Embed Size (px)
DESCRIPTION
presentation
Citation preview
1
MATERIALS USED IN
MAXILLOFACIAL PROSTHESIS
2
Introduction Definition History Review of literature Maxillofacial Impression materials and
advancements Maxillofacial Prosthetic Materials
Auxillary Maxillofacial Materials
Discussion
Conclusion
Reference
3
INTRODUCTION
Facial defects can result from trauma, treatment
of neoplasm’s, or congenital malformations. More
often facial defects referred to the Prosthodontist for
restorations are usually the result of surgical resection
of tumors. Restoration of facial defects is a difficult
challenge for both the surgeon and the Prosthodontist.
Both surgical reconstructions and Prosthodontic
restoration have distinct limitations.
4
The surgeon is limited by the availability of
tissue, the compromise of the local vascular bed
by radiation in tumor patients, the need for
periodic visual inspections of an oncology
defects and the physical condition of the patient.
The Prosthodontist is limited by the inadequate
materials available for facial restoration,
movable tissue bed, difficulty in retaining large
prosthesis and patient acceptance.
5
Maxillofacial prosthesis :-
Any prosthesis used to replace part or all
of the stomatognathic and/or craniofacial
structures
6
There are two ways of presenting an
overview of the subspecialty of maxillofacial
prosthesis. One way is by viewing the patient
‘being treated’ and the other is by the ‘type of
prosthesis’ that is prepared for the patient.
7
I ) Patient wise, they are classified as:
1. Surgical - The defect to be restored was created by a definitive surgical procedure. Ex: Cancer patients
2. Congenital - The defect is a result of congenital or developmental anomaly. Ex: cleft lip /palate and syndromes of head and neck.
3. Traumatic - The defect of the head and neck is a result of a traumatic experience in automobile accidents, industrial accidents or suicidal attempts.
8
II) By type of prosthesis, they can be classified as:
1. Extra oral - Facial restorations. Ex: Nasal
prosthesis, orbital, ocular auricular
2. Intra oral. Ex: Obturator, speech aids,
modified complete or partial dentures and
infant feeding prosthesis.
9
HISTORY:HISTORY:
Even before dentistry attained its status
as a profession, some surgeons had recognized
the limitations inherent in grafting tissue for
repair of certain maxillofacial deficiencies and
had argued the use of prosthesis as an alternate
method.
Artificial eye and foot found in Egyptian
mummy, the use of artificial eye and noses by
the Indians and the Chinese lead us to think that
they applied their skill to prosthetic restoration
also.
10
BEFORE 1600 ADBEFORE 1600 AD
Ambroise pare, (1510-1590) the famous
French surgeon appears to be the first medical
writer on this subject. He recommended a
prosthetic nose, which could be made of gold,
silver, paper and linen cloth glued together. He also
described the fabrication of an auricular prosthesis.
11
1600-18001600-1800
Maxillofacial prosthetics owes much to
Pierre fauchard (1678-1761). Fauchard made a
monumental contribution to prosthetic facial
reconstruction, he made a silver mask to replace
the lost portion of the mandible for a french
soldier. This prosthesis was constructed under the
direction of a military surgeon, in collaboration
with a silversmith for french artillery. The victim
later came to be known as the “GUNNER WITH
THE SILVER MASK”.
12
1800-19001800-1900
William Morton (1819-1868) also did some
pioneer work is Maxillofacial prosthetics. He
constructed a nose out of porcelain for a Boston
lady who had lost her own from a malignant
disease. Dr. Morton attached the nose to her
spectacles.
Frenchman Claude martin published a
book in 1819 and described using a ceramic
material to fabricate a nasal prosthesis.
13
1900-19401900-1940
Upham (1901), a Boston dentist described
the use of vulcanite rubber for the fabrication of
nasal and auricular prosthesis.
In time, however some workers showed
dissatisfaction with vulcanite due to their poor
color stability, translucency and rigidity.
14
In Germany (1913), the gelatin - Glycerin
compounds attracted much attention due to their
ease to manipulate, pliability, translucency and
adaptability of intrinsic coloring to match the
skin. But this material lasted only a few days or a
week.
Bulbulian Clarke then introduced
prevulcanized latex which was used with water
soluable dyes.
