Embed Size (px)
Citation preview

Management of Congenital TrachealStenosisSophie C. Hofferberth, MBBSa, Karen Watters, MB, BCh, BAO, MPHb, Reza Rahbar, DMD, MDb, Francis Fynn-Thompson, MDa
abstract Congenital tracheal stenosis (CTS) is a serious and rare condition. In mostcases, stenotic lesions are composed of complete tracheal rings of cartilage.The severity of symptoms correlates with the length of affected trachea, thepresence of concomitant respiratory conditions, degree of luminal narrowing,and any bronchial involvement. Critically, CTS is a disorder that can lead tolife-threatening respiratory insufficiency in children. Thus, it is a clinical entitythat demands timely diagnosis and treatment. This review will firstly discussthe anatomy and pathophysiology of CTS and outline the various clinicalpresentations associated with the disorder. In addition, methods of diagnosisand treatment strategies will be reviewed, with a focus on contemporarysurgical techniques. Finally, postoperative care of patients with CTS will bereviewed, and a contemporary multidisciplinary management approach willbe presented.
Congenital tracheal stenosis (CTS) isa rare but potentially life-threateningdisorder that often leads to severerespiratory insufficiency, particularlyin neonates and infants. The trueincidence of this complex anomaly isunknown given many infants diebefore the diagnosis is made.1 CTSrepresents a spectrum of stenoticairway lesions that are commonlycomposed of complete tracheal ringsof cartilage that vary in location,length, and severity of luminalnarrowing.1–3 The variability inclinical symptoms, diversity ofassociated cardiovascular anomalies,and scarcity of the disorder presentsignificant challenges to its timely andeffective management. The rarity andcomplexity of CTS demandsa multidisciplinary therapeuticapproach and individualized patientmanagement.4
Although a subset of infants with CTSmay outgrow their tracheal stenosisover time,2,5,6 surgical intervention isoften inevitable for symptomaticpatients. Several operative techniquesfor treating CTS have been described,
including resection with end-to-endanastomosis,7 rib cartilage grafttracheoplasty,8,9 pericardial patchtracheoplasty,5,7,10,11 and slidetracheoplasty.4,5,7,12–17 Additionally,the use of endoscopic stenting as theprimary treatment of CTS was recentlyreported.18 The purpose of this reviewis to (1) provide a comprehensiveoverview of the pathology,presentation, and treatmentindications for CTS, (2) describe theavailable therapeutic options and theiroutcomes, and (3) outlinea contemporary managementapproach for treating patients withCTS. We reviewed all articlespublished from Medline between 1964and 2014 that were identified by usingthe following search terms:“congenital tracheal stenosis,”“complete tracheal rings,”“tracheoplasty,” or “trachealmalformation.” Secondary searcheswere conducted by using the terms“trachea and diagnosis,” “trachea andimaging,” and “endotracheal stent.”The year 1964 marks the firstreported surgical repair of CTS.19
Departments of aCardiac Surgery, and bOtolaryngology,Boston Children’s Hospital, Harvard Medical School, Boston,Massachusetts
Dr Hofferberth conceptualized and designed thestudy, performed data collection, and drafted theinitial manuscript; Drs Watters and Rahbar carriedout the initial analyses, and reviewed and revisedthe manuscript; Dr Fynn-Thompson conceptualizedand designed the study, coordinated and superviseddata collection, and critically reviewed themanuscript; and all authors approved the finalmanuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-3931
DOI: 10.1542/peds.2014-3931
Accepted for publication Mar 25, 2015
Address correspondence to Francis Fynn-Thompson,MD, Department of Cardiac Surgery, BostonChildren’s Hospital, 300 Longwood Ave, Bader 273,Boston, MA 02115. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,1098-4275).
Copyright © 2015 by the American Academy ofPediatrics
FINANCIAL DISCLOSURE: The authors have indicatedthey have no financial relationships relevant to thisarticle to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors haveindicated they have no potential conflicts of interestto disclose.
STATE-OF-THE-ART REVIEW ARTICLE PEDIATRICS Volume 136, number 3, September 2015 by guest on August 19, 2018www.aappublications.org/newsDownloaded from

PATHOLOGY
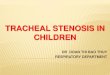
CTS is characterized by a narrowingof the tracheal lumen, mostcommonly secondary to completetracheal cartilage rings and an absentmembranous trachea. Rarely, CTS iscaused by irregular circularcartilaginous plates/ridges, ordisorganized cartilage. Cantrell andGuild19 first described CTS, applyinganatomic criteria to classify theanomaly into 3 morphologicallydistinct types: (1) generalizedhypoplasia; (2) funnel-like stenosis;and (3) segmental stenosis (Fig 1). Intype 1 CTS, the larynx is of normaldiameter, whereas the entire length oftrachea is narrowed from the cricoidto the carina. In type 2 CTS, thesubglottic tracheal diameter is ofnormal caliber; however, the tracheaprogressively narrows more distally,with the maximal point ofconstriction usually located justabove the carina. In type 3 CTS,a short (2–5 cm) segment of tracheais narrowed in an hourglass fashion.An additional classification system onthe basis of functional symptoms wasintroduced in 2003,20 classifying CTSas (1) mild–asymptomatic oroccasional symptoms; (2)moderate–respiratory symptoms,without respiratory embarrassment;and (3) severe–severe symptoms,including respiratory embarrassment.This system also includes anadditional subclassification (A or B)to indicate the presence or absence ofassociated malformations. The global
experience in managing CTS hasdemonstrated a strong correlationexists between anatomic type andfunctional category.
