Embed Size (px)
Citation preview
L i n i t e g a s t r i q u e e t c a n c e r d u s e i n :
u n e a s s o c i a t i o n b n e p a s m 6 c o n n a i t r e
J.M. CONTE, J.C. SOUQUET, P.J. VALET-FE, F. BERGER, B. MOULINIER H6pital Edouard-Herriot, Lyon (France)
Gastric linitis and breast cancer: an association not to be disregarded
Linitis gastrica y cancer de mama: una asociacion a tener en cuenta
RI~SUMI~
Une 6tude r6trospective a retrouv6 des ant6c6dents de cancer du sein chez 8 des 63 patientes ayant toute une linite gastrique. La fr6quence de cette association (12,7 %) sugg6re une liaison entre ces deux pathologies. L'atteinte gastrique correspond h une m6tastase du cancer mammaire. L'6volution relativement lente de ces linites et leur sensibilit6 ~t la chimioth6rapie au moins dans certains cas font I'int6r6t de la connaissance de cette association.
S U M M A R Y
A restrospective s tudy f o u n d that 8 o f 62 patients with a linitis plastica o f the s tomach had been previously treated f o r a breast carcinoma. The f requency o f this association (12, 7 %) suggests that the two tumors are linked. The gastric tumor appears to be a metastasis o f the breast cancer. Due to their relatively s low evolution and their response to chemotherapy and~or hormonotherapy, these metastatic linitis are worth being recognized.
R E S U M E N
Un estudio retrospectivo permit i6 demostrar la existencia de antecedentes de cancer de m a m a en 63 pacientes diagnosticados de linitis g~istrica. La frecuencia de dsta asociaci6n (12, 7 %) sugiere la existencia de una relaci6n entre ambas patologlas. La afectaci6n g~tr ica corresponde a una metd~tasis del cancer mamario. La evoluci6n relativamente lenta de estas linitis y su sensibilidad a la quimioterapia, al menos en algunos casos, hacen interesante el conocimiento de dsta asociaci6n.
La linite gastrique est une forme particuli6re et rare de cancer gastrique (3 ~ 5 %) [7] ; son indivi- dualisation repose sur des crit6res radiologiques, endoscopiques et sur l'6tude anatomopathologique qui met en 6vidence une infiltration sous- muqueuse de la paroi gastrique par un carcinome peu diff6renci6 [7]. Elle apparait souvent chez des patients d'~ge moyen ou avanc6 et s'av6re de mauvais pronostic ; la survie exc6de exceptionnel- lement un an [12].
Certaines observations, le plus souvent isol6es, ont soulign6 la survenue de linite gastrique chez des patientes trait6es auparavant pour un cancer du sein et ont discut6 la nature primitive ou secondaire de l'atteinte gastrique [3, 9, 13, 14]. Une seule s6rie r6trospective, publi6e par une 6quipe de la Mayo Clinic, confirme la r6alit6 de cette forme de linite [6]. L'int6r6t de sa connais-
sance r6side dans le fait que ces m6tastases diges- tives pourraient s'av6rer chimiosensibles e t /ou hor- monod6pendantes comme les autres m6tastases d'origine mammaire.
A propos d'une observation r6cente oh une telle infiltration tumorale sous-muqueuse s'est av6r6e tr6s chimiosensible, ce travail r6trospectif a cherch6 ~ pr6ciser, parmi les patientes ayant une |inite gastrique, la fr6quence et l'6volution de celles qui avaient 6t6 trait6es auparavant pour un ad6nocarcinome mammaire.
OBSER VA TION
Une femme de 47 ans a 6t6 trait6e par mastec- tomie gauche avec curages ganglionnaires (ad6no- pathies envahies) pour un ad6nocarcinome anapla-
Tir6s ~t part : Dr. B. MOULINIER, Service d'H6patogastroen- t6rologie, Pay/lion H Bis, H6pital Ed. Herriot, F-69437 Lyon Cedex 03 (France)
Mots-cl~s : cancer de l 'estomac, cancer du sein, endosonogra- phie, linite gastrique, m6tastases gastriques.
Key-words : breast cancer, endosonography, gastric linitis, gastric metastases, stomach cancer.
