Embed Size (px)
Citation preview
BREAST
Management of the Infected or Exposed BreastProsthesis: A Single Surgeon’s 15-YearExperience with 69 Patients
Scott L. Spear, M.D.Mitchel Seruya, M.D.
Washington, D.C.
Background: In 2004, the senior author (S.L.S.) published an algorithm for themanagement of breast device infection and/or exposure. The purpose of thisstudy was to build on the authors’ prior experience by expanding the cohort ofpatients and to identify risk factors for failed breast device salvage and recurrentinfection/exposure.Methods: A retrospective study was carried out on a single plastic surgeon’sexperience between 1993 and 2008. Patients with infected and/or exposedbreast devices were classified into one of seven groups and salvage rates werecalculated. Patient demographics and wound culture pathogens wereanalyzed as possible risk factors for device loss and recurrent infection/exposure.Results: Over a 15-year period, the senior author managed 69 patients with87 events of breast device infection and/or exposure. The overall salvage ratewas 64.4 percent. Failed device salvage was significantly associated with thepresence of atypical pathogens, such as Gram-negative rods, methicillin-resistant Staphylococcus aureus, and Candida parapsilosis. Recurrent deviceinfection and/or exposure was significantly associated with a history ofradiotherapy or the presence of S. aureus on wound culture.Conclusions: Salvage of the infected and/or exposed breast prosthesis re-mains a challenging yet viable option for a subset of patients. Relativecontraindications include atypical pathogens on wound culture, such asGram-negative rods, methicillin-resistant S. aureus, and C. parapsilosis. Pa-tients with a prior device infection and/or exposure and a history of eitherradiotherapy or S. aureus on wound culture should be monitored closely forsigns of recurrence and managed cautiously in the setting of elective breastsurgery. (Plast. Reconstr. Surg. 125: 1074, 2010.)
Breast implants continue to be a popular op-tion for both aesthetic and reconstructive plas-tic surgery patients. Augmentation mamma-
plasty has seen a 64 percent increase in volumesince the year 2000, and became the top cosmeticprocedure performed in the United States in2007, with 347,500 new cases. Furthermore, pros-thetic breast reconstruction has remained themost common procedure performed for women
with acquired mastectomy defects, representing75.5 percent of all breast reconstruction cases in2007 in the United States.1
Despite improvements in breast implant designand surgical technique, device infection and expo-sure remain real concerns. Rates of infection haveranged from 0.4 to 2.5 percent for augmentationmammaplasty2–6 and from 1 to 35.4 percent forprosthetic breast reconstruction.3,7–13 Further-more, rates of exposure have been reported
From the Department of Plastic Surgery, Georgetown Uni-versity Hospital.Received for publication June 29, 2009; accepted October 22,2009.Poster presented at the 88th Annual Meeting of the AmericanAssociation of Plastic Surgeons, in Rancho Mirage, Cali-fornia, March 21 through 24, 2009.Copyright ©2010 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e3181d17fff
Disclosure: Dr. Spear is a paid consultant forLifeCell Corp. (Branchburg, N.J.) and Allergan,Inc. (Irvine, Calif.). Dr. Seruya has no financialinterest in any of the products, devices, or drugsmentioned in this article.
www.PRSJournal.com1074

between 0.29 and 2 percent for breast augm-entation4,5 and between 0.25 and 8.3 percent fordevice-based breast reconstruction.10,14,15
In the past, common practice was the immediateremoval of the infected or exposed breast prosthe-ses16,17; however, the more recent plastic surgery lit-erature has explored options for device salvage.3,18–32
Methods for salvaging an infected device haveincluded systemic antibiotics combined with eitherconservative wound drainage,3 antibiotic lavage,33
capsulotomy and device exchange,29 capsulecurettage and device exchange,18 antibiotic la-vage followed by capsule curettage and deviceexchange,28 or capsulotomy/curettage/device ex-change followed by postoperative continuous an-tibiotic irrigation.31,32 For exposed breast prosthe-ses, salvage techniques have included conservativewound care with systemic antibiotics,19 device ex-change with primary closure with or without pos-terior capsular flap coverage,25,26 and device ex-change combined with muscular coverage.24
Despite a number of reports focusing on man-agement of the infected or exposed breast pros-thesis, there is still disagreement regarding thewisdom of and indications for device salvage andthe optimal timing, setting, or technique. It wouldbe valuable for plastic surgeons to better define aset of clinical guidelines addressing these very is-sues, given the medical, legal, psychological, andeconomic issues associated with possible implantloss. Device explantation is a traumatic event and,for practical purposes, represents the loss of abreast. Successful device salvage offered to prop-erly selected patients with the greatest possibilityof success would be a highly desirable alternativeto loss of an implant.
In 2004, the senior author (S.L.S.) introducedan algorithm for the management of breast deviceinfection and/or exposure. Patients were strati-fied into one of seven groups of infection/expo-sure, and a treatment strategy was based on theresponse of the infection to initial antibiotic ther-apy and on the availability of soft-tissue coverage.27
As an initial step, that recommendation deservesfurther review to validate its observations and torefine its analysis.
The purpose of the present study was to buildon our prior experience by expanding the cohortof patients and to try to better identify risk factorsfor failed breast device salvage and recurrent in-fection/exposure. With this added information,patients and surgeons can make more informeddecisions regarding the likelihood of saving athreatened breast prosthesis.
PATIENTS AND METHODSA retrospective study was carried out on a sin-
gle plastic surgeon’s experience between 1993 and2008. Patients with infected and/or exposedbreast devices were identified through a combi-nation of quality improvement records of compli-cations, office charts, and hospital records. Eventsof device infection and/or exposure were classi-fied into one of seven groups, as defined by Spearet al.27 as follows: group I, mild infection; group II,severe infection; group III, threatened exposure;group IV, threatened exposure with mild infec-tion; group V, threatened exposure with severeinfection; group VI, actual exposure with no/mildinfection; and group VII, actual exposure withsevere infection. Mild infection was defined aswarmth, swelling, cellulitis, or nonpurulent drain-age that was responsive to initial antibiotic ther-apy. Severe infection was defined as persistent orsubstantial warmth/erythema/swelling despiteantibiotic therapy, purulent drainage, atypicalorganisms on wound culture (e.g., methicillin-resistant Staphylococcus aureus, Gram-negativerods, mycobacteria, or yeast), or serious signsand symptoms of systemic infection (e.g., highfever, hypotension).
Salvage rates for individual classes of breastprosthesis infection and/or exposure were calcu-lated. Salvage rates were reported on a per-eventbasis, given that a number of patients experiencedmore than one episode of infection and/or ex-posure. “Device salvage” was defined as the con-tinued presence of a prosthetic device aftersurgical intervention, though not necessarily reten-tion of the original device.27 Depending on the ini-tial response to antibiotics and the availability ofsoft-tissue coverage, different modalities of devicesalvage were used for the infected or exposed breastdevice, as described previously.27 These included sys-temic antibiotic therapy, wound edge debridement,capsule curettage, capsulectomy, pulse lavage, de-vice position change (e.g., subglandular to subpec-toral), device exchange, primary closure, and/orflap coverage.
