Embed Size (px)
Citation preview
391
Editorial
Le point sur les fenteslabio-alvéolo-palatines
On cleft lipsand cleft palates
Jean-Jacques AKNIN
En cette fin d’année, nous avons le plai-sir d’accueillir Jean-Jacques Aknin. Chefdu département d’Orthopédie Dento-Faciale de la Faculté d’Odontologie deLyon, il est Praticien Hospitalier, et respon-sable de l’Unité Fonctionnelle d’Ortho-pédie Dento-Faciale du Service d’Odon-tologie des Hospices Civils de Lyon.
Eminent membre de l’Association de laRevue d’ODF et nouveau Président de laSFODF, il a rédigé son éditorial sous laforme d’un court article. Il nous offre unesynthèse des réponses à une question d’ac-tualité trop peu connue des praticiens spé-cialisés qui exercent hors des Centreshospitaliers ou hospitalo-universitaires,bien souvent parce que les patients présen-tant des FLAP ne leur sont pas adressés etrestent dans le circuit où ils avaient étéorientés, à l’origine.
Philippe Amat
Les enfants porteurs de fentes palatinessont souvent obligés de parcourir de nom-breux kilomètres pour recevoir leurs soinsorthodontiques. Il serait donc nécessaireque plus de praticiens reçoivent une forma-tion spécialisée dans ces types de traite-ments. Lorsque plus d’orthodontistes serontformés au traitement des FLAP, les patients
As we approach the end of another yearwe have the great pleasure of welcomingJean-Jacques Aknin. He is the Director of theDepartment of Dento-Facial Orthopedics inthe Faculty of Odontology of Lyon and aHospital Practitioner responsible for theFunctional Unit of Dento-Facial Ortho-pedics in the Service of Odontology of theCivil Hospices of Lyons. An eminent mem-ber of the ‘Association of the Revue of theODF and the new President of the SFODF,he has prepared his initial editorial in theform of a short article in which he presentsa synthesis of the responses to a questionthat is important but little known to practi-tioners who do not work in hospital or uni-versity settings, primarily because patientswho suffer from cleft lips and cleft palatesdo not ordinarily consult private practitio-ners, remaining instead under the care ofhospital and university services.
Philippe Amat
Children who suffer from clefts oflips, alveoli, and hard and soft palates,phenomena that occur once in every700 births, are often obliged to travelgreat distances to receive orthodontictreatment. It would seem advisable,accordingly, that more orthodontists betrained in this special area so that
DOI:10.1051/odf:2008045
Adressede correspondance :
J.-J. AKNIN,Facultéd’Odontologie de Lyon,11, rue GuillaumeParadin,69372 Lyon Cedex 08.E-mail : [email protected]
Aknin JJ. Le point sur les fentes labio-alvéolo-palatines. Rev Orthop Dento Faciale 2008;42:391-402.
2-Editorial 4-2008 391-402 02/12/08 12:41 Page 391
Article disponible sur le site http://odf.edpsciences.org ou http://dx.doi.org/10.1051/odf:2008045
Rev Orthop Dento Faciale 42 : 391-402, 2008392
pourront plus facilement consulter l’orthodon-tiste proche de chez eux.
En termes de prévalence, les fenteslabiales, alvéolaires, palatines et vélairesaffectent environ un enfant sur 700 naissances.Longtemps perçues comme des malformationsgraves, lourdes de séquelles, l’avenir des por-teurs de fentes est désormais grandement amé-lioré par les progrès des étapes et techniqueschirurgicales mais aussi par la pluridisciplina-rité de la thérapeutique des fentes.
patients with clefts could receive careat facilities located nearer to theirhomes. Perceived for many years asserious deformities with grave conse-quences, cleft palates can now be treatedwith remarkable facility and successthanks to new procedures and surgicaltechniques and also because of the effi-cacy of the multi-disciplinary thera-peutic approach that has become increa-singly utilized.
J.-J. AKNIN
1 - EMBRYOLOGIE 1 - EMBRYOLOGY
La fusion des bourgeons faciaux est à l’ori-gine de la configuration future de la face.
1 - 1 - Formationdu Palais primaire
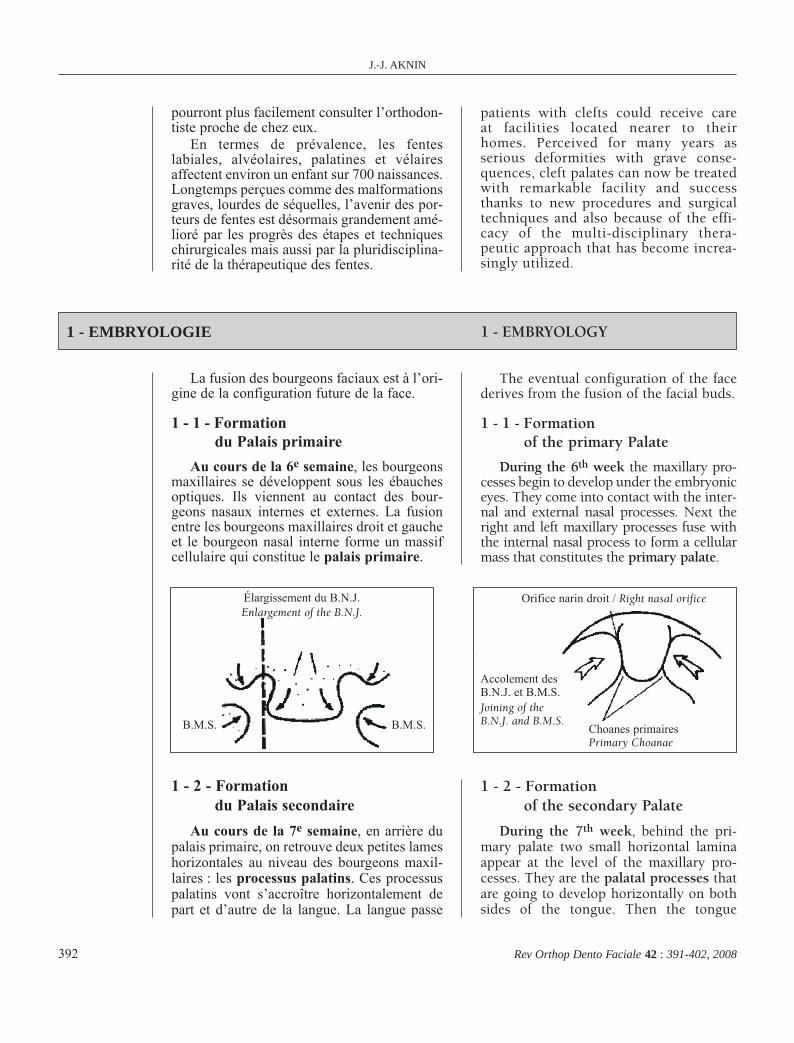
Au cours de la 6e semaine, les bourgeonsmaxillaires se développent sous les ébauchesoptiques. Ils viennent au contact des bour-geons nasaux internes et externes. La fusionentre les bourgeons maxillaires droit et gaucheet le bourgeon nasal interne forme un massifcellulaire qui constitue le palais primaire.
