Embed Size (px)
DESCRIPTION
referat trichomoniasis
Citation preview

LAPORAN KASUS
Oleh :
Vendy Dwi Prastyo, S.Ked
09700218
Pembimbing :
dr.Rudyanto Sp. PD, FINASIM

Identitas Pasien
Nama : Tn. R
Umur : 54 tahun
Alamat : Pralon,Kota Mojokerto
Suku : Jawa
Agama : Islam
Status : Menikah
No RM : S1504065483
Tanggal MRS : 22 Juni 2015
Tanggal Pemeriksaan : 23 Juni 2015

Anamnesa
Keluhan Utama : Sesak nafas
Riwayat Penyakit Sekarang :
Pasien mengeluh sesak nafas sejak ± 2 minggu SMRS, sesak nafas terutama dirasakan saat pasien beraktivitas dan berkurang saat istirahat. Sesak makin memberat 2 hari terakhir. Batuk (-), pilek (-), demam (-). Pasien juga mengeluh kedua tangan dan kedua kaki bengkak sejak ± 1 bulan SMRS. BAK lancar, nyeri (-), BAK berwarna merah 1x sehari SMRS, BAB normal. Selain itu pasien mengeluh mual sejak 2 minggu SMRS, muntah (-), nafsu makan menurun (+), dan perut dirasakan makin membesar 1 minggu terakhir.

Riwayat Penyakit Dahulu :
- DM (-) disangkal
- HT (-) disangkal
- Penyakit jantung disangkal
- Penyakit ginjal disangkal
- Alergi disangkal
Riwayat Penyakit Keluarga :
DM (-), jantung (-), HT (-)
Riwayat Sosial Ekonomi :
Merokok (+) 1 pack/hari, alkohol (-), minum jamu-jamuan (+)
Anamnesa

Anamnesa
Riwayat MRS :
2 minggu yang lalu pasien pernah rawat inap di rumah sakit citra medika mojokerto
Riwayat pengobatan :
Pasien lupa nama obat yang diminum, terakhir kontrol ??

Pemeriksaan Fisik KU : lemah
Kesadaran : Compos Mentis
GCS : 456
TD : 120/90 mmhg
Nadi : 82 x/mnt
T axila : 36,3 0C
RR : 28 x/mnt
SaO2 : 97% dengan O2 nasal canule 4 lpm

Kepala :
a/i/c/d = -/-/-/+
Leher : JVP normal, Pembesaran getah bening (-) Thoraks :
Paru :
Inspeksi : Simetris, retraksi (-), gerak nafas simetris
Palpasi : fremitus raba simetris N
Perkusi : sonor/ sonor
Auskultasi : vesikuler/ vesikuler, Rh -/- Wh -/-
Jantung :
Inspeksi : Ictus cordis tak terlihat
Palpasi : Ictus cordis teraba di ICS VI AAL S
Perkusi : Batas Jantung Kanan ICS IV PSL D
Batas Jantung Kiri ICS VI AAL S
Auskultasi : S1S2 tunggal, murmur (-), gallop (-)
Pemeriksaan Fisik

Pemeriksaan fisik Abdomen :
Inspeksi : rounded
Auskultasi : bising usus + normal
Palpasi : supel, nyeri tekan (-), shifting dullnes (+), Hepar dan lien
tidak teraba membesar
Perkusi : tymphani, Meteorismus (-)
Extremitas : Akral hangat kering (+), pitting oedem (+) pada keempat ekstremitas, CRT <2 dtk

Pemeriksaan penunjang
Pemeriksaan DL
WBC : 8.9
HB : 14,0 g/dl
HCT : 45,7 %
PLT : 228.000

- SGPT : 302
- SGOT : 228
- Urea : 63
- Creatinin : 0.8
- Albumin : 2.6
- Globulin : 2.5
- Total Protein : 5.2
- Bilirubin Total : 4.33
- Bilirubin Direk : 2.36
- Kolesterol : 192
- TG : 66
- GDA : 98
Pemeriksaan penunjang

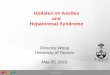
Gelombang P diikuti Q R S kompleks dengan RR interval 13 kotak kecil, HR 115 x/mnt. S di V2 + R di V5 > 35 kotak kecil.
Kesimpulan :
Sinus takikardi + LVH
EKG


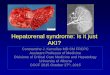
Foto Thorax• Foto thorax AP
• Soft tissue dan tulang dbn
• Jantung : batas jantung kanan normal, batas jantung kiri melebar dengan apeks jantung tertanam, pinggang jantung mendatar
• CTR : 72%
• Paru : corakan vaskular paru meningkat, sudut costophrenicus kanan tajam, kiri tertutup apeks jantung
Kesimpulan :
Kardiomegali + edema paru

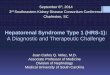
Usg Abdomen
Kesimpulan :Hepatitis kronis dengan ascites, Nefritis bilateral

Diagnosis Primer :
Hepatitis Kronis
Diagnosis Sekunder :
-
Diagnosis Komplikasi :
Decomp cordis functional class IV
Nefritis bilateral
Diagnosis

