Embed Size (px)
DESCRIPTION
Vitamin D Levels
Citation preview

ORIGINAL ARTICLE
Low serum 25-hydroxyvitamin D levels and bronchiolitis severityin Spanish infants
Gloria Moreno-Solís & Fernando Fernández-Gutiérrez & Javier Torres - Borrego &
Ricardo Torcello-Gáspar & José Luis Gómez-Chaparro Moreno & Juan Luis Pérez - Navero
Received: 24 March 2014 /Revised: 12 August 2014 /Accepted: 19 August 2014# Springer-Verlag Berlin Heidelberg 2014
Abstract This cross-sectional study was performed to exam-ine the prevalence of hypovitaminosis D in infants with acutebronchiolitis compared with control subjects and to evaluatethe relationship between serum 25-hydroxyvitamin D (25(OH)D) and the severity of bronchiolitis. Serum 25(OH) D levelswere measured by radioimmunoassay in 48 infants with acutebronchiolitis (2.5±2.0 months) and in 30 healthy infants (3.2±2.3 months). 25(OH) D levels (ng/ml) in children with acutebronchiolitis were significantly lower than in the control group(median 29.9 ng/ml (interquartile range (IQR) 21.4–37.5) ver-sus median 38.2 ng/ml ((IQR 26.1–48.1), p=0.022), mainly ininfants withmoderate–severe bronchiolitis (median 29.8 ng/ml,IQR 19.2–35.9). The prevalence of hypovitaminosis D wasremarkably greater among infants with bronchiolitis than incontrol subjects (52.1 versus 26.6 %). A significant inverse
correlation was found between serum 25-hydroxyvitamin Dlevels and disease severity (rho=−0.457, p<0.001).
Conclusion: The prevalence of hypovitaminosis D is high inSpanish infants with bronchiolitis. The severity of acute bron-chiolitis increases with a decline in serum 25 (OH) D level.
Keywords RSV . Acute bronchiolitis . VitaminD . 25(OH)D . Severity . Immunity
AbbreviationsAAP American Academy of PediatricsAB Acute bronchiolitisALRTI Acute lower respiratory tract infectionCV Coefficient of variationESPGHAN European Society of Paediatric
Gastroenterology, Hepatology and NutritionIQR Interquartile rangeM±SD Mean±standard deviationp p valueRIA RadioimmunoassayRSV Respiratory syncytial virusSPF Sun protection factorIOM The Institute of MedicineUK United KingdomUSA United States of AmericaVDR Vitamin D receptorVDBP Vitamin D binding protein25(OH) D 25-hydroxyvitamin D
Introduction
Acute bronchiolitis (AB) is the most common acute lowerrespiratory tract infection (ALRTI) during infancy and is asignificant cause for hospitalization in the first 12 months of
Communicated by David Nadal
Conversion factors (international units = conventional units) 25-hydroxyvitamin D nanomole/litre=nanogram/milliliter×2.496
G. Moreno-Solís (*) : F. Fernández-Gutiérrez :J. Torres - Borrego :R. Torcello-Gáspar :J. L. Gómez-Chaparro Moreno : J. L. Pérez - NaveroReina Sofía Children’s Hospital, Avda Menéndez Pidal S/N,14004 Córdoba, Spaine-mail: [email protected]
F. Fernández-Gutiérreze-mail: [email protected]
J. Torres - Borregoe-mail: [email protected]
R. Torcello-Gáspare-mail: [email protected]
J. L. Gómez-Chaparro Morenoe-mail: [email protected]
J. L. Pérez - Naveroe-mail: [email protected]
Eur J PediatrDOI 10.1007/s00431-014-2405-4

life [45]. AB is linked with preschool recurrent wheezing inearly childhood and childhood asthma [27, 32]. AB is usuallydefined as the first viral episode of respiratory distress accom-panied by coryza, cough, crackles and wheezing. Clinicaldefinitions of acute viral bronchiolitis vary between countries.While in many countries, including the USA, wheezing isfundamental for the diagnosis, in the UK and some regionsof Europe, and Australia, wheezing is not an obligatory diag-nostic criterion [1, 49]. Bronchiolitis generally occurs in aseasonal pattern with the highest incidence in winter months,when the respiratory syncytial virus (RSV) accounts for themajority of the cases although other viruses have also beeninvolved [36].
The role of vitamin D in the regulation of calcium and bonemetabolism is well established. Recently, new physiologicalfunctions derived from epidemiological and genetic studies, aswell as research in animal models, suggest that vitamin Dplays an important and complex role in immune system func-tion and regulation and in host defences against respiratoryinfections [31, 48, 6, 11]. In this context, vitamin D insuffi-ciency has been linked with greater susceptibility to infec-tions, particularly respiratory ones [15]. There are only a fewstudies in children with conflicting results from differentcountries and latitudes that have determined the correlationbetween vitamin D status and bronchiolitis, although none ofthem focusing exclusively on infants during the first year oflife [24, 29, 34, 41, 42]. Furthermore, none of these studieswere performed in a sunny region of southern Europe
The aim of this cross-sectional study is to examine theprevalence of hypovitaminosis D among infants with ABcompared with control subjects and to find a correlationbetween the severity of bronchiolitis and serum 25-hydroxyvitamin D (25(OH) D) levels.
