Embed Size (px)
Citation preview
87
Innovation in practice
Practice Development in Health Care, 2(2) 87–98, 2003 © Whurr Publishers Ltd
AbstractThe present article describes a project to establish an evidence-based council in a large acuteteaching hospital as a tool for promoting evidence-based practice. The council aimed to giveclinically active nurses ‘ownership’ of research questions and an opportunity to develop confi-dence in their evidence-based practice skills. The development and implementation of theproject are outlined and recommendations for encouraging capacity and the involvement ofnurses with regard to evidence-based practice are provided.
Key words: council, evidence-based practice, ownership, research
IntroductionBasing practice within the NHS on evidence of effectiveness and cost has become oneof the goals of the Department of Health (DoH 1995; DoH 1997). One of the methodsthrough which this goal is being implemented is evidence-based practice. This involvespractitioners identifying a problem, asking a research question, searching the researchliterature and then implementing changes on the basis of the evidence available(White 1997). The overall purpose of evidence-based practice is to provide effectivehealthcare within available limited resources (Colyer and Kamath 1999).
The difficulties of engaging nurses in research and evidence-based practicehave been well documented. Explanations cited for this are that research findings areseen to be of little relevance to nurses working in the clinical area (Burrows andMcLeish 1995) and that nurses lack the necessary skills (English 1994). The lack ofinterest and of skills are likely to be interrelated. Furthermore, the nursing profession
Learning fromexperience: promotingevidence-based practice
Simon Palfreyman—Research Nurse, Sheff ield Vascular Institute, Sheff ieldTeaching Hospitals NHS Trust, UK
Angela Tod—Practice Development Nurse, Cardiology Unit, Sheffield TeachingHospitals NHS Trust, UK
Jane Doyle—Practice Development Nurse and Ward Sister, Cardiology Unit,Sheffield Teaching Hospitals NHS Trust, UK
PDHC 2.2_3rd/crc 17/6/03 3:14 pm Page 87

has been slow to grasp the full implications and opportunities that the evidence-basedpractice agenda has wrought (Bonell 1999). Evidence-based practice allows nurses achance to measure ‘their unique contribution to patient health gain’ (French 1995). Aconsequence of not achieving this is that nursing may be ‘invisible’ to decision-makersin service organization and delivery (French 1997).
In order to fulfil its potential the nursing profession must overcome problemsrelated to nurses’ knowledge, workload, access to resources and power to implementresearch findings (Hunt 1981; le May et al 1998; Nolan et al. 1998; Upton 1999a). Thefrustrating fact is that these issues are not new. Recommendations were made morethan 30 years ago that nursing should be an evidence-based profession (DHSS 1972).
Nurses have been burdened with much historical baggage: the separation ofnursing into clinician, education and research camps (Rafferty et al. 1996); the lack ofclinically relevant research (Blanchard 1996); the limitation of nurses’ autonomy andlack of research skills (Upton 1999b); and insufficient time and resources (Nolan et al.1998).
One of the main justifications that nurses cite in their defence is that nursing isconcerned with feelings, perception and intuition, which may not lend themselves tobeing incorporated into evidence-based practice (Hicks and Hennessy 1997). Inaddition, some hierarchies of evidence (CRD 1996; Michaels and Booth 2001) tend toclass the methodologies used to explore these concepts as low-grade evidence.
Interventions to implement evidence-based practice need to be introduced in astructured fashion. The successful implementation of research into practice has beendescribed as a function of the relationship between the nature of the evidence, itscontext and the mechanism through which change is facilitated (Kitson et al. 1998).Further requirements for successful implementation of evidence-based practice are anorganizational infrastructure to co-ordinate and direct the process (Closs and Cheater1994; le May et al. 1998) and effective facilitation (Kitson et al. 1998).
One prerequisite to the introduction of evidence-based practice into nursing isa reduction in the heavy workload of clinical nurses (Upton 1999a). In addition, it isessential to convince nurses of the relevance of research to their clinical practice(English 1994). Practitioners are often urged to read journals and to use CD-ROMs,but the value of this without adequate training has to be questioned. Unless such skillsare acquired more widely within nursing there is a danger of removing researchquestions away from the clinical environment and into the province of specialists andacademics (Upton 1999b).
