Embed Size (px)
Citation preview

Journal of Diabetes and Its Complications xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Journal of Diabetes and Its Complications
j ourna l homepage: WWW.JDCJOURNAL.COM
Editorial
Lessons from SAVOR and EXAMINE: Some important answers, but manyopen questions☆,☆☆
Type 2 diabetes is a progressive complex metabolic diseaseassociated with bothmicrovascular andmacrovascular complications.The risk of cardiovascular (CV) disease is around two times as high inpeople with diabetes as in people without diabetes (Emerging RiskFactors Collaboration et al., 2010). Improved glycemic control canreduce the risk of many microvascular complications of diabetes suchas diabetic nephropathy, retinopathy and neuropathy (UKPDS, 1998),but three recent studies have not individually shown a favorable effectof intensive glycemic control in reducing macrovascular events inpatients with type 2 diabetes (Action to Control Cardiovascular Risk inDiabetes Study Group, 2008; ADVANCE Collaborative Group, 2008;Duckworth et al., 2009) During the last 25 years all-cause mortality,CV death and CV events were reduced in patients with type 2 diabetesby more than 50% (Gregg et al., 2012; Lind et al., 2013; Preis et al.,2009), mainly by the wide use of lipid lowering and blood pressurelowering drugs. In the secondary prevention of CV events antiplateletdrugs are effective and therefore also standard therapy in diabeticpatients presenting with CVD (Grove & Gregersen, 2012).
Based on the proven effect of HbA1c lowering on microvascularcomplications but some uncertainty over CV benefits, most clinicaldevelopment programs for novel antidiabetes drugs have focusedmainly on glucose lowering. Most patients recruited for regulatoryapproval have had limited duration of diabetes and few complica-tions. Although these types of confirmatory studies established theglucose-lowering properties of novel drugs, CV safety assessment inthe context of the clinical development of glucose-lowering agentshas been largely neglected until recently.
Concerns regarding adverse cardiovascular outcomes with antidi-abetic agents, in particular for rosiglitazone, prompted the Food andDrug Administration (FDA) to issue guidance in December 2008 thatincluded specific requirements for cardiovascular safety assessmentbefore and after the approval of new antidiabetic therapies (http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDrugsAdvisoryCommittee/UCM334550.pdf). Specifically, sponsors were informed that they mustrule out an upper 95% CI of the hazard ratio (HR) for cardiovasuclarevents of 1.8 for their medication before approval and 1.3 afterapproval. As a consequence more than 180,000 patients with type 2diabetes will be included in about 18 CV outcome studies with newantidiabetic drugs (GLP-1 receptor agonists, DPP-4 inhibitors, SGLT2-Inhibitors, Acarbose). In addition to previously published studies with
☆ Declarations of interest: Guntram Schernthaner has consulted for: Amgen,Astrazeneca, BMS, Boehringer Ingelheim, Eli Lilly, Janssen, MSD.
☆☆ Naveed Sattar has consulted for: Astrazeneca, BMS, Sanofi, Amgen, BoehringerIngelheim.
http://dx.doi.org/10.1016/j.jdiacomp.2014.02.0111056-8727/© 2014 Elsevier Inc. All rights reserved.
pioglitazone (PROactive; Dormandy et al., 2005), rosiglitazone (RECORD;Home et al., 2009) and basal insulin glargine (ORIGIN Trial Investigatorset al., 2012), we have now also evidence from two recently publishedDPP-4 inhibitor studies, which investigated saxagliptin (SAVOR; Sciricaet al., 2013) and alogliptin (EXAMINE, White et al., 2013).
Patients randomized to active therapy or placebo in the SAVOR andEXAMINE studies differed in many aspects. Whereas SAVOR recruitedtwo types of patients, one with establised CVD and other withmultiple risk factors (MRF), all patients in EXAMINE had an history ofacute coronary syndrome (Table 1). Thus, prior stroke and PAD wasconsiderably lower in EXAMINE, whereas heart failure at baseline wasdocumented in 28% of patients included in EXAMINE, but in only14.8% and 5.1% respectively in the two groups of patients recruitedinto SAVOR. About two thirds of all patients received metformin atbaseline and sulfonylureas were used by 37–46% of participants(Table 2). Insulin was more often used in SAVOR patients withestablished CVD (42.2%) compared with patients included inEXAMINE (30%), which is likely in part explained by the fact thatmedian duration of diabetes was longer in SAVOR vs. EXAMINE (10.3vs. 7.3 years). Treatment for reducing CV risk factors was extremelygood in both studies; statins and ACE/ARB were used in 80 to 90% andantiplatelet in almost all patients (89–97%), however ß-blockingagents were less used in SAVOR vs. EXAMINE (68 vs. 82%). Asexpected the 25% of patients in SAVOR presenting only with MRFreceived less cardioprotecive therapy (Table 2).
