Embed Size (px)
Citation preview

LIFESTYLE AND CVD RISK IN OLDER ADULTS THE AMERICAN JOURNAL OF GERIATRIC CARDIOLOGY 2004 VOL. 13 NO. 3 153
There are 35 million persons aged 65 years or older in the United States, comprising approxi-
mately 13% of the population.1 These older adults are the fastest-growing segment of the population; by 2030, 70 million persons, or one in every five, will be ≥65 years old.1 Cardiovascular disease (CVD) is the leading cause of death and disability among older adults, who account for a large share of the $200 billion annual US health care expenditures for CVD.2 Better understanding of factors influenc-ing CVD risks and outcomes in this population is clearly of merit. Because atherosclerotic disease is often more advanced late in life, risk factors for CVD may be different among older individuals compared with young or middle-aged adults. Furthermore, risk factors may receive less attention when years of
remaining life are diminished. This may be particu-larly true for lifestyle factors such as diet, physical activity, and smoking. We present evidence from the Cardiovascular Health Study (CHS),3 a population-based, longitudinal cohort study of determinants of cardiovascular events among adults aged ≥65 years, and review other studies for the associations of lifestyle habits, assessed late in life, with CVD risk among older adults. We also summarize gaps in knowledge, directions for future research, and impli-cations for clinical practice and public health.
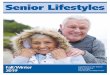
LIFESTYLE HABITS AND CVD RISKLifestyle habits may influence CVD risk via sev-eral pathways (Figure 1). Diet, physical activity, and smoking may affect subclinical disease—as assessed by peripheral vascular, cerebral vascular, and electrocardiographic or echocardiographic
Review PaperLifestyles of Older Adults: Can We Influence Cardiovascular Risk in Older Adults?
Dariush Mozaffarian, MD, MPH;1,2 Linda P. Fried, MD, MPH;5 Gregory L. Burke, MD, MS;6 Annette Fitzpatrick, PhD;3 David S. Siscovick, MD, MPH2–4 From the Channing Laboratory, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, and Departments of Nutrition and Epidemiology, Harvard School of Public Health, Boston, MA;1 Cardiovascular Health Research Unit,2 Departments of Epidemiology3 and Medicine,4 University of Washington, Seattle, WA; the Center on Aging and Health, Departments of Medicine and Epidemiology, The Johns Hopkins University, Baltimore, MD;5 and the Department of Public Health Sciences, Wake Forest University School of Medicine, Winston-Salem, NC6
Address for correspondence: Dariush Mozaffarian, MD, MPH, Harvard School of Public Health, 665 Huntington Avenue, Building 2, Room 315, Boston, MA 02115 E-mail: [email protected]
Influences of lifestyle habits on cardiovascular disease risk among older adults are not well established. The authors present evidence from the Cardiovascular Health Study that dietary, physical activity, and smoking habits assessed late in life are associated with cardiovascular disease risk among adults aged 65 years or older. Persons consuming fatty fish twice per week had a 47% lower risk of coronary death com-pared with those who consumed fatty fish less than once per month, while cereal fiber intake (about two whole-grain bread slices per day) was associated with a 14% lower risk of myocardial infarction or stroke. Modest alcohol intake (1–6 drinks per week) predicted the fewest subclinical cerebrovascular abnormali-ties. Compared with little activity, moderate and high leisure-time activity predicted 28% and 44% lower mortality, respectively, while compared with nonexercisers, low, moderate, and high exercise intensity pre-dicted 30%, 37%, and 53% more years of healthy life, respectively. Former and current smokers had 25% and 44% fewer years of healthy life than those who never smoked; lifetime smoking (pack-years) predicted higher mortality. Clinical practice and public health implications, gaps in knowledge, and future research directions are summarized. (AJCG. 2004;13:153–160) ©2004 Le Jacq Communications, Inc.
www.lejacq.com ID: 2122
modified by: modified date: proofed by: final approval by: approved date: additional comments:
Michael Tuck, MD Chief of Endocrinology & Metabolism
UCLA San Fernando Valley Medical Program
Nasser Mikhail, MD, MSc Chief of Endocrinology & Metabolism
Olive View–UCLA Medical Center
Dalila Corry, MD Chief, Nephrology
Olive View–UCLA Medical Center
Edited By:
Hypertension Management in Patients with Diabetes
(continued)
Regimen Various categories of antihypertensive agents wereemployed as the goal of the study was not to test for aspecific drug but to test how aggressive the physiciansare in managing blood pressure in 5 VA sites in NewEngland between 1990 and 1995. The study data weretaken from chart reviews. Patients were required toattend 1 clinic in general medicine or subspecialty clin-ic during a set period of time. Second, they had to havemade an outcome visit 1.5-2.5 years after the index visit.Third, the patients had to make 1 visit during the indexand outcome visit. They required up to 4 measurementof blood pressure (BP) per visit but in 80.5% only 1 BPwas recorded. Information on changes in antihyperten-sive medications were taken from progress notes, med-ical orders, and pharmacy records looking for anappropriate increase in BP medications if BP was not atgoal. The outcome measure is the level of BP at the out-come visit and then calculating the percentage ofpatients poorly controlled using either a threshold of≥40/90 mm Hg or ≥160/90 mm Hg. They also analyzedby a statistical process whether a patient received moreincreases in therapy than the norm. This process cap-tures those characteristics at each visit associated with agreater likelihood of an increase.