Material and methods
Participants and study design
Hospitalized infants aged 1–11 months admitted to the Paedi-atrics Department at our hospital (latitude 37, 53° N) with afirst episode of bronchiolitis were recruited from December1st 2009 to March 31st 2010. Inclusion criteria were thefollowing: a prodromal history consistent with viral upperrespiratory tract infection (cough, coryza, rhinorrhea), in-creased respiratory effort (tachypnoea, subcostal and intercos-tal retractions–use of accessory muscles) and/or abnormalauscultatory findings (wheezing or crackles). Patients wereexcluded from the study if they had one or more of thefollowing characteristics: premature birth (gestational age<37 weeks); low weight (≤P5) or overweight (≥P85) at birthand at the time of enrollment: history of chronic or congenitaldiseases of the lungs, heart or nervous system:
immunodeficiency or previous treatment with palivizumab.Infants with a history of chronic disorders or prescription ofanymedication that may alter vitamin Dmetabolismwere alsoexcluded.
Bronchiolitis severity was assessed at admission and dailyuntil discharge using a modified Wood Downes clinical bron-chiolitis severity score [12] and transcutaneous oxygen satu-ration. This 14 point scale includes the evaluation of thefollowing criteria: wheezing (0 to 3 points), presence of re-tractions (0 to 3 points), respiratory rate (breaths/minute) (0 to3 points), heart rate (beats/minute) (0 to 3 points), ventilation(0 to 3 points) and cyanosis. Moderate bronchiolitis wasdefined as a score from 4 to 7 and severe bronchiolitis as ascore equal or greater than 8 points.
The control population comprised healthy infants aged<12 months, admitted to the outpatient clinic at our hospitalbetween the same months without respiratory symptoms orany history of hospitalization for bronchiolitis or wheezing.These infants underwent an analytical study indicated forelective surgery. Exclusion criteria were the presence of oneor more of the following: prematurity, low weight or over-weight at birth and the time of enrollment and chronic disor-ders or prescription of any medication that may alter vitaminD metabolism.
Written informed consent was obtained from the parents orlegal guardian of all enrolled children. The study protocol wasapproved by the Ethics Committee before the beginning ofthis study.
At the time of enrollment, anthropometric measurementswere taken. Parents were asked to provide some demo-graphics information, as well as answering about the presenceof certain factors, such as atopic dermatitis, type of feedinghistory (breast milk feeding, formula milk feeding and mixedfeeding), sunlight exposure, sunscreen use and vitamin Dsupplementation [14, 44].
Breast milk feeding was defined as feeding breast milkmore than 80 % of total feeding volume per day. Parentsreported daily intake of milk, cereals and supplements beforeadmission.
With regard to vitamin D intake, the infant formula (begin-ning formula) provides 40–50 IU/100 ml, the infant formula(follow-up formula) 40–80 IU/ml and the breast milk (22–25 IU/l). Cereals provide 300 IU/100 g. VitaminD intake frombreast milk was omitted due to the low amount of vitamin Dand difficulties in evaluating the daily intake accurately. Asreported by caregivers and recommended by the paediatrician,vitamin D supplements were given at a dose of 400 IU/day,beginning a few days after birth, in accordance with theAmerican Academy of Pediatrics (AAP) and the EuropeanSociety of Paediatric Gastroenterology, Hepatology and Nu-trition (ESPGHAN) [7, 47]. Total vitamin D (IU/day) wascalculated from the amount of vitamin D in the diet andsupplements at the time of admission.
Eur J Pediatr

Spent time outdoors for sun exposure was considered if theinfants were exposed to sun at least 2 h a week fully clothedwithout hat and with face and hands uncovered.
Laboratory measurements
Viral diagnosis
In all infants with bronchiolitis, nasopharyngeal aspirate fluidsamples were tested for RSV by direct immunofluorescencetest.
Biochemical analysis: 25(OH) D determination
Blood samples were drawn at admission from antecubitalvein. Serum samples obtained were centrifuged, separated,aliquoted and stored at −80 ° until analyzed. 25(OH) D levelsweremeasured by radioimmunoassay (RIA) (IDS 125I 25(OH)D RIA Kits; Immunodiagnostic System IDS, Ltd., UK). Theinter-assay coefficient of variation (CV) for 25(OH) D variedbetween 5.3 and 6.1 % and the intra-assay CV for 25(OH) Dvaried between 8.2 and 7.3 % [25].