Associated demographics, including patientage, body mass index, former or active tobaccouse, history of chemotherapy, and exposure toradiotherapy, were assessed as possible risk factorsfor device loss and recurrent infection/exposure.Patient demographics were reported on a per-event basis for device loss and on a per-patientbasis for recurrent infection/exposure. This en-sured comprehensive collection and analysis of allavailable data.
Volume 125, Number 4 • Infected or Exposed Breast Prosthesis
1075

Wound culture pathogens were also investi-gated as potential contributors to device loss andrecurrent infection/exposure. Culture data werenot available for every event of infection/expo-sure, as some patients presented without evidenceof wound drainage. Pathogens were reported ona per-event basis for device loss and on a per-patient basis for recurrent infection/exposure.
For statistical analysis, the t test was used forcomparison of continuous variables, given theirnormal distribution and equal variances. The Fish-er’s exact test was used for evaluation of percent-ages or frequencies. A value of p � 0.05 was con-sidered statistically significant.
RESULTSOver a 15-year period, the senior author man-
aged 69 patients with 87 events of breast device in-fection and/or exposure. The mean patient age was49.8 years (range, 17 to 75 years), and the averagebody mass index was 23.4. Smoking history revealedthat 18.4 percent of events involved patients withformer or active tobacco use. Furthermore, 35.6 per-cent of events were associated with a history of che-motherapy use and 23.0 percent of incidents in-volved patients with exposure to radiotherapy.
The mean postoperative time to breast prosthe-sis infection/exposure was 5.5 months, with an over-all device salvage rate of 64.4 percent. Salvage andexplantation rates for individual classes of infectionand/or exposure are listed in Table 1, with a meanfollow-up of 24.7 months. Thirty-four events involvedbreast prostheses with mild infection, classified asgroup I, and were associated with a 100 percentsalvage rate. Twenty-six events concerned deviceswith severe infection, categorized as group II, andresulted in a 30.8 percent salvage rate. Six eventsinvolved threatened device exposure without signsof infection, labeled as group III, and were associ-ated with a 100 percent salvage rate. Three eventsdealt with threatened device exposure with mild in-fection, classified as group IV, and were related to a66.7 percent salvage rate. Five incidents involved
threatened prosthesis exposure with severe infec-tion, categorized as group V, and were associatedwith a 40.0 percent salvage rate. Six events concernedactual device exposure with no/mild infection, labeledas group VI, and were associated with a 66.7 percentsalvage rate. Seven incidents involved actual device ex-posure with severe infection, classified as group VII,and resulted in a 0 percent salvage rate.
Rates of contracture, hematoma, and seromawere investigated for the 56 events of successfuldevice salvage. There was a 1.8 percent rate ofcapsular contracture (Baker grade III/IV) and a1.8 percent incidence of hematoma. There wereno occurrences of seroma or patient death.
Patient demographics and wound pathogenswere evaluated as possible risk factors for faileddevice salvage and as potential predictors for suc-cessful device salvage. As shown in Table 2, eventsof failed device salvage were associated with a sig-nificantly higher degree of atypical pathogens,such as Gram-negative rods, methicillin-resistantStaphylococcus aureus, and Candida parapsilosis, ascompared with events of successful salvage (42.9percent versus 11.5 percent, p � 0.015). Events offailed device salvage trended with an older meanpatient age, in contrast to events of successful sal-vage, yet these results were not statistically signif-icant (age 52.5 years compared with 48.3 years, p �0.069). Failed device salvage events had a higherpercentage of patients with exposure to radiother-apy as compared with successful salvage events, yetthese findings did not reach statistical significance(32.3 percent compared with 17.9 percent, p �0.18). Incidents of failed device salvage had ahigher degree of Gram-negative rods and S. aureuson wound culture in relation to events of success-ful salvage, yet neither result was found to be sta-tistically significant (28.6 percent compare with11.5 percent, p � 0.18; and 25.0 percent comparedwith 7.7 percent, p � 0.14, respectively). Events ofsuccessful prosthesis salvage were associated witha higher percentage of coagulase-negative Staph-ylococcus, in contrast to events of failed salvage;
Table 1. Salvage and Explantation Rates for Different Classes of Infected and/or Exposed Breast Prostheses*
Class of Infection and/or ExposureSuccessful Salvage
Rate (%)Explantation Rate without
Surgical Salvage Attempt (%)
Group I: Mild infection 34/34 (100) 0/34 (0)Group II: Severe infection 8/26 (30.8) 18/26 (69.2)Group III: Threatened exposure 6/6 (100.0) 0/6 (0)Group IV: Threatened exposure with mild infection 2/3 (66.7) 1/3 (33.3)Group V: Threatened exposure with severe infection 2/5 (40.0) 3/5 (60.0)Group VI: Actual exposure with mild infection 4/6 (66.7) 1/6 (16.7)Group VII: Actual exposure with severe infection 0/7 (0) 6/7 (85.7)*Analyzed per event.
Plastic and Reconstructive Surgery • April 2010
1076
however, this too was not statistically significant(30.8 percent compared with 17.9 percent, p �0.35). No statistically significant effects on devicesalvage were noted for body mass index, history oftobacco use, exposure to chemotherapy, or ab-sence of growth on wound cultures.
Patient demographics and wound pathogenswere also evaluated as possible risk factors for re-current device infection and/or exposure. Aslisted in Table 3, patients with recurrent deviceinfection and/or exposure were significantly as-sociated with either a history of radiotherapy orthe presence of S. aureus on wound culture ascompared with patients with a one-time episode(46.2 percent compared with 16.1 percent, p �0.028; and 38.5 percent compared with 5.9 per-cent, p � 0.012, respectively). Although patientswith repeat episodes of infection and/or exposure
had a higher rate of tobacco and chemotherapyuse in relation to patients with a single episode,these findings were not found to be statisticallysignificant (30.8 percent compared with 14.3 per-cent, p � 0.22; and 46.2 percent compared with28.6 percent, p � 0.32, respectively). Patients withrecurrent episodes of device infection and/or ex-posure had a lower degree of Gram-negative rodson wound culture in contrast to patients with aone-time event, yet this was not found to be sta-tistically significant (7.7 percent compared with29.4 percent, p � 0.15). No statistically significanteffects on recurrent device infection and/or ex-posure were noted for age, body mass index, pres-ence of either atypical pathogens or coagulase-negative Staphylococcus on wound culture, orabsence of growth on wound cultures.
