hernia repairs. All four recurrences in the con-ventional herniorrhaphy group occurred in patients under-going repairs without mesh.
Within the past 3 years, we have begun to use greaternumbers of tension-free mesh repairs (Lichtenstein-typerepairs) for both recurrent hernias and for primary hernias.Proponents of the tension-free mesh repairs report recur-rence rates of less than 1%, rejection rates of 0%, and awound infection rate of 0.5% with minimal postoperativepain or disability.23 Although we have not tracked ourresults with these repairs specifically, our impression is thatwe are seeing similar outcomes. These patients have re-duced degrees of postoperative pain and disability and aquicker return to normal activities than patients repairedconventionally without mesh.
Once it became apparent that the modified IPOMmethod yielded an unacceptable recurrence rate, we beganutilizing other laparoscopic repairs on select patients. Boththe TAPP method and TEP method are now offered topatients with bilateral hernias, recurrent hernias, or pa-tients with a need to return to work promptly. Patients whoare not good candidates for general anesthesia or who havehad extensive lower abdominal or pelvic surgery are notoffered the TAPP or TEP repairs. Although follow-up hasbeen too short to draw any meaningful conclusions, patientsatisfaction and acceptance seems to be high. Other inves-tigators have reported excellent short-term and intermedi-ate results with both of these techniques.19,24
Despite promising preliminary results with the modifiedIPOM technique, intermediate follow-up data reveal anunacceptably high recurrence rate and delayed complica-tion rate. Based on these results, we recommend that theIPOM technique should be abandoned. The disparity inoutcome between preliminary follow-up and intermediatefollow-up in this report should serve as a reminder to thesurgical community that long-term (5- to 10-year mini-mum) data should be required before any new herniorrha-phy technique is widely adapted.
REFERENCES1. Maddern GJ, Rudkin G, Bessell JR, et al. A comparison oflaparoscopic and open hernia repair as a day surgical procedure.Surg Endosc. 1994;12:1404–1408.2. Payne JH Jr, Grininger LM, Izawa MT, et al. Laparoscopic oropen inguinal hernia repair? A randomized, prospective trial. ArchSurg. 1994;129:973–979.3. Millikan KW, Losik ML, Doolas A. A prospective comparison oftransabdominal preperitoneal laparoscopic hernia repair versus tra-
LAPAROSCOPIC INTRAPERITONEAL ONLAY INGUINAL HERNIORRHAPHY/KINGSLEY ET AL
THE AMERICAN JOURNAL OF SURGERY® VOLUME 176 DECEMBER 1998 551

ditional open repair in a university setting. Surg Laparosc Endosc.1994;4:247–253.4. Vogt DM, Curet MJ, Pitcher DE, et al. Preliminary results of aprospective randomized trial of laparoscopic onlay versus conven-tional inguinal herniorrhaphy. Am J Surg. 1995;169:84–90.5. Swanstrom LL. Laparoscopic herniorrhaphy. Surg Clin NorthAm. 1996;76:483–491.6. Ger R, Monroe K, Duvivier R, et al. Management of indirectinguinal hernias by laparoscopic closure of the neck of the sac. Am JSurg. 1990;159:370–373.7. Greene F, Kelly W, Olsen D, et al, eds. Laparoscopic HerniaRepair. Laparoscopy in Focus 1. New York: McMahon;1992:Group8:3–6.8. Hawasli A. Laparoscopic inguinal herniorrhaphy: classificationand one year experience. J Laparoendosc Surg. 1992;4:132–143.9. Nyhus LM, Condon RE, Harkins HN. Clinical experiences withpreperitoneal hernial repair for all types of hernia of the groin. Am JSurg. 1960;100:239–244.10. Corbitt JD. Laparoscopic herniorrhaphy: a preperitoneal ten-sion-free approach. Surg Endosc. 1993;7:550–555.11. Arregui ME, Davis CJ, Yucel O, Nagan RF. Laparoscopic meshrepair of inguinal hernia using a preperitoneal approach: a prelim-inary report. Surg Laparosc Endosc. 1992;2:53–58.12. Kavic MS. Laparoscopic hernia repair. Surg Endosc. 1993;7:163–167.13. Ferzli GS, Massad A, Albert P. Extraperitoneal endoscopicinguinal hernia repair. J Laparoendosc Surg. 1992;2:281–286.14. McKernan JB, Laws HL. Laparoscopic repair of inguinal herniausing a totally extraperitoneal prosthetic approach. Surg Endosc.1993;7:26–28.
