Embed Size (px)
Citation preview
Journal Club del venerdìCasi clinici in geriatria
Le cadute. Un punto di vista clinico
Cristina Cornali
14 Marzo 2008
EPIDEMIOLOGIA
Prevalence – U.S.
- 30% community-living fall every year- 50% in nursing home fall every year- 50% repeat fallers
Number of falls increases progressively with age in both sexes and all racial and ethnic groups
(Lancet 2005)
Prevalenza – Italia
Le cadute rappresentano la prima causa di incidenti domestici e anche la prima causa di ricovero e decesso per incidente domestico.
- vittime di incidenti domestici nel 2001: 2.848.000- accessi in PS per un incidente domestico nel 2004: almeno 1.300.000 persone (2% dei residenti) = 10% ricoverate - le cadute rappresentano il 78% degli incidenti domestici (2.221.440) e costituiscono il 56% degli accessi al Pronto soccorso
(PNLG 2007)
Impact of Falls
- 20% need medical attention- 5% hip fracture- 5-10% serious injuries (head injuries, joint
distorsions and dislocations, soft-tissue bruises)
- 25% die within 6 months (falls = 2/3 of accidentaldeath, fifth cause of death in US, ¾ > 65 years)- 25% remain functionally more dependent- 60% have restricted mobility
(Lancet 2005)
Fisiopatologia della caduta nell’anziano
- Riduzione dell’altezza; riduzione della flessione dell’anca e del ginocchio; appiattimento dell’arco del piede- Aumento della rigidità articolare- Alterazioni del centro di gravità, della postura e dell’andatura- Riduzione della forza e della massa muscolare (30-40%)- Modificazioni della coordinazione e senso dell’equilibrio (perdita di cellule di Purkinje e della sostanza nera)- Riduzione della soglia nella sensibilità tattile e vibratoria- Disturbo propiocettivo, ridotta risposta riflessimotoria alla perdita di equilibrio- Ridotta capacità a rispondere agli imput sensoriali e ad evitare le cadute- Riduzione dei tempi di reazione- Ridotta acuità visiva- Ridotta eccitazione vestibolare periferica- Riduzione FC massima e resistenza allo sforzo
Cause mediche di caduta
• Sindromi extrapiramidali• Sindromi del lobo frontale• Idrocefalo • Demenza • Epilessia • Ictus, TIA• Miopatie prossimali• Ipotensione ortostatica; Sincope • Ipersensibilità del senocarotideo• Aritmie• Ischemia
• Anemia; Policitemia• Iposodiemia• Ipoglicemia• Dolore • Ansia
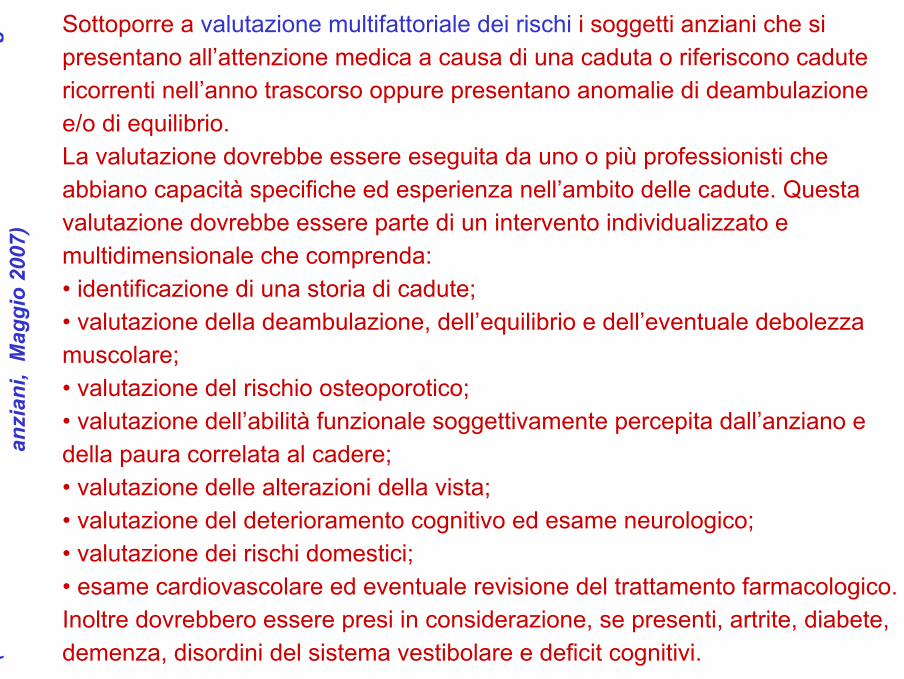
Sottoporre a valutazione multifattoriale dei rischi i soggetti anziani che si presentano all’attenzione medica a causa di una caduta o riferiscono cadute ricorrenti nell’anno trascorso oppure presentano anomalie di deambulazione e/o di equilibrio.La valutazione dovrebbe essere eseguita da uno o più professionisti che abbiano capacità specifiche ed esperienza nell’ambito delle cadute. Questa valutazione dovrebbe essere parte di un intervento individualizzato e multidimensionale che comprenda:• identificazione di una storia di cadute;• valutazione della deambulazione, dell’equilibrio e dell’eventuale debolezza muscolare;• valutazione del rischio osteoporotico;• valutazione dell’abilità funzionale soggettivamente percepita dall’anziano e della paura correlata al cadere;• valutazione delle alterazioni della vista;• valutazione del deterioramento cognitivo ed esame neurologico;• valutazione dei rischi domestici;• esame cardiovascolare ed eventuale revisione del trattamento farmacologico. Inoltre dovrebbero essere presi in considerazione, se presenti, artrite, diabete, demenza, disordini del sistema vestibolare e deficit cognitivi.(P
NLG
–Pr
even
zion
e de
lle c
adut
e da
inci
dent
e do
mes
tico
negl
i an
zian
i, M
aggi
o 20
07)

PREVENZIONE
Shifting the focus in fracture prevention fromosteoporosis to fallsJarvinen T, et al. BMJ 2008, 19 Jan; 336:124-26
Preventing falls is a logical approach to preventing fracture, but can falls be prevented?Evidence from systematic reviews and meta-analyses of randomised trials shows that at least 15% of falls in older people can be prevented, with individual trials reporting reductions of up to50%.
In summary, it is time to shift the focus in fracture prevention fromosteoporosis to falls. Falling is an under-recognised risk factor forfracture, it is preventable, and prevention provides additional healthbenefits beyond avoiding fractures.
Le cadute sono l’epifenomeno di una serie di eventi afferenti a vari domini, la cui definizione permette di compiere scelte preventive nel singolo anziano e in una popolazione.
(Trabucchi, 2008)
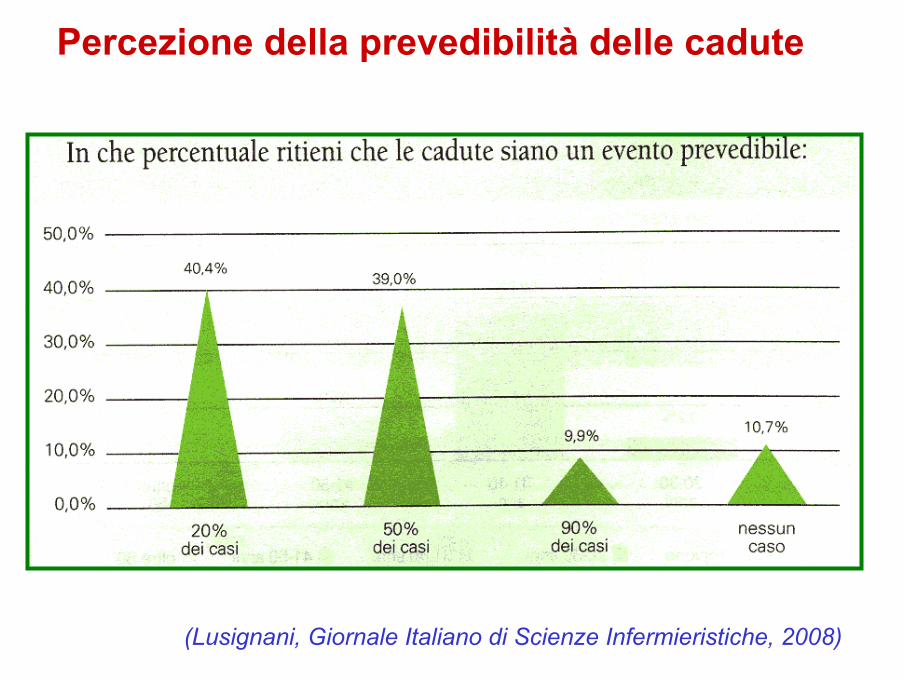
Percezione della prevedibilità delle cadute
(Lusignani, Giornale Italiano di Scienze Infermieristiche, 2008)
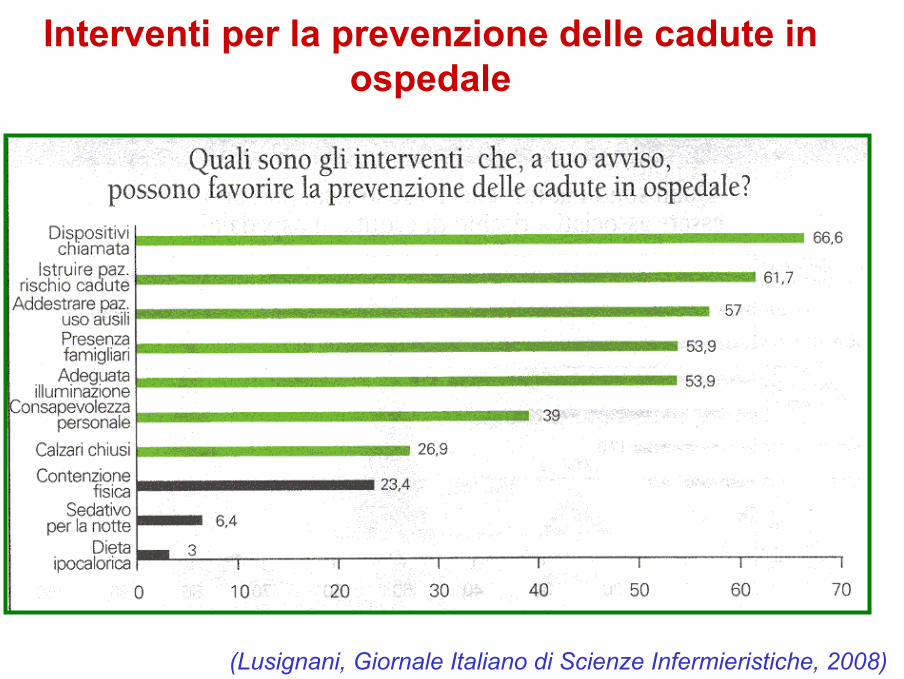
Interventi per la prevenzione delle cadute in ospedale