Palabras-clave : cancer gastrico, cancer de mama, endosono- grafia, linitis gastrica, metastasis gastricas.
Acta Endoscopica Vo lume 18 - N ~ 2 - 1988 1 19
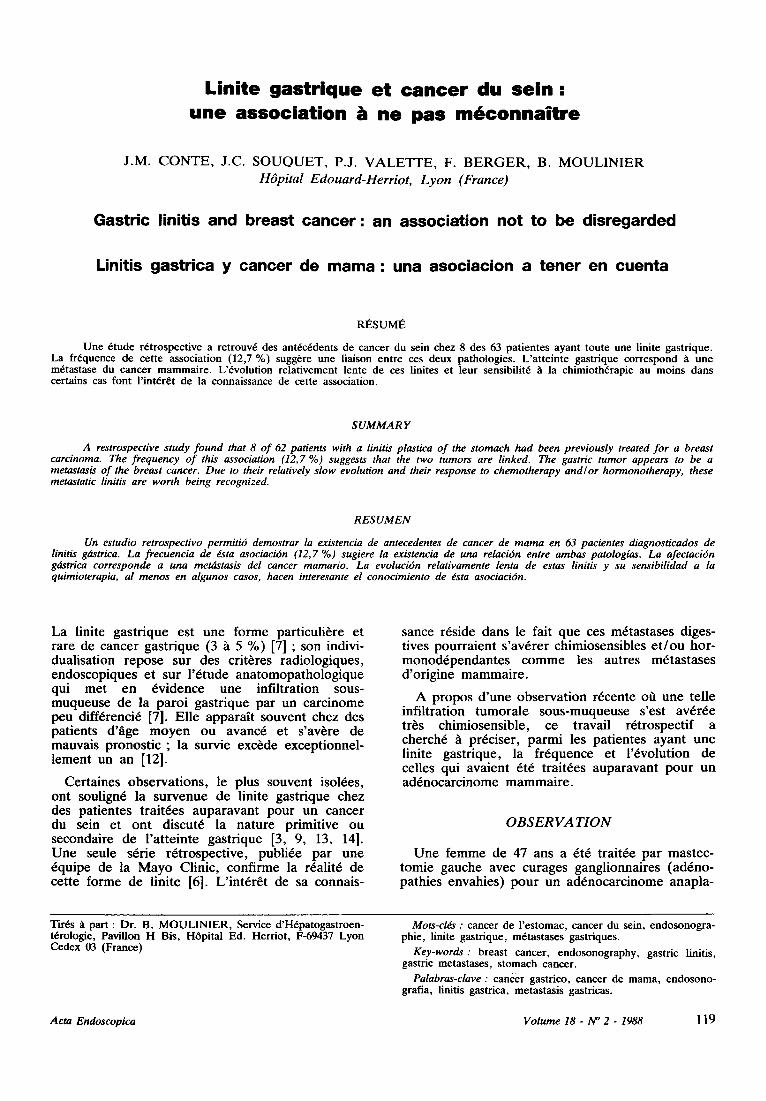
sique du sein gauche en 1977. L'intervention a 6t6 suivie d'une radioth6rapie pelvienne et axillaire puis d'une chimioth6rapie par cyclophosphamide, methotrexate, et fluorouracile (CMF). 11 cures seront r6alis6es jusqu'en 1979. Une hormonoth6ra- pie par tamoxif~ne a 6t6 interrompue en 1982. L'6volution a 6t6 favorable jusqu'en janvier 1986 oO l'6tat g6n6ral de la patiente s'est alt6r6 progres- sivement et of 1 sont apparus des troubles digestifs peu sp6cifiques domin6s par une sensation prEcoce de r6pl6tion gastrique. Une premiere gastroscopie en juillet 1986 a montr6 un estomac infiltr6 avec des plis marqu6s et se distendant real h l'insufla- tion.Les biopsies ont 6t6 n6gatives. Une endosono- graphie (Olympus GF EUM2, 7,5 MHz) a 6t6 alors pratiqu6e qui a montr6 un tr~s net 6paississe- ment de la paroi gastrique fundique essentielle- ment aux d6pens de la couche sous-muqueuse (figure 1). L'aspect permettait d'affirmer la linite
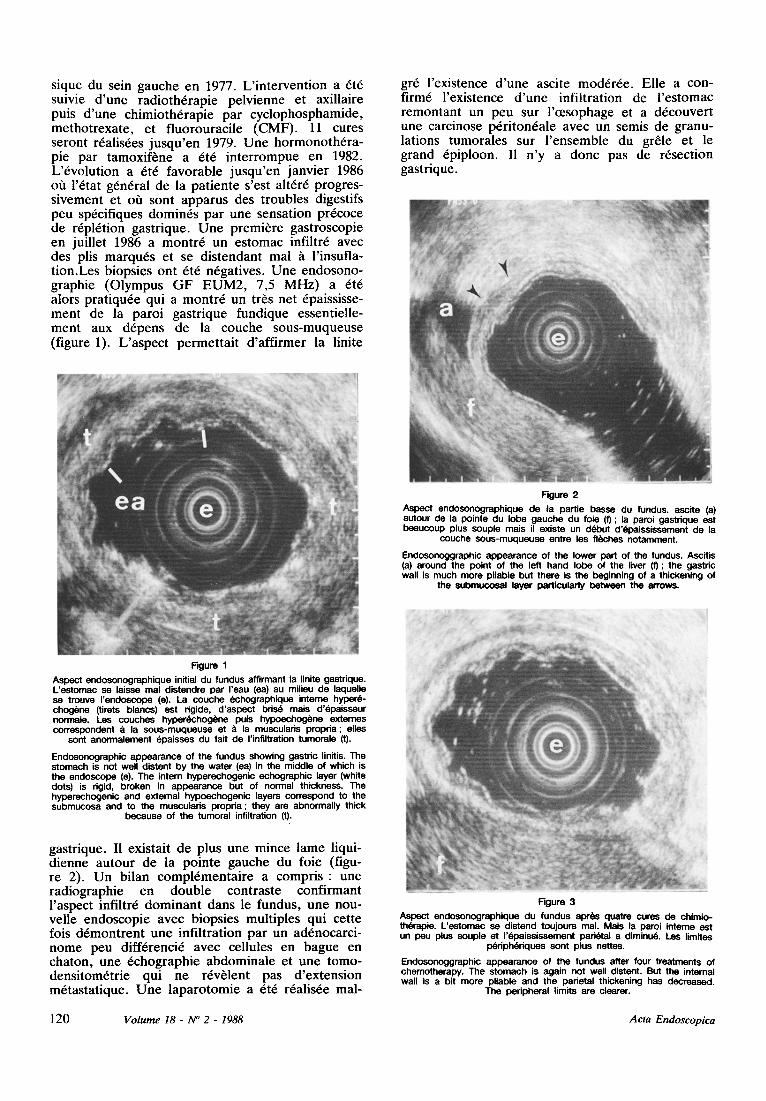
gr6 l'existence d'une ascite mod6r6e. Elle a con- firm6 l'existence d'une infiltration de l'estomac remontant un peu sur l'0esophage et a d6couvert une carcinose p6riton6ale avec un semis de granu- lations tumorales sur l'ensemble du grSle et le grand 6piploon. I1 n'y a donc pas de r6section gastrique.
Figure 2
Aspect andosonographique de la pattie basse du fundus, ascite (a) autour de la pointe du lobe gauche du foie (f) ; la paroi gastrique est beaucoup plus souple mais il existe un d(Yout d'(~oaississement de la
couche sous-muqueuse entre les fl6ches notamment.
Endosonoggraphic appearance of the lower part of the fundus. Ascitis (a) around the point of the left hand lobe of the liver (t) ; the gastric wall is much more pliable but there is the beginning of a thickening of
the submucoeal layer particularly between the arrows.
Figure 1 Aspect andosonographique initial du fundus affirmant la linite gastrique. L'estomac se laisse real distendre par reau (ea) au milieu de laquelle se trouve I'endoscope (e). La couche echographique interne hyper~- chog6ne (tirats biancs) est rigide, d'aspect bds6 mais d'epaisseur normale. Les couches hyper~chogi~ne puis hypoechog6ne externes correspondent tl la sous-muqueuse et & la muscularis propria; elias
sont anormalement 6paisses du fait de I'infiltration tumorale (t).
Endosonographic appearance of the fundus showing gastric linitis. The stomach is not well distant by the water (ea) in the middle of which is the endoscope (e). The intern hyperechogenic echographic layer (white dots) is rigid, broken in appearance but of normal thickness. The hyperechogenic and extemal hypoechogenic layers correspond to the submucosa and to the musculeris propria; they are abnormally thick
because of the tumoral infiltration (t).
gastrique. II existait de plus une mince lame liqui- dienne autour de la pointe gauche du foie (figu- re 2). Un bilan compl6mentaire a compris : une radiographie en double contraste confirmant l'aspect infiltr6 dominant dans le fundus, une nou- velle endoscopie avec biopsies multiples qui cette lois d6montrent une infiltration par un ad6nocarci- nome peu diff6renci6 avec cellules en bague en chaton, une 6chographie abdominale et une tomo- densitom6trie qul ne rEv~lent pas d'extension m6tastatique. Une laparotomie a 6t6 r6alis6e real-
Figure 3
Aspect endosonogrephique du fundus apr~s quatre cures de chimio- th6rapie. L'estomac se distend toujours mal. Mais la paroi interne est un peu plus souple et 1'6paississement parietal a diminud. Les limites
pdriphdriques sont plus nettes.
