Embed Size (px)
Citation preview
Kaohsiung Journal of Medical Sciences (2012) 28, 509e513
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by Elsevier - Publisher Connector
Available online at www.sciencedirect.com
journal homepage: http: / /www.kjms-onl ine.com
CASE REPORT
Lymphoepithelioma-like carcinoma of ureterdA rare casereport and review of the literature
Sheng-Chen Wen a, Jung-Tsung Shen b,*, Mei-Yu Jang b, Kun-Bow Tsai c, Shu-Fang Chang b,Li-Jiun Tsai b, Wen-Jeng Wu b,d
aDepartment of Urology, Kaohsiung Medical University Hospital, Kaohsiung, TaiwanbDepartment of Urology, Kaohsiung Municipal Hsiao-Kang Hospital, Kaohsiung, TaiwancDepartment of Pathology, Kaohsiung Municipal Hsiao-Kang Hospital, Kaohsiung, TaiwandDepartment of Urology, Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung,Taiwan
Received 28 April 2011; accepted 13 July 2011Available online 7 July 2012
KEYWORDSEpsteineBarr virus;Lymphoepithelioma-like carcinoma;Urothelial;Ureter
* Corresponding author. DepartmentKaohsiung City 812, Taiwan.
E-mail address: [email protected]
1607-551X/$36 Copyright ª 2012, Elsedoi:10.1016/j.kjms.2012.04.010
Abstract Lymphoepithelioma-like carcinoma (LELC) is best known to occur in the naso-pharynx. When LELC occurs in the urinary tract, this extremely rare neoplasm most commonlyaffects the bladder but has also been reported in the renal pelvis, ureter, prostate [1], andurethra [2]. We present a case of LELC arising in the right proximal ureter of a 64-year-old malepatient with hydronephrosis and nausea. Computed tomography demonstrated right uretertumor. On biopsy, the patient was diagnosed with infiltrating urothelial carcinoma. An opera-tion consisting of right nephroureterectomy and bladder cuff removal was carried out. Thepathologic examination showed pure subtype of LELC, pT3N0. Unlike lymphoepithelioma inthe nasopharynx, immunohistochemical analysis of this urinary LELC was negative for the Ep-steineBarr virus. No disease progression was noted at 6 months’ follow-up. Only eight previouscases of LELC involving the ureter have been reported, and a review of the available literatureand a summary of ureter cases are presented here. This is the first report of a ureteral LELCcase and third urothelial LELC cases [3] in Taiwan.Copyright ª 2012, Elsevier Taiwan LLC. All rights reserved.
of Urology, Kaohsiung Municipal Hsiao-Kang Hospital, Number 482, Shanming Road, Siaogang District,
m (J.-T. Shen).
vier Taiwan LLC. All rights reserved.