CASE REPORTS
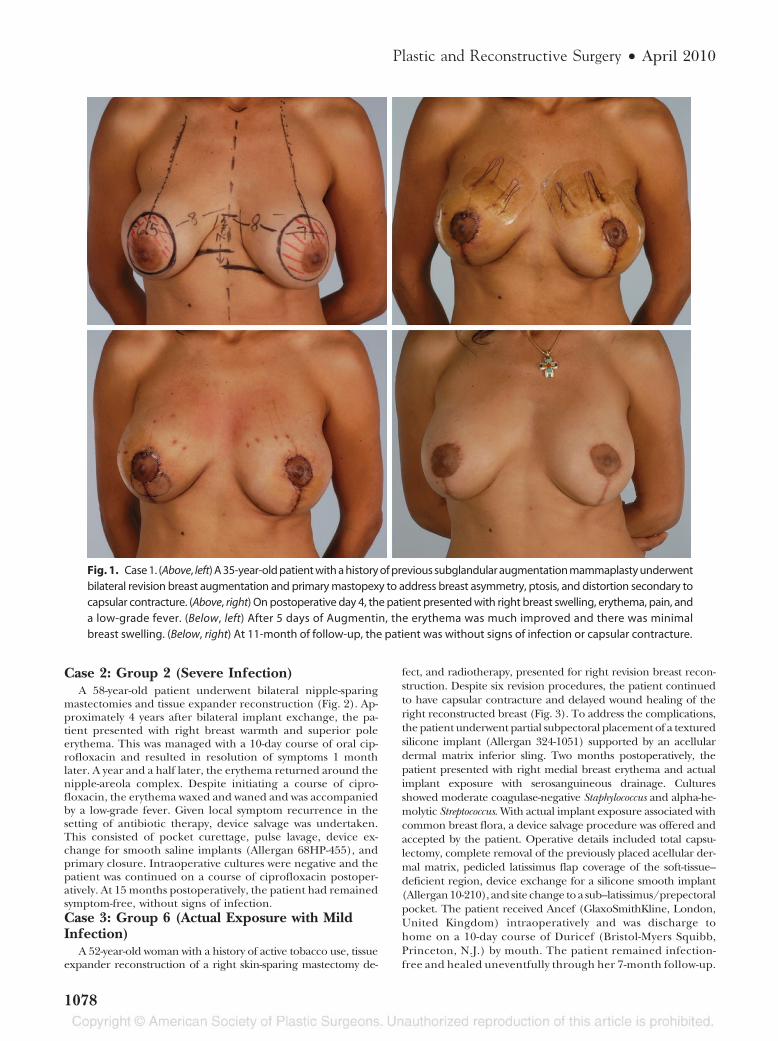
Case 1: Group I (Mild Infection)A 35-year-old patient with a history of previous subglan-
dular augmentation mammaplasty underwent bilateral revi-sion breast augmentation and primary mastopexy to addressbreast asymmetry, ptosis, and distortion secondary to capsu-lar contracture (Fig. 1). Operative steps included bilateraltotal capsulectomies, pocket conversion to a dual plane,placement of silicone smooth implants (Allergan 15-371,15-339; Allergan, Inc., Irvine, Calif.), and circumvertical mas-topexies. On postoperative day 4, the patient presented tothe emergency room with right breast swelling, erythema,pain, and a low-grade fever. This was managed with a one-time dose of vancomycin intravenously, followed by a courseof Augmentin (GlaxoSmithKline, Brentford, London, UnitedKingdom) on discharge. After 5 days of oral antibiotic therapy,the erythema was much improved and there was minimal breastswelling. Symptoms resolved completely following a 10-daycourse of Augmentin and the patient was without signs of in-fection or capsular contracture at 11-month follow-up.
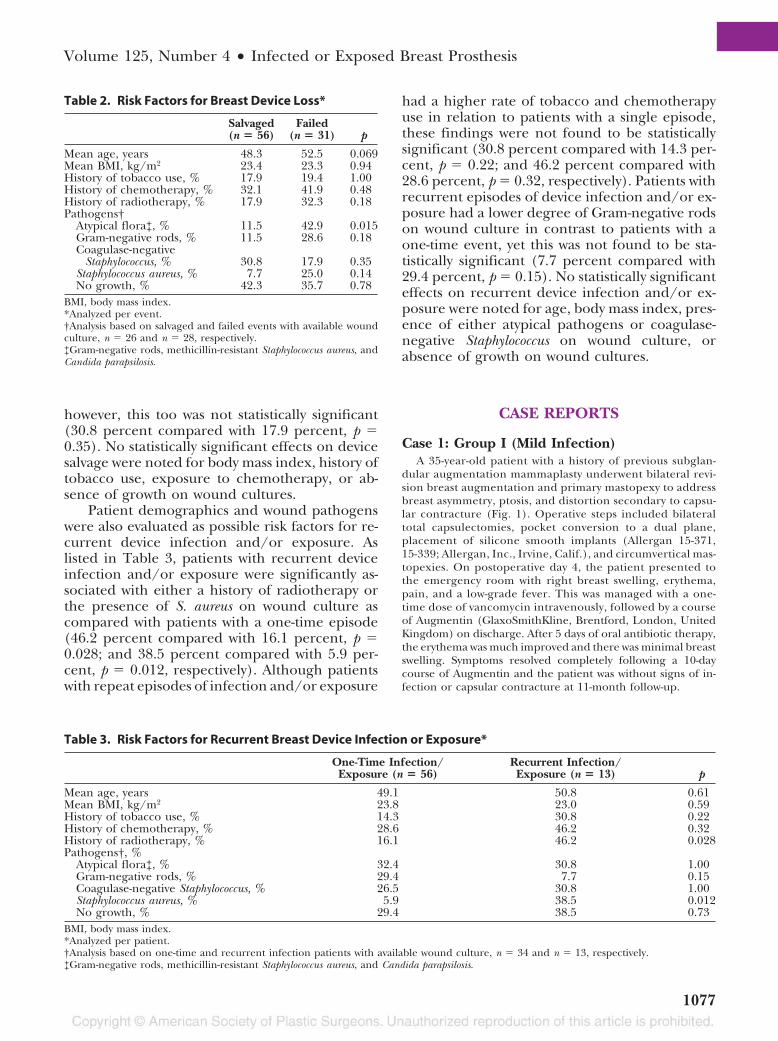
Table 2. Risk Factors for Breast Device Loss*
Salvaged(n � 56)
Failed(n � 31) p
Mean age, years 48.3 52.5 0.069Mean BMI, kg/m2 23.4 23.3 0.94History of tobacco use, % 17.9 19.4 1.00History of chemotherapy, % 32.1 41.9 0.48History of radiotherapy, % 17.9 32.3 0.18Pathogens†
Atypical flora‡, % 11.5 42.9 0.015Gram-negative rods, % 11.5 28.6 0.18Coagulase-negative
Staphylococcus, % 30.8 17.9 0.35Staphylococcus aureus, % 7.7 25.0 0.14No growth, % 42.3 35.7 0.78
BMI, body mass index.*Analyzed per event.†Analysis based on salvaged and failed events with available woundculture, n � 26 and n � 28, respectively.‡Gram-negative rods, methicillin-resistant Staphylococcus aureus, andCandida parapsilosis.