15
1940-19601940-1960
Acrylic resin polymers were introduced and
replaced older vulcanite rubber. Its translucency,
colorability and ease of processing was
attractive to most clinicians. Transparent
photographic paints, acrylic resin polymer stains,
water color, oil colors were also used.
16
1960- 19701960- 1970
Silicone elastomers were introduced
Barnhard was the first to use silicone and
coloring the facial prosthesis by combining a
silicone rubber base material with acrylic resin
polymer stains. Tashma used dry earth
pigments.. Schaaf described the use of artist oil
paint. Fine described the use of colored nylon
flocking
17
1970-19901970-1990
Different types of elastomers came into market.
Lontz – polysiloxane elastomers
Gonzalez - polyurethane elastomers
Lewis - Siphenylenes
Turner - isophorone polyurethane
Drane and udagama - Silastic medical adhesive
silicone type A
18
1990- to present1990- to present
Advances in polymer chemistry has renewed
interest in developing new materials
Gentleman-polyphosphazenes
Silicone block polymers
19
REVIEW OF LITERATURE
20
Aziz T, Waters M, Jagger R J. Biomed Mater
Res B Appl Biomater. 2003; 65 :252. Development
of a new poly(dimethylsiloxane) maxillofacial
prosthetic material.
A new poly(dimethylsiloxane) material with
improved mechanical properties was compared to
commercially available materials. The formulations
developed were based on condensation chemistry
containing a hydroxy-end-blocked
poly(dimethylsiloxane), hydrophobic silica filler,
silane cross-linking agents, and a tin catalyst.
21
A formulation was developed with a base
polymer mix of 80%:20% high- to low-molecular-
weight polymers into which 20% w/w filler was
added. This formulation had a tear strength
better than compared to the commercial
materials
22
Bellamy KE, Waters MG. Biomed Mater Eng. 2005;15:21-7. Designing a prosthesis to simulate the elastic properties of skin.
They discussed a three-layered maxillofacial prosthesis consisting of a silicone rubber base layer, an inner gel layer and an outer polymeric coating (to simulate the elastic properties of skin). Gels were made by the addition of both low and high molecular weight unreactive silicone fluids. The results of the study shows that the gel produced, closely simulates the elastic properties of skin when bonded to a base silicone rubber layer. Further clinical trials are needed.
23
FOR MODELING OF AN EXTRA-ORAL IMPRESSION
• Conventional method (using impression material)
• CT and MRI
• 3-D optical scanner (light source)
24
IMPRESSION MATERIALS
PLASTER OF PARIS
Highly accurate in reproducing details
But it is lengthy and time consuming technique.
Used mainly to reinforce alginate impression.
25
RUBBER BASE IMPRESSION MATERIAL
Provides good details
Mainly for intra oral use
Expensive
26
ALGINATE
Most widely used
Excellent reproduction of details
Overall cost is reasonable
27
Disadvantage of conventional impression
Discomfort to the patient.
Deformation of the soft tissue because of the
weight caused by the impression material.
Master cast for the reconstruction of the orbital
defects usually show the remaining eye closed,
so the technician must rely on other data (e.g.-
photographs) for the design of the orbital
structures.
Testing ability of the clinician.
28
CT AND MRI
The difficulties encountered while using
impression material was overcome by the use of
CT AND MRI
CT AND MRI scan the defect area and a CAD
model of the defective area and the prosthesis
pattern is designed. The prosthesis pattern is
obtained by a procedure known as rapid
prototyping.
