Embed Size (px)
Citation preview

J. clin. Path., 1971, 24, 744-752
Malignant lymphoma of parotid associated withMikulicz disease (benign lymphoepithelial lesion)J. G. AZZOPARDI AND D. J. EVANS
From the Department of Morbid Anatomy, Royal Postgraduate Medical School, London
SYNOPSIS Benign lymphoepithelial lesion (Mikulicz disease) is generally regarded as an inflam-matory disorder of unknown aetiology, characterized by epimyoepithelial islands, and unrelated tomalignant lymphoma. Five cases have been collected which show evidence at the same site of bothMikulicz disease and a malignant lymphoma. The latter took the form of reticulum-cell sarcoma orHodgkin's disease. The two diseases were discovered simultaneously or the malignant lymphomawas detected at a subsequent date. The probable sequence of events is discussed. These cases areregarded as one of the best illustrations in man of an autoimmune disorder being followed by thedevelopment of malignant lymphoma. It is concluded that so-called benign lymphoepithelial lesionis not always innocuous and an attempt is made to establish histological criteria which might beregarded with suspicion in a particular case.
In the older literature a disorder causing enlargementof the salivary glands, in particular the parotids,was variously designated lymphomatoid adenoma(Bauer and Bauer, 1953), lymphoepithelioma (Fein,1940), solid variant of adenolymphoma (Lloyd,1946) by pathologists, and Mikulicz disease by bothclinicians and pathologists. Godwin (1952) coinedthe term 'benign lymphoepithelial lesion' because ofthe doubt that existed about the precise nature ofthe condition and suggested that the name Mikuliczdisease be dropped. Morgan and Castleman (1953)gave a detailed pathological account of this condi-tion to which little has been added since, and theyretained the eponymous designation of Mikuliczdisease. These authors stressed the importance of anepithelial proliferation affecting salivary ducts thattakes the form of epimyoepithelial islands whichwere regarded as characteristic and diagnostic of thecondition. Finding of epimyoepithelial islands cameto be regarded as diagnostic of a pathological entitywhich is benign and unrelated to malignant lym-phoma.Our purpose is to report on five patients who had
evidence of Mikulicz disease (benign lympho-epithelial lesion) and a malignant lymphoma at thesame site, either simultaneously or consecutively.
Source of Material
Two cases were found in an analysis of pathologicalmaterial from patients indexed as Mikulicz diseaseReceived for publication 18 February 1971.
at the London Hospital, one case was sent to us byProfessor R. Goudie of the Royal Infirmary,Glasgow, one was a referral to Professor C. V.Harrison from Dr A. G. Marshall of Wolver-hampton Royal Hospital, and one was a referral toDr B. Castleman at the Massachusetts GeneralHospital, Boston, USA.
CASE 1 E.C. (GLASGOW VICTORIAINFIRMARY AND ROYAL INFIRMARY)A woman aged 53 years developed painless swellingof the right parotid region and was seen at theVictoria Infirmary in 1961, at the age of 56. Unilateralparotid swelling was found, together with a dis-charge from the right ear. The swelling fluctuatedspontaneously in size. A biopsy was reported asconsistent with a diagnosis of Sj6gren's syndrome.Two years later the left parotid gland also becameenlarged. It was noted that she had had xerostomiafor some years but the eyes were normally moist.There was no arthritis and no lacrimal gland swell-ing. A left parotid sialogram showed some dilatationof the common duct and saccular dilatation of itsbranches. In 1964 there was septic infection of bothparotid glands, one of which required surgicaldrainage. Within a few months she had massivebilateral parotid enlargement with shotty nodes onthe left side of the neck. Bilateral partial parotid-ectomies were performed. At operation there wasthought to be infiltration of masseter and sterno-mastoid muscles. Enlarged cervical lymph nodeswere considered to be neoplastic. However, histology
744
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.24.8.744 on 1 Novem
ber 1971. Dow
nloaded from

Malignant lymphoma ofparotid associated with Mikulicz disease (benign lymphoepithelial lesion)
of both parotid glands was again reported as show-ing features of Sjogren's syndrome without evidenceof malignancy. The serum albumin was 2-9 g/100 ml,globulin 2-7 g/100 ml, haemoglobin 11-6 g/100 ml,and white blood cell count 3, 350/cmm. The leftparotid swelling recurred within a month of opera-tion. By April 1965 the left parotid was painful andswollen and there was pharyngeal ulceration centredaround the left tonsil; an emergency tracheostomywas performed together with a biopsy of the parotid.Following a diagnosis of reticulum-cell sarcoma, thepatient was treated with prednisolone and cyclo-phosphamide with temporary improvement. Twomonths later a nodule appeared under the angle ofthe left mandible and this was biopsied. The patientdied shortly afterwards at the age of 60. Biopsies orexcisions were carried out in 1961, 1964, April 1965,and June 1965. Necropsy was performed in 1965.