(Lusignani, Giornale Italiano di Scienze Infermieristiche, 2008)

VALUTAZIONE DEL RISCHIO
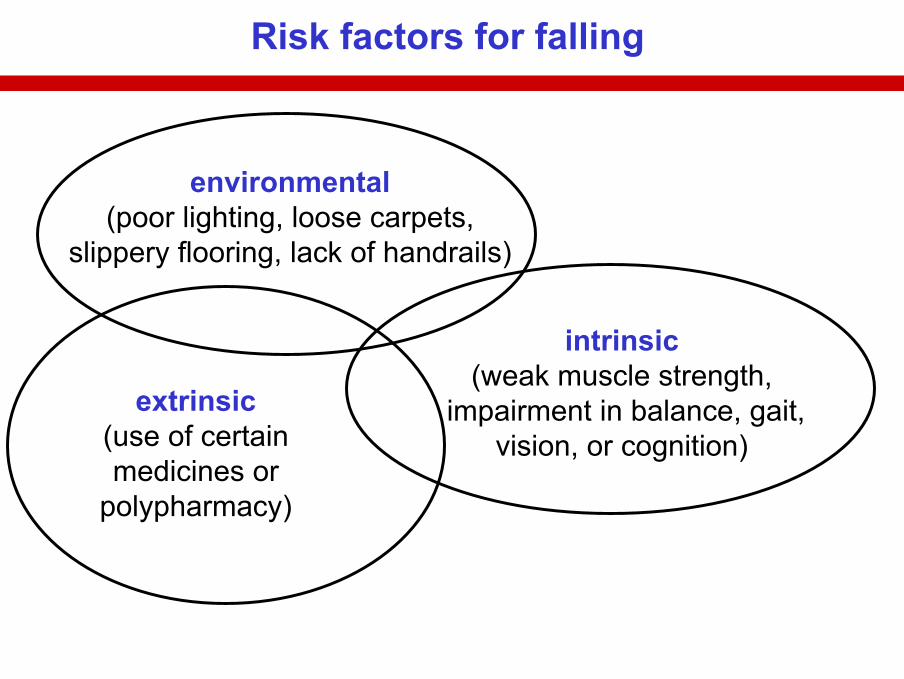
extrinsic(use of certainmedicines or
polypharmacy)
environmental(poor lighting, loose carpets,
slippery flooring, lack of handrails)
intrinsic(weak muscle strength,
impairment in balance, gait,vision, or cognition)
Risk factors for falling
(Lancet 2005)
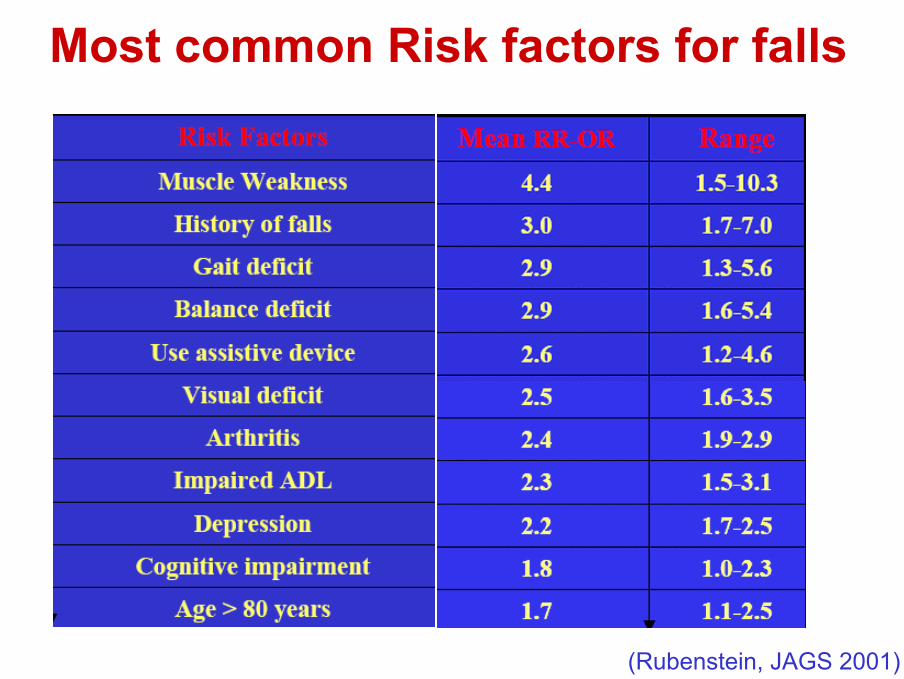
Most common Risk factors for falls
(Rubenstein, JAGS 2001)
• Considerato il rischio elevato di recidiva, si raccomanda di intervistare periodicamente gli anziani per capire se abbiano subito cadute nell’ultimo anno e per conoscerne eventualmente la frequenza, le caratteristiche e il contesto.
• Interrogare gli anziani sulle terapie assunte e tenere sotto rigido controllo i farmaci somministrati.
• Rivedere periodicamente le prescrizioni farmacologiche, con particolare attenzione all’assunzione di farmaci quali BDZ, antidepressivi o all’assunzione simultanea di 3 farmaci. Ove possibile, rimodulare tali prescrizioni al fine di ridurre l’esposizione al rischio.
• I medici responsabili della gestione clinica del paziente devono effettuare o far effettuare un accurato esame della vista.
(PNLG; Maggio 2007)
The use of psychotropic drugs (antidepressants, mainly tricyclic, antipsychotics, long- and short-actingbenzodiazepines) was associated with an increase in the risk of falls.With respect to cardiovascular drugs, a weak association was reported between falls and use of any diuretic, digoxin, or type IA antiarrythmic medicine. However, no statistically significant associations were found between falls and use of thiazides, loop diuretics, angiotensin-converting enzyme (ACE) inhibitors, or calcium channel blockers. Analgesics were not significantly associated with falls.
Older adults taking more than 3 or 4 medicines were at increased risk of recurrent falls.
(Journal of Gerontology, 2007)
Review Article (29 studies)
Medication as a Risk Factor for Falls: Critical SystematicReviewHartikainen S, et al. Journal of Gerontology 2007, 62A(10):1172-81
Benzodiazepines are one of the main risk factors for falls and fractures in older people… not only in long-term use but also after a new prescription. Similar findings were reported; have negative effects on cognition, gait, and balance, the concentration that produces half of a full response forsedation is reduced by 50% in elderly persons. Zolpidem proved to be asrisky as traditional BDZ.Antidepressants, particularly TCAs and SSRIs, seem to be associated with a high risk for falling. SSRIs might carry even higher risks for falling than do traditional antidepressants (serotonin syndrome when used in higher doses or concomitantly with other serotonergic drugs; inappropriateantidiuretic hormone secretion (SIADH); hyponatremia; cardiovascular depressanteffects by inhibiting cardiac Na+ and Ca++ channels).Whether antidepressants that inhibit both serotonin and noradrenalin reuptake (SNRI) are safer than TCAs or SSRIs has yet to be studied.
Review Article (29 studies)
Medication as a Risk Factor for Falls: Critical SystematicReviewHartikainen S, et al. Journal of Gerontology 2007, 62A(10):1172-81
Antipsychotic drugs as a group seem to be associated with an increased risk of falling (extrapyramidal adverse effects; anticholinergic properties and effects on alpha-adrenergic receptors).The relative risk of falls ranged between 1.21 and 11.4, whereas in the meta-analysis of Leipzing et coll. (1999), the pooled OR was 0.41 forpsychiatric inpatients and 1.66 for other participants.More evidence is needed to show whether the new atypical antipsychotic drugs are safer than the traditional ones.
Polypharmacy remained a risk factor for falls only when the medication included at least one drug known to pose a risk for falling. Especiallyconcomitant use of several CNS drugs should be avoided.
• Tenere sotto controllo l’equilibrio e i problemi di deambulazione negli anziani che riferiscono una precedente caduta o che sono considerati a rischio. Valutare il rischio mediante test specifici.
• II medico curante dovrebbe osservare la capacità di un paziente di stare eretto, di girarsi e di sedere, di camminare agevolmente. Qualora si verificassero problemi, l’anziano dovrebbe essere invitato a recarsi presso uno specialista.
• I test ideali per valutare il rischio di caduta devono essere di semplice esecuzione, di breve durata, ripetibili per consentire il follow-up. Risultano avere queste caratteristiche la BergBalance Scale per la valutazione dell’equilibrio, il Timed Up and Go per la valutazione della mobilità e la Tinetti Balance(equilibrio/mobilità).