Endosonoggraphic appearance of the fundus after four treatments of chemotherapy. The stomach is again not well distent. But the internal wall is a bit more pliable and the parietal thickening has decreased.
The peripheral limits are clearer.
120 V o l u m e 1 8 - N ~ 2 - 1 9 8 8 A c t a E n d o s c o p i c a
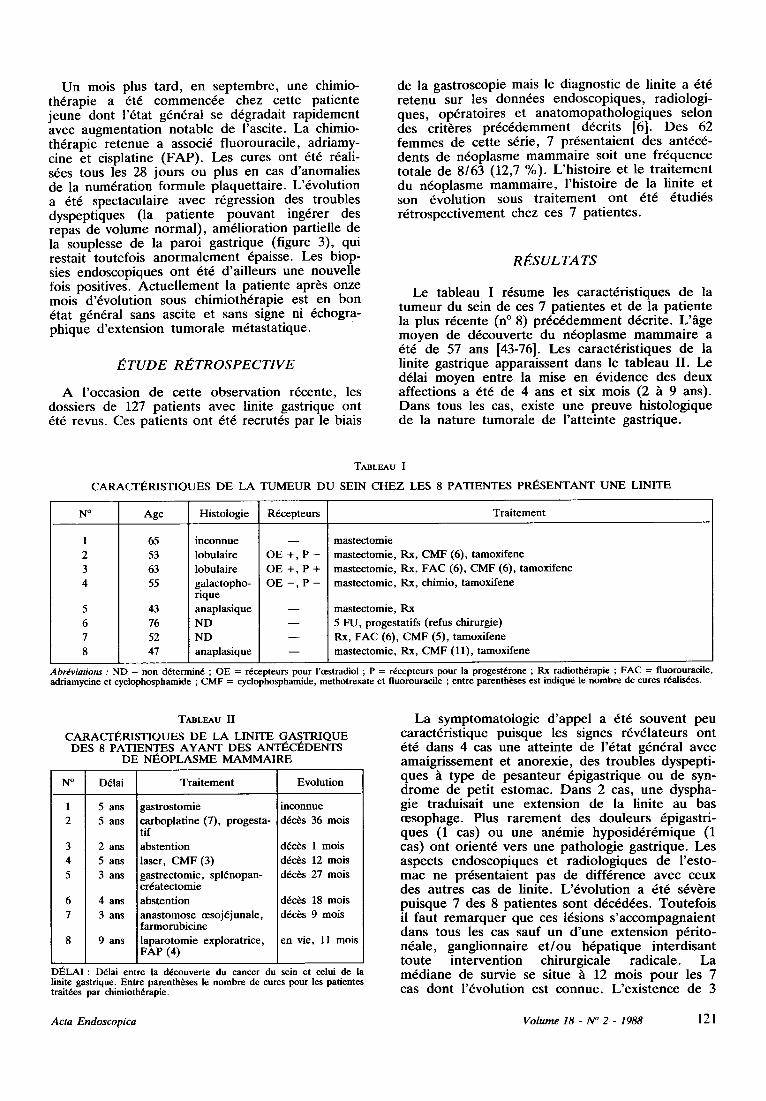
U n mois plus tard , en s ep t embre , une chimio- th6rapie a 6t6 c o m m e n c 6 e chez cet te pat iente j eune dont l '6 tat g6n6ral se d6gradai t r ap idemen t avec augmen ta t i on no tab le de l 'ascite. La chimio- th6rapie re tenue a associ6 f luorouraci le , adr iamy- cine et cisplatine ( F A P ) . Les cures ont 6t6 r6ali- s6es t o u s l e s 28 jours ou plus en cas d ' anomal ies de la num6ra t ion fo rmule p laquet ta i re . L '6vo lu t ion a 6t6 spectaculaire avec r6gression des t roubles dyspept iques (la pa t i en te p o u v a n t ing6rer des repas de vo lume no rma l ) , am61iorat ion partielle de la souplesse de la pa ro i gas t r ique (figure 3), qui restait toutefois a n o r m a l e m e n t 6paisse. Les biop- sies endoscop iques on t 6t6 d 'a i l leurs une nouvel le lois positives. A c t u e l l e m e n t la pa t ien te apr6s onze mois d '6volu t ion sous ch imio th6rap ie est en bon 6tat g6n6ral sans asci te et sans signe ni 6chogr a- ph ique d ' ex tens ion t u m o r a l e m6tas ta t ique .
l ~ T U D E RE, T R O S P E C T I V E
A l 'occas ion de ce t t e obse rva t ion r6cente , les dossiers de 127 pa t ien ts avec linite gastr ique on t 6t6 revus. Ces pa t ien ts on t 6t6 recrut6s par le biais
de la gas t roscopie mais le d iagnost ic de linite a 6t6 r e t enu sur les donn6es e n d o s c o p i q u e s , radio logi - ques , op6ra to i res et a n a t o m o p a t h o l o g i q u e s se lon des cri t6res p r 6 c 6 d e m m e n t d6cri ts [6]. D e s 62 f e m m e s de cet te s6rie, 7 p r6sen ta ien t des ant6c6- dents de n6op lasme m a m m a i r e soit une f r6quence to ta le de 8 /63 (12,7 %). L 'h i s to i re et le t r a i t emen t du n6op la sme m a m m a i r e , l 'h is to i re de la linite et son 6volu t ion sous t r a i t emen t on t 6t6 6tudi6s r6 t rospec t ivemen t chez ces 7 pa t ientes .
