Embed Size (px)
Citation preview

Let’s take another look at our problem cases
PAUL V. REID, D.D.S.
B,ryn Mawr, Pa.
THE theme of this meeting-instability in orthodontic results with the implica- tion of a degree of failure to achieve or ma,intain the perfection we desired- has not been belabored and there are many ways in which it can be discussed without risk of repetition. It would probably be possible to present a carefully selected group of ca,se reports, each with only the slightest suggestion of a localized relapse. The implication would be obvious and would have the salut,ary effect of demonstrating that perfection is a will-of-the-wisp and that we should not worry about it. It would likewise be possible to collect a. group of cases that would be most inappropriate for use in support of a new technique or treatment philosophy. These, to paraphrase the musical record titles, would con- stitute “Cases Not To Pass the American Boards With. ” An essayist could be less disturbed and far more objective if he were to discuss the problem cases of others, for it is much easier to pick out what someone else has overlooked in a case than to be objective wit,11 a trca.tment problem of our own. We view such situations with a different a,nd less inhibited outlook. Probably a, general practitioner, who sees orthodontic results years out of retention, might givt: the fairest and most objective appraisal of all. While he might, be justly critical of procedures that he thought could contribute to premature breakdown of the denture, he would probably be quite tolerant. of moderate relapse in tooth alignment. I have a feeling that, his concept of orthodontic objectives would place function and health well ahead of esthetics. There would also be the nonclinical approach covering aspects of growth and development that are essential but elusive in the considera.tion of any case, and the histologic and experimental aspects of t,reatment and relapse could be detailed to explain, for example, why extraction spaces reopen and rotations are prone to regress.
In my opinion, the value of a symposium lies in utilizing each essayist to the best of his ability by not confining him to just one segment of the topic
Presented before the Northeastern Society of Orthodontists in Montreal, Quebec, Oct. 25, 1965.
266
Volume 5 2 Number 4
Problem cases 267
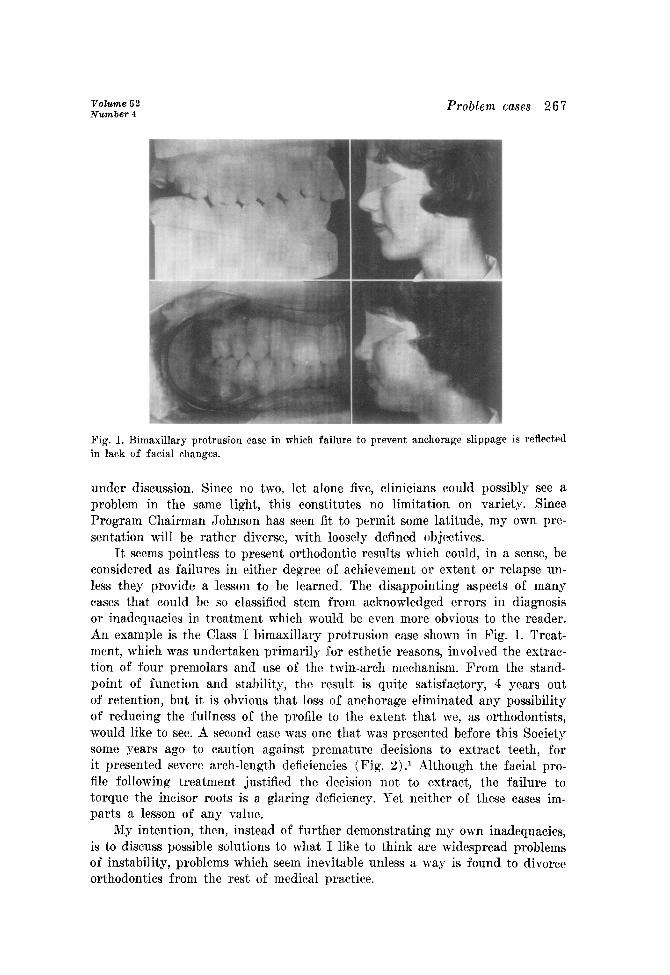
Fig. 1. Bimaxillary protrusion case in which failure to prevent anchorage slippage is reflected in lack of facial changes.
under discussion. Since no two, let alone five, clinicians could possibly see a problem in the same light, this constitutes no limitation on va’riety. Since Program Chairman Johnson has seen fit to permit some latitude, my own pre- sentation will be rather diverse, with loosely defined objectives.
It seems pointless to present orthodontic results which could, in a sense, be considered as failures in either degree of achievement or extent or relapse un- less they provide a lesson to be learned. The disappointing aspects of many cases that could be so classified stem from acknowledged errors in diagnosis or inadequacies in treatment which would be even more obvious to the reader. An example is the Class I bimaxillary protrusion case shown in Fig. 1. Treat- ment, which was undertaken primarily for esthetic reasons, involved the extrac- tion of four premolars and use of the twin-arch mechanism. From the stand- point of function and stability, the result is quite satisfactory, 4 years out of retention, but it is obvious that loss of anchorage eliminated any possibility of reducing the fullness of the profile to t.he extent that we, as orthodontists, would like to see. A second case was one that was presented before this Society some years ago to caution against premature decisions to extract teeth, for it presented severe arch-length deficiencies (Fig. 2) .I Although the facial pro- file following treatment justified the decision not to extract, the failure to torque the incisor roots is a glaring de.ficiency. Yet neither of these cases im- parts a lesson of any value.
My intention, then, instead of further demonstrating my own inadequacies, is to discuss possible solutions to what I like to think are widespread problems of instability, problems which seem inevitable unless a way is found to divorce orthodontics from the rest of medical practice.