(PNLG; Maggio 2007)
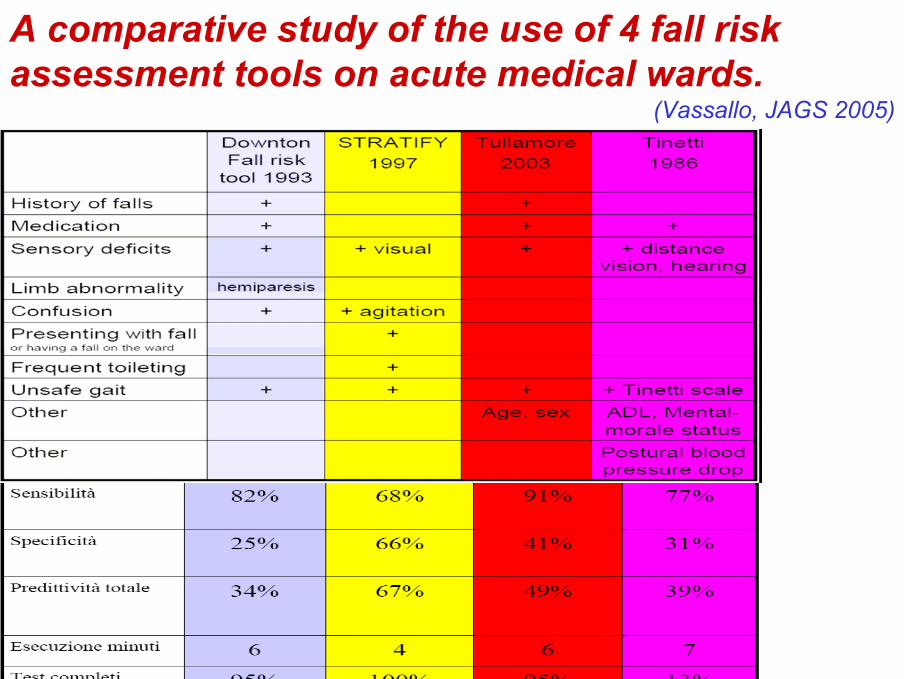
A comparative study of the use of 4 fall riskassessment tools on acute medical wards.
(Vassallo, JAGS 2005)
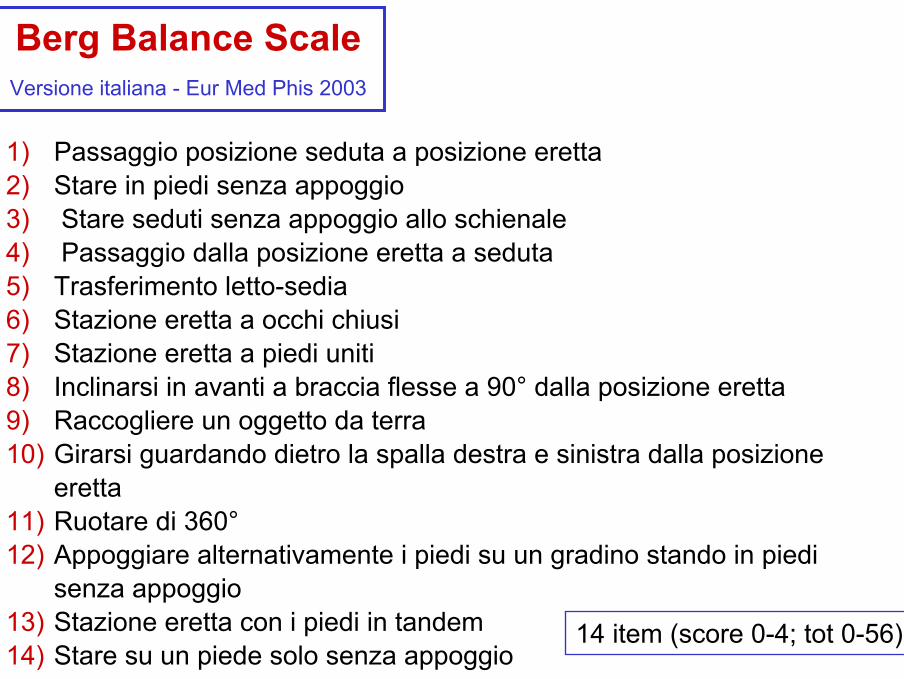
Berg Balance ScaleVersione italiana - Eur Med Phis 2003
1) Passaggio posizione seduta a posizione eretta2) Stare in piedi senza appoggio3) Stare seduti senza appoggio allo schienale4) Passaggio dalla posizione eretta a seduta5) Trasferimento letto-sedia6) Stazione eretta a occhi chiusi7) Stazione eretta a piedi uniti8) Inclinarsi in avanti a braccia flesse a 90° dalla posizione eretta9) Raccogliere un oggetto da terra10) Girarsi guardando dietro la spalla destra e sinistra dalla posizione
eretta11) Ruotare di 360°12) Appoggiare alternativamente i piedi su un gradino stando in piedi
senza appoggio13) Stazione eretta con i piedi in tandem14) Stare su un piede solo senza appoggio
14 item (score 0-4; tot 0-56)
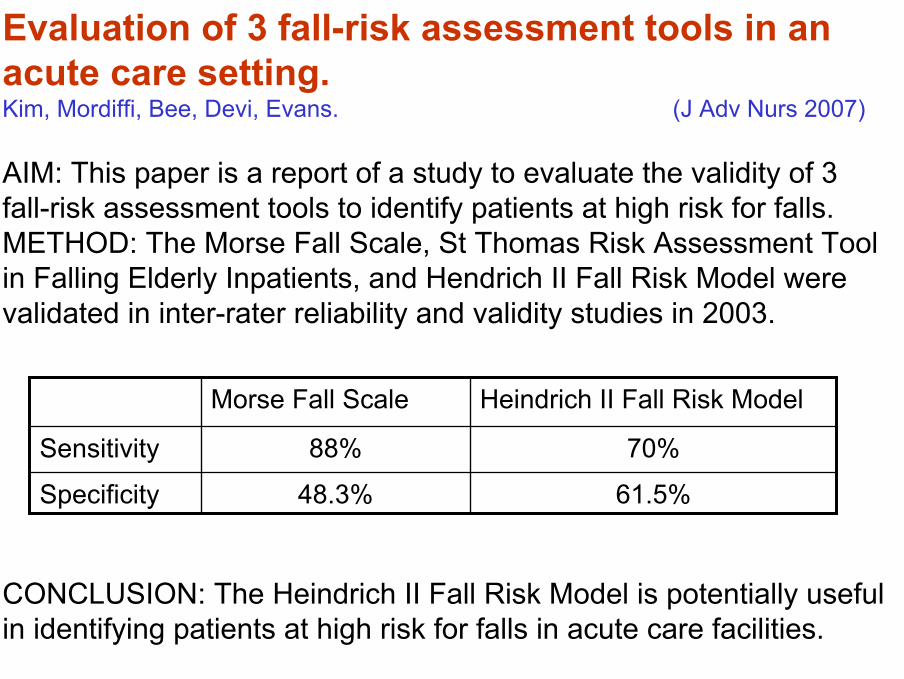
Evaluation of 3 fall-risk assessment tools in an acute care setting.Kim, Mordiffi, Bee, Devi, Evans. (J Adv Nurs 2007)
AIM: This paper is a report of a study to evaluate the validity of 3 fall-risk assessment tools to identify patients at high risk for falls. METHOD: The Morse Fall Scale, St Thomas Risk Assessment Tool in Falling Elderly Inpatients, and Hendrich II Fall Risk Model were validated in inter-rater reliability and validity studies in 2003.
CONCLUSION: The Heindrich II Fall Risk Model is potentially useful in identifying patients at high risk for falls in acute care facilities.
61.5%48.3%Specificity
70%88%Sensitivity
Heindrich II Fall Risk ModelMorse Fall Scale
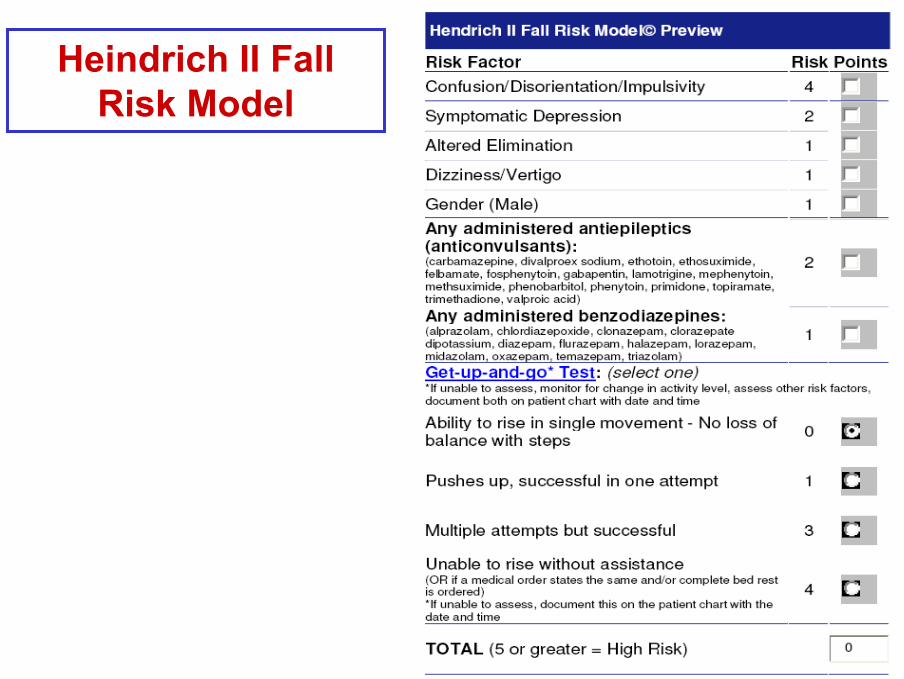
Heindrich II Fall Risk Model
Non vi è sufficiente prova per considerare il deterioramento cognitivo un fattore di rischio di caduta negli anziani. Non vi sono elementi certi per raccomandare o sconsigliare controlli sul deterioramento cognitivo al fine di prevenire le cadute.
