Embed Size (px)
Citation preview

Lymphadenopathy, Cough, and Fever in a51-Year-Old Woman With Systemic LupusErythematosus: Case Report of LymphomatoidGranulomatosisLAUREN A. BESTE,1 ALI ANSARI-LARI,2 MICHAEL BOROWITZ,2 AND JOHN A. FLYNN2
IntroductionLymphomatoid granulomatosis is a rare, often fatal lym-phoproliferative disease that is most common in immuno-suppressed patients such as those with acquired immuno-deficiency syndrome, organ transplant, or Wiskott-Aldrichsyndrome. It has been described in patients with a varietyof autoimmune disorders including Sjogren’s syndrome(1), ulcerative colitis, rheumatoid arthritis (2), Crohn’s dis-ease, Hashimoto thyroiditis, and juvenile rheumatoid ar-thritis (3). This report is the first to describe lymphomatoidgranulomatosis in a patient with systemic lupus erythem-atosus (SLE).
Case ReportThe patient, a 51-year-old African American woman witha 36-year history of SLE presented to our rheumatologyclinic with the symptom of cough. When the patient was ateenager, lupus was diagnosed, in the setting of Raynaud’ssyndrome, arthritis, and cutaneous symptoms. She had abaseline antinuclear antibody titer of 1:640, negative an-ti-Ro and anti-La antibodies, and negative anti–double-stranded DNA antibodies. Over the course of the patient’sdisease, calcinosis universalis developed, which was com-plicated by multiple episodes of cellulitis requiring oper-ative treatment and skin grafting. Otherwise, the patient’slupus was well-controlled while she received long-termtherapy with low-dose steroids. She had no history ofmajor pulmonary infection, pneumonitis, or tobacco use.
The patient presented with a 4-month history of morn-
ing cough. Physical examination revealed bibasilar crack-les, and chest examination demonstrated a nontender,nonfluctuant, mobile lymph node in her left submandibu-
1Lauren A. Beste, BS: Johns Hopkins University School ofMedicine, Baltimore, Maryland; 2Ali Ansari-Lari, MD, Mi-chael Borowitz, MD, PhD, John A. Flynn, MD, MBA: JohnsHopkins Hospital, Baltimore, Maryland.
Address correspondence to John A. Flynn, MD, MBA,Department of Medicine, Johns Hopkins University, 601North Caroline Street #7143, Baltimore, MD 21287. E-mail:[email protected].
Submitted for publication April 23, 2004; accepted inrevised form December 4, 2004.
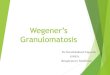
Figure 1. Thoracic computed tomography showing enlarged medi-astinal nodes measuring � 1.0 cm. Patchy areas of nodular consoli-dation are present in all lobes, with the largest consolidation mea-suring 3.8 cm in the right lower lobe and 1.5 cm in the left lower lobe.
Arthritis & Rheumatism (Arthritis Care & Research)Vol. 53, No. 4, August 15, 2005, pp 621–624DOI 10.1002/art.21310© 2005, American College of Rheumatology
TRAINEE ROUNDS
621

lar area measuring 3.0 � 2.0 cm. Pulmonary evaluationincluded a chest radiograph, which showed interstitialfibrosis without adenopathy, and pulmonary functiontests, which showed a mild restrictive ventilatory defectwith a moderate gas transfer defect. Due to periodontaldisease, the patient was started on cefazolin, which re-sulted in initial improvement of adenopathy. This sub-mandibular adenopathy recurred after several weeks, withdevelopment of supraclavicular and axillary lymphade-nopathy. The patient’s cough continued, although she de-nied having chest pain or dyspnea on exertion. Thoraciccomputed tomography showed axillary, mediastinal, andpretracheal adenopathy, with lung nodules up to 2.7 cm indiameter against a background of fine interstitial inflam-mation (Figure 1). Autoimmune serologies were un-changed, with negative antineutrophil cytoplasmic anti-bodies and normal complement levels. Test results forhuman immunodeficiency virus, blastomycosis antigen,histoplasma antigen, mycoplasma antigen, cytomegalovi-rus antigen, and tuberculosis were negative.
Fine-needle aspiration of a supraclavicular node dem-onstrated reactive hyperplasia. Excisional biopsy of theright axillary node was nondiagnostic. Given the nondiag-nostic biopsy results, the adenopathy was believed to berelated to the patient’s lupus, and she was started on an
empirical trial of 20 mg of prednisone daily, which led todramatic improvement of adenopathy and resolution ofcough and fevers.