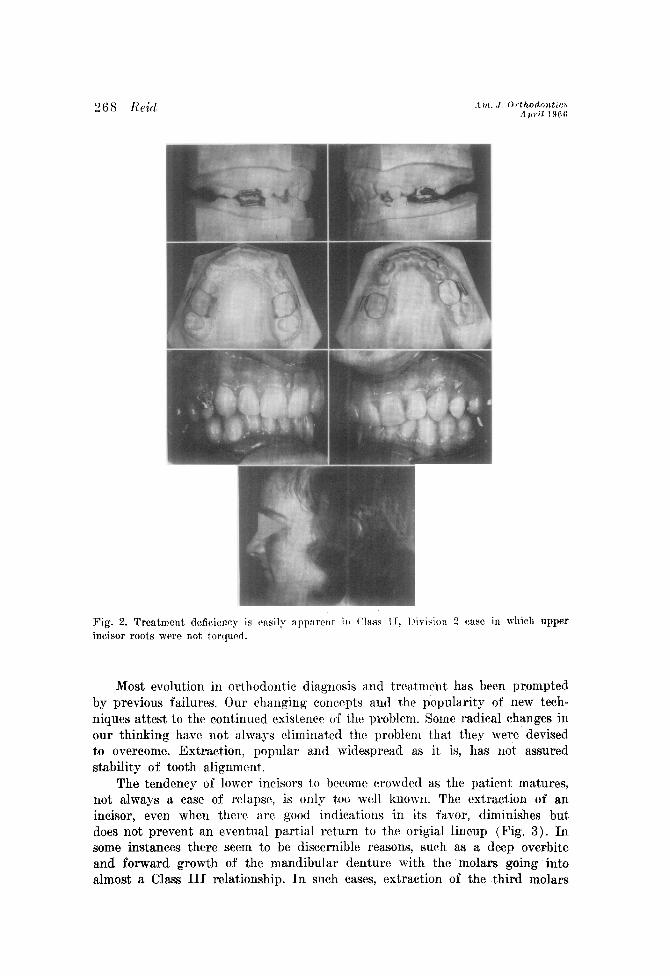
Fig. 2. Treatment deficiency is r>asily appwnt il l (‘1a.w 1 I, I jivision 2 case in which upper incisor roots \vvere not torqucd.
Most evolution in ort.hodontic diagnosis and treatment has been prompted by previous failures. Our changing concepts and t,hc popularity of new tech- niques attest to the continued existence of the problem. Some radical changes in our thinking have not always eliminated the problem that t,hey were devised to overcome. Extraction, popular and widespread as it is, has not assured stability of tooth alignment,
The tendency of lower incisors to become crowded as the patient matures, not always a case of rela,pse, is only t,oo well known. The ext.raction of an incisor, even when there are good indications in its favor, diminishes but does not prevent an eventual partial ret,urn to the origial lineup (Fig. 3). In some instances there seem to be discernible reasons, such as a deep overbite and forward growth of the mandibular denture with the molars going into almost a Class III relationship. In such cases, extraction of the third molars
Volume 52 Number 4
Problem cases 269
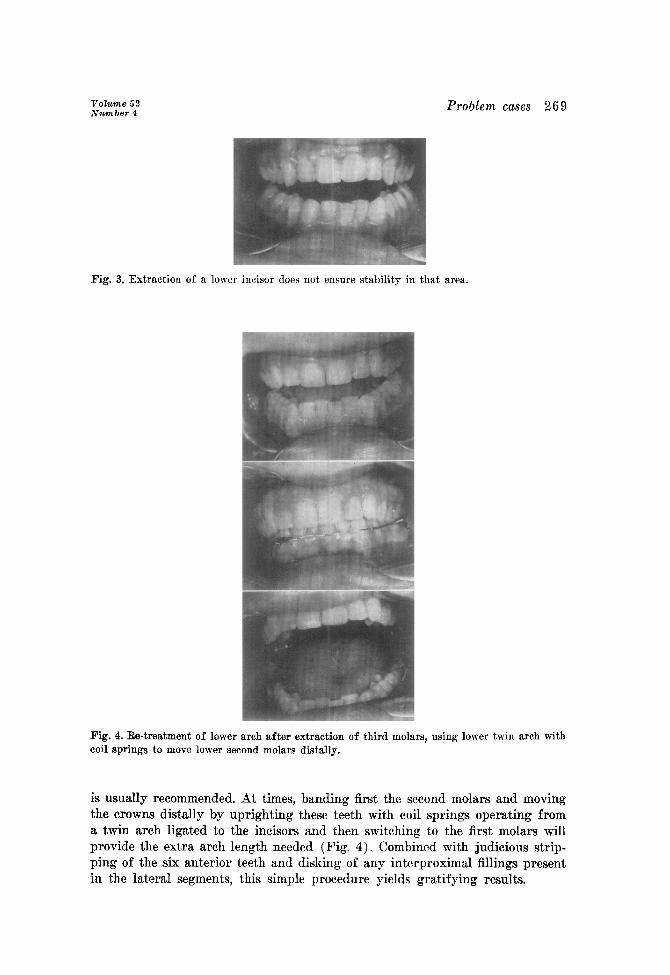
Fig. 3. Extraction of a lower incisor does not ensure stability in that area.
Fig. 4. Re-treatment of lower arch after extraction of third molars, using lower twin arch with coil springs to move lower second molars distally.
is usually recommended. At times, banding first the second molars and moving the crowns distally by uprighting these teeth with coil springs operating from a twin arch ligated to the incisors and then switching to the first molars will provide the extra arch length needed (Fig. 4). Combined with judicious strip- ping of the six anterior teeth and disking of any interproximal fillings present in the lateral segments, this simple procedure yields gratifying results.
For the lower arch T have alkvays atlvocated prolor~~ed rettllltion. 01’ at least periodic observation, even if thcrc \vas no original arch-length &ficisnc3)-. With an;r- original crowding, I recommend that, a canine-to-callill(l srction 1~ left in place until after the third mola,rs have erupted illto func*tion or have, been extracted. Whether or not thestb t&h can influenchc$ the> aligmnttnt. ok’ lower incisors, this routine seems to serve a useful function in my office. 11 the parents insist that this type of retention be removed before the third molar problem has been resolved, they must accept, some responsibilit~~. If they accept m.y recommendation, long retention is ensured. Now that prolonged rcten- tion has become respectable, t,hesr commchnts should 1)~ vcar*y mucall in line with current practice. Where lower incisors have crowdc~l up and the patient can- not be held responsible, as in the case in \vhich no louver retainer was used, I will always offer to replace the lower appliance and attempt realignment, but, not until the third molars have been etxtract,ed. It, is surprising how the en- t,husiasm for re-treatment recedes with this stipulation! Alt,hough this is said with tongue in cheek, it is nevertheless a I’act.