Gli studi analizzati non forniscono sufficienti prove sul deterioramento cognitivo come fattore di rischio. Uno studio di alta qualità, attribuisce al fattore di rischio «deficit cognitivo» un RR=2,27. Un altro studio riporta risultati in contrasto con questo risultato.La linea guida NICE del 2004 riporta due studi condotti su residenti presso il proprio domicilio che riferivano il deterioramento cognitivo come fattore significativo di rischio di caduta (OR=2,2-2,4); inoltre, uno studio di bassa qualità condotto in ambito di assistenza estesa ha descritto un OR=6,2 (1,7-23,3). Tuttavia, nove studi riportati nella linea guida NICE non hanno rilevato che i soggetti anziani con deterioramento cognitivo siano significativamente a rischio di caduta in entrambi gli ambiti.
(PNLG; Maggio 2007)
MENTAL FUNCTIONS AND PHYSICAL PERFORMANCE ABILITIES AS PREDICTORS OF FALLING IN A GERIATRIC EVALUATION AND REHABILITATION UNIT
(Cornali, JAGS 2004)
Of 865 elderly patients consecutively admitted during 27 months, 53 (6.1%) fell during hospitalization.In a multivariate regression model, after adjusting for age, sex, Katz index, Tinetti scale, osteoarthritis, Parkinson’s disease, and stroke, risk factors of falling were: • MMSE OR 1.8 95%CI 1.0–3.3• GDS OR 1.9 95%CI 1.0–3.4• PPT OR 3.2 95%CI 1.3–7.6.
Cognitive deficits and mood disorder may lead to reduced Cognitive deficits and mood disorder may lead to reduced attention, planning, dexterity, coordination, attention, planning, dexterity, coordination, praxispraxis, and other , and other
executive functions, thus contributing executive functions, thus contributing toto the risk of fallingthe risk of falling..PPT is a sensitive instrument on the effect of mental impairmenton mobility.
The relationship between specific cognitive functions and falls in the agingHoltzer R, et al. Neuropsychology 2007 Sep ;21 (5):540-8.
The current study examined the relationship between cognitive function and falls in older people who did not meet criteria for dementia or mild cognitive impairment (N = 172). To address limitations of previous research, the authors controlled for the confounding effects of gait measures and otherrisk factors by means of associations between cognitive function and falls. A neuropsychological test battery was submitted to factor analysis, yielding 3 orthogonal factors (Verbal IQ, Speed/Executive Attention, Memory). Single and recurrent falls within the last 12 months were evaluated.
Multivariate logistic regressions showed that lower scores on Speed/Executive Attention were associated with increased risk of single and recurrent falls. Lower scores on Verbal IQ were related only toincreased risk of recurrent falls. Memory was not associated with eithersingle or recurrent falls. These findings are relevant to risk assessment and prevention of falls and point to possible shared neural substrates of cognitive and motor function.
(PNLG, Maggio 2007)
Interrogare gli anziani per capire se abbiano paura di cadere; in tal caso il livello e la ragione di questa paura dovrebbero essere valutati da una professionista sanitario.
Circa un terzo degli anziani che non ha storie precedenti di cadute ha comunque paura di cadere. La percentuale raddoppia nelle persone che sono già cadute almeno una volta.Ovviamente il fattore “paura” gioca un ruolo molto rilevante nelcondizionare l’anziano e nell’aumentare il suo rischio di incidente, conducendo di fatto a una perdita di indipendenza nello svolgimento delle normali attività quotidiane. I fattori che determinano la paura di cadere sono numerosi e le cause difficili da identificare. E’ importante tuttavia misurarne l’intensità, per intervenire e sostenere gli anziani attraverso interventi educativi e di counselling, che devono essere condotti da professionisti del settore. E’ importante affrontare il tema della paura di cadere con le persone a rischio, indagandone i possibili motivi, l’intensità e i risvolti psicologici, in modo da poter fornire un supporto adeguato.

II medico curante deve chiedere all’anziano se ha paura di cadere: qualora questi dichiarasse di averne, potrebbero essere opportuni sia un approfondimentodelle ragioni che portano a questa paura sia un supporto psicologico.Valutare le caratteristiche psicometriche dei soggetti anziani utilizzando i metodi disponibili al fine di misurare la paura di cadere nei soggetti. Si può ritenere che la ”Tinetti Balance” sia il migliore strumento per misurare la paura di cadere.
(PNLG, Maggio 2007)
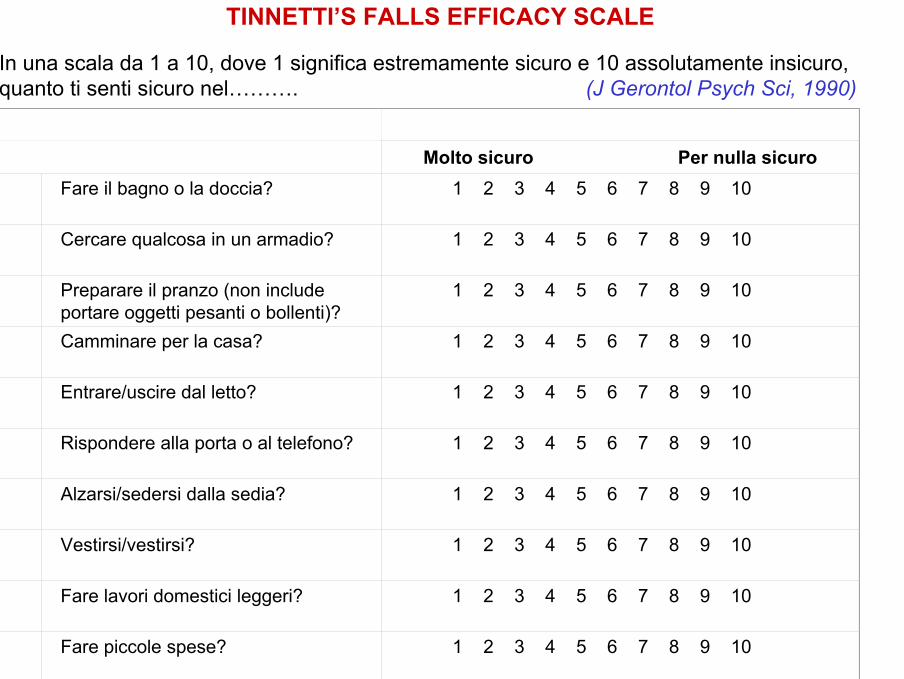
In una scala da 1 a 10, dove 1 significa estremamente sicuro e 10 assolutamente insicuro, quanto ti senti sicuro nel………. (J Gerontol Psych Sci, 1990)
Molto sicuro Per nulla sicuroFare il bagno o la doccia? 1 2 3 4 5 6 7 8 9 10
Cercare qualcosa in un armadio? 1 2 3 4 5 6 7 8 9 10
Preparare il pranzo (non include portare oggetti pesanti o bollenti)?
1 2 3 4 5 6 7 8 9 10
Camminare per la casa? 1 2 3 4 5 6 7 8 9 10
Entrare/uscire dal letto? 1 2 3 4 5 6 7 8 9 10
Rispondere alla porta o al telefono? 1 2 3 4 5 6 7 8 9 10
Alzarsi/sedersi dalla sedia? 1 2 3 4 5 6 7 8 9 10
Vestirsi/vestirsi? 1 2 3 4 5 6 7 8 9 10
Fare lavori domestici leggeri? 1 2 3 4 5 6 7 8 9 10
Fare piccole spese? 1 2 3 4 5 6 7 8 9 10
TINNETTI’S FALLS EFFICACY SCALE
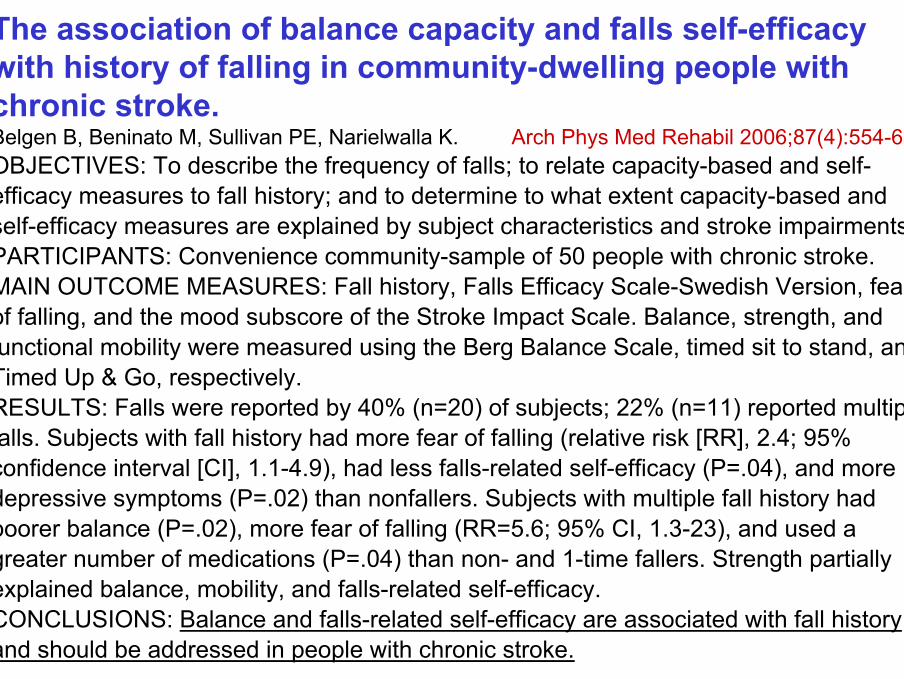
The association of balance capacity and falls self-efficacy with history of falling in community-dwelling people with chronic stroke.Belgen B, Beninato M, Sullivan PE, Narielwalla K. Arch Phys Med Rehabil 2006;87(4):554-61.OBJECTIVES: To describe the frequency of falls; to relate capacity-based and self-efficacy measures to fall history; and to determine to what extent capacity-based and self-efficacy measures are explained by subject characteristics and stroke impairments. PARTICIPANTS: Convenience community-sample of 50 people with chronic stroke. MAIN OUTCOME MEASURES: Fall history, Falls Efficacy Scale-Swedish Version, fear of falling, and the mood subscore of the Stroke Impact Scale. Balance, strength, and functional mobility were measured using the Berg Balance Scale, timed sit to stand, and Timed Up & Go, respectively. RESULTS: Falls were reported by 40% (n=20) of subjects; 22% (n=11) reported multiple falls. Subjects with fall history had more fear of falling (relative risk [RR], 2.4; 95% confidence interval [CI], 1.1-4.9), had less falls-related self-efficacy (P=.04), and more depressive symptoms (P=.02) than nonfallers. Subjects with multiple fall history had poorer balance (P=.02), more fear of falling (RR=5.6; 95% CI, 1.3-23), and used a greater number of medications (P=.04) than non- and 1-time fallers. Strength partially explained balance, mobility, and falls-related self-efficacy. CONCLUSIONS: Balance and falls-related self-efficacy are associated with fall history and should be addressed in people with chronic stroke.