510 S.-C. Wen et al.
Introduction
Lymphoepithelioma is an undifferentiated, malignant,epithelial tumor of the nasopharynx that is histologicallydistinct by virtue of a prominent lymphoid infiltrate sugges-tive of malignant lymphoma [4,5]. Tumors of similar histo-logic type have been described at sites other than thenasopharynx, including the lung, stomach, cervix, and skin,and are known as lymphoepithelioma-like carcinoma (LELC).Primary urothelial LELC, occurring in the bladder, was firstdescribed in 1991 by Zukerberg et al. [6]. LELC is usuallymuscle-invasive at the time of diagnosis (90% are pT2 orpT3) [7]. When LELCs arise from the urinary tract,lymphoepithelioma-like carcinoma bladder (LELCB) is mostcommon. There are around 80 reported cases concerningbladder LELCs to date. As for upper urinary tract LELCs, thereareonly nine cases [8e15] in theureter and sevencases in therenal pelvis [2,16e20]. Amin et al. [21] categorized LELCB aspure (100%), predominant (>50%), and focal (<50%)according to the proportion of LELC and other neoplasmssuch as urothelial carcinoma and squamous cell carcinoma.Patients with pure and predominant LELCB were reported to
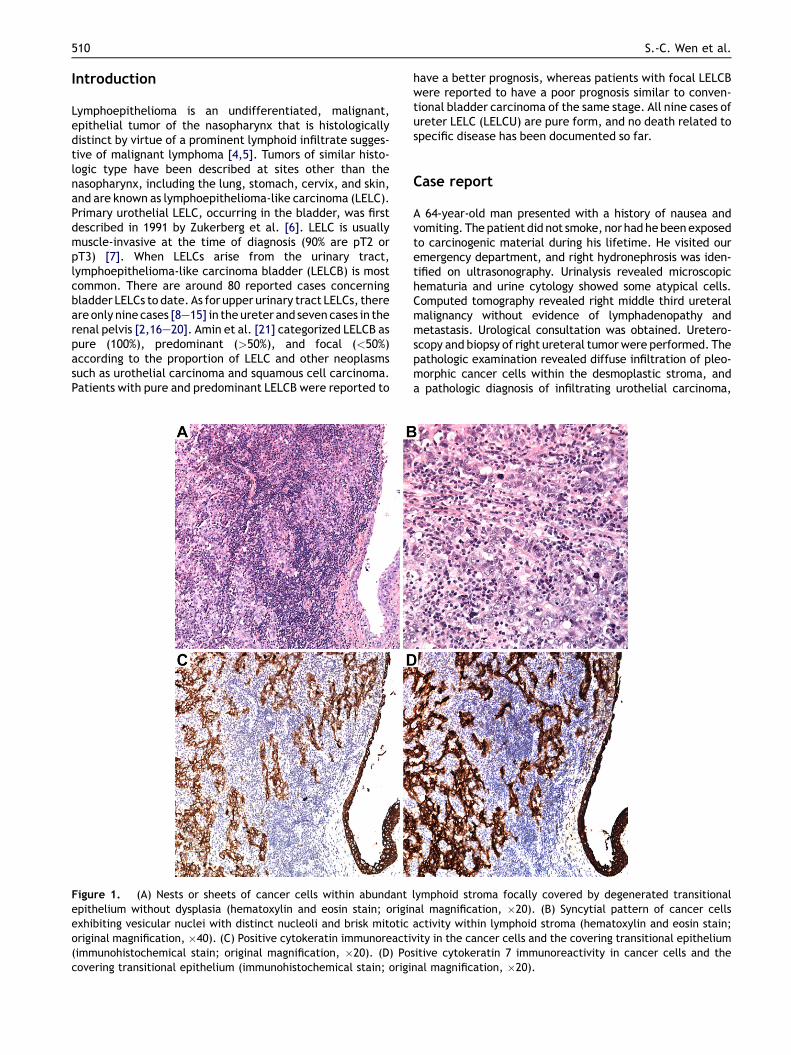
Figure 1. (A) Nests or sheets of cancer cells within abundantepithelium without dysplasia (hematoxylin and eosin stain; originexhibiting vesicular nuclei with distinct nucleoli and brisk mitoticoriginal magnification, �40). (C) Positive cytokeratin immunoreacti(immunohistochemical stain; original magnification, �20). (D) Pocovering transitional epithelium (immunohistochemical stain; origi
have a better prognosis, whereas patients with focal LELCBwere reported to have a poor prognosis similar to conven-tional bladder carcinoma of the same stage. All nine cases ofureter LELC (LELCU) are pure form, and no death related tospecific disease has been documented so far.
