Upload
stallioncode5009
View
222
Download
0
Embed Size (px)
Citation preview
7/21/2019 LCH Sunil Sir
1/25
Langerhans cell histiocytosis: Current insights in a molecular age with
emphasis on clinical oral and maxillofacial pathology practice
John Hicks, DDS, MS, PhD, MD,a and Catherine M. Flaitz, DDS, MS,b Houston, Tex
TEXAS CHILDRENS HOSPITAL, BAYLOR COLLEGE OF MEDICINE, AND THE UNIVERSITY OF TEXASHEALTH SCIENCE CENTER AT HOUSTON
Langerhans cell histiocytosis (LCH) commonly involves the oral and maxillofacial region, and comes to the attention
of dental practitioners when a patient presents with orofacial pain and a bony or soft tissue lesion. This is a relatively rare entity,
which has made it difficult to investigate the clinical, biologic, and molecular aspects of the disease. Treatment protocols are not
well defined, particularly in adults. During the past decade, the Histiocyte Society has formulated various LCH categories, based
on risk stratification, and treatment protocols for the pediatric population. Adult trials are currently available through the
Histiocyte Society. Although there has been considerable controversy, the neoplastic nature of LCH has been established by
demonstrating clonality. LCH symptoms and the development and persistence of LCH lesions have been ascribed to a
chemokine/cytokine storm due to autocrine and paracrine mechanisms. Discovery of biologic, cytogenetic, and molecular
abnormalities in LCH have already affected treatment by providing novel therapeutic targets. (Oral Surg Oral Med Oral Pathol
Oral Radiol Endod 2005;100:S42-66)
Langerhans cell histiocytosis is rare and unique
among human diseases. Our understanding of this
condition has significantly advanced and evolved over
the past century.1,2 Recognition of the disease entity
took a considerable period of time. Although not
recognized as a histiocytic disease, the first case was
described in 1865 in a 4-year-old child with impetigo
andlarge punched-out osteolytic lesions in his calvar-
ium.1,2 At that time, the bony lesions were considered to
be congenital in nature, and the child died 1 month later
of respiratory compromise. The clinical entity Hand-Schuller-Christian disease came about with independent
case reports of children with exophthalmos, polyuria,
great thirst (polydypsia), osteomalacia, and map-like
skull defects by Hand in 1892, Schuller in 1915, and
Christian in 1919.1,2 The disease was initially attributed
to tuberculosis. Letterer-Siwe Disease was initially
described in 1924 by Letterer and later in 1933 by Siwe
as an acute fulminant nonleukemic disorder of the
reticuloendothelial system in 2 young children.1,2 This
condition was characterized by marked splenomeg-
aly, hepatomegaly, lymphadenopathy, localized bone
tumors, hemorrhagic diathesis, anemia, and hyperplasia
of nonlipidized histiocytes. This disease was consid-
ered to be a rare unknown storage disorder. Eosinophilic
granuloma of bone was described first in 1930 by
Mignon as a granulomatous bone lesion in an adolescent
boy.1,2 It was Lichenstein and Jaffe in 1940 who coined
the term eosinophilic granuloma of bone, and these
lesions were thought to represent viral granulomasdespite their propensity to destroy bone.1,2
The suggestion that Hand-Schuller-Christian disease,
Letterer-Siwe disease, and eosinophilic granuloma of
bone were part of thesame disease process with variation
in severity, site of involvement, and stage was made
by Farber in 1941.1,2 Lichenstein and Jaffe embraced
this idea, and in 1953 included allthese entities under the
general category of Histiocytosis X.1-3 This term was
intended to reflect the inflammatory and proliferativenature of the disease. The unification of these three
separately described diseases under one category was
based on the nearly identical histopathologic featuresof the lesions, which were composed of eosinophils,
histiocytes, and lymphocytes. Histiocytosis X was sub-
divided into acute and subacute disseminated, chronic
disseminated, and localized forms. The original disease
designations, Hand-Schuller-Christian disease, Letterer-
Siwe disease, and eosinophilic granuloma, are still used
by some practitioners when referring to the clinical
features of Langerhans cell histiocytosis (LCH).
In the inaugural 1948 volume ofOral Surgery, Oral
Medicine, and Oral Pathology,which has since evolved
aProfessor of Pathology, Medical Director of Surgical and Ultra-
structural Pathology, Texas Childrens Hospital; Medical Director ofTexas Childrens Cancer Center, Cytogenetics and Molecular
Genetics, Baylor College of Medicine; and Adjunct Professor,
Department of Pediatric Dentistry, The University of Texas Health
Science Center at Houston, Dental Branch, Houston, Tex.bDean and Professor, Departments of Diagnostic Sciences and
Pediatric Dentistry, The University of Texas Health Science Center
at Houston, Dental Branch, Houston, Tex.
Received for publication Jun 14, 2005; returned for revision Jun 19,
2005; accepted for publication Jun 24, 2005.
1079-2104/$ - see front matter
2005 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2005.06.016
S42
http://-/?-http://-/?-http://-/?-http://-/?-7/21/2019 LCH Sunil Sir
2/25
into the current journal, eosinophilic granuloma of the
jaw in a 31-year-old man with an anal fistula was
chronicled.3 From 1942 until 1945, the patient under-
went several oral surgical procedures with biopsies
that revealed features that would now be recognized as
LCH, but were referred to as an unusual inflammatory,
infectious, and peculiar granulomatous process. Similarfindings were noted in the anal ulcer. It was not until late
1945 that the quite probable diagnosis of eosinophilic
granuloma of bone was rendered. Radiation therapy was
initiated and the jaw lesions resolved with no evidence
of disease at a 1-year follow-up.
Although LCH is a rare orphan disease, consider-
able advances have been made since the first case report
of eosinophilic granuloma of the jaw occurred in the
1948 volume ofOral Surgery, Oral Medicine, and Oral
Pathology.3 Clinical classification, advances in clinical
and pathologic diagnostic methods, identification of the
responsible cell type, and characterization of cellular
components and molecular genetics in this disease
process have been further defined.
CELL OF ORIGIN: LANGERHANS CELLHISTIOCYTES
Almost 140 years ago, Langerhans cells in the skin
were discovered using gold labeling techniques and
described as being intraepidermal receptors for cutane-
ous nervous system signals.1,2 Little progress was made
in understanding the nature of Langerhans cells until the
early 1960s when electron microscopy became avail-
able. Definitive identification of Langerhans cells was
possible with characterization of a cell-specific organ-elle, the Langerhans body, and the histiocytic nature of
the cell became apparent.1,2 This unique ultrastructural
organelle is commonly known as the Birbeck granule.
With the development of immunocytochemical anti-
body techniques, in situ hybridization, and molecular
techniques, a great deal of knowledge regarding these
cells has been gained. Langerhans cells have proven to
be bone marrowederived antigen processing cells and
represent the most peripheral extension of the immune
system. These cells were considered to be histiocytes.
The pathologic proliferation of these cells is referred to
as LCH.Langerhans cells are derived from CD34-positive
(1) hematopoietic myeloid stem cells in the bone
marrow.4-15 Under the influence of various immune
modulators, the progenitor cells can be induced to
become typical macrophages (histiocytes, monocytes)
or transitional macrophages/dendritic cell precursors.
These precursor cells give rise to a variety of dendritic
cells when specific inducing cytokines, chemokines,
and growth factors are present. Langerhans cells, in-
determinant cells, interdigitating dendritic cells, dermal
dendrocytes, and follicular dendritic cells arise from
these transitional macrophage/dendritic precursors.
Mesenchymal progenitor cells may further influence
differentiation toward dermal dendrocytes and lymph
node follicular dendritic cells.
With the advent of immunocytochemical and flow
cytometric methods, it has been possible to defineseveral different disease entitiesbased on the cell types
and clinical features (Table I).4-15 The contemporary
classification of histiocytic disorders is based on the
cell of origin responsible for the disease, relatively well-
characterized clinical features, the biologic behavior
of the disease, and proven malignant potential. LCH
is classified under dendritic cellerelated disorders of
varied biologic behavior, and the responsible cell is con-
sidered to be an immature dendritic cellthe Langer-
hans cell histiocyte. It is interesting to note that had the
dendritic origin of the proliferating cells in LCH been
recognized during Lichenstein and Jaffes era, this
disease would probably be known currently as Langer-
hans cell dendritocytosis.
LANGERHANS CELLS AND LANGERHANS CELLHISTIOCYTES: A COMPARISON
Langerhans cells are freely mobile cells that originate
from bone marrow myeloid precursors, and migrate via
afferent lymphatic channels to populate the epidermis,
regional lymph nodes, thymic epithelium, and oral and
bronchial mucosa.1,2,4-15 Although these cells represent
less than 2% of the epidermal cell population, their
dendritic processes cover 25% of all epithelial cell
surfaces in the epidermis. Each Langerhans cell pos-sesses many dendritic processes that may overlap with
processes from other Langerhans cells. The Langerhans
cell is a mature dendritic cell that has important immu-
nologic functions. These cells are antigen-presenting
cells, and are capable of presenting alloantigens and
soluble foreign antigens to naive helper T-cell lympho-
cytes (CD4 positive). Langerhans cells are nonadherent
and do not proliferate in normal tissue culture condi-
tions. Even though these cells can endocytose soluble
antigens, they are considered to be nonphagocytic cells.
With the uptake of antigen, Langerhans cells migrate
to afferent lymphatic channels and make their way toparacortical zones in regional lymph nodes. Once there,
the endocytosed antigens are presented to naive helper
T cells. Keratinocytes produce certain cytokines that
can inhibit normal Langerhans cell function. Ultraviolet
light reduces their antigen-presenting function and may
be a primary factor in skin cancer development. Langer-
hans cells may be induced to express CD4 on their
surfaces. This allows for infection by human immuno-
deficiency virus (HIV), andLangerhans cells are consid-
ered a reservoir for this virus. Strong chemoattractants
OOOOE
Volume 100, Number 2 Hicks and Flaitz S43
7/21/2019 LCH Sunil Sir
3/25
that induce migration of Langerhans cells include
interleukin (IL)-1-beta, IL-8, and granulocyte macro-
phage-colony stimulating factor (GM-CSF). Langer-
hans cells also produce IL-1-beta and tumor necrosis
factor (TNF)-alpha. Langerhans cells have not proven to
be clonal. These cells are primary antigen processing
cells, and represent the most peripheral extension of the
immune system.