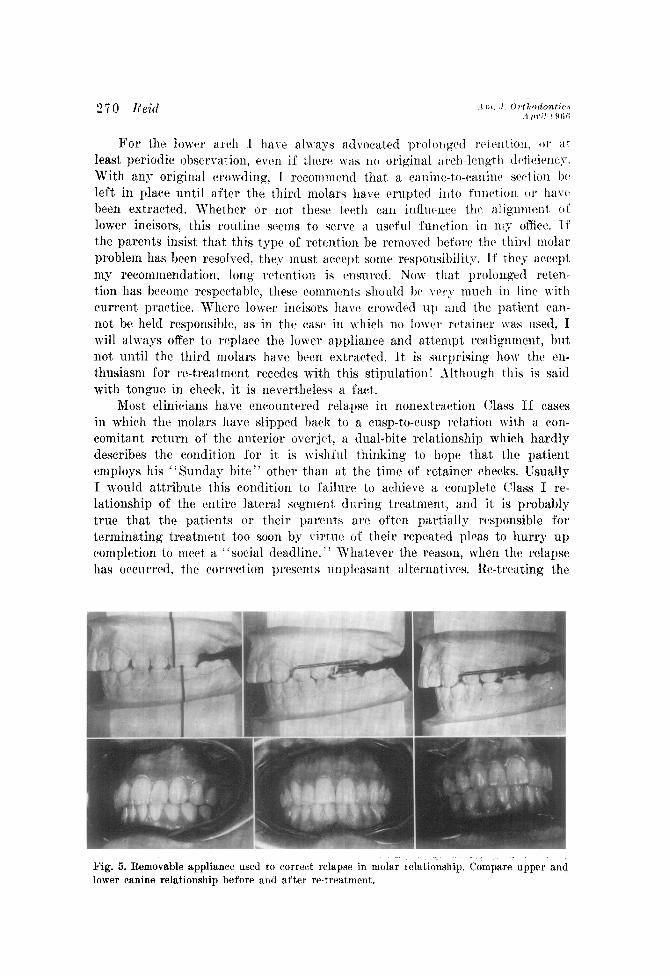
Most clinicians have encountered relapse in nonestraction Class 11 cases in which the molars have slipped back to a cusp-to-cusp relation with a con- comitant return oi’ the anterior overjet. a dual-bite relat,ionship which hardly describes the condition for it is wishful thinking to hope that the patient employs his “Sunday bite” other than at, t.he time of retainer checks. Usually I would attribute this condit,ion to failure to achieve a complete (Yass I re- lationship of the entire lateral segment. during treatment,, and it is probably true that the patients or their parents arc often partially responsible fol terminating treatment too soon bq’ virtue of their repeated pleas to hurry up completion to meet a “social deadline. ” What,ever the reason, when the relapse has occurred, the caorreetion presents unpleasant alternatives. Re-treating the
Fig. 5. Removable appliance used to correct relapse in molar relationship. Compare upper and lower canine relationship before and after re-treatment.
T’olume 52 Number 4
Problem cases 27 1
case is so repugnant to a teen-ager that, although the parent is placated, the orthodontist may have alienated a friend. If re-treatment is to be successful, it is mandatory to overdrive the distal segments; if upper third molars are present and not too close to eruption, extraction of the second molars makes this relatively easy. To make it more acceptable to the patient, the entire re- treatment can be done without fixed labial arches. First, the molars are banded and driven distally into almost a Class III relationship by coil-spring force directed against the buccal tubes via 0.030 inch labial extensions from a Hawley retainer (Fig. 5). The patient can easily insert these into the buccal tubes, thus compressing the strong coil springs.
Premolars and canines can then be retracted with a lingual arch, but care must be taken to take back one tooth at a time. The lingual arch is stopped distal to each canine as the premolars are being moved and distal to each laterial incisor as the canines are finally placed. The incisors can then be re- tracted by going back to the Hawley appliance with a latex elastic labial sec- tion. It must be pointed out, however, that this unpleasant dilemma can be eliminated to a large extent by overtreatment in the first place. Also, although I fully approsve of treating a great many rather extreme Class II cases with- out extracting premolars, the removal of upper second molars is often indicated. Since this can be done during treatment, and not necessarily at the outset, it can be reserved as an “ace in the hole” if one wishes to start conservatively.
An isolated detail of relapse is the reopening of a diastema between the maxillary central incisors. We have all solved this in many ways. The follow-
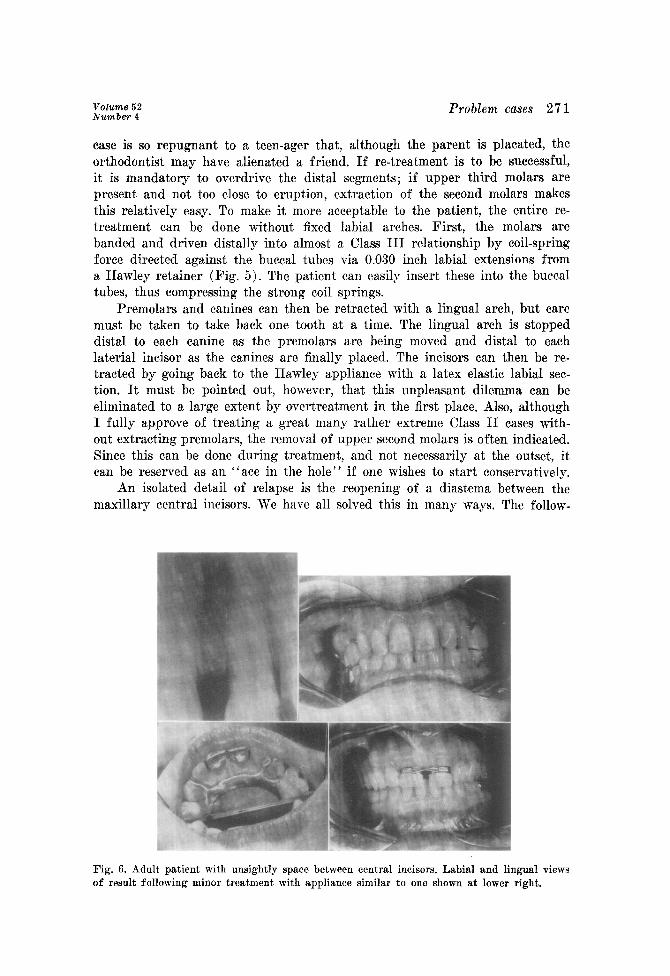
Fig. 6. Adult patient with unsightly space between central incisors. Labial and lingual views of result following minor treatment with appliance similar to one shown at lower right.
272 Reid
ing case is presented primarily to illust~ratc~ one way 01' handling this j)robl~ni in the adult patient.. It may not always hr il qlL&ion oI’ rc~l;~pse ; quittb Crec~uerttl~ a patient’s mother, who has been plaguetl all her lift: by this unsightly condi- tion, seeks correction. The uncrrtainty o I’ rcltention makes one rrlnctant to treat this relatively minor problem.