The eventual configuration of the facederives from the fusion of the facial buds.
1 - 1 - Formationof the primary Palate
During the 6th week the maxillary pro-cesses begin to develop under the embryoniceyes. They come into contact with the inter-nal and external nasal processes. Next theright and left maxillary processes fuse withthe internal nasal process to form a cellularmass that constitutes the primary palate.
1 - 2 - Formationdu Palais secondaire
Au cours de la 7e semaine, en arrière dupalais primaire, on retrouve deux petites lameshorizontales au niveau des bourgeons maxil-laires : les processus palatins. Ces processuspalatins vont s’accroître horizontalement depart et d’autre de la langue. La langue passe
1 - 2 - Formationof the secondary Palate
During the 7th week, behind the pri-mary palate two small horizontal laminaappear at the level of the maxillary pro-cesses. They are the palatal processes thatare going to develop horizontally on bothsides of the tongue. Then the tongue
Élargissement du B.N.J.Enlargement of the B.N.J.
B.M.S. B.M.S.
Accolement desB.N.J. et B.M.S.Joining of theB.N.J. and B.M.S.
Orifice narin droit / Right nasal orifice
Choanes primairesPrimary Choanae
2-Editorial 4-2008 391-402 02/12/08 12:41 Page 392
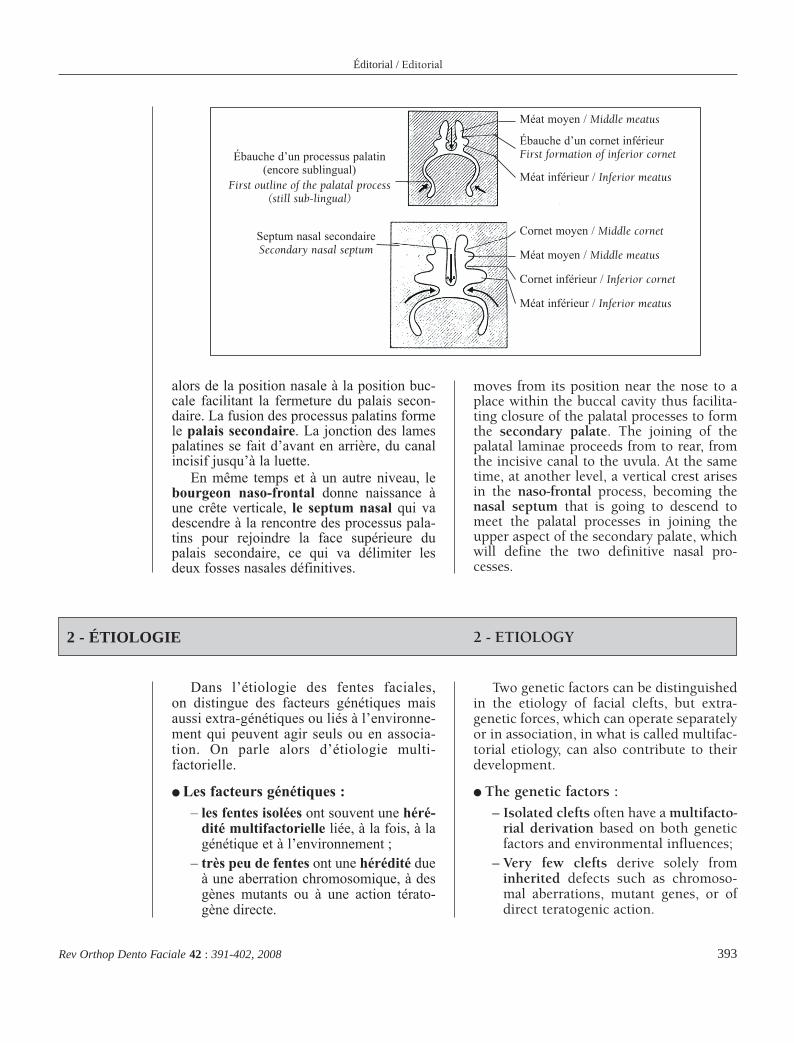
alors de la position nasale à la position buc-cale facilitant la fermeture du palais secon-daire. La fusion des processus palatins formele palais secondaire. La jonction des lamespalatines se fait d’avant en arrière, du canalincisif jusqu’à la luette.
En même temps et à un autre niveau, lebourgeon naso-frontal donne naissance àune crête verticale, le septum nasal qui vadescendre à la rencontre des processus pala-tins pour rejoindre la face supérieure dupalais secondaire, ce qui va délimiter lesdeux fosses nasales définitives.
Éditorial / Editorial
393Rev Orthop Dento Faciale 42 : 391-402, 2008
moves from its position near the nose to aplace within the buccal cavity thus facilita-ting closure of the palatal processes to formthe secondary palate. The joining of thepalatal laminae proceeds from to rear, fromthe incisive canal to the uvula. At the sametime, at another level, a vertical crest arisesin the naso-frontal process, becoming thenasal septum that is going to descend tomeet the palatal processes in joining theupper aspect of the secondary palate, whichwill define the two definitive nasal pro-cesses.