In contrast to normal Langerhans cells, Langerhans
cell histiocytes are immature dendritic cells that areresponsible for a rare, unique disease process
Langerhans cell histiocytosis.1,2,4-15 These histiocytes
are a constituent of lesions occurring in bone, skin,
lymph nodes, spleen, liver, thymus, bone marrow, the
central nervous system, and the gastrointestinal tract.
Despite the activated state of Langerhans cell histio-
cytes, their ability to present antigens is either absent
or rarely observed. These cells do not have the ability
to migrate from the lesional tissue, and along with
inflammatory cells recruit other cells to thelesion. These
unique histiocytes lack dendritic cell processes and
have a round to ovoid, epithelioid morphology. Typical
cytokines produced by Langerhans cell histiocytes
include IL-1-beta, IL-3, IL-4, IL-8, TNF-alpha, and
GM-CSF. These cytokines provide an autocrine, as well
as a paracrine, function in lesion establishment and
persistence. These cells have proven to be clonal.Langerhans cell histiocytes are immature dendritic cells
that lack the ability to be functional antigen-presenting
cells.
The common origin of Langerhanscells andLangerhans
cell histiocytes1,2,4-15 is based on the discovery of Birbeck
granules with transmission electron microscopy. Only
these 2 cell types possess such pentalaminar structures.
Extensive immunocytochemical and flow cytometric
analyses have also provided additional support for the
shared origin of these 2 cell types. Both express S100
protein, HLA-DR, CD1a, and CD207 (langerin), while
being negative for macrophage markers (CD68, lyso-
zyme, CD14, CD163).
LANGERHANS CELL HISTIOCYTOSIS:GENERAL OVERVIEWClassification schemes
Several clinical classifications of LCH are used
by many practitioners (Table II and Table III).4-24
Eosinophilic granuloma represents the most common
form of this disease and is typically a localized, unifocal
osteolytic lesion. Older children and adults are com-
monly affected, but most patients are younger than 20
years of age. Multifocal lesions are less common and
skin lesions are quite rare. Letterer-Siwe disease affectsinfants, with mucocutaneous lesions being common.
Seborrheic dermatitiselike lesions, ulcers, and purpuric
nodules of the skin and subcutis occur at multiple sites.
The lung, liver, and spleen may be involved also. Hand-
Schuller-Christian disease is characterized by a classic
triad with osteolytic lesions, exophthalmos, and diabe-
tes insipidus. Those affected tend be young children.
A unique form of LCH is congenital and typically
undergoes involution over time. Congenital self-healing
LCH presents in the neonate or young infant as viola-
ceous red-brown firm nodules (Table II).18,21,25 Such a
pattern of clinical presentations may raise concernregarding the possibility of congenital leukemia and
neuroblastoma or an infectious process. The presenta-
tion at birth or shortly after is beneficial in identifying
this rare entity and avoiding unnecessary medical man-
agement. Certain ultrastructural features are specific to
the congenital self-healing form of LCH. Young adult
smokers have a unique form of LCH with pulmonary
involvement only (Table II andTable III).4,17,22-24 No
other lesional sites are found in these individuals. The
major sequelae of pulmonary LCH are progressive
Table I. Contemporary classification of histiocyticdisorders*
Disorders of varied biological behavior
Dendritic cellrelated disorders
Langerhans cell histiocytosis
Secondary dendritic processes (association with Hodgkin
lymphoma, acute lymphoblastic leukemia, acute
myelogenous leukemia)Juvenile xanthogranuloma and related disorders
Solitary histiocytomas of various dendritic cell phenotypes
Macrophage-related disorders
Hemophagocytic syndromes
Primary hemophagocytic lymphohistiocytosis
(familial, sporadic, and viral infection associated)
Secondary hemophagocytic lymphohistiocytosis
Infection associated
Malignancy associated
Other
Rosai-Dorfman disease
(sinus histiocytosis with massive lymphadenopathy)
Solitary histiocytoma with macrophage phenotype
Malignant disordersMonocyte-related disorders
Leukemias
Acute monocytic leukemia (FAB M5A and M5B)
Acute myelomonocytic leukemia (FAB M4)
Chronic myelomonocytic leukemia
Extramedullary monocytic tumor of sarcoma
(monocyte-derived granulocytic sarcoma)
Dendritic cellrelated histiocytic sarcoma
Follicular dendritic cell sarcoma
Interdigitating dendritic cell sarcoma
Dendritic cell sarcomas (based on phenotype)
Macrophage-related histiocytic sarcoma
*Modified from reference4: Working Group of The Histiocyte Society
and World Health Organization Committee on Histiocytic/ReticulumCell Proliferations.
OOOOE
S44 Hicks and Flaitz August 2005
http://-/?-http://-/?-7/21/2019 LCH Sunil Sir
4/25
interstitial fibrosis and respiratory compromise. There is
an association with malignant tumor development. This
disease is extremely rare in children.
The most current method for the categorization of
LCH is based on risk stratification of affected individ-
uals into recommended treatment protocols formulatedby the Histiocyte Society.4,17 The Histiocyte Society has
placed LCH into several disease groups (Table II).
Unifocal disease involves a single disease system with a
single site of involvement. There is a good prognosis in
this group, typically composed of older children and
adults. Multifocal single system disease is present when
several lesions are identified in a single organ system.
Bone is most commonly involved, and this representsmultifocal eosinophilic granuloma. The prognosis is
intermediate in this group that typically involves young
children. The worst prognosis is found in the multifocal
multisystem disease group. Multiple lesions are found inmore than one organ group. Commonly affected organ
systems include bone, skin, liver, spleen, and lymph
nodes. Children younger than 2 years of age represent
the majority of patients in this group. The Histiocyte
Society also recognizes congenital self-healing and
pulmonary-only LCH groups. The final disease group is
secondary LCH that is associated with a variety of
tumors. The malignancies most frequently associated
with LCH are leukemias and lymphomas, and less
commonly sarcomas and carcinomas.4,17,26
Table II. Langerhans cell histiocytosis: clinical typesand categorization schemes*
Clinical types of Langerhans cell histiocytosis
Eosinophilic granuloma
Most common form of Langerhans cell histiocytosis
Localized form, most benign
Older children and adults
[75% of affected individuals younger than 20 years of ageUnifocal lesions 3 times more common
(skull[ femur[pelvis[vertebra[jaws)
Multifocal lesions less common (50% skull, 16% jaws)
Rare skin lesions
Letterer-Siwe disease
Usually 1st year of life
Mucocutaneous lesions including gingiva and oral mucosa
Seborrheic dermatitis-like skin lesions
Purpuric red-brown nodules
Ulcerated painful nodules involving perineal, inguinal,
retroauricular, and external auditory canal regions
Lung, liver, and spleen involvement
Hand-Schuller-Christian disease
Usually 2- to 6-year-old children
Classic triad: osteolytic lesions, exophthalmos, and
diabetes insipidus
Skin and oral lesions
Congenital self-healing Langerhans cell histiocytosis
(reticulohistiocytosis, Hashimoto-Pritzker disease)
Pulmonary Langerhans cell histiocytosis
Categorization by Histiocyte Society for treatment
protocols (current)
Unifocal disease
Single system disease with single site of involvement
Most commonly bone
Older children and adults
Good prognosis
Multifocal single system disease
Multiple sites of involvement in single organ system
Most commonly bone
Young children
Intermediate prognosis
Multifocal multisystem disease
Multiple involved sites in more than one organ system
Most commonly bone, skin, liver, spleen, and lymph nodes
Children younger than 2 years of age and infants
Poor prognosis
Congenital self-healing Langerhans cell histiocytosis
Multiple skin lesions at birth or shortly after mimicking
congenital neuroblastoma or leukemia (blueberry
muffin baby)
Neonates and infants
Self-healing involutionPulmonary Langerhans cell histiocytosis
Young adult smokers (smokers malady)
Indolent progression to pulmonary fibrosis
Strong association with malignancies
Extremely rare in children
Secondary Langerhans cell histiocytosis associated
with neoplasms
Acute lymphoblastic and myelogenous leukemias
Chronic myelogenous leukemia
Myelodysplastic disorder association
Non-Hodgkin and Hodgkin lymphoma
Retinoblastoma
Table II. Continued
Osteosarcoma
Thyroid carcinoma
Lung cancer (adenocarcinoma, small cell carcinoma)
Prostate cancer
Breast cancer
Parathyroid adenoma
Pancreatic cystadenoma
Categorization by extent of disease
Restricted Langerhans cell histiocytosis
1. Skin rash with no other sites of involvement
(biopsy proven)
2. Monostotic bone lesions with or without diabetes
insipidus, regional lymph node involvement, or skin rash
3. Polyostotic bone lesions, consisting of several different
bones or \2 bone lesions in a single bone, with or without
diabetes insipidus, regional lymph node involvement, or skin
rash
Extensive Langerhans Cell Histiocytosis
1. Visceral organ involvement with or without bone
involvement, diabetes insipidus, regional lymph node
involvement or skin rash, and without signs of organdysfunction
2. Visceral organ involvement with or without bone
involvement, diabetes insipidus, regional lymph node
involvement or skin rash, and with signs of organ
involvement of lung, liver or hematopoietic system
*Compiled from references4 to 24.
OOOOE
Volume 100, Number 2 Hicks and Flaitz S45
http://-/?-http://-/?-7/21/2019 LCH Sunil Sir
5/25
LCH has also been categorized according to extent of
disease (Table II).2,20 Restricted and extensive cate-
gories have been defined. The restricted LCH category is
composed of skin rash only, monostotic bone lesion, and
polyostotic bone lesion subcategories, as detailed in
Table II. The extensive LCH category is based on vis-ceral organ involvement with or without organ dysfunc-
tion. As expected, outcome is worse in those with
extensive disease versus those with restricted diseases.