The 25(OH) D values were categorized as deficient<20 ng/ml (<50 nmol/l), insufficient 21–29 ng/ml (52.5–72.5 nmol/l) and sufficient ≥30 ng/ml (75 nmol/l) [7, 21–23,37]. Hypovitaminosis D (<30 ng/ml) included vitamin Ddeficiency and insufficiency.
Statistical analysis
Results were presented as mean±standard deviation (M±SD)or median (IQR, interquartile range) for quantitative variablesand for qualitative ones as absolute and relative frequencies.Comparison among groups was done by Chi-squared test inorder to identify differences in categorical variables, the Stu-dent’s t test for normally distributed numeric variables andKruskal-Wallis test andMann-WhitneyU test for skewed dataof serum 25(OH) D levels.
The Spearman’s rho correlation coefficient was used forassociations among variables. All analyses were performedusing the PASW Statistics 18 (Predictive Analytic Softwarefor Windows® SPSS Statistics®, Inc. Chicago, IL, USA).Significance was assumed at p<0.05 (two-tailed).
Results
Forty eight infants diagnosed of bronchiolitis (89.58 % RSVpositive) were recruited in the study. The control populationconsisted of 30 infants. All infants were White European andone infant with AB was born to a Romanian mother. Baselinecharacteristics of patients included are shown in Table 1.
There were no significant statistical differences according togender, type of feeding and vitamin D supplementation be-tween groups. The vitamin D intake of control subjects was188.7±250.8 IU/day compared to 196.2±236.2 IU/day in thebronchiolitis group (p=0.89). Eighteen (37.5 %) infants in thebronchiolitis group and 11 (36.7 %) in the control group weresupplemented with vitamin D doses that were equal to orhigher than 400 IU/day (p=0.94).
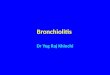
Time outdoors (sun exposure) was at least 2 h per week in21 (84 %) out of 25 infants in the control group and in 25(71.4 %) out of 35 infants in the bronchiolitis group. Accord-ing to the information provided by the family, the time out-doors could not be established accurately in 4 (13.3 %) infantsin the control group and in 13 (27 %) infants in the bronchi-olitis group. Sun exposure was not significantly differentbetween groups. Sunscreen with sun protection factor (SPF)was not applied to any infant. Serum 25(OH) D in control andbronchiolitis cases are shown in Fig. 1. It can be observed, thatserum 25(OH) D levels in the bronchiolitis group were sig-nificantly lower than in the control group of healthy infants(median 29.9 ng/ml (IQR 21.4–37.5) versus median38.2 ng/ml (IQR 26.1–48.1), p=0.022). These values werealso compared between bronchiolitis subgroups according todisease severity (Fig. 2). When comparison was restricted bydisease severity, serum 25(OH) D levels were decreased inmoderate–severe bronchiolitis group compared with controls(median 29.8 ng/ml (19.2–35.9) versus 38.2 ng/ml (26.1–48.1), p=0.026). However, there were no significant differ-ences between the moderate–severe (median 29.8 ng/ml(19.2–35.9)) and the mild bronchiolitis (30.6 ng/ml (23.0–42.6)) subgroups.
In the bronchiolitis group, 23 patients (47.9; 95 % CI=34.1–62%) had sufficient serum25(OH)D levels (≥30 ng/ml).Prevalence of vitamin D insufficiency and deficiency (25(OH)D levels between 21 and 29 ng/ml and <20 ng/ml, respective-ly) was remarkably high, 25 in 48 patients (52.1 %), increas-ing with the severity of the disease: 7 in 18 mild cases (38.9;95 % CI=17.3–64.3 %) and 18 in 30 moderate–severe cases(60; 95% CI=40.6–77.3%), as shown in Table 2. Only one ofthe infants in the moderate–severe bronchiolitis group had25(OH) D levels <10 ng/ml.
Considering the entire bronchiolitis group, there was asignificant inverse correlation between serum 25(OH) Dlevels and disease severity (rho=−0.457, p<0.001).
Discussion
In the present study, serum 25(OH) D levels in infants withbronchiolitis were significantly lower than in the controlgroup. Infants with moderate–severe bronchiolitis had thelowest serum 25(OH) D levels, but no significant differenceswere observed between infants with mild and moderate–
Eur J Pediatr

severe bronchiolitis, probably due to small size of the groups.Furthermore, the prevalence of hypovitaminosis D in infantswith bronchiolitis (52.1 %) was higher than that previouslyreported [34, 41]. Likewise, a significant inverse correlationbetween serum 25(OH) D levels and disease severity wasdemonstrated. These data suggest that vitamin D deficiencyand insufficiency may be linked to bronchiolitis severity.
To the best of our knowledge, a pattern of 25(OH) Ddecrease associated with the severity of bronchiolitis in infantswith acute bronchiolitis in the first year of life, excluding theneonatal period, has not been previously published.
