Embed Size (px)
Citation preview

966
LOCKED UNITS AND LOCKED WARDS
SIR,-20 years in mental hospital work failed to convinceme that locked wards or locked single rooms are anything morethan a confession of clinical or administrative incompetence.Locked wards are derisory: it was a patient who held the keyof our own locked ward for some years. Locked single roomsare more dangerous. At best, we locked patients in thembecause we were frightened of them or angry with them. (Re-grettably, there were other less worthy reasons occasionally.)When a patient is so disturbed that locking him in becomes apossibility, he needs the presence of another person who canwithstand his disturbance until he settles. Isolation is dehu-
manising and inhuman-at least for patients. But (with hind-sight) I suggest that spending 24 h isolated in a locked roomin a mental hospital should be an essential element in the
training of mental-hospital nurses and doctors-and planners.I did not experience it myself: maybe I would have been betterat "’HI inh if T
Radnor House,Church Street, Hay on Wye,via Hereford HR3 5DQ JAMES MATHERS
INTRA-ERYTHROCYTE LITHIUM IONCONCENTRATION AND LONG-TERM
MAINTENANCE TREATMENT
SIR--The increasing use of lithium carbonate for both theshort-term treatment of acute psychiatric disturbance and thelong-term prophylaxis of recurrent affective disorders has beenaccompanied by efforts to characterise those patients who areresponsive to this cation. These efforts have included themeasurement of erythrocyte (R.B.c.) lithium ion (Li+) concen-tration’ in addition to the standard measurement of plasma-lithium. This procedure has been developed for several rea-sons-e.g., there seem to be qualitative similarities betweencation transport in R.B.C.s and in neurons, suggesting that theR.B.C.S may provide a useful model for studies of neuronal elec-trolyte distribution and transport. 2We found that depressed patients who respond to lithium
had significantly higher R.B.c. Li+ concentrations and
R.B.c./plasma Li+ ratios (lithium ratios) than did patients whodid not respond.’ The lithium ratio is u.ider genetic in-
fluence,34 and we have suggested that there may be a groupof patients with affective disorders who are lithium responsiveand whose illness is associated with a genetically determinedabnormality in cation transport across the cell membrane.2We have studied the relation between the prophylactic effect
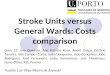
of lithium and the lithium ratio in 31 patients with recurrentaffective disorders. These patients entered the lithium clinicafter January, 1970, were available for study during 1975, andhad received lithium for at least 12 months. The patients(males and females) were aged 21-67 and had in common ahistory of recurrent depression and/or mania extending overmany years and were deemed suitable for a course of Li+ main-tenance therapy. The results are summarised in the table,which shows the mean plasma and R.B.c. Li+ concentrationsand lithium ratio for the "responders" and "non-responders".Responders were those who, after a period of appropriatetreatment and stabilisation, were given lithium. They took thedrug for at least twelve months with no interference in life-
style and did not require any futher antidepressant or anti-manic medications. The non-responders had continuing sig-nificant disruptions of their life-style, were often unable to
continue work, and needed hospital admission and additional
1. Mendels, J., Frazer, A. J. psychiat. Res. 1973, 10, 92. Mendels, J., Frazer, A. Am. J. Psychiat. 1974, 131, 11.3. Dorus, E., Pandey, G. N., Frazer, A., Mendels, J. Archs Gen. Psychiat.
1974, 31, 463.4. Dorus, E., Pandey, G. N., Davis, J. M. ibid. 1975, 32, 1097.
ERYTHROCYTE LITHIUM-ION CONCENTRATION AND RESPONSE TO
LONG-TERM MAINTENANCE TREATMENT
Values as mean+S.E.M.*SlgOlficantly different from "responders" value (p<0.025; two-taded Student’s
t test).tSigmficantly different from "responders" value (P<0.001; Mann-Whitney Utest).
antidepressant and/or antimanic medication. Patients whowere judged equivocal in terms of this differentiation wereexcluded from the tabulation without any knowledge as to
their lithium ratios. We also excluded patients whose meanplasma-lithium was less than 05 mmol/1.The responders had significantly higher lithium ratios
(066±003) than the non-responders (0.44±0.03) despite thefact that the non-responders had a higher mean plasma-lith-ium concentration, presumably the result of efforts to bringabout clinical improvement by further increases in dosage.
These findings provide additional support for the suggestionthat there is a group of patients who are responsive to treat-ment with the lithium ion and who are characterised by acapacity to develop a higher R.B.c. Li+ concentration duringtreatment. If it can be confirmed that prophylactic benefitfrom lithium is not simply a matter of increased dose or plasmaconcentration, but is correlated with the R.B.c. Li+, it wouldbe important to determine if this can be detected early in treat-ment. If so, it may serve as a guide to clinicians with the man-agement of individual patients.Veterans Administration Hospital andUniversity of Pennsylvania,Philadelphia,Pennsylvania 19104, U.S.A.
Centro di Psychiatria,Rome, Italy
J. MENDELSA. FRAZER
J. BARONA. KUKOPUL0SD. REGINALDIL. TONDOB. CALIARI
BACLOFEN IN SCHIZOPHRENIA
SIR Frederiksen’ reported on the efficacy of baclofen(’Lioresal’) for the treatment of schizophrenia. He claimeddramatic results in 13 patients, the effects often being notice-able within a few days. Baclofen is a Y-aminobutyric acid deri-vative which passes through the blood/brain barrier. Confir-mation of these results would be of considerable interestbecause it would implicate another neurotransmitter in the
pathogenesis of this disorder.We have completed a study of this compound and we are less
than enthusiastic with the results. We studied 12 chronic
schizophrenic patients (7 male, 5 female), mean age 43 (range27-50), mean length of hospital admission 16 years (range2-25). All patients were physically healthy, all were treatmentresistant (i.e., schizophrenic patients who required neurolepticsbut who did not respond sufficiently well to be placed in thecommunity). Such patients do show a positive if mild benefi-cial effect on active antipsychotic medication. After a four-week drug-free period they received baclofen the dose of.whichby the end of five weeks had reached 80 mg in 5 and 120 mgin 7 of the 12 patients. By the sixth week all patients reached120 mg which has been set as the maximum dose on the basisof animal toxicity studies. Compared with their drug-free base-
1. Frederiksen, P. K. Lancet, 1975, i, 702.