An x-ray film (Fig. 6) showing such a diastema in a SO-year-old patient was sent to my 0ffic.e by the paticnt.‘s dentist with a note requesting that. I merely close this one space and lcavcl the retention problem to him. Space closure was easily achieved by placing Johnson bands on the central incisors, with a ribbon-arch section serving as a trolley and elastic ligature used as the motivating force. The operative dental procedure involved placement of pinlays on the two incisors. \Vith the USC of a pin alignc~r, called a Ponto- structor, a single casting can bc made or individual ones can btt soldered. The patient,‘8 complete satisfaction with the simplicity and speed with which her problem was eliminated has conrincrd rno t,hat, previous effort,s to move all six anterior teeth together and to construct inlays for the fitxt, premolars have not been warranted in adult, patients with similar problems. In the past, it
has been difficult in our area to persuade dentists to tie incisors together. This would seem to be the most feasible wag to handle the older patient, in whom
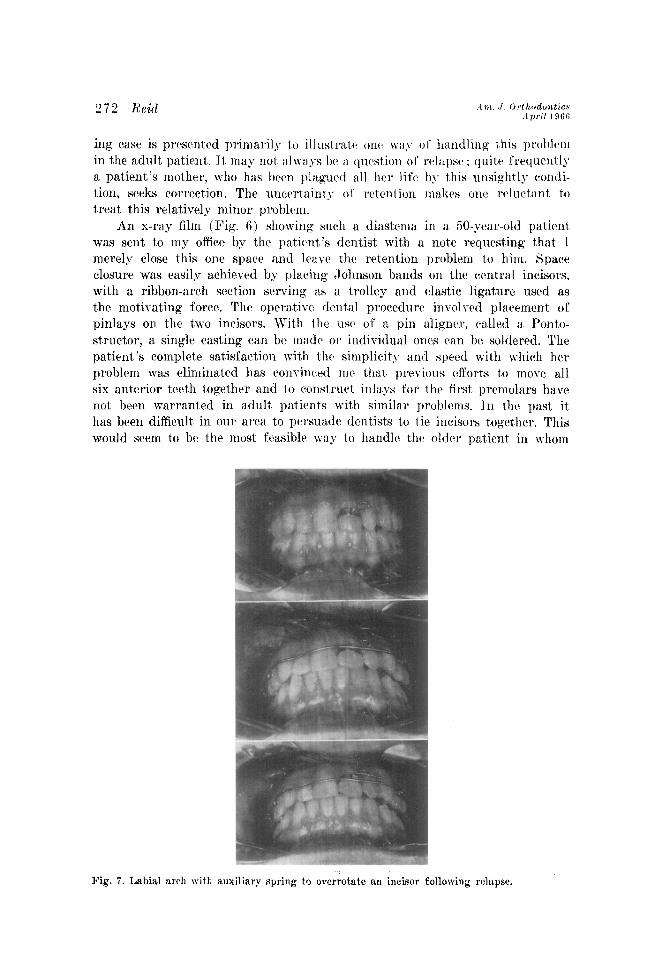
Fig. 7. Labial arch with auxiliary spring to overrotate an incisor following relapse.
Volume 52 Number 4
Problem cases 273
the occlusion is good and the diastema is due entirely to a tooth-size disharmony between the arches.
When one incisor has a persistent tendency to relapse, overrotation is the best corrective measure. For this purpose, a labial arch with a finger spring, as advocated by A. F. Jackson2 engaging a rotation attachment on the tooth in question does the job rapidly and effectively. The point of contact between the arch wire and the tooth acts as a fulcrum. The degree of overrotation is left to the operator’s discretion (Fig. ‘7).
The foregoing suggestions may seldom have application to a particular prob- lem in your practice, or you may have far better solutions when the occasion arises. In any event, none of the problems themselves are of great concern and, collectively, they represent but a segment of the general topic with which we are concerned today.
My prima.ry objective is to discuss our problem eases in a more general way. It would be desirable for all of us to look at some of our results, both good and not so good, a second time. By doing so, we might put the terms success and failure as applied to our treated cases into proper perspective.
We have all had results which disturb us because we failed to reach the objectives that we set for ourselves. This is all aside from the patients’ or parents’ reaction, for, in general, we seem to satisfy their hopes. Quite probably we have other cases in which we achieved limited success but which do not con- cern us because we are either unaware of or at least unconcerned by our shortcomings. Each of us has his own criteria for making such a judgment. Unfortunately, we are much more aware and prone to be highly critical when observing finished cases treated by our colleagues, as documented by casts, photographs, and tracings which do not exhibit perfectio8n in incisor align- ment and posterior interdigitation, marked improvement in facial profile, and close conformity to cephalometric means. We are swayed too much by the end result, and we give too little consideration to the original condition.
I am emboldened to speak on this subject because during the past several years I have had the opportunity to appraise more than my share of ortho- dontic results produced by a widely distributed cross section of the younger experienced orthodontists in this country. The degree of perfection achieved in the majority of these finished cases is most satisfying and, at the same time, disturbing to the observer’s ego. Their general excellence is a tremendous trib- ute to the quality of current orthodontic training. Nonetheless, objective crit- icism cannot overlook the fact that the degree of difficulty of many of the cases which turned out so successfully was not great, nor was the diversity such that it represented a true cross section of any average practice. It seems illogical, in judging success or failure, to base such a judgment, upon the end result alone and to exclude any consideration of the starting point. Limitations in- herent in the ease, or the absence of such limitations, should influence our sub- jective appreciation of the result.