Results Patients with diabetes had worse BP control than thosewithout diabetes. The mean systolic BP was 148.4 mmHg in diabetic patients and 143.8 mm Hg in nondiabetics.There were no differences in mean diastolic pressure. Atotal of 73% of diabetics had BP ≥140/90 mm Hg com-pared to 66% of nondiabetics. Most patients had elevat-ed systolic BP (57%). The proportion of patients with≥160/90 mm Hg was not different between groups.Hypertensive patients with diabetes received less inten-sive antihypertensive medication than patients withoutdiabetes even after using regression models adjusting forother baseline patient characteristics.
5
Hypertension Management in Patients with Diabetes
Title Hypertension management in patients with diabetes: theneed for more aggressive therapy.
Authors Berlowitz DR, Ash AS, Hickey EC, et al.
Reference Diabetes Care 2003;26:355-359.
Disease Diabetes mellitus and hypertension.
Purpose To determine the adequacy of blood pressure control inhypertensive diabetic male patients based on currentguidelines for target blood pressure levels in diabetichypertensive patients.
Design Retrospective from abstracted medical records.
Patients 800 male patients from 5 Department of Veterans Affairs(VA) sites, 274 patients with diabetes and hypertension,and 526 nondiabetic hypertensive subjects with durationof hypertension 12.95.2 and 12.45.4 years, respec-tively. There were 32% nonwhites among the diabeticsubjects and 35% nonwhites in the nondiabetic group.Subjects in both groups were on 1-3 antihypertensivemedications. Body mass index was 29.24.8 and 27.84.3kg/m2 in diabetic and nondiabetics with hypertension.
Follow-up 2 years.
NEW
NEW
NEW
NEW
NEW
Oth
er c
ompr
ehen
sive
rev
iew
s av
aila
ble
thro
ugh
Le Ja
cq C
omm
unic
atio
ns, I
nc.
Alle
rgy
Tria
ls R
evie
w •
Car
diov
ascu
lar
Dev
ice
Tria
ls R
evie
w •
Car
diov
ascu
lar
Tria
ls R
evie
w, 8
th E
diti
on •
Der
mat
olog
y Tr
ials
Rev
iew
• O
besi
ty T
rial
s Re
view
ECG
Tri
als
Revi
ew •
Gas
troe
nter
olog
y Tr
ials
Rev
iew
• In
fect
ious
Dis
ease
Tri
als
Revi
ew •
Lip
id-L
ower
ing
Clin
ical
Tri
als
Revi
ew •
Neu
rolo
gy T
rial
s Re
view
O
ncol
ogy
Tria
ls R
evie
w •
Pai
n M
anag
emen
t Tr
ials
Rev
iew
• P
sych
iatr
ic D
rug
Revi
ew •
Rhe
umat
olog
y Tr
ials
Rev
iew
• S
port
s M
edic
ine
Tria
ls R
evie
wU
rolo
gy T
rial
s Re
view
• V
eter
inar
y Tr
ials
Rev
iew
An
indi
spen
sibl
e re
fere
nce
for p
hysi
cian
s,
med
ical
pro
fess
iona
ls,
clin
icia
ns, a
nd
rese
arch
ers
to a
ssis
t in
keep
ing
up to
dat
e w
ith
the
tria
ls th
at h
ave
been
refe
renc
ed in
the
med
ical
lite
ratu
re.
Dia
bet
es T
rial
s R
evie
wEd
ited
by
Mic
hael
Tuc
k, M
D; N
asse
r M
ikha
il, M
D, M
Scan
d D
alila
Cor
ry, M
D
Con
tact
you
r R
elia
nt
rep
rese
nta
tive
or
call
800
.475
.214
0fo
r a
FRE
E c
opy
(wh
ile
sup
pli
es la
st)
Tria
ls in
clud
ed:
Dia
bete
s an
d O
besi
tyPr
even
tion
or
Del
ay o
f Dia
bete
sPh
arm
acol
ogic
al T
her
apy
ofD
iabe
tes
Mel
litus
Insu
lin R
egim
ens
Dia
beti
c N
eph
ropa
thy
Dia
beti
c N
euro
path
yD
iabe
tes
in P
edia
tric
sC
ardi
ovas
cula
r C
ompl
icat
ion
s of
Dia
bete
sD
yslip
idem
ia in
Dia
bete
sPr
elim
inar
y R
epor
tsSe
xual
Dys
fun
ctio
n in
Dia
bete
s
NEW
NEW
NEW
NEW
NEW
Trials included:
Diabetes and Obesity
Prevention or Delay of Diabetes
Pharmacological Therapy ofDiabetes Mellitus
Insulin Regimens
Diabetic Nephropathy
Diabetic Neuropathy
Diabetes in Pediatrics
Cardiovascular Complications of Diabetes
Dyslipidemia in Diabetes
Preliminary Reports
Sexual Dysfunction in Diabetes
Diabetes Trials ReviewEdited by Michael Tuck, MD; Nasser Mikhail, MD, MSc
and Dalila Corry, MD
225225
Now Available!
LLC
Provided as an Educational Service ByProvided as an Educational Service By
NEW
NEW
NEW
NEW
NEW
Contact your Reliant representativeor call 800.475.2140
for a FREE copy (while supplies last)
The American Journal of Geriatric Cardiology (ISSN 1076-7460) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.

LIFESTYLE AND CVD RISK IN OLDER ADULTS154 THE AMERICAN JOURNAL OF GERIATRIC CARDIOLOGY 2004 VOL. 13 NO. 3
abnormalities—that may affect subsequent clinical events. Lifestyle habits may also directly influence risk of myocardial infarction (MI), stroke, or death. Each of these effects may be mediated by traditional risk factors (such as serum lipids or blood pressure) or other pathways related to CVD (such as systemic inflammation or arrhythmia). To elucidate potential influences of lifestyle on CVD risk among older adults, we examined evidence from CHS for associations of diet, physical activ-ity, and smoking with CVD risk factors, subclinical disease, and clinical CVD.