Karatekin et al. [29] described subclinical vitamin D defi-ciency in 25 newborns with acute lower respiratory tractinfection (ALRTI). Roth et al. [42], in a study conducted withchildren in Bangladesh with an average age of 4.2 months(aged 1–18 months), found a significant association betweenlow vitamin D status and early ALRTI. However, a fewstudies have evaluated the relationship between vitamin Dstatus and disease severity. Inamo et al. [24], in a Japaneseretrospective study in 28 hospitalized children (aged 1–48months) with ALRTI, suggested that low serum 25(OH) Dconcentrations (<10 ng/ml) may be correlated with the sever-ity of ALRTI.
In contrast, two Canadian studies [34, 41], showed nosignificant differences in mean serum 25(OH) D levels be-tween the entire ALRTI group and controls. In one of thesestudies, Roth et al. [41] also found that vitamin D status wasnot associated with the risk of hospitalization for bronchiolitisin children, with an average age of 13.3 months (age rangedfrom 1 to 25 months). In the other study, in children less than5 years (average age 13.6 months), McNally et al. [34] sug-gested that vitamin D deficiency was not associated withmild–moderate ALRTI, but with severe cases that requiredadmission to the Paediatric Intensive Care Unit. Iqbal et al., inanother case control study in 38 patients (aged 6 monthsthrough 12 years) hospitalized for viral respiratory diseasesshowed that hypovitaminosis D (25(OH) D level <30 ng/ml)was common but it was not significantly associated with thepresence or severity of respiratory diseases [26].
Likewise, Belderbos et al. demonstrated that vitamin Ddeficiency in healthy neonates is associated with an increasedrisk of ALRTI in the first year of life [5]. In addition, Camargoet al. confirmed these findings in a birth cohort from NewZealand, in which low 25(OH) D levels in cord blood wereassociated with an increased risk of respiratory infections at3 months of age and recurrent wheezing in early childhood
Table 1 Baseline characteristicsfrom study participants
Data are expressed as median±IQR
Controls (n=30) Infants withbronchiolitis (n=48)
p value
Age (months) (mean±SD) 2.25 (1.5–5.0) 2.0 (1.0–3.0) 0.08
Sex: male, n (%) 15 (50 %) 27 (56.3 %) 0.61
Breastfeeding, n (%) 25 (83.3) 38 (79.2 %) 0.21
Atopic dermatitis, n (%) 4 (13.3 %) 6 (12.5 %) 0.46
Vitamin D supplementation, n (%) 10 (30 %) 13 (27.1 %) 0.37
Sun exposure (%) 21/25 (84 %) 25/35 (71.4 %) 0.30
25
(OH
) D
Fig. 1 Serum 25 (OH) D (ng/ml)from control infants and infantswith bronchiolitis. Box andwhisker plots represent: Lowerwhisker median (black bars), andupper whisker. Data are expressedas median and IQR. p valuebetween groups is shown
Eur J Pediatr

[10]. In another study, Shin et al. [43] reported that cord bloodvitamin D insufficiency or deficiency in healthy neonates wasnot associated with an increased risk of AB by 6 months ofage.
In the control group of healthy infants, serum 25(OH) Dlevels agreed with previous studies [2, 13, 16, 34, 41], espe-cially with those found in infants living in northern Spain witha different latitude of 43° N [13].
Factors associated with vitamin D status in children includeage, latitude, season of year, urban environment, dietary vita-min D intake, skin pigmentation, sun exposure, sunscreen useand nutrition [14, 38]. There were no differences betweenurban and rural areas regarding lifestyle characteristics suchas air pollution, green areas, walking areas and building andoutdoor activities associated with sun exposure.
However, as it is shown in our study, 70 % of infants in thecontrol group and 62.9 % in the bronchiolitis group did notreceive vitamin D supplementation. Thus, compliance withthe American Academy of Pediatrics recommendation to
provide 400 IU per day of vitamin D is very low. It isimportant for paediatricians and health care professionals toensure that this effective and preventive strategy is conductedin all healthy infants who are completely or partially breastfed,and in any infant who consumes <1,000 ml formula/day,during the first year of life.
Factors that may affect the cutaneous synthesis of vitaminD such as the degree of skin pigmentation, sunscreen orcoverage of the skin were similar in both groups. All infantsin both groups were light-skinned and sunscreen was notapplied during this time period. On the other hand, it shouldbe kept in mind that children younger than 6 months be keptout of direct sunlight to reduce the risks of skin cancer [4].Furthermore, the production of vitamin D in the skin afterexposure to sunlight in winter is negligible in areas located at alatitude greater than 40 °. In our study, these variables did notdiffer between the two groups and therefore these cannot beresponsible for the lower values of serum 25(OH) D levelsfound in the bronchiolitis group.