Table 3. Risk Factors for Recurrent Breast Device Infection or Exposure*
One-Time Infection/Exposure (n � 56)
Recurrent Infection/Exposure (n � 13) p
Mean age, years 49.1 50.8 0.61Mean BMI, kg/m2 23.8 23.0 0.59History of tobacco use, % 14.3 30.8 0.22History of chemotherapy, % 28.6 46.2 0.32History of radiotherapy, % 16.1 46.2 0.028Pathogens†, %
Atypical flora‡, % 32.4 30.8 1.00Gram-negative rods, % 29.4 7.7 0.15Coagulase-negative Staphylococcus, % 26.5 30.8 1.00Staphylococcus aureus, % 5.9 38.5 0.012No growth, % 29.4 38.5 0.73
BMI, body mass index.*Analyzed per patient.†Analysis based on one-time and recurrent infection patients with available wound culture, n � 34 and n � 13, respectively.‡Gram-negative rods, methicillin-resistant Staphylococcus aureus, and Candida parapsilosis.
Volume 125, Number 4 • Infected or Exposed Breast Prosthesis
1077
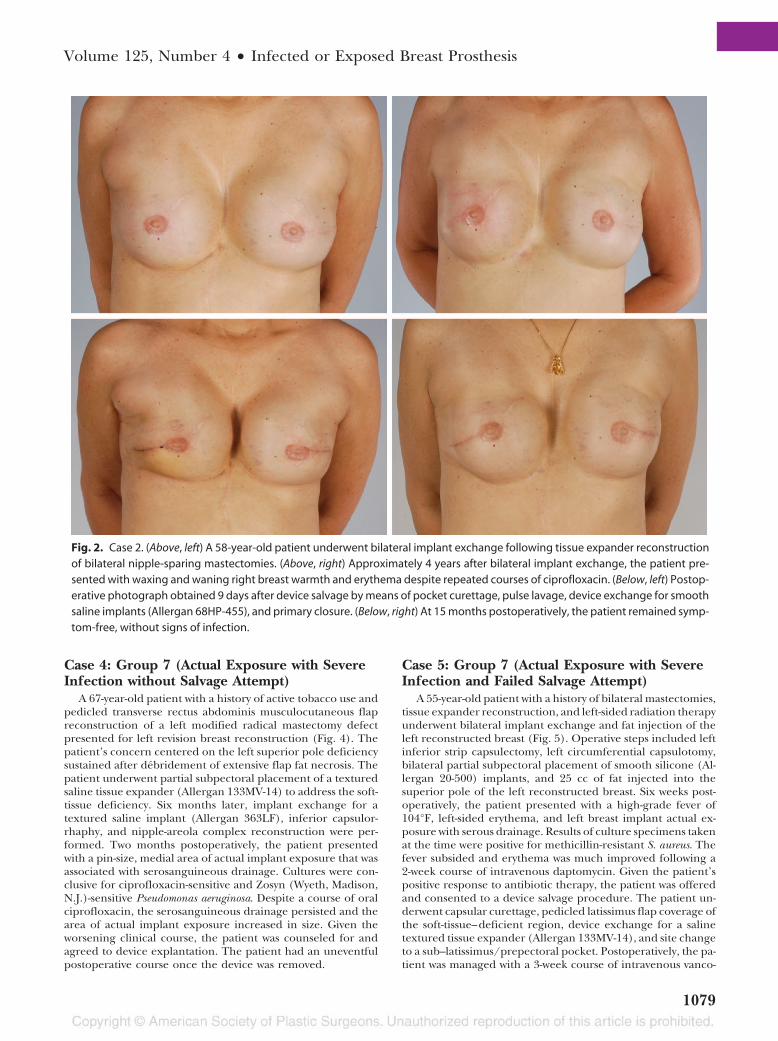
Case 2: Group 2 (Severe Infection)A 58-year-old patient underwent bilateral nipple-sparing
mastectomies and tissue expander reconstruction (Fig. 2). Ap-proximately 4 years after bilateral implant exchange, the pa-tient presented with right breast warmth and superior poleerythema. This was managed with a 10-day course of oral cip-rofloxacin and resulted in resolution of symptoms 1 monthlater. A year and a half later, the erythema returned around thenipple-areola complex. Despite initiating a course of cipro-floxacin, the erythema waxed and waned and was accompaniedby a low-grade fever. Given local symptom recurrence in thesetting of antibiotic therapy, device salvage was undertaken.This consisted of pocket curettage, pulse lavage, device ex-change for smooth saline implants (Allergan 68HP-455), andprimary closure. Intraoperative cultures were negative and thepatient was continued on a course of ciprofloxacin postoper-atively. At 15 months postoperatively, the patient had remainedsymptom-free, without signs of infection.Case 3: Group 6 (Actual Exposure with MildInfection)
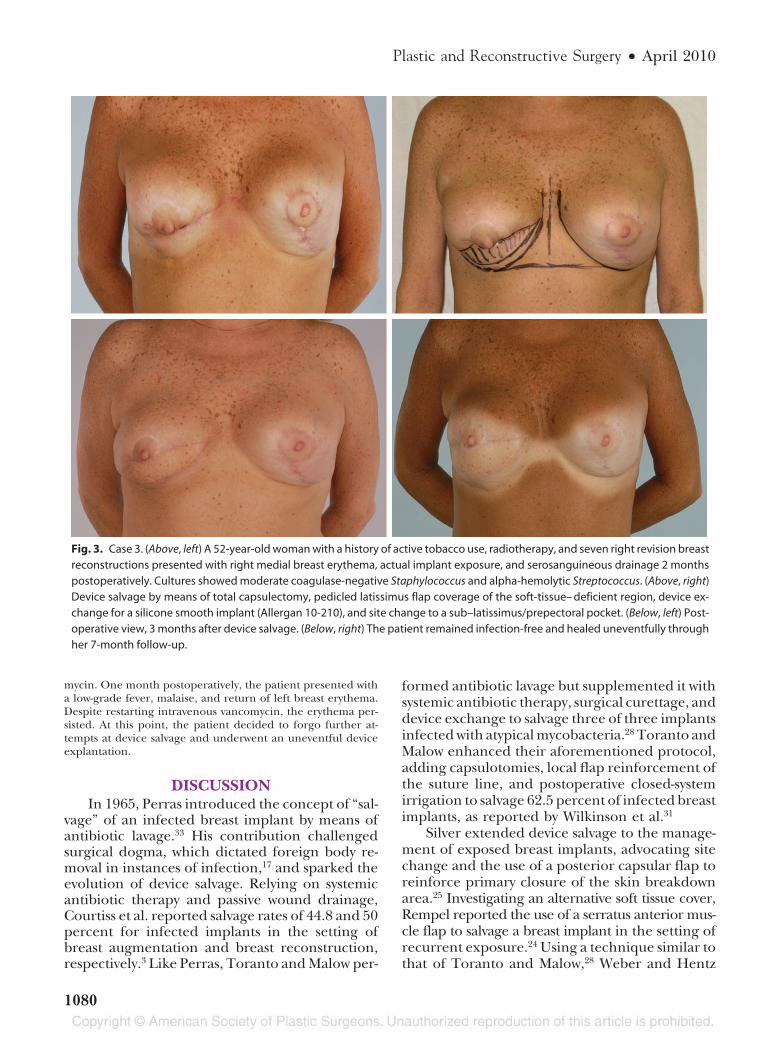
A 52-year-old woman with a history of active tobacco use, tissueexpander reconstruction of a right skin-sparing mastectomy de-
fect, and radiotherapy, presented for right revision breast recon-struction. Despite six revision procedures, the patient continuedto have capsular contracture and delayed wound healing of theright reconstructed breast (Fig. 3). To address the complications,the patient underwent partial subpectoral placement of a texturedsilicone implant (Allergan 324-1051) supported by an acellulardermal matrix inferior sling. Two months postoperatively, thepatient presented with right medial breast erythema and actualimplant exposure with serosanguineous drainage. Culturesshowed moderate coagulase-negative Staphylococcus and alpha-he-molytic Streptococcus. With actual implant exposure associated withcommon breast flora, a device salvage procedure was offered andaccepted by the patient. Operative details included total capsu-lectomy, complete removal of the previously placed acellular der-mal matrix, pedicled latissimus flap coverage of the soft-tissue–deficient region, device exchange for a silicone smooth implant(Allergan 10-210), and site change to a sub–latissimus/prepectoralpocket. The patient received Ancef (GlaxoSmithKline, London,United Kingdom) intraoperatively and was discharge tohome on a 10-day course of Duricef (Bristol-Myers Squibb,Princeton, N.J.) by mouth. The patient remained infection-free and healed uneventfully through her 7-month follow-up.