R I ~ S U L T A T S
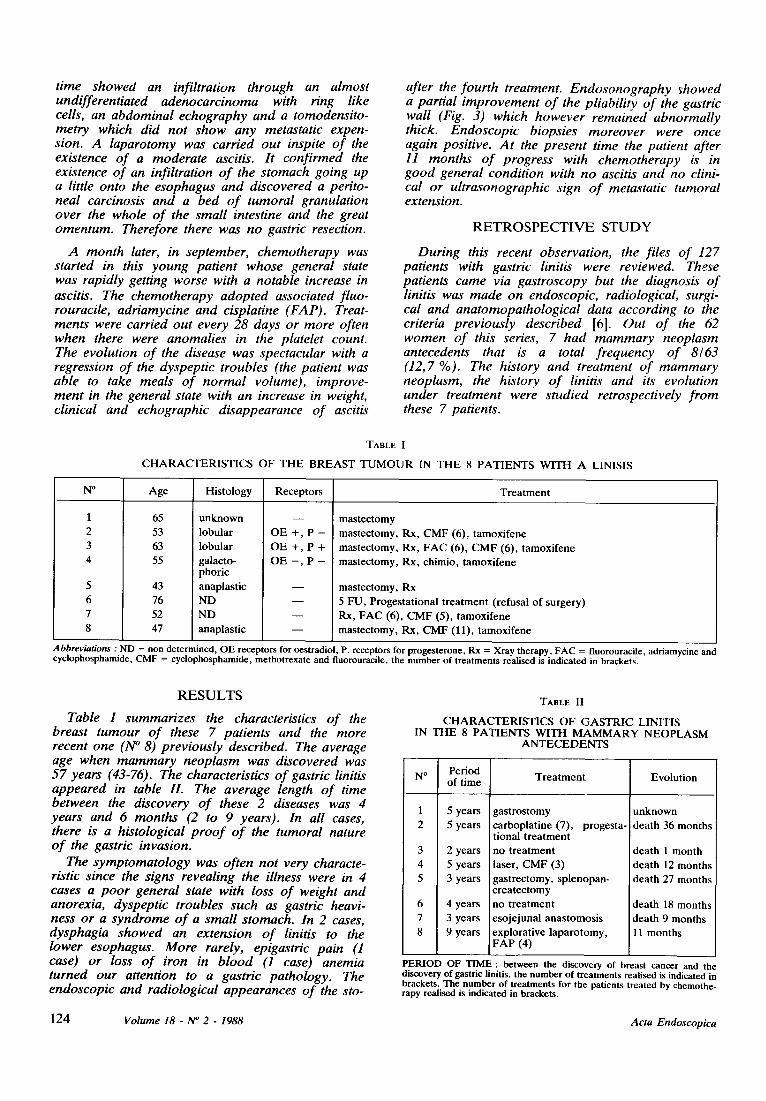
Le tab leau I r6sume les carac t6r is t iques de la t u m e u r du sein de ces 7 pa t ien tes et de la pa t i en te la plus r6cente (n ~ 8) p r 6 c 6 d e m m e n t d6cri te . L ' h g e m o y e n de d6couver te du n 6 o p l a s m e m a m m a i r e a 6t6 de 57 ans [43-76]. Les carac t6r is t iques de la linite gas t r ique appara issent dans le t ab leau I I . Le d61ai m o y e n ent re la mise en 6v idence des deux affect ions a 6t6 de 4 ans et six mois (2 ~ 9 ans). D a n s t o u s l e s cas, existe une p r euve h i s to log ique de la na ture tumora le de l ' a t te in te gas t r ique .
TABLEAU I
CARACTI~RISTIQUES DE LA TUMEUR DU SEIN CHEZ LES 8 PATIENTES PRI~SENTANT UNE LINITE
N ~ Age Histologie R6cepteurs Traitement
65 53 63 55
43 76 52 47
inconnue lobulaire lobulaire galactopho- rique anaplasique ND ND anaplasique
OE +, P - OE + , P + OE - , P -
mastectomie mastectomie, Rx, CMF (6), tamoxifene mastectomie, Rx, FAC (6), CMF (6), tamoxifene mastectomie, Rx, chimio, tamoxifene
mastectomie, Rx 5 FU, progestatifs (refus chirurgie) Rx, FAC (6), CMF (5), tamoxifene mastectomie, Rx, CMF (11), tamoxifene
Abrdviations : ND = non d6termin6 ; OE = r6cepteurs pour l'oestradiol ; P = r6cepteurs pour la progest6rone ; Rx radioth6rapie ; FAC = fluorouracile, adriamycine et cyclophosphamide ; CMF = cyclophosphamide, methotrexate et fluorouracile ; entre parenth6ses est indiqu6 le nombre de cures r6alis6es.
TABLEAU II
CARACTI~RISTIQUES DE LA LINITE GASTRIQUE DES 8 PATIENTES AYANT DES ANTI~CI~DENTS
DE Ni~OPLASME MAMMAIRE
N ~ D61ai Traitement Evolution
1 5 ans gastrostomie inconnue 2 5 ans carboplatine (7), progesta- d6c6s 36 mois
tif 3 2 ans abstention d6c6s 1 mois 4 5 ans laser, CMF (3) d6c6s 12 mois 5 3 ans gastrectomie, spl6nopan- d6c6s 27 mois
cr6atectomie 6 4 ans abstention d6c6s 18 mois 7 3 ans anastomose cesoj6junale, d6c6s 9 mois
farmorubicine 8 9 alas laparotomie exploratrice, en vie, 11 mois
FAP (4)
DI~LAI : D~lai entre la d6couverte du cancer du sein et celui de la linite gastrique. Entre parenth6ses le nombre de cures pour les patientes trait6es par chimioth6rapie.
L a s y m p t o m a t o l o g i e d ' a p p e l a 6t6 s o u v e n t peu carac t6r is t ique puisque les signes r6v61ateurs on t 6t6 dans 4 cas une a t te inte de l '6 ta t g6n6ral avec ama ig r i s semen t et anorexie , des t roub les dyspept i - ques ~ type de pe san t eu r 6pigas t r ique ou de syn- d r o m e de pet i t e s tomac . D a n s 2 cas, une dyspha- gie t raduisai t une ex tens ion de la linite au bas ~esophage. Plus r a r e m e n t des dou leu r s 6pigastr i- ques (1 cas) ou une an6mie h y p o s i d 6 r 6 m i q u e (1 cas) on t or ien t6 vers une pa tho log i e gas t r ique . Les aspects endoscop iques et r ad io log iques de l ' es to- m a c ne pr6sen ta ien t pas de di f f6rence avec ceux des au t res cas de linite. L ' 6 v o l u t i o n a 6t6 s6v6re pu i sque 7 des 8 pat ientes sont d6c6d6es . Tou te fo i s il faut r e m a r q u e r que ces 16sions s ' a c c o m p a g n a i e n t dans t o u s l e s cas sauf un d ' u n e ex tens ion p6r i to- n6ale , gangl ionnai re e t / o u h6pa t ique in te rd i san t t ou t e in te rvent ion chirurgicale radica le . L a m 6 d i a n e de survie se situe h 12 mois p o u r les 7 cas d o n t l '6volu t ion est c o n n u e . L ' ex i s t ence de 3
Acta Endoscopica Volume 18- N ~ 2 - 1988 121
survies prolong6es /~ plus de 18 mois dont 2 en l 'absence de toutes r6sections chirurgicales est noter dans de telles conditions.
D I S C U S S I O N
Le cancer du sein est le plus fr6quent des n6o- plasmes f6minins puisque touchant environ une femme sur treize [8]. I1 est caract6ris6 par des m6tastases fr6quentes, parfois tardives, et qui r6pondent souvent h la chimioth6rapie ou aux trai- tements h vis6e hormonale [2]. Les m6tastases digestives de cancer mammaire autres qu'h6pati- ques ont 6t6 surtout d6crites par les s6ries autopsi- ques [1,4]. Celles-ci montrent que les localisations gastriques secondaires sont les plus f r6quentes (5 15 %) devant les localisations coliques [5]. Les 16sions gastriques se pr6sentent le plus souvent sous forme d 'une infiltration de la sous- muqueuse et de la musculaire propre ressemblant ~ celle observ6e dans la linite [1]. Des 16sions nodulaires sont possibles mais plus rares, elles envahissent la paroi gastrique ~ partir de la s6reuse et peuvent s 'ulc6rer h la surface de la muqueuse.