Control group Mild bronchiolitis Moderate-severe
bronchiolitis
p<0.05
ns
ns
38.2
(26.1-48)30.2
(23.0-42.6)29.8
(19.2-35.9)2
5(O
H)
D
Fig. 2 Serum 25(OH) D levels(ng/ml) control infants and infantswith bronchiolitis stratified bydisease severity. Box and whiskerplots represent: Lower whisker,median (black bars), and upperwhisker. Data are expressed asmedian and IQR. ns no significantp value among groups
Table 2 Proportion of study par-ticipants stratified according todeficient, insufficient and suffi-cient serum 25(OH) vitamin Dlevels
Hypovitaminosis D
Deficiency(<20 ng/ml)
Insufficiency(20–29 ng/ml)
Sufficiency(≥30 ng/ml)
Controls (n=30) 4 (13.33 %) 4 (13.33 %) 22 (73.33 %)
Cases (n=48) 9 (18.8 %) 16 (33.3 %) 23 (47.9 %)
Mild bronchiolitis (n=18) 1 (5.6 %) 6 (33.3 %) 11 (61.1 %)
Moderate–severe bronchiolitis (n=30) 8 (26.7 %) 10 (33.3 %) 12 (40 %)
Eur J Pediatr

An entirely new role of vitamin D action has been identi-fied since the discovery of vitamin D receptor (VDR) expres-sion in almost all immune cells (e.g., lymphocytes B and T,neutrophils, macrophages) and in other systems like on respi-ratory epithelial cells [3, 19].
It is exciting to speculate that the pathophysiology ofALRTI may be related to the role of vitamin D in the activityof the innate immune system. Non-classical response to vita-min D has been recognized as an important mediator of innateimmune response and antimicrobial activity [19, 20]. In fact, anumber of studies have established that vitamin D could play amajor role in innate immunity with antimicrobial productionof peptides such as cathelicidin and defensins [8, 20, 30].Cathelicidins help to prevent infections by bacteria and virus-es, including Mycobacterium tuberculosis and RSV [30]. Inchildren aged <2 years hospitalized with bronchiolitis lowlevels of hCAP-18 (cathelicidin antimicrobial peptide) wereassociated with RSV infections and an increased severity ofbronchiolitis [33]. Furthermore, adequate vitamin D levelswould contribute to diminish inflammation and the severityof disease in patients infected with RSV [17]. Recently, VDRgene polymorphisms have been described to help predictsusceptibility to RSV bronchiolitis [28, 35, 46]. Taken togeth-er, these data support the role of vitamin D as an importantfactor associated with risk of lower respiratory tract infection.
There is a continued debate on the optimal 25(OH) Dconcentration and the cutoff values for vitamin D deficiencyand insufficiency. The association of vitamin D insufficiencywith different diseases and the importance of maintainingsufficient 25(OH) D levels greater than 30 ng/ml for non-skeletal benefits have been pointed out [18, 21, 23]. TheInstitute of Medicine (IOM, USA) [40] established that25(OH) D levels of 20 ng/ml (50 nmol/l) were sufficient foroptimal bone health and immune health and concluded thatthere was insufficient evidence to recommend any activevitamin D supplementation. In contrast, according to theconsensus guideline from the US Endocrine Society [22],vitamin D deficiency is defined as a 25(OH) D levels lessthan 20 ng/ml (50 nmol/l) and vitamin D insufficiency as25(OH) D levels of 21 to 29 ng/ml (52.5 to 72.5 nmol/l). Thisguideline strongly recommends circulating levels of 25(OH)D higher than 30 ng/ml for optimal bone and immune health.
One of the major strengths of our cross-sectional study isthat serum 25(OH) D levels were measured during infantdisease. On the other hand, confounding factors such as low-or overweight were controlled (exclusion criteria) and therewere no differences between groups regarding type of feeding,vitamin D supplementation and sun exposure. However, wecannot be certain that other confounder factors have alteredour findings such as genetic variants in vitamin D bindingprotein (VDBP) [17, 20] or VDR gene polymorphisms [28,35, 46] which are able to influence intracrine and endocrinefunctions of vitamin D.
Randolph et al. suggested that vitamin D binding protein(VDBP, Gc-globulin) haplotypes especially GC1s may in-crease the risk of RSV bronchiolitis [39]. This haplotype isassociated with higher VDBP levels resulting in less freelyavailable vitamin D. Relevant literature has recently revealeda strong association of VDR gene polymorphisms with therisk of bronchiolitis or as factors for severe RSV disease [28,35, 46]. Moreover, Stoppelenburg et al. highlighted that it isnot understoodwhy the VDRFokI polymorphism predisposesto severe bronchiolitis and provided mechanistic insight thatthe FokI-VDR polymorphism renders STAT 1 mediated anti-viral immune reactions to RSV infections non responsive tovitamin D control, resulting in enhanced immunopathologyand exacerbated RSV bronchiolitis [46]. These findings maycontribute to better understanding the role of the vitamin Dpathway in RSV bronchiolitis.