Treatment decisions may be based on this categorization
system with some protocols.
EpidemiologyLCH is a rare disease that affects 5 children per
million population and about 1 to 2 adults per million
population.1,2,4-6,9,15-17,22-25 It is predominantly a child-
hood disease with more than 50% of affected individuals
being younger than 15 years. The peak incidence is
between 1 and 4 years of age. This disease (Table III)
affects a young agepopulation (mean age27 years), with
a young adult smoker population affected by pulmonary-
only disease (mean age 41 years) and primarily neonates
Table III. Langerhans cell histiocytosis: clinical fea-tures*
Distribution by category, %
Unifocal disease 36
Multifocal single system disease 33
Multifocal multisystem disease 31
Age (mean)
Langerhans cell histiocytosis (all) 27 yUnifocal single system disease 18 y
Multifocal single system disease 26 y
Multifocal multisystem disease 25 y
PulmonaryLangerhanscellhistiocytosis 41 y
Congenital self-healing Langerhans
cell histiocytosis
5.2 d
Langerhans cell histiocytosis (all)
Age range Neonate to 83 y
\20 years of age 42%
Gender, M:F
Langerhans cell histiocytosis (all) 1.0:1.1
Pulmonary Langerhanscell histiocytosis 1.0:2.2
Congenital self-healing Langerhans
cell histiocytosis
1.0:1.0
Presenting clinical features, %
Local bone pain 41
Dyspnea 14
Malaise 9
Abnormal chest x-ray 9
Painful scalp mass 7
Pneumothorax 6
Diabetes insipidus 5
Scalp rash 3
Skin rash on trunk 3
Head and neck lymphadenopathy 2
Otitis media 2
Mucous membrane ulcer 2
Orbital proptosis 2
Chronic cough 1Scrotal mass \1
Pathologic fracture \1
Loose teeth \1
Cor pulmonale \1
Bony involvement sites, %
Head and neck
Skull 27-43
Mandible 7-9
Maxilla 1
Cervical vertebra 2
Extremities
Lower extremity, proximal 14-15
Upper extremity, proximal 6-7
Lower extremity, distal 2-3
Upper extremity, distal 1-2Ribs 10-14
Pelvis 9-12
Thoracic, lumbar, and sacral
vertebrae
5-10
Scapula 5
Clavicle 3
Treatment and outcome
Unifocal bone disease Local Excision with or
without radiation
11% Relapse
97% Disease-freesurvival
Table III. Continued
Multifocal bone disease only Local excision with or
without radiation
and/or chemotherapy
76% Relapse
91% Disease-freesurvival
6% Alive with disease
3% Died of diseaseMultifocal multisystem disease Combination surgery, che-
motherapy, and radiation
95% Relapse
74% Disease-freesurvival
11% Alive with disease
15% Died of disease
Pulmonary disease only Prednisone and/or
chemotherapy and/or
surgery
85% Disease-freesurvival
4% Alive with
progressive disease
11% Died of disease
Morbidity: lifelong sequelae
Diabetes iInsipidus
Growth hormone deficiency
Orthopedic problems
Pulmonary fibrosis
Biliary cirrhosis
Cerebellar ataxia
Cognitive dysfunction
Mortality with or without risk
organ involvement (lung, liver,
bone marrow, spleen), %
Without risk organ involvement 10
With risk organ involvement 30-50
*Compiled from references7, 16, and 17.
OOOOE
S46 Hicks and Flaitz August 2005
http://-/?-http://-/?-7/21/2019 LCH Sunil Sir
6/25
with congenital self-healing disease (mean age 5.2
days). Unifocal single system, multifocal single system,
and multifocal multisystem disease tend to be nearly
equally represented (Table III). The gender ratio is equal
in all LCH categories, with the exception of pulmonary-
only disease, where women are affected more than twice
as often.The most commonpresenting symptom is local bone
pain (41%,Table III).7,16,17 Various symptoms based on
organ system involvement have been noted (Table III).
Of interest for the head and neck region are painful scalp
mass (6%), scalp rash (3%), cervical lymphadenopathy
(2%), otitis media (2%), mucous membrane ulcer (2%),
orbital proptosis (2%), and, rarely, loose teeth (\1%).
Despite the low proportion of symptoms in the head and
neck region, bony involvement by LCH is quite com-
mon (Table III). The skull and mandible are frequently
affected, as well.
Treatment of LCH has been quite variable during
the past 50 years, and there has been a lack of coordi-
nated treatment protocols, particularly for adults (Table
III).2,7,16 With unifocal bone disease, local excision withor without radiation therapy has led to more than 95%
disease-free survival. However, relapse occurs in about
10% of cases. Multifocal bone disease may have similar
surgical treatment with or without the addition of
chemotherapy. Relapses are quite frequent with multi-
focal bone disease (76%). However, disease-free sur-
vival can be achieved in most of the affected patients
(91%). A small proportion of individuals die of their
disease (3%). Treatment of multifocal multisystem
disease employs the combination of surgery, chemo-therapy, and radiation therapy. The vast majority of
individuals have relapses (95%). One sixth will die of
disease. Disease-free survival is achieved by about 75%
of affected individuals. With pulmonary disease only,
treatment is quite variable ranging from prednisone
therapy to chemotherapy to surgery for lesions com-
promising the respiratory tract. A certain percentage of
individuals die of disease (11%). Disease-free survival
is noted in 85%. This form of LCH may have ongoing
progressive interstitial fibrosis in many affected pa-
tients, even when tobacco use is discontinued.
LCH produces lifelong effects, the nature of whicharedependent on the organ system(s) involved (Table
III).7,16,17 In particular when there is hypothalamic/pituitary gland involvement, the affected individual
may experience diabetes insipidus and growth hormone
deficiency. Central nervous system lesions may lead to
cerebellar ataxias with gait and mobility abnormalities
and cognitive dysfunction. With extensive or multifocal
bony lesions, skeletal growth and orthopedic abnor-
malities may be seen. The liver is particularly suscep-
tible to biliary cirrhosis due to bile duct damage and
sclerosis caused by the infiltration of Langerhans cell
histiocytes.
Certain organ systeminvolvement increases the risk
for mortality (Table III).7,16,17 High-risk organs include
the lung, liver, bone marrow, and spleen. Death occurs in
30% to 50% of those with high-risk organ involvement,
comparedwith only 10% without lesions in these organs.Certain factors are predictive of progressive
disease in LCH (Table IV).7,16,17 Several factors have
an extremely high relative risk for progressive disease,
such as osseous and mucocutaneous disease, osseous
and extraosseous disease, and treatment relapse with
multifocal multisystem disease. The presence of these
factors necessitates aggressive therapy. In the pediatric
age group, risk stratification for more intensive treat-
ment is based on sites of involvement.17 Low-risk sites
are defined as skin, bone, lymph nodes, and pituitary
glands. High-risk sites include lung, liver, bone marrow,
and spleen. Special sites that demand more aggressivetherapy are the mastoid bone, orbit, temporal bone, and
central nervous system.
Children and adults show different patterns of
involvement by LCH (Table V).16,17,22-24 Bone disease
is extremely frequent in children and less frequent in
adults. The jaws are involved in 30% of adults, but in
less than 10% of children. Skull lesions are about twice
as common in children. Skin disease is seen with equal
frequency. Pulmonary disease either in multifocal or
isolated LCH is very frequent in adults and infrequent
Table IV. Predictive factors in progression of Lang-erhans cell histiocytosis and low-risk and high-riskcategories for pediatric Langerhans cell histiocytosis*
Predictive factors in progression Relative risk
Osseous and mucocutaneous disease 40.7
Osseous and extraosseous disease 37.3
Treatment relapse with multifocal
multisystem disease
37.2
Osseous disease involving 3 or more bones 6.1
Mucous membrane disease 5.1
Hepatosplenomegaly in patient younger
than 3 years old
4.5
Pituitary-hypothalamic axis involvement
and multisystem disease
2.2
Younger than 5 years of age at presentation 2.1
3 or more organ systems involved by disease 1.8
Pediatric categorization for therapy
Low-risk sites: skin, bone, lymph nodes,
and pituitary
High-risk sites: lung, liver, bone marrow,
and spleen
Special site lesions: skull (mastoid, orbit,
temporal bone; associated with diabetes
insipidus and parenchymal brain lesions
with neurodegenerative process)
*Compiled from references16, 17.
OOOOE
Volume 100, Number 2 Hicks and Flaitz S47
http://-/?-http://-/?-7/21/2019 LCH Sunil Sir
7/25
to rare in children. Genital lesions are frequent in adults
and rare in children. Diabetes insipidus is found fre-
quently in both children and adults.
ORAL AND MAXILLOFACIAL LANGERHANSCELL HISTIOCYTOSIS
LCH involves the head and neck region quite
commonly, and, in particular, the bones of the skull
and jaws (Table IV, Table V, Figs 1-4).27-35 With oral and
maxillofacial LCH (Table V, Fig 1-4), more than 90% of
affected individuals are younger than 40 years of age,
with a mean age of about 19 years. Unifocal single
system disease represents about 50% of maxillofacial
LCH, with multifocal single system disease and mul-
tifocal multisystem disease equally distributed in the
remaining 50% of cases. The jaws are involved twice
as frequently as the oral soft tissues. The mandible is
3 times more frequently affected than the maxilla. Theposterior regions of the jaws are more frequently in-
volved than the anterior regions. Oral soft tissue lesions
are most commonly found with the gingiva and hard
palate. The floor of the mouth, maxillary sinus, and
buccal mucosaeach account forless than 10% of lesions.
