Embed Size (px)
Citation preview

--e.
REVIEW ARTICLI
MAGNETIC RESONANCE IMAGING:
ITS APPLICATION TO MALE INFERTILITY
R. DALE MCCLURE, M.D.
HEDVIG HRICAK, M.D.
From the Departments of Urology and Radiology, University of California School of Medicine, and the Veterans Administration Medical Center, San Francisco, California
The introduction of magnetic resonance imag- ing (MRI) to clinical medicine has, within the past two years, added a new dimension to uro- logic diagnosis. MRI’s unique tissue contrast provides anatomic detail exceeding that of any other imaging technique. In addition, MRI pro- vides information regarding the chemical en- vironment and blood flow and promises to eval- uate indirectly the functional status of a variety of organs.
The pelvis is particularly well evaluated by MRI.1,2 Its inherent tissue contrast, provided by abundant fat surrounding genitourinary and gastrointestinal organs, and its relative immo- bility during the respiratory cycle assure excel- lent image quality. In contrast to computed to- mography (CT), MRI is not compromised by artifacts from overlying bone or surgical clips. In contrast to ultrasound, MRI is not dependent on the patient’s body build or the expertise of the operator. In MRI, no ionizing radiation is used, and no iodinated contrast agents are nec- essary.
In our initial experience with MRI in the re- productive tract of infertile men, we have dem- onstrated a number of abnormalities of the seminal vesicle caused by neoplasia, infection, hemorrhage, and congenital anomalies.
Physical Basis of MRI
The concepts fundamental to the under- standing of MRI have been reviewed in detail in several recent reports. 3~9 Magnetic resonance imaging refers to the absorption and re-emis- sion of radiofrequency (RF) electromagnetic energy by certain nuclei when placed in a
magnetic field. Atomic nuclei with an odd number of protons or neutrons or both possess spin, which results in the production of a tiny magnetic field intrinsic to each nucleus. This naturally occurring magnetic moment or field provides the handle by which the nuclei can be manipulated by an external magnetic field. Ex- amples of naturally occurring isotopic species of atoms with an odd atomic number are: carbon- 13, oxygen-17, fluorine-19, sodium-23, phos- phorous-31, and (the most abundant in living tissues) hydrogen-l. This natural abundance of hydrogen atoms is based on the ubiquity of wa- ter and lipids within living tissues.
Normally these nuclei with spin have a ran- dom orientation with no net magnetization vec- tor. When an external magnetic field is applied, the nuclei tend to align themselves parallel and anti-parallel to the external field. The number of nuclei oriented parallel to the applied field outnumbers the anti-parallel nuclei and net magnetization occurs. When an RF pulse is ap- plied to the magnetized protons, they are de- flected either 90” or 180” from their original orientation. In time these energized protons re- turn to equilibrium. In so doing, they emit energy in an RF range that may be detected by a radio receiver coil and analyzed by computer. By virtue of various physical characteristics, this returning frequency can be localized. The computer can compare it to the returning fre- quency of the other nuclei in similar or dissimi- lar areas and, on the basis of the difference in these signals, construct a map of the locations of these signal-emitting protons. This becomes the MR image.
UROLOGY I FEBRUARY 1986 / VOLUME XXVII, NUMBER 2 91

Thus, MRI is based on the ability to induce and monitor the resonance of a magnetic mo- ment of nuclei in the presence of magnetic fields. By the use of magnetic fields whose strength varies with position (gradients), it is possible to define both the location and concen- tration of resonant nuclei and thereby create images that reflect their distribution in tissue. Hydrogen, being the most sensitive for MRI of all the stable nuclei and also the most abundant nucleus in the body, is ideally suited.
The intensity of the signal is not simply a re- flection of hydrogen density, because the ob- served intensity is strongly modulated by local physical and chemical factors, including molec- ular structure, elemental composition, tem- perature, and viscosity. All these factors affect Ti and Tz relaxation times. Commonly referred to as magnetic relaxation times, T1 (spin-lattice, or longitudinal relaxation time) and Tz (spin- spin relaxation time) are exponential time con- trasts that differ in different tissues. Tz is measured in milliseconds, and Ti in seconds. The time interval between an applied RF pulse and signal reception is a measure of the role of signal delay and is designated by the instru- ment parameter TE (echo delay time).
