Embed Size (px)
Citation preview

Livedoid vasculitis: a manifestation of the antiphospholipidsyndrome?
K.M.ACLAND, A.DARVAY, S.H.WAKELIN* AND R.RUSSELL-JONESDepartment of Dermatology, Ealing Hospital, Southall, Middlesex, UB1 3HW, U.K.*St John’s Institute of Dermatology, St Thomas’ Hospital, Lambeth Palace Road, London SE1 7EH, U.K.
Accepted for publication 12 August 1998
Summary Livedoid vasculitis, otherwise known as segmental hyalinizing vasculitis or livedo reticularis withsummer ulceration, is a chronic disease with lesions affecting the feet and lower legs. Early lesionsshow petechiae, but characteristic features are recurrent, bizarrely shaped ulcers that heal to leavehyperpigmentation and atrophie blanche. The aetiology of the disorder is unknown, but thehistology shows fibrin deposition within both the wall and lumen of affected vessels. The absenceof a sufficient perivascular infiltrate or leucocytoclasia argues against a vasculitis, being more inkeeping with a thrombo-occlusive process. Four patients with livedoid vasculitis with ulceration aredescribed, all of whom had associated raised anticardiolipin antibodies but no other evidence ofsystemic disease. We suggest that livedoid vasculitis may be a manifestation of the antiphospholipidsyndrome and recommend that all patients are screened for this. We also discuss treatment optionsfor this often resistant condition.
Key words: antiphospholipid syndrome, livedoid vasculitis, livedo reticularis with summer ulceration.
Livedoid vasculitis is an uncommon condition that mostcommonly affects young to middle-aged women. It ischaracterized by purpuric macules and papules of thelower legs and feet. These are due to infarction withinthe small vessels and may break down to form painful,irregularly shaped ulcers, which then heal slowly, leav-ing stellate white scars or atrophie blanche. Livedoidvaculitis is normally described as occurring in isolation,but there have been rare reports of an association withvarious antiphospholipid antibodies. We report fourpatients with livedoid vasculitis, in all of whom thedisease was associated with raised antiphospholipidantibodies and two of whom demonstrated otherfeatures of the antiphospholipid syndrome. Althoughlivedoid vasculitis can occur without autoantibodies, wewould strongly recommend that all patients arescreened for underlying conditions.
Case reports
Patient 1
A 35-year-old man first presented to the accident and
emergency unit of our institution in September 1996with an extensive spontaneous deep vein thrombosis ofhis right femoral vein. He was treated with anti-coagulation. He then presented to the dermatologydepartment in April 1997 with a 1-month history ofan itchy rash on the lower leg. Clinically, there was alivedo pattern of pigmentation, irregular ulceration andevidence of lipodermatosclerosis. The following investi-gations were normal or negative: antineutrophil cyto-plasmic antigen antibodies, autoantibodies, hepatitisscreen, rheumatoid factor, cryoglobulins, complement,antinuclear antibodies, full blood count, erythrocytesedimentation rate (ESR) and liver function tests. How-ever, he did have a raised IgA at 4·47 g/L (normal0·80–2·8 g/L) with normal electrophoresis and araised anticardiolipin antibody of the IgG subclass at13.6 U/mL (normal <9 U/mL). Histology showedevidence of a hyalinizing vasculitis and immuno-fluorescence showed focal deposits of IgM, IgG and C3in the dermal blood vessel walls. He was started on oralaspirin 150 mg daily with good response. Repeat mea-surements of anticardiolipin antibodies were also raised.However, in view of his thrombosis in association withanticardiolipin antibodies, long-term anticoagulationhas now been instituted.
British Journal of Dermatology 1999; 140, 131–135.
131q 1999 British Association of Dermatologists
Correspondence: DrK.M.Acland, Dermatological Surgery and LaserUnit, St John0s Institute of Dermatology, St Thomas’ Hospital, LondonSE1 7EH, U.K.

Patient 2
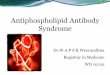
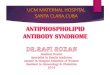
A 27-year-old woman presented in 1979 with a 6-month history of a rash and ulceration on the lowerlegs. These ulcers were bizarre in appearance withsharply demarcated edges, induration and telangiecta-sia (Fig. 1). A diagnosis of dermatitis artefacta wasconsidered, but a biopsy showed evidence of a hyaliniz-ing vasculitis with fibrinoid deposits around the vesselsand thrombosis within (Fig. 2). A vasculitis screen wasentirely normal apart from a markedly raised anti-cardiolipin antibody subclass IgG at 70·9 U/mL(normal <9 U/mL) There was no evidence of anyother associated problems and the patient initiallyresponded well to dapsone 100 mg daily; however, sherelapsed despite an increased dose and failed to respondto nicotinic acid 300 mg and guanethidine 30 mg daily.She was therefore started on stanozolol 5 mg twice daily,to which she had an excellent response. She becamepregnant and had to discontinue treatment with arelapse of her condition. Dapsone was therefore insti-tuted once more, with good effect. This was laterdiscontinued and the patient remains well with nofurther episodes.