Case report
A 64-year-old man presented with a history of nausea andvomiting. The patient did not smoke, nor had hebeenexposedto carcinogenic material during his lifetime. He visited ouremergency department, and right hydronephrosis was iden-tified on ultrasonography. Urinalysis revealed microscopichematuria and urine cytology showed some atypical cells.Computed tomography revealed right middle third ureteralmalignancy without evidence of lymphadenopathy andmetastasis. Urological consultation was obtained. Uretero-scopy and biopsy of right ureteral tumorwere performed. Thepathologic examination revealed diffuse infiltration of pleo-morphic cancer cells within the desmoplastic stroma, anda pathologic diagnosis of infiltrating urothelial carcinoma,
lymphoid stroma focally covered by degenerated transitionalal magnification, �20). (B) Syncytial pattern of cancer cellsactivity within lymphoid stroma (hematoxylin and eosin stain;vity in the cancer cells and the covering transitional epitheliumsitive cytokeratin 7 immunoreactivity in cancer cells and thenal magnification, �20).
reatm
ent
Follow-up
(mo)
Outcome
Pure
ormixed
/psoashitch
12NED
Pure
18NED
Pure
18NED
Pure
30NED
Pure
36Diedof
pancreaticCA3y
postoperative
ly
Pure
24NED
Pure
5NED
Pure
/partial
rectomy
5NED
Pure
18.5
DSS
Z10
0%Allpure
6NED
Pure
able;NEDZ
noevidence
ofdisease;NUZ
nephroureterectomy;
logica
lly.
Lymphoepithelioma-like carcinoma of the ureter 511
high grade, wasmade. After a discussion with this patient andhis family, right radical nephroureterectomywithbladder cuffremoval was carried out.
Upon opening of the ureter, a solitary 2.2-cm ulceratedtumor was identified protruding into the lumen of themiddle ureter, around 14 cm from the distal margin of thesurgical resection. No other lesion was noted on the bladdercuff, ureter, or renal pelvis. Histologic sections of theneoplasm showed that the tumor had invaded beyond themuscularis propria into the periureteric tissue. The tumorwas composed of nests or sheets within abundant lymphoidstroma focally covered by degenerated transitionalepithelium without dysplasia (Figs. 1A and 1B). Neoplasticcells showed positive immunohistochemical staining forcytokeratin 7 (Figs. 1C and 1D); a cytokeratin 20 stain waspositive in the superficial transitional epithelium butnegative in the cancer cells. Latent membrane protein 1immunostaining and in situ hybridization for EpsteineBarrvirus were (EBV) negative.
The patient did not receive any adjuvant chemotherapyand radiotherapy postoperatively. He remains well withoutevidence of disease at 6 months after the surgery.
Table
1Su
mmary
oflymphoepithelioma-likeca
rcinoma(LELC
)ca
sesin
theureter.
Case
Year
Laterality
Loca
tionof
ureter
Gender
Age
Hematuria
OtherS/S
Stage
T
Chalik[8]
1998
RD
M75
(þ)
flankpain
T3N
0M0
Uw
Ng[10]
1999
RU
F62
(þ)
flankpain
T2N
0M0
NU
Roig
[11]
2001
LU
M58
(þ)
N/A
T3N
0M0
NU
Terai[12]
2005
RD
M73
(þ)
N/A
pT2N
0NU
Ozand
Sedmak[14]
2005
LM
F71
(þ)
N/A
N/A
NU
PeterMa[9]
2008
LD
F64
(þ)
N/A
T2N
xMx
UDaniela
[7]
2010
RM
M71
(þ)
N/A
T2N
0M0
NU
Val-Bernal[13]
2010
LM
F76
(e)
Recu
rrent
UTI
N/A
Uw
neph
Meanand
proportion
R(55.6%
)L(44.4%
)U/M
/L(33.3%
/33
.3%/3
3.3%
)M
(55.6%
)F(44.4%
)68
.22
88.89%
* All>T1
Presentca
se20
10R
UM
64(þ
)Nausea
pT3N
0M0
NU
DZ
lowerthird;DSS
Zdisease-specificsurvival;FZ
female;LZ
left;MZ
male;MZ
middle
third;N/A
Znotapplic
RZ
righ
t;UZ
upperthird;UZ
ureterectomy;
w/Z
with.
