Embed Size (px)
Citation preview

Journal of Infection (I984) 9, I6I - I66
Loa loa : t h e u s e o f a b l o o d c e l l s e p a r a t o r to r e d u c e m i c r o f i l a r a e m i a b e f o r e s p e c i f i c c h e m o t h e r a p y
A. A. Saeed,* P. J. Green,T M. Naoroz , t H. A. Lee~ and G. Venkat R a m a n ~
Departments of * Virology, Public Health Laboratory, tHaematology and ~Renal Medicine, St Mary's General Hospital, Milton Road,
Portsmouth P03 6AQ
Accepted for publication IO January I984
Summary
Three years after returning to the U.K. a 58-year-old British engineer, who had worked in the Nigerian oilfields for 24 years, was found to have Loa loa. His midday microfilarial count ranged between I2 x io 6 and I6 × IO 6 parasites per litre. Before starting treatment, I litre of leucocyte/platelet-rich plasma was removed by means of a blood cell separator.
Six intermittent cycles of blood separation were performed during a single 4-h session around midday in order to coincide with the period of maximum microfilarial presence in the peripheral circulation. This resulted in a 5o % reduction of the microfilaraemia.
Where facilities for blood cell separation are available, this procedure, together with appropriate chemotherapy, should be particularly beneficial in the management of heavy filarial infections.
Introduction
Chemotherapy for the treatment of Loa loa is not without complications. The widely used drug diethylcarbamazine (DEC) results in rapid immobilisation of the microfilariae, which are then trapped and destroyed in the liver. 1 During treatment, patients often experience malaise, fever, pruritus, joint swellings and pain. ~ A more serious problem is the risk of central nervous system involvement in heavy infections, presumably due either to released neurotoxins from the disintegrating parasites ~ or a hypersensitivity reaction similar to that of post-vaccinial or post-infectious encephalomyelitis. ~ In a review of the literature, Stanley and Kelp found five patients who developed various neurological manifestations with considerable morbidity, and also reported their own experience with one case of ascending myelitis following treatment with DEC.
Whether or not microfilariae are involved in either the aetiology or patho- genesis of the side-effects following drug therapy, their removal would be desirable to reduce the risk of developing these reactions. Andrd and colleagues ~ advocated exchange blood transfusion to reduce microfilaraemia in excess of 5o × Io 6 parasites per litre. An alternative approach is reported in which a blood cell separator may be used for this purpose.
oi63-4453/84/o5oi6I + 06 $02.00/0 © I984 The British Society for the Study of Infection

I 6 2 A.A. SAEED E T A L .
P a t i e n t a n d m e t h o d s
In March I983 a 58-year-old British engineer repor ted to his family doctor with intermit tent claudication and pain along the muscles of the thighs particularly on exertion. On a routine b lood examination, numerous microfilariae were seen in a stained film. These were subsequent ly identified as Loa loa microfilariae by demonstra t ion of the sheath by means of the special Mayer ' s haemalum stain, and by the characteristic terminal nucleus that reaches to the tip of the tail. The patient had spent 24 years working in the oil fields of Nigeria, an area endemic for Loa loa, and had re turned to Britain three years earlier.
H e was admit ted to hospital for further parasitological investigation and for careful assessment of his symptoms. H e had no history of calabar swellings, skin rash, fever or eye problems. H e had two attacks of malaria during his stay in Nigeria and was treated as an outpatient. H e was a heavy smoker. Physical examination revealed no significant abnormalit ies apart f rom poor peripheral pulses in the legs. Calabar swellings were not found. Blood indices on admission were normal (Table I) and malaria parasites were not seen. Liver funct ion tests were normal except for a slight rise in alkaline phosphatase (96 IU/1). A test for H B s A g was negative. Stools were free of ova, cysts and parasites. X-rays of the pelvis showed calcification of the iliac and femoral arteries compatible with the recent symptoms of claudication.
Microfilarial counts done at midday fluctuated be tween I2 x io 8 and I6 x io 6 parasites per litre while a midnight count showed only 8 x Io 5 parasites per litre. This diurnal periodicity is typical of Loa loa. N o other filarial species were seen on repeated examination of b lood films. These counts were done on conventional thick blood films prepared from Io gl b lood and stained with IO % Giemsa stain as descr ibed by Na than and colleagues 6 in order to minimise the loss of microfilariae from smears during the processing of the slides. At least ioo gl were counted for each blood specimen.
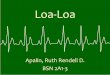
Before apheresis, the sedimentat ion characteristics of the microfilariae were assessed by centrifugation in a Win t robe tube (3ooo rpm for 30 minutes). T he parasites in the centr i fuged specimen of b lood (o'5 ml) were then counted alive in each of ten fractions prepared by pipet t ing 5o gl volumes sequentially starting from the top of the plasma layer. Each count was done on Io ktl specimens under low magnification. In this small volume spread under a cover slip (size 2o m m x 2o mm) the motili ty of the microfilariae was effectively reduced and thereby enabled an accurate count to be made. Appropr ia te dilutions of the dense cellular fractions were made in order to make it easier to see and count the parasites. As shown in Fig. I, most microfilariae ( 7 7 0 ) were found in the buffy coat layer, followed by 2I % and 2 % respectively in the upper two fractions of the packed red blood cells. T h e lower fractions and the plasma were free of parasites.
On the basis of these findings it was decided to use the b lood cell separator to remove the buffy coat as well as a port ion of the adjacent fraction of red blood cells and to transfuse back to the patient the remaining red b lood cells and the plasma. By means of a Haemonet ic 3o-S Blood Processor (Massachuset ts , U.S.A.) , the patient received six cycles of discontinuous flow centrifugation yielding about 15o ml buffy coat concentrate per cycle. Wi th a collecting bowl

