Embed Size (px)
Citation preview

LATE EFFECTS OF
CHILDHOOD CANCERMariana Kruger
M Med Paed, M Phil, PhD
Paediatrics & Child Health, Faculty of Medicine &
Health Sciences
Stellenbosch University

“Cure is not
Enough!”Dr Gulio D’Angio

Kate Moss
Connecticut Children’s Medical Center
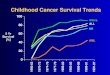
Childhood cancer survival
• Childhood cancer = success story

Current aim of childhood cancer
treatment
Maximize Cure
Minimize toxicity

Background
• 1 in 285 children will develop a cancer
before 20 years of age
• +/- 1000 children diagnosed annually in
South Africa
• Well established treatment centers since
1987
– Known number of Survivors - ?????

Definition of survivorship
• Survivor of childhood cancer 5 years post
treatment for a childhood/adolescent
cancer (Clinical definition)

Childhood cancer survivors
• 72% long term childhood cancer survivors
know their diagnosis and past treatment
• Only 35% know that their serious health
problems were due to childhood cancer
treatmentLandier W, et al. Pizzo & Poplack Section 6

Barriers to Health Care
• Less than 25% of childhood cancer
survivors have adequate follow up
• Reasons
– Historical less emphasis on long term
survivors
– Anxiety or post traumatic stress syndrome
– Poor transition to adult health services

What determine long term
effects?• Cancer type
• Individual patient’s genetics
• Treatment modalities – each with unique
toxicities
– Surgery
– Chemotherapy
– Radiotherapy
– Stem cell or bone marrow transplant

Late effects of childhood cancer
• 75% will suffer a long term effect
– 40% will suffer a significant late effect ranging from
severe to fatal
• Need lifelong surveillance for long term effects
of previous treatments
Landier W, et al. Pizzo & Poplack Section

Auditory long term effects

Auditory screening• Ototoxicity
– Cancer treatment: Platinum-based chemotherapy,
aminoglycoside antibiotics, radiation
– Audiologic evaluation at end of treatment
• Platinum-based therapy
• 30Gy or more cranial irradiation: Ongoing as radiotherapy
can cause progressive hearing loss
• Crucial to identify hearing loss early in young children as
speech is still in development
• Ongoing audiology follow up
• School assistance if hearing impaired

Occular late effects

Occular screening• Occular
– Treatment modalities: Surgery, steroids, radiotherapy
– Cataracts, glaucoma, retinopathy, xeropthalmia,
orbital hypoplasia
– Opthalmoscopic examination – depending on
treatment modality annually when >30Gy
radiotherapy received or every three-years if less
– Visual acuity annually
– School assistance if visually impaired

Dental and oral sequelae

Dental and oral screening• Teeth abnormalities due to chemotherapy
(alkylating agents < 5 years of age) & radiation >
20 Gy to mouth
– Tooth or root agenesis, thinning & shortening
– Micordontia
– Enamel dysplasia
• Mouth complications after head & neck
radiotherapy
– Xerostomia, salivary gland dysfunction
– Peridontal disease
– Osteoradionecrosis if mandible was involved

Neurocognitive sequelae

Neurocognitive sequelae• Cranial radiation & antimetabolite chemotherapy
– Especially young children with brain tumours very vulnerable
for radiotherapy
– Usually 1-2 years post treatment
– Failure to acquire new abilities
– Learning disabilities
• Inattention, slow in processing new information, memory
impairment, verbal impairment
– Receptive and expressive language problems
– Genetic susceptibility
– Annual assessment: Baseline assessment to be repeated at key
transition points and assist with vocational training

Cardiovascular sequelae

Cardiovascular sequela• Anthracyclines specifically
– Direct myocardial toxicity (formation of free radicals)
– Early (1st year of treatment) or delayed
– Cumulative dose <300 mg/m2 less likely to cause damage
– Worsened
• Young age & concomitantly radiation to mediastinum
• Interindividual variability
• Mediastinal Radiation
• Constrictive pericarditis, cardiomyopathy, valvular or coronary
heart disease, conduction abnormalities

Cardiovascular sequela• Management
– Cardioprotection during treatment
• liposomal anthracyclines & cardioprotectants
• Long term – more prone to hypertension, dislipidemia
• Screening recommendations
• Serial echocardiogram – annually to 5-year intervals depending on
cumulative dose of anthracyclines
• Exercise
– Aerobic exercise should be encourages
– Avoid isometric activities
• Weight lifting & wrestling

Pulmonary sequelae

Pulmonary sequelae
• Pulmonary fibrosis
– Mediastinal Radiation
– Chemotherapy
• Bleomycin – dose dependent
• Stem cell transplantation (SCT)
– Major cause of morbidity/mortality
– Restrictive or obstructive lung disease
– Intensity of SCT therapy plus cumulative previous therapy
– Total body irradiation (TBI) – obliterative bronchiolitis,

Pulmonary sequelae
• Baseline pulmonary functional tests & repeated
as clinically indicated
– Repeat if significant surgery is to be done
• Annual assessment for chronic cough or
dyspnea
• Smoking to be avoided at all costs
• Best – preventative: carefully monitoring
cumulative doses during treatment

Kidney sequelae

Kidney sequelae
• Chemotherapy nephrotoxicity
– Acute irreversibly renal failure
– Progressive chronic renal failure
– Renal tubular dysfunction
– Ifosfamide – up to 30% with residual disease: proximal tubular
dysfunction
• 5% significant Fanconi renal syndrome
– Cis-Platinum – Damage to glomerulus and distal tubule
• Radiation nephropathy
– Same as above
– Hyperfiltration injury
– Radiation nephritis lasting 3-12 months post radiation