*There
were
twoca
seswithoutdescriptionoftumorstage
.Allreportedca
seswere
diagn
osedmuscle-inva
sive
patho
Discussion
LELCs can arise in many sites, such as the salivary gland,thymus, lung, stomach, skin, and urothelium. The first caseof urothelium (bladder) was reported in 1991 by Zukerberget al. [6], and LELCs have been classified as a separatevariant of urothelial carcinoma in the World Health Orga-nization 2004 classification of urothelial tumors [22].Besides arising in the bladder, LELCs arising from the renalpelvis [2,16e20], ureter [8e15], prostate [1], and urethra[2] were also reported. In order to characterize themalignancy, LELC is subdivided histologically based on thepercentage of non-LELC components. The subtypes werepure (100%), predominant (more than 50%), and focal (lessthan 50%), according to Amin et al.’s suggestion [21].According to the study of Porcaro et al. [7], LELCB histo-logical subtypes resulted pure in 40%, predominant in 37%,and focal in 23%. They also observed that the disease-freesurvival and disease-specific survival rate was 81% and93% in the pure LELCB group (mean follow-up, 48 months),82% and 93% in the predominant LELCB group (mean follow-up, 32 months), and 0% and 0% in the focal LELCB group(mean follow-up, 30 months), respectively [7]. That is tosay, the purer the LELCs cells, the better the prognosis.
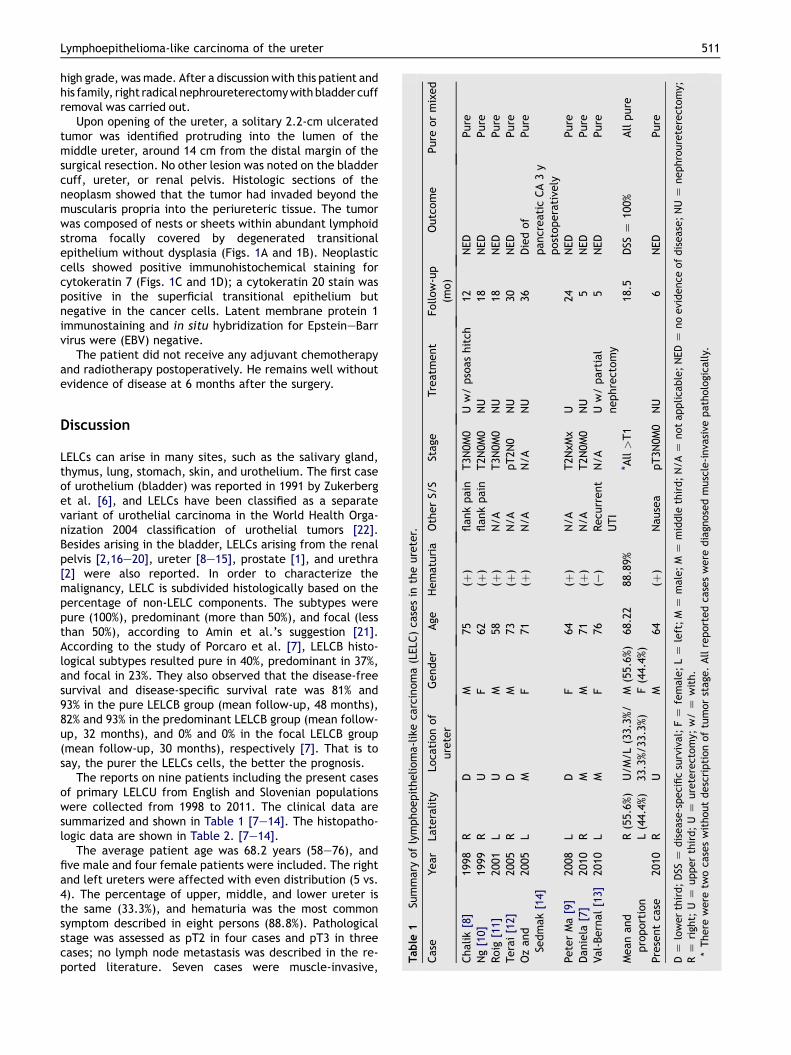
The reports on nine patients including the present casesof primary LELCU from English and Slovenian populationswere collected from 1998 to 2011. The clinical data aresummarized and shown in Table 1 [7e14]. The histopatho-logic data are shown in Table 2. [7e14].