The picture is not all negative; nurses do seem to have a positive attitudetowards the concept of evidence-based practice—even if they are unable to commit theenergy or mobilize the skills necessary to overcome the major barriers to its adoption.Such barriers are often outside individual nurses’ sphere of influence and are related toinfrastructure and organization (Upton 1999a). The indication in the literature is thatnurses appreciate the need for, and potential benefits of, research and evidence-basedpractice (McSherry 1997; Upton 1999a). Current evidence suggests repeatedly that
88 Palfreyman et al.
PDHC 2.2_3rd/crc 17/6/03 3:14 pm Page 88
much failure to utilize research in practice has been attributed to nurses’ lack of confi-dence in their knowledge and skills related to research (Pearcey 1995). Alsoemphasized is the lack of time and accessibility of resources (Upton 1999a).
An alternative explanation for nurses not engaging in evidence-based practiceis that nurse researchers are not asking questions that are relevant to clinically activenurses (Upton 1999b).
The aim of the present project was to harness this positive attitude and toenable nurses to feel some ownership of evidence-based practice.
Project historyThe project was a product of discussions between the authors and a charge nurse whoworked in the Northern General Hospital, Sheffield. Three of these individuals weredelegates at the Royal College of Nursing research conference at Keele University inApril 1999. The general feeling was that there was a distinct lack of presentations atthe conference that were directly applicable to clinically active nurses.
From general discussions a solution began to emerge. One individual hadattended a presentation by Professor Gene Marsh, at the ‘Partnership into theMillennium’ conference (Marsh and Hopkins 1999), in which a project aiming toestablish an evidence-based council was described.
An outline proposal was developed by the authors, based on the presentationby Professor Marsh. In order to gauge support for the project, a series of open seminarswas held, to which all clinical staff with an interest in evidence-based practice wereinvited. The outline proposal was presented at the seminars and feedback requestedfrom attendees. The response to the project was overwhelmingly positive from thenurses working at the trust.
The proposal was submitted to the Foundation of Nursing Studies for funding.The endorsement of the Nursing Executive Group, consisting of nurse managers ofclinical departments, was also sought and obtained. The Nursing Executive Groupagreed in principle to allow members of the council time off from their clinical area toattend council meetings.
The project was successful in its application to the Foundation of NursingStudies and funding was obtained both to support the council and the education ofcouncil members. The Northern General Hospital, Sheffield, agreed to support thesecondment of a facilitator to assist with the co-ordination of the council.
Project planThe structures incorporated within the proposal were designed to aid the implemen-tation of evidence-based practice for nurses and allied health professionals by use of abottom-up approach. The plan was to establish a hospital-wide network of directorate-based journal clubs, to which nurses could bring research questions relevant to their
Learning from experience 89
PDHC 2.2_3rd/crc 17/6/03 3:14 pm Page 89

local areas and learn how to answer them. The journal clubs would be co-ordinated byan evidence-based council that would act as a resource and link between journal clubsfrom the different areas within the trust.
The plan was to establish a hospital-wide network of directorate-based journal clubs, to which nurses could bring researchquestions relevant to their local areas and learn how to answerthem.
The remit of the council was to increase the profile of evidence-based practicewithin the hospital and to co-ordinate local journal clubs. Membership consisted ofclinically active staff from each department within the trust. Initially, each councilmember underwent a short course on evidence-based practice, to improve their basicskills and understanding of research methods. Details of this course are given in asubsequent section.
By creating a forum for discussion for ward-based nurses, the council aimed toenable staff to compare and discuss relevant issues across department and directorateboundaries. In addition, it would permit dissemination of existing evidence and help togenerate priorities for future research activity that could be adopted by the trust.