By electronically varying the field strength and RF pulse duration and frequency rapidly, the resultant MRI signals can be differentially received by an RF monitor. By virtue of sophis- ticated computer transformation and recon- struction, the MRI signals can provide a proton density image (depicting their relative position and density), which can reveal subtle dif- ferences within and between tissues. This var- iability in the field strength and, thus, variable excitation of selected nuclei at a given RF pulse sequence can be used to develop images in al- most any plane desired.
During image formation, RF pulses must be repetitively applied to result in appropriate data points. However, if the repetition is too rapid, recovery of magnetization by the protons (realignment) cannot be established between pulses, and a weak MRI signal is produced. Therefore, the time interval between successive RF pulses (TR) is important in determining the amount and nature of information obtained. Increasing the TR can increase the intensity of the signal, depending on Tr, but this also in- creases the scanning time. The appropriate TR can enhance contrast between tissues and can provide inl&mation about their nature. By varying the field strength, pulse sequences, and
radio wave frequency and intensity, the result- ant MR image can be made to reflect one or more of several MRI parameters inherent to the tissue being examined.
Three tissue parameters are used in MRI re- construction: Ti, Tz, and proton (hydrogen) density. These parameters may be imaged sepa- rately or in combination; each may also be vari- ably weighed in process and image. Besides tis- sue parameters, several machine variables affect the character of MR images. Three types of RF pulse sequence (saturation recovery, in- version recovery, and spin-echo) may be dif- ferentially emphasized to exclude one or more of the tissue parameters.
Normal Pelvic Anatomy by MRI
Urinary bladder The inherent tissue contrast of the bladder,
provided by abundant perivesical fat (high signal intensity), and its relative immobilization during the respiratory cycle assure excellent im- age quality. The urinary bladder can be seen in the transverse, sagittal, and coronal planes. The degree of bladder distention does not influence its depiction. A distended bladder will displace bowel loops outside the pelvis, but mesenteric fat and small bowel loops may still produce an artifact at the bladder dome. Bones in the pelvis are easily recognized on MRI and do not cause artifacts. Cortical bone, which emits no signal, is seen as a low-intensity image surrounding the high-intensity bone marrow.
The T1 and T2 relaxation times of urine are high. By varying the spin-echo images, dif- ferent signal intensities of urine may be seen. By lengthening the repetition time (TR) or echo delay (TE) time, the intensity of the urine in- creases, while the signal intensity for the blad- der wall shows a relative decrease. Thus, by us- ing longer TR and TE sequences, one can assess the bladder wall thickness and its regularity.
Seminal vesicles The size and configuration of the seminal
vesicles are clearly displayed in their location behind the bladder imbedded in retroperitoneal fat. On transaxial and sagittal scans, one can demonstrate the angle between seminal vesicles and the urinary bladder. As with other body tis- sue, the signal intensity from seminal vesicles depends on the scanning sequences. They have a medium-intensity signal on the short pulse se- quence (TR = 0.5 seconds). By increasing the
92 UROLOGY i FEBRUARY 1986 / VOLUME XXVII, NUMBER 2

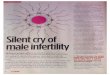
FIGURE 1. (A) Transaxial MR image (TR = 0.5 set, TE = 28 msec) of tlormal mak pe1vi.y demonstrates seminal cc~.sicles (arrows), urinary bladder (b), pelaic jut (j). in ernal obturator mr~l~ (0). and rcctrtm (R). t Striated muscles haoe loa-intensity signal; jut and medullary bone emit high-intensitly .sig,ral (c.g.. marrow jut in femoral head (F]); and cortical bone shows absence ojs’ignal. (B) Sagittal MR image (TR = 0.5 .sw. TE = 28 mscc) after transurethral resection of prostate. Wide prostatic urethra (11) and .scminal cc.viclc (arrotcj (b = bladder: R = rectum). (C) Coronal MR image (TR = 0.5 sec. TE = 28 mscc) of Iwrmul male p&is dernonstrate,s ductus dejerens (dd) and its ampulla (a). Lccator ani mu.vc1e.y (L) ure clearI!/ outlirwd by jut and abut rectlrm (R). (D) Coronal MR image (TR = 1.5 sec. TE = 28 msec) of .same pelcis (C) at ,xlighthy more posterior lcuel .shows seminal cesicles (arroahead.s) and surrounding jut (0 = internal obtrrrator mwclc).