Within 3 months the nodes had regained their bulk inthe setting of steroid tapering. Repeat pulmonary functiontesting showed progression of restrictive lung disease.Spiking fevers developed, and the patient was admitted forfurther evaluation. Chest and abdominal computed tomog-raphy showed small pericardial effusion, enlarged periaor-tic and celiac nodes, a prominent spleen with small calci-fications, and bilaterally enlarged kidneys. Bronchialalveolar lavage with transbronchial biopsy was nondiag-nostic, with negative stains for acid-fast bacilli and fungi.The bone marrow aspirate was unremarkable. Renal bi-opsy revealed tubular atrophy and neutrophilic infiltrate,necrotic glomeruli, and interstitial fibrosis without evi-dence of glomerulonephritis. Internal fibrosis of interlob-ular-sized arteries was noted. The patient underwent openlung biopsy, with pathology showing angiocentric T cell–rich B cell lymphoma with positive in situ hybridizationfor Epstein-Barr virus (EBV) (Figure 2). Stains for acid-fastbacilli, fungi, and bacteria were negative. A diagnosis oflymphomatoid granulomatosis was made.
A treatment protocol with interferon �-2b was initiatedand the patient reported an improved energy level, less
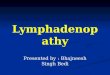
Figure 2. Lymphomatoid granulomatosis involving lung. A, Hemotoxylin and eosin–stained section of a tumor noduleshowing atypical lymphoid infiltrate (original magnification � 50). B, At a higher magnification (400 �), manylymphocytes appear large, with prominent nucleoli. There are scattered small mature lymphocytes in the background.The infiltrate also showed angiocentricity with angiodestructiveness. C, Immunohistochemical stain for CD20 high-lights numerous B cells. There were scattered CD3-positive T cells in the background (not shown). D, In situhybridization for Epstein-Barr virus (EBER) shows positive cells.
622 Beste et al

dyspnea on exertion, and a 6–7 pound weight gain. Ap-proximately 1 month after the initiation of chemotherapy,she was readmitted because of fever, acute renal failure,increasing respiratory insufficiency with bilateral lung in-filtrates, and hypotension requiring mechanical ventila-tion and vasopressors. After initial stabilization, she wasstarted on a cycle of rituximab plus etoposide, cyclosphos-phamide, doxorubicin, vincristine, and prednisone. Com-puted tomography showed improvement in lymphadenop-athy. The patient was successfully extubated. On day 1after extubation, she experienced multiple intracranialhemorrhages as well as diffuse white matter changes that,on magnetic resonance imaging, were believed to repre-sent posterior reversible leukoencephalopathy. She wasnoted to have thrombocytopenia and International Nor-malized Ratio of 1.3. The patient was reintubated, and thecoagulopathy was corrected. Despite aggressive manage-ment, followup images remained unchanged and shenever fully regained consciousness. According to the fam-ily’s wishes, the patient was designated “do-not-resusci-tate,” and she died 45 days after the original admission.
Post mortem examination revealed evidence of lympho-matoid granulomatosis predominantly affecting the lungs,kidneys, and brain, with microscopic disease foundthroughout the body (Figure 3). Multifocal cerebral hem-orrhages were secondary to involvement of cerebral vas-culature with lymphoma. Because the hemorrhages werenot severe enough to cause herniation, her terminal de-cline was considered to be attributable to systemic burdenof disease.
Discussion
Lymphomatoid granulomatosis is a rare entity that wasfirst described in 1972, by Liebow and colleagues, amongpatients with Wegener’s granulomatosis (4). It is an angio-centric, angiodestructive lymphoproliferative disordercharacterized by nodular mass lesions. The pathogenesisof the malignancy has been related to EBV infection of Bcells (5). Additional histopathologic features include poly-morphic lymphoid infiltrates, vascular infiltration, and ne-crosis (4). Abundant reactive T cells and a vasculitic com-ponent are seen (5). The malignant B cells, which are oftenmonoclonal or oligoclonal, stain positive for EBV. How-ever, most of the infiltrating cells are reactive T cells.
Lymphomatoid granulomatosis is most common in the4th through 6th decades of life, occurring �3 times asoften in men as in women. Generally, the 3 most commoninitial symptoms are fever, cough, and dyspnea (4). Thelung is the most commonly affected organ, followed by theskin, kidney, spleen, and liver. Lymphadenopathy is com-paratively rare, occurring in �7–8% of cases (2,6), al-though lymph node involvement is found in up to 40% ofpatients at autopsy (7). The clinical course is variable, andthere are some reports of spontaneous regression (2,6).However, in the largest study of lymphomatoid granulo-matosis to date, a median survival of 20 months in patientsreceiving chemotherapy and steroids was reported (2).
Results of cohort studies attempting to evaluate overallmalignancy rates in patients with lupus have been mixed.Although large controlled studies have yet to be carried
Figure 3. Lymphomatoid granulomatosis involving the lung andkidney. A, Right lower lobe of the lung, showing multiple nodulesof tumor with necrosis, ranging in size from 0.2–3.0 cm. B, Rightkidney, showing multiple nodules of necrotic tumor involving thecortex and medulla. The largest nodule measured 5.0 cm in itsgreatest dimension.