Quelques cas isol6s de linite survenant dans les suites de cancer du sein ont fait discuter la patho- g6nie de l 'a t teinte tumorale gastrique et noter leur 6volution relat ivement lente, ce qui est exception- nel dans les linites habituelles [6]. Mais c 'est ~ une 6tude r6cente de WJ Cormier et al [6] que revient le m6rite d 'avoir soulign6 la fr6quence relative (31 cas en 30 ans) et les cons6quences th6rapeutiques de cette association. Ces donn6es sont confirm6es par notre travail qui 6tudie r6trospect ivement une s6rie de linites gastriques cons6cutives recrut6es par l ' interm6diaire de l 'endoscopie. 12,5 % des patientes avec une linite gastrique avaient 6t6 trai- t6es auparavant pour un cancer du sein. Ce pour- centage 61ev6 sugg~re bien une liaison entre les deux pathologies.
Le d6veloppement de deux cancers est une 6ventualit6 rare et pourrait 6tre favoris6e par la chimioth6rapie administr6e lors du t ra i tement du premier cancer. 6 des 8 patientes de cet te s6rie ont 6t6 effect ivement trait6es par diverses chimio- th6rapies. Toutefois le suivi de pat ientes trait6es pour un cancer du sein montre que l 'apparit ion d 'un second cancer est un ph6nom6ne rare et que la tumeur est alors except ionnel lement digestive [5].
Dans la plupart des cas de notre s6rie comme de ceux de la lit t6rature, la linite s 'accompagne de m6tastases osseuses, h6patiques ou p6riton6ales, 6voquant une diss6mination g6n6ralis6e. Ainsi, chez la pat iente n ~ des m6tastases sous-cutan6es puis osseuses ont pr6c6d6 le diagnostic de linite de 18 et 6 mois respectivement. Dans cet te 6tude r6trospective, il s 'est av6r6 impossible de comparer l 'histologie des tumeurs mammaires et gastriques. Toutefois dans les cas de la li t t6rature of~ cette
comparaison a 6t6 possible, les deux 16sions ont les m6mes aspects histologiques [6], apportant un argument suppl6mentaire pour la nature secon- daire de la 16sion gastrique. Des r6cepteurs l 'oestradiol ont 6t6 mis en 6vidence au niveau des cellules tumorales gastriques dans le cas (n ~ 7) de cette s6rie. Toutefois cette constatation ne consti- tue pas une preuve v6ritable de la filiation entre les deux tumeurs . Au total, il est logique de consid6rer ces 16sions gastriques comme secon- daires h celles du sein.
Le d61ai de 4 h 5 ans entre le diagnostic des 2 tumeurs correspond h ce qui a 6t6 d6crit dans la s6rie de la Mayo Clinic et aux donn6es concernant les m6tastases du cancer du sein [2]. I1 faut toute- lois signaler la possibilit6 de d6couverte concom- mitante des deux n6oplasmes [12, 14]. La pr6ces- sion de la linite sur le cancer du sein semble exceptionnelle. Les tumeurs lobulaires du sein donneraient pr6f6rentiel lement ces linites m6tasta- tiques [6]. Toutefois notre observation montre que des tumeurs anaplasiques peuvent aussi avoir ce type de diss6mination.
Les caract6ristiques cliniques, endoscopiques ou radiologiques de la linite m6tastatique sont sans particularit6 par rappor t aux autres formes de linite gastrique. Les m6mes difficult6s de diagnos- tic sont rencontr6es. I1 faut signaler ici, ~ propos de notre observat ion, l 'int6r6t potentiel de l 'endo- sonographie pour la mise en 6vidence de l'infiltra- tion tumorale sous-muqueuse [10, 15] et pour la surveillance des t rai tements chimioth6rapiques. Cette propri6t6 a d'ailleurs dgj~ 6t6 rapport6e pour les lymphomes gastriques [16].
I1 est surtout impor tant de consid6rer l '6volution de ces 8 patientes. Des 8 patientes, une seule a pu subir une r6section gastrique, car dans les 7 autres cas la diffusion tumora le s 'opposait ~ toute r6sec- tion. l 'extension des 16sions au d6part, 3 survies sup6rieures ou 6gales ~ 18 mois sont observ6es et une pat iente est en vie avec un recul de 11 mois apr6s avoir pr6sent6 une r6ponse object ive ~ la chimioth6rapie. Cet te chimioth6rapie est du type de celle utilis6e dans les ad6nocarcinomes gastri- ques mais le f luorouraci le et l 'adriblastine ont sans conteste une efficacit6 dans le t ra i tement des m6tastases mammaires . Cormier et al [6] rappor- tent une survie sup6rieure ~ 2 ans dans plus d 'un tiers des 31 cas de leur s6rie, une constatat ion similaire ~t la n6tre. Ces notions poussent ~ trai ter ces linites comme des m6tastases du cancer du sein. L'uti l isation d 'une chimioth6rapie et d 'une hormonoth6rapie doit 6tre probablement pr6f6r6e
la chirurgie qui, dans ce contexte de diss6mina- tion n6oplasique, a peu de chance d '6tre curative.
En conclusion, ce travail montre la f r6quence relative de l 'association cancer du sein-linite gastri- que. Cette derni6re correspond au moins dans certains cas ~ une m6tastase du n6oplasme mam- maire et r6pond ~ la chimioth6rapie et ~ l 'hormo- noth6rapie. Son t ra i tement doit donc 6tre diff6rent d 'une linite gastrique habituelle. I1 est donc impor-
122 V o l u m e 18 - N ~ 2 - 1 9 8 8 A c t a E n d o s c o p i c a
tant devant route linite chez une femme de recher- chef les an t rcrdents de nroplasme du sein et de rraliser un bilan mammaire pour 61iminer une
association de ce type en raison des possibilitrs thrrapeutiques suggrrres par notre 6tude et les cas de la l i t trrature.