pulse sequence intervals, the signal intensity in- due to the rapid blood flovv. The ductus def- creases. erens on all images emits signals of medium in-
Prosta tu gland tensity that increase with longer echo-delay
The homogeneous medium-intensity signal of times (TE) and longer pulse sequence intervals
the prostate can be distinguished in its relation (TR). The undescended testis within the in-
to the bladder floor, rectum, and symphysis pu- guinal canal can be easily detected on T,-
bis by combined multiplanar images. The pros- weighted imaging. On that sequence, the testis
tate, with a pencil-like rim of lower intensity is imaged with medium intensity, in contrast to
surrounding the gland, will be distinct from the the high intensity of adipose tissue.
thick symmetrical levator ani and the rectum.
Inguinal canal Material and Methods
The ductus deferens and internal spermatic Imaging techniques
vessels can be easily distinguished in the in- All MR images were obtained with a guinal canal. Vessels, particularly arteries Diasonics MT/S system with a 0.5 Tesla super- (higher velocity), are imaged with low intensity conducting magnet operating at 0.35 Tesla,
uRoI,oG1 FEBRUARY 1986 VOLUME XXVII, NUSIBER 2 93

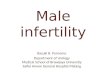
FIGURE 2. Normal vasogram shows ductus def- evens (dd), ampulla (A), seminal vesicles (ar- rowhead), and reflur into bladder.
with a resonant frequency of 15 MHz for proton imaging. The spin-echo imaging technique with various combinations of repetition times (TR), 0.5, 1 .O, 1.5, or 2.0 seconds, was used. Echo delay times (TE) of 28 and 56 msec were always obtained. Multislice image acquisition enabled 5 (TR = 0.5 set) to 20 (TR = 2.0 set) adjacent anatomic sections to be obtained. Two-dimensional Fourier transform was used to generate images with pixel shapes of 2.0 x 2.0 or 1.7 x 1.7 in a 128 x 256 matrix. The sequential slices were 7 mm thick, with a 3-mm gap between slices. The transaxial plane was used in all cases, and additional coronal and sagittal sections were obtained as necessary.
The normal pelvic anatomy imaged by MRI is seen in Figure 1 and by conventional inter- ventional radiography (vasogram) in Figure 2.
Case abstracts We used MRI to assess the pelvic anatomy of
seven men undergoing evaluation for infertility. Case 1. This twenty-six-year-old man had a
history of cystic fibrosis. Repeated semen analy- ses showed azoospermia with semen volumes less than 1 ml. On physical examination, both testes were of normal size and consistency. The left epididymis and vas felt normal. On the right, only the head of the epididymis was palpable, and there was no palpable vas. MRI revealed the absence of the right seminal vesicle and a hypoplastic left seminal vesicle (Fig. 3).
- FIGURE 3. Case 1. Transarial Ml? image (TR = 0.5 see, TE = 28 msec) demonstrates absence of right seminal vesicle and hypoplastic left seminal vesicle (arrow). (B = bladder; R = rectum; 0 = in- ternal obturator muscle; F = femoral head).
FIGURE 4. Case 2. Coronal Ml? image (TR = 1.5 set, TE = 28 msec). High-intensity signal of right vesicle (arrow) indicates presence of blood.
Case 2. This twenty-four-year-old man presented with infertility of two years’ duration and a recent history of hematospermia. Semen analysis revealed counts of 15-25 x 10e/ml with 50 per cent motility, grade 214, and morphologic findings of >70 per cent normal sperm. Numerous red and white blood cells were seen on each semen sample, but urinalysis showed only red blood cells. The prostate felt soft but nontender. MRI revealed blood in the right seminal vesicle, confirming our clinical impression of hematospermia and inflamma- tion in the seminal vesicles (Fig. 4).
94 UROLOGY i FEBRUARY 1986 / VOLUME XXVII, NUMBER 2

FIGURE 5. Case 3. (A) Seminal vesiculogram shows both right and left ductus deferens (dd) and ampulla (a). Non-filling in presence of reflux into bladder in- dicates absence or complete obstruction of seminal vesicles. (B) Transaxial MR image (TR = 1.0 set, TE = 56 msec) shows bilaterally absent seminal ves- icles (b = bladder; R = rectum;f = fat). (C) Trans- axial MR image (TR = 0.5 set, TE = 28 msec) of same patient at more caudal level shows bilateral ampullae of ductus deferens (arrows).