2 - ÉTIOLOGIE 2 - ETIOLOGY
Dans l’étiologie des fentes faciales,on distingue des facteurs génétiques maisaussi extra-génétiques ou liés à l’environne-ment qui peuvent agir seuls ou en associa-tion. On parle alors d’étiologie multi-factorielle.
● Les facteurs génétiques :– les fentes isolées ont souvent une héré-
dité multifactorielle liée, à la fois, à lagénétique et à l’environnement ;
– très peu de fentes ont une hérédité dueà une aberration chromosomique, à desgènes mutants ou à une action térato-gène directe.
Two genetic factors can be distinguishedin the etiology of facial clefts, but extra-genetic forces, which can operate separatelyor in association, in what is called multifac-torial etiology, can also contribute to theirdevelopment.
● The genetic factors :
– Isolated clefts often have a multifacto-rial derivation based on both geneticfactors and environmental influences;
– Very few clefts derive solely frominherited defects such as chromoso-mal aberrations, mutant genes, or ofdirect teratogenic action.
Ébauche d’un processus palatin(encore sublingual)
First outline of the palatal process(still sub-lingual)
Méat moyen / Middle meatus
Ébauche d’un cornet inférieurFirst formation of inferior cornet
Méat inférieur / Inferior meatus
Cornet moyen / Middle cornet
Méat moyen / Middle meatus
Cornet inférieur / Inferior cornet
Méat inférieur / Inferior meatus
Septum nasal secondaireSecondary nasal septum
2-Editorial 4-2008 391-402 02/12/08 12:41 Page 393
J.-J. AKNIN
394 Rev Orthop Dento Faciale 42 : 391-402, 2008
Palais primairePrimary palate
Processus palatinPalatal process
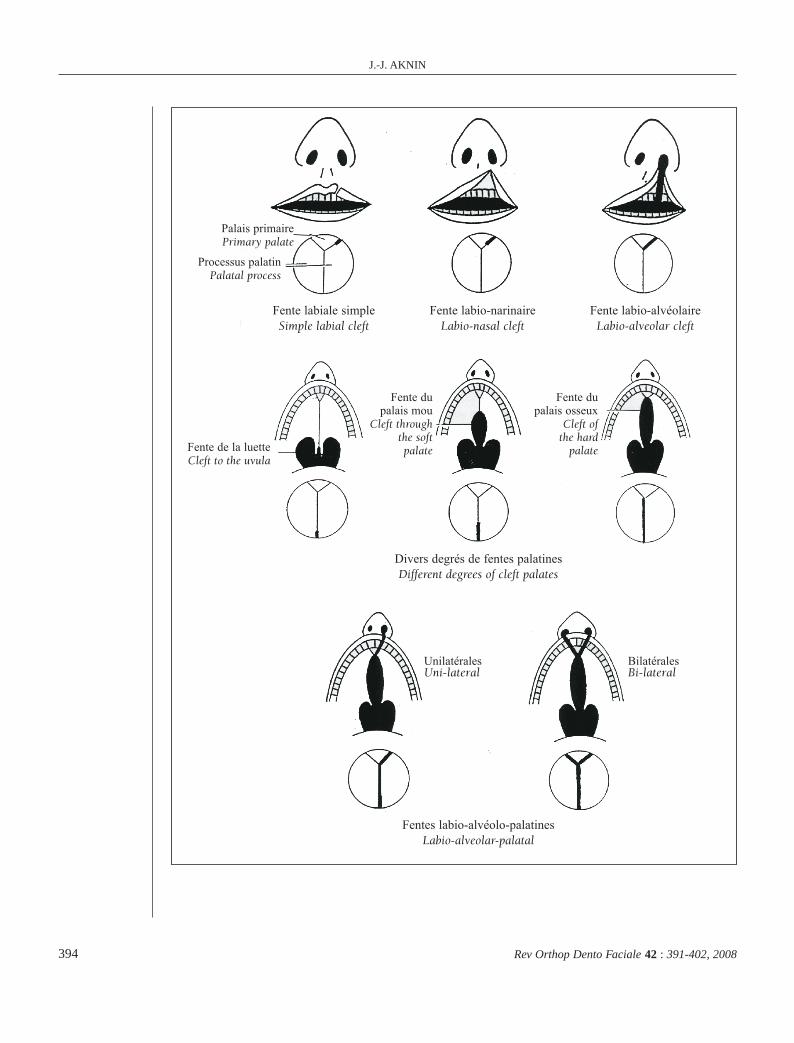
Fente labiale simpleSimple labial cleft
Divers degrés de fentes palatinesDifferent degrees of cleft palates
Fentes labio-alvéolo-palatinesLabio-alveolar-palatal
Fente labio-narinaireLabio-nasal cleft
Fente labio-alvéolaireLabio-alveolar cleft
Fente de la luetteCleft to the uvula
Fente dupalais mou
Cleft throughthe softpalate
Fente dupalais osseux
Cleft ofthe hard
palate
UnilatéralesUni-lateral
BilatéralesBi-lateral
2-Editorial 4-2008 391-402 02/12/08 12:41 Page 394
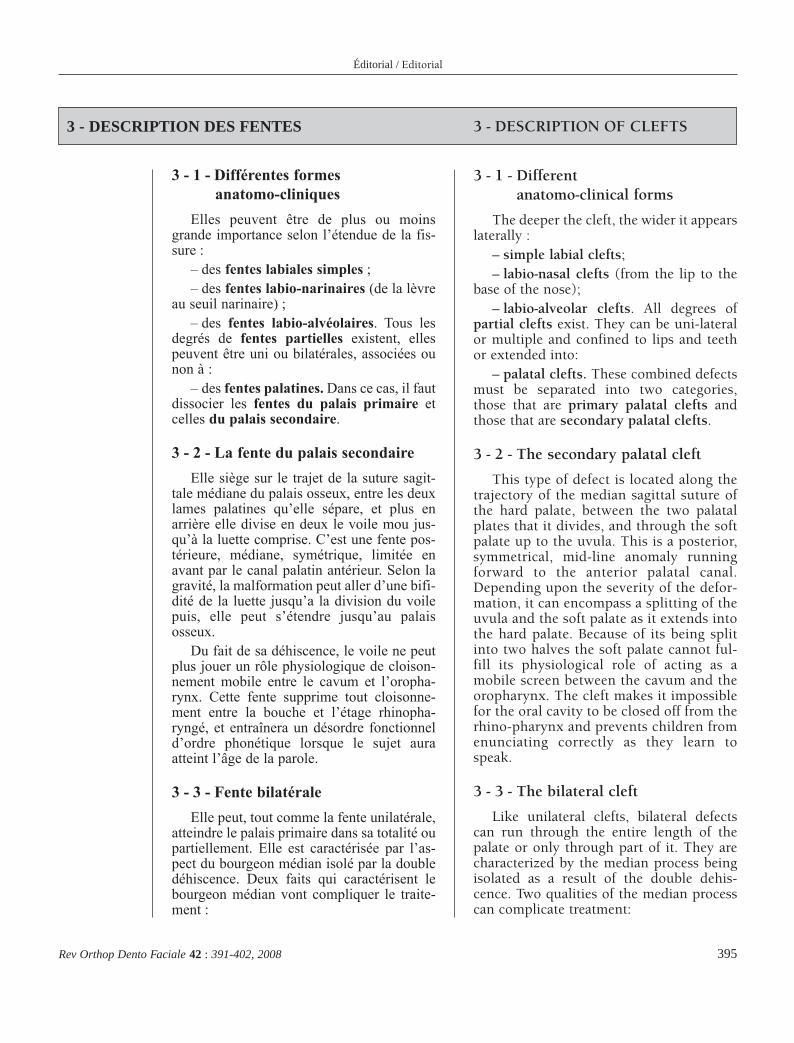
3 - 1 - Différentes formesanatomo-cliniques
Elles peuvent être de plus ou moinsgrande importance selon l’étendue de la fis-sure :
– des fentes labiales simples ;– des fentes labio-narinaires (de la lèvre
au seuil narinaire) ;– des fentes labio-alvéolaires. Tous les
degrés de fentes partielles existent, ellespeuvent être uni ou bilatérales, associées ounon à :
– des fentes palatines. Dans ce cas, il fautdissocier les fentes du palais primaire etcelles du palais secondaire.
3 - 2 - La fente du palais secondaire
Elle siège sur le trajet de la suture sagit-tale médiane du palais osseux, entre les deuxlames palatines qu’elle sépare, et plus enarrière elle divise en deux le voile mou jus-qu’à la luette comprise. C’est une fente pos-térieure, médiane, symétrique, limitée enavant par le canal palatin antérieur. Selon lagravité, la malformation peut aller d’une bifi-dité de la luette jusqu’a la division du voilepuis, elle peut s’étendre jusqu’au palaisosseux.