The most common oral cavity signs and symptoms at
presentation are intraoral mass, pain, gingivitis, loose
teeth, oral mucosal ulcer, impaired healing, and halito-
sis. Extraoral signs and symptoms are quite common,
and include soft tissue and bone lesions outside the oral
cavity. Diabetes insipidus, lymphadenopathy, anemia,
skin lesions, exophthalmos, and hepatomegaly are lesscommon. The skull and lower extremities are the most
common extraoral sites of bony involvement.
Jaw lesions tend to have a unilocular radiolucent
appearance (Table VI, Fig 3), with well-demarcated
borders in two thirds of the cases and poorly defined
borders in the remainder.27-35 Tooth displacement is
associated with about half of the bony lesions. Root
resorption is seen less frequently.
Surgical management alone is used in 50% of cases
with an additional 23% of the lesions being treated with
both surgery and radiation therapy.27-35 Radiation alone
is used in one fifth of affected individuals. Chemo-
therapy and intralesional steroid injection are infre-
quently employed.
Recurrence of LCH is variable, but similaramong the
various disease categories (Table VI). 27-35 A single
recurrence is noted in 15% and a second recurrence inless than 5% of patients. Treatment modalities vary in
the proportion of cases with recurrences. Chemotherapy
has had no reported recurrences, however this form of
therapy has not been used frequently enough to assess its
effect accurately. Surgery alone has a 12% recurrence
rate, compared with 25% for radiation therapy alone and
19% for combined surgery and radiation therapy.
Survival in oral and maxillofacial LCH is quite
favorable with only 7% of patients dead from disease
(Table VI).27-35 Following treatment, there was no
evidence of disease in slightly over half of the patients;
while 17% were alive with disease.
PATHOLOGIC FEATURES OF LANGERHANSCELL HISTIOCYTOSISLight microscopic features
The histopathologic features of LCH are well char-
acterized and recognized readily by oral and maxillo-
facial pathologists (Fig 5).1,2,4-7,9-12,21,36-38 The typical
lesion is composed of an admixture of Langerhans cell
histiocytes, intermediate cells and interdigitating cells
of a dendritic cell lineage, T-cell lymphocytes, eosin-
ophils, and macrophages. The hallmark cell is the
Langerhans cell histiocyte. This cell has abundant
eosinophilic to amphophilic cytoplasm and a nucleusthat appears reniform, deeply indented, or grooved. The
number of eosinophils is quite variable from being
abundant with eosinophilic abscesses to sparse or even
absent. Occasional giant cells representing fusion of
either macrophages or Langerhans cell histiocytes may
be seen. The presence of this granulomatous inflamma-
tion with occasional giant cells raises the concern for an
infectious process, such as tuberculosis in the past, and
viral infection with an agent that is capable of inducing
syncytial (giant) cells. Necrosis within this granulom-
atous lesion is not unusual, and again reinforced the
suggestion in the past that these lesions represented aninfectious process. The lesions vary from an indistinct
focus with blending into the adjacent normal tissue to
nodular in appearance, depending on tissue types in-
volved. Although present, mitotic activity tends to be
low to moderate without atypical mitotic figures. The
lesions may take on a more atypical appearance and
appear as epithelioid granulomas (Fig 5, D) that lack
the typical features of LCH. The lesions may resemble
other histiocytic lesions, such as early juvenile xantho-
granuloma that lack characteristic Touton giant cells.
Table V. Comparison of childhood and adult Langer-hans cell histiocytosis
Children Adults
Bone disease Extremely frequent Frequent
Jaws 8% 30%
Skull 40% 21%
Skin disease Frequent Frequent
Dental disease Infrequent Frequent
Pulmonary disease Infrequent Very frequent
Pulmonary disease alone Rare Very frequent
Genital involvement Rare Frequent
Diabetes insipidus Frequent Frequent
Compiled from references 22-24.
OOOOE
S48 Hicks and Flaitz August 2005
7/21/2019 LCH Sunil Sir
8/25
Definitive diagnosis with these atypical lesions requires
immunocytochemistry and occasionally electron mi-
croscopy.
Immunocytochemical featuresLCH can be distinguished from other dendritic cell
disorders on the basis of cytoplasmic and cell surface
markers that it expresses (Table VII, Fig 6).5,11,12,21,36-38
In the past, S100 protein, Lag antigen, and peanut
agglutinin were used. With the development of more
specific and sensitive antibodies to cell surface mark-
ers associated with Langerhans cell histiocytes, these
markers are rarely used for diagnostic purposes. CD1a
(OKT6) is a well-recognized marker that immunoreacts
with Langerhans cells in the epidermis. This antibody
also identifies Langerhans cell histiocytes, cortical
thymocytes, and interdigitating dendritic cells within
the dermis andlymph nodes. Langerhans cell histiocytes
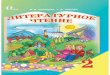
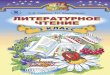
Fig 1. Clinical appearance of oral and maxillofacial Langerhans cell histiocytosis (LCH).A, Seborrheic-like dermatitis appearance
of LCH in postauricular region.B, Diffuse gingival enlargement secondary to LCH. C, Infiltration of maxillary frenum by LCH.
D, Maxillary alveolar and palatal LCH mass. E, Palatal diffusely ulcerated LCH. (Fig 1, A and B courtesy of Dr Moise Levy,
Houston Tex; Fig 1C courtesy of Dr Megan Dishop, Houston Tex; Fig 1, E reprinted with permission from Eisen D, Lynch D,
editors. The mouth: diagnosis and treatment. St. Louis, Mo: Elsevier Publishers; 1998.)
OOOOE
Volume 100, Number 2 Hicks and Flaitz S49
7/21/2019 LCH Sunil Sir
9/25
demonstrate a membranous to cytoplasmic pattern
with the CD1a antibody (Fig 6, A). According to the
Histiocyte Society, a definitive diagnosis of LCH maybe rendered with the appropriate histopathology and
when immunoreaction with CD1a is present. This
antibody may be used with formalin-fixed paraffin-
embedded tissues, and eliminates the need for frozen
tissue for immunocytochemistry.
More recently, a highly specific and sensitive anti-
body against Langerhans cells and Langerhans cell
histiocytes has become commercially available (Fig 6,
B).21,39-43 CD207 (langerin) is a monoclonal antibody
against a type II transmembrane protein expressed with
Langerhans cells and Langerhans cell histiocytes.
CD207 reacts with a 40-kD langerin protein purportedly
specific to these cells. Langerin is located on the cellsurface of Langerhans cells and Langerhans cell histi-
ocytes and induces membrane superimposition and
zippering that leads to Birbeck granule formation
(LC granules, Birbeck-Broadbent granules). These
pentalaminar structures with a bulbous end (tennis
racket and handle) represent a means to capture antigen
for antigen processing. These structures are rapidly
internalized into the cells. The CD207 (langerin) anti-
body requires antigen unmasking with formalin-fixed,
paraffin-embedded tissues.
Fig 2. Diagnostic imaging of skull and rib in LCH. A, Well-circumscribed parietal bone LCH lesion. B, Destruction of
right zygomatic process of maxilla secondary to LCH with significant soft tissue component. C, Bilateral mastoid involvement by
LCH with soft tissue mass anteriorly displacing ears bilaterally. D, Left rib with loss of cortical bone and soft tissue mass bulging
into parietal pleura.
OOOOE
S50 Hicks and Flaitz August 2005
7/21/2019 LCH Sunil Sir
10/25
Fig 3. Clinical and radiographic appearance of oral and maxillofacial LCH.A and B, Young child with gingival soft tissue LCH
mass (A) with mild lingual displacement of the primary molars and a diffuse radiolucent lesion ( B) with loss of bone surrounding
the primary first molar and mesial root of primary second molar. C-E,A 34-year-old woman with erythematous lingual mucosa
adjacent to a second molar (C) with root canal therapy 6 years previously. Periapical radiograph (D) with diffuse bone loss
secondary to biopsy-proven LCH. E, Same patient with progressive mandibular and maxillary LCH involvement with tooth loss
over a 3-year period. F and G, Elderly man with diffusely erythematous mandibular gingiva and mucosa with tissue loss due to
LCH (F). Periapical radiograph (G) reveals diffuse bone loss secondary to LCH. (Fig 3, A and B reprinted with permission from
Neville B, Damm D, Allen C, Bouquot J, editors. Oral and maxillofacial pathology. 2nd ed. St. Louis, Mo: WB Saunders Co; 2002.
Fig 3, C, D, and Ecourtesy of Dr Brad Neville and Dr John Hann, Charleston SC. Fig 3, Fand G courtesy of Dr Alan Gould,
Crestwood, Ky.)
OOOOE
Volume 100, Number 2 Hicks and Flaitz S51
7/21/2019 LCH Sunil Sir
11/25
Fig 3. Continued.
OOOOE
S52 Hicks and Flaitz August 2005
7/21/2019 LCH Sunil Sir
12/25
Fig 4. Congenital self-healing LCH.A, Periorbital nodular lesions in a neonate. B, Characteristic histopathologic appearance of
LCH with admixture of Langerhans cell histiocytes with deeply indented, grooved, and reniform nuclei and abundant eosinophilic
to amphophilic cytoplasm, eosinophils and lymphocytes (hematoxylin and eosin, original magnification 3400). C, Concentric
laminated bodies in Langerhans cell histiocytes pathognomonic for congenital self-healing LCH (transmission electron
microscopy, original magnification 310 000). (Fig 4, A courtesy of Dr Denise Walker Metry, Houston Tex.)
OOOOE
Volume 100, Number 2 Hicks and Flaitz S53
7/21/2019 LCH Sunil Sir
13/25
Differentiation of LCH from other dendritic cell dis-
orders is important. The immunophenotypes of dendritic
cell disorders are presented in Table VII.5,11,12,21,36-43
Dendritic cell disorders may contain a certain percent-
age of normal Langerhans cells that are trafficking
back to regional lymph nodes to perform their antigen-
presenting cell functions. In such cases, where there may
be a certain population of Langerhans cells or macro-
phages that have morphology similar to Langerhans cell
histiocytes, further characterization with immunocyto-
chemistry would be necessary. Xanthogranulomatous
processes are defined by immunoreaction with dendritic
cell markers (Factor XIIIa, fascin) and macrophage
markers (CD68 [PGM1], CD163). It is important to
recognize that juvenilexanthogranuloma may be seen
in children with LCH.44-46 Juvenile xanthogranuloma
may appear before, concurrent with, or following the
diagnosis of LCH. Children with juvenile xanthogran-
ulomas should be evaluated for and have appropriate
follow-up to assess concurrent or development of LCH.