INTERVENTO
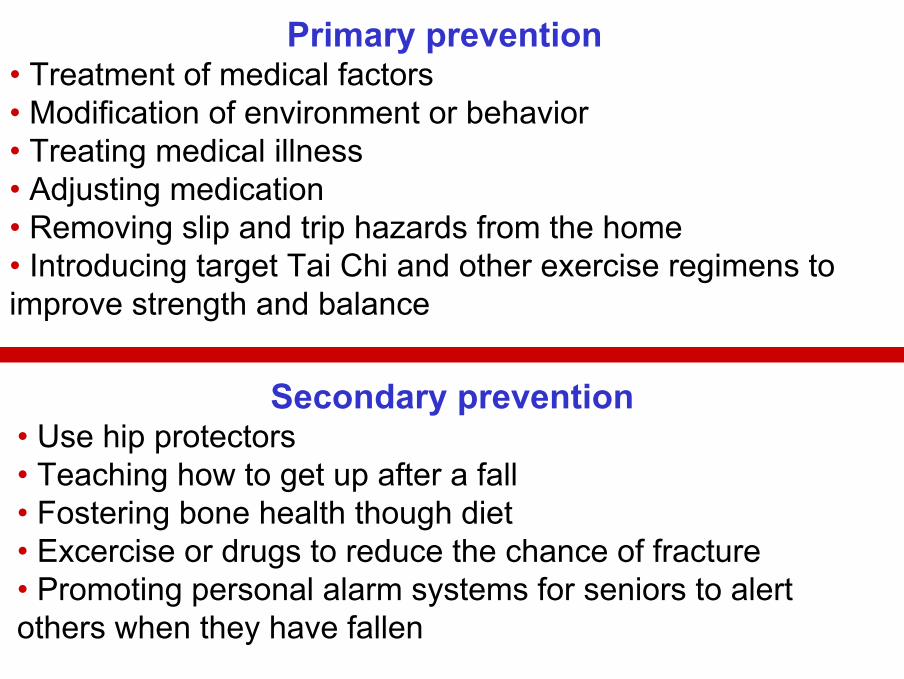
Primary prevention• Treatment of medical factors• Modification of environment or behavior• Treating medical illness• Adjusting medication• Removing slip and trip hazards from the home• Introducing target Tai Chi and other exercise regimens toimprove strength and balance
Secondary prevention• Use hip protectors• Teaching how to get up after a fall• Fostering bone health though diet• Excercise or drugs to reduce the chance of fracture• Promoting personal alarm systems for seniors to alertothers when they have fallen
Un approccio multidisciplinare, multidimensionale alla gestione di soggetti anziani vittime di cadute traumatiche che sono stati trattati in ambito di assistenza di base o di assistenza in fase acuta è stato descritto come pacchetto di intervento efficace in due studi. Importanti componenti del trattamento devono essere la valutazione della salute generale del paziente, interventisui fattori di rischio e un dettagliato piano di dimissione.Il primo obiettivo da porsi nella presa in carico della persona anziana è un’accurata valutazione clinica. L’attenzione dovrebbe essere rivolta a identificare e possibilmente a trattare le patologie o le condizioni che potrebbero favorire l’insorgenza di cadute.
NB = nelle U.O.Ortopedia, nei PS!!
(PNLG, Maggio 2007)
• Sono raccomandati programmi di intervento personalizzati tesi a migliorare la forza, la deambulazione e l’equilibrio.
• Fornire informazioni e interventi educativi mirati alla consapevolezza dei rischi. Offrire alle persone che sono dimesse dall’ospedale o dal Pronto soccorso in seguito a caduta un controllo della situazione ambientale e dei pericoli presenti attraverso l’esecuzione di visite domiciliari.
• Consigliare agli anziani l’installazione di dispositivi (spie antincendio, strisce antiscivolo, maniglie ecc.) che possano rendere più sicuro l’ambiente domestico.
(PNLG, Maggio 2007)
• Tramite il personale sanitario che si occupa di cadute è importante supportare gli anziani con informazioni sia verbali sia scritte relative alle cadute. In particolare su questi argomenti:
• quali misure adottare per prevenire le cadute e come prevenirle con l’esercizio;
• quali sono i benefici fisici e psicologici che possono derivare dalla prevenzione dei rischi di caduta;
• come comportarsi in seguito a una caduta;• dove trovare consigli e assistenza.
Se necessario, dovrebbero essere fornite informazioni agli anziani anche in lingue diverse dall’italiano; i programmi di prevenzione delle cadute dovrebbero anche contribuire a migliorare l’autostima e diminuire la paura di cadere. (PNLG, Maggio 2007)
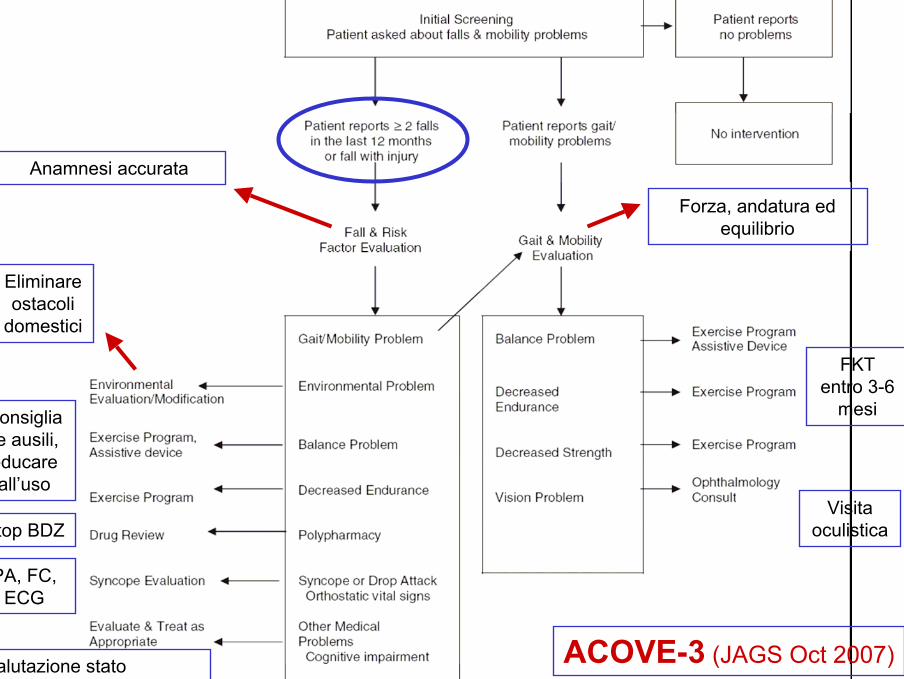
ACOVE-3 (JAGS Oct 2007)
Anamnesi accurata
PA, FC, ECG
Visita oculistica
Forza, andatura ed equilibrio
Valutazione stato cognitivo ultimi 3-6 mesi
Eliminare ostacoli
domestici
Stop BDZ
Consigliare ausili, educare all’uso
FKT entro 3-6
mesi
(Prevention of Falls and consequent injuries in elderly people, Lancet 2005)
Rethinking individual and community fall preventionstrategies: a meta-regression comparing single and multifactorial interventionsCampbell AJ, Robertson MC. Age and Ageing 2007;36:656–662
The meta-analyses demonstrate that the delivery of single factorinterventions to selected populations is as effective in reducing fallsas delivering multifactorial interventions to at risk community populations (mean reduced falls = 24%).
Single interventions need to be carefully directed to the appropriate population. Such interventions are highly successful when used in populations where the risk factor addressed accounts for a largeproportion of the falls risk. Such a specific intervention is ineffective ifit does not alter the risk factor, or the risk factor accounts for a smallproportion of the risk.