Du fait de sa déhiscence, le voile ne peutplus jouer un rôle physiologique de cloison-nement mobile entre le cavum et l’oropha-rynx. Cette fente supprime tout cloisonne-ment entre la bouche et l’étage rhinopha-ryngé, et entraînera un désordre fonctionneld’ordre phonétique lorsque le sujet auraatteint l’âge de la parole.
3 - 3 - Fente bilatérale
Elle peut, tout comme la fente unilatérale,atteindre le palais primaire dans sa totalité oupartiellement. Elle est caractérisée par l’as-pect du bourgeon médian isolé par la doubledéhiscence. Deux faits qui caractérisent lebourgeon médian vont compliquer le traite-ment :
Éditorial / Editorial
395Rev Orthop Dento Faciale 42 : 391-402, 2008
3 - 1 - Differentanatomo-clinical forms
The deeper the cleft, the wider it appearslaterally :
– simple labial clefts;– labio-nasal clefts (from the lip to the
base of the nose);– labio-alveolar clefts. All degrees of
partial clefts exist. They can be uni-lateralor multiple and confined to lips and teethor extended into:
– palatal clefts. These combined defectsmust be separated into two categories,those that are primary palatal clefts andthose that are secondary palatal clefts.
3 - 2 - The secondary palatal cleft
This type of defect is located along thetrajectory of the median sagittal suture ofthe hard palate, between the two palatalplates that it divides, and through the softpalate up to the uvula. This is a posterior,symmetrical, mid-line anomaly runningforward to the anterior palatal canal.Depending upon the severity of the defor-mation, it can encompass a splitting of theuvula and the soft palate as it extends intothe hard palate. Because of its being splitinto two halves the soft palate cannot ful-fill its physiological role of acting as amobile screen between the cavum and theoropharynx. The cleft makes it impossiblefor the oral cavity to be closed off from therhino-pharynx and prevents children fromenunciating correctly as they learn tospeak.
3 - 3 - The bilateral cleft
Like unilateral clefts, bilateral defectscan run through the entire length of thepalate or only through part of it. They arecharacterized by the median process beingisolated as a result of the double dehis-cence. Two qualities of the median processcan complicate treatment:
3 - DESCRIPTION DES FENTES 3 - DESCRIPTION OF CLEFTS
2-Editorial 4-2008 391-402 02/12/08 12:41 Page 395
– il est très hypoplasié ;– l’orientation normale de l’ensemble du
bourgeon médian est fortement perturbée, lebourgeon peut être basculé jusqu’a 45° versl’avant.
3 - 4 - Croissance des tissus mous
Le profil cutané est le reflet du profilsquelettique sous-jacent. Ainsi les enfantsporteurs de fente faciale seront affectésd’une dysharmonie du profit cutané, dueaux déformations squelettiques initiales,aux déficits tissulaires variables selon lespatients et aux séquelles des interventionschirurgicales.