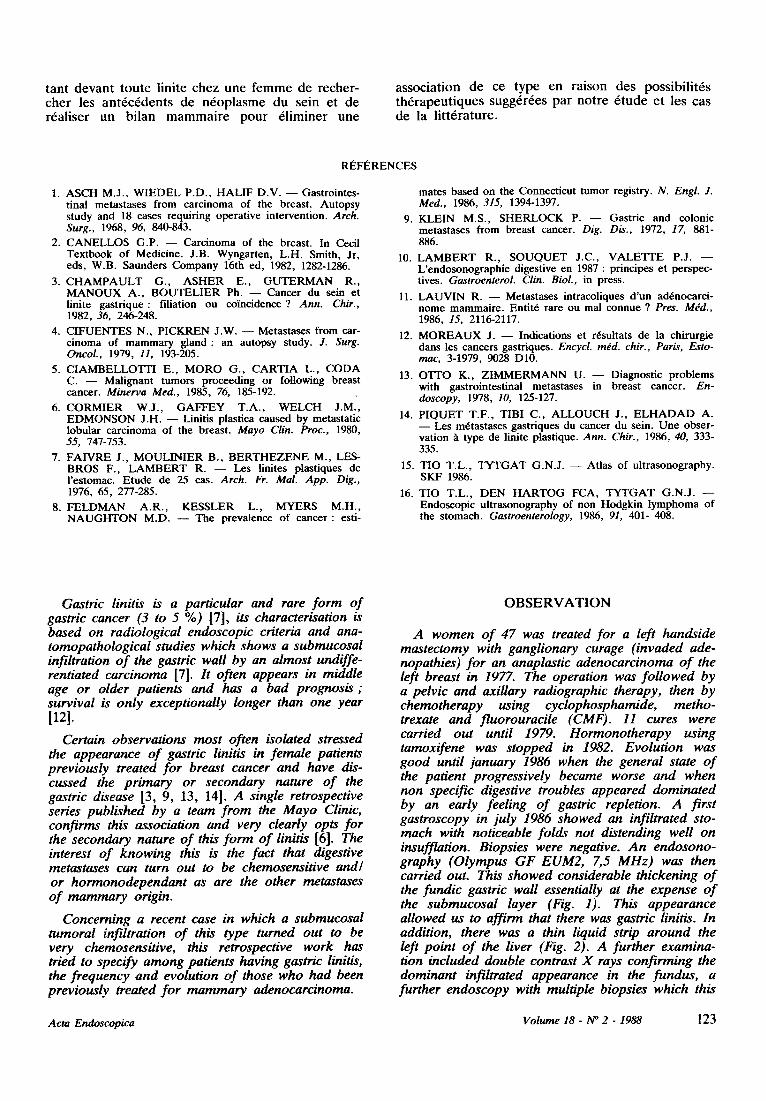
RI~.F~RENCES
1. ASCH M.J., WIEDEL P.D., HALIF D.V. - - Gastrointes- tinal metastases from carcinoma of the breast. Autopsy study and 18 cases requiring operative intervention. Arch. Surg., 1968, 96, 840-843.
2. CANELLOS G.P. - - Carcinoma of the breast. In Cecil Textbook of Medicine. J.B. Wyngarten, L.H. Smith, Jr, eds, W.B. Saunders Company 16th ed, 1982, 1282-1286.
3. C H A M P A U L T G., A S H E R E., G U T E R M A N R., M A N O U X A. , B O U T E L I E R Ph. - - Cancer du sein et linite gastr ique: filiation ou coincidence ? Ann. Chir., 1982, 36, 246-248.
4. CIFUENTES N., PICKREN J.W. - - Metastases from car- cinoma of mammary g land: an autopsy study. J. Surg. Oncol., 1979, 11, 193-205.
5. CIAMBELLOTTI E., M O R O G., C A R T I A L., COD A C. - - Malignant tumors proceeding or following breast cancer. Minerva Med., 1985, 76, 185-192.
6. C ORMIER W.J. , GAFFEY T.A. , WELCH J.M., EDMONSON J.H. - - Linitis plastica caused by metastatic lobular carcinoma of the breast. Mayo Clin. Proc., 1980, 55, 747-753.
7. FAIVRE J., MOULINIER B., B E R T H E Z E N E M., LES- BROS F., L A M B E R T R. - - Les linites plastiques de I'estomac. Etude de 25 cas. Arch. Fr. Mal. App. Dig., 1976, 65, 277-285.
8. FELDMAN A.R. , KESSLER L., MYERS M.H., N A U G H T O N M.D. - - The prevalence of cancer : esti-
mates based on the Connecticut tumor registry. N. Engl. J. Med., 1986, 315, 1394-1397.
9. KLEIN M.S., SHERLOCK P. - - Gastric and colonic metastases from breast cancer. Dig. Dis., 1972, 17, 881- 886.
10. L A M B E R T R., S O U Q U E T J.C., V A L E T r E P.J. - - L'endosonographie digestive en 1987 : principes et perspec- tives. Gastroenterol. Clin. Biol., in press.
11. LAUVIN R. - - Metastases intracoliques d 'un adrnocarci- nome mammaire. Entit6 rare ou mal connue ? Pres. M~d., 1986, 15, 2116-2117.
12. M O R E A U X J. - - Indications et rrsultats de la chirurgie dans les cancers gastriques. Encycl. mdd. chir., Paris, Esto- mac, 3-1979, 9028 D10.
13. OTTO K., Z IMMERMA N N U. - - Diagnostic problems with gastrointestinal metastases in breast cancer. En- doscopy, 1978, 10, 125-127.
14. P IQ U ET T.F. , TIBI C., A L L O U C H J., E L H A D A D A. - - Les mrtastases gastriques du cancer du sein. Une obser- vation ~ type de linite plastique. Ann. Chir., 1986, 40, 333- 335.
15. TIO T.L. , T Y T G A T G.N.J. - - Atlas of ultrasonography. SKF 1986.
16. TIO T.L. , DEN H A R T O G FCA, T Y T G A T G.N.J. - - Endoscopic ultrasonography of non Hodgkin lymphoma of the stomach. Gastroenterology, 1986, 91, 401- 408.
Gastric linitis is a particular and rare form of gastric cancer (3 to 5 %) [7], its characterisation is based on radiological endoscopic criteria and ana- tomopathological studies which shows a submucosal infiltration o f the gastric wall by an almost undiffe- rentiated carcinoma [7]. It often appears in middle age or older patients and has a bad prognosis ; survival is only exceptionally longer than one year [12].
Certain observations most often isolated stressed the appearance o f gastric linitis in female patients previously treated for breast cancer and have dis- cussed the primary or secondary nature o f the gastric disease [3, 9, 13, 14]. A single retrospective series published by a team from the Mayo Clinic, confirms this association and very clearly opts for the secondary nature o f this form of linitis [6]. The interest o f knowing this is the fact that digestive metastases can turn out to be chemosensitive and/ or hormonodependant as are the other metastases o f mammary origin.
Concerning a recent case in which a submucosal tumoral infiltration o f this type turned out to be very chemosensitive, this retrospective work has tried to specify among patients having gastric linitis, the frequency and evolution o f those who had been previously treated for mammary adenocarcinoma.