(Lancet 2005)
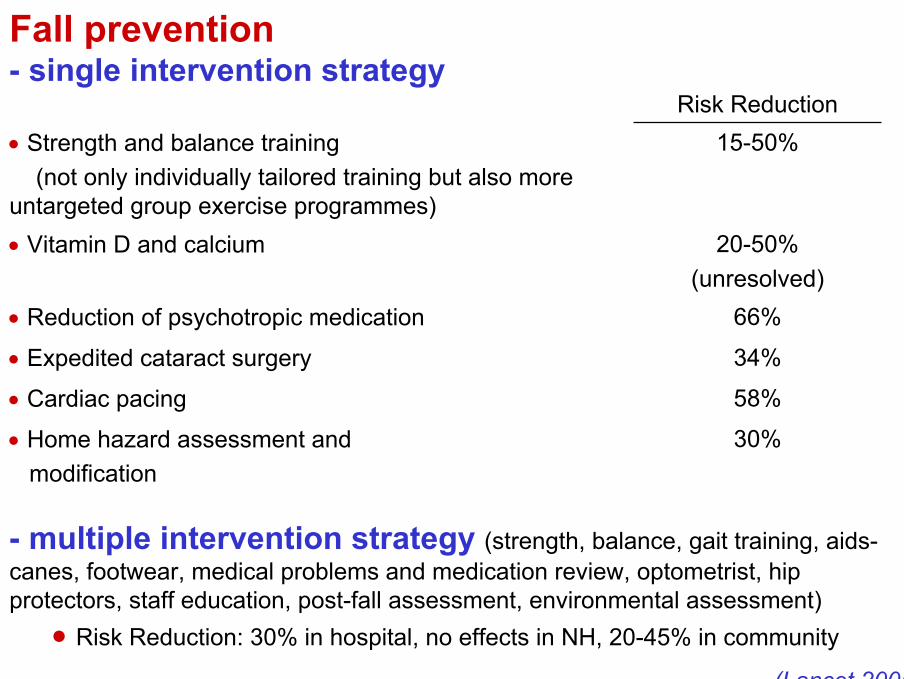
Fall prevention- single intervention strategy
Risk Reduction
30%• Home hazard assessment and modification
58%• Cardiac pacing
34%• Expedited cataract surgery
66%• Reduction of psychotropic medication
20-50%(unresolved)
• Vitamin D and calcium
15-50%• Strength and balance training (not only individually tailored training but also more
untargeted group exercise programmes)
- multiple intervention strategy (strength, balance, gait training, aids-canes, footwear, medical problems and medication review, optometrist, hipprotectors, staff education, post-fall assessment, environmental assessment)
• Risk Reduction: 30% in hospital, no effects in NH, 20-45% in community
In the United Kingdom the national service framework forolder people, published in 2001, required the NationalHealth Service to establish multifactorial programmes for fallprevention. The National Institute for Health and Clinical Excellence(NICE) clinical practice guideline for the assessment and prevention of falls in older people recommended thatmultifactorial risk assessment and individualisedinterventions should be undertaken. Such services (falls clinics) have now been introducedthroughout the UK NHS but in the absence of any evidenceabout the optimum configuration, they have varied in location, skill mix, assessments, and interventions offered.
No clear overall effect was found on the number of fallers during follow-up(18 studies; RR 0.91, 95%CI 0.82 - 1.02) or fall related injuries (8 studies;RR 0.90, 0.68 - 1.20).
VERSUS
The Cochrane review (2003): unselected populations (4 trials) = RR for the number of fallers of 0.73 (95%CI 0.63 - 0.85); populations with previous falls (5 trials) = RR for fallers 0.86 (95%CI 0.76 - 0.98).
Another earlier review (BMJ 2004; 13 trials of multifactorial riskassessment, some of which were done in care home or hospital settings) RR 0.82 (95%CI 0.72 - 0.94).
Multifactorial assessment and targeted intervention forpreventing falls and injuries among older people incommunity and emergency care settings: systematic review and meta-analysisGates S, et al. BMJ, 2008;336:130-3.
This systematic review found little evidence to support the effectiveness of multifactorial interventions to prevent falls and injuries in older people in community and emergency care settings. No clear reduction was found in the number of people having at least one fall, the number having fall related injuries, or use of health services.Higher intensity interventions that provide treatments to address riskfactors rather than information and referral may be more effective. The costs of implementation of these interventions have not beenextensively studied but as they are likely to be expensive the costeffectiveness of this type of intervention is questionable.
Multifactorial assessment and targeted intervention forpreventing falls and injuries among older people incommunity and emergency care settings: systematic review and meta-analysisGates S, et al. BMJ, 2008;336:130-3.
Interventions for Preventing Falls in Acute- and Chronic-Care Hospitals: A Systematic Review and Meta-Analysis.Coussement J, et al. JAGS 2008;56:29–36.
8 studies
CONCLUSIONS: this meta-analysis found no conclusiveevidence that hospital fall prevention programs can reducethe number of falls or fallers.
Effects were noted only for patients admitted for longer periodsof time, namely in studies conducted in long-stay geriatric or rehabilitation settings. Precisely in these settings, like in residential care homes and community care, the likely delayedbenefit from interventions such as calcium plus vitamin D3, physiotherapy, and medical review can be better achieved thanin an acute setting.
Limits of multiple-intervention
• Cannot distinguish between the independent role of individual modified risk factor
• Cannot established which part of the intervention iseffective
• To implement a complex intervention when, in truth, the use of 1 or 2 of its components is equally effective
• Intensive and expensive labour; no cost-effective
In this systematic review and meta-analysis we found some evidence formodest reductions- in rates of falls in hospital patients with multifaceted interventions
(RR 0.82 95%CI 0.68 - 0.99)- in rates of hip fractures with hip protectors in people in care homes
(RR 0.67 95%CI 0.46 - 0.98).
However, we found insufficient evidence for any other interventions (multifaceted interventions in NH, removal of physical restraint, fall alarmdevices, exercise, changes in the physical environment, calcium and vitamin D in care homes, medication review).
BUT …
One third of older adults fall each year, placing them at risk for serious injury, functional decline, and health care utilization. Despite the availability of effectivepreventive approaches, policy and clinical efforts at preventing falls among older adults have been limited. In this article we present the burden of falls, review evidenceconcerning the effectiveness of fall-prevention services, describe barriers for cliniciansand for payers in promoting these services, and suggest strategies to encourage greater use of these services. The challenges are substantial, but strategies for incrementalchange are available while more broad-based changes in health care financing and clinical practice evolve to better manage the multiple chronic health conditions, including falls, experienced by older Americans.
Incidence of In-Hospital Falls in Geriatric Patients Beforeand After the Introduction of an Interdisciplinary Team–Based Fall-Prevention Interventionvon Renteln-Kruse W, et al. JAGS 2007;55:2068–2074.
A structured fall-prevention program was introduced in aclinical setting with existing geriatric multidisciplinary care.The measures undertaken were targeted toward improvement of patients’ active transfer, safe use of the toiletand bathroom, appropriate use of aids and mobility devices, and patient and caregiver education. A significant reductionin fall incidence and the relative risk of falling followedintroduction of the intervention.
NB: length of stay 20 days
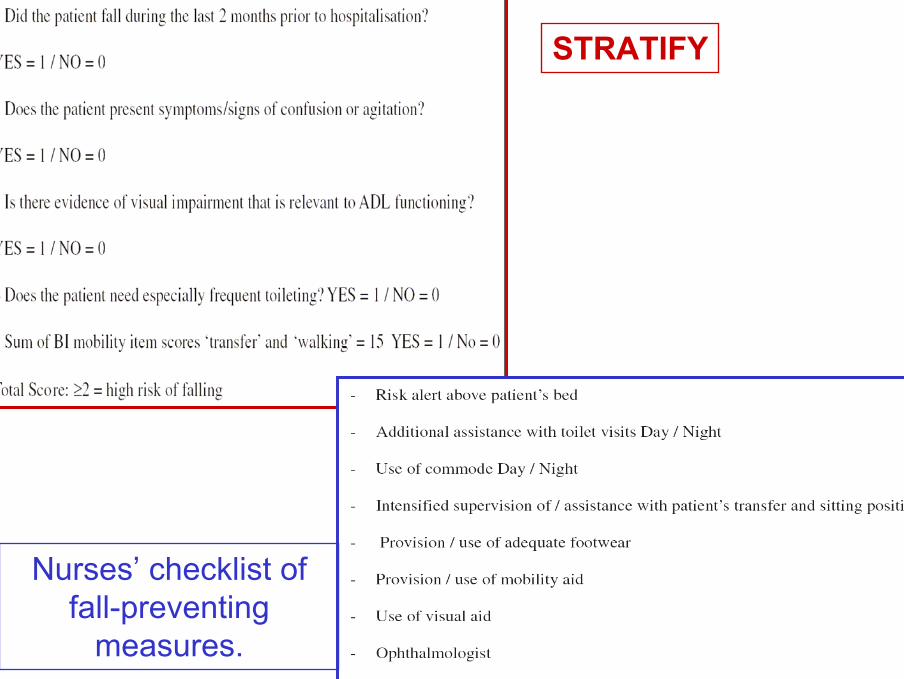
STRATIFY
Nurses’ checklist of fall-preventing
measures.
Can volunteer companions prevent fallsamong inpatients? A feasibility study using a pre-post comparative design.
Giles LC, Bolch D, Rouvray R et al.BMC Geriatr 2006;6:11.
There were no inpatient falls after the introduction of volunteers to ‘‘sit’’ with patients identified as being at high risk of falling.
A randomised controlled trial of Tai Chi and resistance exercise on bone health, muscle strength and balance in community-living elderlypeople.Woo J, et al. Age Ageing 2007 May;36(3):262-8.
Interventions to reduce fear of falling in community-livingolder people: a systematic review.Zijlstra GA, et al. J Am Geriatr Soc 2007 Apr;55(4):603-15.
A randomized, controlled trial of tai chi for the prevention of falls: the Central Sydney tai chi trial.Voukelatos A, et al. J Am Geriatr Soc 2007 Aug;55(8):1185-91.
-28%
NO
Tai-Chi C’uan is a promising type of balanceexercise, although it requires furthereveluation before it can be recommended asthe preferred balance training (grade of evidence C, Guideline for prevention of falls in Older Persons -Rubenstein,JAGS 2001)
RSA
We know all falls cannot be prevented. How should institutional falls be interpreted?Undoubtedly falls do reflect the quality of care provided.Falls need to be interpreted
A) at the istitutional level – by examining staffing levels, the environment and circumstances in which residents are falling
B) at the individual level – by examining factors such prescriptions, reversible visual impairment, and use of walking aids.