J.-J. AKNIN
396 Rev Orthop Dento Faciale 42 : 391-402, 2008
– it is very hypoplastic;– the normal orientation of the totality
of the median process having beenseriously disturbed, it may be tilted forwardas much as 45°.
3 - 4 - Growth of soft tissues
The exterior, cutaneous appearance ofcleft palate patients reflects the underlyingskeletal status. Accordingly, children withfacial clefts will have malformed profilesbecause of the basic initial deformity andthe subsequent soft tissue defects that willvary in response to the types of surgicaltreatment they have received.
4 - LES ANOMALIES DENTAIRES 4 - ASSOCIATED DENTAL ANOMALIES
4 - 1 - Anomalies de nombre
● Les agénésies des incisives latéralessont fréquentes :
– du côté de la fente dans 40 % des cas endenture permanente, et 27 % en denture tem-poraire ;
– du côté sain dans 11 % des cas.
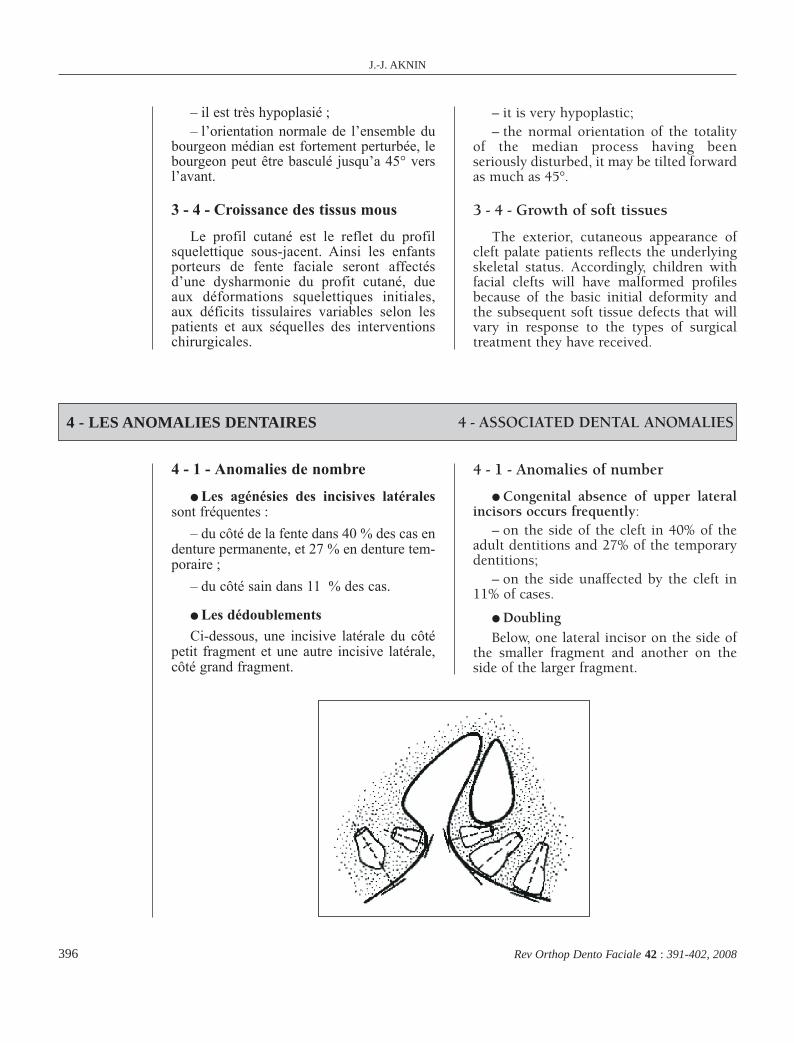
● Les dédoublements
Ci-dessous, une incisive latérale du côtépetit fragment et une autre incisive latérale,côté grand fragment.
4 - 1 - Anomalies of number
● Congenital absence of upper lateralincisors occurs frequently:
– on the side of the cleft in 40% of theadult dentitions and 27% of the temporarydentitions;
– on the side unaffected by the cleft in11% of cases.
● DoublingBelow, one lateral incisor on the side of
the smaller fragment and another on theside of the larger fragment.
2-Editorial 4-2008 391-402 02/12/08 12:41 Page 396
Ils concernent les incisives latérales ducoté de la fente, dans 22 % des cas en den-ture permanente, et 42,5 % en denture tem-poraire. On retrouve alors une incisivelatérale sur chacune des deux berges de lafente.
4 - 2 - Anomalies de positionLe mauvais agencement des germes den-
taires est dû à la désorganisation des basesosseuses, elle-même due à la non fusion desbourgeons embryonnaires.
4 - 3 - Anomalies de formeLa dent la plus touchée est l’incisive
latérale, elle présente alors un aspect rizi-forme.
Éditorial / Editorial
397Rev Orthop Dento Faciale 42 : 391-402, 2008
Doubling affects lateral incisors on theside of the cleft in 22% of the cases in thepermanent dentition and in 42,5% of tempo-rary dentitions. In these cases lateral incisorsappear on each of the two sides of the cleft.
4 - 2 - Anomalies of position
The poor arrangement of tooth budsresults from a disorganization of basal bone,itself a victim of failure of embryonic seg-ments to fuse properly.
4 - 3 - Anomalies of form
The tooth most often malformed is thelateral incisor which presents a riziform orpeg-shaped appearance or be absent enti-rely.
5 - LES RAPPORTS D’OCCLUSION 5 - OCCLUSAL RELATIONSHIPS
● Sens sagittal : la rétrusion maxil-laire et la fausse promandibulie fré-quentes dans les fentes congénitalesnous dévoilent une classe III squeletti-que avec une dysharmonie dento-alvéo-laire n’apparaissant qu’au maxillairepuisque la mandibule ne subit pas de mal-formation.