FIGURE 6. Case 4. (A) Unilateral vasogram demonstrates beaded vas (dd) ending in abscess cavity (ab). (B) Coronal MR image (TR = 0.5 set, TE = 56 msec) shows normal signal intensity of right seminal vesicle. Left ,seminal vesicle (arrow) is smaller and has lower intensity signal, indicating fibrosis secondary to previous infection.
UROLOCl ' FEBRUARY 1986 i VOLUMEXXVILNUMBER2 95

FIGURE 7. Case 5. (A) Coronal Ml? image (TR = 1.5 set, TE = 28 msec) of patient with hematospermia. Blood within ejaculatory duct (arrow) produces high signal intensity. Medium-intensity mass (T) is present in region of right seminal vesicle. (B) Transaxial Ml? image (TR = 2.0 set, TE = 28 msec).
Case 3. In this twenty-four-year-old man semen analysis revealed azoospermia with vol- umes of O-2-0.5 ml. Both testes were of normal size and consistency; vasa and epididymides were present and felt normal. Seminal vesicu- lography showed both the right and left ductus deferens and ampullae. Nonfilling in the pres- ence of reflux into the bladder indicated ab- sence or complete obstruction of the seminal vesicles (Fig. 5A), and MRI confirmed bilateral absence of seminal vesicles but presence of bi- lateral ampullae of the ductus deferens (Fig. 5B, C).
Case 4. This thirty-year-old man had had a right orchiectomy for tuberculous involvement. The solitary left testicle was of normal size and consistency. Unilateral vasography demon- strated a beaded vas ending in an abscess cavity (Fig. 6A). MRI revealed a small atrophic left seminal vesicle associated with a chronic abscess cavity (Fig. 6B).
Case 5. This thirty-five-year-old man re- ported repeated episodes of hematospermia. Findings on physical examination revealed a mass in the right seminal vesicle. Rectal biopsy of the lesion was consistent with schwannoma. MRI identified both the mass and the blood in the ejaculatory duct (Fig. 7).
Case 6. This twenty-year-old man pre- sented with infertility of three years’ duration. Semen analysis revealed counts of lo-20 x 106/ ml with motility of 40-60 per cent, grade 2/4, and normal morphology. A large number of red
FIGURE 8. Case 6. Coronal MR image (TR = 1.5 see, TE = 28 msec) shows large mass (T) of medium signal intensity in region of ampulla of left ductus deferens. Arrow indicates blood within ejaculatory duct.
blood cells were seen on fresh semen samples. Findings at physical examination were entirely normal. MRI demonstrated a mass in the region of the ampulla of the left ductus deferens as well as blood within the ejaculatory duct (Fig. 8).
Case 7. This thirty-two-year-old man pre- sented with infertility of two years’ duration. At age fourteen, he had received injections (pos- sibly human chorionic gonadotropin) for an
96 UROLOGY / FEBRUARY1986 i VOLUMEXXVII.NUMBER2

undescended right testicle. Repeated semen analyses revealed counts of < 1 x 10e/ml with motility of 20 per cent and grade l/4. On physi- cal examination, the solitary left testis was smaller than normal and a large left varicocele was palpable. The right testis was not palpable. MRI demonstrated the undescended testicle, measuring 2.6 x 3.8 cm, in the right inguinal canal (Fig. 9A); it was also visible on CT scan of the pelvis (Fig. 9B).
Comment
Magnetic resonance imaging is ideally suited to pelvic evaluation. The absence of ionizing ra- diation is particularly advantageous in patients of reproductive age. The very sensitive soft-tis- sue contrast resolution yields clearly visible in- terfaces between pelvic fat and the geni- tourinary organs and allows discrimination of the regional anatomy of the seminal vesicles, prostate gland, and urinary bladder. Respira- tory motion does not affect the pelvic organs, and pelvic bone and surgical clips do not create significant artifacts in MR images. Bladder dis- tention, required by ultrasound for an acoustic window, is not essential in MRI.