Loa loa : reduction of microfilaraemia ~63
~ J
e l
-.I--
0
tq ~
o ~o ~ ~o ~ ~
e~
x ~ - ~ - a ~ . ~ - ~
=o X (,.~'~
oo
%
X , ~ . , ~
x , , ~ , 5 , ,~ - .
't,I
%
x ~ , ~ ' ~ , . o
~o~
" ~ x ' - " ~
_ ~ ~ "-d .~
"~ o.u Oo g
d
z~

164 A. A. S A E E D E T A L .
Microfilorioe per 10/21
Wintrobe tube Blood cell separator
Plasma 2 (0"5%)
880 (77°/°) v . v : . . . • . v . . . . . . . . . . . . . . . . . . . .
iiiiiiiiiiil 260 (21%) . . . : : . . . . . . . . . . . . . . . . . . . . . . - : . . . . .
iiiiii::ii!ii 30 c 2 O/o~ iliiiiiii!i! ~'""""'i 0
q i 0
Removed buffy coot and red blood cells 578 (75.7%)
Red blood cells 80 (26%)
Fig. I. Dis t r ibut ion of microfilariae after centrifugation of blood in a Wint robe tube (o'5 ml centrifuged at 3ooo rpm for 3o minutes) and in the blood cell separator (55o ml centr ifuged at 48oo rpm for 30 minutes) .
of 55o ml capacity, about two-thi rds of the patient 's total b lood volume was processed. The 4-h procedure was per formed around midday in order to coincide with the per iod of max imum numbers ofmicrofilariae in the peripheral circulation.
A direct count per formed at the end of the first cycle demonst ra ted a number closely similar to that in the Win t robe tube (Fig. I). T he buffy coat (I5O ml) contained 73'7 % of the parasites as compared with 26 % in the red blood cell fraction (25o ml) and o'3 % in the plasma (I5O ml). T h e small n u m b e r of parasites found in the plasma resulted from insufficient centrifugation of the last por t ion of b lood reaching the machine towards the end of the cycle. One litre of bul ly coat concentrate was eventually removed by apheresis. It contained 36 × IO 6 microfilariae, approximately 5o % of the concentrat ion of circulating parasites. The blood count d ropped from I4 × IO 6 parasites per litre to 7"6 x IO 6 parasites per litre at the end of the procedure . T h e next day there was no evidence of resurgence ofmicrofilariae, the midday count being 8-2 × io 6 parasites per litre. T rea tmen t with D E C was started immediately with a dose of 5o mg which was gradually increased t o a max imum of zoo mg t. d. s. by the end of the week. This dose was maintained for a fur ther 3 weeks. T he microfilaraemia d ropped precipi tously after chemotherapy (Table I). Within seven days the count was only I4 × IO 4 parasites per litre. Microfilariae could not be detected at the end of the t reatment or 2 months later.
The only significant change in blood indices was a reduct ion in platelets from 2~7 x lO9/1 to I38 × IO9/1 at the end of apheresis, bu t the n u m b e r re turned to normal shortly afterwards (Table I). A modera te eosinophilia of i2 % was detected after the end of t reatment with D E C and was presumably a reaction to proteins l iberated from the killed parasites. This rise was temporary as the eosinophil count was found to be normal a few weeks later (Table I).

