Embed Size (px)
DESCRIPTION
A COMPARARATIVE EFFECT OF MATRABASTI AND SNEHAPANA (SHAMANA SNEHAPANA) WITH SUKUMARAKUMARAKA GHRITA IN THE MANAGEMENT OF VATASHTILA (BENIGN PROSTATE HYPERPLASIA).” VIJAYAMAHANTESH. M. HUGAR Post graduate department of Panchakarma,Shri D. G. Melmalagi Ayurvedic Medical College,Gadag – 582103.
Citation preview

By
VIJAYAMAHANTESH. M. HUGAR
Dissertation Submitted to the Rajiv Gandhi University Of Health Sciences,Karnataka, Bangalore.
In partial fulfillment of the requirements for the degree of
AYURVEDA VACHASPATHI M.D. (PANCHAKARMA)
In
PANCHAKARMA
Under the guidance of
Dr. P. Shivaramudu,M.D. (Ayu)
And co-guidance of
Dr. Shashidhar. H. Doddamani,M.D. (Ayu)
Post graduate department of Panchakarma, Shri D. G. Melmalagi Ayurvedic Medical College,
Gadag – 582103.
2006.
“A COMPARARATIVE EFFECT OF MATRABASTI AND
SNEHAPANA (SHAMANA SNEHAPANA) WITHSUKUMARAKUMARAKA GHRITA IN THE MANAGEMENTOF VATASHTILA (BENIGN PROSTATE HYPERPLASIA).”
Rajiv Gandhi University Of Health Sciences, Karnataka, Bangalore.
DECLARATION BY THE CANDIDATE
hereby declare that this dissertation / thesis entitled
“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana
Snehapana) with Sukumarakumaraka Ghrita In the Management ofSnehapana) with Sukumarakumaraka Ghrita In the Management ofSnehapana) with Sukumarakumaraka Ghrita In the Management ofSnehapana) with Sukumarakumaraka Ghrita In the Management ofSnehapana) with Sukumarakumaraka Ghrita In the Management of
Vatashtila (Benign Prostate Hyperplasia).”Vatashtila (Benign Prostate Hyperplasia).”Vatashtila (Benign Prostate Hyperplasia).”Vatashtila (Benign Prostate Hyperplasia).”Vatashtila (Benign Prostate Hyperplasia).” is a bonafide and genuine
research work carried out by me under the guidance of
Dr.P.Shivaramudu, M.D. (Ayu), Professor, Post-graduate department of
Panchakarma and co-guidance of Dr. Shashidhar. H. Doddamani, M.D.(Ayu),
Assistant Professor, Post graduate department of Panchakarma.
Date:Place:
I
VIJAYAMAHANTESH. M. HUGAR
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entit led
“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana
Snehapana) with Sukumarakumaraka Ghrita In the ManagementSnehapana) with Sukumarakumaraka Ghrita In the ManagementSnehapana) with Sukumarakumaraka Ghrita In the ManagementSnehapana) with Sukumarakumaraka Ghrita In the ManagementSnehapana) with Sukumarakumaraka Ghrita In the Management
of Vatashtila (Benign Prostate Hyperplasia).”of Vatashtila (Benign Prostate Hyperplasia).”of Vatashtila (Benign Prostate Hyperplasia).”of Vatashtila (Benign Prostate Hyperplasia).”of Vatashtila (Benign Prostate Hyperplasia).” is a bonafide research
work done by VIJAYAMAHANTESH. M. HUGAR in partial fulfillment
of the requirement for the degree of Ayurveda Vachaspathi. M.D.
(Panchakarma).
Date:
Place: Dr. P. Shivaramudu, M.D. (Ayu).
Professor
Post graduate department of Panchakarma.