The average patient age was 68.2 years (58e76), andfive male and four female patients were included. The rightand left ureters were affected with even distribution (5 vs.4). The percentage of upper, middle, and lower ureter isthe same (33.3%), and hematuria was the most commonsymptom described in eight persons (88.8%). Pathologicalstage was assessed as pT2 in four cases and pT3 in threecases; no lymph node metastasis was described in the re-ported literature. Seven cases were muscle-invasive,
Table 2 Ureter lymphoepithelioma-like carcinoma (LELC) neoplasms pathologic staining summary.
Case report CD20 CD3 CD30 Ck AE1/3 CK7 CK20 EBV Other stains Urine cytology
Chalik [8] (þ) (þ) N/A N/A (þ) (þ) N/A CD68 AtypiaNg [10] N/A (þ) N/A (þ) N/A N/A (e) AE3(e) N/ARoig [11] N/A N/A N/A (þ) N/A N/A (e) p53 HER2/neu/c-erb B2 UCHL-1 N/ATerai [12] (þ) (þ) N/A (þ) (e) (e) (e) MalignantOz and Sedmak [14] N/A N/A N/A N/A N/A N/A N/A N/APeter Ma [9] (e) N/A N/A (þ) (þ) (e) (e) NegativeDaniela [7] N/A N/A N/A (þ) (þ) (þ) (e) p63þ CK903 N/AVal-Bernal [13] N/A (þ) (þ) (þ) (þ) N/A N/A CK18,p53 MalignantPresent case N/A N/A N/A N/A (þ) (e) (e) AtypiaPercentage 66.67% 100% 1/1 100% 83.33% 40% 0% Abnormal: 80%
512 S.-C. Wen et al.
whereas no description was given in the other two cases. Inall cases, LELCUs were treated with surgery alone withoutneoadjuvant or adjuvant chemotherapy and radiotherapy(including radical nephroureterectomy and bladder cuffremoval in 6, ureterectomy in 2, and partial nephrectomycombined with ureterectomy in 1). The mean follow-upperiod was 18.5 months (range 5e36 months). The outcomeshowed that eight patients (88.89%) lived with no evidenceof the disease, and one patient (11.11%) died for causesunrelated to the primary disease (pancreatic cancer 3 yearspostoperatively). The survival rate related to ureteral LELCwas 100% (compared to 93% both in pure and predominantLELCB and 0% in focal LELCB [7]).
Positive antibody reaction against cytokeratin 7 andcytokeratin AE1/3 was noted in the literature with rates of100% (6 out of 6) and 83.33% (5 out of 6), respectively. Suchfindings may suggest the epithelial component of theseneoplasms. Nasopharyngeal lymphoepithelioma has a closepathogenic relationship with EBV, and there is a strongassociation between p53 overexpression and EBV-encodedRNA status in the nasopharynx [23]. Besides arising from thenasopharynx, lymphoepithelioma from the lung, stomach,thymus, and salivary gland also showed the existence ofEBV [23e30]. However, urothelial LELC (includes currentcase) occurring in the renal pelvis, bladder, prostate, andurethra failed to demonstrate the presence of EBV. Thesedata suggested that EBV is not necessary for the develop-ment of LELC, and abnormalities of p53 regulation arecrucial in the development of urothelial LELC [31e34].