A recently published metanalysis of DPP-4 inhibitors and CV riskshowed rather promising results (Monami, Ahrén, Dicembrini, &Mannucci, 2013). The MH–OR (95% CI) for DPP-4 inhibitors versuscomparators (placebo or active control) was 0.71 [0.59;0.86], 0.64[0.44;0.94], 0.77 [0.48;1.24] and 0.60 [0.41;0.88] for MACE, myocar-dial infarction, stroke and mortality, respectively. More specific, theMH-OR for MACE with saxagliptin was 0.67 [0.45;0.99] based on 15studies and 0.86 [0.25;2.93] for alogliptin based on only 5 studies.However, the mean observation period of the 63 trials was only44 weeks, and the CV event rate was extremely low in both the DPP-4inhibitor arms (263 events in 23 451 patients years; 0.73%) andcomparator arms (232 events in 16 962 patient years; 0.89%). Takinginto account the rather small difference in the event rate of only 0.16%and the fact that these studies were not controlled for the use ofcardioprotective drugs, the value of such information is potentiallylimited and could even be misleading, hence the need for robustlyadjudicated randomised placebo-controlled clinical trials.
The SAVOR study was originally designed as a superiority studytesting the hypothesis that treatment with saxagliptin is safe andreduces CV events in high-risk patients with T2DM (Scirica et al., 2013),whereas the primary objective of EXAMINE (White et al., 2013) was to

Table 1Cardiovascular history at baseline (%).
SAVOR EXAMINE
Established CVD MRF Acute coronary syndrome
Number 12.927 3.573 5.380MI 47.9 1.3 77.0⁎
ACS 0 0 23.0Stroke 16.0 0.8 7.2PAD 14.9 1.1 9.5CHF 14.8 5.1 28.0
MRF: multiple risk factors; MI: myocardial infarction; *acute myocardial infarction.PAD: peripherial arterial disease; CHF: congestive heart failure.Scirica BM, et al. N Engl J Med. 2013; 369: 1317-1326, White WB et al. N Engl J Med.2013; 369:1327-1335.
Table 3Effect of saxagliptin or alogliptin versus placebo on the primary endpoint (composite ofdeath from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke) inSAVOR and EXAMINE.
Saxagliptin (n = 8280) Placebo (n = 8212) Hazard ratio (95% Cl) p Value
no (%)613 (7.3) 609 (7.2) 1.00 (0.89–1.12) 0.99
Alogliptin (n = 2679) Placebo (n = 2701) Hazard ratio (95% Cl) p Value
no (%)316 (11.8) 305 (11.3) 0.96 (≤1.16) 0.32
2 Editorial / Journal of Diabetes and Its Complications xxx (2014) xxx–xxx
demonstrate the noninferiority of MACE on alogliptin versus placebo inthe treatment of type 2 diabetes in a high-risk CV patient group.
The primary endpoint - composite of death from cardiovascularcauses, nonfatal myocardial infarction, or nonfatal stroke – was notdifferent between the DPP-4 inhibitor and the placebo arms in bothSAVOR and EXAMINE (Table 3) irrespective of the small difference inthe median exposure time (25 versus 18 months). These findingsdemonstrate that saxagliptin and alogliptin are safe concerning CVD,but cannot further reduce the risk of the primary endpoint whenadded to other antidiabetic and cardioprotective drugs in type 2diabetic patients with a high CV risk. Are these data surprising? Not atall. The HbA1c lowering potency of saxagliptin and alogliptin at studyend versus baseline or the control groups was rather modest in bothstudies (0.30 and 0.36%), although one must accept that neither studywas designed as a glycaemia-differential trial. In addition the reportedpleiotropic CV effects of DPP-4 inhibitors on lipid or blood pressurelowering are quite modest (Scheen, 2013). It appears from this workthat reducing glucose by a small or even modest amount is highlyunlikely to lead to CV risk reduction, at least in the short period overwhich trials are conducted. One might also conclude that in order tomeaningfully reduce CV events in patients with diabetes, cholesteroland BP reduction together with smoking cessation are of paramountimportance. In this way, the results of the SAVOR and EXAMINEreinforce the need to re-challenge the glycamia paradigm in diabetes,as has been recently done (Sattar, 2013).