1961 Biopsy specimenThis shows histology typical of a benign lympho-epithelial lesion (Fig. 1).
1964 Excision specimenIn 1964 an excision specimen, 90 g of parotid tissuefrom the left side and 65 g from the right side, wasreceived in the laboratory. Four blocks of tissue areavailable for study. They all show the generalstructural features of benign lymphoepithelial lesion,but with a few additional features. (1) There is amarked histiocytic infiltration throughout most ofthe lymphoid background (Fig. 2). (2) In one blockthere are a few foci of necrosis on the lympho-histiocytic background. These measure up to 2 mmin diameter and are not obviously related to epithelialtissue. (3) Perhaps the most sinister feature is thepresence in one area of one block of a quite differentcytology from the rest of the tissue (Fig. 3). Hereepimyoepithelial islands are absent and, instead of alymphoid and histiocytic background, there is amass of pleomorphic reticulum cells with prominentnucleoli and numerous mitoses. We regard this focusas probable malignant lymphoma.
April 1965 biopsy specimenFour blocks of parotid and one block of lymph nodeare available for study. The parotid tissue shows areticulum-cell sarcoma with sparse remnants ofductal epithelium, including epimyoepithelial islands(Fig. 4). The node is replaced by reticulum-cellsarcoma.
June 1965 biopsy specimenTwo blocks of lymph nodes show replacement byreticulum-cell sarcoma.Necropsy (Dr W. P. Duguid at Glasgow Royal
Infirmary) showed grossly enlarged lymph nodes(some of which were necrotic) extending from theangle of the jaw to the hilum of the lungs. Thespleen (80 g), liver, and femoral bonemarrow showedno evidence of tumour.
CASE 2 P.W. (LONDON HOSPITAL)A woman aged 52 years complained of a lumpanterior to the left ear present for four years. A tenseswelling of the parotid was found on examination.This was excised and, following a diagnosis ofHodgkin's disease, she was given a course of deepx-ray therapy. Four years later she developed aswelling under the left jaw. Enlarged lymph nodeswere palpated in the posterior triangle and below theangle of the jaw. A further course of deep x-raytherapy was given. Two years later an enlarged nodewas again palpated in the neck but no treatment wasgiven. After another three years the positionappeared unchanged, haemoglobin was 14-8 g/100 ml, white blood cell and differential counts werenormal, and the erythrocyte sedimentation rate(Westergen) was 36 mm in one hour. Three yearslater the spleen was palpable and a 'small dose' ofx rays was given to the region. Her condition re-mained fairly static for about nine years. She under-went partial gastrectomy for a benign peptic ulcerand was found at this time to have atrial fibrillation.A biopsy of a cervical node was again diagnosed asHodgkin's disease. Three years later bilaterallyenlarged cervical nodes were present, larger on theleft side than the right. A lump was again palpatedat the angle of the left jaw. Enlarged axillary nodeswere now present. The spleen was palpable twofingerbreadths below the costal margin and the liverfour fingerbreadths below the costal margin. Fivemonths later the cervical nodes had enlarged con-siderably in size and a biopsy at this time wasreported as showing necrotic malignant tumour.She died 16 months later with clinical evidence ofpersistent malignant lymphoma. No necropsy wascarried out.
Biopsies were carried out in 1936, 1959, and 1962.The 1936 specimen consists of fragmented re-
sected parotid tissue. The changes can be dividedinto two: changes in the salivary parenchyma andan infiltration by malignant lymphoma. The changesin the parenchymal tissue consist of acinar atrophywith persistent salivary ducts. The ducts are in partsvirtually normal, in parts hyperplastic but with twocell layers and a central lumen still identifiable, whilein other areas there are solid epimyoepithelial isletswith varying amounts of associated 'hyaline'material (Fig. 5). In addition there is a pleomorphicinfiltration with Hodgkin tissue. Reed-Stemnbergcells are plentiful. Numerous histiocytic foci are
745
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.24.8.744 on 1 Novem
ber 1971. Dow
nloaded from

b-4
.