Rosai-Dorfman disease is characterized by reactivity
with S100 protein and macrophage markers, as well as
Table VI. Oral and maxillofacial Langerhans cellhistiocytosis: clinical features*
Mean age, y (range) 18.9 (Neonate-53)
Age, y
\10 29%
10-19 22%
20-39 44%
40-53 5%Gender ratio, M:F 3.9:1.0
Unifocal disease, % 49
Multifocal single system disease, % 25
Multifocal multisystem disease, % 25
Sites involved, %
Jaws 67
Mandible 76
Posterior 68
Anterior 32
Maxilla 24
Posterior 63
Anterior 37
Oral soft tissues 33
Gingiva 76
Hard palate 10
Floor of mouth 6
Maxillary sinus 5
Buccal mucosa 4
Symptoms at presentation, %
Mass/Lesion 59
Pain 46
Gingivitis 43
Loose teeth 41
Oral ulcer 19
Impaired healing 13
Halitosis 12
Masticatory problems 9
Vincents infection 7
Gingival bleeding 6Paresthesia 4
Extraoral symptoms at presentation, % 70
Extraoral lesions 50
Soft tissue lesion only 7
Bone and soft tissue 43
Diabetes insipidus 16
Lymphadenopathy 16
Anemia 15
Skin lesions 12
Exophthalmos 10
Hepatosplenomegaly 9
Otitis media 8
Fever 7
Leukocytosis 2
Mental disability 2Extraoral sites of involvement, %
Skull 37
Lower extremity 28
Upper extremity 13
Ribs 13
Lung 12
Skin 10
Liver 10
Spine 7
Orbit 7
Cervical lymph nodes 6
Table VI. Continued
Submandibular gland 2
Parotid gland 2
Radiographic appearance, %
Unilocular radiolucent lesions 100
Well-demarcated borders 63
Borders poorly corticated 24
Poorly defined borders 12Displaced teeth 51
Root resorption 17
Periosteal reaction 8
Treatment, %
Surgery alone 50
Radiation therapy alone 20
Surgery and radiation therapy 23
Chemotherapy 7
Intralesional steroids 1
Recurrence, %
Unifocal disease, 16
Multifocal single system disease 22
Multifocal multisystem disease 15
Single recurrence 15
Two recurrences 4
Surgery alone 12
Radiation therapy 25
Surgery and radiation therapy 19
Chemotherapy 0
Outcome, %
No evidence of disease 53
Alive with disease 17
Alive, status not known 7
Died of disease 7
Died of other causes 11
Died of unknown cause 3
*Compiled from references27-35.
OOOOE
S54 Hicks and Flaitz August 2005
http://-/?-http://-/?-7/21/2019 LCH Sunil Sir
14/25
emperipolesis (leukocytes passing through the cyto-
plasm of macrophages).5-11,12,21,36-43 Indeterminantdendritic cell histiocytomas immunoreact with CD1a,
S100 protein, and fascin.5-11,12,21,36-43 Interdigitating
dendritic cell histiocytoma have a similarimmunophe-
notype, but also display CD83 expression.5-11,12,21,36-43
Follicular dendritic cell histiocytoma becomes an issue
if a lymph node or the spleen contains a histiocytic
lesion.5-11,12,21,36-43
The expression of CD21 and CD35would help to differentiate this tumor from other
histiocytic lesions.
Ultrastructural featuresThe gold standard for definitive diagnosis of LCH
is examination of tissue using transmission electron
microscopy (Table VIII, Fig 7).1,2,4-6,9,11,12,21,38 The
identification of Birbeck granules in the cytoplasm or
within the cell border of lesional cells provides the final
evidence necessary in difficult to characterize tumors, or
when there are aberrant immunocytochemical results.
All forms of LCH possess Birbeck granules. The typicalgranule is composed of a rod-shaped or tennis rackete
shaped structure with a length varying from 200 to
400 nm and a width of 33 nm. The rod (handle) region
has a zipper-like morphology and has been described as
pentalaminar owing to a central striated membrane anda
double electron dense outer sheath. The granules are
more easily identified in early lesions, rather than inlong-standing lesions. Birbeck granules tend to be rare
when LCH involves the liver, spleen, and gastrointesti-
nal tract. Other ultrastructural structures present within
the cytoplasm of Langerhans cell histiocytes are curvi-
linear and multivesicular bodies, tubuloreticular inclu-
sions, and cylindrical confronting cisterna.
Congenital self-healing LCHCongenital self-healing LCH deserves special atten-
tion because this disease spontaneously resolves over
Fig 5. Histopathologic features of LCH. A, Abundant eosinophils with frequent histiocytes and less apparent lymphocytes
(hematoxylin and esocin, original magnification 3100). B and C, Langerhans cell histiocytes with abundant eosinophilic to
amphophilic cytoplasm and deeply indented, reniform, and grooved nuclei (hematoxylin and eosin, original magnification 3400).
D,Atypical LCH lesion composed of epithelioid Langerhans cell histiocytes with abundant eosinophilic cytoplasm and lacking
typical reniform nuclei (hematoxylin and eosin, original magnification 3200). These histiocytic cells immunoreacted with CD1aand CD207, as well as demonstrated Birbeck granules (not shown).
OOOOE
Volume 100, Number 2 Hicks and Flaitz S55
7/21/2019 LCH Sunil Sir
15/25
several months and may be confused with multifocal
single system or multifocalmultisystem disease that
requires treatment.4,17,21,25 Congenital self-healing
LCH has an identical histopathology and immunophe-
notype like all other forms of LCH, but has unique
ultrastructural features (Fig 4, Table VIII). Transmissionelectron microscopy will reveal laminated dense bodies
with a concentric myelin-like morphology and non-
laminated dense bodies. Birbeck granules are found, but
tend to be detected in less than one third of the
Langerhans cell histiocytes. The presence of laminated
dense bodies provides definitive proof for the diagnosis
of congenital-self healing LCH. This form of LCH
occurs predominantly in children younger than 1 year of
age. It is recommended that any child younger than 2
years with evidence of LCH should have transmission
electron microscopy performed on the biopsy or resec-
tion tissue to confirm or refute the diagnosis of typical
LCH or congenital self-healing LCH.
Tissue availability for electron microscopicevaluation
Ideally, tissue should be set aside in 2% to 3% bu f-
fered glutaraldehyde for possible ultrastructural study.21
In most oral and maxillofacial pathology services,
electron microscopy is not a high priority. Ultrastruc-
tural examination can be performed on residual tissue
fixed in buffered 10% formalin without deleterious
results. Alternatively, a portion of lesional tissue may be
removed from a tissue block and undergo paraffin
recovery, and then transmission electron microscopic
examination. Ultrastructure may be compromised to a
certain extent, however the tumor-defining structures
(Birbeck granules, laminated dense bodies) are usually
of adequate quality to provide for a definitive diagnosis.Stringent control of processing temperature of the tissue
and low-melting point paraffin for embedding the tissue
allows for better preservation of ultrastructural features.
RECOMMENDED EVALUATION FOLLOWINGDIAGNOSIS OF LANGERHANS CELLHISTIOCYTOSIS
Once a biopsy-proven diagnosis is obtained, the
patient should undergo referral to a specialist who is
well versed in LCH (pediatric or adult hematologist/
oncologist). For appropriate classification, the following
are recommended4,6,9,17:
d Thorough clinical examinationd Complete blood cell count with hematocrit, hemo-
globin, and platelet countd Liver function tests (serum transaminases, alkaline
phosphatase, bilirubin, albumin, total protein)d Coagulation studies (prothrombin and partial throm-
boplastin time, fibrinogen)d Urine osmolarityd Arginine vasopressin study for diabetes insipidusd Chest radiographd Skeletal radiograph surveyd
CT or ultrasound of chest and/or abdomen if organsystem involvement suspectedd MRI of the brain if central nervous system involve-
ment suspectedd Respiratory function tests if respiratory involvement
suspectedd Diagnostic endoscopy if gastrointestinal symptoms
suspected
BIOLOGIC, CYTOGENETIC, ANDMOLECULAR ASPECTSLCH: The Chemokine/Cytokine Storm
As noted previously, Langerhans cell histiocytes areconsidered to be immature dendritic cells that fail to
undergodifferentiationto mature dendritic cells.4,15,47-49
Similar to immature dendritic cells, Langerhans cell
histiocytes express receptors for inflammatory chemo-
kines (CCR1, CCR2, CCR5, CCR6, CXCR1), which
allow for the recruitment of additional immature den-
dritic cells (Table IX).50-54 Langerhans cell histiocytes
fail to mature and do not down-regulate the above-
mentioned chemokines associated with immature den-
dritic cells. In addition, these histiocytes fail to display
Table VII. Immunocytochemical features of dendriticcell disorders*
Langerhans cell histiocytosis
Markers important for diagnosis:
CD1a, CD207 (Langerin), S100, Lag antigen
Additional markers:
HLA-DR, E-cadherin, peanut agglutinin, CD4, CD31, CD40,
CD49d, CD52, CD54, CD80, CD86, CD116 (GM-CSFR),CD209 (DC-SIGN), CCR6, PLAP, NSE, vimentin, IL2-R
(CD25), IFN-gamma, TNF-alpha, acid phosphatase, CD68
(weak), LCA (CD45 weak), lysozyme weak)
Xanthogranuloma family (juvenile xanthogranuloma,
Erdheim-Chester disease, xanthoma disseminatum,
dermal dendrocytomas)
Factor XIIIa, Fascin, CD68 (PGM1), CD163, CD14,
Ki-M1P, CD45
Rosai-Dorfman disease (sinus histiocytosis with massive
lymphadenopathy, sinus dendritic cell)
CD68, S100, fascin, CD163, cathepsin E, alpha-1-antitrypsin,
Si-M9, CD31
Dendritic cell histiocytoma, indeterminant cell type
CD1a, S100, fascin, CD45
Dendritic cell histiocytoma, interdigitating dendritic cell type
CD1a, S100, Fascin, CD83, CD45
Dendritic cell histiocytoma, follicular dendritic cell type
CD21, CD35, Ki-M4, Fascin, S100 variable (6)
*Compiled from references5, 11, 12, 21, 36-43.