The case shown in Fig 8 illustrates the need to assess all the pertinent factors. The patient, a boy aged 91/2 years in the Hellman III B stage, came to the clinic at the University of Pennsylvania with a severe Class II, Division
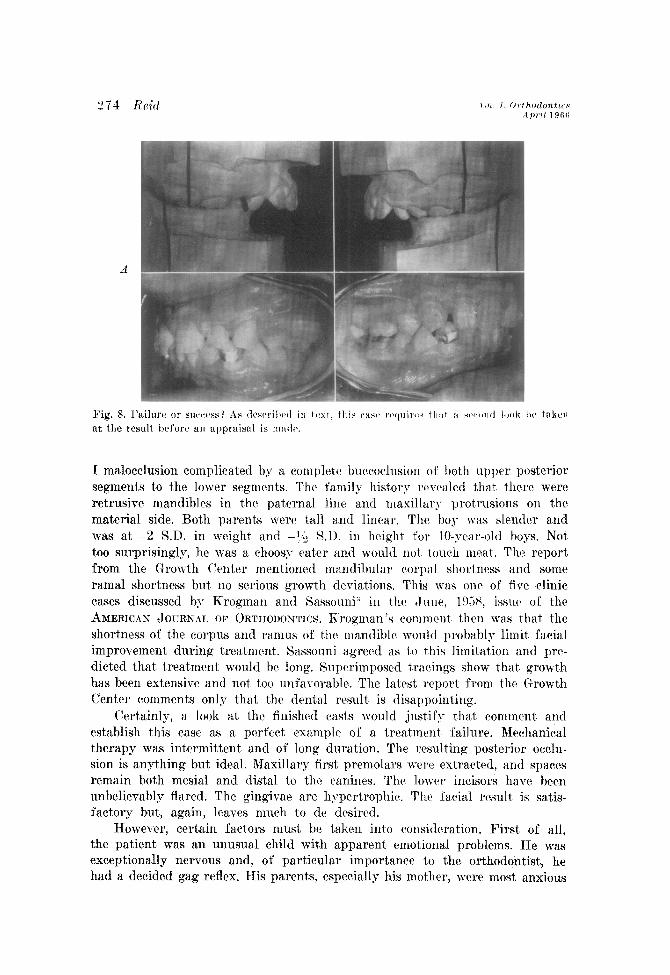
A
I malocclusion complicated hy a complctc huccoclusion OF both upper posterior segments to the lower segments. The family hist,or,v rerraled that there were retrusive mandibles in the paternal line and masillar~- protrusions on the material side. Bot,h parents were tall and linear. The boy was slender and was at -2 S.D. in weight and -?$ 8.1). in height for IO-,vcar-oltl boys. Not too surprisingly, he was a choosp eater and would not. touch meat. The report from the Growth Center mentioned mandibular corJ)>ll shortness and some ramal shortness but no serious growth deviations. This was one of fire clinic cases discussed by Krogman and Sassouni” in t,hr ~Jnue, 1958, issucl of the AMERICAN cJ~~~~~~ OE' ORTHODONTICS. Krogman’s comment then was that the shortness of the corpus and ramus of th(l ma.ndihlt~ would probably limit facial improvement during treatment. Sassouni agreed as to t>his limitation and prc- dieted that treatment would be long. Superimposed tracings show t,hat. growth has been extensive and not too unfavorable. The latest report, from the (Growth Center comments only that, the dental result, is disappointing.
Certainly, a look at the finished casts would justify that comment and establish this case as a perfect example of a treatment, Sailure. Mechanical therapy was int,ermittent and of long duration. The resulting posterior occlu- sion is anything but ideal. Maxillary first, premola.rs were extracted, and spaces remain both mesial and distal to the canines. The lower incisors have been unbelievably flared. The gingivae are hypertrophic. The facial result is satis- factory but, again, leaves much to de desired.
However, certain factors must. he taken into consideration. First of all, the patient was an unusual child with apparent emotional problems. He was exceptionally nervous and, of particular importance to the orthodontist, he had a decided gag reflex. IIis parents, especially his mother, were most anxious
Volume 52 Number 4
Problem cases 275
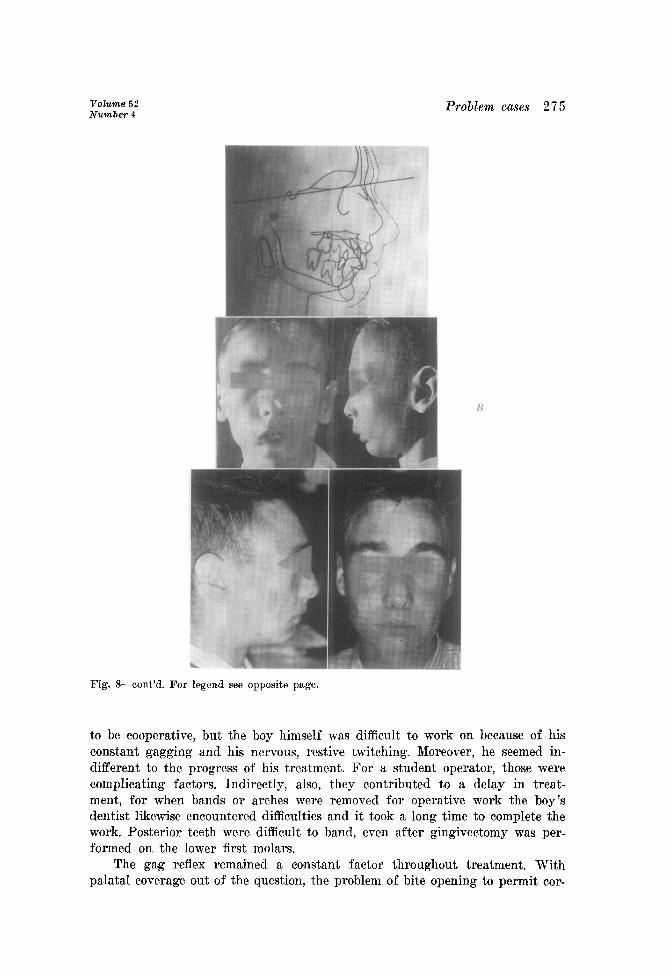
B
Fig. G-eont’d. For legend see opposite page.
to be cooperative, but the boy himself was difficult to work on because of his constant gagging and his nervous, restive twitching. Moreover, he seemed in- different to the progress of his treatment. For a student operator, those were complicating factors. Indirectly, also, they contributed to a delay in treat- ment, for when bands or arches were removed for operative work the boy’s dentist likewise encountered difficulties and it took a long time to complete the work. Posterior teeth were difficult to band, even after gingivectomy was per- formed on the lower first molars.
The gag reflex remained a constant factor throughout treatment, With palatal coverage out of the question, the problem of bite opening to permit cor-
A ~1. J. iirthodontics April 1966
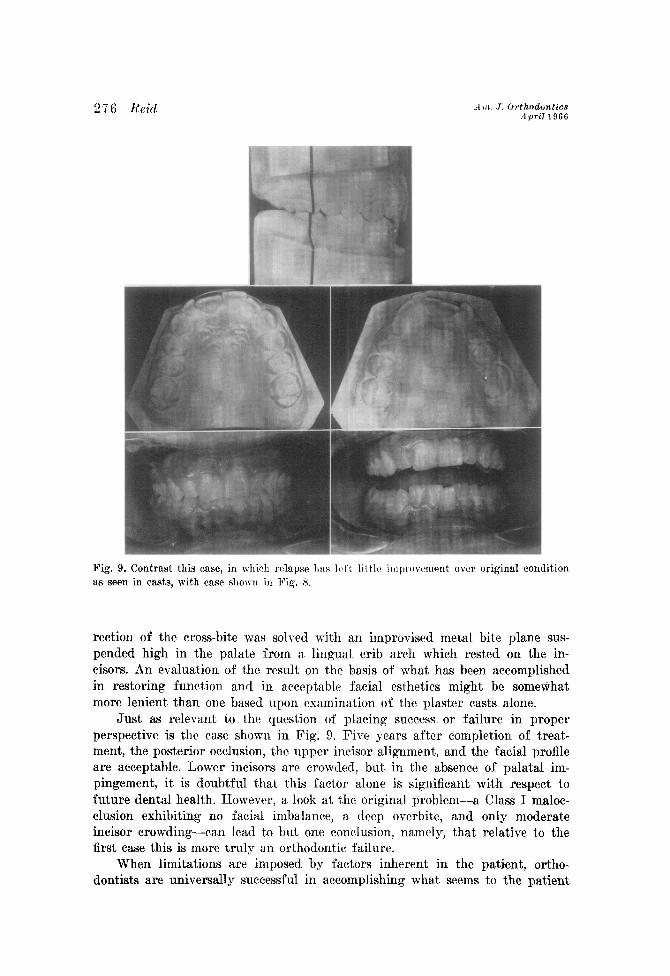
Fig. 9. Contrast this case, in which relapse 11:rs Itsft little improvement over original condition as seen in cwts, with ease shown in Fig. X.