Patient 3
A 30-year-old woman presented in 1990 with idio-pathic thrombocytopenic purpura. This resolved withoral steroids. She presented again in December 1992
132 K.M.ACLAND et al.
q 1999 British Association of Dermatologists, British Journal of Dermatology, 140, 131–135
Figure 1. Ulceration, purpura and atrophieblanche are evident on lower legs of patient 2.
Figure 2. Photomicrographs which show hyalinizing vasculitis withfibrinoid deposits around vessels (a) and thrombosis within (b), butwith no evidence of leucocytoclasia (haematoxylin and eosin, originalmagnification, (a) × 40, (b) × 200).

with painful ulcers and swelling of the lower legs andfeet. These healed, leaving atrophie blanche andhyperpigmentation. At that time she was treated withTrental, low-dose aspirin and dapsone, to whichshe responded well. In 1997, she developed furtherulceration and pain, and investigations at that timeshowed a raised anticardiolipin antibody subclass IgMat 43 U/mL normal <10 U/mL). A subsequent test on aseparate occasion showed a raised IgG at 11·1 U/mL.Her ESR was raised at 26 mm/h and IgA low at 0·8 g/L(normal 2·1–4·5 g/L). All other investigations werenormal. Histology showed fibrinoid necrosis and throm-bosis of blood vessels and immunofluorescence showeddeposits of IgM, C3 and fibrin in the vessel walls. Shewas treated with intravenous methylprednisolone andoral prednisolone with moderate response only and wastherefore started on danazol 200 mg daily with goodclinical response. She remains in remission at present.
Patient 4
A 17-year-old man was seen because of a 3-year historyof an intermittent eruption around both ankles. Theseeruptions were associated with ulceration, which wouldthen heal to leave atrophic scars. He was otherwisewell. On examination there was a livedoid rash withhyperpigmentation around the ankles and feet withcribriform ulceration and atrophie blanche. All investi-gations were unremarkable apart from an elevatedanticardiolipin antibody of the IgM subclass at 15·7 U/mL (normal <10 U/mL). He was commenced on aspirin75 mg twice daily
Discussion
Livedoid vasculitis was first described in 1967 by Bardand Winkelman.1 They described patients with atrophieblanche and cutaneous ulceration; six of these patientshad connective tissue disease, and in one lupus anti-coagulant was found. Antiphospholipid antibody testswere not then available. Since then many other nameshave been applied to this condition, including segmentalhyalinizing vasculitis, atrophie blanche, livedo reticu-laris with summer/winter ulceration, hypersensitivity-type vasculitis and most recently the acronym PURPLE2
(painful purpuric ulcers with reticular pattern of thelower extremities) has been coined. Clinically, it ischaracterized by focal purpuric painful lesions thatmay ulcerate and then heal with porcelain-white, stel-late, atrophic scarring, telangiectasia, haemosiderindeposition and hyperpigmentation. The course of the
disease is often chronic with seasonal exacerbations andrecurrences.
The pathogenesis of this condition is not fully under-stood and has been a subject of much debate. Thehistology differs from that of other types of vasculitisin that a perivascular infiltrate and leucocytoclasia areinconspicuous even in early lesions.3 Fibrin depositionoccurs within the walls of affected vessels. There isthrombus formation within the lumen and red cellextravasation in the surrounding dermis. At a latestage there is epidermal atrophy with thickened hyali-nized vessels and deposition of haemosiderin.4 Thesefeatures favour a thrombo-occlusive vasculopathyrather than a vasculitis per se.