(McMurdo, Age Ageing 2004)
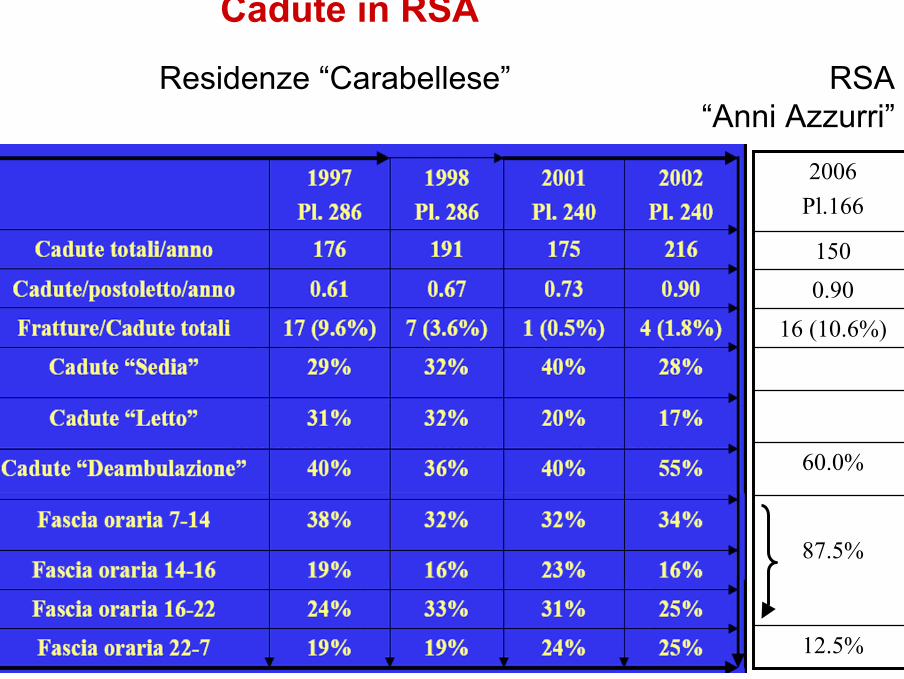
Cadute in RSA
12.5%
87.5%
60.0%
16 (10.6%)0.90150
2006Pl.166
Residenze “Carabellese” RSA “Anni Azzurri”
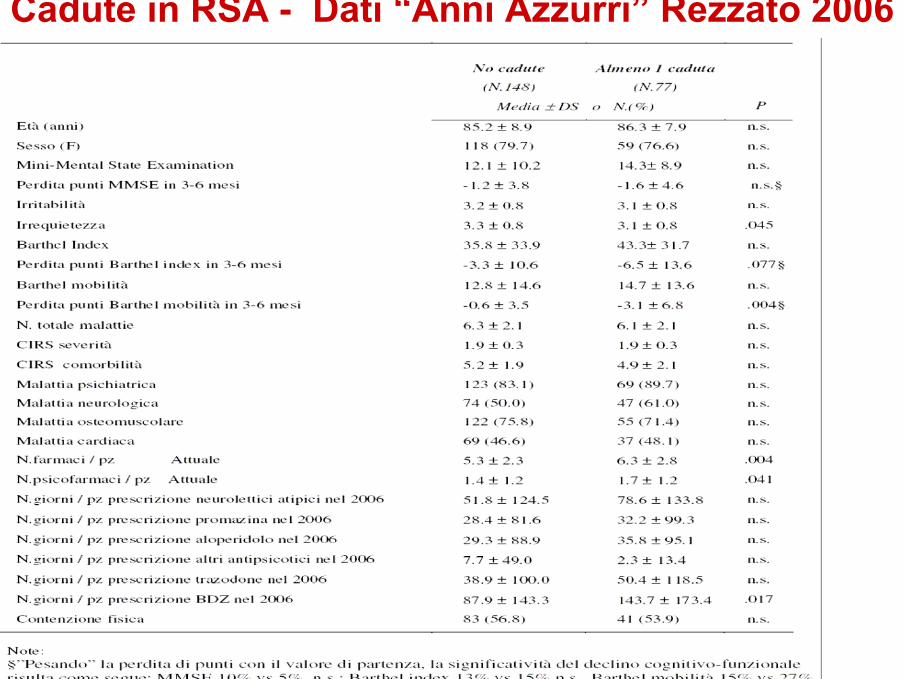
Cadute in RSA - Dati “Anni Azzurri” Rezzato 2006
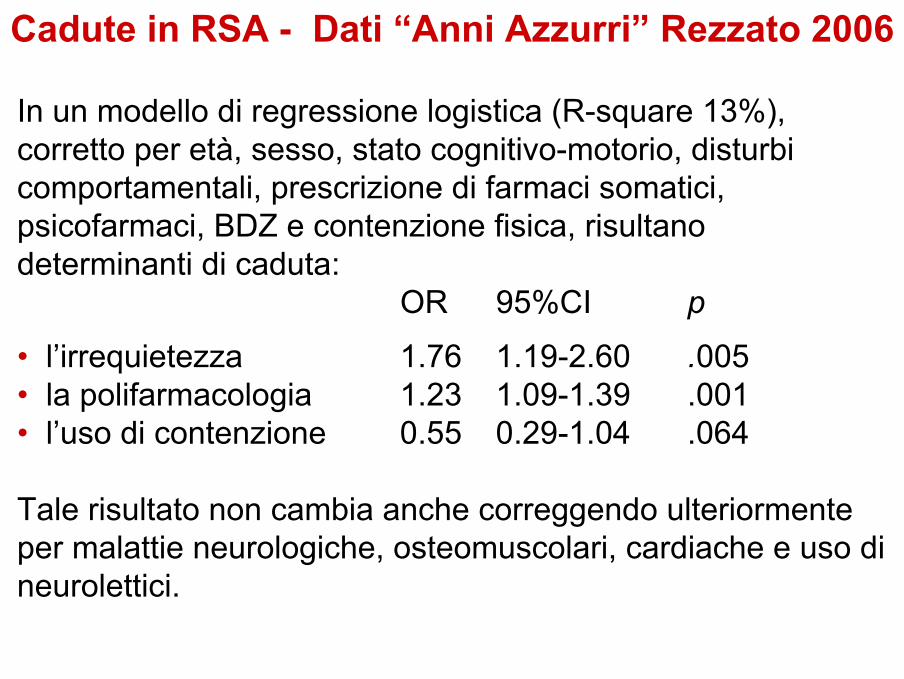
In un modello di regressione logistica (R-square 13%), corretto per età, sesso, stato cognitivo-motorio, disturbi comportamentali, prescrizione di farmaci somatici, psicofarmaci, BDZ e contenzione fisica, risultano determinanti di caduta:
OR 95%CI p
• l’irrequietezza 1.76 1.19-2.60 .005• la polifarmacologia 1.23 1.09-1.39 .001• l’uso di contenzione 0.55 0.29-1.04 .064
Tale risultato non cambia anche correggendo ulteriormente per malattie neurologiche, osteomuscolari, cardiache e uso di neurolettici.
Cadute in RSA - Dati “Anni Azzurri” Rezzato 2006
Raccomandazioni per la prevenzione dellecadute in Long-term Care
Guideline for prevention of falls in Older Persons(Rubenstein, JAGS 2001)
• Assessment: “”Should be asked at least 1 a year aboutfalls” + “Get up and Go” test
• Multy-factorial Inetrventions:1) staff education programs2) gait training and advice on the appropriate use of assistive devices3) review and modification of medications, especially psychotropic medications
Falls in the nursing home: Are they preventable?Vu MO, Weintraub N, Rubenstein LZ. J Am Med Dir Assoc. 2005 May-Jun;6(3 Suppl):S82-7
CONCLUSION: Based on the current literature, an effectivemultifaceted fall prevention program for nursing home residentsshould include risk factor assessment and modification, staff education, gait assessment and intervention, assistive deviceassessment and optimization, as well as environmentalassessment and modification. Although there is no associationbetween the use of hip protectors and fall rates, their use should beencouraged because the ultimate goal of any fall preventionprogram is to prevent fall-related morbidity.
There is a little doubt that prevention of falls is a complex area giventhe methods by which we identify and define risk, the heterogeneityof the population at risk and the modes of intervention on offer. Are all falls of equal impact and are all interventions of equal value withinand between different at-risk population?
Caso clinico N.1 Maria D, 84 anni, Novembre 2007
Vive al proprio domicilio, frequenta un CDI, aiutata dai famigliari per il resto della giornata.Anamnesi:- Malattia di Parkinson (stadio 3 sec.Hoehn-Yahr), complicata da decadimento cognitivo lieve e disturbi comportamentali (ansia, depressione)- Poliartrosi e osteoporosi severa (crollo vertebale D7); lesione cuffia dei rotatori destra- Disturbo dell’equilibrio e della marcia con cadute ricorrenti- Scompenso diastolico da cardiopatia ipertensiva e valvolare (stenosi aortica moderata e steno-insufficienza mitralica lieve)- Gastroduodenite cronica; malattia diverticolare del colon; emorroidi II grado- Anemia lieve a genesi mista (perdita e disordine cronico)- Insufficienza renale cronica lieve- Trombosi retinica con cecità destra (7/’07)
Caso clinico N.1 Maria D, 84 anni, Novembre 2007
Terapia: Furosemide 25mg Ramipril 2.5mgL-Dopa/Carbidopa 250mg x3 Rivastigmina 3mg x2ASA 100mg Sertralina 50mgTrazodone 10mg x3 Lorazepam 1mgLansoprazolo 15mg Risedronato 35mg/settCa-vit.D
MMSE 22/30Barthel index 30/100Tinetti’s scale 7/28
Caduta accidentale nel tentativo di depositare un piatto in un armadio della cucina
⇒ Frattura pertrocanterica femore destro (osteosintesi con chiodo gamma)
⇒ Istituzionalizzazione (MMSE 22/30, BI 23/100, Tinetti 4/28)
Caso clinico N.2 Virgilio P, 78 anni, Luglio 2007
Vive al proprio domicilio con la moglie.