This study has some limitations. It is a cross-sectional studynot proving causation.Moreover, due to the small sample size,it is difficult to apply the results of this study to the generalpopulation. It remains unclear whether low 25(OH) D levelfound in infants with bronchiolitis is a factor contributing toinfection or a result of having the disease. It should have beenimportant to consider measurements of 25(OH) D previous todisease or in cord blood to help clarifying this issue.
The US Endocrine Society clinical practice guideline [22]recommends screening only in populations at risk as no evi-dence currently exists to support screening at a populationlevel. However, we are of opinion that infants at risk ofhypovitaminosis D should be considered as candidates forscreening during the fall and winter months. The US Endo-crine Society (2011) [22] and ESPGHAN (2013) [7], recom-mend that 400 IU per day may be needed for infants aged lessthan 1 year. However, to raise the serum level of 25(OH)Dconsistently above 30 ng/ml (75 nmol/l), it may be required atleast 1,000 IU per day of vitamin D, a higher dose than thatrecommended [22, 7, 47].
In conclusion, this study shows that hypovitaminosis D ishighly prevalent in infants with bronchiolitis in a populationfrom southern Spain. Infants with moderate–severe bronchi-olitis had the 25(OH) D lowest levels. We suggest an adequatecompliance with vitamin D prophylaxis, particularly in thefirst year of life to achieve sufficient levels of 25(OH) D,which may help to reduce the burden of bronchiolitis duringthe first year of life. Further multicenter and randomizedprospective trials are required to clarify these questions.
Acknowledgments We are grateful to AntonioMartin, laboratory tech-nician, for technical support in the laboratory measurements, nursing stafffor their involvement and parents of all infants for their participation in thestudy
Conflicts of interest Authors do not have any conflict of interest inrelation to this work. The study was partially funded by a grant from theSpanish Society of Paediatric Pulmonology (SENP).
Eur J Pediatr

References
1. American Academy of Pediatrics. Subcommittee on Diagnosis andManagement of Bronchiolitis (2006) Diagnosis and management ofbronchiolitis. Pediatrics 118:1774–93
2. Alonso A, Rodríguez J, Carvajal I, Prieto ML, Rodríguez RM, PérezAM, Santos F (2011) Prophylactic vitamin D in healthy infants:assessing the need. Metabolism 60(12):1719–1725
3. Baeke F, Gysemans C, Korf H, Mathieu C (2010) Vitamin D insuf-ficiency: implications for the immune system. Pediatr Nephrol 25(9):1597–1606
4. Balk SJ, Council on Environmental Health, Section on Dermatologyfrom American Academy of Pediatrics (2011) Ultraviolet radiation: ahazard to children and adolescents. Pediatrics 127(3):e791–817
5. Belderbos ME, Houben ML, Wilbrink B, Lentjes E, Bloemen EM,Kimpen JL, Rovers M, Bont L (2011) Cord blood vitamin D defi-ciency is associated with respiratory syncytial virus bronchiolitis.Pediatrics 127(6):e1513–e1520
6. Bergman P, Lindh AU, Björkhem-Bergman L, Lindh JD (2013)Vitamin D and respiratory tract infections: a systematic review andmeta-analysis of randomized controlled trials. PLoS One 19,8(6):e65835
7. Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T,Dawson-Hughes B (2006) Estimation of optimal serum concentra-tions of 25-hydroxyvitamin D for multiple health outcomes. Am JClin Nutr 84(1):18–28
8. Bozzetto S, Carraro S, Giordano G, Boner A, Baraldi E (2012)Asthma, allergy and respiratory infections: the vitamin D hypothesis.Allergy 67(1):10–17
9. Braegger C, Campoy C, Colomb V, Decsi T, Domellof M, FewtrellM, Hojsak I, Mihatsch W, Molgaard C, Shamir R, Turck D, vanGoudoever J, ESPGHAN Committee on Nutrition (2013) Vitamin Din the healthy European paediatric population. J Pediatr GastroenterolNutr 56(6):692–701
10. CamargoCA, Ingham T,Wickens K, Thadhani R, Silvers KM, EptonMJ, Crane J (2011) Cord-blood 25-hydroxyvitamin D levels and riskof respiratory infection, wheezing, and asthma. Pediatrics 127(1):e180–e187