DIETARY HABITSFish and n-3 Fatty Acids. The n-3 polyunsatu-rated fatty acids include eicosapentaenoic acid (EPA, 20:5n-3) and docosahexaenoic acid (DHA, 22:6n-3), long-chain fatty acids found in fish and seafood, and α-linolenic acid (18:3n-3), an intermediate-chain fatty acid found in nuts, soy, canola, and flaxseed. In predominantly middle-aged populations, evidence indicates that consumption of EPA and DHA, and possibly α-linolenic acid, decreases risk of fatal (pri-marily arrhythmic) coronary heart disease (CHD).4–8
These relationships have been evaluated among older adults.9,10 In CHS, usual fish consumption was assessed in participants free of known CVD at base-line using a food frequency questionnaire.10 Intake of tuna or other broiled or baked fish correlated with plasma phospholipid EPA+DHA (r=0.55; p<0.001), while intake of fried fish or fish sand-wiches (fish burgers) did not (r=0.04; p=0.78), con-sistent with lean types of fish typically fried (cod,
pollack). Distributions of fish consumption among these older adults are shown in Table I.
In cross-sectional unadjusted analyses, tuna/other fish intake was associated with lower systolic blood pressure, C-reactive protein, and prevalence of diabetes; fried fish/fish sandwich intake was associated with higher systolic blood pressure, body mass index, and prevalence of diabetes. Both tuna/other fish and fried fish/fish sandwich intake were positively associated with low-density lipoprotein cholesterol, while tuna/other fish was positively associated and fried fish/fish sandwich intake was negatively associated with high-density lipoprotein (HDL) cholesterol.
Incidence of CHD death (including arrhythmic CHD death) and nonfatal MI were prospectively ascertained over 11 years of follow-up. After adjust-ment for other risk factors, tuna/other fish intake was associated with lower risk of both total and arrhythmic CHD death (p for trend=0.002 and 0.001, respectively), with a trend toward lower risk of nonfatal MI (p for trend=0.10) (Table I). This lower risk appeared related to consumption of long-chain n-3 fatty acids: each 1 g/d of estimated dietary EPA+DHA was associated with 55% lower risk of arrhythmic CHD death (hazard ratio [HR], 0.45; 95% confidence interval [CI], 0.25–0.81). In contrast, fried fish/fish sandwich intake was not associated with lower CHD risk, but with trends toward higher risk (Table I).
Associations between plasma phospholipid fatty acids (biomarkers of dietary fatty acid intake) and CHD risk were evaluated using stored blood samples in a case-control study nested within CHS, including 54 cases of fatal CHD (67% due to arrhythmia), 125 cases of nonfatal MI, and 179 matched controls.11 After adjustment for potential confounders, each standard deviation increase in EPA+DHA levels was associated with 70% lower risk of fatal CHD (odds ratio [OR], 0.30; 95% CI, 0.12–0.76) but not nonfatal MI (OR, 0.97; 95% CI=0.71–1.33). In similar analyses, α-linolenic acid levels were also associated with lower risk of fatal CHD (OR, 0.48; 95% CI, 0.24–0.96) but not nonfatal MI (OR, 1.07; 95% CI, 0.81–1.41).
Conclusions. Among older adults, consumption of tuna or other broiled or baked fish is associated with lower risk of CHD death, particularly arrhyth-mic CHD death. The inverse association with fatal arrhythmic events is consistent with known anti-arrhythmic effects of n-3 fatty acids.12 Levels of both long-chain (EPA+DHA) and intermediate-chain (α-linolenic acid) n-3 fatty acids appear to be
1
Lifestyle
Diet Physical activity
Smoking
Clinical Events
MI CHD death
Stroke
Total mortality
Subclinical Disease
PVD Carotid IMT MRI findings
ECG/Echo findings
CVD risk factors
CVD risk factors
Figure 1. Potential influences of lifestyle habits on cardiovascular disease. CVD=cardiovascular dis-ease; PVD=peripheral vascular disease; IMT=intima-medial thickness; MRI=magnetic resonance imaging; ECG=electrocardiography; Echo=echocardiography; MI=myocardial infarction; CHD=coronary heart disease
The American Journal of Geriatric Cardiology (ISSN 1076-7460) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.

LIFESTYLE AND CVD RISK IN OLDER ADULTS THE AMERICAN JOURNAL OF GERIATRIC CARDIOLOGY 2004 VOL. 13 NO. 3 155
associated with a lower risk of CHD death. In con-trast, consumption of fried fish or fish sandwiches is associated with trends toward higher risk, which may be due to residual confounding or (although not directly assessed) may reflect adverse effects related to mercury ingestion or trans fatty acids and lipid oxidation products in fried fats/oils.13–15
Future Directions. Confirmation and further inves-tigation of potential differences between types of fish meals and preparation methods is warranted. Potentially protective effects of α-linolenic acid require verification in additional observational stud-ies and clinical trials.
Dietary Fiber. In predominantly middle-aged popu-lations, dietary fiber has been associated with lower CVD risk, particularly fiber from cereal sources (including whole grains and bran), rather than fruit or vegetable sources.16–18 Potential cardiovascular benefits of fiber include effects on serum lipids, postprandial glucose and triglyceride levels, insulin sensitivity, and blood pressure.19–21 These potential mechanisms may have less effect in older adults, when atherosclerosis may be more advanced.