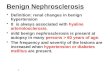
Fig. 1. Fig. 2.Fig. 1 Case 1: benign lymphoepithelial lesion with characteristic epimyoepithelial islands, acinar atrophy, andlymphoid infiltrate. Haemalum and eosin (H and E) x 150.Fig. 2 Case 1: epimyoepithelial islands on a lymphohistiocytic background. H and E. x 150.
Fig. 3. Fig. 4.Fig. 3 Case 1: focus ofpleomorphic reticulum cells from same specimen as in Figure 2. H and E. x 330.Fig. 4 Case 1: appearance offrank reticulum-cell sarcoma in parotid tissue in 1965 specimen. H and E. x 525.
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.24.8.744 on 1 Novem
ber 1971. Dow
nloaded from

Malignant lymphoma ofparotid associated with Mikulicz disease (benign lymphoepithelial lesion)
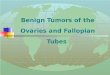
Fig. 5 Case 2: epimyoepithelial island with hyalinematerial in centre. H and E. x 330.
present and sometimes these are discrete enough toresemble miniature 'sarcoids' (Fig. 6). There is heavyinfiltration with eosinophils, with a tendency forthem to be aggregated in the histiocytic foci.
1959 biopsyThis is a lymph node with destruction of the archi-tecture and replacement by H4odgkin tissue. Histio-cytes are somewhat less conspicuous than previouslywhile plasma cells are more numerous. Typical Reed-Stemnberg cells are again present.
1962 biopsyThis shows a partially necrotic malignant lymphomawithout evidence of preexisting nodal tissue. Thereis infiltration of fibrous tissue and muscle by thepleomorphic infiltrate.
CommentThe disease ran an indolent course, the patient dying28 years after the diagnosis of Hodgkin's disease.
Fig. 6 Case 2: histiocytic aggregate forming a 'sarcoid'in the Hodgkin tissue. H and E. x 330.
CASE 3 I.B. (LONDON HOSPITAL)A woman aged 35 years at the time of the firstsurgical intervention had a swelling of the right sideof the face for three days in 1945, at the age of 25.This subsided completely and spontaneously. Thefollowing year there was a recurrence of the swellingfor a few days, with a discharge into the mouth fromthe right cheek. Two years later there was recurrentpainful swelling in the same site which lasted four tofive weeks. There was no further trouble until sixyears later when in 1954 a lump appeared in theparotid region. This persisted for five months. Onexamination there was diffuse swelling of the rightparotid with a more definite nodular swelling, 2-5 cmdiameter, at the angle of the jaw. A mass of tissue3 x 2-5 x 2 5 cm was excised from the parotid.Five years later she presented herself at OldchurchHospital, Romford, where she was referred to theradiotherapy department. A chest radiographshowed a right hilar mass. Enlarged bilateral cervicalnodes were present and a large right axillary node.
747
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.24.8.744 on 1 Novem
ber 1971. Dow
nloaded from

J. G. Azzopardi and D. J. Evans
A cervical node was biopsied. Following a diagnosisof reticulum-cell sarcoma, deep x-ray therapy wasgiven to the chest and neck, but her general condi-tion was too poor to complete the course. She diedwithin a month of presenting herself at OldchurchHospital. No necropsy was carried out.