CTS is often associated with abnormalbronchial branching patterns.Commonly seen anomalousarborization patterns include trachealbronchus, bridging bronchus,bronchial trifurcation, and unilateralbronchial and lung agenesis. Trachealbronchus (also referred to as “pigbronchus”) is an anomaly in whichthe origin of the right upper lobebronchus is from the right lateral wallof the trachea.21 Bridging bronchus isa malformation wherein the rightmiddle and lower lobes of the lungare supplied by a horizontal bronchusarising from the left mainbronchus.22–24 Bronchial trifurcationinvolves tracheal division into 3bronchi at the level of the carina. Inchildren with unilateral lung agenesis,the trachea continues into the right orleft main bronchus, with thecontralateral bronchus being eitherabsent or severely hypoplastic.25
Isolated CTS is present in just 10% to30% of patients,13,20,26,27 instead it isfrequently associated with othercardiovascular and extrathoracicanomalies. Cardiovascular anomaliesoccur in up to 70% of patients13 andinclude pulmonary artery sling,patent ductus arteriosus, atrial septaldefect, ventricular septal defect,atrioventricular septal defect, doubleaortic arch, partial anomalouspulmonary venous connection,Tetralogy of Fallot, completetransposition of the great arteries,and tricuspid atresia.28 Thecomplexity of these associatedanomalies often complicates thediagnosis of CTS and compoundsoperative risk.29 Associatedextrathoracic congenital anomaliesinclude gastrointestinal, renal, andskeleton abnormalities, includingvertebral defects-anal atresia-cardiovascular anomalies-tracheoesophageal fistula withesophageal atresia-radial and renaldysplasia-limb defects/vertebral
defects-anal atresia-tracheoesophageal fistula withesophageal atresia-radial and renaldysplasia syndromes and anorectalmalformations.
CLINICAL PRESENTATION
The broad spectrum of stenoticlesions in CTS, ranging from short-segment tracheal narrowing tocomplete tracheobronchialhypoplasia, leads to a wide variabilityin clinical presentations. The severityof airway symptoms generallycorresponds with the degree ofairway obstruction.2 Based on thepattern and severity of symptoms, 3groups of patients with CTS can beidentified:
Minimal Symptoms/IncidentalFinding
In this group, CTS is often diagnosedincidentally, or during workup forbiphasic wheeze, a commonpresentation of mildly symptomaticpatients.30,31 Some patients with mildstenosis may remain undiagnoseduntil late childhood or earlyadolescence, when there is oftena tendency to develop exercise-associated respiratory difficulties. Forthese patients, thorough workup anddiligent monitoring is warranted todetermine an appropriatemanagement strategy.6
Symptomatic-Neonatal Period
This group of patients developsrespiratory distress within the firsthours to days of life. Presentingsymptoms include stridor, cyanoticspells or coarse cough, and assistedventilation is often required forcritical respiratory insufficiency,particularly in the setting of complexassociated cardiovascularmalformations. These patientspresent the greatest challenge forclinicians, with severe associatedcongenital anomalies and concurrentrespiratory infections often leadingthese patients to present ina critically ill state. The outcomes for
FIGURE 1Anatomic classification of CTS from Cantrelland Guild19; type 1 is generalized hypoplasia,type 2 is funnel type stenosis, and type 3 issegmental stenosis.
PEDIATRICS Volume 136, number 3, September 2015 e661 by guest on August 19, 2018www.aappublications.org/newsDownloaded from

this group reflect this; studies havedemonstrated 70% to 100%mortality in newborns with CTS whopresent in a critically ill state, withthe major prognostic factor being thepresence and severity of associatedcardiovascular anomalies.2,20,29 Thecomplexity of these patients demandsa multidisciplinary managementapproach, including appropriatecounseling of parents regarding thepotential for poor outcomes.
Symptomatic-Infancy
This cohort usually presents withrespiratory symptoms near the end ofthe first year of life, when physicalactivity increases. Symptoms ofairflow limitation, including wheeze,exertional shortness of breath, andincreased work of breathing becomeapparent. Some data suggestnonsurgical management is a feasibleoption because some children mayoutgrow their CTS2; however, evenjust a minor respiratory infection canprecipitate acute respiratory distressin these patients. Operative mortalityfor this group has been reported at16% to 20%.29 Patients with Cantrelltype 1 (generalized hypoplasia) CTSmorphology are most likely to beseverely symptomatic in theneonatal/early infancy period, andhave a high rate of associatedcardiovascular anomalies.29,32
DIAGNOSTIC EVALUATION
Several diagnostic approaches havebeen used in patients with CTS, withsome variability in practice patternsamong major referral centers.3,33 Thegold standard for definitive diagnosisof CTS is rigid laryngobronchoscopyunder general anesthesia. Directvisualization of the airway enablesaccurate assessment of the length anddiameter of the stenosed trachealsegment. Care should always be takenin performing rigid bronchoscopy; itrequires general anesthesia, andminor mucosal damage mayprecipitate edema and criticalobstruction in patients with severe
airway stenosis. Some clinicians favortracheobronchography; however, thisis not widely used due to risk ofinducing mucosal edema and causingrespiratory decompensation.34 Othershave advocated the use of virtualendoscopy to evaluate post stenosisbronchi and distal airway anatomy inpatients with extreme airwaynarrowing. This approach uses high-resolution multirow detectorcomputed tomography (CT) scanningto obtain high-resolution 3-dimensional endoluminal images tothe level of the segmental bronchi.35
Contrast chest CT scans with 3-dimensional reconstruction is widelyused to delineate major thoracicvessel and airway anatomy. However,this modality frequentlyunderestimates the degree and lengthof airway narrowing, and henceshould be used as an adjunctiveinvestigative tool only.29 MRI hasbeen demonstrated to be an effectiveand noninvasive imaging modality todelineate associated intracardiac andvascular anomalies in patients withCTS. However, the clinicalcharacteristics of the CTS patientpopulation often limits its utility;general anesthesia is often requiredto obtain an MRI in an infant or child,and patients with severe CTS arefrequently intubated beforeundergoing investigations, therebylimiting accurate imaging of thenative airway. Echocardiography is animportant tool to exclude associatedcardiac malformations. The clinicalpractices of major internationalreferral centers have evolved to nowinclude echocardiography in thediagnostic workup of all patientspresenting with suspected CTS.13,33
Figure 2 outlines a diagnosticalgorithm for the investigation ofpediatric patients presenting withsymptoms concerning for CTS.