ENDORSEMENT BY THE H.O.D AND PRINCIPAL OF
THE INSTITUTION
This is to certify that the dissertation entitled
“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana
Snehapana) with Sukumarakumaraka Ghrita In the ManagementSnehapana) with Sukumarakumaraka Ghrita In the ManagementSnehapana) with Sukumarakumaraka Ghrita In the ManagementSnehapana) with Sukumarakumaraka Ghrita In the ManagementSnehapana) with Sukumarakumaraka Ghrita In the Management
of Vatashtila (Benign Prostate Hyperplasia).”of Vatashtila (Benign Prostate Hyperplasia).”of Vatashtila (Benign Prostate Hyperplasia).”of Vatashtila (Benign Prostate Hyperplasia).”of Vatashtila (Benign Prostate Hyperplasia).” is a bonafide re-
search work done by VIJAYAMAHANTESH. M. HUGAR under the
guidance of Dr.P. Shivaramudu, M.D. (Ayu), Professor, Postgraduate depart-
ment of Panchakarma and co-guidance of Dr. Shashidhar.H. Doddamani,
M.D. (Ayu), Assistant Professor, Post graduate department of Panchakarma.
Dr. G. Purushothamacharyulu, M.D. (Ayu) Dr. G. B. Patil.
Professor & H.O.D, Principal.
Post graduate department of Panchakarma.
CERTIFICATE BY THE CO- GUIDE
This is to cert i fy that the dissertat ion enti t led
“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana“A Compararative Effect of Matrabasti And Snehapana (Shamana
Snehapana) with Sukumarakumaraka Ghrita In the ManagementSnehapana) with Sukumarakumaraka Ghrita In the ManagementSnehapana) with Sukumarakumaraka Ghrita In the ManagementSnehapana) with Sukumarakumaraka Ghrita In the ManagementSnehapana) with Sukumarakumaraka Ghrita In the Management
of Vatashtila (Benign Prostate Hyperplasia).”of Vatashtila (Benign Prostate Hyperplasia).”of Vatashtila (Benign Prostate Hyperplasia).”of Vatashtila (Benign Prostate Hyperplasia).”of Vatashtila (Benign Prostate Hyperplasia).” is a bonafide re-
search work done by VIJAYAMAHANTESH. M. HUGAR in partial
fulfillment of the requirement for the degree of Ayurveda Vachaspathi.
M.D. (Panchakarma).
Date: Dr. Shashidhar.H. Doddamani, M.D. (Ayu).
Place: Assistant Professor,
Post graduate Department of Panchakarma.
COPYRIGHT
Declaration by the candidate
I hereby declare that the Rajiv Gandhi University of Health
Sciences, Karnataka shall have the rights to preserve, use and
disseminate this dissertation / thesis in print or electronic format
for academic / research purpose.
Date:
Place:
© Rajiv Gandhi University of Health Sciences, Karnataka.
VIJAYAMAHANTESH. M. HUGAR
i
ACKNOWLEDGEMENT “Many hands make light work”. I take this opportunity to mention my deep
gratitude to several personalities who have helped me in the successful completion of this
work.
I express my obligation to my honorable H.O.D, Dr. G. Purushothamacharyulu
M.D. (Ayu), H.O.D., P.G. Department of Panchakarma, P.G.S&R, D.G.M.A.M.C, Gadag
for his critical suggestions and expert guidance for the completion of this work.
I express my obligation to my honorable guide Dr. P. Shivaramudu M.D (Ayu),
Assistant Professor, for his critical suggestions and expert guidance for the completion of
this work.
I am extremely grateful and obliged to my co-guide Dr. Shashidhar.H.
Doddamani, Asst. Professor, P.G.S.&R, D.G.M.A.M.C, Gadag for his guidance and
encouragement at every step of this work.
I express my deep gratitude to Dr .G.B Patil, Principal, D.G.M.A.M.C, Gadag,
for his encouragement as well as providing all necessary facilities for this research work.
I express my sincere gratitude to Lecturer Dr. Santhosh. N. Belavadi MD (Ayu),
Lecturer for their sincere advices and assistance.