1955 Excision specimenA mass of parotid parenchyma, 4 x 3 x 1-5 cm,which on section consists of whitish, friable nodularareas up to 0-8 cm diameter. Sections show featurestypical of a benign lymphoepithelial lesion as de-scribed by Morgan and Castleman (1953) as well ascertain unusual features. The typical features includelymphoid infiltration of salivary parenchyma thatrespects lobular boundaries, acinar atrophy, andepimyoepithelial islands (Fig. 7). In other respects,however, the lesion was not typical and was pickedout as unusual while studying a series of 10 un-selected cases indexed as 'Mikulicz disease' from theLondon Hospital. The subsequent behaviour wasnot known at the time. It differs in three essential
respects: (1) it contains large numbers of immaturecells of the lymphoid series in addition to maturelymphocytes (Fig. 8). These immature cells, con-stituting about 50% of the lymphoid cells, alearranged in anastomosing bands and clumps, oftenclearly related to the epithelial element. While thisappearance is described and illustrated by Morganand Castleman in 'Mikulicz disease', these authorsdo state that in 17 of their 18 cases mature lymphoidcells predominated. (2) There are focal areas, mainlyin the bands of immature lymphoid cells, with largenumbers of mitoses, up to five per high-power field.(3) Areas of necrosis are present in the lymphoidtissue, mainly in relation to epithelial zones. Thereis no evidence that this necrosis is related to inflam-mation in the ducts. This feature is not present inour other cases of benign lymphoepithelial lesionnor, to our knowledge, has it been noted by otherworkers. On these grounds, we regard this as at leastan unusually active variant of benign lympho-epithelial lesion, with a suspicion that incipient neo-plastic change may also be present.
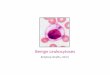
Fig. 7 Case 3: running across the top of the photo- Fig. 8 Case 3: low-power view showing broad bandsmicrograph is the edge ofa large epimyoepithelial island; ofpaler-staining immature cells between the usualthis is set in a lymphoid background. H and E. x 330. mature lymphoid infiltrate. H and E. x 110.
748
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.24.8.744 on 1 Novem
ber 1971. Dow
nloaded from

Malignant lymphoma ofparotid associated with Mikulicz disease (benign lymphoepithelial lesion)
1960 Biopsy specimenThis consists of two cervical nodes. The architectureof these is completely destroyed and replaced by areticulum-cell sarcoma with some histiocytic differen-tiation.
CASE 4 E.W. (ROYAL HOSPITAL,WOLVERHAMPTON)A woman aged 60 years complained of a painlessswelling in the left parotid region for eight years. Asuperficial parotidectomy was carried out. Investiga-tions at this time were normal. The patient presentedsix years later with a three months' history of right-sided painless parotid swelling. Examination revealeda diffusely enlarged mobile right parotid gland with-out evidence of facial palsy. On exploration, theparotid gland appeared normal but pushed forwardsby several enlarged lymph nodes at the lower andposterior margins. The nodes were biopsied and adiagnosis of Hodgkin's disease was made. The
haemoglobin was 11-7 g/100 ml but the rest of theblood count was normal. The chest radiograph wasnormal. Examination revealed a little firm swellingbelow the lobe of the left ear. One large, mobile, firmgland was palpated in the right axilla. There was noother lymphadenopathy and no splenomegaly. Shewas referred for deep x-ray therapy but failed to keepher appointment and was lost to follow-up for five-and-a-half years. In September 1967, her generalpractitioner was contacted and elicited the informa-tion that the patient still had swelling in the rightparotid region. This was said to fluctuate in sizefrom time to time and was described as the size of a'small lemon'. A few months later she was admittedto another hospital with what was now 'an enormousswelling on the right side of her face and neck'. Abiopsy was taken. She was seen at the radiotherapydepartment of the Royal Hospital where, apart froma huge soft swelling of the right parotid region, shewas found to have discrete enlarged nodes in both
Fig. 10 Case 4: higher magnification ofan epithelialFig. 9 Case 4: epimyoepithelial islands set in a mature islandfrom same specimen as in Figure 9. H and E.lymphoid background. H and E. x 140. x 330.
749
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.24.8.744 on 1 Novem
ber 1971. Dow
nloaded from

J. G. Azzopardi and D. J. Evans
Fig. 11 Case 4: Hodgkin tissue in node that alsocontains epimyoepithelial islands. H and E. x 330.
cervical chains, more marked on the right than theleft, and enlarged right axillary nodes. She was
treated with deep x-ray therapy with remission ofthe swelling. She was admitted to yet anotherhospital on 1 February 1969 with a history of leftlower chest pain, sweats, and fever. There was pro-gressive dysphagia, some epigastric pain, and weightloss. Prominent nodes were present in the rightinguinal and axillary regions but there was no
obvious recurrence in the parotid area. There was a
central tender epigastric mass and an enlarged spleen.Chest radiographs showed enlarged mediastinalnodes and clear lung fields. Barium swallow showeda deformity in the gastric fundus. It was consideredlikely that she now had extensive malignant lym-phoma. She was finally admitted to the RoyalHospital on 12 February 1969 for chemotherapy forHodgkin's disease but she died on 15 February.Unfortunately, no necropsy was carried out.