THERAPEUTIC APPROACHES ANDTREATMENT INDICATIONS
CTS is a complex disease processthat demands a multidisciplinary
therapeutic approach tosuccessfully meet the diverse needsof a complicated patientpopulation.3,34,36 The contemporarymanagement of CTS at majortertiary centers involves anintegrated, multidisciplinary teamapproach with expertise incardiothoracic surgery,otolaryngology, cardiology,pulmonology, andanesthesiology.13,25,33 An importantconsideration is that inappropriateor untimely intervention haspotential to precipitate a criticalairway event in patients with CTS.This further emphasizes theimportance of treating patients withCTS in a specialized,multidisciplinary center with theexpertise and resources to deal withsuch a complication. Nevertheless,in the event that a child doespresent to an underresourcedcenter with critical airway stenosis,extracorporeal membraneoxygenation support presentsa suitable option as a bridgetherapy. This strategy enables initialstabilization of the patient andfacilitates transfer toa multidisciplinary center where thechild can undergo definitive repairof his or her airway lesion.
Selection of an appropriate treatmentstrategy depends on the following:(1) the patient’s clinical status, (2) theseverity and extent of the trachealstenosis, and (3) the presence ofassociated congenital anomalies.20
Elliot et al3 described 4 keycomponents that indicate the severityof CTS: (1) narrowness of the trachea;(2) extent of tracheal involvement;(3) bronchial involvement; and (4)the presence or absence of completetracheal rings.
Until the 1980s, CTS was managedconservatively, with only a fewgroups reporting success withsurgical intervention.19,37,38 The pooroutcomes associated with earlyattempts at surgical repair led toa general consensus that CTS was not
e662 HOFFERBERTH et al by guest on August 19, 2018www.aappublications.org/newsDownloaded from

amenable to operative repair; instead,many clinicians employed palliativestrategies such as tracheostomy totreat CTS.26 There are some data tosupport the implementation ofa conservative management strategyin a subset of patients with CTS whohave been demonstrated to outgrowtheir tracheal stenosis by the age of7 to 9 years.2 However, it isimperative that careful long-termclinical monitoring is employed,given a significant number of thesepatients will eventually requiresurgical intervention to treatworsening symptoms.2,6,20 Recently,the use of endotracheal stents as theprimary treatment modality wasreported in 5 patients with CTS;however, only modest outcomeswere reported, with excessivegranulation tissue formation andrestenosis being major long-termcomplications.18 Nevertheless, theutility of adjunctive tracheal stenting
to manage residual stenosispostsurgical intervention has beenwidely demonstrated.5,13,33,39,40
Indications for surgery are primarilybased on functional status,20 wherebyany patient presenting withsignificant respiratory symptomsgenerally meets the criteria foroperative intervention. Anycombination of the followingsymptoms may be exhibited:persistent wheeze, dyspnea, repeatedrespiratory infections refractory tomedical therapy, failure to wean fromventilator support, or unsuccessfulventilator support. A pediatric patientcan typically tolerate up to 50%narrowing of the tracheal diameterbefore developing significantrespiratory symptoms20; therefore,overt respiratory symptoms are animportant indicator for surgery.Although some early studies basedtheir management approach solely on
the degree of tracheal stenosis,41–43
the contemporary surgical treatmentparadigm for CTS is fundamentallybased on the clinical status of eachindividual patient.
SURGICAL TECHNIQUES AND OUTCOMES
Cantrell and Guild19 reported the firstsuccessful surgical repair of CTS in1964 when they performed resectionof a bridging bronchus with side-to-side anastomosis. The use of trachealresection and primary anastomosiswas further explored by Carcassonneet al44 in 1973, and others into theearly1980s.31,45,46 However, thisprocedure was found to beunsuccessful in treating patients withlong-segment CTS. In response,Kimura et al8 implemented a trachealgraft technique to widen the airwaydiameter. Since then, numeroussurgical reconstructive techniqueshave been described for CTS(Table 1). Current surgical optionsinclude the following: (1) resectionand primary anastomosis; (2) patchtracheoplasty with nontrachealautologous tissue (costal cartilage,pericardium); (3) slide tracheoplasty;and (4) tracheal transplant withcadaveric tracheal homograft.47–49
Only the most frequently usedtechniques are described here.
Resection and Primary Anastomosis
Primary resection of the stenosedtracheal segment and primaryreconstruction by end-to-endanastomosis is a suitable operativechoice for patients with short-segment CTS (Cantrell type 3;Fig 3).40,44,50–52 Theoretically, thistechnique maintains a normaltracheal diameter; however,anastomotic tension may causesutures to cut through, leading tofibrosis, scarring, and the potentialfor recurrent stenosis. Nevertheless,a number of reported series havedemonstrated excellent outcomesusing tracheal resection in selectedpatients with short segment trachealstenosis.40,53,54 A global mortality
FIGURE 2Proposed diagnostic workup for a child presenting with symptoms suggestive of CTS. LPA, leftpulmonary artery.
PEDIATRICS Volume 136, number 3, September 2015 e663 by guest on August 19, 2018www.aappublications.org/newsDownloaded from

rate of less than 9% has beenreported for patients who haveundergone primary resection andanastomosis, demonstrating thefeasibility of this operative strategyfor patients with short segment CTS.