Neutral data for the clinically important endpoint of death,nonfatal myocardial infarction and stroke (Table 4) were not onlyseen for saxagliptin and alogliptin, but previously also for basal insulin(ORIGIN) and for canagliflozin in the preliminary analysis of theCANVAS trial (Janssen Research & Development LLC, 2012; Neal et al.,2013).). In PROactive (Dormandy et al., 2005) the use of pioglitazonewas associated with a significant reduction of the triple endpoint, butthe primary endpoint including peripheral and coronary revascular-isation was not significantly reduced. In contrast to the newer studies
Table 2Antidiabetic and cardiovascular medication at baseline (%).
SAVOR EXAMINE
Established CVD MRF Acute coronary syndrome
Number 12.927 3.573 5.380Metformin 65.5 74.4 66.0Sulfonylureas 37.4 42.3 46.0Insulin 42.2 30.7 30.0Statins 82.7 62.2 90.5ACE/ARB 78.8 77.4 81.5β-blockers 68.3 36.4 82.0Antiplatelet therapy 88.7 54.4 97.2
MRF: multiple risk factors.Scirica BM, et al. N Engl J Med. 2013; 369: 1317-1326, White WB et al. N Engl J Med.2013; 369:1327-1335.
statins were far less used in PROactive which might explain whypioglitazonewas able to show some antiatherogenic effects in that trial.
The HbA1c lowering observed with saxagliptin in SAVOR wasassociated with a small increase in hypoglycemic events, which wasrelated to the combination with sulfonylureas as reported at the EASD2103. An increased risk of hypoglycemia associated with the use ofsaxagliptin was only seen in those patients presenting with HbA1c atbaseline b 7.0% (HR1.40; 95%CI 1.17, 1.69; p b 0.001), but not in patientspresenting with HbA1c N 7.0% at baseline (as reported at the AHA).
Perhaps the most notable findings was the observation of morepatients in the saxagliptin group than in the placebo group beinghospitalized for heart failure (3.5% vs. 2.8%; hazard ratio, 1.27; 95% CI,1.07 to 1.51; p = 0.007). As expected the risk for heart failurehospitalisation (HF) was closely related to NT-proBNP levels atbaseline in both the saxagliptin and control arms. In patients with thehighest quartile of NT-proBNP levels at baseline (333–46,627) the riskfor HF hospitalisation was10.9% in the saxagliptin group and 8.9% inthe placebo arm (HR 1.31 95%CI 1.0–1.6; p = 0.021). The risk for HFhospitalisation associated with the use of saxagliptin was highest inthe first 6 months (HR 1.80; 1.29–2.54; p b 0.001) and declinedthereafter, HR 1.48 after 1 year and 1.28 after 2 years (Scirica et al.(2013). As expected prior HF was the strongest predictor of HFhospitalisation during the study (HR 4.17; 3.48–4.99; p b 0.001),followed by impaired kidney function (eGFR b 50 ml/min) (HR 2.39;1.98–2.88; p b 0.001) and increased (N30 mg/g) albumin/creatinineratio (HR 2.18; 1.81–2.63; p b 0.001). Other variables such as high age(N75 years) or previous myocardial infarction were less predictive(Scirica et al. (2013)).