In CHS, usual intake of cereal, fruit, and veg-etable fiber was assessed among persons free of known CVD at baseline using a food frequency questionnaire.22 Assessment of fiber intake was validated in a subset of participants, with estimat-ed dietary fiber intake by the food frequency ques-tionnaire and the average of six 24-hour dietary recalls having a correlation of 0.56 (p<0.001).22 The main sources of cereal fiber were dark breads and high-fiber or bran cereals; of fruit fiber were apples, oranges, and bananas; and of vegetable fiber were beans, broccoli, peas, corn, and cau-liflower. For cereal fiber, mean daily intake was approximately the fiber content of two slices of whole-grain bread (4.2 g/d); for fruit fiber, 1 large apple (5.2 g/d); and for vegetable fiber, 1 large stalk of cooked broccoli (6.9 g/d).
In cross-sectional unadjusted analyses, cereal fiber intake was inversely associated with systolic blood pressure, triglycerides, and fasting glucose levels and positively associated with HDL choles-terol levels. Cereal fiber intake was also inverse-ly associated with ultrasound-defined internal carotid intima-medial thickness, a measure of subclinical disease.
Table I. Risk of Incident Coronary Heart Disease According to Fish Consumption*
FREQUENCY OF CONSUMPTION
<1/MO 1–3/MO 1/WK 2/WK 3+/WK P FOR TREND
Tuna/other fish n=381 n=917 n=800 n=610 n=1202
Total CHD death 1.0 (referent) 0.78 (0.47–1.28) 0.77 (0.45–1.32) 0.53 (0.30–0.96) 0.47 (0.27–0.82) 0.002
Arrhythmic CHD death
1.0 (referent) 0.86 (0.45–1.63) 0.81 (0.40–1.66) 0.50 (0.23–1.07) 0.32 (0.15–0.70) 0.001
Nonfatal MI 1.0 (referent) 0.81 (0.51–1.26) 0.71 (0.44–1.15) 0.75 (0.46–1.21) 0.67 (0.42–1.07) 0.10
Fried fish/fish sandwich
n=1287 n=1848 n=204 n=512 n=59
Total CHD death 1.0 (referent) 1.23 (0.83–1.83) 1.61 (0.88–2.94) 1.14 (0.68–1.91) 1.37 (0.48–3.90) 0.35
Arrhythmic CHD death
1.0 (referent) 1.22 (0.71–2.08) 1.95 (0.91–4.18) 1.54 (0.82–2.90) † 0.28
Nonfatal MI 1.0 (referent) 1.28 (0.93–1.77) 1.58 (0.93–2.70) 1.22 (0.82–1.82) 1.93 (0.91–4.08) 0.11
CHD=coronary heart disease; MI=myocardial infarction; *values are hazard ratios (95% confidence intervals) compared with intake less than once per month, adjusted for age, sex, education, diabetes, smoking, body mass index, systolic blood pressure, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, C-reactive protein, and intake of tuna/other fish or fried fish/fish sandwich, saturated fat, alcohol, beef/pork, fruits, and vegetables; †single event limits estimation of risk
Table II. Risk of Incident Cardiovascular Disease According to Dietary Fiber Consumption*
QUINTILES OF CONSUMPTION
I II III IV V P FOR TREND
Cereal fiber 1.0 (referent) 0.92 (0.74–1.15) 0.83 (0.67–1.04) 0.82 (0.65–1.03) 0.79 (0.62–0.99) 0.02
Fruit fiber 1.0 (referent) 0.94 (0.75–1.18) 0.85 (0.67–1.08) 0.95 (0.76–1.20) 0.99 (0.78–1.25) 0.98
Vegetable fiber 1.0 (referent) 0.98 (0.78–1.23) 1.12 (0.90–1.40) 0.80 (0.63–1.02) 1.08 (0.86–1.36) 0.95
*Values are hazard ratios (95% confidence intervals) comparing quintiles II–V to the lowest quintile of cereal, fruit, or vegetable fiber intake in a model including age, sex, education, diabetes, smoking, physical activity, exercise intensity, alcohol intake, and cereal, fruit, and vegetable fiber intake.
The American Journal of Geriatric Cardiology (ISSN 1076-7460) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.

LIFESTYLE AND CVD RISK IN OLDER ADULTS156 THE AMERICAN JOURNAL OF GERIATRIC CARDIOLOGY 2004 VOL. 13 NO. 3
Incidence of CVD (CHD death, nonfatal MI, and stroke) was prospectively ascertained over 8.6 years of follow-up. After adjustment for potential confounders, intake of cereal fiber, but not fruit or vegetable fiber, was inversely associated with incident CVD (p for trend=0.02, 0.98, and 0.95, respectively) (Table II). Each 4.6 g/d cereal fiber—approximately the fiber content of two slices of whole-grain bread—was associated with 14% lower risk of incident CVD (HR, 0.86; 95% CI, 0.75–0.99).
Conclusions. Among older adults, dietary fiber from cereals and whole grains, but not fruits or vegetables, is associated with lower risk of CVD. Modest differences in intake, such as two slices of whole-grain bread per day, are associated with lower risk.
Future Directions. Further study is required to investigate potential mechanisms and alternative explanations for the inverse relationship of cereal fiber, but not fruit or vegetable fiber, with CVD risk among older adults.