Patch Tracheoplasty
Rib Cartilage Tracheoplasty
In 1982, Kimura et al8 reported thefirst successful repair of long segmentCTS by using rib cartilagetracheoplasty in a 12-month-oldchild. Their technique consisted ofreconstruction of the anteriortracheal wall by using 2 pieces ofcostal cartilage and was subsequentlyperformed successfully in othercenters.55,56 Jaquiss et al57 reportedfavorable outcomes in their series of6 patients with CTS who underwentanterior tracheal reconstruction byusing rib cartilage as theaugmentation patch, reporting 1 caseof graft dehiscence, and no deaths at4.5 years follow-up. Despite a numberof small series reporting satisfactoryearly outcomes,58–60 several seriouscomplications were observed inpatients treated with this technique.Complications included anastomoticleakage, necrosis, granulation tissueformation, and recurrent stenosis atthe suture line. DeLorimier et al50
observed excessive granulation tissueformation when using rib cartilage
graft $30% of the airwaycircumference. Furthermore, ribcartilage tracheoplasty was shown tobe associated with high rates ofreintervention for residual trachealstenosis, and a high late mortalityrate secondary to airwaycomplications.61
Pericardial Patch Tracheoplasty
Idriss et al62 were the first to reportthe use of pericardial patchtracheoplasty in 5 patients with CTS.To perform this repair,cardiopulmonary bypass (CPB) isinitiated, then a vertical incision ismade into the stenosed trachealsegment, and a patch of harvestedautologous pericardium is sutured inplace. The final step is suspension ofthe patch to surrounding mediastinalstructures to prevent collapse intothe tracheal lumen. Advantages of thistechnique include the following:pliability of the pericardial patch,minimal dissection to expose theanterior tracheal surface, andestablishment of an airtight sutureline. Bando et al63 observed normaltracheal growth and epithelialdevelopment in the follow-up of 12patients with CTS who underwentpericardial patch tracheoplasty.However, a major drawback of thistechnique is the formation ofexcessive granulation tissue arising
from the devascularized surface ofthe pericardial patch. This frequentlyrequires multiple bronchoscopicdebridement procedures to removeexcessive granulation tissue andenable reepithelialization tooccur.62–66
To date, the most robust data on thepericardial patch tracheoplastytechnique is derived from 2 series.Firstly, in 2001, Backer et al40
reviewed their long-term outcomesby using pericardial patchtracheoplasty to treat CTS. In theirseries of 28 patients, the meanpostoperative length of stay was 60days and there were 3 (6%) earlydeaths. Seven (25%) patientsrequired reoperation or endoscopicstenting for residual tracheal stenosisand there were 5 (18%) late deaths.40
More recently, Fanous et al10
reported their long-term outcomesutilizing pericardial patchtracheoplasty in 26 patients with CTS.They reported 3 (11%) in-hospitaldeaths, whereas only 2 (9%) patientsrequired late airway reintervention.All other survivors remainedasymptomatic at a median follow-upof 11 years.
Slide Tracheoplasty
Tsang and Goldstraw17 first proposeda technique termed “slidetracheoplasty” in 1989. This
TABLE 1 Historical Outcomes of Surgical Techniques Used in Repair of CTS
Source No. of Patients Surgical Technique Age, mo Associated CardiovascularDefects (%)
Deaths (%) Survivors/Late AirwayReintervention
Length ofFollow-up, mo
Andrews et al 199477 15 Pericardial patch 7.7 5 (33) 7 (47) 8/5 19Bando et al63 12 Pericardial patch 6.7 8 (67) 1 (8) 10/2 66Kamata et al59 11 Costal cartilage patch 5.1 7 (64) 5 (45) 6/3 7Backer et al40 28 Pericardial patch 6.5 8 (29) 7 (25) 21/6 131
12 Tracheal autograft 4.5 2 (17) 1 (8) 11/4 318 Tracheal resection 4 0 0 8/0 392 Slide tracheoplasty 5 1 (50) 1 (50) 1/0 48
Grillo et al14 8 Slide tracheoplasty 84 5 (63) 0 8/1 70.63 Tracheal resection 6 1 (33) 0 3/1 54
Tsugawa et al61 12 Costal cartilage patch 6.9 7 (58) 4 (25) 8/3 14417 Slide tracheoplasty 10.5 15 (88) 4 (24) 13/6 25
Li et al16 14 Slide tracheoplasty 2.4 10 (71) 2 (14) 12/4 40Manning et al33 80 Slide tracheoplasty 8.7 24 (60) 4 (5) 76/23 12Antón-Pacheco et al 39 14 Slide tracheoplasty 8.7 9 (64) 0 14/3 75Chung et al 201478 18 Slide tracheoplasty 2.5 13 (72) 1 (6) 17/4 17Butler et al13 101 Slide Tracheoplasty 5.8 72 (71) 12 (11) 89/45 55
Inclusion criteria: $10 patients in a reported series.
e664 HOFFERBERTH et al by guest on August 19, 2018www.aappublications.org/newsDownloaded from

operation was initially performed in 2infants with funnel-shaped trachealstenosis; 1 died secondary topulmonary infections, the other hada patent airway at 9 years postrepair. A subsequent series of 4patients was reported by Grillo,30
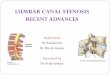
who augmented the technique toestablish the contemporary slidetracheoplasty operation. In thisprocedure, the trachea is dividedhorizontally at the midpoint of thestenotic segment. The upper stenoticsegment is incised verticallyposteriorly, and the lower segment isincised anteriorly for the full lengthof the stenosis. The right-angledcorners produced by these divisionsare trimmed above and below, andthe 2 ends are then slid over eachother (Fig 4). The circumference ofthe stenosed segment is doubled,resulting in a quadrupled cross-sectional area.30 Further, the stenoticsegment is foreshortened only halfits length, thereby reducinganastomotic tension. A potentialpitfall is the risk of injuring vitalstructures (recurrent laryngealnerve, esophagus, pulmonaryvessels) due to the extensivedissection and reconstruction that isrequired.