The theory of a vaso-occlusive pathogenesis is sup-ported by a number of studies that have looked atmarkers of a thrombotic state. McCalmont et al.5
found elevated fibrinopeptide A levels in six patientswith livedoid vasculitis. This is a peptide that resultsfrom cleavage from thrombin. It is a specific marker ofthrombin generation in vivo but does not point to aspecific thrombotic defect. Pizzo et al.6 found thatpatients with atrophie blanche had defective release ofvascular plasminogen activator when compared withhealthy volunteers, which was confirmed by Klein andPittelkow,7 who also described increased levels ofplasminogen activator inhibitor in these patients.Tsutsui et al.8 reported decreased thrombomodulinexpression in four patients with livedoid vasculitis andhence proposed a mechanism of action for beraprostsodium, a prostacyclin analogue. Thrombomodulin is atransmembrane glycoprotein which, when bound to itscofactor thrombin on endothelial cells, has antithrom-botic function and accelerates the activation of proteinC. Protein C deficiency9 and increased platelet aggrega-tion10 have also been reported in association withlivedoid vasculitis. These findings are also supportedby reports of successful treatment with tissue plasmino-gen activator,7 prostacyclin infusions11 and antiplateletdrugs,12 although there is also a report of failure oftreatment with tissue plasminogen activator.13
Livedoid vasculitis has been described as a sole entity2
and in association with other conditions, primarilysystemic lupus erythematosus, but antiphospholipidantibodies have only been reported rarely.1,14,15 Theassociation of livedo reticularis with anticardiolipinantibodies16 is well known, but an association withlivedoid vasculitis is less clearly defined. However,ulceration and scarring are recognized cutaneous mani-festations of antiphospholipid antibodies and there maybe a subset of patients with antiphospholipid antibodies
LIVEDOID VASCULITIS 133
q 1999 British Association of Dermatologists, British Journal of Dermatology, 140, 131–135

who have livedoid vasculitis.17 Antiphospholipid anti-bodies are a group of autoantibodies directed againstphospholipid compounds. They comprise the lupusanticoagulants and the anticardiolipin antibodies.Phospholipids are important at several points in theextrinsic, intrinsic and common pathways of the coa-gulation cascade18 and, although the link betweenantiphospholipid antibodies and thrombosis has notbeen finalized, a number of mechanisms have beenproposed, including alterations in fibrinolysis and plate-let activation and abnormalities of proteins S and C.19
Recently, potential target antigens for antiphospho-lipid antibodies have been identified. These includeprothrombin, protein S and protein C and B2-glyco-protein (B2-GPI). The effect of antiphospholipid anti-body binding to these targets is variable, for examplethe function of protein C is inhibited but the activity ofB2-GPI is enhanced. B2-GPI enhances binding of anti-phospholipid antibodies to phospholipids and may beessential for the development of the antiphospholipidsyndrome. It has a number of anticoagulant properties,inhibiting the contact phase of blood coagulation andplatelet aggregation and the prothrombinase activity ofplatelets. In conjunction with phospholipids, which maybe exposed as a result of endothelial cell and plateletdamage, B2-GPI acts as a target for antiphospholipidantibodies resulting in interference with the clottingcascade in a positive way and leading to a hypercoagul-able state.19 Coagulation may occur in both small andlarge vessels, with the most frequent complication,venous occlusion, occurring in the deep vessels of thelower limbs, as in patient 1. Arterial occlusions oftenresult in transient ischaemic attacks and strokes, butocclusion of the smaller dermal vessels may result in theclinical picture of livedoid vasculitis. The antiphospho-lipid syndrome itself comprises recurrent thromboses(either arterial or venous), repeated fetal loss, thrombo-cytopenia and a persistently raised IgG anticardiolipinantibody titre or lupus anticoagulant. A raised IgMantibody titre may also occur. IgG antibodies may bemore strongly associated with complications than IgMantibodies, but this is unclear, and there does not appearto be an association with the level of antibody titre andrisk of complications.20 Livedoid vasculitis may occurin conjunction with this syndrome or as a separateentity.
Other authors have described livedoid vasculitis as anautoimmune phenomenon supported by the presence ofimmunoreactants in the vessel walls. Shroeter et al.21
found IgM deposition in all 13 patients tested and fibrinin 11 of 12, but many of their patients had underlying
systemic and immunological diseases; in another studyin which systemic diseases were excluded, immuno-fluorescence in the patient population was negative.5
Two of our patients demonstrated immunoreactantsin the vessels. There is no consensus regarding thetreatment of livedoid vasculitis. Various antithromboticagents have been used, including tissue plasminogenactivator,7 prostacyclin,11 sodium beraprost,8 ketan-serin22 and antiplatelet therapy.12 Corticosteroids havealso been used successfully, and more recently there hasbeen success with danazol, which has fibrinolytic activ-ity.23,24 Dapsone was used in our second patient as it issuccessful in the treatment of idiopathic vasculitis.Guanethidine and nicotinamide were also used as theformer is thought to act as a vasodilator and the latterhas anecdotally been reported to be successful. How-ever, if livedoid vasculitis occurs in conjunction withantiphospholipid antibodies, treatment may need to bemore actively pursued in order to prevent furtherthromboses. However, there is no current study toindicate that prophylactic treatment is useful in patientswith the syndrome who have not had a history ofthromboses. If thromboses have occurred, warfarin isthe treatment of choice, although again there is a lack ofconsensus and both low-dose heparin and the combina-tion of low-dose warfarin and aspirin have been used.Steroids and immunosuppressive drugs have not beenshown to have long-term benefit.25
It would seem that livedoid vasculitis may represent aclinical manifestation of a heterogeneous group of dis-eases that cause an occlusive vasculopathy or that itmay occur as a sole entity. However, whenever it isencountered the patient should be investigated foran underlying cause and treated actively ifantiphospholipid antibodies are present.