15. Stoppa RE, Waarlaumont CR. The preperitoneal approach andprosthetic repair of groin hernia. In: Nyhus LM, Condon RE, eds.Hernia. ed 3. Philadelphia: JB Lippincott; 1989.16. Toy FK, Smoot RT. Toy-Smoot laparoscopic hernioplasty. SurgLaparosc Endosc. 1991;1:151–155.17. Lichtenstein IL, Shulman AG, Amid PK. The cause, preven-tion, and treatment of recurrent groin hernia. Surg Clin North Am.1993;73:529–544.18. Beets GL, Oosterhuis KJ, Go PM, et al. Long-term follow-up(12–15 years) of a randomized controlled trial comparing Bassini-Stetten, Shouldice, and high ligation with narrowing of the inter-nal ring for primary inguinal hernia repair. J Am Coll Surg. 1997;185:352–357.19. Liem MS, Van Der Graff Y, Van Steensel CJ, et al. Compar-ison of conventional anterior surgery and laparoscopic surgery foringuinal hernia repair. NEJM. 1997;336:1541–1547.20. Salerno GM, Fitzgibbons RJ Jr, Corbitt JD Jr, et al. Laparo-scopic inguinal hernia repair. In: Zucker KA, ed. Surgical Laparos-copy Update. St. Louis: Quality Medical Publishing; 1993:373–394.21. Phillips EH, Rosenthal R, Fallas M, et al. Reasons for earlyrecurrence following laproscopic hernioplasty. Surg Endosc. 1995;9:140–145.22. Vader VL, Vogt DM, Zucker KA, et al. Adhesion formation inlaparoscopic hernia repair. Surg Endosc. 1997;11:825–829.23. Amid PK, Shulman AG, Lichtenstein IL. Critical scrutiny ofthe open “tension-free” hernioplasty. Am J Surg. 1993;165:369–371.24. Fitzgibbons RJ Jr, Camps J, Cornet DA, et al. Laparoscopicinguinal herniorrhaphy. Results of a multicenter trial. Ann Surg.1995;221:3–13.
DISCUSSIONF. Charles Brunicardi, MD (Houston, Texas): The au-
thors are to be congratulated for performing a randomizedprospective trial, for their diligence in follow-up, and fortheir honesty. The authors compared laparoscopic intra-peritoneal onlay mesh technique with Gortex mesh andcompared it with Bassini or McVay techniques. Fifty-eightpatients were randomized to either laparoscopic or openhernia repairs, and then followed up for 41 months with an86% follow-up. The initial laparoscopic hernia repair re-sults demonstrate that the patients with the lap repairrequired much less narcotic medication postoperatively,suggesting less postoperative pain, and a much quickerreturn to full activity than patients with open repair.
The authors published these optimistic early results in theAmerican Journal of Surgery in 1995. However, a 41-monthfollow-up in 86% of the patients revealed a 43% recurrencerate for the laparoscopic onlay technique and a 15% recur-rence rate for the open repairs using Bassini or McVaytechnique. The authors now conclude that the laparo-scopic intraperitoneal onlay inguinal herniorrhaphy is afailed technique and should be abandoned.
My first question is, was a statistical analysis performed onthis data? I have several other questions for Dr. Kingsley.The recurrence rates are high in both the laparoscopic andthe open groups, compared with multiple trials that havebeen published, and what are the reasons for these exces-sive rates in both groups? In terms of the onlay technique,was the hernia sac left in place? How was the inferiorlateral aspect of the patch fixed?
The manuscript also states that eight surgeons were re-sponsible for the recurrences. Since the study was con-
ducted at both the university and the VA, perhaps a flaw inthe study was the use of so many surgeons. So my finalquestions are: Could you please describe the laparoscopicexpertise of the surgeons, and were residents involved indoing the cases? I find from my own experience in ateaching institution that laparoscopic hernias are advancedprocedures and are difficult to teach. The results depend onprecise placement and fixation of the mesh. Our experi-ence at Baylor with hundreds of preperitoneal laparoscopichernia repairs suggests that it is an excellent techniquewith a 1% to 2% recurrence rate, as reported in numerousother studies, such as those of Dr. Payne and Dr. McKier-nan.
Patrick R. Reardon, MD (Houston, Texas): It seems tome that with 86% follow-up, one way to look at it is topresume that all the patients lost to follow-up either did ordid not have a recurrence. If 14% of your patients did havea recurrence and you add that percentage to either group,the numbers for both groups are unacceptable. It also seemsto me that you might want to add to your conclusions thatthe primary tissue repairs for conventional repairs are un-acceptable, since all the recurrences occurred in the pri-mary tissue repairs. I presume you’re implying that noneoccurred in the open mesh repairs you did.
R. Phillip Burns, MD (Chattanooga, Tennessee): I’d liketo ask if your data do not reflect more a failure of thematerial used, ie, the mesh to PTFE graft, than it does theprocedure? In other words, what are your results if you hadused a mesh polypropylene graft? Because in animal studiesthat we’ve done in a similar procedure, this has not beenour result at all.