Slide tracheoplasty has severaladvantages: (1) less risk ofendoluminal granuloma formation;blood supply is preserved and therepair utilizes native trachealcartilage lined with ciliatedepithelium. This enables shorterpostoperative intubation periods and
fewer bronchoscopicreinterventions13,33; (2) satisfactorytracheal growth post repair14,67; (3)the technique is not limited by lengthof tracheal stenosis68,69; (4) lowincidence of anastomotic problems,including leakage, mediastinitis,fibrosis, or recurrent stenosis13,14,33;and (5) a modified slide tracheoplastycan be successfully performed in alltypes of long-segment CTS, includingpatients with bronchial stenosis andtracheal bronchus anomalies.12,70
Numerous recent reportsdemonstrate slide tracheoplasty haslower mortality and postoperativeairway complication rates comparedwith other techniques.13,33 In a seriesof 80 patients, Manning et al33
reported 4 deaths (5%) and airwayreintervention in 23 (29%) patientsat 12 months follow-up. Butler et al13
performed slide tracheoplasty in 101consecutive patients; overall, 12(12%) deaths occurred, with 45(44%) patients requiring trachealballoon dilatation and 22 (21%)undergoing tracheal stenting postinitial repair.
CPB AND MANAGEMENT OFASSOCIATED CARDIOVASCULARANOMALIES
Contemporary surgical managementof CTS involves a median sternotomy
approach and the use of CPB.13,33 Forpatients undergoing isolated trachealsurgery, single venous cannulationand normothermic CPB is a favoredapproach.33 Associatedcardiovascular anomalies are mostcommonly repaired during the sameprocedure, typically before thetracheal repair. A frequentlyencountered concomitantcardiovascular anomaly is pulmonaryartery sling. Patients with thisanomaly usually undergo trachealrepair on CPB, followed bytransection of the left pulmonaryartery, relocation of the vesselanterior to the trachea, andreimplanted onto the mainpulmonary artery. For associatedintracardiac lesions, bicavalcannulation, moderate hypothermia,and cardioplegic arrest are surgicaltechniques that may be indicateddepending on the specific cardiacanomalies being repaired.13,33,40
POSTOPERATIVE CARE
The extreme heterogeneity andcomplexity of the CTS patientpopulation presents difficultmanagement challenges for clinicians.The standard of care for has evolvedto an integrated, multidisciplinaryteam-based approach.33,39
Multidisciplinary, team-based care
FIGURE 3Examples of short segment (A, distal trachea;B, proximal trachea) CTS treated by using theresection and primary anastomosis techniqueby using running suture.
FIGURE 4Slide tracheoplasty technique. A, Extent of stenosed trachea is identified. Stenotic segment is dividedtransversely in its midpoint. The upper stenotic segment is incised vertically posteriorly and thelower segment is incised anteriorly for the full length of stenosis. B, Right-angled corners producedby these divisions are trimmed above and below. C, The 2 ends are slid together after placement ofrunning sutures around the entire oblique circumference of the tracheoplasty. D and E, The trachealcircumference is doubled, resulting in quadrupled cross-sectional area.
PEDIATRICS Volume 136, number 3, September 2015 e665 by guest on August 19, 2018www.aappublications.org/newsDownloaded from

has significantly improvedperioperative outcomes in patientswith CTS, reducing the duration of
mechanical ventilation, and length ofICU and hospital stay.4 Severalcenters have evolved their
postoperative management to favorearlier extubation of patients withCTS. Many perform bedside fiberoptic
FIGURE 5Postoperative management protocol for CTS. CICU, cardiac intensive care unit; ORL, otolaryngology.
e666 HOFFERBERTH et al by guest on August 19, 2018www.aappublications.org/newsDownloaded from

bronchoscopy at 24 to 48 hourspostsurgery to facilitate earlier weanfrom mechanical ventilation.13,33
Currently, no established protocolexists for postoperative management.Herein is a multidisciplinarymanagement algorithm to help guidepostoperative care (Fig 5) of patientswith CTS. Major postoperative airwaycomplications include anastomoticbreakdown with subsequent air leak,tracheal narrowing secondary toexcessive granulation tissueformation or restenosis at the sutureline.
Post discharge, any child presentingwith symptoms of airway narrowingshould undergo evaluation withdirect laryngoscopy andbronchoscopy. If significant trachealrestenosis is present, rigidbronchoscopic balloon dilatation ofthe stenosed segment is performed.In children who develop excessivegranulation tissue at the anastomoticsite, local steroid injection has beensomewhat effective in reducingfurther granulation tissue andstenosis. The role of topicalapplication of mitomycin-C continuesto be evaluated.71,72 Moreover, recentstudies have demonstrated thatinhaled budesonide can also besuccessful in treating patients whodevelop excessive trachealgranulation tissue post CTSrepair.73,74
CONCLUSIONS
CTS is an important pediatricanomaly that often presents as a life-threatening emergency. Timely andeffective treatment of CTS is oftenchallenging due to the diversity ofclinical presentations, complexassociated anomalies, and rarity ofthe disorder. Optimal outcomes areachieved by managing patients withCTS in specialized centers that havea focused interest andmultidisciplinary expertise. Slidetracheoplasty is now recognized asthe procedure of choice, irrespectiveof airway anatomy and length of
tracheal stenosis, whereas segmentalresection and anastomosis is a viabletreatment option in the subset ofpatients with CTS with discreet,short-segment stenosis. Postoperativeairway stenosis is routinely managedby using endoscopic balloondilatation techniques. Trachealstenting may also be used as anadjuvant therapy, yet this strategycarries its own additional morbidityand is currently only used as salvageprocedure. Nevertheless, trachealstenting shows promise to becomea more feasible adjunctive therapy,with recent reports demonstratingnovel new technologies, such asbioabsorbable materials75 and 3-dimensional printer deriveddevices,76 can be used to designairway stents that are anatomicallyspecific for a given patient.