Fig. 1. Case 1. (Above, left) A 35-year-old patient with a history of previous subglandular augmentation mammaplasty underwentbilateral revision breast augmentation and primary mastopexy to address breast asymmetry, ptosis, and distortion secondary tocapsular contracture. (Above, right) On postoperative day 4, the patient presented with right breast swelling, erythema, pain, anda low-grade fever. (Below, left) After 5 days of Augmentin, the erythema was much improved and there was minimalbreast swelling. (Below, right) At 11-month of follow-up, the patient was without signs of infection or capsular contracture.
Plastic and Reconstructive Surgery • April 2010
1078
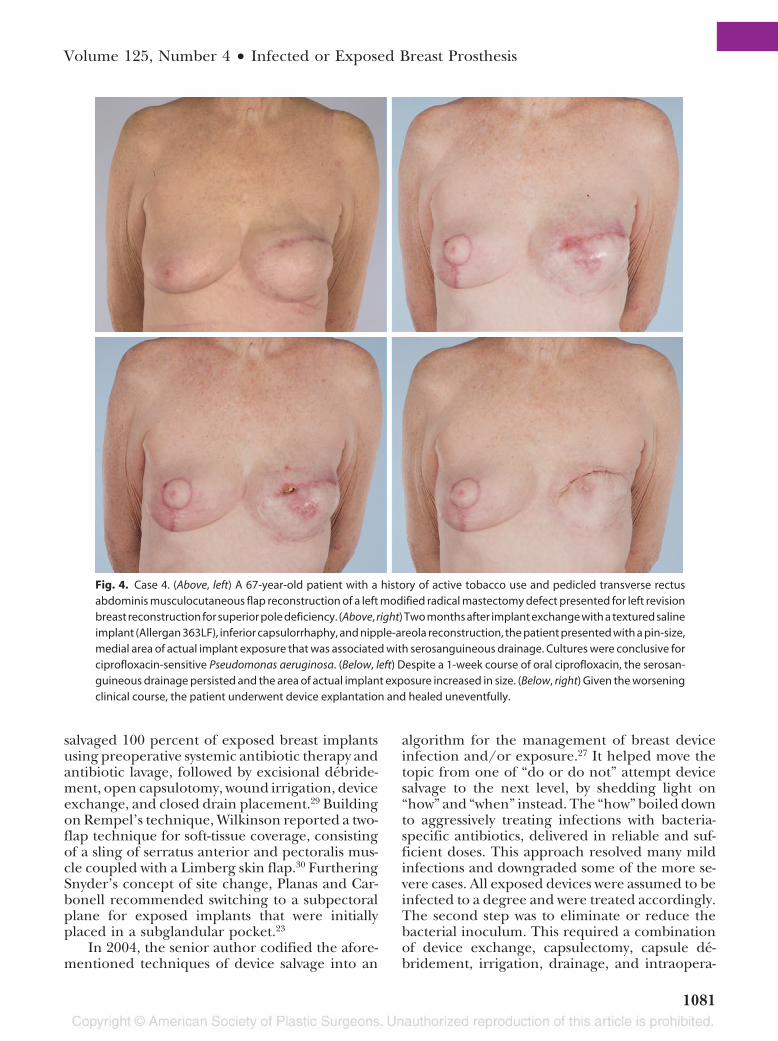
Case 4: Group 7 (Actual Exposure with SevereInfection without Salvage Attempt)
A 67-year-old patient with a history of active tobacco use andpedicled transverse rectus abdominis musculocutaneous flapreconstruction of a left modified radical mastectomy defectpresented for left revision breast reconstruction (Fig. 4). Thepatient’s concern centered on the left superior pole deficiencysustained after debridement of extensive flap fat necrosis. Thepatient underwent partial subpectoral placement of a texturedsaline tissue expander (Allergan 133MV-14) to address the soft-tissue deficiency. Six months later, implant exchange for atextured saline implant (Allergan 363LF), inferior capsulor-rhaphy, and nipple-areola complex reconstruction were per-formed. Two months postoperatively, the patient presentedwith a pin-size, medial area of actual implant exposure that wasassociated with serosanguineous drainage. Cultures were con-clusive for ciprofloxacin-sensitive and Zosyn (Wyeth, Madison,N.J.)-sensitive Pseudomonas aeruginosa. Despite a course of oralciprofloxacin, the serosanguineous drainage persisted and thearea of actual implant exposure increased in size. Given theworsening clinical course, the patient was counseled for andagreed to device explantation. The patient had an uneventfulpostoperative course once the device was removed.