OOOOE
S56 Hicks and Flaitz August 2005
http://-/?-http://-/?-7/21/2019 LCH Sunil Sir
16/25
chemokines (CXCR4, CCR7) that are constitutively
expressed by mature dendritic cells. High levels of
other inflammatory chemokines (CCL20/MIP-3alpha,
CCL2/MCP-1, CCL3/MIP-1alpha, CCL4/MCP-4alpha,
CCL5/RANTES, CXCL8/IL-8, CXCL10/IL-10) are re-
leased by Langerhans cell histiocytes, and these chemo-
kines are also associated with immature dendritic cells.
These chemokines are important in the recruitment of
circulating immature dendritic cells, as well other im-
mune cell types (T lymphocytes, macropaghes, eosino-
phils). Langerhans cell histiocytes have high levels of
CD14, CD86, and intracellular MHC class II, and lack
CD83, CD86, and DC-LAMP, which are characteristicfor immature dendritic cells.4-15,17 It is quite obvious why
Langerhans cell histiocytes are considered to be in an
arrested state of activation and differentiation. This would
also explain thelack of thin, fingerlikedendritic processes
seen in normal Langerhans cells (mature dendritic cells),
and the characteristic ovoid to round morphology of
Langerhans cell histiocytes (immature dendritic cells).
The lack of maturation also prevents Langerhans cell
histiocytes from leaving the lesion site.
Up-regulation of many cytokines have been demon-
strated with LCH (Table IX).17,52-60 Histopathologic
examination of lesions notes a mixture of Langerhanscell histiocytes, lymphocytes (predominantly helper
[CD4] T lymphocytes), eosinophils, and macrophages.
Each of these cell types produces cytokines in the
lesions, which result in autocrine and paracrine stimu-
lation of the lesional cells. The major players are con-
sidered to be the Langerhans cell histiocytes and T-cell
lymphocytes (predominantly helper CD4 lymphocytes).
Major factors that participate are the cytokines IL-1,
IL-3, IL-4, IL-5, IL-8, IL-10, GM-CSF, TNF-alpha,
transforming growth factor (TGF)-beta, and leukemia
inhibitory factor (LIF) (Table IX). Many of the cyto-
kines favor recruitment of Langerhans cell progenitors
and rescue from apoptosis. Langerhans cell histiocytes,
macrophages, and T cells produce IL-10, GM-CSF, and
interferon (INF)-alpha. IL-1 is derived from Langerhans
cell histiocytes. T-cell lymphocytes synthesize IL-2,
IL4, IL-5 and TNF-alpha. Eosinophils produce IL-5,
INF-alpha, GM-CSF, IL-7, and IL-10.
These cytokines are important because they create
a cytokine storm in which autocrine and paracrine
stimulation is established among the cells, and in
particular, the Langerhans cell histiocytes and helper
T lymphocytes (CD4).17,52-60 For example, Langerhanscell histiocytes are stimulated by IL-1 and IL-2 pro-
duced by T lymphocytes. Both of these cell types also
upregulate INF-alpha, which stimulates IL-1 produc-
tion. Recruitment of Langerhans cell progenitors
occurs, in part, under the influence of GM-CSF that
is produced by both Langerhans cell histiocytes and
CD4 T lymphocytes. Interestingly, serum GM-CSF and
IL-2 levels are dramatically increased in patients
with multifocal multisystem disease. GM-CSF, IL-3,
TNF-alpha and other cytokines act as chemoattractants
for CD341 Langerhans cell precursors, eosinophils,
neutrophils, and macrophages. TNF-alpha inhibitsspon-taneous apoptosis of Langerhans cell histiocytes, there-
by promoting their survival. This anti-apoptotic effect is
further enhanced by IL-1-alpha, GM-CSF, and IL-3.
Only recently has it been possible to evaluate
expression profiles for LCH using laser capture micro-
dissection, RNA amplification, and gene microarray
techniques.60 Certain differences in cytokine expression
have been found. With LCH involving the liver and
spleen, the cytokines IL-13, nuclear factor kappa
B (NFkB), TNF receptor, p55, receptor-activator of
Fig 6. Immunocytochemical identification of LCH. A, Langerhans cell histiocytes reacting in a cytoplasmic pattern with
CD1a (immunocytochemistry anti-CD1a antibody, original magnification 3400). B, Langerhans cell histiocytes reacting in a
cytoplasmic pattern with CD207/langerin (immunocytochemistry anti-CD207 antibody, original magnification 3400).
OOOOE
Volume 100, Number 2 Hicks and Flaitz S57
7/21/2019 LCH Sunil Sir
17/25
NF-kappa B ligand (RANKL), CD40-L and TGF-beta
receptor are significantly upregulated, compared with
normal Langerhans cells. Bone-only disease has a
different expression profile than multisystem disease.
The upregulated cytokines and genes in bone-only
disease, compared with multisystem disease, are CD40/
CD40L, GM-CSF, GM-CSF receptor, IL-1-3 receptor-1,
IL-2, IL-5 receptor, TNF-alpha, TGF-beta, TNF re-
ceptor associated factor 1 (TRAF1), and TRAF6. The
discovery of differences in cytokine and gene profile
expression for specific forms of LCH provides potential
avenues to explore in understanding pathogenesis andnew targets for therapy.
The symptoms associated with LCH, such as fever
and failure to thrive, have been associated with the
chemokine/cytokine storm effect.17,50-57,60 In addi-
tion, several of these factors promote osteoclastic
activity and osteolysis, promote fibrosis (liver andlung fibrosis, hypothalamic/pituitary axis sclerosis
leading to diabetes insipidus), hematologic dysfunction,
angiogenesis, and overgrowth of granulation tissue.
In addition to the chemokines and cytokines involved
in lesion formation with LCH, many different growth
factors, regulators of the cell cycle, adhesion molecules
andimmunologicmarkers have been implicated (Table
IX).17,52,53,56,58-69 It is obvious that the process of lesion
formation in LCH is quite complex, and involves
numerous mediators that cross-talk among the vari-ous cell types.
Lack of viral etiologyAt one point, the issue of whether LCH had a viral
etiology was raised. Convincing evidence from several
investigations using in situ hybridization and poly-
merase chain reaction techniques, as well as viralcul-
tures, has not surfaced to support a viral etiology.69-71
Adenovirus, cytomegalovirus, Epstein-Barr virus, her-
pes simplex virus, human herpesvirus type 6, HIV,
human T-cell leukemia virus types I and II, and
parvovirus have been shown not to be present in LCH.Some investigators have noted immunohistochemicalstaining for human herpesvirus 6 in lesions, but there
were no serologic data that showed a recent infection
had occurred. It was concluded that reactivation of a
latent viral infection could be the explanation, which is
common among herpesvirus family members.
Neoplastic process, cytogenetics, and moleculargenetics in LCH
During the past decade, there has been controversy
regarding whether LCH is a neoplastic or reactive
process (Table X).17,47,48,72-74 Clonal expansion of
Langerhans cell histiocytes has been shown repeatedly
in eosinophilic granuloma, Letterer-Siwe disease, and
Hand-Schuller-Christian disease. Clonality in these
disease processes has been proven by both human
androgen receptor (HUMARA) DNA assay and T-cell
receptor analysis.17,72-74 Of interest is the fact that the
pulmonary only form of LCH that occurs in young adult
smokers has not proven in multiple investigations to be
clonal. This would fit the clinical scenario, because it is
possible for these lesions to regress with smoking
cessation. Although not studied, lack of clonality in
congenital self-healing LCH would be expected.
Further evidence for a neoplastic process is familialclustering of LCH with multiple affected rela-
tives.17,74,75 Familial clustering of LCH accounts for
only about 1% of the cases. An association between
Table VIII. Langerhans cell histiocytosis: diagnosticcriteria
Presumptive diagnosis
Granulomatous inflammation and hallmark Langerhans cell
histiocytes identified on routinely stained tissue sections
(characteristic histopathology)
Definitive diagnosis
Characteristic histopathology and Birbeck granules on electronmicroscopy and/or CD1a immunoreactivity (CD207
Langerin substitute for CD1a)
Immunocytochemistry important for diagnosis
Positive for: CD1a, CD207 (langerin), S100 protein,
peanut agglutinin (PNA)
Negative for: Factor XIIIa, fascin
Ultrastructural features important for diagnosis
Langerhans cell histiocytosis
LC granules (Birbeck granules, pentalaminar structures)y
Multivesicular bodies
Curvilinear membranous formations (worm structures)
Tubuloreticular structures
Cylindrical confronting cisternae (comma-shaped structures)
Congenital self-healing Langerhans cell histiocytosis
(Reticulohistiocytosis; Hashimoto-Pritzker disease)
Laminated dense bodies (concentric, myelin-like bodies)y
Nonlaminated dense bodiesy
LC granules (Birbeck granules, pentalaminar structures,
\30% of Langerhans cell histiocytes)y
Compiled from references 1-6, 9-12, 17, 21, 25, 38.yTumor-defining structures.