ABBREVIATIONS
CPB: cardiopulmonary bypassCTS: congenital tracheal stenosis
REFERENCES
1. Herrera P, Caldarone C, Forte V, et al. Thecurrent state of congenital trachealstenosis. Pediatr Surg Int. 2007;23(11):1033–1044
2. Cheng W, Manson DE, Forte V, et al. Therole of conservative management incongenital tracheal stenosis: anevidence-based long-term follow-upstudy. J Pediatr Surg. 2006;41(7):1203–1207
3. Elliott M, Roebuck D, Noctor C, et al. Themanagement of congenital trachealstenosis. Int J Pediatr Otorhinolaryngol.2003;67(suppl 1):S183–S192
4. Kocyildirim E, Kanani M, Roebuck D, et al.Long-segment tracheal stenosis: slidetracheoplasty and a multidisciplinaryapproach improve outcomes and reducecosts. J Thorac Cardiovasc Surg. 2004;128(6):876–882
5. Antón-Pacheco JL, Cano I, Comas J, et al.Management of congenital trachealstenosis in infancy. Eur J CardiothoracSurg. 2006;29(6):991–996
6. Rutter MJ, Willging JP, Cotton RT.Nonoperative management of completetracheal rings. Arch Otolaryngol HeadNeck Surg. 2004;130(4):450–452
7. Backer CL, Mavroudis C, Holinger LD.Repair of congenital tracheal stenosis.Semin Thorac Cardiovasc Surg PediatrCard Surg Annu. 2002;5:173–186
8. Kimura K, Mukohara N, Tsugawa C, et al.Tracheoplasty for congenital stenosis ofthe entire trachea. J Pediatr Surg. 1982;17(6):869–871
9. Tsugawa C, Kimura K, Muraji T, NishijimaE, Matsumoto Y, Murata H. Congenitalstenosis involving a long segment of thetrachea: further experience inreconstructive surgery. J Pediatr Surg.1988;23(5):471–475
10. Fanous N, Husain SA, Ruzmetov M,Rodefeld MD, Turrentine MW, Brown JW.Anterior pericardial tracheoplasty forlong-segment tracheal stenosis: long-term outcomes. J Thorac CardiovascSurg. 2010;139(1):18–23, discussion23–25
11. Hazekamp MG, Koolbergen DR, Kersten J,Peper J, de Mol B, König-Jung A.Pediatric tracheal reconstruction withpericardial patch and strips ofautologous cartilage. Eur J CardiothoracSurg. 2009;36(2):344–351, discussion 351
12. Beierlein W, Elliott MJ. Variations in thetechnique of slide tracheoplasty torepair complex forms of long-segmentcongenital tracheal stenoses. Ann ThoracSurg. 2006;82(4):1540–1542
13. Butler CR, Speggiorin S, Rijnberg FM,et al. Outcomes of slide tracheoplasty in101 children: a 17-year single-centerexperience. J Thorac Cardiovasc Surg.2014;147(6):1783–1789
14. Grillo HC, Wright CD, Vlahakes GJ,MacGillivray TE. Management ofcongenital tracheal stenosis by means ofslide tracheoplasty or resection andreconstruction, with long-term follow-upof growth after slide tracheoplasty. JThorac Cardiovasc Surg. 2002;123(1):145–152
15. Lang FJ, Hurni M, Monnier P. Long-segment congenital tracheal stenosis:treatment by slide-tracheoplasty. JPediatr Surg. 1999;34(8):1216–1222
16. Li X, Cheng LC, Cheung YF, Lun KS, ChauKT, Chiu SW. Management of symptomaticcongenital tracheal stenosis in neonates
PEDIATRICS Volume 136, number 3, September 2015 e667 by guest on August 19, 2018www.aappublications.org/newsDownloaded from

and infants by slide tracheoplasty: a 7-year single institution experience. Eur JCardiothorac Surg. 2010;38(5):609–614
17. Tsang V, Murday A, Gillbe C, Goldstraw P.Slide tracheoplasty for congenital funnel-shaped tracheal stenosis. Ann ThoracSurg. 1989;48(5):632–635
18. Maeda K, Ono S, Tazuke Y, Baba K. Long-term outcomes of congenital trachealstenosis treated by metallic airwaystenting. J Pediatr Surg. 2013;48(2):293–296
19. Cantrell JR, Guild HG. CongenitalStenosis of the Trachea. Am J Surg. 1964;108:297–305
20. Antón-Pacheco JL, Cano I, García A,Martínez A, Cuadros J, Berchi FJ.Patterns of management of congenitaltracheal stenosis. J Pediatr Surg. 2003;38(10):1452–1458
21. McLaughlin FJ, Strieder DJ, Harris GB,Vawter GP, Eraklis AJ. Tracheal bronchus:association with respiratory morbidity inchildhood. J Pediatr. 1985;106(5):751–755
22. Gonzalez-Crussi F, Padilla LM, Miller JK,Grosfeld JL. “Bridging bronchus.” Apreviously undescribed airway anomaly.Am J Dis Child. 1976;130(9):1015–1018
23. Rishavy TJ, Goretsky MJ, Langenburg SE,Klein MD. Anterior bridging bronchus.Pediatr Pulmonol. 2003;35(1):70–72
24. Topcu S, Liman ST, Sarisoy HT, BabaogluA, Ozker E. Stenotic bridging bronchus:a very rare entity. J Thorac CardiovascSurg. 2006;131(5):1200–1201
25. Speggiorin S, Torre M, Roebuck DJ,McLaren CA, Elliott MJ. A newmorphologic classification of congenitaltracheobronchial stenosis. Ann ThoracSurg. 2012;93(3):958–961
26. Benjamin B, Pitkin J, Cohen D. Congenitaltracheal stenosis. Ann Otol RhinolLaryngol. 1981;90(4 pt 1):364–371
27. Heimansohn DA, Kesler KA, TurrentineMW, et al. Anterior pericardialtracheoplasty for congenital trachealstenosis. J Thorac Cardiovasc Surg.1991;102(5):710–715, discussion 715–716
28. Yamaguchi M, Oshima Y, Hosokawa Y,et al. Concomitant repair of congenitaltracheal stenosis and complex cardiacanomaly in small children. J ThoracCardiovasc Surg. 1990;100(2):181–187