Alcohol Use. Modest alcohol consumption has favorable associations with serum lipids and CHD risk in predominantly middle-aged populations.23 In CHS, usual frequency of alcohol consumption and types of alcoholic beverages consumed (wine, beer, liquor) were assessed annually. Changes in
consumption during the past 5 years were also assessed. At base-line in 1989–1990, 48% of CHS participants did not drink alcohol, 39% drank up to one drink per day, 10% drank one to three drinks per day, and 3% drank four or more drinks per day.24
In cross-sectional multivariate analyses in CHS, alcohol use predicted lower triglyc-erides (p<0.05) and higher HDL cholesterol (p<0.001).25 Lower tri-glycerides and higher HDL cholesterol levels were associated with a lower risk of prevalent stroke in men (p<0.05 for triglycerides;
p<0.01 for HDL) and a lower risk of prevalent CHD in men (p=0.06 for triglycerides; p<0.0001 for HDL) and women (p<0.01 for triglycerides; p<0.001 for HDL).25
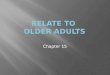
In 1992–1994, CHS participants underwent brain magnetic resonance imaging (MRI) with standardized assessment of white matter grade, cerebral infarcts, ventricular size, and sulcal size.26 Associations of alcohol consumption with subclinical (MRI-defined) cerebrovascular disease, which predicts future clini-cal strokes and poorer cognitive and neurological function,27,28 were assessed among participants with-out clinical history of cerebrovascular disease.29 After adjustment for other risk factors, the fewest white matter grade abnormalities were seen among those consuming one to six drinks per week, compared with higher or lower consumption (p for quadratic term=0.01)(Figure 2). Alcohol consumption was inversely associated with cerebral infarcts (41% lower risk for 15+ drinks per week compared with abstain-ers, p for trend=0.004) but positively associated with MRI measures of brain atrophy (32% and 53% higher risk of increased ventricular and sulcal size for 15+ drinks per week compared with abstainers, p for trend=0.006 and 0.007, respectively).
After adjustment for other risk factors, alcohol use was not associated with 5-year mortality in CHS.24 However, among older adults in CHS who were gen-erally healthy at baseline (free of known CVD, chronic obstructive pulmonary disease [COPD], or cancer),
0.4
0.6
0.8
1
1.2
1.4
1.6
None <1 1 - 6 7 - 14 15+
Usual Weekly No. of Drinks
OddsRatio
Sulcal Size
Ventricular Size
Infarct
White MatterGrade
Figure 2. Risk of subclinical cerebrovascular disease as determined by magnetic resonance imaging findings of the brain among persons free of known clinical history of cerebrovascular disease, according to usual alcohol consumption. Odds ratios derived from ordinal regression models, adjusting for age, race, gender, education, income, marital status, current smoking, former smoking, diabetes, body mass index, total cholesterol, atrial fibrillation, congestive heart failure, and leisure-time activity; abstainers were the reference group for all comparisons, and former drinkers were excluded. Used with permission from Stroke. 2001;32:1939–1946.29
The American Journal of Geriatric Cardiology (ISSN 1076-7460) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.

LIFESTYLE AND CVD RISK IN OLDER ADULTS THE AMERICAN JOURNAL OF GERIATRIC CARDIOLOGY 2004 VOL. 13 NO. 3 157
reported wine drinking late in life was associated with a trend toward 11% more years of continued health (years free of CVD, COPD, cancer, or death from any cause) (HR, 1.11; 95% CI, 0.99–1.24) in multivariate analyses.30 In other cohort studies of older adults, there appears to be a J- or U-shaped relationship between alcohol consumption and total mortal-ity, with lowest risk at approximately one drink per day.31,32 Investigation of associations between alcohol consumption and specific CVD events, such as MI or stroke, is currently in progress in CHS.
Conclusions. Among older adults, alcohol consump-tion is associated with a favorable lipid profile, including higher HDL cholesterol and lower tri-glycerides. Modest alcohol intake (approximately one to six drinks per week) is associated with lower risk of subclinical cerebral vascular abnormalities, while greater intake is associated with brain atrophy. In some, though not all, studies, modest alcohol use late in life predicts lower total mortality.
Future Directions. Relationships of alcohol use late in life—including different types of alco-holic beverages—with mortality and specific CVD events require further investigation.
Other Dietary Factors. Potential influences of other dietary factors (e.g., saturated fat intake) on CVD risk late in life are not well established. Additional investigation of relationships between diet and CVD risk among older adults is needed.
PHYSICAL ACTIVITYPhysical inactivity is a well recognized risk factor for CVD.33 In CHS, leisure-time activity (kilocalories per week) was assessed using a modified Minnesota Leisure Time Activities questionnaire, evaluating frequency and duration of 15 different activities during the prior 2 weeks.34 Exercise intensity was
also separately characterized, with responses includ-ing no exercise or low, medium, or high intensity of exercise.35 Distributions of leisure-time activity and exercise intensity in CHS are shown in Table III.