Like nasopharyngeal lymphoepithelioma, LELCB was re-ported to be sensitive to both cisplatin-based chemo-therapy and radiotherapy. Chemotherapy includes three tofive courses of methotrexate, vinblastine, doxorubicin, andcisplatin, as reported in the literature [21,27,35e37].Chemotherapy and radiotherapy were not administeredalone, but were used as adjuvant therapy for treating“focal” subtype LELCB. In the case of “pure” and“predominant” subtypes, Porcaro et al. [7] reported thatthere was no clear benefit for adjuvant therapy. For thesame reason, all LELCUs reported in the literature were of“pure” subtypes, and all these cases did not recur aftersurgical treatment alone. The reason why LELCs of “pure”or “predominant” subtypes have better prognosis thanthose of “focal subtypes” has not been well understood sofar. Zukerberg et al. [6] considered that the purer compo-nent of LELC may incite stronger immune reaction by the
host, such as hematuria and pyuria. On the contrary, webelieve that the stronger immunity status of the host mayincite fewer (and purer) varieties of components of LELC,and a stronger immune status of the host has a betterprognosis than a more vulnerable immune status.
Malignant urine cytology is usually associated withconventional urothelial carcinoma. Discussions on thecytology of lymphoepithelioma are rare, and there are onlyfew reports about the cytological presentation of thesetumors in the nasopharynx, lungs, and salivary glands.Atypical and malignant cells in urine cytological examina-tion were reported in the two cases of LELCB [38,39] andfour cases of LELCU (including the current case) [9,13,14].Cai and Parwani [40] reported that cytomorphologicfeatures included large tumor cells with high nuclear tocytoplasmic ratios, vesicular chromatin, and prominentnucleoli, presenting as single cells or intermixed withinflammatory cells [40]. However, a diagnosis made on thebasis of a urine specimen is very difficult because of therarity of the tumor. Urine cytology is very simple andnoninvasive. Neoplasms of conventional urothelial carci-noma and LELC could be diagnosed or monitored by urinecytology, especially for high-grade neoplasms.
To sum up, LELCUs are extremely rare neoplasmsand are almost muscle-invasive at diagnosis. LELCUsusually present as hematuria, and a definite diagnosis isvery challenging to make before many specimensare obtained. However, LELCUs have been successfullytreated with surgery alone (without adjuvant therapy),and the disease-specific survival rate is excellentin the limited number of published reports. To date,we report the ninth documented case of LELCUs.We believe that more cases of urothelial LELCare needed to fully understand the nature of this rareentity. This is the first report of a ureteral LELC case andthird urothelial LELC cases3 in Taiwan population.
References
[1] Lopez-Beltran A, Cheng L, Prieto R, Blanca A, Montironi R.Lymphoepithelioma-like carcinoma of the prostate. HumPathol 2009;40:982e7.
[2] Tamas EF, Nielsen ME, Schoenberg MP, Epstein JI. Lymphoe-pithelioma-like carcinoma of the urinary tract: a clinicopath-ological study of 30 pure and mixed cases. Mod Pathol 2007;20:828e34.
Lymphoepithelioma-like carcinoma of the ureter 513
[3] Chen KC, Yeh SD, Fang CL, Chiang HS, Chen YK. Lymphoepi-thelioma-like carcinoma of the urinary bladder. J Formos MedAssoc 2003;102:722e5.
[4] Carbone A, Micheau C. Pitfalls in microscopic diagnosis ofundifferentiated carcinoma of nasopharyngeal type (lym-phoepithelioma). Cancer 1982;50:1344e51.
[5] OppedalBR,BohlerPJ,MartonPF,BrandtzaegP.Carcinomaofthenasopharynx.Histopathologicalexaminationwith supplementaryimmunohistochemistry. Histopathology 1987;11:1161e9.
[6] Zukerberg LR, Harris NL, Young RH. Carcinomas of the urinarybladder simulating malignant lymphoma. A report of fivecases. Am J Surg Pathol 1991;15:569e76.
[7] Porcaro AB, Gilioli E, Migliorini F, Antoniolli SZ, Iannucci A,Comunale L. Primary lymphoepithelioma-like carcinoma ofthe urinary bladder: report of one case with review andupdate of the literature after a pooled analysis of 43 patients.Int Urol Nephrol 2003;35:99e106.
[8] Allende DS, Desai M, Hansel DE. Primary lymphoepithelioma-like carcinomaof the ureter. AnnDiagn Pathol 2010;14:209e14.