11. Camargo CA Jr, Ganmaa D, Frazier AL, Kirchberg FF, Stuart JJ,Kleinman K, Sumberzul N, Rich-Edwards JW (2012) Randomizedtrial of vitamin D supplementation and risk of acute respiratoryinfection in Mongolia. Pediatrics 130(3):e561–7
12. Ferrés J (1992) Inhalation therapy in the newborn. Anales Españolesde Pediatría 36(49):160–3
13. Gallo S, Comeau K, Vanstone C, Agellon S, Sharma A, Jones G,Weiler H (2013) Effect of different dosages of oral vitamin D sup-plementation on vitamin D status in healthy, breastfed infants: arandomized trial vitamin D supplementation in healthy infants.JAMA 309(17):1785–1792
14. Gordon CM, Feldman HA, Sinclair L, Williams AL, Kleinman PK,Perez-Rossello J, Cox JE (2008) Prevalence of vitamin D deficiencyamong healthy infants and toddlers. Arch Pediatr Adolesc Med162(6):505–512
15. Grant WB (2008) Variations in vitamin D production could possiblyexplain the seasonality of childhood respiratory infections in Hawaii.Pediatr Infect Dis J 27(9):853
16. Greer FR, Searcy JE, Levin RS, Steichen JJ, Asch PS, Tsang RC(1981) Bone mineral content and serum 25-hydroxyvitamin D con-centration in breast-fed infants with and without supplemental vita-min D. J Pediatr 98(5):696–701
17. Hansdottir S, Monick MM, Lovan N, Powers L, Gerke A,Hunninghake GW (2010) Vitamin D decreases respiratory syncytialvirus induction of NF-κB–linked chemokines and cytokines in air-way epithelium while maintaining the antiviral state. J Immunol184(2):965–974
18. Henry HL (2011) Regulation of vitamin D metabolism. Best PractRes Clin Endocrinol Metab 25(4):531–541
19. HewisonM (2010) Vitamin D and the immune system: new perspec-tives on an old theme. Endocrinol Metab Clin N Am 39(2):365–379
20. Hewison M (2012) An update on vitamin D and human immunity.Clin Endocrinol 76(3):315–325
21. HolickMF (2007) VitaminD deficiency. N Engl JMed 357(3):266–28122. Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley
DA, Heaney RP, Weaver CM (2011) An Endocrine Society clinicalpractice guideline. evaluation, treatment and prevention of vitamin Ddeficiency. J Clin Endocrinol Metab 96:1911–1930
23. Hollis BW (2010) Assessment and interpretation of circulating 25-hydroxyvitamin D and 1, 25-dihydroxyvitamin D in the clinicalenvironment. Endocrinol Metab Clin N Am 39(2):271–286
24. Inamo Y, Hasegawa M, Saito K, Hayashi R, Ishikawa T, Yoshino Y,Fuchigami T (2011) Serum vitamin D concentrations and associatedseverity of acute lower respiratory tract infections in Japanese hospi-talized children. Pediatr Int 53(2):199–201
25. Iqbal S (1994) Vitamin D metabolism and the clinical aspects ofmeasuring metabolites. Ann Clin Biochem 31:109–124
26. Iqbal S, Mosenkis EV, Jain P, Wiles A, Lerner J, Benton AS,Chamberlain JM, Freishtat RJ, Teach SJ (2013) Vitamin D in pedi-atric inpatients with respiratory illnesses. Hosp Pediatr 3(4):371–6
27. Jackson DJ, Lemanske RF Jr (2010) The role of respiratory virusinfections in childhood asthma inception. Immunol Allergy Clin NAm 30(4):513–522
28. Janssen R, Bont L, Siezen CL, Hodemaekers HM, Ermers MJ,Doornbos G, Hoebee B (2007) Genetic susceptibility to respiratorysyncytial virus bronchiolitis is predominantly associated with innateimmune genes. J Infect Dis 196(6):826–834
29. Karatekin G, A Kaya OSG (2007) Association of subclinical vitaminD deficiency in newborns with acute lower respiratory infection andtheir mothers. Eur J Clin Nutr 63(4):473–477
30. Liu PT, Stenger S, Li H, Wenzel L, Tan BH, Krutzik SR, Modlin RL(2006) Toll-like receptor triggering of a vitamin D-mediated humanantimicrobial response. Science 311(5768):1770–1773
31. Mansbach JM, Camargo CA (2008) Bronchiolitis: lingering ques-tions about its definition and the potential role of vitamin D.Pediatrics 122(1):177–179
32. Mansbach JM, Camargo CA Jr (2009) Respiratory viruses in bron-chiolitis and their link to recurrent wheezing and asthma. Clin LabMed 29(4):741–755
33. Mansbach JM, Piedra PA, Borregaard N, Martineu AR, NeumanMI,Espinola JA, Camargo CA Jr (2012) Serum cathelicidin level isassociated with viral etiology and severity of bronchiolitis. JAllergy Clin Immunol 130(4):1007–8