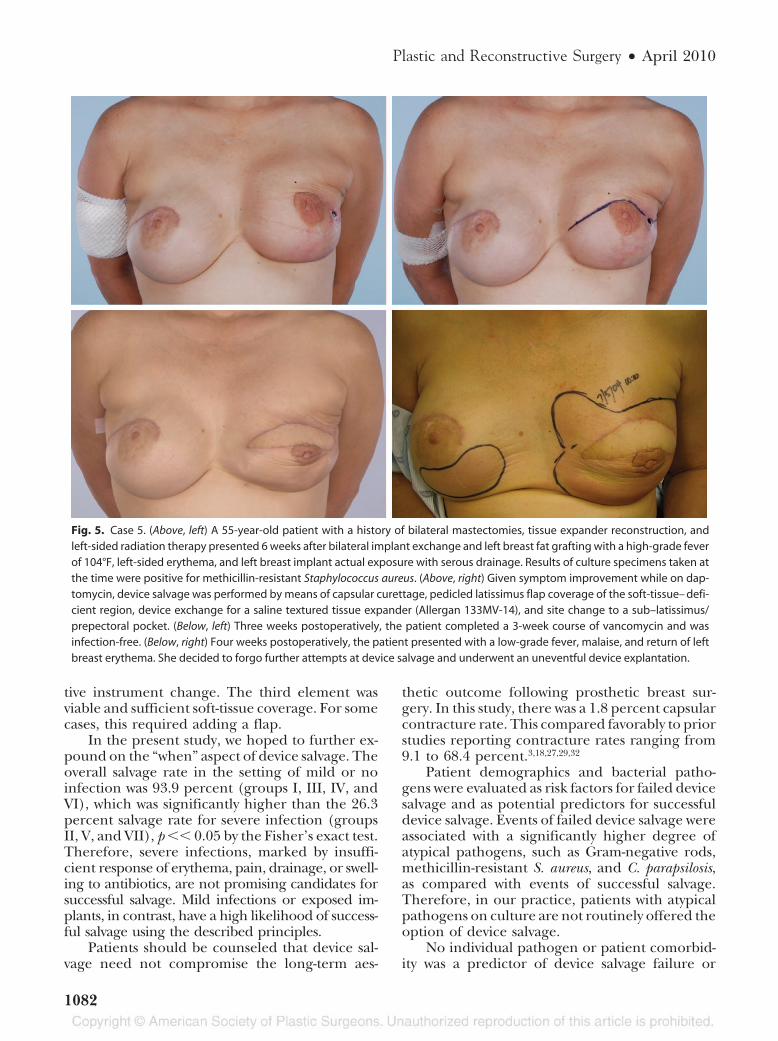
Case 5: Group 7 (Actual Exposure with SevereInfection and Failed Salvage Attempt)
A 55-year-old patient with a history of bilateral mastectomies,tissue expander reconstruction, and left-sided radiation therapyunderwent bilateral implant exchange and fat injection of theleft reconstructed breast (Fig. 5). Operative steps included leftinferior strip capsulectomy, left circumferential capsulotomy,bilateral partial subpectoral placement of smooth silicone (Al-lergan 20-500) implants, and 25 cc of fat injected into thesuperior pole of the left reconstructed breast. Six weeks post-operatively, the patient presented with a high-grade fever of104°F, left-sided erythema, and left breast implant actual ex-posure with serous drainage. Results of culture specimens takenat the time were positive for methicillin-resistant S. aureus. Thefever subsided and erythema was much improved following a2-week course of intravenous daptomycin. Given the patient’spositive response to antibiotic therapy, the patient was offeredand consented to a device salvage procedure. The patient un-derwent capsular curettage, pedicled latissimus flap coverage ofthe soft-tissue–deficient region, device exchange for a salinetextured tissue expander (Allergan 133MV-14), and site changeto a sub–latissimus/prepectoral pocket. Postoperatively, the pa-tient was managed with a 3-week course of intravenous vanco-
Fig. 2. Case 2. (Above, left) A 58-year-old patient underwent bilateral implant exchange following tissue expander reconstructionof bilateral nipple-sparing mastectomies. (Above, right) Approximately 4 years after bilateral implant exchange, the patient pre-sented with waxing and waning right breast warmth and erythema despite repeated courses of ciprofloxacin. (Below, left) Postop-erative photograph obtained 9 days after device salvage by means of pocket curettage, pulse lavage, device exchange for smoothsaline implants (Allergan 68HP-455), and primary closure. (Below, right) At 15 months postoperatively, the patient remained symp-tom-free, without signs of infection.
Volume 125, Number 4 • Infected or Exposed Breast Prosthesis
1079
mycin. One month postoperatively, the patient presented witha low-grade fever, malaise, and return of left breast erythema.Despite restarting intravenous vancomycin, the erythema per-sisted. At this point, the patient decided to forgo further at-tempts at device salvage and underwent an uneventful deviceexplantation.
DISCUSSIONIn 1965, Perras introduced the concept of “sal-
vage” of an infected breast implant by means ofantibiotic lavage.33 His contribution challengedsurgical dogma, which dictated foreign body re-moval in instances of infection,17 and sparked theevolution of device salvage. Relying on systemicantibiotic therapy and passive wound drainage,Courtiss et al. reported salvage rates of 44.8 and 50percent for infected implants in the setting ofbreast augmentation and breast reconstruction,respectively.3 Like Perras, Toranto and Malow per-
formed antibiotic lavage but supplemented it withsystemic antibiotic therapy, surgical curettage, anddevice exchange to salvage three of three implantsinfected with atypical mycobacteria.28 Toranto andMalow enhanced their aforementioned protocol,adding capsulotomies, local flap reinforcement ofthe suture line, and postoperative closed-systemirrigation to salvage 62.5 percent of infected breastimplants, as reported by Wilkinson et al.31
Silver extended device salvage to the manage-ment of exposed breast implants, advocating sitechange and the use of a posterior capsular flap toreinforce primary closure of the skin breakdownarea.25 Investigating an alternative soft tissue cover,Rempel reported the use of a serratus anterior mus-cle flap to salvage a breast implant in the setting ofrecurrent exposure.24 Using a technique similar tothat of Toranto and Malow,28 Weber and Hentz
Fig. 3. Case 3. (Above, left) A 52-year-old woman with a history of active tobacco use, radiotherapy, and seven right revision breastreconstructions presented with right medial breast erythema, actual implant exposure, and serosanguineous drainage 2 monthspostoperatively. Cultures showed moderate coagulase-negative Staphylococcus and alpha-hemolytic Streptococcus. (Above, right)Device salvage by means of total capsulectomy, pedicled latissimus flap coverage of the soft-tissue– deficient region, device ex-change for a silicone smooth implant (Allergan 10-210), and site change to a sub–latissimus/prepectoral pocket. (Below, left) Post-operative view, 3 months after device salvage. (Below, right) The patient remained infection-free and healed uneventfully throughher 7-month follow-up.