29. Chiu PP, Kim PC. Prognostic factors in thesurgical treatment of congenital tracheal
stenosis: a multicenter analysis of theliterature. J Pediatr Surg. 2006;41(1):221–225, discussion 221–225
30. Grillo HC. Slide tracheoplasty for long-segment congenital tracheal stenosis.Ann Thorac Surg. 1994;58(3):613–619,discussion 619–621
31. Grillo HC, Zannini P. Management ofobstructive tracheal disease in children.J Pediatr Surg. 1984;19(4):414–416
32. Backer CL, Mavroudis C, Dunham ME,Holinger LD. Repair of congenitaltracheal stenosis with a free trachealautograft. J Thorac Cardiovasc Surg.1998;115(4):869–874
33. Manning PB, Rutter MJ, Lisec A, Gupta R,Marino BS. One slide fits all: theversatility of slide tracheoplasty withcardiopulmonary bypass support forairway reconstruction in children. JThorac Cardiovasc Surg. 2011;141(1):155–161
34. Loeff DS, Filler RM, Vinograd I, et al.Congenital tracheal stenosis: a review of22 patients from 1965 to 1987. J PediatrSurg. 1988;23(8):744–748
35. Hoppe H, Dinkel HP, Walder B, von AllmenG, Gugger M, Vock P. Grading airwaystenosis down to the segmental levelusing virtual bronchoscopy. Chest. 2004;125(2):704–711
36. Matúte JA, Romero R, Garcia-Casillas MA,et al. Surgical approach to funnel-shaped congenital tracheal stenosis. JPediatr Surg. 2001;36(2):320–323
37. Harrison MR, Heldt GP, Brasch RC, deLorimier AA, Gregory GA. Resection ofdistal tracheal stenosis in a baby withagenesis of the lung. J Pediatr Surg.1980;15(6):938–943
38. Kleinhaus S, Winslow PR, Sheran M,Boley SJ. Evolution of individualizedmanagement of tracheal obstruction. JPediatr Surg. 1978;13(6D):669–676
39. Antón-Pacheco JL, Comas JV, Luna C,et al. Treatment strategies in themanagement of severe complicationsfollowing slide tracheoplasty in children.Eur J Cardiothorac Surg. 2014;46(2):280–285, discussion 285
40. Backer CL, Mavroudis C, Gerber ME,Holinger LD. Tracheal surgery inchildren: an 18-year review of fourtechniques. Eur J Cardiothorac Surg.2001;19(6):777–784
41. Effmann EL, Fram EK, Vock P, Kirks DR.Tracheal cross-sectional area inchildren: CT determination. Radiology.1983;149(1):137–140
42. Minato N, Itoh K, Ohkawa Y, et al.[Treatment of congenital trachealstenosis. Retrospective study of thirteencases]. Nippon Geka Gakkai Zasshi. 1989;90(3):434–439
43. Terada M, Hotoda K, Toma M, Hirobe S,Kamagata S. Surgical management ofcongenital tracheal stenosis. Gen ThoracCardiovasc Surg. 2009;57(4):175–183
44. Carcassonne M, Dor V, Aubert J,Kreitman P. Tracheal resection withprimary anastomosis in children. JPediatr Surg. 1973;8(1):1–8
45. Mansfield PB. Tracheal resection ininfancy. J Pediatr Surg. 1980;15(1):79–81
46. Nakayama DK, Harrison MR, de LorimierAA, Brasch RC, Fishman NH.Reconstructive surgery for obstructinglesions of the intrathoracic trachea ininfants and small children. J PediatrSurg. 1982;17(6):854–868
47. Jacobs JP, Elliott MJ, Haw MP, Bailey CM,Herberhold C. Pediatric trachealhomograft reconstruction: a novelapproach to complex tracheal stenosesin children. J Thorac Cardiovasc Surg.1996;112(6):1549–1558, discussion1559–1560
48. Jacobs JP, Quintessenza JA, Andrews T,et al. Tracheal allograft reconstruction:the total North American and worldwidepediatric experiences. Ann ThoracSurg. 1999;68(3):1043–1051, discussion1052
49. Messineo A, Filler RM, Bahoric A, SmithCR. Repair of long tracheal defects withcryopreserved cartilaginous allografts. JPediatr Surg. 1992;27(8):1131–1134,discussion 1134–1135
50. deLorimier AA, Harrison MR, Hardy K,Howell LJ, Adzick NS. Tracheobronchialobstructions in infants and children.Experience with 45 cases. Ann Surg.1990;212(3):277–289
51. Grillo HC. Tracheal reconstruction.Indications and techniques. ArchOtolaryngol. 1972;96(1):31–39
52. Salzer GM, Hartl H, Wurnig P. Treatmentof tracheal stenoses by resection ininfancy and early childhood. ProgPediatr Surg. 1987;21:72–75
e668 HOFFERBERTH et al by guest on August 19, 2018www.aappublications.org/newsDownloaded from

53. Cotter CS, Jones DT, Nuss RC, Jonas R.Management of distal tracheal stenosis.Arch Otolaryngol Head Neck Surg. 1999;125(3):325–328
54. Jonas RA, Spevak PJ, McGill T, CastanedaAR. Pulmonary artery sling: primaryrepair by tracheal resection in infancy. JThorac Cardiovasc Surg. 1989;97(4):548–550
55. Campbell DN, Lilly JR. Surgery for totalcongenital tracheal stenosis. J PediatrSurg. 1986;21(11):934–935
56. Saad SA, Falla A. Management ofintractable and extensive trachealstenosis by implantation of cartilagegraft. J Pediatr Surg. 1983;18(4):472–474
57. Jaquiss RD, Lusk RP, Spray TL,Huddleston CB. Repair of long-segmenttracheal stenosis in infancy. J ThoracCardiovasc Surg. 1995;110(5):1504–1511,discussion 1511–1512