34. McNally J, Leis K, Matheson LA, Karuananyake C, Sankaran K,Rosenberg AM (2009) Vitamin D deficiency in young children withsevere acute lower respiratory infection. Pediatr Pulmonol 44(10):981–988
35. McNally JD, Sampson M, Matheson LA, Hutton B, Little J (2014)Vitamin D receptor (VDR) polymorphisms and severe RSV bronchi-olitis: A systematic review and meta-analysis. Pediatr Pulmonol49(8):790–799
36. Nair H, Nokes DJ, Gessner BD, DheraniM,Madhi SA, Singleton RJ,Campbell H (2010) Global burden of acute lower respiratory infec-tions due to respiratory syncytial virus in young children: a system-atic review and meta-analysis. Lancet 375(9725):1545–1555
37. Płudowski P, Karczmarewicz E, Bayer M, Carter G, Chlebna-SokółD, Czech-Kowalska J, Dębski R, Decsi T, Dobrzańska A, Franek E,Głuszko P, GrantWB, HolickMF, Yankovskaya L, KonstantynowiczJ, Książyk JB, Księżopolska-Orłowska K, Lewiński A, Litwin M,Lohner S, Lorenc RS, Lukaszkiewicz J, Marcinowska-SuchowierskaE, Milewicz A, Misiorowski W, Nowicki M, Povoroznyuk V,Rozentryt P, Rudenka E, Shoenfeld Y, Socha P, Solnica B, SzaleckiM, Tałałaj M, Varbiro S, Zmijewski MA (2013) Practical guidelines
Eur J Pediatr

for the supplementation of vitamin D and the treatment of deficits inCentral Europe—recommended vitamin D intakes in the generalpopulation and groups at risk of vitamin D deficiency.Endokrynologia Polska 64(4):319–27
38. Pludowski P, Grant WB, Bhattoa HP, Bayer M, Povoroznyuk V,Rudenka E, Ramanau H, Varbiro S, Rudenka A, Karczmarewicz E,Lorenc R, Czech-Kowalska J, Konstantynowicz J (2014) Vitamin Dstatus in Central Europe. Int J Endocrinol. doi:10.1155/2014/589587.
39. Randolph AG, YipWK, Falkenstein-Hagander K, Weiss ST, JanssenR, Keisling S, Bont L (2014) Vitamin D-binding protein haplotype isassociated with hospitalization for RSV bronchiolitis. Clin ExpAllergy 44(2):231–7
40. Ross AC, Manson JE, Abrams SA, Aloia JF, Brannon PM, ClintonSK, Shapses SA (2011) The 2011 report on dietary reference intakesfor calcium and vitamin D from the Institute of Medicine: whatclinicians need to know. J Clinic Endocrinol Metabol 96(1):53–58
41. RothDE, Jones AB, Prosser C, Robinson JL, Vohra S (2007)VitaminD status is not associated with the risk of hospitalization for acutebronchiolitis in early childhood. Eur J Clin Nutr 63(2):297–299
42. Roth DE, Shah R, Black RE, Baqui AH (2010) Vitamin D status andacute lower respiratory infection in early childhood in Sylhet,Bangladesh. Acta Paediatr 99(3):389–393
43. Shin YH, Yu J, Kim KW, Ahn K, Hong SA, Lee E, Yang SI, JungYH, Kim HY, Seo JH, Kwon JW, Kim BJ, Kim HB, Shim JY, KimWK, Song GJ, Lee SY, JangGC, SuhDI, Yang HJ, Kim BS, Choi SJ,
Oh SY, Kwon JY, Lee KJ, Park HJ, Lee PR, Won HS, Hong SJ,COCOA study group (2013) Association between cord blood 25-hydroxyvitamin D concentrations and respiratory tract infections inthe first 6 months of age in a Korean population: a birth cohort study(COCOA). Korean J Pediatr 56(10):439–45
44. Somech R, Tal G, Gilad E, Mandelberg A, Tal A, Dalal I (2006)Epidemiologic, socioeconomic, and clinical factors associated withseverity of respiratory syncytial virus infection in previously healthyinfants. Clin Pediatr 45(7):621–627
45. Stockman LJ, Curns AT, Anderson LJ, Fischer-Langley G (2012)Respiratory syncytial virus-associated hospitalizations among infantsand young children in the United States, 1997–2006. Pediatr InfectDis J 31(1):5–9
46. Stoppelenburg AJ, Von Hegedus JH, Huis in’t Veld R, Bont L, BoesM (2014) Defective control of vitamin D receptor-mediated epithelialSTAT1 signalling predisposes to severe respiratory syncytial virusbronchiolitis. J Pathol 232(1):57–64
47. Wagner CL, Greer FR (2008) Prevention of rickets and vitamin Ddeficiency in infants, children, and adolescents. Pediatrics 122(5):1142–1152
48. Walker VP, Modlin RL (2009) The vitamin D connection topediatric infections and immune function. Pediatr Res 65:106R–113R
49. Zorc JJ, Hall CB (2010) Bronchiolitis: recent evidence on diagnosisand management. Pediatrics 125(2):342–9
Eur J Pediatr