In cross-sectional analyses, both leisure-time activity and exercise intensity were associated with traditional and nontraditional CVD risk factors in CHS.34,35 Compared with the lowest quartile of leisure-time activity, persons in the highest quartile had 19%, 6%, and 4% lower levels of C-reactive protein, white blood cells, and fibrinogen, respec-tively (p<0.01 for each), after adjustment for poten-tial confounders.34 Leisure-time activity was also inversely associated with body mass index, waist-hip ratio, fasting glucose, and fasting insulin (p<0.001 for each).34 Among participants free of known CVD or impaired physical function, exercise intensity was inversely associated with fasting insulin levels (p<0.001), serum fibrinogen (p=0.01), peripheral arterial disease as assessed by ankle-arm index (p=0.01), and electrocardiographic evidence of MI (p<0.001) after adjustment for other risk factors.35
Exercise intensity and leisure-time activity are also both associated with clinical events late in life. Among CHS participants free of known CVD, COPD, or cancer at baseline, exercise was positively associated with continued years of healthy life (years free from CVD, COPD, can-cer, or death from any cause).30 During 7 years of follow-up, 66% of men with high exercise intensity remained healthy compared with 52% of nonexercisers (p<0.01), while 79% of women with high exercise intensity remained healthy compared with 65% of nonexercisers (p<0.001). In a multivariate stepwise model evaluating the most important factors associated with years of healthy life, low exercise intensity was associ-ated with 30% more years, moderate exercise intensity with 37% more years, and high exer-cise intensity with 53% more years of healthy
Table III. Years of Healthy Life and Total Mortality According to Physical Activity*
EXERCISE INTENSITY
NONE (N=173) LOW (N=1018) MODERATE (N=654) HIGH (N=197) P FOR TREND
Years of healthy life**
1.0 (referent) 1.30 (1.07–1.56) 1.37 (1.13–1.67) 1.53 (1.18–1.98) <0.001
LEISURE-TIME ACTIVITY (KCAL/WK)
<67 (N=566) 67–472 (N=846) 473–979 (N=936) 980–1889 (N=1168) >1890 (N=1669) P FOR TREND
Total Mortality† 1.0 (referent) 0.78 (0.60–1.00) 0.81 (0.63–1.05) 0.72 (0.55–0.93) 0.56 (0.43–0.74) <0.005
*Values are hazard ratios (95% confidence intervals); **survival free from cardiovascular disease, chronic obstructive pulmonary disease, cancer, or death, adjusted for age, gender, income, change in finances, waist circumference, smoking, wine use, and aspirin use; †adjusted for age, gender, income, weight, blood pressure, smoking, congestive heart failure, abnormal ejection fraction, aortic stenosis, abnormal electrocardiogram, carotid stenosis, forced vital capacity, diuretic use, self-assessed health, difficulties with activities of daily living, fasting glucose, albumin, and creatinine
The American Journal of Geriatric Cardiology (ISSN 1076-7460) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.

LIFESTYLE AND CVD RISK IN OLDER ADULTS158 THE AMERICAN JOURNAL OF GERIATRIC CARDIOLOGY 2004 VOL. 13 NO. 3
life, compared with nonexercisers (p<0.001 for each) (Table III). In separate analyses, greater leisure-time activity also predicted lower total mortality (Table III).24
Conclusions. Among older adults, greater leisure-time activity and exercise intensity are associated with a more favorable CVD risk profile, less sub-clinical disease, and better clinical outcomes. Even modest leisure-time activity and low exercise inten-sity are associated with lower risk, compared with less activity and no exercise.
Future Directions. Relationships of physical activity with specific CVD events such as MI and stroke, as well as potential mechanisms for these associations, should be investigated among older adults.
SMOKINGCigarette smoking is a well established risk factor for CVD among young and middle-aged populations.36 In cross-sectional analyses in CHS, smoking was associ-ated with prevalent subclinical disease, including ultra-sound-defined internal carotid artery stenosis and inti-ma-medial thickness,37,38 MRI-defined cerebral white matter abnormalities,27 and a subclinical CVD index based on electrocardiographic, echocardiographic, carotid, and ankle-arm index abnormalities.39 Smoking also was associated with prevalent CVD morbidity in
CHS, including angina, intermittent claudication, and impaired cognitive function.27,39
In a prospective analysis from CHS among older adults free of MI at baseline, current smoking was associated with a trend toward higher risk of inci-dent MI (relative risk, 1.36; 95% CI, 0.96–1.93) after adjustment for age, sex, and prevalent CVD.40 Further adjustment for subclinical disease measures mitigated this association, suggesting that smoking may influence risk of MI in older adults via effects on subclinical disease. Among CHS participants free of known CVD, COPD, or cancer at baseline, smok-ing status was associated with years of continued good health, with 25% and 44% fewer years among former smokers and current smokers, respective-ly, compared with participants who never smoked (p<0.001) (Table IV).30 Furthermore, lifetime smok-ing history (average packs per day × years of smok-ing) was strongly associated with total mortality in CHS (p<0.005) (Table IV).24 Other cohort studies of older adults demonstrate similar findings, with higher total mortality among current smokers com-pared with former smokers, including persons who stopped smoking after age 65 years.41–43
Conclusions. Cigarette smoking is associated with subclinical disease, CVD morbidity, and clinical events among older adults. Both current smoking and life-time smoking exposure are associated with higher
158
Table V. Lifestyle Habits* Associated With Lower Risk of Cardiovascular Disease Among Older Adults: Summary of Evidence From the Cardiovascular Health Study
Consumption of tuna or other broiled or baked fish two or more times per week (intake of nuts, soy, canola, or flaxseed oil may also be beneficial)
Consumption of dietary fiber from cereals and whole grains (e.g., two slices of whole grain bread per day)Low-to-moderate alcohol intake (approximately one to six drinks per week)Regular leisure time activity (as appropriate to health status)Regular exercise of at least low intensity (after evaluation by a physician)Smoking cessation
*Dietary, physical activity, and smoking habits assessed late in life
Table IV. Years of Healthy Life and Total Mortality According to Smoking Status*
SMOKING STATUS
NEVER (N=1221) FORMER (N=574) CURRENT (N=246) P FOR TREND
Years of healthy life** 1.00 (referent) 0.75 (0.68–0.84) 0.56 (0.48–0.66) <0.001
LIFETIME PACK-YEARS
NONE (N=2358) 1–25 (N=1119) 26–50 (N=952) >50 (N=645) P FOR TREND
Total Mortality† 1.00 (referent) 1.10 (0.88–1.38) 1.13 (0.90–1.43) 1.58 (1.25–2.00) <0.005
*Values are hazard ratios (95% confidence intervals); **survival free from cardiovascular disease, chronic obstructive pulmo-nary disease, cancer, or death, adjusted for age, gender, income, change in finances, waist circumference, exercise intensity, wine use, and aspirin use; †adjusted for age, gender, income, weight, blood pressure, physical activity, congestive heart failure, abnormal ejection fraction, aortic stenosis, abnormal electrocardiogram, carotid stenosis, forced vital capacity, diuretic use, self-assessed health, difficulties with activities of daily living, fasting glucose, albumin, and creatinine
The American Journal of Geriatric Cardiology (ISSN 1076-7460) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.