29
Disadvantage
Radiation is more with CT
Length of the time that the patient is required to
be exposed and remain motionless- during MRI
scanning
30
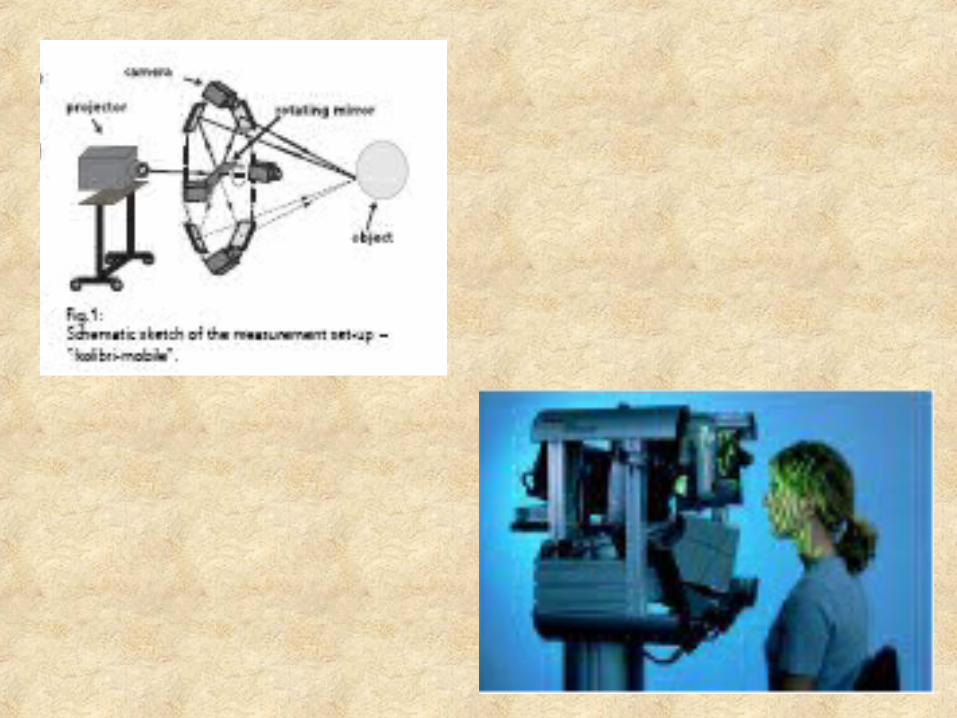
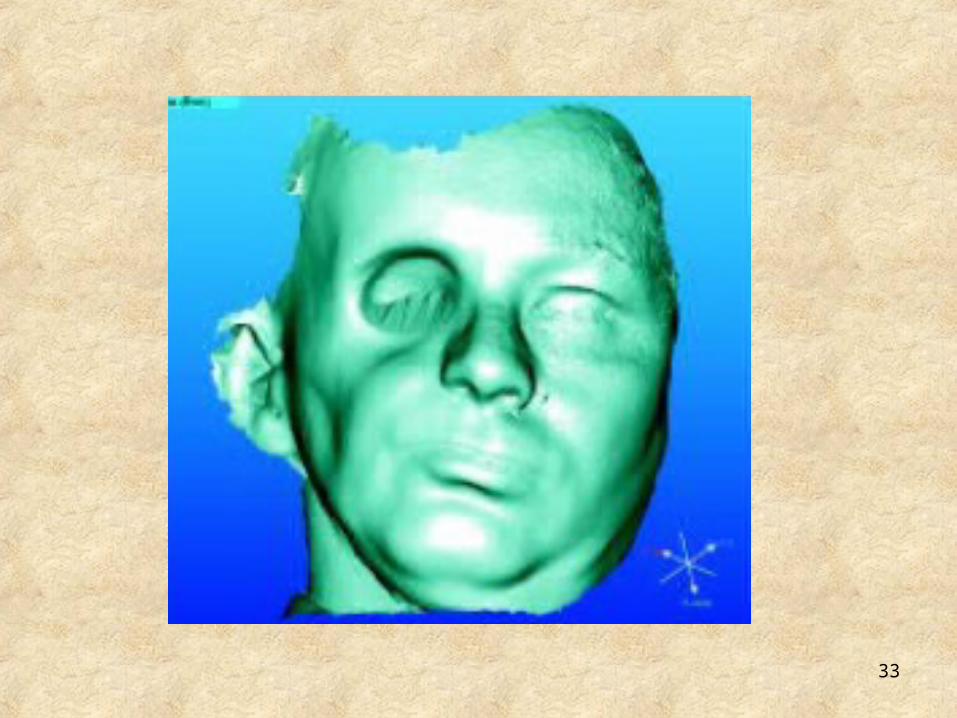
OPTICAL THREE DIMENSIONAL SCANNER
Newer device used to scan the facial defect
and reproduce a model
It is a mobile multi-view 3D measuring
system based on self calibration projection
technology.
It facilitate the fully automatic recording of
the body parts from various direction in one
measuring process
31
32
A transmission grating with parallel lines
inside the projector produced a fringe pattern on
the face
These pattern are recorded by camera and
transmitted to the PC
The generated CAD model is converted
into a physical model by means of a rapid
prototyping procedure.