Lymphomatoid Granulomatosis in a 51-Year Old Woman With SLE 623

out, most cohort studies have demonstrated elevated ratesof hematologic cancers compared with the rate in thegeneral population (8–11). The biologic mechanism for theincreased risk of lymphoid malignancies in SLE is not yetunderstood. Persistent inflammation and lymphocyte hy-peractivity in concert with poor immune surveillance havebeen theorized to play a role (8). Somatic CD95 (Fas/Apo1) mutations have been identified in both non-Hodgkin’slymphoma and autoimmune conditions, including SLE,possibly indicating that both disorders share failure ofapoptosis of autoreactive lymphocytes (12). Murine andhuman mutations in CD95/CD95 ligand (CD95L) havebeen associated with a range of phenotypes, including alupus-like syndrome as well as apoptotic defects in lym-phocytes (13), although abnormalities of CD95/CD95Lhave not consistently been found among lupus patients(14). Finally, an increased prevalence of the oncogenicEBV has been reported in lupus, potentially predisposingto B cell lymphomas such as lymphomatoid granulomato-sis (15). Although these mechanisms are promising, fur-ther study is needed to clarify the etiology of increasednon-Hodgkin’s lymphoma in lupus.
REFERENCES
1. Capron F, Audouin J, Diebold J, Ameille J, Lebeau B, Roch-emaure J. Pulmonary polymorphic centroblastic type malig-nant lymphoma in a patient with lymphomatoid granuloma-tosis, Sjogren syndrome and other manifestations of adysimmune state. Pathol Res Pract 1985;179:656–65.
2. Katzenstein AL, Carrington CB, Liebow AA. Lymphomatoidgranulomatosis: a clinicopathologic study of 152 cases. Can-cer 1979;43:360–73.
3. Pisani RJ, DeRemee RA. Clinical implications of the his-topathologic diagnosis of pulmonary lymphomatoid granulo-matosis. Mayo Clin Proc 1990;65:151–63.
4. Liebow AA, Carrington CR, Friedman PJ. Lymphomatoidgranulomatosis. Hum Pathol 1972;3:457–558.
5. Guinee D Jr, Jaffe E, Kingma D, Fishback N, Wallberg K,Krishnan J, et al. Pulmonary lymphomatoid granulomatosis:evidence for a proliferation of Epstein-Barr virus infectedB-lymphocytes with a prominent T-cell component and vas-culitis. Am J Surg Pathol 1994;18:753–64.
6. Koss MN, Hochholzer L, Langloss JM, Wehunt WD, LazarusAA, Nichols PW. Lymphomatoid granulomatosis: a clinico-pathologic study of 42 patients. Pathology 1986;18:283–8.
7. Fauci AS, Haynes BF, Costa J, Katz P, Wolff SM. Lymphoma-toid granulomatosis: prospective clinical and therapeutic ex-perience over 10 years. N Engl J Med 1982;306:68–74.
8. Sultan SM, Ioannou Y, Isenberg DA. Is there an association ofmalignancy with systemic lupus erythematosus? An analysisof 276 patients under long-term review. Rheumatology (Ox-ford) 2000;39:1147–52.
9. Cibere J, Sibley J, Haga M. Systemic lupus erythematosus andthe risk of malignancy. Lupus 2001;10:394–400.
10. Mellemkjaer L, Andersen V, Linet MS, Gridley G, Hoover R,Olsen JH. Non-Hodgkin’s lymphoma and other cancers amonga cohort of patients with systemic lupus erythematosus. Ar-thritis Rheum 1997;40:761–8.
11. Nived O, Bengtsson A, Jonsen A, Sturfelt G, Olsson H. Malig-nancies during follow-up in an epidemiologically definedsystemic lupus erythematosus inception cohort in southernSweden. Lupus 2001;10:500–4.
12. Gronbaek K, Straten PT, Ralfkiaer E, Ahrenkiel V, AndersenMK, Hansen NE, et al. Somatic Fas mutations in non-Hodgkin’s lymphoma: association with extranodal diseaseand autoimmunity. Blood 1998;92:3018–24.
13. Vaishnaw AK, Toubi E, Ohsako S, Drappa J, Buys S, Estrada J,et al. The spectrum of apoptotic defects and clinical manifes-tations, including systemic lupus erythematosus, in humanswith CD95 (Fas/APO-1) mutations. Arthritis Rheum 1999;42:1833–42.
14. Mysler E, Bini P, Drappa J, Ramos P, Friedman SM, KrammerPH, et al. The apoptosis-1/Fas protein in human systemiclupus erythematosus. J Clin Invest 1994;93:1029–34.
15. James JA, Kaufman KM, Farris AD, Taylor-Albert E, LehmanTJ, Harley JB. An increased prevalence of Epstein-Barr virusinfection in young patients suggests a possible etiology forsystemic lupus erythematosus. J Clin Invest 1997;100:3019–26.
DOI 10.1002/art.21362
Erratum
In the article by Merkesdal et al published in the April 2005 issue of Arthritis & Rheumatism (pp 234–240), thestatement “Drs. Merkesdal and Ruof contributed equally to this work” was inadvertently omitted.
We regret the error.
624 Beste et al