Excisions or biopsies were carried out in 1955,1962, and 1968.
Excision specimen from left parotid in 1955Parotid tissue consisted of soft enlarged lobules.The general architectural features are characteristicof benign lymphoepithelial lesion, with preservationof lobular outlines, parenchymal atrophy, conversionof ducts to epimyoepithelial islands, and a massiveinfiltration with lymphoid cells that are predomin-antly mature (Figs. 9 and 10). More detailed exam-ination, however, reveals a few unusual features. (1)Eosinophil polymorphonuclear cells, rare in ourcontrol series of benign lymphoepithelial lesion,are sprinkled through the tissue in large numbers.(2) Plasma cells, uncommon in this condition,except at the'advancing edge' of the lesion, are easilyfound. (3) Abnormal reticulum cells are present.These are sometimes sparse (1/HPF), sometimesconcentrated with as many as 20/HPF. They have acopious cytoplasm, a large usually ovoid or reniformnucleus, and between one and three nucleoli. Themost disturbing reticulum cells have a single large,eosinophilic nucleolus and a folded nucleus. Veryoccasional cells of this type with mirror-imagenuclei are present.
1962 BiopsyThree right juxtaparotid lymph nodes show destruc-tion of architecture and replacement by Hodgkintissue (Fig. 11). Mitoses are numerous. Of the threenodes, two have salivary duct inclusions. Thesehave been converted to epimyoepithelial islands. Theislands are sometimes apparently distorted intolinear streaks as if by tumour compression. Noparotid gland proper is included in the sections butthe point to be stressed is the existence side by sideof epimyoepithelial islands and of malignantlymphoma.
1968 BiopsyA lymphoid mass is divided by broad fibroustrabeculae. The lymphoid mass consists of Hodgkintissue which, compared with the previous biopsy,shows lymphocytic depletion. There is some histio-cytic proliferation but eosinophils and plasma cellsare scanty.
CommentThe illness spanned a period of 22 years. Hodgkin'sdisease was known to be present for 14 years.
CASE 5This is a brief note on a case included by courtesy ofDr B. Castleman.A woman aged 69 years complained of an asymp-
tomatic mass in the parotid gland. Hepatospleno-megaly was found on examination. Malignantlymphoma was suspected clinically. Bone marrow
750
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.24.8.744 on 1 Novem
ber 1971. Dow
nloaded from

Malignant lymphoma ofparotid associated with Mikulicz disease (benign lymphoepithelial lesion)
aspiration showed 'slight lymphocytosis' which wasnot considered diagnostic. The parotid mass wasresected. Subsequently she was found to have apositive rheumatoid factor and a serum albumin-globulin ratio of 1:1 with elevation of the fl-globulinfraction. The patient had no arthritis and no clinicalevidence of the sicca syndrome. Nine weeks afterthe first surgical operation, she was readmitted forexcision of ipsilateral enlarged cervical nodes.
Excisions were performed in August 1969 andNovember 1969. Two slides of the original materialwere sent to Dr Castleman for consultation: thesewere considered to be representative of the totalmaterial blocked. The general pattern of the parotidtissue in these slides is characteristic of benignlymphoepithelial lesion. However, on closer inspec-tion, two features deserve further comment: (1)bands of immature lymphoid cells cuff some of theepithelial islands, though they constitute a muchsmaller proportion of the total infiltrate than in case3; reticulum cells and some histiocytes are also scat-tered randomly through the infiltrate especially inone of the two slides. (2) There are two foci, thelarger 4mm in maximum diameter, in which epimyo-epithelial islands are absent and in which theinfiltrate consists mainly of reticulum cells, as seenin the 1964 specimen of case 1. The second specimenconsisted of seven lymph nodes between I and 2 cmdiameter. A section of one of these was sent to Dr B.Castleman who diagnosed Hodgkin's disease.Professor C. V. Harrison also made a diagnosis ofHodgkin's disease, of the diffuse lymphocytic andhistiocytic variety, though with capsular invasion.Both thought that, in retrospect, Hodgkin tissue wasprobably present in the first specimen also.
