Embed Size (px)
Citation preview
British Journal of Haematology, 1990, 76, 560-563
Correspondence
LONG-TERM SURVIVAL IN ACUTE LEUKAEMIA IN ADULTS
Brincker & Christensen (1990) conclude, on the basis of the study of long-term survival in 403 patients with acute leukaemia, that no significant improvement in the treatment of acute myeloblastic leukaemia (AML) has occurred over the last two decades.
We also tried to determine the true incidence of long-term survival (> 36 months) and the impact of chemotherapy on complete remission (CR) rate and median survival of the entire population of patients with AML. The analysis of all the patients with AML diagnosed during 1972-81 (group A, M/F= 1601128, median age= 57.5158.0 years) and during 1982-87 (group B, M/F= 102/87, median age=58/58 years) was done regardless of age and whether or not any therapy was administered or remission achieved. (JankoviC et al, 1989, 1990). The patients in groups A and B were treated with a variety of 'conventional' (low-dose) and 'intensive' induction protocols, respectively.
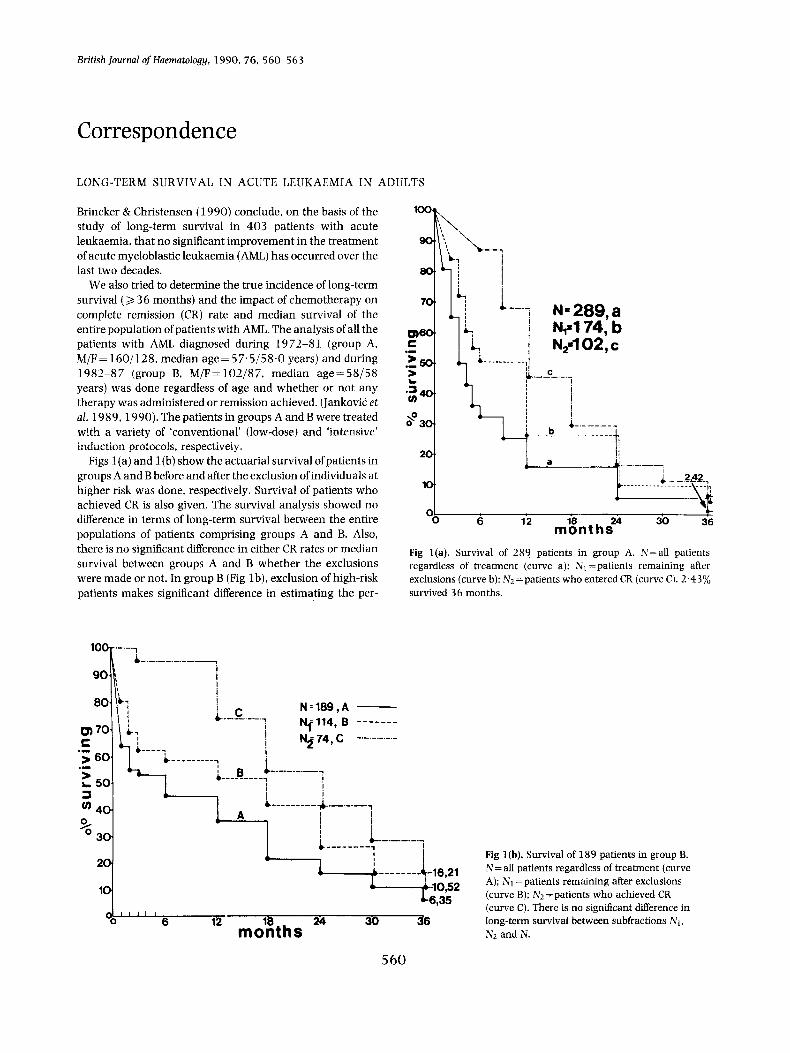
Figs l (a ) and l(b) show the actuarial survival of patients in groups A and B before and after the exclusion of individuals at higher risk was done, respectively. Survival of patients who achieved CR is also given. The survival analysis showed no difference in terms of long-term survival between the entire populations of patients comprising groups A and B. Also, there is no significant difference in either CR rates or median survival between groups A and B whether the exclusions were made or not. In group B (Fig lb), exclusion of high-risk patients makes significant difference in estimating the per-
6 12 24 30 36 mbsnths Fig l(a). Survival of 289 patients in group A. N=all patients regardless of treatment (curve a); N1 =patients remaining after exclusions (curve b): Nl =patients who entered CR (curve C1. 2.43% survived 36 months.
Fig l(b). Survival of 189 patients in group B. N=all patients regardless of treatment (curve A): N1 =patients remaining after exclusions (curve B): Nl =patients who achieved CR (curve C). There is no significant difference in long-term survival between subfractions N1, N2 and N.