LIFESTYLE AND CVD RISK IN OLDER ADULTS THE AMERICAN JOURNAL OF GERIATRIC CARDIOLOGY 2004 VOL. 13 NO. 3 159
risk. Older adults who have stopped smoking have lower risk than those who continue to smoke.
Future Directions. Continued investigation of rela-tionships of smoking (including age at quitting and years since quitting) with risk of CHD, stroke, and death among older adults will further elucidate risks of smoking and benefits of cessation late in life.
CONCLUSIONSEvidence from CHS suggests that diet, physical activity, and smoking habits late in life may influ-ence CVD risk. Compared with medical or surgical interventions, such lifestyle changes are relatively low risk, low cost, and widely applicable. Therefore, even small changes in risk due to these lifestyle fac-tors may be significant on a population level. The findings from CHS suggest several potential targets for CVD prevention among older adults (Table V). However, while these observed associations in CHS were independent of a variety of other participant risk factors and characteristics, these findings do not establish causality. Additionally, each of these lifestyle habits was assessed late in life, and wheth-er the observed associations are related to current or lifetime lifestyle habits requires further investi-gation. Future research should be directed toward the potential effects of these and other lifestyle habits on CVD risk factors, subclinical disease, and clinical events among older adults.
Disclosure: At the time the manuscript was completed, Dr. Mozaffarian was with the Veterans Affairs Puget Sound Health Care System, and salary support was provided by a VA Health Services Research & Development fellowship. The research reported in this article was supported by contracts N01-HC-85079 through N01-HC-85086, N01-HC-35129, and N01 HC-15103 from the National Heart, Lung, and Blood Institute, US Department of Health and Human Services. For a full list of participating CHS investigators and institutions, see “About CHS: Principal Investigators and Study Sites” at http://chs-nhlbi.org.
REFERENCES
1 US Census Bureau. National population projections. Available at: http://www.census.gov/population/projections/nation/summary/np-t3-f.txt. Accessed December 23, 2002.
2 American Heart Association. 2002 Heart and Stroke Statistical Update. Dallas, TX: American Heart Association; 2001.
3 Fried LP, Borhani NO, Enright P, et al. The Cardiovascular Health Study: design and rationale. Ann Epidemiol. 1991;1:263–276.
4 Siscovick DS, Raghunathan TE, King I, et al. Dietary intake and cell membrane levels of long-chain n-3 polyun-saturated fatty acids and the risk of primary cardiac arrest. JAMA. 1995;274:1363–1367.
5 Albert CM, Hennekens CH, O’Donnell CJ, et al. Fish
consumption and risk of sudden cardiac death. JAMA. 1998;279:23–28.
6 Hu FB, Bronner L, Willett WC, et al. Fish and omega-3 fatty acid intake and risk of coronary heart disease in women. JAMA. 2002;287:1815–1821.
7 Burr ML, Fehily AM, Gilbert JF, et al. Effects of changes in fat, fish, and fibre intakes on death and myocardial reinfarction: diet and reinfarction trial (DART). Lancet. 1989;2:757–761.
8 Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: GISSI-Prevenzione trial. Lancet. 1999;354:447–455.
9 Kromhout D, Feskens EJ, Bowles CH. The protective effect of a small amount of fish on coronary heart dis-ease mortality in an elderly population. Int J Epidemiol. 1995;24:340–345.
10 Mozaffarian D, Lemaitre RN, Kuller LH, et al. Cardiac benefits of fish consumption may depend on the type of fish meal consumed: the Cardiovascular Health Study. Circulation. 2003;107:1372–1377.
11 Lemaitre RN, King IB, Mozaffarian D, et al. n-3 Polyunsaturated fatty acids, fatal ischemic heart disease, and nonfatal myocar-dial infarction in older adults: the Cardiovascular Health Study. Am J Clin Nutr. 2003;77:319–325.
12 McLennan PL. Myocardial membrane fatty acids and the antiarrhythmic actions of dietary fish oil in animal mod-els. Lipids. 2001;36(suppl):S111–S114.
13 Salonen JT, Seppanen K, Nyyssonen K, et al. Intake of mercury from fish, lipid peroxidation, and the risk of myocardial infarction and coronary, cardiovascu-lar, and any death in eastern Finnish men. Circulation. 1995;91:645–655.
14 Ascherio A, Katan MB, Zock PL, et al. Trans-fatty acids and coronary heart disease. N Engl J Med. 1999;340:1994–1998.
15 Williams MJ, Sutherland WH, McCormick MP, et al. Impaired endothelial function following a meal rich in used cooking fat. J Am Coll Cardiol. 1999;33:1050–1055.
16 Rimm EB, Ascherio A, Giovannucci E, et al. Vegetable, fruit, and cereal fiber intake and risk of coronary heart disease among men. JAMA. 1996;275:447–451.
17 Wolk A, Manson JE, Stampfer MJ, et al. Long-term intake of dietary fiber and decreased risk of coronary heart dis-ease among women. JAMA. 1999;281:1998–2004.
18 Ascherio A, Rimm EB, Hernan MA, et al. Intake of potassium, magnesium, calcium, and fiber and risk of stroke among US men. Circulation. 1998;98:1198–1204.