Fig 7. Ultrastructure of LCH.A, Large histiocytic cells with abundant cytoplasm and deeply indented and irregular nuclei with
dispersed chromatin (transmission electron microscopy, original magnification 31500).B and C, Birbeck granules (LC granules)
characterized as tennis rackets with handles (arrow). More often, Birbeck granules are found as pentalaminar rod (handle only of
tennis racket) structures only, with some having rudimentary bulbous ends (transmission electron microscopy, original
magnification 328 000). (Fig 7, B and Ccourtesy of Dr Gary Mierau, Denver, Colo.)
OOOOE
S58 Hicks and Flaitz August 2005
7/21/2019 LCH Sunil Sir
18/25
OOOOE
Volume 100, Number 2 Hicks and Flaitz S59
7/21/2019 LCH Sunil Sir
19/25
mannose-binding lectin alleles and susceptibility to
LCH in family members has been suggested as one
possible mechanism. In addition, LCH has occurred in
identical twins, with similar clinical features, dissem-
inated disease, and same sites of involvement.74,75 There
is an 86% concordance rate for identical twins, but no
evidence for concordance with fraternal twins.
Certain HLA haplotypes in different ethnic groups
increase the susceptibility for development of LCH.76
The exact reason for this is not known currently, but is
under investigation. Constitutional or acquired chromo-
somal instability may be another factor in LCH
development.74,75 This is illustrated by a child with an
unknown DNA breakage syndrome who developed
LCH, in addition to ataxia, ocular telangiectasia, and
chromosomal instability.77 Finally, there is a known
increased incidence of other malignancies in children
with LCH (acute and chronic leukemias, lymphomas,
solid tumors;Table II).4,17,26,69,74,78
Comparative genomic hybridization (CGH), loss of
heterozygosity (LOH), and conventional cytogenetics
have demonstrated several genomic abnormalities intissue from LCH (Table X).73,79-81 In particular, certain
chromosomal sites that have losses or gains in DNA
sequences and/or loss of heterozygosity in LCH are loci
where tumor suppressor genes are housed. One such
site in LCH is the short arm (p) of chromosome 1,
particularly 1p36. There are several tumor suppressor
genes at the 1p36 locus (IDE, CDC2L1, PAN, PAX7,
E2F2,TNFR-2,TCEB). Deletions and loss of heterozy-
gosity of the 1p arm have also been associated with
neuroblastoma, B cell chronic lymphocytic leukemia,
and Wilms tumor. Loss of chromosome 7 has been
noted on CGH and LOH studies with LCH. The tumorsuppressor gene plasminogen activator inhibitor is
located on this chromosome. Chromosome 7 loss and
abnormalities are linked to Fanconis anemia, myelo-
dysplastic disorders, and acute myeloid leukemia. 49,78
With LCH, chromosome 9 is affected by loss of DNA
sequences and loss of heterozygosity at 9p21.73,79-81
At chromosome 9p21 are several regulators of the
cell cycle (cyclin-dependent kinases, cyclin-dependent
kinase inhibitors, CDKN2A, p14, p15, p16).
Chromosome 9q is where the tuberous sclerosis tumor
Table IX. Cell proliferation factors in Langerhans cellhistiocytosis
Chemokines
CCR1
CCR2
CCR5
CCR6
CCL2/MCP-1CCL3/MIP-1alpha
CCL4/MCP-4alpha
CCL5/RANTES
CCL17/TARC
CCL20/MIP-3 alpha
CXCL8/IL-8
CXCL10/IL-10
CXCL11/I-TAC
CXCR1
CXCR3
Cytokines
Interleukins (IL) 1, 2, 3, 4, 6, 8, 9, 10, 11, 12, 13, 17, 22
Interferon-gamma (IFN)
Tumor necrosis factor (TNF)-alpha
TNF-receptor (p75)
TNF receptor associated factor (TRAF1, TRAF6)
Granulocyte macrophage-colony stimulating factor (GM-CSF)
GM-CSF receptor (GM-CSFR)
Macrophage-colony stimulating factor (M-CSF)
Stem cell factor (CD341)
Leukemia inhibitory factor (LIF)
CD40 ligand and receptor
Transforming growth factor (TGF)-alpha and beta
TGF-beta receptor
RANKL (receptor-activator of NF-kappa B ligand)
NF-kappa B (nuclear factor kappa B)
FMS-like tyrosine kinase ligase (FLT3-L; colony stimulating
factor 1 receptor, formerly McDonough feline sarcoma viral
oncogene homolog)Angiotensin-converting enzyme (ACE)
Prostaglandin E2
Exotaxin 1, 2, 3
Leptin
Growth Factors
Fibroblastic growth factor 6, 14 (FGF)
Vascular endothelial growth factor (VEGF)
Platelet-derived growth factor-receptor beta (PDGF-R beta)
PDGF-alpha
Bone morphogenic protein 8 (BMP)
Thrombopoietin
Allograft inflammatory factor 1
Cell cyclerelated gene products
MDM2
p53
p55
p21
p16
Rb
Bcl2
Cell adhesion
CD2
CD44
CD54
CD58
CD11c
Table IX. Continued
Immunologic markers
CD1a (OKT6)
CD207 (langerin)
CD4
CD45
MHC II
Compiled from references4-15, 17, 47-69.
OOOOE
S60 Hicks and Flaitz August 2005
7/21/2019 LCH Sunil Sir
20/25
suppressor gene is found. Loss of heterozygosity with
the short arm (p) of chromosome 17 has been identified
in LCH.73,79-81 The tumor suppressor genep53 is located
at 17p13. Loss of heterozygosity has been demonstrated
on the long arm (q) of chromosome 22 in LCH. 73,79-81
The tumor suppressor gene NF2 is located on chromo-
some 22q. In addition, gains at chromosome 4q and 12phave been observed in osteosarcomas (4q), gliomas
(12p), and B-cell chronic lymphocytic leukemias
(12p).73,79-81 LCH has been shown to have DNA
sequence gains along the long arm (q) of chromosome
4 and with chromosome 12.
The finding of cytogenetic abnormalities in chromo-
some 7 (Table X) has further strengthened the link
that LCH is a myeloid stem cell disorder.49,73,78-81
Chromosomal abnormalities associated with chromo-
some 7 include Fanconis anemia, myelodysplastic
disorders, and acute myeloid leukemia. Recently, there
have been several children with concurrent LCH and
myelodysplasia. Interestingly, myelofibrosis may be
seen in LCH and has been ascribed to bone marrow
involvement. Perhaps greater attention will be directedtoward chromosome 7 in LCH on the basis of these
findings.
Cytogenetic studies (Table X) have shown that
tumor suppressor genes (p53), oncogenes (c-myc,
h-ras), adhesion molecules (E-cadherin), cell surface
immunologic markers, growth factors, and apoptotic
defects participate in LCH to some degree.69,72-75,80,81
These factors represent potential targets for therapy.
CURRENT TREATMENT PROTOCOLS ANDINNOVATIVE THERAPEUTIC AGENTS
Over the past decade, the Histiocyte Society initiated
a series of treatment protocols for LCH aimed at the
pediatric population, andmore recently has opened an
adult protocol (Table XI).15,17,82-86 The first pediatric
protocol (LCH-I) began in 1991 and was targeted
toward multisystem disease. The study analyzed the
effect of vinblastine and etoposide in combination with
intravenous steroids. The overall response was similar
with either treatment (58% vs 65% for vinblastine vs
etoposide). Survival was also not statistically different
between the groups (76% for vinblastine, 83% foretoposide). Of interest was the determination that chil-
dren who failed to respond to therapy within a 6-week
period were at increased risk for treatment failure and
required a different therapy. Mortality in these poor
responders was 66%. LCH-II compared treatment with
vinblastine, oral prednisone, and mercaptopurine with
or without etoposide. The addition of etoposide did not
provide any difference in survival, relapse, or toxicity.
Because of the risk for a second malignancy (myeloid
leukemia) with etoposide, this drug is no longer used
in LCH protocols. The prior finding of decreased sur-
vival in children who did not respond to therapy after
6 weeks was again noted (good responders 88% sur-
vival, poor responders 17% survival). The current
protocol (LCH-III) compares different therapies for
multisystem disease with high-risk sites, multisystem
disease with low-risk sites, multifocal single system
disease, and localized special site disease. This study
is currently accruing patients and results are not yetavailable.
The Histiocyte Society has recently launched a
protocol for adults with LCH (Table X).17,82-86 The
treatment groups are single system disease, central
nervous system disease, isolated pulmonary disease,
and multisystem disease. Accrual is ongoing and results
are not available at the present time.
The therapies available for those children and adults
not enrolled into the Histiocyte Society protocols are
determined by the patients oncologist on a case-by-case
Table X. Langerhans cell histiocytosis: cytogeneticsand molecular genetics*
Evidence for neoplastic process
Clonal expansion of Langerhans cell histiocytosis
Human androgen receptor (HUMARA) DNA assay
T-cell receptor analysis
Familial occurrence with multiple affected relatives and
identical twinsMannose-binding lectin allele
Immune system gene dysregulation
Increased incidence of other malignancies
HLA haplotypes (chromosome 6)
DR4, Cw7, B7, B8 (Caucasians, United States)
B7, DR2 (England)
B61, Cw7 (Japanese)
Comparative genomic hybridization (CGH)
Loss of DNA sequences on chromosomes
1p (1p36, 1p21-36), 2, 5, 6, 7, 9, 11p, 16, 17, 22q
Gain of DNA sequences on chromosomes
2q, 4q, 12
Loss of heterozygosity (LOH) with chromosomes
1p, 1p36, 1p22, 1p13, 1q31, 1q, 3p, 4q35, 5q, 7, 7p21, 7p15, 9, 9p,
9p21, 17p, 22, 22q, 22q11
Other cytogenetic abnormalities reported
t(7;12)(q11.2;p13)
Myelodysplastic disorder association (chromosome 7)
Paracentric inversion 13q
Susceptibility to chromatid and chromosomal breakage
Constitutional chromosomal instability
Chromosomal pulverization with herpesvirus and respiratory
syncytial virus
p53 overexpression
c-myc overexpression
H-ras overexpression
E-cadherin underexpression
Aneuploidy (DNA index[1.5)
Apoptosis defects
*Compiled from references17, 21, 69,72-75, 80, 81.