33
34
ADVANTAGE
The body parts are exposed to light and
recorded optically.
Time taken for measurement-10 to 20 seconds.
Accuracy- 100µm.
35
RAPID PROTOTYPING
Rapid prototyping, operate on the principle
of depositing materials in layers or slices to build
up a model rather than forming a model from a
solid block. The use of a CT OR MRI allows
parts of the body to be serially recorded slice by
slice. Similarly, an object can be reproduced
slice by slice using the three dimensional
computed data in conjunction with a rapid
prototyping machine
36
STEREOLITHIOGRAPHY
It is a method of rapid prototyping that
uses data obtained from CT OR MRI scan
stored in 3-dimensional form
37
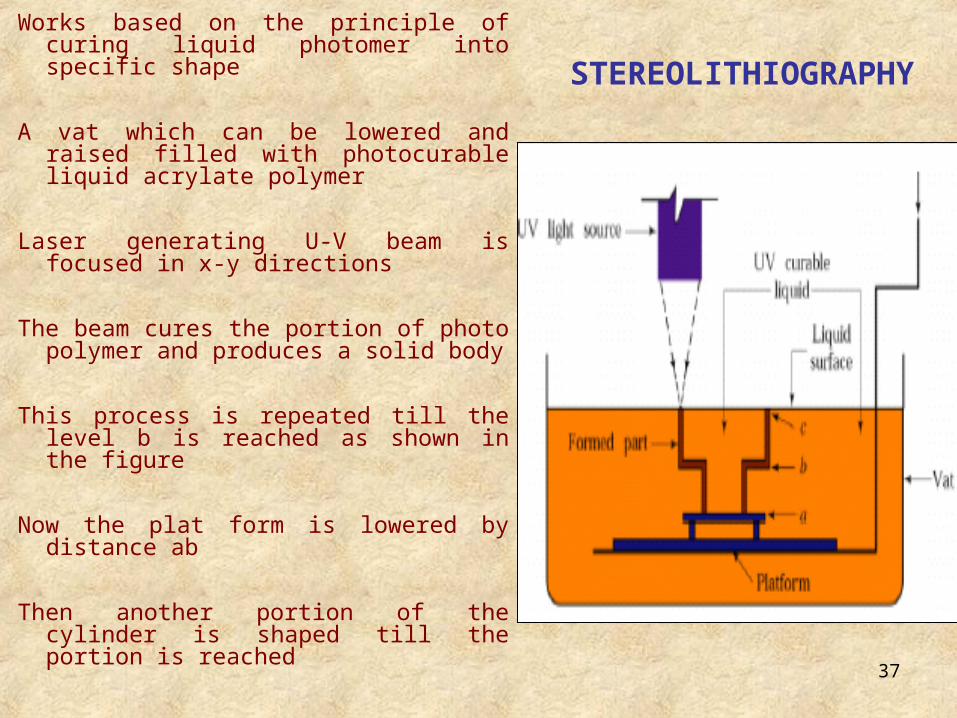
Works based on the principle of curing liquid photomer into specific shape
A vat which can be lowered and raised filled with photocurable liquid acrylate polymer
Laser generating U-V beam is focused in x-y directions
The beam cures the portion of photo polymer and produces a solid body
This process is repeated till the level b is reached as shown in the figure
Now the plat form is lowered by distance ab
Then another portion of the cylinder is shaped till the portion is reached
STEREOLITHIOGRAPHY
38
MATERIALS USED IN MAXILLOFACIAL
PROSTHESIS
39
Generally an ideal material should have the following characteristics –
Non-toxic. Odorless. High tear strength. High edge strength. Ease of processing. Dimensionally stable during and after processing. Ease of intrinsic and extrinsic coloring with
commercially available colorants. Ease of repair and refabrication if needed.
40
Chemically inert after processing.
Non-porous after processing.
Long shelf life.
Long working time.
No water sorption.
Translucent.
Softness compatible to tissue.
Usable life of two years or more.
41
A number of materials are available and have been used for facial prosthesis. The materials currently in use are:
I. ACRYLIC RESINS
The material is readily available and most dentists are familiar with its physical to chemical properties and processing techniques. These materials can be successfully employed in specific types of facial defects particularly those in which little movement occurs in the tissue bed during function.