O B S E R V A T I O N
A women o f 47 was treated for a left handside mastectomy with ganglionary curage (invaded ade- nopathies) for an anaplastic adenocarcinoma o f the left breast in 1977. The operation was followed by a pelvic and axillary radiographic therapy, then by chemotherapy using cyclophosphamide, metho- trexate and fluorouracile (CMF). 11 cures were carried out until 1979. Hormonotherapy using tamoxifene was stopped in 1982. Evolution was good until january 1986 when the general state o f the patient progressively became worse and when non specific digestive troubles appeared dominated by an early feeling o f gastric repletion. A first gastroscopy in july 1986 showed an infiltrated sto- mach with noticeable folds not distending well on insufflation. Biopsies were negative. An endosono- graphy (Olympus GF EUM2, 7,5 MHz) was then carried out. This showed considerable thickening o f the fundic gastric wall essentially at the expense o f the submucosal layer (Fig. 1). This appearance allowed us to affirm that there was gastric linitis. In addition, there was a thin liquid strip around the left point o f the liver (Fig. 2). A further examina- tion included double contrast X rays confirming the dominant infiltrated appearance in the fundus, a further endoscopy with multiple biopsies which this
Acta Endoscopica Volume 18- lV ~ 2 - 1988 123
time showed an infiltration through an almost undifferentiated adenocarcinoma with ring like cells, an abdominal echography and a tomodensito- metry which did not show any metastatic expen- sion. A laparotomy was carried out inspite of the existence of a moderate ascitis. It confirmed the existence of an infiltration of the stomach going up a little onto the esophagus and discovered a perito- neal carcinosis and a bed of tumoral granulation over the whole of the small intestine and the great omentum. Therefore there was no gastric resection.
A month later, in september, chemotherapy was started in this young patient whose general state was rapidly getting worse with a notable increase in ascitis. The chemotherapy adopted associated fluo- rouracile, adriamycine and cisplatine (FAP). Treat- ments were carried out every 28 days or more often when there were anomalies in the platelet count. The evolution of the disease was spectacular with a regression of the dyspeptic troubles (the patient was able to take meals of normal volume), improve- ment in the general state with an increase in weight, clinical and echographic disappearance of ascitis
after the fourth treatment. Endosonography showed a partial improvement of the pliability of the gastric wall (Fig. 3) which however remained abnormally thick. Endoscopic biopsies moreover were once again positive. At the present time the patient after 11 months of progress with chemotherapy is in good general condition with no ascitis and no clini- cal or uhrasonographic sign of metastatic tumoral extension.
R E T R O S P E C T I V E S T U D Y
During this recent observation, the files of 127 patients with gastric linitis were reviewed. These patients came via gastroscopy but the diagnosis of linitis was made on endoscopic, radiological, surgi- cal and anatomopathological data according to the criteria previously described [6] . Out of the 62 women of this series, 7 had mammary neoplasm antecedents that is a total frequency of 8/63 (12,7 %). The history and treatment of mammary neoplasm, the history of linitis and its evolution under treatment were studied retrospectively from these 7 patients.
TABLE I
C H A R A C T E R I S T I C S O F T H E B R E A S T T U M O U R IN T H E 8 P A T I E N T S W I T H A LINISIS
N ~ Age His tology Receptors T r e a t m e n t
65 53
63 55
43 76
52 47
u n k n o w n lobular lobular
galacto- phoric
anaplast ic N D
N D
anaplast ic
O E + , P -
O E + , P + O E - , P -
mas tec tomy
mas tec tomy, Rx, C M F (6), t amoxi fene
mas tec tomy, Rx, F A C (6), C M F (6), t amoxi fene mas tec tomy, Rx, chimio, t amoxi fene
mas tec tomy, Rx
5 FU, Progesta t ional t r ea tmen t (refusal of surgery) Rx, F A C (6), C M F (5), t amoxi fene
mas tec tomy, Rx, C M F (11), t amoxi fene
Abbreviations : ND = non determined, OE receptors for oestradiol, P. receptors for progesterone, Rx = Xray therapy, FAC = fluorouracile, adriamycine and cyclophosphamide, CMF = cyciophosphamide, methotrexate and fluorouracile, the number of treatments realised is indicated in brackets.
R E S U L T S
Table I summarizes the characteristics of the breast tumour of these 7 patients and the more recent one (N ~ 8) previously described. The average age when mammary neoplasm was discovered was
Period 57 years (43-76). The characteristics of gastric linitis N ~ of t ime
appeared in table IL The average length of time between the discovery of these 2 diseases was 4
1 5 years years and 6 months (2 to 9 years). In all cases, 2 5 years there is a histological proof of the tumoral nature of the gastric invasion. 3 2 years
The symptomatology was often not very characte- 4 5 years ristic since the signs revealing the illness were in 4 5 3 years cases a poor general state with loss of weight and anorexia, dyspeptic troubles such as gastric heavi- 6 4 years
ness or a syndrome of a small stomach. In 2 cases, 7 3 years
dysphagia showed an extension of linitis to the 8 9 y e a r s lower esophagus. More rarely, epigastric pain (1 case) or loss of iron in blood (1 case) anemia turned our attention to a gastric pathology. The endoscopic and radiological appearances of the sto-
TAaLE II
C H A R A C T E R I S T I C S O F G A S T R I C LINITIS IN T H E 8 P A T I E N T S W I T H M A M M A R Y N E O P L A S M
A N T E C E D E N T S
T r e a t m e n t Evolut ion
gas t ros tomy carboplat ine (7), progesta- tional t r ea tmen t
no t r ea tment laser, C M F (3) gas t ree tomy, sp lenopan- c rea tec tomy
no t r ea tmen t eso je juna l anas tomos i s explorat ive l aparo tomy, F A P (4)
u n k n o w n
dea th 36 mon ths
dea th 1 mon th dea th 12 mon ths dea th 27 months
dea th 18 mon ths dea th 9 months 11 mon ths
PERIOD OF TIME : between the discovery of breast cancer and the discovery of gastric linitis, the number of treatments realised is indicated in brackets. The number of treatments for the patients treated by chemothe- rapy realised is indicated in brackets.