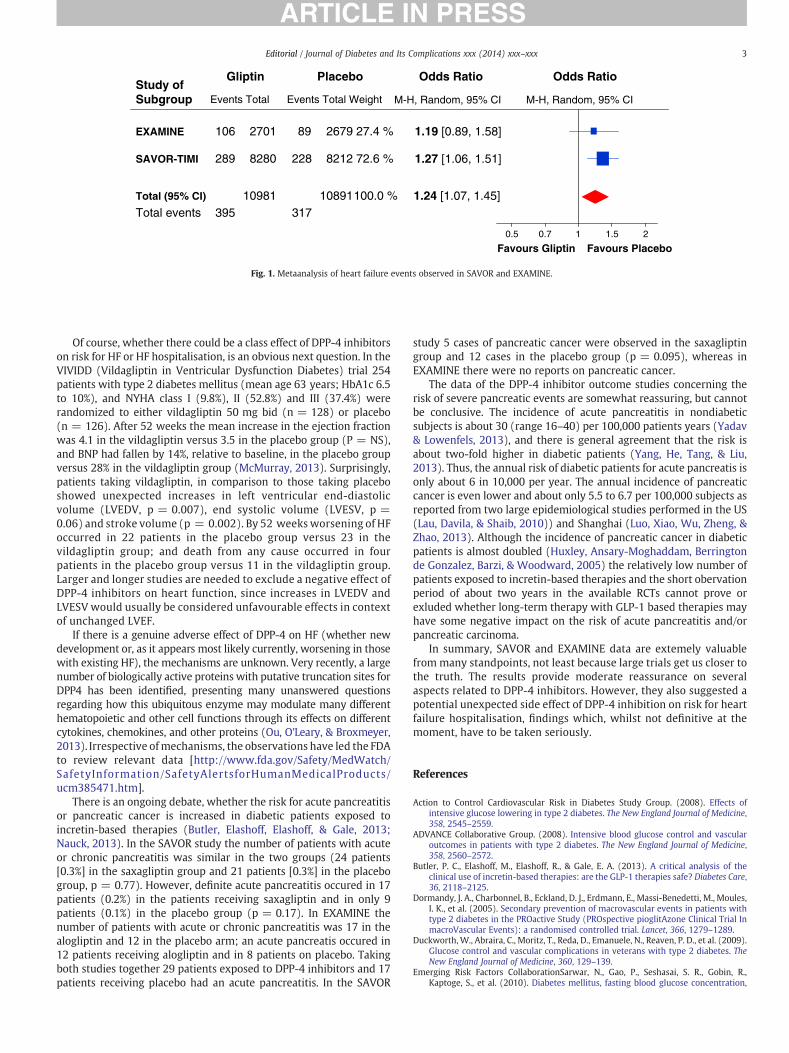
The overall risk of hospitalization for HF in the SAVOR studywas ~ 2% annually, 289 cases of HF hospitalisation were observed inthe saxagliptin arm and 228 in the placebo arm. A similar trend wasalso observed in EXAMINE, 106 patients in the alogliptin arm and 89patients in the placebo arm were hospitalised for HF. Fig. 1 shows themetaanalyis combining data from both studies and indicates anincreased risk of HF hospitalisation with the use of DPP-4 inhibitors,395 cases of HF with DPP-4 inhibitors versus 317 with placebo (HR1.24 (1.07–1.44). It may be somewhat surprising that the increase inHF hospitalisation risk associated with alogliptin was apparently lessclear cut despite prior HF being almost doubled in EXAMINE versusSAVOR. The higher use of ß-blocking agents and the more frequentmedical controls with treatment adapations in EXAMINEmight be oneof the potential explanations, amongst other explanations.
Table 4Effect of glucose lowering drugs on the combined endpoint of CV mortality, nonfatalmyocardial infarction and stroke.
Antidiabetic drug HR p value
• PROactive Pioglitazone 0.84 (Cl 0.72–0.98) 0.02• ORIGIN Insulin Glargine 1.02 (Cl 0.94–1.11) NS• SAVOR Saxagliptin 1.00 (Cl 0.89–1.12) NS• EXAMINE Alogliptin 0.96 (Cl 0.80–1.15) NS• CANVAS Canagliflozin 1.00 (CI 0.72, 1.39) NS
Favours Gliptin20.5 1
Favours Placebo0.7 1.5
M-H, Random, 95% CIM-H, Random, 95% CIEvents Total
Odds Ratio
Events Total Weight
GliptinStudy of Subgroup
27.4 %
317100.0 %
Total events
EXAMINE
SAVOR-TIMI
Total (95% CI)
72.6 %
89
228
2701
39510981
8280
106
289
1.19 [0.89, 1.58]
1.24 [1.07, 1.45]
1.27 [1.06, 1.51]
2679
10891
8212
Placebo Odds Ratio
Fig. 1. Metaanalysis of heart failure events observed in SAVOR and EXAMINE.