42
Heat polymerizing MMA is preferred over
the autopolymerizing form because of the
presence of free toxic tertiary amines in the later.
Facial prosthesis made of this material remains
serviceable up to 2 years but required
occasional repainting of the surface. With age,
however the prosthesis becomes shiny and
crazing is noted.
43
Advantages:
a. Both intrinsic and extrinsic coloration can be
performed.
b. Has good edge strength
c. Alterations can be easily affected.
d. Compatible with most adhesive systems
e. Color stability is good in heat polymerized MMA.
f. Can be easily relined with tissue conditioner of
denture liner.
44
Disadvantages:
a) Rigidity, therefore its usefulness is
compromised in highly movable tissue beds
leading discomfort and expose of margins.
b) High thermal conductivity.
c) Duplication is not possible because of
destruction of the mould during removal from
flasks.
45
II. ACRYLIC CO-POLYMERS
Conta and Hildested did extensive study on this material but did not receive wide acceptance, despite being soft and elastic because of a number of objectionable properties like poor edge strength, poor durability, degradation when exposed to sunlight.
Disadvantages:
Processing and Coloration are difficult.
The completed restoration often tacky, predisposing to dust collection and staining
46
III. VINYL POLYMERS AND COPOLYMERS
a. Commonly marketed as (Realistic and Mediplast, prototype III)
Is a flexible plastic material basically plasticized polyvinyl Chlorides (PVC) or copolymer of Polyvinyl acetate.
The primary deficiency arises from the leaching of the plasticizer and resulting hardening of the prosthesis.
The lifespan as reported by Castleberry (1973) has been extended to 9-11 months.
47
Advantages:
Adaptable to both extrinsic and intrinsic
coloration.
Flexible.
Disadvantages:
Migration of plasticizer leading to discoloration
and hardening.
Easily get stained when exposed to ultra-violet
light, peroxide and ozone.
48
Poor edge strength.
Tend to absorb sebaceous secretions,
cosmetics and solvents.
They soil easily because of surface tackiness.
Metal moulds are required, as curing is
accomplished at high temperatures
49
IV. POLYURETHANE ELASTOMERS:
(Epithane - 3)
These elastomers are called so because they
contain urethane linkages. They arise from two
major reactants. In the presence of a catalyst, a
polymer terminating with an isocynate is combined
with one terminating with a hydroxyl group. Varying
the amount of isocynate will change the physical
properties of the final product.
50
They are quite elastic and flexible
especially well suited to defects with movable
tissue bed.
Isocynate are moisture sensitive and when
water contamination occurs, gas bubbles causes
defects and poor curing of the material. The
reaction must be carried out in a dry
atmosphere. The processing temperature is
100o C.
51
Advantages:
Good edge strength.
Can be colored both intrinsically and
extrinsically.
Superior cosmetic results when compared to
other materials currently available.
Stone molds are acceptable but care should be
taken to thoroughly dehydrate before
processing.
52
Disadvantages:
Difficult to process consistency.
Isocyanides, as these compounds are toxic and
moisture sensitive due to which gas bubbles can
accumulate and cause defects and poor curing.
Extrinsic coloration tends to wear off rapidly.
Clinically, the life range from minimum 3 months
to maximum 6 months.
Poor compatibility with existing adhesive
systems.
53
V. SILICONE ELASTOMER
The silicones are probably the most widely used
materials for facial restoration. Silicones are a
combination of organic and inorganic
compounds. The first step in their production is
the reduction of silica to elemental silicon. Then
by various reactions the silicone is combined
with methyl chloride to form dimethyl
dichlorosixane, which when it reacts with water
forms a polymer.
54
These polymers are translucent, watery
white fluids whose viscosity is determined by
length of the polymer chain. Polydimethyl
Siloxane commonly referred to as silicone is
made from these silicone fluid polymers. Most
rubbery forms are compounded with fillers that
provide additional strength. Additives are used to
provide color. Antioxidants and vulcanizing
agents are used to transform the raw mass from
or plastic to a rubbery -resin during processing.
55
The long-chained polymer which is cross-
linked create a network that can be separated
only with difficulty. This network makes the
silicones especially resistant to degradation from
UV light exposure.