Plastic and Reconstructive Surgery • April 2010
1080
salvaged 100 percent of exposed breast implantsusing preoperative systemic antibiotic therapy andantibiotic lavage, followed by excisional debride-ment, open capsulotomy, wound irrigation, deviceexchange, and closed drain placement.29 Buildingon Rempel’s technique, Wilkinson reported a two-flap technique for soft-tissue coverage, consistingof a sling of serratus anterior and pectoralis mus-cle coupled with a Limberg skin flap.30 FurtheringSnyder’s concept of site change, Planas and Car-bonell recommended switching to a subpectoralplane for exposed implants that were initiallyplaced in a subglandular pocket.23
In 2004, the senior author codified the afore-mentioned techniques of device salvage into an
algorithm for the management of breast deviceinfection and/or exposure.27 It helped move thetopic from one of “do or do not” attempt devicesalvage to the next level, by shedding light on“how” and “when” instead. The “how” boiled downto aggressively treating infections with bacteria-specific antibiotics, delivered in reliable and suf-ficient doses. This approach resolved many mildinfections and downgraded some of the more se-vere cases. All exposed devices were assumed to beinfected to a degree and were treated accordingly.The second step was to eliminate or reduce thebacterial inoculum. This required a combinationof device exchange, capsulectomy, capsule de-bridement, irrigation, drainage, and intraopera-
Fig. 4. Case 4. (Above, left) A 67-year-old patient with a history of active tobacco use and pedicled transverse rectusabdominis musculocutaneous flap reconstruction of a left modified radical mastectomy defect presented for left revisionbreast reconstruction for superior pole deficiency. (Above, right) Two months after implant exchange with a textured salineimplant (Allergan 363LF), inferior capsulorrhaphy, and nipple-areola reconstruction, the patient presented with a pin-size,medial area of actual implant exposure that was associated with serosanguineous drainage. Cultures were conclusive forciprofloxacin-sensitive Pseudomonas aeruginosa. (Below, left) Despite a 1-week course of oral ciprofloxacin, the serosan-guineous drainage persisted and the area of actual implant exposure increased in size. (Below, right) Given the worseningclinical course, the patient underwent device explantation and healed uneventfully.
Volume 125, Number 4 • Infected or Exposed Breast Prosthesis
1081
tive instrument change. The third element wasviable and sufficient soft-tissue coverage. For somecases, this required adding a flap.
In the present study, we hoped to further ex-pound on the “when” aspect of device salvage. Theoverall salvage rate in the setting of mild or noinfection was 93.9 percent (groups I, III, IV, andVI), which was significantly higher than the 26.3percent salvage rate for severe infection (groupsII, V, and VII), p �� 0.05 by the Fisher’s exact test.Therefore, severe infections, marked by insuffi-cient response of erythema, pain, drainage, or swell-ing to antibiotics, are not promising candidates forsuccessful salvage. Mild infections or exposed im-plants, in contrast, have a high likelihood of success-ful salvage using the described principles.
Patients should be counseled that device sal-vage need not compromise the long-term aes-
thetic outcome following prosthetic breast sur-gery. In this study, there was a 1.8 percent capsularcontracture rate. This compared favorably to priorstudies reporting contracture rates ranging from9.1 to 68.4 percent.3,18,27,29,32
Patient demographics and bacterial patho-gens were evaluated as risk factors for failed devicesalvage and as potential predictors for successfuldevice salvage. Events of failed device salvage wereassociated with a significantly higher degree ofatypical pathogens, such as Gram-negative rods,methicillin-resistant S. aureus, and C. parapsilosis,as compared with events of successful salvage.Therefore, in our practice, patients with atypicalpathogens on culture are not routinely offered theoption of device salvage.
No individual pathogen or patient comorbid-ity was a predictor of device salvage failure or
Fig. 5. Case 5. (Above, left) A 55-year-old patient with a history of bilateral mastectomies, tissue expander reconstruction, andleft-sided radiation therapy presented 6 weeks after bilateral implant exchange and left breast fat grafting with a high-grade feverof 104°F, left-sided erythema, and left breast implant actual exposure with serous drainage. Results of culture specimens taken atthe time were positive for methicillin-resistant Staphylococcus aureus. (Above, right) Given symptom improvement while on dap-tomycin, device salvage was performed by means of capsular curettage, pedicled latissimus flap coverage of the soft-tissue– defi-cient region, device exchange for a saline textured tissue expander (Allergan 133MV-14), and site change to a sub–latissimus/prepectoral pocket. (Below, left) Three weeks postoperatively, the patient completed a 3-week course of vancomycin and wasinfection-free. (Below, right) Four weeks postoperatively, the patient presented with a low-grade fever, malaise, and return of leftbreast erythema. She decided to forgo further attempts at device salvage and underwent an uneventful device explantation.
Plastic and Reconstructive Surgery • April 2010
1082

success. Similar to the findings of Yii and Khoo, ahistory of radiotherapy did not affect the salvageoutcome.32 In contrast to Yii and Khoo, growth ofS. aureus on cultures was not found to be a riskfactor for failed device salvage. To explain thediscrepancy, all cases of device loss with S. aureusin the study by Yii and Khoo were in the setting ofunattempted device salvage secondary to patientpreference and not attributable to failed salvageprocedures.
We also found that the absence of bacterialgrowth on culture did not impact the likelihoodof device salvage. No growth of bacteria maysignify a true reduction in colonies versus ster-ilization without elimination of bacterial patho-gens. The variability of bacterial clearance as-sociated with “no growth” may explain why itdoes not serve as a predictor of device salvagefailure or success.
Although a history of radiotherapy or the pres-ence of S. aureus on wound culture did not affectthe success of device salvage, they both were sig-nificantly associated with recurrent device infec-tion and/or exposure. In practice, patients witheither of these risk factors should be monitoredclosely for signs of recurrent breast prosthesis in-fection/exposure. In the setting of elective breastsurgery, these patients need to be managed cau-tiously and covered with historically effective peri-operative antibiotics.
This study addresses the “when” aspect ofbreast device salvage, but it does have several lim-itations. First, the lack of statistical significance forspecific comorbidities or pathogens as risk factorsfor breast device loss or recurrent infection/ex-posure may stem from the small sample size forsubgroup analysis rather than the true absence ofa statistical difference. Second, our reported sal-vage rates seemingly underestimate the success ofdevice salvage in situations of true attempts. Of the31 events of device explantation, 29 incidents werein the setting of unattempted device salvage,whereas only two events were secondary to faileddevice salvage. Therefore, one needs to under-stand the distinction between failed salvage versusunattempted salvage when interpreting the afore-mentioned salvage rates. Lastly, because of theretrospective collection of data, it is possible thatevents of infection and/or exposure may havebeen misclassified or unidentified. All efforts weremade to identify incidents of breast device infec-tion and/or exposure and correlate the eventswith documented patient signs, symptoms, andculture data.
CONCLUSIONSSalvage of the infected and/or exposed breast
prosthesis remains a challenging but viable optionfor a subset of patients. Keys to success includeculture-directed antibiotics, capsulectomy, deviceexchange, and adequate soft-tissue coverage. Rel-ative contraindications to breast device salvage in-clude atypical pathogens on wound culture, suchas Gram-negative rods, methicillin-resistant S. au-reus, and C. parapsilosis. Patients with a prior deviceinfection and/or exposure and a history of eitherradiotherapy or S, aureus on wound culture shouldbe closely monitored for signs of recurrent breastprosthesis infection/exposure and managed cau-tiously in the setting of elective breast surgery.