Journal clubsJournal clubs provide a way of making a clear link between practice and research(Sheehan 1994; Kirchhoff and Beck 1995; Koziol-McLain and Tanabe 1996; le May1999) and have been recommended as a way of enhancing research awareness(McSherry 1997). They are also a method whereby individuals can keep up to datewith research (Upton 1999b), improve participants’ ability to critique research andmake changes in practice based on evidence (Koziol-McLain and Tanabe1996).Applying research to practice is about change and a journal club may allow staff toview such change as non-threatening and positive (Kettles 1997).
As a way of allowing two-way communication between the council and clini-cally based healthcare professionals, a network of journal clubs was established at localward or department level. Membership of the journal club aimed to be based on openaccess and was drawn from clinically active staff within each area. A condition ofassociation with the council was that members of the evidence-based council wereallocated time within the journal club to disseminate council information and activ-ities to journal club members. This time also provided an opportunity for concerns tobe identified within the journal clubs and for feedback to the evidence-based councilfor further discussions and action. Creating this dialogue between both forums allowedward-based research concerns to be discussed and prioritized at a hospital-wide level.
The creation of these two structures provided a framework to in whichpromote evidence-based practice within the trust. It was to foster an environment to
90 Palfreyman et al.
PDHC 2.2_3rd/crc 17/6/03 3:14 pm Page 90
bridge the theory–practice gap by offering a way of increasing understanding of, andrelevance of, research activities from the perspective of ward- and department-basednurses and allied health professionals.
Project implementation
Establishment of the evidence-based council
The post of council facilitator was advertised as a part-time secondment opportunity. Anursing sister with experience in evidence-based practice and practice development,from the cardiac intensive care unit, was appointed to the post. She had had activeinvolvement in practice development and evidence-based practice. The post was origi-nally for the 18 months of the Foundation of Nursing Studies grant, but was extendedpending a long-term decision from the trust in 2003 with regard to continued fundingand support for the council.
The Nurse Executive Group agreed to the principle that council members wereallowed time to attend meetings, education and training. However, it was left toindividual departments and council members as to how this was to be arranged. Aproject steering group was established to oversee the implementation of the project.
Recruitment of council representatives was from clinical staff departmentsacross the trust. Nominations were sought from managers in various clinical areas, atleast one nursing representative and a deputy were recruited from each directorate, aswere representatives from allied health professionals. The aim was to ensure that eacharea was represented at council meetings.
Early in the consultation process it was decided that the council should bemultiprofessional. The majority felt that the initiative should be inclusive and notrestricted to nurses only. However, unexpected resistance to integration was encoun-tered from a minority of nurses. The allied health professionals who were approachedabout involvement in the council asked that they be kept informed of council work.The dietician and occupational therapy representatives have attended meetingsregularly and their contribution has been invaluable.
Several members were ‘co-opted’ from key departments that support evidence-based practice, these included:
● the University of Sheffield health sciences librarian● a member of the trust practice development support team● clinical effectiveness and audit department representatives.
An example of the benefits brought by the co-opted representatives is thatthrough liaison with the librarian £500 was made available to fund informationresources for the council. Librarians also assisted in the provision of information skillstraining and dissemination of evidence via the Sheffield Evidence for Effectiveness andKnowledge (SEEK) database.