124 Volume 18 - N ~ 2 - 1988 Acta Endoscopica
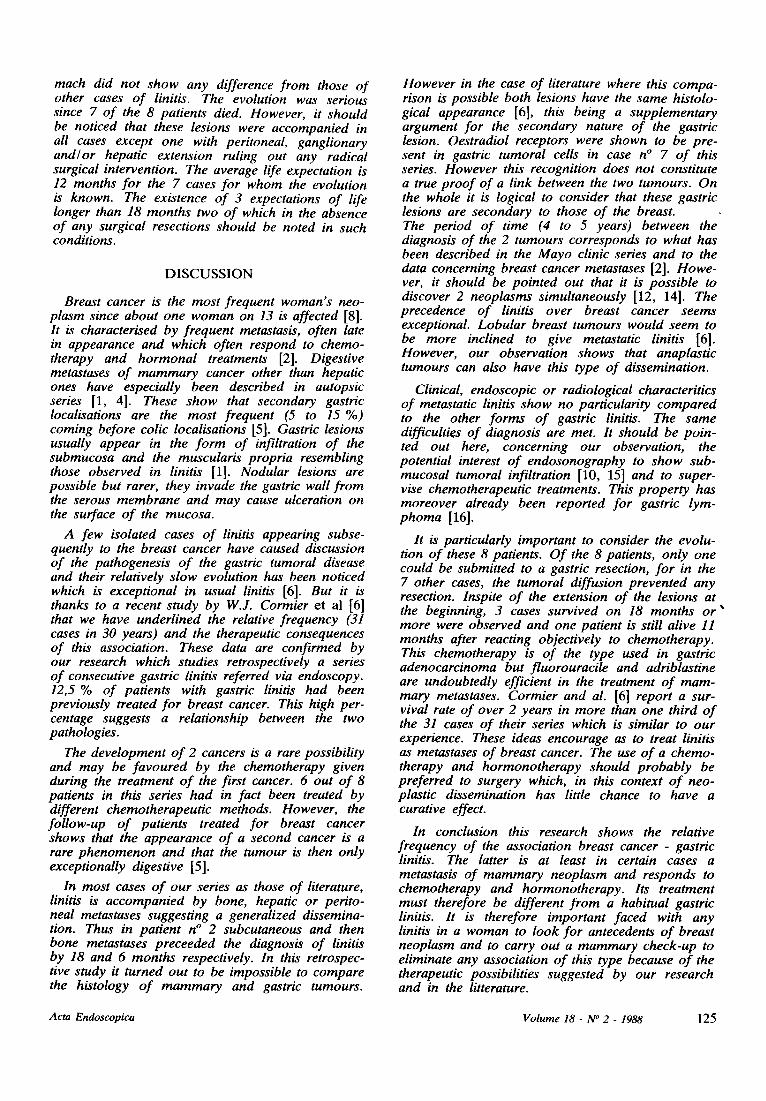
mach did not show any difference from those of other cases of linitis. The evolution was serious since 7 of the 8 patients died. However, it should be noticed that these lesions were accompanied in all cases except one with peritoneal, ganglionary and~or hepatic extension ruling out any radical surgical intervention. The average life expectation is 12 months for the 7 cases for whom the evolution is known. The existence of 3 expectations of life longer than 18 months two of which in the absence of any surgical resections should be noted in such conditions.
DISCUSSION
Breast cancer is the most frequent woman's neo- plasm since about one woman on 13 is affected [8]. It is characterised by frequent metastasis, often late in appearance and which often respond to chemo- therapy and hormonal treatments [2]. Digestive metastases o f mammary cancer other than hepatic ones have especially been described in autopsic series [1, 4]. These show that secondary gastric localisations are the most frequent (5 to 15 %) coming before colic localisations [5]. Gastric lesions usually appear in the form of infiltration of the submucosa and the muscularis propria resembling those observed in linitis [1]. Nodular lesions are possible but rarer, they invade the gastric wall from the serous membrane and may cause ulceration on the surface of the mucosa.
A few isolated cases of linitis appearing subse- quently to the breast cancer have caused discussion of the pathogenesis o f the gastric tumoral disease and their relatively slow evolution has been noticed which is exceptional in usual linitis [6]. But it is thanks to a recent study by W.J. Cormier et al [6] that we have underlined the relative frequency (31 cases in 30 years) and the therapeutic consequences of this association. These data are confirmed by our research which studies retrospectively a series of consecutive gastric linitis referred via endoscopy. 12,5 % of patients with gastric linitis had been previously treated for breast cancer. This high per- centage suggests a relationship between the two pathologies.
The development o f 2 cancers is a rare possibility and may be favoured by the chemotherapy given during the treatment o f the first cancer. 6 out of 8 patients in this series had in fact been treated by different chemotherapeutic methods. However, the follow-up of patients treated for breast cancer shows that the appearance of a second cancer is a rare phenomenon and that the tumour is then only exceptionally digestive [5].
In most cases of our series as those of literature, linitis is accompanied by bone, hepatic or perito- neal metastases suggesting a generalized dissemina- tion. Thus in patient n ~ 2 subcutaneous and then bone metastases preceeded the diagnosis of linitis by 18 and 6 months respectively. In this retrospec- tive study it turned out to be impossible to compare the histology of mammary and gastric tumours.
However in the case of literature where this compa- rison is possible both lesions have the same histolo- gical appearance [6], this being a supplementary argument for the secondary nature of the gastric lesion. Oestradiol receptors were shown to be pre- sent in gastric tumoral cells in case n ~ 7 of this series. However this recognition does not constitute a true proof of a link between the two tumours. On the whole it is logical to consider that these gastric lesions are secondary to those of the breast. The period of time (4 to 5 years) between the diagnosis of the 2 tumours corresponds to what has been described in the Mayo clinic series and to the data concerning breast cancer metastases [2]. Howe- ver, it should be pointed out that it is possible to discover 2 neoplasms simultaneously [12, 14]. The precedence of linitis over breast cancer seems exceptional. Lobular breast tumours would seem to be more inclined to give metastatic linitis [6]. However, our observation shows that anaplastic tumours can also have this type of dissemination.
Clinical, endoscopic or radiological characteritics of metastatic linitis show no particularity compared to the other forms of gastric linitis. The same difficulties of diagnosis are met. It should be poin- ted out here, concerning our observation, the potential interest of endosonography to show sub- mucosal tumoral infiltration [10, 15] and to super- vise chemotherapeutic treatments. This property has moreover already been reported for gastric lym- phoma [16].
It is particularly important to consider the evolu- tion of these 8 patients. Of the 8 patients, only one could be submitted to a gastric resection, for in the 7 other cases, the tumoral diffusion prevented any resection. Inspite of the extension of the lesions at the beginning, 3 cases survived on 18 months or" more were observed and one patient is still alive 11 months after reacting objectively to chemotherapy. This chemotherapy is of the type used in gastric adenocarcinoma but fluorouracile and adriblastine are undoubtedly efficient in the treatment of mam- mary metastases. Cormier and al. [6] report a sur- vival rate of over 2 years in more than one third of the 31 cases of their series which is similar to our experience. These ideas encourage as to treat linitis as metastases of breast cancer. The use of a chemo- therapy and hormonotherapy should probably be preferred to surgery which, in this context of neo- plastic dissemination has little chance to have a curative effect.
In conclusion this research shows the relative frequency of the association breast cancer - gastric linitis. The latter is at least in certain cases a metastasis of mammary neoplasm and responds to chemotherapy and hormonotherapy. Its treatment must therefore be different from a habitual gastric linitis. It is therefore important faced with any linitis in a woman to look for antecedents of breast neoplasm and to carry out a mammary check-up to eliminate any association of this type because of the therapeutic possibilities suggested by our research and in the litterature.
Acta Endoscopica Volume 18- N ~ 2- 1988 125





