560

Correspondence 5 6 1 Table I. Effect of exclusions in AML patients (groups A and B) on CR and median survival
Analysis of patients still included
No. CR. No. (%) Med. survival (months)
A B Exclusion criteria A B A B
No exclusions 289 189 102 (35.29) 74(39.12) 3 3 A. Untreated (n=35), (n=27) 254 162 102 (40.15) 74(45.67) 4 4.5 A, B. Partially treated (n=26). (n=21) 228 141 102 (44.73) 74(52.48) 4.5 5.5 A, B, C. Aged 70 or over, fully treated (n=37). (n=11) 191 130 96(50.26) 2 (55.38) 6 7.0
A, B. C. D. E. Previous disease fully treated ( n = 5), (n= 7) 174 114 90 (5 1.72) 70 (61.40) 7 13 A.B.C.D.Preleukaemicphase,fullytreated(n=12), ( n = 9 ) 179 121 91 (50.83) 71 (58.67) 7 10
No exclusions= the entire population of patients; A=patients untreated for any reason; B=patients who received treatment but did not complete one full course: C=patients aged 70 or over who received full treatment: D=patients with preleukaemic phase who received full treatment: E = patients with previous chemotherapy or coincident malignant disease who received full treatment.
centage of long-term survivors (6.35 v. 16.21%, P < 0 . 0 5 ) which is not the case in group A (Fig l a ) patients (2.42 v. 7.54%. P> 0.05). Overall, standard induction treatment appears not to be significantly inferior to the substantially intensified induction regimens.
Table I shows the effect of specific steps in patient exclusion from the study according to the Toronto Leukemia Study Group’s criteria (Toronto Leukemia Study Group, 1986) on both CR rates and median survival. There is no significant difference in any respect between groups A and B.
We agree with Brincker & Christensen (1990) and Gale & Lee (1 990) that improvements in chemotherapy may reflect inadvertently biased statistical processing of data or refine- ments of exclusion criteria rather than the genuine thera- peutic progress over time.
Institute of Haematology, Utiivevsity Cfinicd Center, I 7 .OOO Belgrade, ul. Dr Koste TodoroviCa br.2, Yugoslavia
M. D. Co~ovri. G. M. JANKOVIC M. D. PETKOVI~
REFERENCES
Brincker, H. & Christensen. B.E. (1990) Long-term survival and late relapses in acute leukaemia in adults. British Journal of Haemato-
Gale, R.P. & Lee, M.L. (1990) Do different therapies of AML produce different outcomes? Leukemia Research, 14, 207-208.
JankoviC. G.M., RistiC, M.S., PetroviC, M.D., colovik, M.D., RistiC, S.M., JanEiC, M.S., TomaSeviC. R., Bogdanovic. G., RadovaEevik. R., et a1 (1 990) Effect of exclusions according to the Toronto Leukemia Study Group’s criteria on the therapy success in patients with acute myeloblastic leukaemia. Serbian Archives (in press). [In Serbo-Croat.]
JankoviC. G.M., RistiE. M.S.. ColoviC, M.D., PetroviC. M.D.. RistiC. S.M., JanEid, M.S.. TomaSeviC, R., Bogdanovik, G. & RadovanEeviC, R. (1989) Effect of exclusions of the patients at higher risk on the results of the treatment of patients with acute myeloblastic leukaemia. Bilten for Haernatology and Transfusiology, 14, 13 3- 138. [In Serbo-Croat.]
Toronto Leukemia Study Group (1986) Results of chemotherapy for unselected patients with acute myeloblastic leukaemia: effect of exclusions and interpretation of results. Lancet. i, 786-788.
logy. 74, 156-160.
SYNGENEIC BONE MARROW TRANSPLANTATION FOR APLASTIC ANAEMIA
We read with interest the report of Gibson & Gordon-Smith (1990) on long-term bone marrow culture (LTBMC) in aplastic anaemia. We report the findings of both short and LTBMC in one of triplets who underwent syngeneic bone marrow transplantation (BMT) for aplastic anaemia.
P.C., a 17-year-old boy, was diagnosed as having severe idiopathic aplastic anaemia. Peripheral blood counts were as follows: Hb 8.1 g/dl, WBC 1.3 x 109/1 (25% polys), platelets 10 x 1OY/1. retics 0.4%. Bone marrow aspirate and biopsy confirmed a diagnosis of aplasia. The patient had visited the U.S.S.R. 6 months prior to the onset of aplasia and had been admitted to hospital with jaundice 2 months prior to the onset of aplasia. Serology, including hepatitis C antibodies on
at least two occasions, was consistently negative in the patient, both parents and his siblings.
The patient received a syngeneic BMT on 11 December 1989 from one of his triplet brothers (2.6 x lo8 nucleated cells/kg body weight). He was conditioned with cyclophos- phamide 200 mg/kg and received no prophylaxis against graft-versus-host disease (GVHD). Blood counts showed partial recovery at day 14 and a subsequent pancytopenia ensued. Four weeks later the patient’s blood counts recovered and he was discharged from hospital 6 weeks following BMT. Since then, the patient has remained clinically well although he has a consistent mild thrombocytopenia and the white cell count has never gone beyond 3 . 5 x 109/l. He is currently