Learning from experience 91
PDHC 2.2_3rd/crc 17/6/03 3:14 pm Page 91
92 Palfreyman et al.
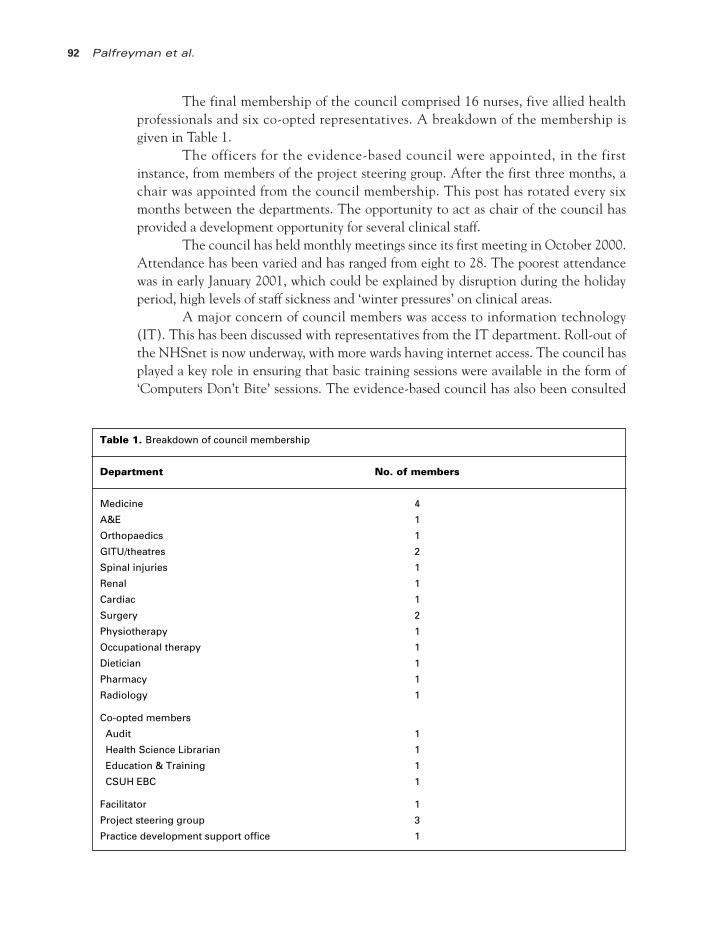
The final membership of the council comprised 16 nurses, five allied healthprofessionals and six co-opted representatives. A breakdown of the membership isgiven in Table 1.
The officers for the evidence-based council were appointed, in the firstinstance, from members of the project steering group. After the first three months, achair was appointed from the council membership. This post has rotated every sixmonths between the departments. The opportunity to act as chair of the council hasprovided a development opportunity for several clinical staff.
The council has held monthly meetings since its first meeting in October 2000.Attendance has been varied and has ranged from eight to 28. The poorest attendancewas in early January 2001, which could be explained by disruption during the holidayperiod, high levels of staff sickness and ‘winter pressures’ on clinical areas.
A major concern of council members was access to information technology(IT). This has been discussed with representatives from the IT department. Roll-out ofthe NHSnet is now underway, with more wards having internet access. The council hasplayed a key role in ensuring that basic training sessions were available in the form of‘Computers Don’t Bite’ sessions. The evidence-based council has also been consulted
Table 1. Breakdown of council membership
Department No. of members
Medicine 4
A&E 1
Orthopaedics 1
GITU/theatres 2
Spinal injuries 1
Renal 1
Cardiac 1
Surgery 2
Physiotherapy 1
Occupational therapy 1
Dietician 1
Pharmacy 1
Radiology 1
Co-opted members
Audit 1
Health Science Librarian 1
Education & Training 1
CSUH EBC 1
Facilitator 1
Project steering group 3
Practice development support office 1
PDHC 2.2_3rd/crc 17/6/03 3:14 pm Page 92

and has advised on the development and implementation of four multi-media learningzones across the trust.
The council is keen to identify clinical issues of concern that may prompt thedevelopment of new research and audit. Considerable time has been spent discussingissues related to nutrition—which emerged as a clinical topic that crossed professionaland departmental boundaries. The council produced a discussion document that waswidely disseminated across the trust, including the clinical governance and bench-marking groups. The document highlighted existing local evidence, examples of goodpractice and ongoing areas of concern. Work has commenced on the development of aresearch proposal to further explore factors influencing malnutrition in hospital.
Education and training
Following a needs assessment exercise, council members reviewed the educationopportunities available for developing skills in evidence-based practice. They decidedto use the ‘Evidence Based Health Care’ open learning package developed by NHSEAnglia and Oxford. Funding from the Foundation of Nursing Studies was used toprovide an external facilitator, who had previously delivered the training within thehospital. The trust education and training department funded resource packs for allcouncil members.
The training package was delivered twice over a 12-month period, with theaim of each council member being offered a place on the course. The course involvedattending four taught days, delivered by the training facilitator and members of theproject steering group.
The education package allowed council members to search and appraise theliterature related to an issue of concern in their clinical area, and to generate an actionplan. Members were assessed via a written assignment summarizing their literaturesearch and appraisal—with recommendations for their clinical practice and by theirpreparation of a poster of the course work, suitable for presentation at a conference.