References1 Bard JW, Winkelmann RK. Livedo vasculitis: segmental hyalinising
vasculitis of the dermis. Arch Dermatol 1967; 96: 489–99.2 Papi M, Didona B, De Pita O et al. PURPLE (atrophie blanche):
clinical, histological and immunological study of twelve patients.J Eur Acad Dermatol Venereol 1997; 9: 129–33.
3 Gibson LE, Su WP. Cutaneous vasculitis. Rheum Dis Clin N Am1995; 21: 1097–113.
4 Milstone LM, Braverman IM, Lucky P, Fleckman P. Classification andtherapy of atrophie blanche. Arch Dermatol 1983; 119: 963–9.
5 McCalmont CS, McCalmont TH, Jorizzo JL et al. Livedo vasculitis:vasculitis or thrombotic vasculopathy? Clin Exp Dermatol 1992;17: 4–8.
6 Pizzo SV, Murray JC, Gomas SL. Atrophie blanche: a disorderassociated with defective release of t-PA. Arch Pathol Lab Med 1986;110: 517–19.
7 Klein KL, Pittelkow MR. Tissue plasminogen activator for the
134 K.M.ACLAND et al.
q 1999 British Association of Dermatologists, British Journal of Dermatology, 140, 131–135

treatment of livedoid vasculitis. Mayo Clin Proc 1992; 67: 923–33.
8 Tsutsui K, Shirasaki F, Takata M, Takehara K. Successful treat-ment of livedo vasculitis with beraprost sodium: a possiblemechanism of thrombomodulin upregulation. Dermatology1996; 192: 120–4.
9 Baccard M, Vignon-Pennamen MD, Janier M et al. Livedo vasculitiswith protein C system deficiency. Arch Dermatol 1992:128:1410–11.
10 Drunker CR, Duncan WC. Antiplatelet therapy in atrophieblanche and livedo vasculitis. J Am Acad Dermatol 1982; 7:359–63.
11 Hoogenberg K, Tupker RA, Van Essen LH et al. Successful treat-ment of ulcerating livedo reticularis with infusions of prostacyclin.Br J Dermatol 1992; 127: 64–6.
12 Yamamoto M, Danno K, Shio H, Imamura S. Antithrombotictreatment in livedo vasculitis. J Am Acad Dermatol 1988; 18:57–62.
13 Murrell DF, Jensen J, Hill C, O’Keefe EJ. Failure of livedoid vasculitisto respond to tissue plasminogen activator. Arch Dermatol 1995;131: 231–2.
14 Grattan CEH, Burton JL, Boon AP. Sneddon’s syndrome (livedoreticularis and cerebral thrombosis) with livedo vasculitis andanticardiolipin antibodies. Br J Dermatol 1989; 120: 441–7.
15 Grob JJ, Bonerandi JJ. Thrombotic skin disease as a marker of
the anticardiolipin syndrome. J Am Acad Dermatol 1989; 20:1063–9.
16 Ascherson RA, Mayou SC, Merry P et al. The spectrum of livedoreticularis and anticardiolipin antibodies. Br J Dermatol 1989;120: 215–21.
17 Asherson RA, Cervera R. Antiphospholipid syndrome. J InvestDermatol 1993; 100(2): 1–27s.
18 Nahass GT. Antiphospholipid antibodies and the antiphospholipidantibody syndrome. J Am Acad Dermatol 1997; 36: 149–68.
19 Gibson GE, Daniel Su WP, Pittelkow MR. Antiphospholipid anti-bodies and the skin. J Am Acad Dermatol 1997; 36: 970–82.
20 Muir K. Anticardiolipin antibodies and cardiovascular disease. J RSoc Med 1995; 88: 433–6.
21 Schroeter AL, Diaz-Perez JL, Winkelmann RK, Jordon RE. Livedovasculitis (the vasculitis of atrophie blanche). Arch Dermatol 1975;111: 188–93.
22 Rustin MHA, Bunker CB, Dowd PM. Chronic leg ulceration withlivedoid vasculitis, and response to ketanserin. Br J Dermatol 1989;120: 101–5.
23 Hsiao GH, Chiu HC. Low dose danazol in the treatment of livedoidvasculitis. Dermatology 1997; 194: 251–5.
24 Hsiao GH, Chiu HC. Livedoid vasculitis. Response to low dosedanazol. Arch Dermatol 1996; 132: 749–51.
25 Hughes GRV, Khamashta M. The antiphospholipid syndrome. J RColl Phys 1994; 28: 301–4.
LIVEDOID VASCULITIS 135
q 1999 British Association of Dermatologists, British Journal of Dermatology, 140, 131–135