LAPAROSCOPIC INTRAPERITONEAL ONLAY INGUINAL HERNIORRHAPHY/KINGSLEY ET AL
552 THE AMERICAN JOURNAL OF SURGERY® VOLUME 176 DECEMBER 1998

CLOSINGDarra Kingsley, MD: As to the first question concerning
statistical analysis on our data, the parameters that wefollowed initially were fairly subjective. And I couldn’tanswer that. What are the reasons for excessive recurrencerates? It is unclear why we had such excessive recurrencerates in both our laparoscopic and conventional hernior-rhaphy groups. As mentioned, surgeon experience andlevel of training did not seem to significantly contribute torecurrence. The concern exists because of the study’s de-sign, a prospective randomized trial, showing recurrencerate to triple when comparing conventional with laparo-scopic herniorrhaphy.
Was the hernia sac left in place? As mentioned, thehernia sac was not excised. Instead, any abdominal visceralocated within the sac were simply reduced prior to meshfixation. The IPOM technique is designed to keep dissec-tion to a minimum, making the repair practical as both atime-saving technique, and as one with relatively low peri-operative morbidity (ie, pain, bleeding) related to dissec-tion. As noted, in our study, the onlay technique actuallyhad a shorter operative time than conventional: 63.2 min-utes compared with 80.9 minutes. The only dissectionutilized was to expose Cooper’s ligament for adequate meshfixation. This was in an attempt to lessen recurrence rates,the majority of which are thought to be secondary to meshmigration.
How was the patch fixed? The inferior lateral aspect ofthe expanded PTFE graft was fixed to the iliopubic tract,utilizing an endoscopic hernia stapler. Care was taken tovisualize crucial nerves and vascular landmarks through thethin peritoneal membrane, and to avoid damage to thesestructures. Superiorly, the mesh was attached to the trans-versus abdominus arch. The inferior medial aspect wasapproximated to Cooper’s ligament, following a minimalamount of dissection overlying this important structure.
Was it a flaw to use so many surgeons? In the IPOMrepair, five surgeons were responsible for 10 recurrences,one surgeon for three, three surgeons for two each, and onesurgeon for one recurrence. In the open repair group, foursurgeons were responsible for one recurrence each. All ofthe surgeons involved were experienced laparoscopic sur-geons. The study itself was not initiated until the tech-nique had been practiced in a nonrandomized population,and the results appeared promising. Residents were indeedutilized in the operative procedures described in our study.
It was felt that the effort should be realistic, which, in ourteaching hospitals, includes the use of resident surgeons. Iflaparoscopic herniorrhaphy is a technique that we areendorsing for general acceptance, it must be able to beutilized by a large and diverse surgical community, includ-ing surgeons in training. As mentioned, no significantrelationship was noted when analyzing recurrence rates andthe operating surgeons or surgeon experience/level of train-ing.
In addressing recurrences in patients lost to follow-up, itmust be assumed that still more recurrences occurred in thepatient population lost to follow-up. Similarly, since not allof our patient population was accessible for physical in-spection of repair adequacy, and in light of the fact thatsome recurrences/complication are asymptomatic, it maybe assumed that an even higher rate of failure existed.
Are primary repairs in conventional herniorrhaphy un-acceptable? Indeed, all of our recurrences in the conven-tional herniorrhaphy group (4 of 27) occurred in patientsundergoing repairs without mesh. It has long been thoughtthat recurrence in conventional herniorrhaphy was due totissue/suture line tension. This has significantly affectedour practice at both hospitals. The tension-free mesh repairis used very commonly, and is fast becoming our standardof care.
In addressing the cause of recurrence as a consequence ofthe material utilized, we used an expanded PTFE graftmaterial, shown in several studies to be less reactive, inhopes of avoiding complications from intra-abdominal ad-hesions. Clearly, this same characteristic decreased incor-poration and/or increased migration of the mesh, bothfactors thought to contribute to recurrence in the IPOMrepair.
Whatever the cause, the results of this study havechanged our surgical practices at both hospitals. Althoughapparently valid at the time of our study’s conception, theIPOM technique has been abandoned for TEP and TAPPrepairs. A select population is currently offered laparo-scopic herniorrhaphy, primarily patients with bilateral her-nias at time of presentation and those with recurrent her-nias. Lastly, as previously mentioned, the majority of ouropen repairs currently utilize mesh, in a tension-free repair.
We would hope that whatever the material or modifica-tion, the surgical community would utilize our study, andothers like it, in abandoning the use of IPOM herniorrha-phy.
LAPAROSCOPIC INTRAPERITONEAL ONLAY INGUINAL HERNIORRHAPHY/KINGSLEY ET AL
THE AMERICAN JOURNAL OF SURGERY® VOLUME 176 DECEMBER 1998 553