[9] Chalik YN, Wieczorek R, Grasso M. Lymphoepithelioma-likecarcinoma of the ureter. J Urol 1998;159:503e4.
[10] Ma P, Leonard T, Trussell JC. Lymphoepithelioma-like carci-noma of the ureter discovered intraoperatively duringa hysterectomy. Can J Urol 2008;15:4421e4.
[11] Ng KF, Chen TC, Chang PL. Lymphoepithelioma-like carcinomaof the ureter. J Urol 1999;161:1277e8.
[12] Roig JM, Amerigo J, Velasco FJ, Gimenez A, Guerrero E,Soler JL, et al. Lymphoepithelioma-like carcinoma of ureter.Histopathology 2001;39:106e7.
[13] Terai A, Terada N, Ichioka K, Matsui Y, Yoshimura K, Wani Y.Lymphoepithelioma-like carcinoma of the ureter. Urology2005;66:1109.e13e5.
[14] Val-Bernal JF, Gonzalez-Marquez P, Ballestero R, Zubillaga S.Primary lymphoepithelioma-like carcinoma of the ureter. AnnDiagn Pathol; 2011.
[15] Zdenka Ov�cak BS. Lymphoepithelioma-like carcinoma of theureterda case report. Zdrav Vestn; 2005:711e2.
[16] Cohen RJ, Stanley JC, Dawkins HJ. Lymphoepithelioma-likecarcinoma of the renal pelvis. Pathology 1999;31:434e5.
[17] Fukunaga M, Ushigome S. Lymphoepithelioma-like carcinomaof the renal pelvis: a case report with immunohistochemicalanalysis and in situ hybridization for the EpsteineBarr viralgenome. Mod Pathol 1998;11:1252e6.
[18] Haga K, Aoyagi T, Kashiwagi A, Yamashiro K, Nagamori S.Lymphoepithelioma-like carcinoma of the renal pelvis. Int JUro 2007;14:851e3.
[19] Perez-Montiel D, Wakely PE, Hes O, Michal M, Suster S. High-grade urothelial carcinoma of the renal pelvis: clinicopatho-logic study of 108 cases with emphasis on unusual morphologicvariants. Mod Pathol 2006;19:494e503.
[20] Yamada Y, Fujimura T, Yamaguchi T, Nishimatsu H, Hirano Y,Kawamura T, et al. Lymphoepithelioma-like carcinoma of therenal pelvis. Int J Urol 2007;14:1093e4.
[21] Amin MB, Ro JY, Lee KM, Ordonez NG, Dinney CP, Gulley ML,et al. Lymphoepithelioma-like carcinoma of the urinarybladder. Am J Surg Pathol 1994;18:466e73.
[22] Eble JNSG, Epstein JI, Sesterhenn IA, editors. World Health-Organisation classification of tumours. Tumours of the uri-narysystem and male genital organs. Lyon: IARC Press; 2004.p. 90e109.
[23] Gulley ML, Amin MB, Nicholls JM, Banks PM, Ayala AG,Srigley JR, et al. EpsteineBarr virus is detected in
undifferentiated nasopharyngeal carcinoma but not inlymphoepithelioma-like carcinoma of the urinary bladder.Hum Pathol 1995;26:1207e14.
[24] Butler AE, Colby TV, Weiss L, Lombard C. Lymphoepithelioma-like carcinoma of the lung. Am J Surg Pathol 1989;13:632e9.
[25] Cho HJ, Kim JY, Yoo J, Lee SS. Gastric carcinoma withlymphoid stroma: incidence of EBV and Helicobacter pyloriinfection. Appl Immunohistochem Mol Morphol 2003;11:149e52.
[26] Hartmann CA, Roth C, Minck C, Niedobitek G. Thymic carci-noma. Report of five cases and review of the literature. JCancer Res Clin Oncol 1990;116:69e82.
[27] Holmang S, Borghede G, Johansson SL. Bladder carcinomawith lymphoepithelioma-like differentiation: a report of 9cases. J Urol 1998;159:779e82.