Bladder sequelae

Bladder abnormalities
• Chemotherapy especially alkylating agents
– Haemorrhagic cystitis
– Bladder fibrosis
– Neurogenic bladder
• Radiation
• Similar with reduced bladder capacity
• Partial cystectomy
• Screening & follow up
– Careful history especially regarding voiding pattern
– Screen for culture negative haematuria (at least 2 occasions) &
refer to nephrologist
– Bladder dysfuntion – Urology opinion

Genitourinary follow up• Monitoring of urea and creatinine with
electrolytes
• Blood pressure monitoring
• Avoidance of nephrotoxic medicines eg
aminoglycosides, ibuprofen
• Sport participation – careful risk/benefit
assessment as certain sport can cause renal
injury e.g. marathon, iron man competitions

Gastro-intestinal sequelae

Gastro-intestinal sequelae
• Radiation
– Enteritis & fibrosis
• Strictures, ulcers, fistulas
• Stomach & small intestine more susceptible
• Liver toxicity
– Veno-occlusive disease & portal hypertension – 6-thioguanine
– Viral hepatitis
– Cirrhosis
• Screening & follow up
– Liver biopsy if indicated clinically
– Monitor for hepatomegaly, malabsorption & icterus

Endocrinology sequelae

Endocrinology sequelae• Thyroid
– Radiation – hypothyroidism
– Physical examination & annual thyroid function tests
• Gonadal function – Radiation, chemotherapy & surgery
related
– Males
• Testis radiation – Azzoospermia
• Infertility - Alkylating agents, heavy metals, dacarbazine, procarbazine
• Surgery can lead to impotence & retrograde ejaculation
– Females – alkylating agents
• Acute ovarian failure – loose ovarian function during cancer treatment
• Premature ovarian failure – early menopause before 40 yrs of age
• Screening – history, physical examination, serum
gonadotrophin levels

Pregnancy

Pregnancy
• In general not more adverse events reported in
successful pregnancies of long term survivors
• Probability of live birth less than for male
siblings
• Radiation to pelvis
– Increased risk of prematurity & low birth weight
– Malposition of fetus
– Threatened labour
– May require high risk obstetric servicesLandier W, et al. Pizzo & Poplack Section

Musculoskeletal complications

Musculoskeletal complications
• Functional & cosmetic disabilities
– Scoliosis
– Avascular necrosis
– Reduced bone mineral density
– Osteoporosis especially brain tumour survivors after radiation
• Screening & follow up
– Scoliosis risk – 6-monthy evaluation during growth spurt in
adolescence
– Diagnostic radiographs

Growth

Growth
• Decreased linear growth
– Brain tumours with >30Gy to hypothalamus & pituitary
gland
– Direct inhibition of spinal growth – radiation
– Chemotherapy induce temporary growth retardation
• Screening and management
– Monitoring serial height and weight
– Growth hormone prior to closure of epiphysis if
indicated

Obesity

Obesity• Body mass index > 30 kg/m2
• Brain tumours and ALL patients
• Insulin resistance – ALL
– Central obesity
– Elevated blood glucose
– Dyslipidemia
– Hypertension
– Pro-inflammatory & prothrombotic state
• Screening & follow up
– Annual follow up with blood glucose monitoring
– Life style management

Second malignancies

Second malignancies
• Therapy-related
– Myelodysplastic syndromes or AML – 2% 15 years after treatment
for ALL , lymphomas or sarcomas
• Alkylating agents & topoisomerase II inhibitor-related type
– Solid tumours
• Breast cancer, lung cancer & thyroid cancer after Hodgkin lymphoma with
radiation to chest or neck
• Radiation related sarcomas
• Melanoma – Stem cell transplantation and retinoblastoma survivors
• Brain tumours – meningiomas or gliomas after radiation to brain
• Nonmelanoma skin cancers
• Genetic susceptibility
– Li-Fraumeni syndrome

Challenges for Health Care
System• Transition of care
– Transfer from paediatric oncologist to adult physician
• No dedicated interesting group of physicians to take over such care
• Education of long term survivors
– Need to recognize their health care problems and seek early
health care assistance
• Adherence to follow up and life style plans
• Permanent and regular updated health care record

Models for long term care
• USA – Passport for Care (NCI, COG &
National Cancer Survivor Study – NCSS)
• EU Survivorship Passport (European
Network for Cancer Research in Children
and Adolescents - ENCCA)

Passport of
Care
• Internet-based tool
• Individualized,
accurate, & timely
health care
information
• Monitoring &
management
recommendations

Challenges for the childhood
cancer survivor• Education
– Learning disabilities
– Difficult placement in appropriate school
environment
– College & vocational training

Challenges for the childhood
cancer survivor• Economic issues
– Cost of health care
• Difficult to access medical care coverage
with high costs due to previous history of
cancer
– Insurance coverage
• Reluctance in issuing life coverage
– Employment – 1.37 times more likely
not to be employed

Recommendation for SA
• Develop electronic “passport of care” for all chronic
diseases in childhood
• Engage with adult physicians to establish health care
pathways for continuing health care and follow up for
childhood cancer survivors in adulthood
• Advocacy with medical aids and insurance
companies to assist survivors
• Engagement with education system to ensure
appropriate education with vocational training
• Advocacy with employers to ensure fair chance in
seeking employment

Needs Team work

Thank your for your attention
Dankie vir u aandag
Nkosi