● Sens transversal : une endomaxilliepeut être ou non accompagnée d’uneendoalvéolie maxillaire. Les points inter-incisifs sont déviés. On notera l’impor-tance du décalage entre le grand et le petitfragment maxillaire basculé du côtéinterne, celui-ci entravant considérable-ment l’alignement dentaire, et l’occlu-sion.
● In the sagittal sense: The maxillaryretrusion and the pseudo mandibular protru-sion in congenital cleft palate cases reflect anunderlying Class III skeletal condition withan arch length discrepancy in the maxilla anda mandible unaffected by malformation.
● In the transverse sense: a retrudedmaxilla may or may not be accompanied bya retrusion of the alveolar process. Theupper mid-line is deviated. A small sizedmaxilla may or may not be accompanied byan alveolar process reduced in bulk. Theincisal mid-line is deviated. The difference insize between the large and the small maxil-lary fragment, which is tilted toward themedian, is marked. The mal-position of thissmaller portion causes major deviations intooth alignment and occlusal relationships.
6 - L’AUDITION ET LA PHONATION 6 - HEARING AND SPEECH
L’audition est perturbée dans 75 %des cas du fait de l’entrée d’air dansl’oreille moyenne entraînant une modifi-cation de la ventilation et des pressionstympaniques.
The hearing of cleft palate patients isadversely affected in 75 % of the casesbecause of the intrusion of air into themiddle ear, which modifies breathing capa-city and tympanic pressures.
2-Editorial 4-2008 391-402 02/12/08 12:41 Page 397
6 - 1 - Le bilan phonétiqueDu fait de la communication bucco-
nasale, on observe une fuite d’air facilementdécelable. Les causes de l’insuffisance fonc-tionnelle du voile entraînant une déperditionnasale sont : un voile divisé, un voile tropcourt, un voile inerte. Dans les trois cas, unphénomène compensatoire peut se mettre enplace. Si ce phénomène compensatoire faitdéfaut, il faudra placer un obturateur.
J.-J. AKNIN
398 Rev Orthop Dento Faciale 42 : 391-402, 2008
6 - 1 - Impact on patients’ phonics
Because of the open communication bet-ween the oral and nasal cavities, air canescape readily. The types of soft palateinsufficiency leading to loss of function are:divided palate, excessively short palate, andinert palate. In all three instances, compen-satory functioning may be established, butif that does not occur, dentists should pro-vide patients with obturators.
7 - LE TRAITEMENT CHIRURGICAL INITIAL 7 - INITIAL SURGICAL TREATMENT
Ainsi, il est important de souligner laprise en charge multidisciplinaire despatients, de leur plus jeune âge jusqu’à l’âge adulte.
7 - 1 - Le calendrier opératoireIl varie selon les écoles mais pour simpli-
fier cet éditorial nous pouvons présentercelui de Psaume et Maleck qui est adopté etmis à jour par l’équipe Lyonnaise de la cli-nique du Val d’Ouest :
● Fentes labio-alvéolaires isoléesLèvre + narine : 2 mois (+ conformateur
narinaire).
● Fentes labio-palatines unilatéralestotales
Véloplastie : 3 mois (staphyloraphie).Lèvre + narine + palais osseux (Urano-
plastie) : 5 mois (+ conformateur narinaire).Pharyngoplastie avant 6 ans (avant l’en-
trée au CP).
● Fentes labio-palatines bilatéralestotales
Obturateur néo-natal souple : 3 mois.Véloplastie : 3 mois.1er côté de la lèvre, palais osseux, nez : 5
mois.2e côté de la lèvre : 7 mois.
● Fentes vélo-palatinesFentes qui ne concernent que le voile :
3 mois.Voile + Palais : en deux temps : 3 mois et
5 mois.
It is important to emphasize that amulti-disciplinary team should take chargeof the patent’s treatment from the earliestpossible age until adulthood.
7 - 1 - The operatory timetable
Schedules vary from one dental depart-ment to another, but to keep this presenta-tion uncomplicated we shall offer Psaumeand Maleck technique that the team fromLyons is using the clinic Val d’Ouest:
● Isolated labio-alveolar cleft
Lip + nose: 2 months (+ nasal conforma-tor).
● Total unilateral labio-palatal clefts
Soft palate correction: 3 months (sta-phyloraphy).
Lip + nose+ hard palate (Uranoplasty):5 months (+ nasal conformator).
Pharyngoplasty before 6 years (beforebeginning kindergarten).
● Total bilateral labio-palatal clefts
Soft neo-natal obturator: 3 months.Veloplasty: 3 months.1st on the side of the lip, hard palate,
nose: 5 months.2nd on the side of the lip: 7 months.
● Soft palate-hard palate clefts
Clefts affecting only the soft palate:3months.
Soft palate + Hard palate: in two stages:3 months and 5 months.
2-Editorial 4-2008 391-402 02/12/08 12:41 Page 398
Il peut commencer en denture tempo-raire afin d’établir au plus tôt une fonctionéquilibrée pour une croissance et un déve-loppement harmonieux :
– dans le sens transversal, une expan-sion maxillaire permet de corrigerl’endomaxillie. L’appareil de choix est le«Quad Helix» ;
– dans le sens sagittal, la rétromaxilliepeut être corrigée par des tractions extra-orales (masque de Delaire) qui permettentde compenser les défauts de croissanceosseuse afin de réduire la classe III sque-lettique. Une mécanique de classe III rem-place avantageusement le masque deDelaire anciennement préconisé.
Éditorial / Editorial
399Rev Orthop Dento Faciale 42 : 391-402, 2008
Orthodontists can begin treating cleftpalate patients with orthopedic deviceswhen they are still in the temporary denti-tion stage to establish functional equili-brium as soon as possible so as to encourageharmonious growth and development offacial structures.
– In the transverse sense the appliance ofchoice is a Quad Helix to expand the constrai-ned maxilla toward normal dimensions.
– In the sagittal sense use of the mask ofDelaire can be used to compensate for skeletaldefects by moving the maxilla forward whileholding back mandibular growth. TraditionalClass III mechanics can supplement thisextra-oral force.