The ability to obtain axial, sagittal, and cor- onal sections without reformatting, as is neces- sary for computed tomography, is another ad- vantage of MRI. The acquisition of images is sensitive to hydrogen density, Tr and Tz relax- ation times, and blood flow. The inherent tissue properties (T,, T, or [ + 11) are sufficient for MRI to distinguish among various normal and abnormal tissue types.
Compared with ultrasound, MRI has better spatial resolution, provides more specific tissue characterization, and is less operator-depend- ent. MRI is not affected by the patient’s body habitus, and intestinal gas is not a problem in imaging the pelvis.
Magnetic resonance imaging has a resolution superior to that of any other imaging tech- nique. Its contrast range in soft tissue can ex- ceed 500 per cent, whereas that of computed tomography is only approximately 7 per cent.‘O
Although there are significant advantages to MRI, there are also several disadvantages. It is slow in comparison with other contempora- neous imaging modalities, and in approxi- mately 2 per cent of patients claustrophobia de- velops when passing through the scanner. MRI is difficult for very ill patients who need con- tinuous life support. Pacemakers may become unstable during scanning,‘O and there is a po-
FIGURE 9. Case 7. (A) Coronal T,-weighted MR image demonstrates testis in right inguinal region (black arrow). (Open arrow = spervnatic cord.) (B) CT Scan corroborated diagnosis.
tential hazard for individuals with ferro- magnetic prostheses or vascular clips.” Body temperature may increase during MRI scanning when the magnetic field strength is ~1.5 Tesla. In our experience with strengths up to 0.5 Tesla, no adverse biologic effects have been seen.
MRI has allowed us to evaluate our infertile patients noninvasively without exposing them to ionizing radiation. It has enabled us to visu- alize the seminal vesicles accurately and re- liably, regardless of the presence of obstruction of the ductus deferens. Hemorrhage, congenital abnormalities, tumors, and infective processes
UROLOGY i FEBRUARY 1986 / VOLUME XXVII, NUMBER 2 97

(abscesses) can be easily visualized in the pelvic secondary sexual organs. In cryptorchid pa- tients, the testis can be localized. Although MRI has great sensitivity, its specificity at present is low. However, for selected cases of male infer- tility, MRI has proved to be an excellent diagnostic aid.
Department of Urology, U-518 University of California
San Francisco, California 94143 (DR. MCCLURE)
ACKNOWLEDGMENTS. To Drs. Richard D. Amelar, Law- rence Dubin, David F! Gerstman, and A. R. Ramchan- dran for allowing us to report Case 7.
References
1. Bryan PJ, et al: NMR scanning of the pelvis: initial expe- rience with a 0.3 T system, AJR 141: 1111 (1983).
2. Hricak H, et al: Anatomy and pathology of the male pelvis by magnetic resonance imaging, ibid 141: 1101 (1983).
3. Pykett IL, et al: Principles of nuclear magnetic resonance imagine, Radiolow 143: 157 (1982).
Y Y
4. Pykett IL: NMR imaging in medicine, Scientif Am 246: 78 (1982).
5. Oldendorf WH: NMR imaging: its potential clinical impact, Hosp Pratt 17: 114 (1982).
6. Hricak H: Pelvis, in Margulis AR, Higgins CB, Kaufman L, and Crooks LE (Eds): Clinical Magnetic Resonance Imaging, San Francisco, Radiology Research and Education Foundation, chapt. 15, 1983, pp 229-250.
7. Partain CL, Price RR, Rollo FD, and James AE: Nuclear Magnetic Resonance (NMR) Imaging, Philadelphia, W.B. Saun- ders Co., 1983.
8. Margulis AR, Higgins CB, Kaufman L, and Crooks LE (Eds): Clinical Magnetic Resonance Imaging, San Francisco, Ra- diology Research and Education Foundation, 1983.
9. Kaufman L, Crooks LE, and Margulis AR (Eds): Nuclear Magnetic Resonance Imaging in Medicine, New York, Igaku- Shoin, 1981.
10. Pavlicek W, et ~2: The effects of nuclear magnetic reso- nance on patients with cardiac pacemakers, Radiology 147: 149 (1983).
11. New PFJ, et al: Potential hazards and artifacts of ferro- magnetic and nonferromagnetic surgical and dental materials and devices in nuclear magnetic resonance imaging, ibid 147: 139 (1983).
98 UROLOGY I FEBRUARY 1986 i VOLUME XXVII, NUMBER 2