19 Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Energy, Carbohydrates, Fiber, Fat, Protein, and Amino Acids (Macronutrients). Washington, DC: National Academies Press; 2002.
20 Anderson JW. Dietary fiber prevents carbohydrate-induced hypertriglyceridemia. Curr Atheroscler Rep. 2000;2:536–541.
21 Burke V, Hodgson JM, Beilin LJ, et al. Dietary protein and soluble fiber reduce ambulatory blood pressure in treated hypertensives. Hypertension. 2001;38:821–826.
22 Mozaffarian D, Kumanyika SK, Lemaitre RN, et al. Cereal, fruit, and vegetable fiber intake and the risk of cardiovas-cular disease in elderly individuals: the Cardiovascular Health Study. JAMA. 2003;289:1659–1666.
23 Marmot MG. Alcohol and coronary heart disease. Int J Epidemiol. 2001;30:724–729.
24 Fried LP, Kronmal RA, Newman AB, et al. Risk factors for
The American Journal of Geriatric Cardiology (ISSN 1076-7460) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.

LIFESTYLE AND CVD RISK IN OLDER ADULTS160 THE AMERICAN JOURNAL OF GERIATRIC CARDIOLOGY 2004 VOL. 13 NO. 3
5-year mortality in older adults: the Cardiovascular Health Study. JAMA. 1998;279:585–592.
25 Ettinger WH, Wahl PW, Kuller LH, et al. Lipoprotein lipids in older people. Results from the Cardiovascular Health Study. The CHS Collaborative Research Group. Circulation. 1992;86:858–869.
26 Bryan RN, Manolio TA, Schertz LD, et al. A method for using MR to evaluate the effects of cardiovascular dis-ease on the brain: the cardiovascular health study. Am J Neuroradiol. 1994;15:1625–1633.
27 Longstreth WT Jr, Manolio TA, Arnold A, et al. Clinical correlates of white matter findings on cranial mag-netic resonance imaging of 3301 elderly people. The Cardiovascular Health Study. Stroke. 1996;27:1274–1282.
28 Kuller LH, Shemanski L, Manolio T, et al. Relationship between ApoE, MRI findings, and cognitive function in the Cardiovascular Health Study. Stroke. 1998;29:388–398.
29 Mukamal KJ, Longstreth WT Jr, Mittleman MA, et al. Alcohol consumption and subclinical findings on mag-netic resonance imaging of the brain in older adults: the Cardiovascular Health Study. Stroke. 2001;32:1939–1946.
30 Burke GL, Arnold AM, Bild DE, et al. Factors associated with healthy aging: the Cardiovascular Health Study. J Am Geriatr Soc. 2001;49:254–262.
31 Scherr PA, LaCroix AZ, Wallace RB, et al. Light to moder-ate alcohol consumption and mortality in the elderly. J Am Geriatr Soc. 1992;40:651–657.
32 Goldberg RJ, Burchfiel CM, Reed DM, et al. A prospec-tive study of the health effects of alcohol consumption in middle-aged and elderly men. The Honolulu Heart Program. Circulation. 1994;89:651–659.
33 Fletcher GF, Balady G, Blair SN, et al. Statement on exercise: benefits and recommendations for physical activ-ity programs for all Americans. A statement for health professionals by the Committee on Exercise and Cardiac Rehabilitation of the Council on Clinical Cardiology, American Heart Association. Circulation. 1996;94:857–862.
34 Geffken DF, Cushman M, Burke GL, et al. Association between physical activity and markers of inflammation in a healthy elderly population. Am J Epidemiol. 2001;153:242–250.
35 Siscovick DS, Fried L, Mittelmark M, et al. Exercise intensity and subclinical cardiovascular disease in the elderly. The Cardiovascular Health Study. Am J Epidemiol. 1997;145:977–986.
36 Lakier JB. Smoking and cardiovascular disease. Am J Med. 1992;93:8S–12S.
37 Tell GS, Polak JF, Ward BJ, et al. Relation of smoking with carotid artery wall thickness and stenosis in older adults. The Cardiovascular Health Study. The Cardiovascular Health Study (CHS) Collaborative Research Group. Circulation. 1994;90:2905–2908.
38 Howard G, Manolio TA, Burke GL, et al. Does the association of risk factors and atherosclerosis change with age? An analysis of the combined ARIC and CHS cohorts. The Atherosclerosis Risk in Communities (ARIC) and Cardiovascular Health Study (CHS) investigators. Stroke. 1997;28:1693–1701.
39 Kuller L, Borhani N, Furberg C, et al. Prevalence of subclini-cal atherosclerosis and cardiovascular disease and associa-tion with risk factors in the Cardiovascular Health Study. Am J Epidemiol. 1994;139:1164–1179.
40 Psaty BM, Furberg CD, Kuller LH, et al. Traditional risk factors and subclinical disease measures as pre-dictors of first myocardial infarction in older adults: the Cardiovascular Health Study. Arch Intern Med. 1999;159:1339–1347.
41 Sunyer J, Lamarca R, Alonso J. Smoking after age 65 years and mortality in Barcelona, Spain. Am J Epidemiol. 1998;148:575–580.
42 Tessier JF, Nejjari C, Letenneur L, et al. Smoking and eight-year mortality in an elderly cohort. Int J Tuberc Lung Dis. 2000;4:698–704.
43 Lam TH, He Y, Shi QL, et al. Smoking, quitting, and mor-tality in a Chinese cohort of retired men. Ann Epidemiol. 2002;12:316–320.
160
The American Journal of Geriatric Cardiology (ISSN 1076-7460) is published bimonthly (Jan., March, May, July, Sept., Nov.) by Le Jacq Communications, Inc., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2004 by Le Jacq Communications, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.