56
The process of cross-linking the polymers
is referred to as vulcanization. Vulcanization
occurs both with and without heat and depends
on the catalytic or cross-linking agents utilized.
Depending on the method of vulcanization, two
forms are available:
1. Those that require heat - Heat vulcanized
(HTV)
2. Those that vulcanize at room temperature-
Room temperature vulcanized (RTV)
57
Silicones are classified into four groups according
to their application
1. Implant grade- material that can be implanted
interstitially.
2. Medical grade- for external use eg-
maxillofacial silicones.
3. Clean grade.
4. Industrial grade- both are used for industrial
application.
58
Heat Vulcanized Silicones (HTV):
Supplied as one component or two component putty.
The catalyst or vulcanizing agent is
dichlorobenzoyl peroxide or platinum salt,
depending on the type of polymerization.
Various amounts of filler are added to these
polymers depending on the degree of hardness,
strength and elongation desired. The more filler, the
harder and less resilient the compounded rubber will
be.
59
The filler is very pure finely divided silica
with a particle size of about 30.
Co-Polymers like methyl vinyl or methyl
phenyl siloxy radical are added for softness
and tear strength.
Advantages:
a. Exhibit excellent thermal stability.
b. Color stable.
c. Biologically inert.
60
Disadvantages:
a. Do not posses sufficient elasticity to function in
movable tissue bed.
b. Poor edge strength.
c. Are opaque and have lifeless appearance.
61
Room temperature silicones (RTV)
It is a viscous silicone polymer that
includes a filler and catalyst, which also acts as
cross-linking agent.
Stannous octoate is the common catalyst
used.
Filler, like diatomaceous earth are added
to increase strength.
The properties of RTV are similar to the
HTV types, except for the ease of processing of
RTV’s.
62
Advantages:
Same as HIV Silicones.
Easy to process and stone molds can be used.
Disadvantages:
Same as HTV silicones except for its ease in
processing.
63
FOAMING SILICONES
It is a form of RTV silicone. They reduce the weight of prosthesis because of formation of bubbles within the mass.
The basic silicone has an additive so that a gas is released, when catalyst stannous octoate is introduced. The gas forms bubbles within the vulcanizing silicone. After the silicone is processed, the gas is eventually released leaving a spongy material. And the formation of bubbles within the mass can cause the volume to increase by as much as seven times.
64
DISADVANTAGE
Has reduced strength.
Susceptible to tearing.
Because of these problems its use is limited.
65
VI. SIPHENYLENES: (polytetramethylsiphenylenesiloxanedimethylsiloxane)
These belong to silicone family that contain methyl and phenyl group.
It is a pourable, viscous, room temperature vulcanizing liquid.
Three component kit
Consist of a base resin
crosslinking agent- tetrapropoxysilane
catalyist- organotin
Siphenylenes elastomers feels like skin.
66
Are biocompatible, resistance to degradation on exposure to ultraviolet light and heat.
Have good edge strength and colorability.
Advantage:
Edge strength and colorability is superior to silicones.
Disadvantages:
Not enough clinical trials have been done due to limited research on this material.
High cost.
67
SILICONE BLOCK POLYMERS
Developed to improve some of the weakness of
silicone elastomers.
Incorporates poly methyl methacrlyate into
silicone block.
Has been found to be more tear resistant than
conventional cross linked silicone polymers.
68
POLYPHOSPHAZENES
It has been developed for resilient denture
liner.
Properties of this material is been modified
to satisfy the requirements for fabrication of
maxillofacial material.
69
AUXILLARY MAXILLOFACIAL MATERIALS:
Primers
These are used to promote bonding of silicone and other maxillofacial material.

70
FACIAL PROSTHETIC
ADHESIVES
Facial prosthesis
may be retained by
mechanical means or
by the use of
adhesives.
71
No one adhesive will behave in the same
way to different patient. This mainly due to
adhesive reacting to various skin types, ie oily,
dry, flaky etc and each skin type will exhibit
varying degree of retention.
72
They can be classified as
Pastes. (PSA 1)
Liquids [paintable (pros-Aide, DC-355) or
spray-on (DC MED)].
Double sided tapes( 3M biface tape).
73
TISSUE CONDITIONING
Used to prevents the skin damage when
removing the adhesives. It forms a protective
barrier.