3Editorial / Journal of Diabetes and Its Complications xxx (2014) xxx–xxx
Of course, whether there could be a class effect of DPP-4 inhibitorson risk for HF or HF hospitalisation, is an obvious next question. In theVIVIDD (Vildagliptin in Ventricular Dysfunction Diabetes) trial 254patients with type 2 diabetes mellitus (mean age 63 years; HbA1c 6.5to 10%), and NYHA class I (9.8%), II (52.8%) and III (37.4%) wererandomized to either vildagliptin 50 mg bid (n = 128) or placebo(n = 126). After 52 weeks the mean increase in the ejection fractionwas 4.1 in the vildagliptin versus 3.5 in the placebo group (P = NS),and BNP had fallen by 14%, relative to baseline, in the placebo groupversus 28% in the vildagliptin group (McMurray, 2013). Surprisingly,patients taking vildagliptin, in comparison to those taking placeboshowed unexpected increases in left ventricular end-diastolicvolume (LVEDV, p = 0.007), end systolic volume (LVESV, p =0.06) and stroke volume (p = 0.002). By 52 weeks worsening of HFoccurred in 22 patients in the placebo group versus 23 in thevildagliptin group; and death from any cause occurred in fourpatients in the placebo group versus 11 in the vildagliptin group.Larger and longer studies are needed to exclude a negative effect ofDPP-4 inhibitors on heart function, since increases in LVEDV andLVESV would usually be considered unfavourable effects in contextof unchanged LVEF.
If there is a genuine adverse effect of DPP-4 on HF (whether newdevelopment or, as it appears most likely currently, worsening in thosewith existing HF), the mechanisms are unknown. Very recently, a largenumber of biologically active proteins with putative truncation sites forDPP4 has been identified, presenting many unanswered questionsregarding how this ubiquitous enzyme may modulate many differenthematopoietic and other cell functions through its effects on differentcytokines, chemokines, and other proteins (Ou, O'Leary, & Broxmeyer,2013). Irrespective ofmechanisms, the observations have led the FDAto review relevant data [http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm385471.htm].
There is an ongoing debate, whether the risk for acute pancreatitisor pancreatic cancer is increased in diabetic patients exposed toincretin-based therapies (Butler, Elashoff, Elashoff, & Gale, 2013;Nauck, 2013). In the SAVOR study the number of patients with acuteor chronic pancreatitis was similar in the two groups (24 patients[0.3%] in the saxagliptin group and 21 patients [0.3%] in the placebogroup, p = 0.77). However, definite acute pancreatitis occured in 17patients (0.2%) in the patients receiving saxagliptin and in only 9patients (0.1%) in the placebo group (p = 0.17). In EXAMINE thenumber of patients with acute or chronic pancreatitis was 17 in thealogliptin and 12 in the placebo arm; an acute pancreatis occured in12 patients receiving alogliptin and in 8 patients on placebo. Takingboth studies together 29 patients exposed to DPP-4 inhibitors and 17patients receiving placebo had an acute pancreatitis. In the SAVOR
study 5 cases of pancreatic cancer were observed in the saxagliptingroup and 12 cases in the placebo group (p = 0.095), whereas inEXAMINE there were no reports on pancreatic cancer.
The data of the DPP-4 inhibitor outcome studies concerning therisk of severe pancreatic events are somewhat reassuring, but cannotbe conclusive. The incidence of acute pancreatitis in nondiabeticsubjects is about 30 (range 16–40) per 100,000 patients years (Yadav& Lowenfels, 2013), and there is general agreement that the risk isabout two-fold higher in diabetic patients (Yang, He, Tang, & Liu,2013). Thus, the annual risk of diabetic patients for acute pancreatis isonly about 6 in 10,000 per year. The annual incidence of pancreaticcancer is even lower and about only 5.5 to 6.7 per 100,000 subjects asreported from two large epidemiological studies performed in the US(Lau, Davila, & Shaib, 2010)) and Shanghai (Luo, Xiao, Wu, Zheng, &Zhao, 2013). Although the incidence of pancreatic cancer in diabeticpatients is almost doubled (Huxley, Ansary-Moghaddam, Berringtonde Gonzalez, Barzi, & Woodward, 2005) the relatively low number ofpatients exposed to incretin-based therapies and the short obervationperiod of about two years in the available RCTs cannot prove orexluded whether long-term therapy with GLP-1 based therapies mayhave some negative impact on the risk of acute pancreatitis and/orpancreatic carcinoma.