Loa loa : reduction of microfilaraemia 165
Discuss ion
It has been shown that large numbers of microfilariae can be removed from the peripheral circulation by means of a blood cell separator. The procedure was well tolerated by the patient and 36 million microfilariae representing approximately half the load of circulating parasites were removed during a single session. It should be emphasised that removal of all parasites was not attemped as those not circulating cannot be removed by this procedure. Recently, Muylle and colleagues v independently reported the use of the same technique in two patients in whom initial adverse reactions to DEC were not encountered after apheresis ofmicrofilariae. They also demonstrated that it was possible to repeat the procedure on three consecutive days. As in the present study, however, the decrease in platelets limited any further apheresis. Initially it had been hoped t o pass the patient's blood through a 4o ~tm blood filter ( 'Ult ipor ' , Pall Biomedical Products, Glen Cove, N.Y.) and to remove the microfilariae by means of a simple extracorporeal circuit. In vitro studies, however, revealed that the filter would not, in fact, entrap the microfilariae. Apheresis was therefore explored. A similar filter has been used successfully to remove a large proportion of Loa loa microfilariae from banked blood. 8 Filtration on days I and 21 during storage of the blood reduced the concen- tration of parasites by 80 % and 92 % respectively.
Apart from surgical removal of adult filarial worms, being required when they are accessible, DEC remains the chemotherapeutic agent of choice in the treatment of loiasis. Nevertheless it should be remembered that the destruction of large numbers of parasites may cause severe reactions especially i~ heavily infected patients. In order to avoid this problem, Stanley and Kelp suggested that the asymptomatic patient need not be treated, but as with this patient, it is arguable whether such a view is acceptable in the case of imported loiasis. The tendency therefore is to treat rather than wait for symptoms of the disease to develop. The significant reduction of parasites by means of apheresis was encouraging and in the absence of any side-effects to treatment with DEC the authors felt sufficiently confident to discharge the patient from hospital one week later and for him to continue treatment at home.
The diurnal periodicity of the microfilariae in Loa loa enabled us to perform the procedure during the day. This caused minimum inconvenience to the patient, while at the same time it ensured maximum extraction of the parasites. Such advantages would be lacking in the case of the strictly nocturnal Wuchereria bancrofti and, to a lesser extent, in that of Brugia malayi which has nocturnal and semi-periodic types.
Although the procedure is relatively simple, its application in endemic areas may be limited by expense and lack of facilities. On the other hand, imported cases similar to the one discussed here may be occasionally encountered in the more developed countries. It is these patients who should benefit from the widely available blood cell separators located in blood transfusion centres and in hospital departments. In the U.K., 451 cases of filarial infections were notified to the Public Health Laboratory Service Communicable Disease Surveillance Centre between 1975 and 1982; 41 of these were confirmed as Loa loa. It is likely that importation of the disease will continue.

166 A . A . SAEED E T A L .
I n conc lus ion it is be l ieved that this t e c h n i q u e has a useful place in the m a n a g e m e n t o f loiasis. C o m b i n e d wi th c h e m o t h e r a p y it shou ld resul t in g rea te r benef i t t han t r e a t m e n t wi th D E C alone.
(We thank Dr D. Denham for his advice and for reviewing the manuscript, our laboratory staff for valuable technical assistance and Miss S. Hayter for secretarial help.)
R e f e r e n c e s
I. WoodruffAW. Destruction of microfilariae ofLoa loa in liver in loiasis treated with banocide (hetrazan). Tram R Soe Trop Med Hyg 1951 ; 44: 479-480.
2. Manson Bahr PEC, Apted FIC, eds Manson's Tropical Diseases. London: Bailli~re Tindall, 1982; I6I-I64.
3. Brumpt LC, P~quignot H, Lhermitte F, Petithory J, Remy H. Loase avec microfilar~mie 61ev6e, enc6phalite th6rapeutique, traitement par exsanguino-transfusion. BullM~m Soc M~d H3pit Paris 1966; II7: IO49-IO58.
4. Stanley SL, Kell O. Ascending paralysis associated with diethylcarbamazine treatment of M. loa loa infection. Trop Doct 1982; I2: 16-19.
5. Andr6 R, Brumpt LC, Obriot J, Petithory J. Loase avec microfilar~mie exceptionnellement ~lev6e. Int~r~t th~rapeutique de l'exsanguino-transfusion. Bull M~m Soc M~d H3pit Paris 1966; I I7: IO59-IO6I.
6. Nathan MB, Lambourne A, Monteil S. Evaluation of a membrane (Nuclepore) filtration method using capillary blood for the detection of microfilariae. Ann Trop Med Parasitol 1982; 76: 339-345.
7. Muylle L, Taelman H, Moldenhauer R, Van Brabant R, Peetermans ME. Usefulness of apheresis to extract microfilarias in the management of loiasis. Br MedJ 1983; ii: 519-52o.
8. AuBuchon JP, Dzik WH. Survival of Loa loa in banked blood. Lancet 1983; i: 648.