OOOOE
Volume 100, Number 2 Hicks and Flaitz S61
http://-/?-http://-/?-7/21/2019 LCH Sunil Sir
21/25
basis.17,82-85 Therapies vary considerably from surgical
curettage to excision with or without the addition of
radiation or chemotherapy. The Histiocyte Society is
contemplating recommending multiagent chemother-
apy for bone-only disease (unifocal or multifocal). Thisis based on clinical data indicating that single agent
chemotherapy, radiation therapy, or observation only is
associated with a high recurrence rate (50% to 80%)
compared with multiagent chemotherapy (18%, Table
X). In fact, some knowledgeable clinicians recommend
chemotherapy with extensive jawinvolvement to avoid
heroic surgery and loss of teeth.17 They contend that a
6-month course of vinblastine and prednisone has a high
likelihood to cure the disease, allow bone redeposition,
and avoid tooth loss.
Certain late effects among pediatric survivors of
LCH are more common that others (Table X).15,17,82-86
Late effects are about 3 times as common with multi-
system disease than with single system disease. Diabetes
insipidusand orthopedic problems occurin about 20%to
25% of children. Tooth loss is noted in less than 10%.
INNOVATIVE THERAPEUTIC AGENTSWith the identification of cytokines, chemokines,
growth factors, and various other proliferation factors in
LCH, avenues for employing new therapeutic agents
become available.17,82,83,87-94 One such agent is 2-CDA
Table XI. Treatment protocols and late effects inLangerhans cell histiocytosis*
Treatment protocols by The Histiocyte Society
LCH-I pediatric clinical trial: multisystem disease
Vinblastine and intravenous steroid or
Etoposide (possible risk of second malignancy)
and intravenous steroid
Prognostic factors in pediatric LCH-II clinical trialTherapeutic response at 6 weeks in high-risk patients
Good response: 94% survival
Poor response: 34% survival
LCH-II pediatric clinical trial: multisystem disease
for high-risk sites
Vinblastine, oral prednisone, mercaptopurine or
Vinblastine,oral prednisone,mercaptopurine, etoposide
Prognostic factors in pediatric LCH-II clinical trial
Therapeutic response at 6 weeks in high-risk patients
Good response: 88% survival
Poor response: 17% survival
Age: No effect on survival
LCH-III pediatric randomized clinical trial
Multisystem disease with high-risk sites
(lung, liver, bone marrow, spleen)
A: Vinblastine and prednisone for 12 months
B: Vinblastine, prednisone, and methotrexate
(1st 6 weeks),
Followed by maintenance vinblastine and
methotrexate, daily oral mercaptopurine and
oral methotrexate weekly for 12 months
Multisystem disease with low-risk sites
(skin, bone, lymph nodes, pituitary)
Vinblastine and prednisone (6 or 12 months)
Single system multifocal disease
Localized special sites (mastoid, orbit, temporal bones)
LCH-A-I adult clinical trial
Single system disease
CNS disease: vinblastine and prednisone
Isolated pulmonary disease: vinblastine and prednisone
Multisystem disease: vinblastine and prednisone
Current treatment reported for those not on The Histiocyte
Association LCH protocols
Unifocal osseous lesion
Surgical curettage or excision
Radiation therapy
Single agent chemotherapy
Combination of above
Multisystem, refractory, relapsing or progressive disease
Chemotherapy with or without radiation therapy
Comparison of bone disease recurrence
Multiagent chemotherapyBone-only disease: 18% recurrence
(unifocal or multifocal)
Single-agent chemotherapy, radiotherapy
or observation only
Bone-only disease: 50%-80% recurrence
Late effects among long-term pediatric survivors, %
At least 1 permanent consequence
All groups 52
Multisystem disease 71
Single system disease 24
Diabetes insipidus 24
Table XI. Continued
Orthopedic abnormalities 20
Hearing loss 13
Neurologic consequences 11
Growth retardation 9
Ophthalmic problems 8
Tooth loss 7
Pulmonary problems 4Skin problems 2
Innovative therapeutic agents
2-CDA (2-chloro-29-deoxyadenosine, cladribine)
Deoxycoformycin
Thalidomide
Alemtuzumab (anti-CD52 antibody)
Retinoic acid
Interleukin-2
Interferon-alpha
Cyclosporin A
Tacrolimus (FK506)
Monoclonal antibody against CD1a and CD207
(langerin)
Intralesional injection of steroids or chemotherapeutic
agent
Phototherapy (ultraviolet light treatment for skin disease)
Bone marrow transplantation (allogeneic or autologous
stem cell)
LCH, Langerhans cell histiocytosis; CNS, central nervous system.
*Compiled from references15, 17, 82-95.
OOOOE
S62 Hicks and Flaitz August 2005
http://-/?-http://-/?-7/21/2019 LCH Sunil Sir
22/25
(2-chloro-29-deoxyadenosine; cladribine).87 This agent
has previously shown good results with lymphoblastic
leukemia, hairy-cell leukemia, chronic lymphocytic leu-
kemia, and Waldenstroms macroglobulinemia. Initial
studies in children with refractory or progressive multi-
focal bone disease or multiorgan disease involvement
have shown promise. All patients had a clinical responsewith 70% requiring no additional therapy after a median
of 50 months follow-up. The other 30% required addi-
tional therapy to become disease-free. Because 2-CDA
is a potent immunosuppressive agent, toxicity was
limited to manageable myelosuppression. Deoxycofor-
mycin is a therapeutic agent related to 2-CDA, which
has been used to a limited extent in other neoplastic
processes, and may be worth further investigation in
LCH.
Thalidomide has been used as a therapeutic agent
with cutaneous LCH with considerable success.88,89 In
13 adult patients, good responses were noted with
resolution of ulcers located on the skin and inguinal,
genital, and perianal areas, with replacement by scar
tissue. The lesions regressed within 1 to 3 months, butrecurred if oral thalidomide treatment was discontinued.
None of the patients reported peripheral neuropathy.
The teratogenic side effect of this drug is well known,
and birth control is mandated in females of child-
bearing age. Thalidomide is an inhibitor of TNF-alpha
and IL-6. Both of these cellular factors participate in
LCH disease. Of interest, another TNF-alpha inhibitor,
etanercept, has shown similar effects in a single case
study.
A monoclonal antibody against CD52 (alemtuzumab)has recently been developed, and is effective indeplet-
ing lymphocytes and dendritic cells in vivo.90 Quite
exciting is the finding that CD52 is expressed on
Langerhans cell histiocytes, but not on normal
Langerhans cells within the epidermis. This finding is
encouraging and provides potential targeted therapy for
patients with refractory high-risk disease resistant to
current therapy. Alemtuzumab has been well tolerated
in clinical trials with refractory chronic lymphocytic
leukemia patients.
Retinoic acid has the ability to induce differentiation
in several different cell types, including leukemic cells,neuroblastoma cells, and Langerhans cell histiocytes
in vitro.91,92 In patients with LCH, retinoic acid hasinduced remission in some cases and stabilized disease
progression in others. Additional coordinated studies
are necessary to determine the therapeutic potential of
this agent in LCH.
Several other therapeutic agents may induce immune
modulation (IL-2, IFN-alpha) or suppress the immune
system (cyclosporine A, tacrolimus).73,79-81-83,93,94
Monoclonal antibodies directed against CD1a or per-
haps even CD207 (langerin) may be employed as
treatment in the near future. Individual case reports have
shown regression of LCH lesions with intralesional
steroid and chemotherapeutic agent administration.17,95
The role of bone marrow transplantation and stem cell
reconstitution are still under investigation as treatment
adjuncts for refractory high-risk patients.
17,82,83
SUMMARYWhen the sentinel case report of eosinophilic gran-
uloma of the jaw with anal involvement was published
almost 6 decades ago, this entity had only recently been
included in the new category of Histiocytosis X.3 The
cell of origin was not known, however the transitive
phases between eosinophilic granuloma of the bone and
Letterer-Siwe disease was noted by the author due to
the histologic picture of both lesions showing eosin-
ophilic infiltration in the tissue3 (p. 256). As noted in the
current review, Langerhans cell histiocytes have been
determined to be the prime component of this disease. It
is also obvious that this cell is an immature dendritic cell
and not a histiocyte at all.
No doubt the extended period from presentation to
diagnosis with Schroffs case3 was related to the rarity
of such a lesion and lack of familiarity with this entity
by pathologists some 60 years ago. Only about 65 cases
were described in the worlds literature at that time.3
Although a rare orphan disease, LCH is readily
identified now by general and oral and maxillofacial
pathologists, as well as by residents in-training. The
clinical and radiographic features in the affected
gentleman are identical to those seen in patients withLCH today. While more sophisticated diagnostic imag-
ing techniques are available, current dental practitioners
use the same radiographic methods used more than 60
years ago to evaluate patients for jaw lesions. Many
sophisticated diagnostic tools are available to modern
day practitioners, such as computed tomography (CT),
magnetic resonance imaging (MRI), nuclear bone scans,
and positron emission tomography (PET). These may be
used to define the jaw lesions or for detection of other
organ and bone involvement.
Confirmation of the diagnosis of LCH has changed
considerably since the early 1940s. Electron micros-copy became available as a diagnostic tool in the early
1950s and was widely adopted in the late 1960s. A
lesion-defining ultrastructural feature for Langerhans
cell histiocytes was discovered in the early 1960sthe
Birbeck granule. The identification of this structure in
both normal Langerhans cells in the epidermis and in
histiocytes within lesional tissue provided the evi-
dence for the cell of origin for LCH. At the time of
Schroffs case report in 1948,3 immunocytochemical
techniques with tissue sections were not yet available.
OOOOE
Volume 100, Number 2 Hicks and Flaitz S63
7/21/2019 LCH Sunil Sir
23/25
By the late 1970s, several immunocytochemical anti-
bodies had been developed for diagnostic purposes, but
required that lesional tissue be frozen at 708C.