In summary, SAVOR and EXAMINE data are extemely valuablefrom many standpoints, not least because large trials get us closer tothe truth. The results provide moderate reassurance on severalaspects related to DPP-4 inhibitors. However, they also suggested apotential unexpected side effect of DPP-4 inhibition on risk for heartfailure hospitalisation, findings which, whilst not definitive at themoment, have to be taken seriously.
References
Action to Control Cardiovascular Risk in Diabetes Study Group. (2008). Effects ofintensive glucose lowering in type 2 diabetes. The New England Journal of Medicine,358, 2545–2559.
ADVANCE Collaborative Group. (2008). Intensive blood glucose control and vascularoutcomes in patients with type 2 diabetes. The New England Journal of Medicine,358, 2560–2572.
Butler, P. C., Elashoff, M., Elashoff, R., & Gale, E. A. (2013). A critical analysis of theclinical use of incretin-based therapies: are the GLP-1 therapies safe? Diabetes Care,36, 2118–2125.
Dormandy, J. A., Charbonnel, B., Eckland, D. J., Erdmann, E., Massi-Benedetti, M., Moules,I. K., et al. (2005). Secondary prevention of macrovascular events in patients withtype 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial InmacroVascular Events): a randomised controlled trial. Lancet, 366, 1279–1289.
Duckworth, W., Abraira, C., Moritz, T., Reda, D., Emanuele, N., Reaven, P. D., et al. (2009).Glucose control and vascular complications in veterans with type 2 diabetes. TheNew England Journal of Medicine, 360, 129–139.
Emerging Risk Factors CollaborationSarwar, N., Gao, P., Seshasai, S. R., Gobin, R.,Kaptoge, S., et al. (2010). Diabetes mellitus, fasting blood glucose concentration,

4 Editorial / Journal of Diabetes and Its Complications xxx (2014) xxx–xxx
and risk of vascular disease: a collaborative meta-analysis of 102 prospectivestudies. Lancet, 375, 2215–2222.
Gregg, E. W., Cheng, Y. J., Saydah, S., Cowie, C., Garfield, S., Geiss, L., et al. (2012). Trendsin death rates among U.S. adults with and without diabetes between 1997 and2006: findings from the National Health Interview Survey. Diabetes Care, 35,1252–1257.
Grove, E. L., & Gregersen, S. (2012). Antiplatelet therapy in patients with diabetesmellitus. Current Vascular Pharmacology, 10, 494–505.
Home, P. D., Pocock, S. J., Beck-Nielsen, H., Curtis, P. S., Gomis, R., Hanefeld, M., et al.(2009). Rosiglitazone evaluated for cardiovascular outcomes in oral agentcombination therapy for type 2 diabetes (RECORD): a multicentre, randomised,open-label trial. Lancet, 373, 2125–2135.
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDrugsAdvisoryCommittee/UCM334550.pdf
Huxley, R., Ansary-Moghaddam, A., Berrington de Gonzalez, A., Barzi, F., & Woodward,M. (2005). Type-II diabetes and pancreatic cancer: a meta-analysis of 36 studies.British Journal of Cancer, 92, 2076–2083.
Janssen Research & Development LLC (2012). Advisory committee briefing materials:Canagliflozin as an adjunctive treatment to diet and exercise alone or co-administered with antihyperglycemic agents to improve glycemic control in adultswith type 2 diabetes mellitus. Endocrinologic and Metabolic Drugs AdvisoryCommittee, 1–184.
Lau, M. K., Davila, J. A., & Shaib, Y. H. (2010). Incidence and survival of pancreatic headand body and tail cancers: a population-based study in the United States. Pancreas,39, 458–462.