8 - LE TRAITEMENT ORTHOPÉDIQUE (ODF) 8 - ORTHOPEDIC TREATMENT
9 - LE TRAITEMENT ORTHODONTIQUE 9 - ORTHODONTIC TREATMENT
En denture mixte, les objectifs du trai-tement sont les suivants :
– contenir les fragments osseux dis-joints ;
– corriger les malpositions incisives ;toujours garder l’espace de l’incisive laté-rale (elle sera le plus souvent remplacée parun implant en fin de croissance et aprèsgreffe osseuse initiale) ;
– mettre en occlusion normale les pré-molaires et les canines ;
– restituer une courbe d’arcade normaleau maxillaire ;
– corriger les inversions de l’articulédentaire.
Après cette étape de traitement en den-ture mixte, une plaque palatine de conten-tion maintient les résultats acquis.
● Le moment de la greffe varie : selonl’âge du sujet et de sa motivation, selonles stades d’éruption (souvent anar-chiques) et de maturation radiculaire, selonla position et les axes des germes den-taires.
In the mixed dentition, the objectives oftreatment are to:
– solidify disparate osseous fragments;– correct the malpositions of the incisors
while preserving space for the missing ordeformed lateral incisor, which will mostoften be replaced with an implant after pla-cement of an initial bone graft and the end ofthe growth period;
– restore the premolars and the canines tonormal occlusion;
– restore the maxillary arch to a normalcontour;
– correct any cross bite relationships.After this mixed dentition stage of treat-
ment, a palatal acrylic retainer can be used tomaintain the corrections.
● The time for a bone graft varies inaccordance with the age of patients and theirmotivation, according to the stage of erup-tion, which is often chaotic in cleft palatepatients, according to stage of root matura-tion, and according to the positions and longaxes of the unerupted permanent teeth.
2-Editorial 4-2008 391-402 02/12/08 12:41 Page 399
Le choix du moment de la greffeosseuse est un thème de recherche cli-nique actuel, il est variable selon leséquipes, il peut être réalisé, entre 8 anset 10 ans. Avant l’éruption de la canineou après l’éruption de la canine dans lepetit fragment vers l’âge de 12 ans endenture adolescente. Le dentoscan per-met de visualiser en 3D, le volume de lafente et sa localisation.
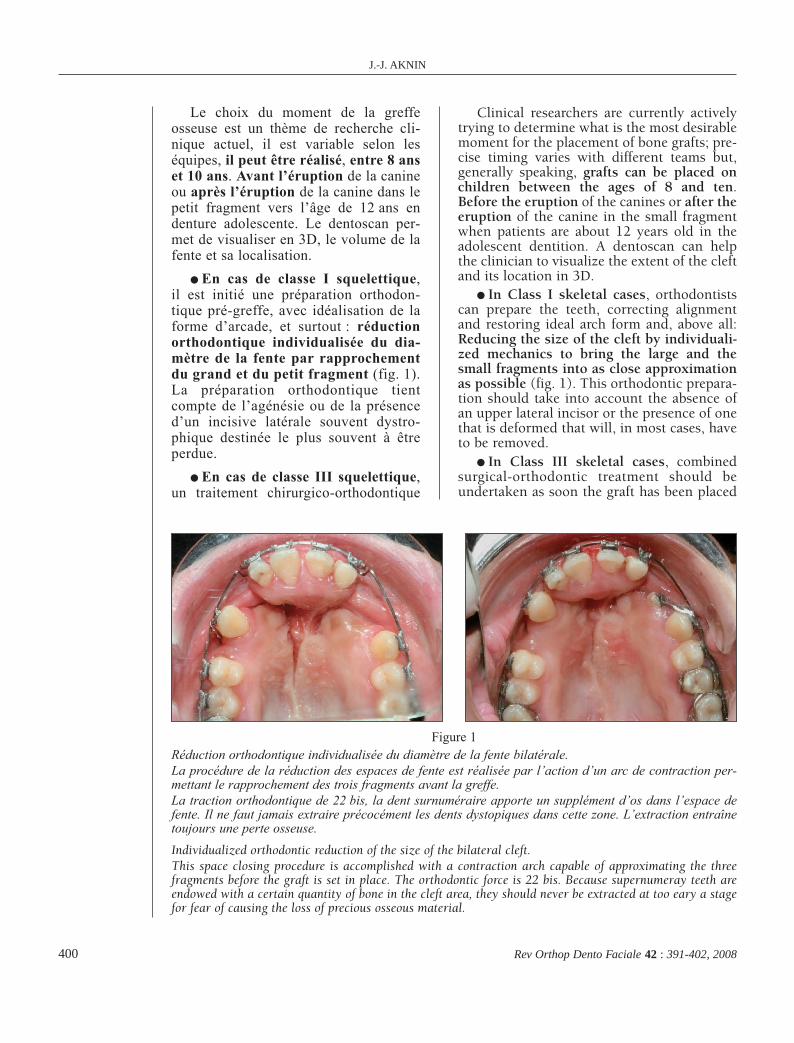
● En cas de classe I squelettique,il est initié une préparation orthodon-tique pré-greffe, avec idéalisation de laforme d’arcade, et surtout : réductionorthodontique individualisée du dia-mètre de la fente par rapprochementdu grand et du petit fragment (fig. 1).La préparation orthodontique tientcompte de l’agénésie ou de la présenced’un incisive latérale souvent dystro-phique destinée le plus souvent à êtreperdue.
● En cas de classe III squelettique,un traitement chirurgico-orthodontique
J.-J. AKNIN
400 Rev Orthop Dento Faciale 42 : 391-402, 2008
Clinical researchers are currently activelytrying to determine what is the most desirablemoment for the placement of bone grafts; pre-cise timing varies with different teams but,generally speaking, grafts can be placed onchildren between the ages of 8 and ten.Before the eruption of the canines or after theeruption of the canine in the small fragmentwhen patients are about 12 years old in theadolescent dentition. A dentoscan can helpthe clinician to visualize the extent of the cleftand its location in 3D.