Discussion
Because of the confusion over nomenclature, wehave been obliged sometimes to use the term'Mikulicz disease'. It is used here in the sense of thepathological process that also goes by the name ofbenign lymphoepithelial lesion. We are not describ-ing a clinical syndrome. It is worth pointing out thatnone of our five cases had rheumatoid arthritis andtherefore none falls into the clinical category ofSjogren's syndrome. Our pathological findings, incases of Mikulicz disease, are essentially similar tothose of Morgan and Castleman (1953), but wewould stress especially the dominance of maturelymphoid elements. Bands of immature lymphoidcells, related especially to epithelial elements, are avery prominent feature of our case 3. They are de-scribed as a feature of Mikulicz disease by Castle-man, but on present evidence we reserve judgmentabout the significance of this finding.
The distinctive feature of these five patients is thatthey all had histological evidence of benign lympho-epithelial lesion, and that they also had evidence,simultaneously or at a later date, of malignantlymphoma in the same anatomical site. Since themalignant lymphoma started at the same site as theother very rare disease in all five cases, the relation-ship is clearly not fortuitous. Nor can the malignantlymphoma be attributed to radiotherapy or othertreatment, since both diseases were either presentfrom the start or else diagnosed before any radiationtherapy was given.The precise relationship of the two diseases is
complex and may not be uniform in all cases.Malignant lymphoma may have led to the develop-ment of epimyoepithelial islands in patients in whomthe two pathological processes were discoveredsimultaneously. This applies particularly to the casesof Hodgkin's disease, in which lymphocytes are con-sidered to be reactive rather than neoplastic. Thoughimpossible to exclude, we regard this as less likelythan the alternatives. The second possibility is thatMikulicz disease may progress into a malignantlymphoma or, thirdly, both diseases may be expres-sions of the same underlying host defect. This defectmight consist of mutant cells giving rise to an auto-immune process on the one hand and to malignantdisease of lymphoid tissue on the other. The conceptof a relationship between autoimmune disease andmalignant lymphoma is not a new one. Some workersbelieve that Hashimoto's disease of the thyroid iscomplicated occasionally by malignant lymphoma ofthis organ (Cox, 1964). Idiopathic steatorrhoea maybe complicated by the development of malignantlymphoma in the jejunum, though the relationshipin this case is more complex, involving ingestion of aforeign protein in the pathogenesis of the initial dis-order. Interestingly enough, reticulum cell sarcomaand Hodgkin's disease are also the two types ofmalignant lymphoma that develop in patients withidiopathic steatorrhoea. A related but complexsituation may be found also in the development ofmalignant lymphoma following the administrationof antilymphocytic sera in patients with renal trans-plants (Doll and Kinlen, 1970). In mice autoimmunehaemolytic anaemia precedes the development ofcertain malignant lymphomas (Mellors, 1966). Inthis paper we have put forward what we regard asstrong evidence of a relationship between benignlymphoepithelial lesion and malignant lymphoma.That Mikulicz disease is an autoimmune disorder isstrongly supported by clinical studies, morpho-logical patterns, and the serological evidence (BritishMedical Journal, 1967). We believe that the patientsreported on here represent one of the most convinc-ing instances of a relationship between autoimmune
751
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.24.8.744 on 1 Novem
ber 1971. Dow
nloaded from

752
disease and the subsequent development of malig-nant lymphoma in man.
Talal and Bunim (1964) and Talal, Sokoloff, andBarth (1967) described the development of reticulumcell sarcoma in distant sites in five patients withSjogren's syndrome. In none of these cases was thereany involvement of the salivary glands by malignantlymphoma, though this may be inherent in theirmethod of selection. These authors described otherextrasalivary lymphoid abnormalities in theirpatients: thest, include primary macroglobulinaemiaand a peculiar disorder which they regarded pro-visionally as a pseudolymphoma. In view of the factthat one of the latter patients had reticulosarcoma atnecropsy, we have reservations about this conceptof a pseudolymphoma.Our main purpose here is to draw attention to the
fact that epimyoepithelial islands are not necessarilyindicative of a benign pathological process. Certainlythey are usually diagnostic of specific benign diseaseprocesses that affect the salivary and certain otherglands. However, the pathological picture of benignlymphoepithelial lesion does not exclude a malignantlymphoma developing simultaneously or subse-quently in the same anatomical region. Doubtless,the majority of cases remain benign throughout*their course but equally malignant lymphoma mustbe recognized as a complication of some cases. Sinceour cases are derived from several sources it is im-possible to estimate the incidence of this complica-tion. This can only be determined from the study ofa large series with a prolonged follow up. While wecannot yet draw conclusions about the relationshipbetween our cases and the type of patient reportedon by Talal et al, we suspect that they may representdifferent aspects of a spectrum.