Lind, M., Garcia-Rodriguez, L. A., Booth, G. L., Cea-Soriano, L., Shah, B. R., Ekeroth, G.,et al. (2013). Mortality trends in patients with and without diabetes in Ontario,Canada and the UK from 1996 to 2009: a population- based study. Diabetologia, 56,2601–2608http://dx.doi.org/10.1007/s00125-013-3063-1 (A corrected version ofthe paper is available at:).
Luo, J., Xiao, L., Wu, C., Zheng, Y., & Zhao, N. (2013). The incidence and survival rate ofpopulation-based pancreatic cancer patients: Shanghai Cancer Registry 2004–2009. PLoS One, 8(10), e76052.
McMurray, J. (2013). Vildagliptin shows no adverse effect on ejection fraction indiabetic patients with HF. Presented at the Heart Failure Congress 2013, Lisbon,Portugal, May 25–28, 2013 (abstract).
Monami, M., Ahrén, B., Dicembrini, I., & Mannucci, E. (2013). Dipeptidyl peptidase-4inhibitors and cardiovascular risk a meta-analysis of randomized clinical trials.Diabetes, Obesity & Metabolism, 15, 112–120.
Nauck, M. A. (2013). A critical analysis of the clinical use of incretin-based therapies:the benefits by far outweigh the potential risks. Diabetes Care, 36, 2126–2132.
Neal, B., Perkovic, V., de Zeeuw, D., Mahaffey, K. W., Fulcher, G., Stein, P., et al. (2013).Rationale, design, and baseline characteristics of the Canagliflozin Cardiovascular
Assessment Study (CANVAS)–a randomized placebo-controlled trial. AmericanHeart Journal, 166, 217–223.
ORIGIN Trial Investigators, Gerstein, H. C., Bosch, J., Dagenais, G. R., Díaz, R., Jung, H.,et al. (2012). Basal insulin and cardiovascular and other outcomes in dysglycemia.The New England Journal of Medicine, 367, 319–328.
Ou, X., O'Leary, H. A., & Broxmeyer,H. E. (2013). Implications ofDPP4modification of proteinsthat regulate stem/progenitor and more mature cell types. Blood, 122, 161–169.
Preis, S. R., Hwang, S. J., Coady, S., Pencina, M. J., D'Agostino, & Savage, P. J. (2009).Trends in all-cause and cardiovascular disease mortality among women and menwith and without diabetes mellitus in the Framingham Heart Study, 1950 to 2005.Circulation, 119, 1728–1735.
Sattar, N. (2013). Revisiting the links between glycaemia, diabetes and cardiovasculardisease. Diabetologia, 56, 686–695.
Scheen, A. J. (2013). Cardiovascular effects of dipeptidyl peptidase-4 inhibitors: fromrisk factors to clinical outcomes. Postgraduate Medicine, 125, 7–20.
Scirica, B. M., Bhatt, D. L., Braunwald, E., Steg, P. G., Davidson, J., Hirshberg, B., et al.(2013). SAVOR-TIMI 53 Steering Committee and Investigators. Saxagliptin andcardiovascular outcomes in patients with type 2 diabetes mellitus. The New EnglandJournal of Medicine, 369, 1317–1326.
UK Prospective Diabetes Study (UKPDS) Group (1998). Intensive blood-glucose controlwith sulphonylureas or insulin compared with conventional treatment and risk ofcomplications in patients with type 2 diabetes (UKPDS 33). Lancet, 352, 837–853.
White, W. B., Cannon, C. P., Heller, S. R., Nissen, S. E., Bergenstal, R. M., Bakris, G. L., et al.(2013). EXAMINE Investigators. Alogliptin after acute coronary syndrome inpatients with type 2 diabetes. The New England Journal of Medicine, 369, 1327–1335.
Yadav, D., & Lowenfels, A. B. (2013). The epidemiology of pancreatitis and pancreaticcancer. Gastroenterology, 144, 1252–1261.
Yang, L., He, Z., Tang, X., & Liu, J. (2013). Type 2 diabetes mellitus and the risk of acutepancreatitis: a meta-analysis. European Journal of Gastroenterology & Hepatology,25, 225–231.
Guntram SchernthanerDepartment of Medicine I, Rudolfstiftung Hospital, Vienna, Austria
E-mail address: [email protected]
Naveed SattarInstitute of Cardiovascular & Medical Sciences,
BHF Glasgow Cardiovascular Research Centre, University Of Glasgow
Available online xxxx