Scott L. Spear, M.D.Georgetown University Hospital
3800 Reservoir Road, NWPHC Building, 1st FloorWashington, D.C. 20007
REFERENCES1. American Society of Plastic Surgeons. National Clearinghouse
of Plastic Surgery Statistics: 2007. Available at: http://www.plasticsurgery.org/Media/Press_Kits/Procedural_Statistics.html. Accessed January 15, 2009.
2. Araco A, Gravante G, Araco F, Delogu D, Cervelli V, Wal-genbach K. Infections of breast implants in aesthetic breastaugmentations: A single-center review of 3,002 patients. Aes-thetic Plast Surg. 2007;31:325–329.
3. Courtiss EH, Goldwyn RM, Anastasi GW. The fate of breastimplants with infections around them. Plast Reconstr Surg.1979;63:812–816.
4. Cunningham B. The Mentor Core Study on Silicone Memo-ryGel Breast Implants. Plast Reconstr Surg. 2007;120:19S–29S;discussion 30S–32S.
5. De Cholnoky T. Augmentation mammaplasty: Survey of com-plications in 10,941 patients by 265 surgeons. Plast ReconstrSurg. 1970;45:573–577.
6. Stevens WG, Pacella SJ, Gear AJ, et al. Clinical experiencewith a fourth-generation textured silicone gel breast implant:A review of 1012 Mentor MemoryGel breast implants. AesthetSurg J. 2008;28:642–647.
7. Alderman AK, Wilkins EG, Kim HM, Lowery JC. Complica-tions in postmastectomy breast reconstruction: Two-year re-sults of the Michigan Breast Reconstruction Outcome Study.Plast Reconstr Surg. 2002;109:2265–2274.
8. Armstrong RW, Berkowitz RL, Bolding F. Infection followingbreast reconstruction. Ann Plast Surg. 1989;23:284–288.
9. Cordeiro PG, McCarthy CM. A single surgeon’s 12-year ex-perience with tissue expander/implant breast reconstruc-tion: Part I. A prospective analysis of early complications.Plast Reconstr Surg. 2006;118:825–831.
10. Disa JJ, Ad-El DD, Cohen SM, Cordeiro PG, Hidalgo DA. Thepremature removal of tissue expanders in breast reconstruc-tion. Plast Reconstr Surg. 1999;104:1662–1665.
11. Nahabedian MY, Tsangaris T, Momen B, Manson PN. Infec-tious complications following breast reconstruction with ex-panders and implants. Plast Reconstr Surg. 2003;112:467–476.
Volume 125, Number 4 • Infected or Exposed Breast Prosthesis
1083

12. Spear SL, Majidian A. Immediate breast reconstruction intwo stages using textured, integrated-valve tissue expandersand breast implants: A retrospective review of 171 consecu-tive breast reconstructions from 1989 to 1996. Plast ReconstrSurg. 1998;101:53–63.
13. Spear SL, Pelletiere CV. Immediate breast reconstruction intwo stages using textured, integrated-valve tissue expandersand breast implants. Plast Reconstr Surg. 2004;113:2098–2103.
14. Pusic AL, Cordeiro PG. An accelerated approach to tissueexpansion for breast reconstruction: Experience with intra-operative and rapid postoperative expansion in 370 recon-structions. Plast Reconstr Surg. 2003;111:1871–1875.
15. Slavin SA, Colen SR. Sixty consecutive breast reconstructionswith the inflatable expander: A critical appraisal. Plast Re-constr Surg. 1990;86:910–919.
16. Snyderman RK, ed. Breast Augmentation. St. Louis: Mosby;1973.
17. Southwick HW, Economou SG, Otten JW. Prosthetic replace-ment of chest-wall defects; an experimental and clinicalstudy. AMA Arch Surg. 1956;72:901–907.
18. Chun JK, Schulman MR. The infected breast prosthesis aftermastectomy reconstruction: Successful salvage of nine im-plants in eight consecutive patients. Plast Reconstr Surg. 2007;120:581–589.
19. Fodor L, Ramon Y, Ullmann Y, Eldor L, Peled IJ. Fate ofexposed breast implants in augmentation mammoplasty.Ann Plast Surg. 2003;50:447–449.
20. Harving S, Ravnsbaek J, Johansen LV. Salvage of exposed im-plants. Scand J Plast Reconstr Surg Hand Surg. 1989;23:143–144.
21. Kendrick AS, Chase CW. Salvage of an infected breast tissueexpander with an implant sizer and negative pressure woundmanagement. Plast Reconstr Surg. 2008;121:138e–139e.
22. Marsh JL, Stevens WG, Smith GL, Krogstad DJ. Reinsertabil-ity after breast prosthesis pocket infection: An experimentalstudy. Plast Reconstr Surg. 1982;69:234–237.
23. Planas J, Carbonell A. Salvaging the exposed mammary pros-thesis. Aesthetic Plast Surg. 1995;19:535–540.
24. Rempel JH. Treatment of an exposed breast implant bymuscle flap and by fascia graft. Ann Plast Surg. 1978;1:229–232.
25. Silver HL. Treating the complications of augmentation mam-maplasty. Plast Reconstr Surg. 1972;49:637–638.
26. Snyder GB. Treatment of an exposed breast implant by re-implantation behind the posterior wall of the capsule. PlastReconstr Surg. 1975;56:97–98.
27. Spear SL, Howard MA, Boehmler JH, Ducic I, Low M, Ab-bruzzesse MR. The infected or exposed breast implant: Man-agement and treatment strategies. Plast Reconstr Surg. 2004;113:1634–1644.
28. Toranto IR, Malow JB. Atypical mycobacteria periprostheticinfections: Diagnosis and treatment. Plast Reconstr Surg. 1980;66:226–228.
29. Weber J Jr, Hentz RV. Salvage of the exposed breast implant.Ann Plast Surg. 1986;16:106–110.
30. Wilkinson TS. Breast Augmentation. New York: Springer-Ver-lag; 1994.
31. Wilkinson TS, Swartz BE, Toranto IR. Resolution of late-developing periprosthetic breast infections without prosthe-sis removal. Aesthetic Plast Surg. 1985;9:79–85.
32. Yii NW, Khoo CT. Salvage of infected expander prosthesesin breast reconstruction. Plast Reconstr Surg. 2003;111:1087–1092.
33. Perras C. The prevention and treatment of infections followingbreast implants. Plast Reconstr Surg. 1965;35:649–656.
www.editorialmanager.com/prsSubmit your manuscript today through PRS’ Enkwell. The Enkwell submission and review Web site helps makethe submission process easier, more efficient, and less expensive for authors, and makes the review processquicker, more accessible, and less expensive for reviewers. If you are a first-time user, be sure to register onthe system.
Plastic and Reconstructive Surgery • April 2010
1084





