[28] Kuo T, Hsueh C. Lymphoepithelioma-like salivary glandcarcinoma in Taiwan: a clinicopathological study of nine casesdemonstrating a strong association with EpsteineBarr virus.Histopathology 1997;31:75e82.
[29] Takeuchi H, Fujita H, Iwasaki F, Takeuchi T, Imadome K,Okumiya T, et al. A case of EpsteineBarr Virus (EBV)-associ-ated thymic carcinoid and investigation of existence of EBV-infected cells in thymus and thymic tumors. J Clin Microbiol2004;42:2850e4.
[30] Young RH, Eble JN. Unusual forms of carcinoma of the urinarybladder. Hum Pathol 1991;22:948e65.
[31] Chen W, Cooper NR. EpsteineBarr virus nuclear antigen 2 andlatent membrane protein independently transactivate p53through induction of NF-kappaB activity. J Virol 1996;70:4849e53.
[32] Gulley ML, Burton MP, Allred DC, Nicholls JM, Amin MB, Ro JY,et al. EpsteineBarr virus infection is associated with p53accumulation in nasopharyngeal carcinoma. Human Pathology1998;29:252e9.
[33] Izquierdo-Garcia FM, Garcia-Diez F, Fernandez I, Perez-RosadoA,SaezA, Suarez-VilelaD,etal. Lymphoepithelioma-likecarcinoma of the bladder: three cases with clinicopathologicaland p53 protein expression study. Virchows Arch 2004;444:420e5.
[34] Niemhom S, Kitazawa S, Murao S, Kunachak S, Maeda S. Co-expression of p53 and bcl-2 may correlate to the presence ofEpsteineBarr virus genome and the expression of proliferatingcell nuclear antigen in nasopharyngeal carcinoma. CancerLett 2000;160:199e208.
[35] Constantinides C, Giannopoulos A, Kyriakou G, Androulaki A,Ioannou M, Dimopoulos M, et al. Lymphoepithelioma-likecarcinoma of the bladder. BJU Int 2001;87:121e2.
[36] Dinney CP, Ro JY, Babaian RJ, Johnson DE. Lymphoepitheliomaof the bladder: a clinicopathological study of 3 cases. J Urol1993;149:840e1.
[37] Lopez-Beltran A, Luque RJ, Vicioso L, Anglada F, Requena MJ,Quintero A, et al. Lymphoepithelioma-like carcinoma of theurinary bladder: a clinicopathologic study of 13 cases. Virch-ows Arch 2001;438:552e7.
[38] Guresci S, Simsek G, Kara C, Tezer A, Bozkurt O, Unsal A.Cytology of lymphoepithelioma-like carcinoma of the urinarybladder. Cytopathology 2009;20:268e9.
[39] Ward JN, Dong WF, Pitts Jr WR. Lymphoepithelioma-likecarcinoma of the bladder. J Urol 2002;167:2523e4.
[40] Cai G, Parwani AV. Cytomorphology of lymphoepithelioma-likecarcinoma of the urinary bladder: report of two cases. DiagnCytopathol 2008;36:600e3.





![Lymphoepithelioma-like gastric carcinoma: A case report ... · like gastric carcinoma (LELGC), first described by Watanabe et al[2] in 1976 as gastric carcinoma with a lymphoid stroma,](https://img.pdfslide.net/doc/110x75/5fc7c574c9fbf527a569fd63/lymphoepithelioma-like-gastric-carcinoma-a-case-report-like-gastric-carcinoma.jpg)










![Is gastric lymphoepithelioma-like carcinoma a special ...undifferentiated nasopharyngeal carcinoma (NPC) [1–3]. They are rare and have been reported in different anatomic sites,](https://img.pdfslide.net/doc/110x75/5f3129982544021a1b48ce5f/is-gastric-lymphoepithelioma-like-carcinoma-a-special-undifferentiated-nasopharyngeal.jpg)