rection of the cross-bite was solved with an improvised metal bite plane sus- pended high in the palate from a lingual crib arch which rested on the in- cisors. An evaluation of the result on t.he basis of what has been accomplished in restoring function and in acceptable fa.cial esthetics might be somewhat more lenient than one based upon examination of the plaster casts alone.
Just as releTant to the question of placin g success or failure in proper perspective is the case shown in Fig. 9. Five years after completion of treat- ment, the posterior occlusion, the upper incisor alignment, and the facial profile are acceptable. Lower incisors are crowded, but in the absence of palatal im- pingement, it is doubtful that this factor alone is significant with respect to future dental health. However, a look at the original problem-a Class I maloc- clusion exhibiting no facial imbalance, a deep overbite, and only moderate incisor crowding-can lead to but one conclusion, namely, that relative to the first case this is more truly an orthodontic failure.
When limitations are imposed by factors inherent in the patient, ortho- dontists are universally successful in accomplishing wha.t seems to the patient
Volume 5 2 Number 4
Problem cases 277
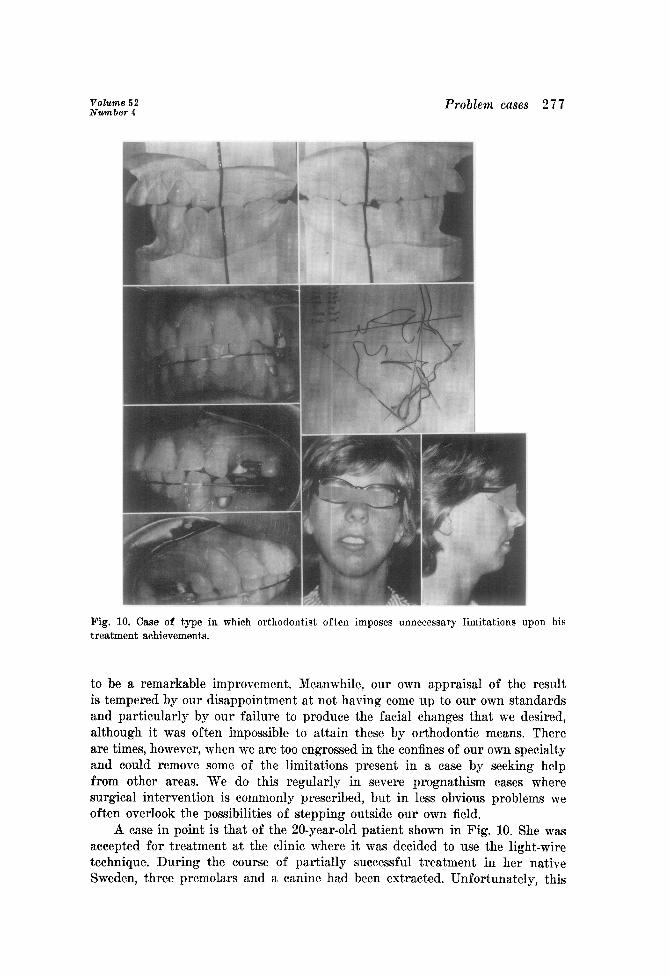
Fig. 10. Case of type in which orthodontist often imposes unnecessary limitations upon his treatment achievements.
to be a remarkable improvement. Meanwhile, our own appraisal of the result is tempered by our disappointment at not having come up to our own standards and particularly by our failure to produce the facial changes that we desired, although it was often impossible to attain these by orthodontic means. There are times, however, when we are too engrossed in the confines of our own specialty and could remove some of the limitations present in a case by seeking help from other areas. We do this regularly in severe prognathism cases where surgical intervention is commonly prescribed, but in less obvious problems we often overlook the possibilities of stepping outside our own field.
A case in point is that of the 20-year-old patient shown in Fig. 10. She was accepted for treatment at the clinic where it was decided to use the light-wire technique. During the course of partially successful treatment in her native Sweden, three premolars and a canine had been extracted. Unfortunately, this
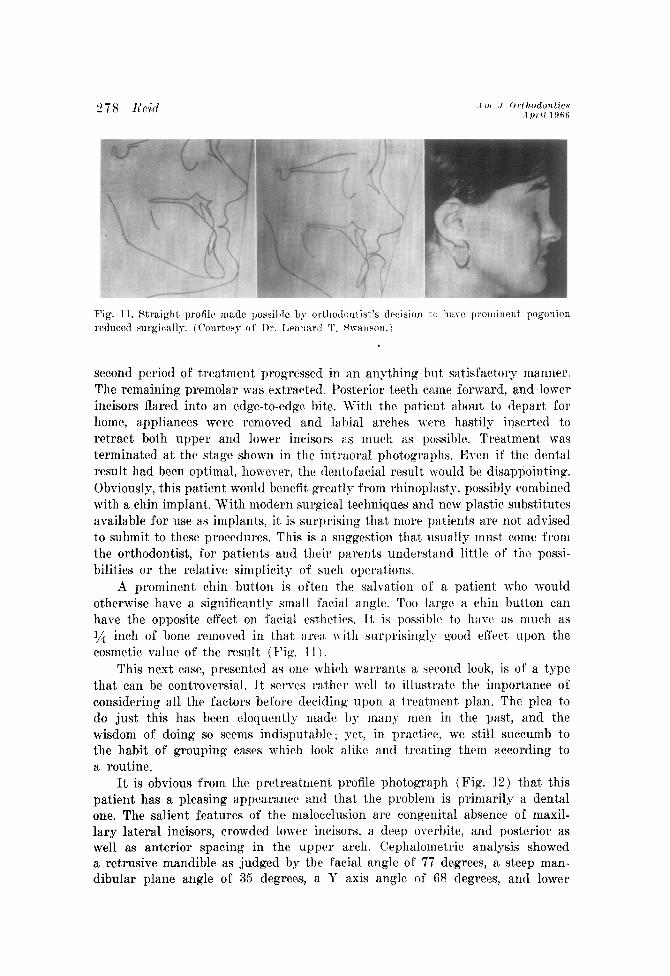
second period of treatment progressed in an anything but satisfactory manner. The remaining premolar was extracted. Posterior teeth rame forward, and lower incisors flared into an edge-to-edge bite. With the patient about to depart for home, appliances were removed and labial arches wrrc hastily insert,ed t.o retract both upper and lower incisors as much as possible. Treatment, was terminated at the stage shown in the intraoral photographs. Even if the dcnt,al result had been optimal, however, the denlofacial result would be disappointing. Obviously, this patient would benefit. greatly from rhinoplast,y, possibly combined with a chin implant. With modern surgical techniques and new plastic substitutes available for use as implants, it. is surprising that. more patients are not advised to submit to these procedures. This is iI suggestion that> usually must come from the orthodontist, for pabients and their parents underst,and little of the possi- bilities or the relative simplicit,y of such operations.