A poster competition was held, as a lunchtime event, with prizes of booktokens presented by representatives from the Foundation of Nursing Studies, theSchool of Nursing and the hospital Professional and Practice DevelopmentDepartment. Many posters demonstrated some change in practice or future projectwork resulting from a review and application of evidence. The winners of the postercompetition were from occupational therapy, dietetics and nursing.
Journal clubs
A mapping exercise was performed to identify any existing journal clubs and practicedevelopment groups across the trust. Some areas had well-established journal clubs ortheir equivalent. Others had none or the clubs had failed to thrive. The council helpedto reinvigorate existing groups and to establish new groups with the help of its facili-tator. Success in establishing journal clubs was very mixed, with some areas trying toidentify the best format and content to ensure staff involvement. However, the idea of
Learning from experience 93
PDHC 2.2_3rd/crc 17/6/03 3:14 pm Page 93

two-way communication has been realized, with members of journal clubs feeding backto the council about progress, developments and clinical issues identified by the clubsand groups. Where problems have been encountered in developing or maintaining ajournal club, council members have offered peer support and advice.
Evaluation of the evidence-based councilAn evaluation of the evidence-based council was devised and integrated with a largertrust-wide evidence-based practice study. Ethical Committee approval was obtained forevaluation of the evidence-based council. Evaluation involved the use of a question-naire survey and a qualitative study employing semi-structured interviews. The samplecomprised nurses and physiotherapists working in surgical, medical and specialist areas.
The survey found that information from clients, and personal experience, wereamong the greatest sources of knowledge, with the internet used least. Nurses weremore likely than physiotherapists to use their intuition, policy and procedure manuals,and medical staff as sources of information. The factor that provided the greatestperceived barrier for both nurses and physiotherapists was insufficient time to findinformation—with more than 72% of all respondents reporting this as a barrier. Theleast-cited barrier was the culture of the ward. When examining skills in evidence-based practice, nurses were more likely than physiotherapists to rate themselves asnovices in terms of finding, reviewing and using research evidence.
The results of the survey were presented at the Royal College of Nursing inter-national research conference in Glasgow in 2001. Work is currently underway to writeup the evaluation for publication.
Lessons learntA number of lessons were learnt during the course of the project.
Organizational endorsement
The principle and aims of the evidence-based council were endorsed by the trust, inparticular by its Nursing Executive Group, and included in its nursing strategy.However, in reality, many council members had problems negotiating time to attendmeetings and the educational programme. This was attributed to staff shortages andconsequent difficulties in being released from the ward.
An additional complication was that during the project the two NHS trustswithin Sheffield (the Northern General and Central Sheffield University hospitals)merged, creating delays in resolving attendance problems as the entire managementstructure was reorganized. Key problems were uncertainties about authority andaccountability that this situation generated.
94 Palfreyman et al.
PDHC 2.2_3rd/crc 17/6/03 3:14 pm Page 94
Recommendations
● Ownership of the project by clinical staff is essential, but for the initiative tosurvive there needs to be support from the organization. This needs to be morethan just notional endorsement and should include releasing staff from clinicalareas to attend meetings and projects concerned with the evidence-based council.
● A way of facilitating such support may be to include initiatives into truststrategies and targets for evidence-based practice.
Ownership of the project by clinical staff is essential, but forthe initiative to survive there needs to be support from theorganization.
Council membership
It has proved difficult to recruit the range of clinically active staff initially intended.Council membership was predominantly made up of clinical nurse educators and nursespecialists. This may have been because these groups have the necessary autonomy andflexibility within their everyday activities to allow them to attend meetings.
Recommendation
● The relevance of council activity to clinical managers may be increased byhaving a role description for members and including this in their individualperformance reviews (IPR).
Multidisciplinary involvement
The council was established to be inclusive to allied health professionals. Some alliedhealth professionals have consistently attended council meetings and proved to bevaluable contributors to work undertaken. An example of this is the work on nutrition,where the dietician representative’s knowledge was invaluable.