● In Class I skeletal cases, orthodontistscan prepare the teeth, correcting alignmentand restoring ideal arch form and, above all:Reducing the size of the cleft by individuali-zed mechanics to bring the large and thesmall fragments into as close approximationas possible (fig. 1). This orthodontic prepara-tion should take into account the absence ofan upper lateral incisor or the presence of onethat is deformed that will, in most cases, haveto be removed.
● In Class III skeletal cases, combinedsurgical-orthodontic treatment should beundertaken as soon the graft has been placed
Figure 1Réduction orthodontique individualisée du diamètre de la fente bilatérale.La procédure de la réduction des espaces de fente est réalisée par l’action d’un arc de contraction per-mettant le rapprochement des trois fragments avant la greffe.La traction orthodontique de 22 bis, la dent surnuméraire apporte un supplément d’os dans l’espace defente. Il ne faut jamais extraire précocément les dents dystopiques dans cette zone. L’extraction entraînetoujours une perte osseuse.
Individualized orthodontic reduction of the size of the bilateral cleft.This space closing procedure is accomplished with a contraction arch capable of approximating the threefragments before the graft is set in place. The orthodontic force is 22 bis. Because supernumeray teeth areendowed with a certain quantity of bone in the cleft area, they should never be extracted at too eary a stagefor fear of causing the loss of precious osseous material.
2-Editorial 4-2008 391-402 02/12/08 12:41 Page 400
Le moment du traitement chirurgico-orthodontique des fentes a évolué par l’im-portance accordée maintenant aux praxiesdans la croissance faciale.
Les séquences thérapeutiques sontcomplexes et chaque protocole comportedes avantages et des inconvénients.
La difficulté de ces traitements résidedans le compromis à adopter, dans lequelselon Talmant : «il faut trouver le meilleuréquilibre possible entre la répartition ana-tomique la plus parfaite et la plus faiblerançon cicatricielle.»
La qualité des résultats sera influencéepar le le calendrier thérapeutique, et sur-tout par l’étroite coopération et la compré-hension réciproque du chirurgien et de
Éditorial / Editorial
401Rev Orthop Dento Faciale 42 : 391-402, 2008
The multi-disciplinary team evaluates theproper time for beginning surgical orthodon-tic treatment of clefts based on the interfe-rences the defect is exerting on normal facialgrowth.
The sequence of the therapeutic stages iscomplex; every variation in protocol has itsadvantages and disadvantages.
The difficulty in making treatment choicesderives from the compromises each requires,as explained by Talmant, “We must find thebest possible balance between the most per-fect anatomic restoration and the lowest pos-sible ransom paid in post-operative scarring.”
The therapeutic calendar, especially as it isaffected by the reciprocal understanding andcooperation of orthodontists and surgeons, willinfluence the quality of the results obtained.
10 - CONCLUSIONS
est envisagé (une fois la greffe réalisée etconsolidée).
Préparation orthodontique pré-greffe(si elle n’a pas déjà été faite), idéali-sation des formes d’arcades, réduc-tion orthodontique individualiséedu diamètre de la fente, greffe osseuse(14 ans). Correction orthodontique descompensations. Chirurgie orthogna-thique : Lefort 1 avancée et pharyngo-plastie à évaluer. Ceci est suivi d’unefinition orthodontique (six mois).(Veiller au parallélisme des axes dansla zone de l’implant qui remplaceral’incisive latérale absente). Puis d’unecontention fixée en attendant l’im-plant.
● La chirurgie de la lèvre ou du nez(septum nasal, en fin de croissance) peutintervenir une fois le rempart dento-alvéolaire reconstitué.
● La contention : par arc transpalatinsous peine de récidive de la correction dusens transversal. Cette contention estquasi-permanente.
and become well established. Orthodonticpreparatory treatment, if it has not alreadybeen completed, will have restoration of idealarch form as its goal.
Individualized orthodontic reduction ofthe cleft, Osseous graft, at the age of 14.
Individualized orthodontic reduction ofthe size of the cleft , Bone graft (14 years).Compensatory orthodontic corrective treat-ment, Orthognathic surgery: Lefort 1 advance-ment and need for pharyngoplasty to beevaluated. When these procedures are com-pleted, a six month fine detail orthodonticfinishing treatment should include root paral-leling in the implant zones where missinglateral incisors will have been replaced.Finally fixed retention is used until theimplant can be placed.
● Surgery of the lip or nose (septum nasal,at the end of the growth period) this can takeplace once the dento-alveolar rampart hasbeen reconstituted.
● Retention: unless a transpalatal arch isused there is always the risk of relapse of thepalatal expansion achieved. This fixed reten-tion has to be quasi-permanent.
2-Editorial 4-2008 391-402 02/12/08 12:41 Page 401
l’orthodontiste. Nous pouvons considérerqu’actuellement le traitement des fentespalatines a nettement progressé grâce, bienentendu, à l’amélioration certaine de laprise en charge chirurgicale mais surtoutgrâce à l’approche pluridisciplinaire chi-rurgien pédiatrique, chirurgien maxillo-facial, implantologiste, dentiste avec uneintervention de l’orthodontiste à tous lesstades du traitement. Le traitement estlourd mais efficace et apporte de bonsrésultats.
J.-J. AKNIN
402 Rev Orthop Dento Faciale 42 : 391-402, 2008
At the present time, we can safely assertthat the treatment of palatal clefts has greatlyimproved, thanks, of course, to definiteimprovement in surgical techniques, but also,in a more important global fashion, because ofthe increasingly effective multi-disciplinarycoordination of the efforts of pediatric sur-geons, maxillo-facial surgeons, implantolo-gists, general dentists, and the guidinginterventions of orthodontists at every stageof treatment, which is enormously demandingbut provides even more enormous dividendsfor the patients it serves.
La Revue d’O.D.F.à votre service sur Internet
www.revue-odf.org
2-Editorial 4-2008 391-402 02/12/08 12:41 Page 402





