Planning
Planning diagnosa :
- Profil lipid
- LFT
- Foto thorak
- EKG
- Monitor produksi urine
Planning Terapi:
-Infus PZ lifeline 7 tpm
-O2 nasal 4 lpm
-Inj furosemide 1-0-0
-Inj pantoprasol 3 x 1 amp
-Inj granisentron 3 x 1 amp

Follow Up 23-06-2015S O A P
-pasien mengeluh sesak nafas - kedua kaki dan tangan bengkak- mata bengkak- mual +- ma/mi ↓↓
Ku : LemahKes : CM GCS : 456T :120/90 mmHgN : 82 x/mntTemp : 36,3 0CRR : 22x/mnt K/L : A-/I-/C-/D+Tho : c/ s1s2 tunggal m-p/ ves/ves rh -/- wh -/-Abd : soepel, BU + N, met -, ascites +, H/L ttb, shifting dullnes +Ext : akral hangat +/+, odem + (tangan dan kaki)GDA : 92 mg/dlProd urine : 1000 cc
Hepatitis chronis + nefritis bilateral + decomp cordis fc IV
-Planning dx : profil lipid
-Planning terapi: -Infus PZ lifeline 7tpm - O2 nasal 3 lpm - inj. Lasix 1-0-0 - inj. Pantoprazol 3x1 amp - inj. Granisentron 3x1 amp

Follow Up 24-06-2015S O A P
-sesak nafas +-Kedua tangan dan kaki bengkak- mata bengkak- mual +- ma/mi ↓↓
Ku : LemahKes : CM GCS : 456T :100/70 mmHgN : 80 x/mntTemp : 36,9 0CRR : 24x/mntK/L : A-/I-/C-/D+Tho : c/ s1s2 tunggal m-p/ ves/ves rh -/- wh -/-Abd : soepel, BU + N, met –, ascites +, shifting dullnes +Ext : akral hangat +/+, odem +(tangan dan kaki)Prod urine : 1500 ccAlbumin : 2.6Globulin : 2.5SGOT : 302SGPT : 228
Hepatitis chronis + nefritis chronis + decomp cordis fc IV
-Planning dx : foto thorax, EKG,USG abdomen
-Planning terapi: -Infus PZ lifeline 7tpm -oksigen nasal 3 lpm -Inj. Lasix 1-0-0 -Inj. Pantoprazol 3x1 amp -inj.granisentron 3x1 amp

Follow Up 25-06-2015S O A P
-sesak nafas +-Kedua tangan dan kaki bengkak- mata bengkak-Batuk +- mual +- ma/mi ↓↓
Ku : cukupKes : composmentis GCS : 456T :110/80 mmHgN : 90 x/mntTemp : 36 0CRR : 24x/mntK/L : A-/I-/C-/D+, oedem palpebra +Tho : c/ s1s2 tunggal m-p/ ves/ves rh +/+ wh -/-Abd : soepel, BU + N, met –,ascites +Ext : akral hangat +/+, odem +(tangan dan kaki)Prod urin : 3000 cc
Hepatitis chronis +nefritis bilateral + decomp cordis fc IV
Planning dx : EKG basal-Planning terapi: -Infus PZ lifeline 7tpm- -oksigen nasal 3 lpm -Inj. Lasix 1-0-0 -Inj. Pantoprazol 3x1 amp -inj.granisentron 3x1 amp -Konsul dokter jantung

Follow Up 26-06-2015S O A P
-sesak nafas + berkurang-Kedua tangan dan kaki bengkak- mata bengkak berkurang-Batuk+- mual -- ma/mi (+) sedikit
Ku : cukupKes : composmentisGCS : 456T :100/70 mmHgN : 120x/mntTemp : 37,7 0CRR : 28x/mntK/L : A-/I-/C-/D+Tho : c/ s1s2 tunggal m-p/ ves/ves rh +/+ wh -/-Abd : soepel, BU + N, met –,ascites +Ext : akral dingin +/+, odem +(tangan dan kaki)Prod urine: 2000 cc
Hepatitis chronis + nefritis bilateral + decomp cordis fc IV
Planning terapi: -Infus PZ lifeline 7tpm- -oksigen nasal 3 lpm -Inj. Lasix 1-0-0 -Inj. Pantoprazol 3x1 amp -inj.granisentron 3x1 amp-curcuma 3x1 Advis dr.Ratna, Sp.JP :- Furosemid 1x1

Follow Up 27-06-2015S O A P
-sesak nafas + berkurang-Kedua tangan dan kaki bengkak berkurang- mata bengkak (-)- mual +- ma/mi (+)sedikit
Ku : cukupKes : compGCS : 456T :110/80 mmHgN : 84x/mntTemp : 36 0CRR : 20x/mntK/L : A-/I-/C-/D+Tho : c/ s1s2 tunggal m-p/ ves/ves rh +/+ wh -/-Abd : soepel, BU + N, met –,ascites +Ext : akral dingin +/+, odem +(tangan dan kaki) berkurangProd urine :2500cc
Hepatitis chronis + nefritis bilateral + decomp cordis fc IV
Planning dx : SGOT SGPT ulangPlanning terapi: -Infus PZ lifeline 7tpm- -oksigen nasal 3 lpm -Inj. Lasix 1-0-0 -Inj. Pantoprazol 3x1 amp -inj.granisentron 3x1 amp-curcuma 3x1-furosemid 1x1