However, there was some initial resistance from nurses to the proposal that thecouncil should be multidisciplinary. The nature of such responses from a minority ofnurses highlights the future need to facilitate a collaborative approach to evidence-based practice, research and practice development.
Recommendation
● Clinical priorities should be central to evidence-based practice. In addition, amultidisciplinary approach ensures a broad range ofexpertise and perspectivesare included.
Learning from experience 95
PDHC 2.2_3rd/crc 17/6/03 3:14 pm Page 95
Education and training
The education and training offered to council members was highly valued. Membersreported that the training was of particular use because it was skills-based and was ofpractical help in their evidence-based practice work. The education package allowedthem to work on a topic of clinical relevance to their practice. The experience of theproject highlights a need for a systematic approach to the education and training ofnurses and allied health professionals with regard to evidence-based practice. Thismust include widespread, basic skills-based training. Two evaluations conducted withinthe trust at the same time also revealed a need for information skills training.
Recommendation
● Funding for education in evidence-based practice is essential so that allmembers have baseline skills.
● The relevance of training may be increased by linking it to clinical issues.
Journal clubs
Establishing journal clubs that are attractive and accessible to staff has been anongoing challenge for council members. A flexible definition as to what constituted ajournal club was adopted as some nurses were deterred by the name. Many directoratesfound that meetings which had a practice development emphasis, rather than criticalappraisal, proved more popular. It was considered important for meetings to be locallyappropriate in terms of time, duration and format.
Recommendation
● These can be difficult to establish and maintain but a facilitator can make thiseasier.
Facilitation
Overall, the success of the council was largely due to the work of the facilitator. Theproject steering group and council members have had to balance council work withthat of their substantive posts. The facilitator was the only individual who had oneday of protected time to work on council business. This was invaluable in ensuringthe co-ordination of meetings, support of council members, evaluation of thecouncil, the education programme and supporting the development of the journalclubs.
Recommendation
● Having a specific individual who has protected time to facilitate council activ-ities is crucial to any evidence-based council.
96 Palfreyman et al.
PDHC 2.2_3rd/crc 17/6/03 3:14 pm Page 96

ConclusionsThe project made a clear contribution to clinical governance and evidence-basedpractice targets within the local trust, through its contribution to groups established bythe trust. It has also given nurses a mechanism for discussing evidence-based practiceon a hospital-wide basis. The project also increased the skills of council members inevidence-based practice through an educational programme. The council alsogenerated discussion documents and is in the process of developing fundable researchprojects.
Despite the successes, this initiative highlighted a number of concerns thatothers involved in the promotion of evidence-based practice might consider:
● Residual resistance to collaboration and multidisciplinary working still existsamong some nurses.
● A large proportion of nurses lack basic information skills, for example literaturesearching and appraisal.
● Despite endorsement at the highest level of an organization, there are hugepractical problems in clinical staff being released from wards to participate inevidence-based practice activity.
● Some nurses, exhausted from the demands of their clinical work, are increas-ingly unwilling to undertake evidence-based practice activities in their owntime, despite retaining a positive attitude to evidence-based practice.
On a more positive note, much has been achieved with limited funding.Although there is still a long way to go, the project has made significant headway inachieving the initial objectives.
Update 2003
The project continues to evolve. Now that the newly merged trust is settling down, anextensive review of the activities of the council has been conducted, highlightingachievements, difficulties and proposals for the future. Initial responses to the reviewhave been very positive. Having evaluated the progress of the council to date, theproject is ready to move on to the next phase.
ReferencesBlanchard H. Factors inhibiting the use of research in practice. Professional Nurse 1996; 11: 524.Bonell C. Evidence-based nursing: a stereotyped view of quantitative and experimental research could work
against professional autonomy and authority. Journal of Advanced Nursing 1999; 30: 18–23.Burrows D, McLeish K. A model for research based practice. Journal of Clinical Nursing 1995; 4: 243–247.Closs SJ, Cheater FM. Utilization of nursing research: culture, interest and support. Journal of Advanced
Nursing 1994; 19: 762–773.