A prominent chin button is often the salvation of a patient. who would otherwise have a significantly small facial angle. Too large a. chin button can have the opposite effect on facial esthet.ic~s. Tt is possiblr to have as much as I/$ inch of bone removed in that arca \vith surprisingly good effect upon the cosmetic value of the result (Fig. 11 )
This next case, presented as one which warrants a sc~nd look, is of a t,ype that can be controversial. It serv(‘s rather well t.o illust.rate the importance of considering all the factors before decidin, w upon a treat.ment plan. The plea to do just this has been eloquently made by many men in the past,, and the wisdom of doing so seems indisputable; yet, in practice, we still succumb to the habit of grouping cases which look alike and treating them according to a routine.
It is obvious from the pretreatment profile photograph (Fig. 12) that this patient has a pleasing appearance and that the problem is primarily a dental one. The salient features of the malocclusion arc congenital absence of maxil- lary lateral incisors, crowded lower incisors, a deep overbite, and posterior as well as anterior spacing in the upper arch. Cephalometric analysis showed a retrusive mandible as judged by the facial angle of 77 degrees, a steep man- dibular plane angle of 35 degrees, a Y axis angle of 68 degrees? and lower
Volume 52 Number 4
Problem cases 279
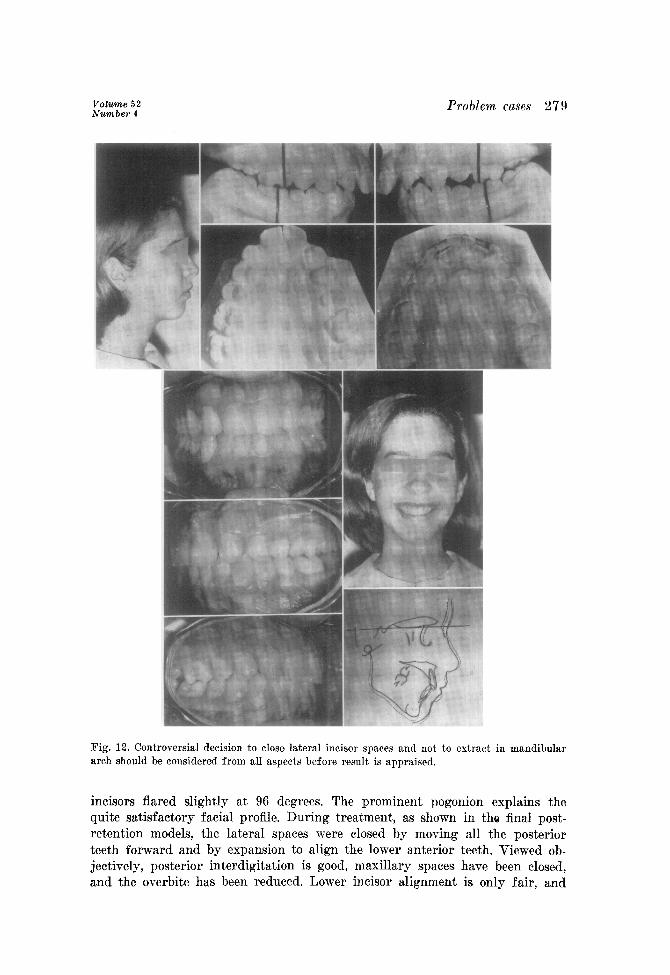
Fig. 12. Controversial decision to close lateral incisor spaces and not to extract in mandibular arch should be considered from all aspects before result is appraised.
incisors flared slightly at 96 degrees. The prominent pogonion explains the quite satisfactory facial profile. During treatment, as shown in the final post- retention models, the lateral spaces were closed by moving all the posterior teeth forward and by expansion to align the lower anterior teeth. Viewed ob- jectively, posterior interdigitation is good, maxillary spaces have been closed, and the overbite has been reduced. Lower incisor alignment is only fair, and
the stability of the lateral incisors can he qucstionctl. The original facial photo- graph showed a well-balanced face, whi~~h was not as retrognathic as the tracing would lead one to expect, Growth was mainly downward, as expected. One could point out that the tendency of t,hc lower lateral incisors to relapse shows that the lower premolars should have been ext,racted. but this does not ncces- sarily ensure against the same thing happening. The de&ion not, to -rtaplace the lateral incisors is subject to question, for some hold to t.hct opinion t1:a.t space closure is contraindicated, particularly for the female patient. It is this aspect of the case that concerns us Mar. There arc pc&cctly good ar~lmcnts to show that unless room is made for upper lateral incisors, the basic interarch harmony essential to sat.isfactory esthetics cannot exist. It. would have to be conceded, however, that some replacements might restore this same basic harmony and yet fall far short of producing the cosmetic effect desired. Even the finest prosthetic restorations lack the perfect, translucency of the natural teeth. If the replacements ha,vc other d&ciencies as well, the entire effect, can be most disappointing, sometimes undoing the best efforts of the orthodontist. The case that we have been discussing was treated in t,he clinic, and the ex- pense of placing bridges was a, factor to be considered. Posttreatment photo- graphs indicate an acceptable esthetic result. For another case this rnight be the wrong treatment plan, but. in this instance it would seem to be appro- priate.