It would clearly be valuable if one could dis-tinguish cases of benign lymphoepithelial lesion thatwere completely innocent from those with a malig-nant potential. In one of our cases (case 2) the diag-nosis of Hodgkin's disease was fairly obvious patho-logically from the start. Interest centres chiefly onthe other four cases. In one case (case 1) there wasnothing to distinguish the original specimen from atypical benign lymphoepithelial lesion. In the otherthree cases, however, there were certain debatablefeatures that might have had a bearing on the subse-quent course. These include tracts of immaturelymphoid cells, unexplained foci of necrosis, and adiffuse or focal histiocytic reaction on the general
J. G. Azzopardi and D. J. Evans
lymphoid background. In one case eosinophil andplasma cell infiltration, together with scatteredabnormal reticulum cells, were the first indicators ofcomplicating Hodgkin's disease. In another case,paucity or absence of epimyoepithelial islands overrelatively large tracts of tissue (with their presenceelsewhere) was one of the featuresarousingsuspicion.At present we can only conclude that the finding ofthese features in a case of benign lymphoepitheliallesion may indicate a greater likelihood of the devel-opment of malignant lymphoma. On the basis ofour case 1, however, we think that probably all casesof benign lymphoepithelial lesion have a degree ofmalignant potential though the degree of risk hasstill to be determined.
We wish to thank Professor I. Doniach for allowingaccess to the London Hospital material andProfessorR. Goudie and Dr A. G. Marshall for supplyingclinicopathological data from cases 1 and 4. We areindebted to Dr B. Castleman for allowing us toinclude case 5 and for his opinion on this case. Weare grateful to Professor C. V. Harrison for hiscriticism of the manuscript. Our thanks are due alsoto the technical staff of the department of morbidanatomy and to Miss Anne Walker for secreterialhelp.
References
Bauer, W. H., and Bauer, J. D. (1953). Classification of glandulartumors of salivary glands; study of 143 cases. Arch. Path., 55,328-346.
British Medical Journal (1967). Sjogren's syndrome (Leading article).Brit. med. J., 3, 260.
Cox, M. T. (1964). Malignant lymphoma of thyroid. J. clin. Path., 17,591-601.
Doll, R., and Kinlen, L. (1970). Immunosurveillance and cancer:epidemiological evidence. Brit. med. J., 4, 420-422.
Fein, M. J. (1940). Lympho-epithelioma of the parotid gland. Amer.J. Cancer, 40, 434-440.
Godwin, J. T. (1952). Benign lymphoepithelial lesion of the parotidgland (adenolymphoma, chronic inflammation, lympho-epithelioma, lymphocytic tumor, Mikulicz disease) report ofeleven cases. Cancer (Philad.), 5, 1089-1103.
Lloyd, 0. C. (1946). Salivary adenoma and adenolymphoma. J. Path.Bact., 58, 699-710.
Mellors, R. C. (1966). Autoimmune disease in NZB/BL mice. H.Autoimmunity and malignant lymphoma. Blood, 27, 435.448.
Morgan, W. S., and Castleman, B. (1953). Clinicopathologic study ofMikulicz's disease. Amer. J. Path., 29, 471-503.
Talal, N., and Bunim, J. J. (1964). The development of malignantlymphoma in the course of Sj6gren's syndrome. Amer. J. Med.,36, 529-540.
Talal, N., Sokoloff, L., and Barth, W. F. (1967). Extrasalivary lym-phoid abnormalities in Sjogren's syndrome (reticulum cellsarcoma, 'pseudolymphoma', macroglobulinemia). Amer. J.Med., 43, 50-65.
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.24.8.744 on 1 Novem
ber 1971. Dow
nloaded from