Learning from experience 97
PDHC 2.2_3rd/crc 17/6/03 3:14 pm Page 97
98 Palfreyman et al.
Colyer H, Kamath P. Evidence-based practice. A philosophical and political analysis: some matters forconsideration by professional practitioners. Journal of Advanced Nursing 1999; 29: 188–193.
Centre for Reviews and Dissemination (CRD). Undertaking Systematic Reviews of Research onEffectiveness: CRD Guidelines for Those Carrying Out or Commissioning Reviews. York: Centre forReviews and Dissemination, 1996.
Department of Health and Social Security (DHSS). Report of the Committee on Nursing (Briggs Report;5115). London: HMSO, 1972.
Department of Health (DoH). Research and Development: Towards an Evidence-based Health Service.London: HMSO, 1995.
Department of Health (DoH). The New NHS: Modern, Dependable. London: HMSO, 1997.English I. Nursing as a research-based profession: 22 years after Briggs. British Journal of Nursing 1994; 3:
402–406.French B. The role of outcomes in the measurement of nursing. Nurse Researcher 1995; 2: 5–13.French B. British studies which measure patient outcome, 1990–1994. Journal of Advanced Nursing 1997;
26: 320–328.Hicks C, Hennessy D. Mixed messages in nursing research: their contribution to the persisting hiatus
between evidence and practice. Journal of Advanced Nursing 1997; 25: 595–601.Hunt J. Indications for nursing practice; the use of research findings. Journal of Advanced Nursing 1981; 6:
189–194.Kettles AM. Research means more than randomised trials. Nursing Standard 1997; 11: 32–33.Kirchhoff KT, Beck SL. Using the journal club as a component of the research utilization process. Heart
and Lung: Journal of Critical Care 1995; 24: 246–250.Kitson A, Harvey G, McCormack B. Enabling the implementation of evidence-based practice: a
conceptual framework. Quality in Health Care 1998; 7: 149–158.Koziol-McLain J, Tanabe P. The research column. Reviewing the research literature: you don’t have to do
it alone. Journal of Emergency Nursing 1996; 22: 352–355.le May A. Evidence-based Practice. London: E Map Health Care Ltd, 1999.le May A, Mulhall A, Alexander C. Bridging the research–practice gap: exploring the research cultures of
practitioners and managers. Journal of Advanced Nursing 1998; 28: 428–437.Marsh GW, Hopkins S. Barriers to Research Utilisation in an Acute Care Trust. Proceedings of the
Partnership in the Millenium Conference, Sheffield, 1999.McSherry R. What do registered nurses and midwives feel and know about research? Journal of Advanced
Nursing 1997; 25: 985–998.Michaels JA, Booth A. Pragmatic system for the grading of evidence and recommendations in clinical
guidelines. Journal of Clinical Excellence 2001; 3: 139–143.Nolan M, Morgan L, Curran M et al. Evidence based care: can we overcome the barriers? British Journal of
Nursing 1998; 7: 1273–1278.Pearcey PA. Achieving research-based nursing practice. Journal of Advanced Nursing 1995; 22: 33–39.Rafferty AM, Allcock N, Lathlean J. The theory/practice ‘gap’: taking issue with the issue. Journal of
Advanced Nursing 1996; 23: 685–691.Sheehan J. A journal club as a teaching and learning strategy in nurse teacher education. Journal of
Advanced Nursing 1994; 19: 572–578.Upton D. Attitudes towards, and knowledge of, clinical effectiveness in nurses, midwives, practice nurses
and health visitors. Journal of Advanced Nursing 1999a; 29: 885–893. Upton DJ. How can we achieve evidence-based practice if we have a theory–practice gap in nursing today?
Journal of Advanced Nursing 1999b; 29: 549–555.White SJ. Evidence-based practice and nursing: the new panacea? British Journal of Nursing 1997; 6:
175–178.
Address for correspondence: Simon Palfreyman, Vickers 16, Northern GeneralHospital, Sheffield, S5 7AU (E-mail: [email protected]).
PDHC 2.2_3rd/crc 17/6/03 3:14 pm Page 98