It is not, the relapse of lower incisors, of rotations in general, or retro- gressive changes in mesiodista,l arch relationship, frustrating as they ma.y be, that should be of major conc.ern in orthodontics today. Nor is it the presence of obvious limitations in the individual patient. In the majority of cases when relapse occurs it does not mean that treatment has failed, except in a, relative sense. As for inherent limita.tions, orthodontists have always managed the majority of such cases in at least a satisfactory manner. There is a potentially more insidious type of failure which stems from what is sometimes almost an obsession with all-or-none orthodontic treatment which has a.s its goal perfec- tion in tooth alignment and conformity of dental and facial pattern to a pre- conceived norm. This obsession sometimes tends to blind one to the real respon- sibilities of our specialty. As so well spelled out by Dewel in the brochure pre- pared by his Council on Education, the principal objective of orthodontics is the prevention of malocclusion and its principal rcs~onsihility is’ the super- vision of growth and derclopmtnt of the dentiCon and its associated facial structure from birth to dental maturity. When WC allow onrselves to become more concerned with the efficiency of appliances in closing spaces, managing overbites, and accomplishing ideal cuspal relationships than with the guidance of the developing dentition and thr timing of our interceptive or corrective procedures in a developing malocclusion, WC may have increased our percentage of successful results-but have w fulfilled our prime responsibility as members of a health profession ?
The possibilities of deciduous-and mixed-dentition treatment are far t,oo often overlooked. Admittedly, primary treatment in the majority of cases is not final, and it is not always feasible, but more than occasionally even the
Volume 52 Number 4
Problem cases 281
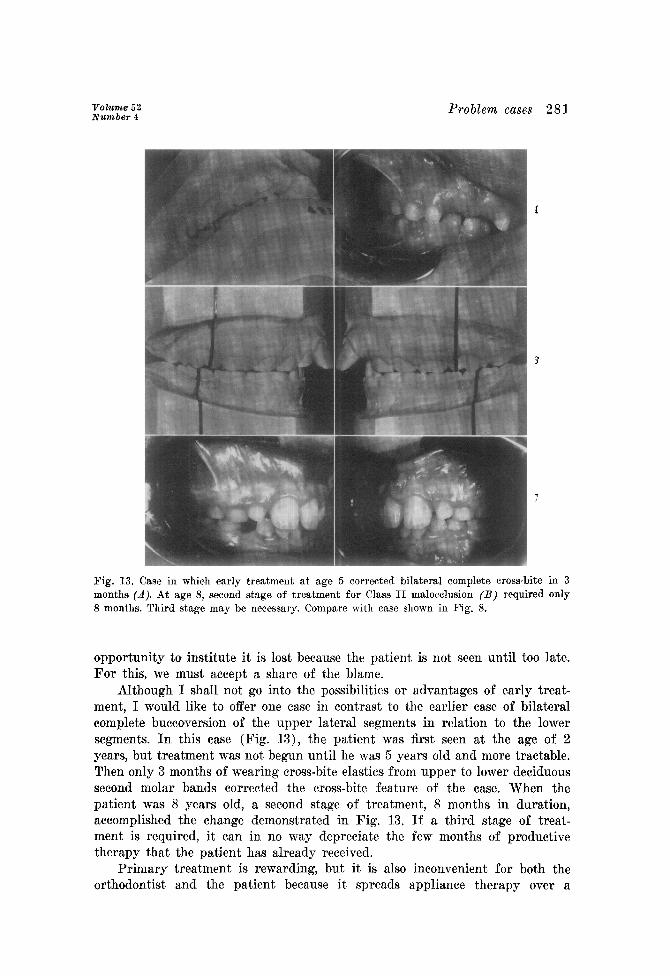
Fig. 13. Case in which early treatment at age 5 corrected bilateral complete cross-bite in 3 months c.4). At age 8, second stage of treatment for Class II malocclusion (B) required only 8 months. Third stage may be necessary. Compare with case shown in Fig. 8.
opportunity to institute it is lost because the patient is not seen until too late. For this, we must accept a share of the blame.
Although I shall not go into the possibilities or advantages of early treat- ment, I would like to offer one ease in contrast to the earlier case of bilateral complete buccoversion of the upper lateral segments in relation to the lower segments. In this case (Fig. 13)) the patient was first seen at the age of 2 years, but treatment was not begun until he was 5 years old and more tractable. Then only 3 months of wearing cross-bite elastics from upper to lower deciduous second molar bands corrected the cross-bite feature of the case. When the patient was 8 years old, a second stage of treatment, 8 months in duration, accomplished the change demonstrated in Fig. 13. If a third stage of treat- ment is required, it can in no way depreciate the few months of productive therapy that the patient has already received.
Primary treatment is rewarding, but it is also inconvenient for both the orthodontist and the patient because it spreads appliance therapy over a
necessarily long period 01’ tiinrb. 1 t is i1ls0 open 10 111tf argument that oft (sn after a severe condition has I)cen carrircl to a stag0 th:r t. is far fronl c~onlpl~%~, the patient, does not seek the prc>scribcvl second stagr of trratmc~nt and has therefore been “shortchanged. ’ ’
In rebuttal, 1 can only say that i-f a patient rccc4vrs sufficient, treatment in a primary phase to remove him from the category of a dentofacially handi- capped person and dots not choose to seek the final E>has( of treatment, the orthodontist should not bc too disturbed.
If this presentation has covered the general thcmc of discussion in loose fashion, it was prepared with the full realization that one person can at best offer only a few suggestions for coping wit,h t,he inevitable disapp0intment.s that we all have in our clinical therapy. Ort,hodontics would be unique in the field of medical practice if these problems did not exist . At times we must accept full responsibility for results which do not measure up to our own standards. Aga.in, factors over which we have little control may have imposed limitations on our treatment.
We certainly learn from our own errors, and as long as we can differentiate between true limitations and self-imposed limitat,ions which stem from con- fining our t,hinking to stereotyped c,hannels, we should not be too self-critical. Finally, if we stop to remind ourselves periodically of the objecti\-es that we really seek in orthodontics, we may be a bit. less complatynt about our SUCCCSSHS.
REFERENCES
1. Reid, P. V.: Extractions in the Problem Case, SM. J. ORTHOLWXTJCS 45: 30, 1959. 2. Jackson, LI. F.: The Labial Auxiliary Spring, TNT. J. ORTHonoNTla 15: 33.41, 1929. 3. Krogman, IV. &I., and Sassouni, V.: A Meaningful Tntrrptatiorr of Guowvth and Growth
Data by the C’linician, AM. .J. ORTI-IOI)(?N’I’I(‘S 44: -LlS> 195X.
864 County Line Rd.