Anamnesi:- Ipertensione arteriosa sistemicaTerapia: Ramipril+Idroclortiazide 5+12.5mg
MMSE 30/30Barthel index 100/100Tinetti’s scale 28/28
Caso clinico N.2 Virgilio P, 78 anni, Luglio 2007
Caduta mentre pattinava su strada a causa di terreno accidentato
⇒ Trauma cranico lieve (GCS 15), ⇒ Ferite lacero-contuse al mento e in
sede frontale⇒ Frattura scomposta del condilo
mandibolare sinistro
⇒ Ritorno a domicilio(MMSE 30/30, BI 100/100, Tinetti 28/28)
Caso clinico N.3 Fausto P, 80 anni, Febbraio 2008
Vive solo al proprio domicilio.Anamnesi:- Carcinoma prostatico (trattato con radioterapia, in attuale follow-up: non riattivazione di malattia) - Diabete mellito tipo 2- Ipertensione arteriosa sistemica- Sincope con trauma cranico lieve (12/’07)
Terapia: Doxazosina 2mg Glibenclamide 2.5mg x2
MMSE 27/30Barthel index 100/100Tinetti’s scale 25/28
Caso clinico N.3 Fausto P, 80 anni, Febbraio 2008
Caduta secondaria a sincope verosimilmente da ipotensione ortostatica(mentre si alzava dalla sedia dopo pranzo)
⇒ Trauma cranico lieve ⇒ Ferita lacero-contusa fronto-parietale⇒ Durante i primi minuti di osservazione in PS, arresto cardio-
respiratorio, risoltosi con RCP⇒ Alla ripresa dello stato di coscienza, riscontro di tetraparesi
flaccida AAII, deficit di sensibilità tattile-dolorifica a livello di T1⇒ Frattura-lussazione di C3-C4 (non indicazione NCH)
⇒ Trasferimento in Reparto riabilitativo(MMSE 27/30, BI 0/100, Tinetti 0/28, tracheostomizzato,
parziale recupero mobilità spontanea arto inferiore sinistro)
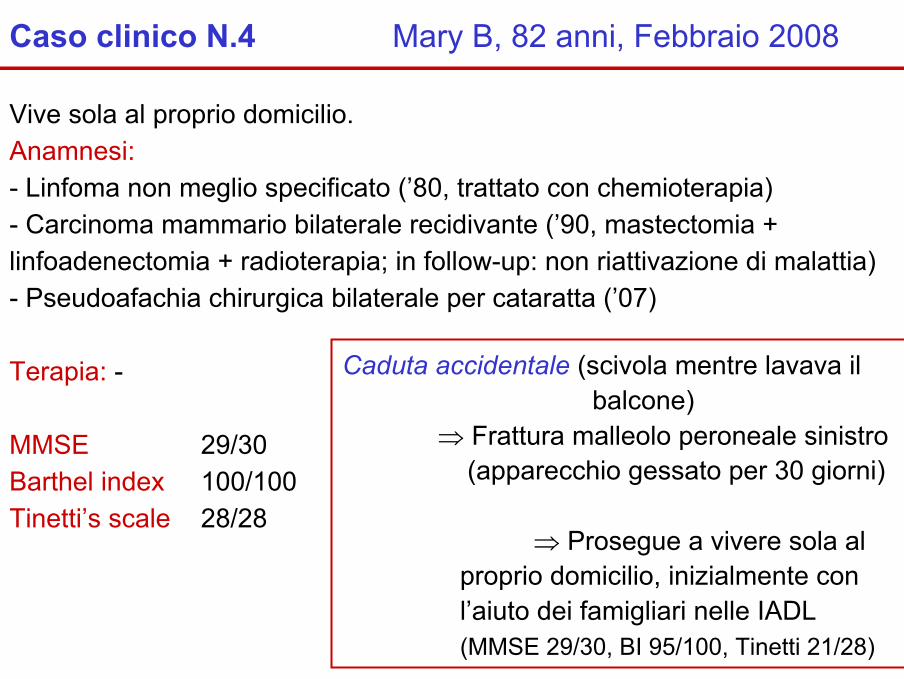
Caso clinico N.4 Mary B, 82 anni, Febbraio 2008
Vive sola al proprio domicilio.Anamnesi:- Linfoma non meglio specificato (’80, trattato con chemioterapia)- Carcinoma mammario bilaterale recidivante (’90, mastectomia + linfoadenectomia + radioterapia; in follow-up: non riattivazione di malattia)- Pseudoafachia chirurgica bilaterale per cataratta (’07)
Terapia: -
MMSE 29/30Barthel index 100/100Tinetti’s scale 28/28
Caduta accidentale (scivola mentre lavava il balcone)
⇒ Frattura malleolo peroneale sinistro (apparecchio gessato per 30 giorni)
⇒ Prosegue a vivere sola al proprio domicilio, inizialmente con l’aiuto dei famigliari nelle IADL(MMSE 29/30, BI 95/100, Tinetti 21/28)
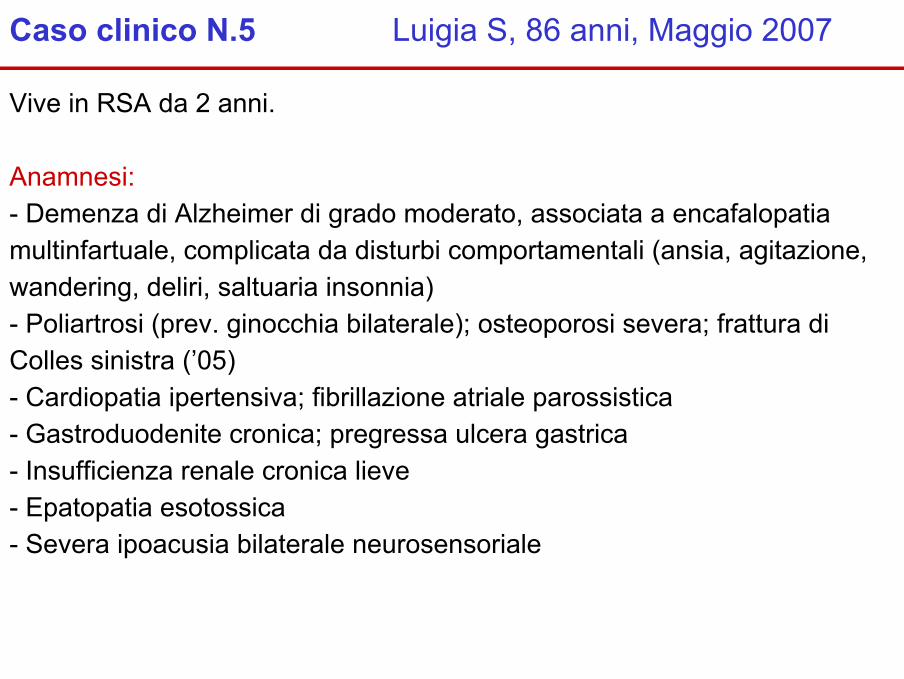
Caso clinico N.5 Luigia S, 86 anni, Maggio 2007
Vive in RSA da 2 anni.
Anamnesi:- Demenza di Alzheimer di grado moderato, associata a encafalopatiamultinfartuale, complicata da disturbi comportamentali (ansia, agitazione, wandering, deliri, saltuaria insonnia) - Poliartrosi (prev. ginocchia bilaterale); osteoporosi severa; frattura di Colles sinistra (’05)- Cardiopatia ipertensiva; fibrillazione atriale parossistica - Gastroduodenite cronica; pregressa ulcera gastrica- Insufficienza renale cronica lieve- Epatopatia esotossica- Severa ipoacusia bilaterale neurosensoriale
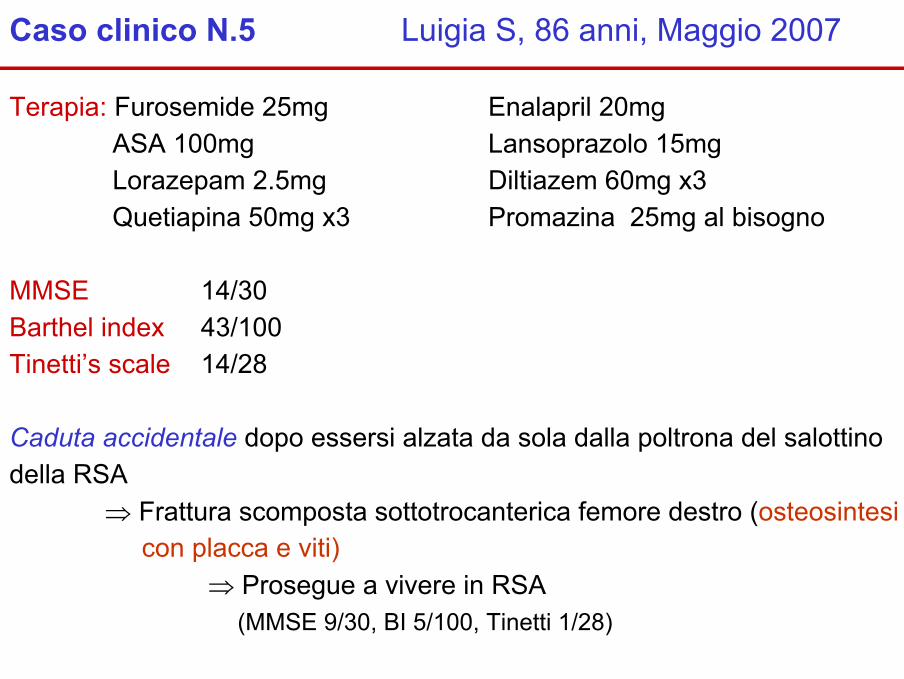
Caso clinico N.5 Luigia S, 86 anni, Maggio 2007
Terapia: Furosemide 25mg Enalapril 20mgASA 100mg Lansoprazolo 15mgLorazepam 2.5mg Diltiazem 60mg x3Quetiapina 50mg x3 Promazina 25mg al bisogno
MMSE 14/30Barthel index 43/100Tinetti’s scale 14/28
Caduta accidentale dopo essersi alzata da sola dalla poltrona del salottino della RSA
⇒ Frattura scomposta sottotrocanterica femore destro (osteosintesicon placca e viti)
⇒ Prosegue a vivere in RSA (MMSE 9/30, BI 5/100, Tinetti 1/28)
Fattori correlati alle cadute e al loro esito:- stato funzionale pre-morboso- comorbilità- stato cognitivo- dinamica dell’evento- il caso
Sintesi casi clinici
Tutte le cadute sono sindromi geriatriche?
ovvero
Di quali cadute si deve occupare il geriatra?