S O A P
-sesak nafas (-)-Kedua tangan dan kaki bengkak (-)- mata bengkak (-)-Batuk -- mual -- ma/mi (+) dbn
Ku : cukupKes : composmentisGCS : 456T :100/70 mmHgN : 120x/mntTemp : 37,7 0CRR : 28x/mntK/L : A-/I-/C-/D+Tho : c/ s1s2 tunggal m-p/ ves/ves rh +/+ wh -/-Abd : soepel, BU + N, met –,ascites + berkurangExt : akral dingin +/+, odem +(tangan dan kaki)Prod urin :SGOT : 65SGPT : 101
Hepatitis chronis + nefritis bilateral + decomp cordis fc IV
Planning terapi: -Infus PZ lifeline 7tpm- -oksigen nasal 3 lpm -Inj. Lasix 1-0-0 -Inj. Pantoprazol 3x1 amp -inj.granisentron 3x1 amp-curcuma 3x1-furosemid 1x1
Follow Up 28-06-2015

S O A P
-Pasien mengatakan tidak sesak-tangan dan kaki tidak bengkak-mual (-)-pusing (-)-ma/mi (+) dbn
Ku : cukupKes : compGCS : 456T :110/80 mmHgN : 84x/mntTemp : 36,2 0CRR : 28x/mntK/L : A-/I-/C-/D-Tho : c/ s1s2 tunggal m-p/ ves/ves rh +/+ wh -/-Abd : soepel, BU + N, met –,ascites -Ext : akral dingin +/+, odem -/-
Hepatitis chronis + nefritis bilateral + decomp cordis fc IV
ACC KRS hari ini :Terapi :-lanzoprazole 2x1-curcuma 3x1-furosemid 2x1 tab
Follow Up 29-06-2015

PEMBAHASAN

HEPATITIS

Hepatitis Kronis
Definisi :
Proses peradangan pada jaringan hati dengan derajat nekrosis yang bervariasi yang berjalan kronis selama 6 bulan atau lebih

Etiologi
Umumnya hepatitis kronis disebabkan oleh karena satu varian virus hepatitis saja. Penyebab tersering adalah virus hepatitis C (60-70% kasus). Virus hepatitis B sekitar (5-7% kasus), diikuti oleh infeksi hepatiti D dan penggunaan obat-obatan
A. Hepatitis autoimun
B. Penyakit hati metabolik
C. Infeksi virus
D. Obat-obatan

Klasifikasi Hepatitis kronik persisten
Hepatitis kronik aktif

Manifestasi klinik

Komplikasi

Hepatorenal Syndrome
Functional renal failure
Absence of Histological changes
Occurs in patients with chronic liver disease
Progressive liver failure and ascites
Can occur acutely in certain settings
Spontaneous bacterial peritonitis
Large volume paracentesis without albumin
Marked renal vasoconstriction
Reduced GFR
Hepatorenal Syndrome is a severe complication of end stage liver disease associated with an 80%-95% mortality at 2 weeks.



Clinical Types of HRS
Type 1
Rapid decline in renal function
Doubling of serum Cr >132 or reduction in 24h CrCl to <40ml/min
Less than 2 weeks
Spontaneous
Associated with SBP (20%) or large volume paracentesis w/o albumin (15%)

Type 2
Slower decline in renal function
Criteria for type 1 HRS not met
Development of diuretic resistant or refractory ascites
Clinical Types of HRS

Diagnosis
Lack of specific testing Diagnosis of exclusion Differential Diagnosis of renal failure in
cirrhosis :• Hypovolaemia (GI hemorrhage, shock)• Nephrotoxins (drugs, contrast)• Glomerulonephritis (Hep B and C)• Acute Tubular Necrosis • Obstruction

Diagnostic Criteria
Major Criteria
Chronic or acute liver disease with advanced liver failure or portal hypertension
Low GFR (Cr > 132-mol/L OR CrCl < 40mL/min)
Exclusion of shock, ongoing bacterial infection, volume depletion, and use of nephrotoxic drugs
No improvement in renal function despite stopping diuretics and volume repletion with 1.5L of saline
No proteinuria or ultrasonographic evidence of obstruction or parenchymal renal disease

Diagnostic Criteria
Minor Criteria
Urine volume < 500mL/day
Urine sodium < 10mEq/L
Urine osmolality > plasma osmolality
Urine RBCs < 50 per hpf
Serum sodium < 130mEq/L

Treatment of HRS
Vasoconstrictors
• Often combined with albumin
• Vasopressin analogues (Terlipressin)
TIPS (Transjugular Intrahepatic Portal Systemic Shunt)
Liver Transplantation

TERIMAKASIH...