Comfeel protective film
It contains ethoxyethyl acid co-polymer ethyl
acetate
When applied it forms a chemical film that is
compatible with adhesives, so increasing the
adhesion qualities of the prosthesis to the skin
74
Skin prep protective dressing (Smith & Nephew
Inc) are used to enhance the prosthesis
adhesion and to protect the skin from trauma.
Composition
Isopropyl alcohol.
Butyl esters of poly vinyl methacrylate/ methyl
methacrylate copolymer.
Acteyl tributyl citrate
75
Technique of application of adhesives
Apply the adhesive to 6 to 7mm of the
periphery of the fitting surface
To prevent the break down of the fine thin
edges, leave the last 4mm without any
adhesives, instead Vaseline may be applied to
them to make the margin disappear
76
ADHESIVE REMOVER
The biggest
problem as far as the
patient is concerned is
the removal of the
remaining residual
adhesive from the skin.
77
Plaster remover.
Zoff prosthetic cleanser. Trichloroethane
Thackeray cleanser.
Acetone.
Krylon medican spirit gum remover
Uni-solve adhesive remover
Isoparaffin.
Isopropyl alcohol.
Dipropylene glycol methyl ether.
Aloe extract.
78
Technique of removal
To remove the prosthesis
Lift the edge using a cotton bud or gauze
soaked in the remover, slowly working around
and under the fitting surface, lifting the
prosthesis away from the skin as you go.
79
To clean the adhesive from the skin
Soak a piece of gauze in the remover and
by gently rubbing and turning the gauze
constantly. Finish off by washing with soap and
water.
80
To clean the prosthesis
Initially rub the thumb over the fitting
surface, causing the adhesive to “ball” for easy
removal. Finally use the gauze soaked in
remover to clean the fitting surface.
If still traces of adhesive remain soak the
prosthesis in the solvent for one or two minutes
and then use a gauze swab.
81
DISCUSSION
Since the sixteenth century acquired surgical
defects have been restored by prosthetic
replacements constructed from a variety of
materials and techniques. The cosmetic and
functional disabilities following radical surgery for
oral and paraoral cancer are significant and
disabling. Definitive reconstruction should be
performed wherever possible as part of the
ablative procedure.
82
When definitive reconstruction is
coordinated and combined with maxillofacial
prosthetic rehabilitation, head and neck defects
can be restored to near-normal function and
appearance in many cases. The traditional
concept of a one-time prosthesis that supplies the
patient's requirements through the course of life
is no longer realistic or valid.
83
Identification of the variable factors that
influence the serviceability of prostheses for the
treatment of jaw defects is important and useful
information for the patient, the family of the
patient, the rehabilitative team, and third-party
payers.
84
CONCLUSION
Jaw defects affect many vital functions
(that is, respiration, mastication, deglutition,
speech, and aesthetics). Ideally, any anatomic
defect should be surgically reconstructed.
However, when surgical reconstruction is
contraindicated, prosthetic reconstruction must
be employed to restore anatomy, function, and
aesthetics.
85
Effective communication between the
surgeon and the maxillofacial Prosthodontist is
essential for developing a realistic treatment plan
or rehabilitation of patients undergoing resection.
Preoperative consultations allow the
prosthodontist to make recommendations to the
surgeon to achieve better prosthetic results.
86
The team concept, in which the head and
neck surgeon, speech pathologist, radiation
oncologist, maxillofacial Prosthodontist, and
other members of the health profession function
together in planning the rehabilitation and
primary modes of therapy, ensures the patient's
early and successful rehabilitation
87
REFERENCE Maxillo Facial Rehabilitation – Prosthodontic and
surgical consideration.
JOHN BEUMER. Clinical Maxillofacial Prosthetics -
THOMAS D. TAYLOR. Prosthetic rehabilitation-
KEITH F THOMAS.
88













![The manufacture of a maxillofacial prosthesis from an ... · PDF fileand medical industries, and multi-axis machining is mainly used to produce them [9]. Nevertheless, ... of the NX-Siemens-PLM](https://img.pdfslide.net/doc/110x75/5ab180677f8b9a1d168cc062/the-manufacture-of-a-maxillofacial-prosthesis-from-an-medical-industries-and.jpg)