58. Forsen JW Jr, Lusk RP, Huddleston CB.Costal cartilage tracheoplasty forcongenital long-segment trachealstenosis. Arch Otolaryngol Head NeckSurg. 2002;128(10):1165–1171
59. Kamata S, Usui N, Ishikawa S, et al.Experience in tracheobronchialreconstruction with a costal cartilagegraft for congenital tracheal stenosis. JPediatr Surg. 1997;32(1):54–57
60. Lobe TE, Hayden CK, Nicolas D,Richardson CJ. Successful managementof congenital tracheal stenosis ininfancy. J Pediatr Surg. 1987;22(12):1137–1142
61. Tsugawa C, Nishijima E, Muraji T, et al.Tracheoplasty for long segmentcongenital tracheal stenosis: analysis of29 patients over two decades. J PediatrSurg. 2003;38(12):1703–1706
62. Idriss FS, DeLeon SY, Ilbawi MN, GersonCR, Tucker GF, Holinger L. Tracheoplastywith pericardial patch for extensivetracheal stenosis in infants and children.J Thorac Cardiovasc Surg. 1984;88(4):527–536
63. Bando K, Turrentine MW, Sun K, et al.Anterior pericardial tracheoplasty forcongenital tracheal stenosis:intermediate to long-term outcomes. AnnThorac Surg. 1996;62(4):981–989
64. Cosentino CM, Backer CL, Idriss FS,Holinger LD, Gerson CR, Mavroudis C.Pericardial patch tracheoplasty forsevere tracheal stenosis in children:intermediate results. J Pediatr Surg.1991;26(8):879–884, discussion 885
65. Dunham ME, Holinger LD, Backer CL,Mavroudis C. Management of severecongenital tracheal stenosis. Ann OtolRhinol Laryngol. 1994;103(5 pt 1):351–356
66. Kim HK, Kim YT, Sung SW, et al.Management of congenital trachealstenosis. Eur J Cardiothorac Surg. 2004;25(6):1065–1071
67. Manson D, Filler R, Gordon R. Trachealgrowth in congenital tracheal stenosis.Pediatr Radiol. 1996;26(6):427–430
68. Acosta AC, Albanese CT, Farmer DL,Sydorak R, Danzer E, Harrison MR.Tracheal stenosis: the long and the shortof it. J Pediatr Surg. 2000;35(11):1612–1616
69. Macchiarini P, Dulmet E, de MontprevilleV, Mazmanian GM, Chapelier A, DartevelleP. Tracheal growth after slidetracheoplasty. J Thorac Cardiovasc Surg.1997;113(3):558–566
70. Garabédian EN, Le Bret E, Corré A, et al.Tracheal resection associated with slide
tracheoplasty for long-segmentcongenital tracheal stenosis involvingthe carina. J Thorac Cardiovasc Surg.2001;121(2):393–395
71. Rahbar R, Shapshay SM, Healy GB.Mitomycin: effects on laryngeal andtracheal stenosis, benefits, andcomplications. Ann Otol Rhinol Laryngol.2001;110(1):1–6
72. Simpson CB, James JC. The efficacy ofmitomycin-C in the treatment oflaryngotracheal stenosis. Laryngoscope.2006;116(10):1923–1925
73. Airway Reconstruction Team. Recentchallenges in the management ofcongenital tracheal stenosis: anindividualized approach. J Pediatr Surg.2005;40(5):774–780
74. Yokoi A, Nakao M, Bitoh Y, Arai H, OshimaY, Nishijima E. Treatment of postoperativetracheal granulation tissue with inhaledbudesonide in congenital trachealstenosis. J Pediatr Surg. 2014;49(2):293–295, discussion 295
75. Zhu GH, Ng AH, Venkatraman SS, et al. Anovel bioabsorbable drug-elutingtracheal stent. Laryngoscope. 2011;121(10):2234–2239
76. Zopf DA, Hollister SJ, Nelson ME, Ohye RG,Green GE. Bioresorbable airway splintcreated with a three-dimensionalprinter. N Engl J Med. 2013;368(21):2043–2045
77. Andrews TM, et al. Tracheoplasty forcongenital complete tracheal rings. ArchOtolaryngol Head Neck Surg. 1994;120(12):1363–1369
78. Chung SR, et al. Clinical outcomes ofslide tracheoplasty in congenitaltracheal stenosis. Eur J CardiothoracSurg. 2015;47(3):537–542; discussion 542
PEDIATRICS Volume 136, number 3, September 2015 e669 by guest on August 19, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2014-3931 originally published online August 24, 2015; 2015;136;e660Pediatrics
Sophie C. Hofferberth, Karen Watters, Reza Rahbar and Francis Fynn-ThompsonManagement of Congenital Tracheal Stenosis
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/136/3/e660including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/136/3/e660#BIBLThis article cites 78 articles, 0 of which you can access for free at:
Subspecialty Collections
ers_subhttp://www.aappublications.org/cgi/collection/cardiovascular_disordCardiovascular Disordershttp://www.aappublications.org/cgi/collection/cardiology_subCardiologyhttp://www.aappublications.org/cgi/collection/birth_defects_subBirth Defectssubhttp://www.aappublications.org/cgi/collection/fetus:newborn_infant_Fetus/Newborn Infantfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on August 19, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2014-3931 originally published online August 24, 2015; 2015;136;e660Pediatrics
Sophie C. Hofferberth, Karen Watters, Reza Rahbar and Francis Fynn-ThompsonManagement of Congenital Tracheal Stenosis
http://pediatrics.aappublications.org/content/136/3/e660located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on August 19, 2018www.aappublications.org/newsDownloaded from