I express my sincere gratitude to Dr. V. Varadacharyulu M.D (Ayu), Dr.M.C.Patil
M.D (Ayu), Dr. Dilip Kumar M.D. (Ayu), Dr. Mulgund M.D (Ayu), Dr. K.S.R.Prasad
M.D. (Ayu) (Osm), M.A. (Jyotish), Dr. R.Y.Shettar M.D. (Ayu), Dr. Kuner Sankh M.D.
(Ayu), Dr. Girish Danappagoudar Dr. Jagadish Mitti M.D. (Ayu), Dr. Shashidhar
Nidagundi M.D. (Ayu) and other PG staff for their constant encouragement.
I express my sincere gratitude to Dr. Venkatesh S. Karanth M.D. (Patho) D.N.B.
Lecturer Shri. Nandakumar (Statistician), for their sincere advices and assistance.
I also express my sincere gratitude to Shri. V.M. Mundinamani (Librarian), Dr. S.
D. Yerageri, Dr. D. M. Patil, Dr. S. A. Patil, Dr. P.C. Chappanamath, Dr. M. V. Aiholi,
Dr. B. S. Patil, Dr. S. B. Govindappanavar, Dr. B. G. Swamy, Shri. C.S. Bhatt, Dr. U. V.
Purad, Dr. Mallagoudar, Dr. R.K. Gachhinmath, Dr. G.S. Hiremath, Dr. Avvani, Dr. S.
H. Radder, Dr. C. S. Hiremath, Dr. Juktihiremath, Dr. Kudarikannur, Dr. R.R. Joshi, Dr.
K.S. Paraddi, Dr. V. M. Sajjan for their support in the clinical work.
i
ii
Shri. B.S. Tippanagoudar (lab technician), Shri. Basavaraj (X-ray technician), Mr.
Shavi, Mr. Nabhi, Mr. Kulkarni, Mr. Hatti and other hospital and office staff for their
kind support in my study.
I express my sincere thanks to my colleagues and friends Dr. Ratna Kumar, Dr.
Uday Kumar, Dr. Jayaraj Basarigidad, Dr.P.Chandramouleeswaran, Dr. Kendadamath
Dr. Shaila. B, Dr. Santhosh.L.Y, Dr. Subin Vaidyamadham, Dr. Febin .K. Anto, Dr,
Satheesha.R, Dr., Dr. K. Krishnakumar, Dr. Ashwini Dev, Dr. Suresh Hakkandi, Dr.
Vijay Hiremath, Dr. Manjunath Akki, Dr. L. R.Biradar, Varsha.S. Kulkarni, Dr.
Hadimani, Dr. C. S.Hanumanta Gouda, Dr.Shankargouda, and other post graduate
scholars for their support.
I also express my obligations to my friends Dr. B.L. Kalamath, Dr. Venkareddy,
Dr. Basavaraj Ghanti, Dr. Pradip, Dr. Sajjan, Dr. Ashok Bhingi, Dr. Umesh Kumbar, Dr.
Devendrappa Budi, Dr. Shubu Prasad, Dr. Ashok M.G., Dr. Payappagouda, Dr.
Madhushri, Praveen. Dr. hemanta. Manju. Kushi. Kittu. etc.
I acknowledge my patients for their wholehearted consent to participate in this
clinical trial. I express my thanks to all the persons who have helped me directly and
indirectly with apologies for my inability to identify them individually.
I am highly thankful to my parents Shri. Mahadevappa D. Hugar & Smt.
Sarojadevi M. Hugar for her constant help and encouragement throughout the work. I am
also thankful to my beloved brother Mr. Vasanth Mrs. Geetha for their constant support
and encouragement.
Date : VIJAYAMAHANTESH. M. HUGAR.
Place : Gadag.
ii
iii
List of Abbreviations Used
⇒ A. Hr.. – Ashtanga hridaya.
⇒ A. S. – Ashtanga samgraha.
⇒ B. P. – Bhavaprakasha.
⇒ B. R. – Bhaishajya ratnavali.
⇒ Ch. – Charaka.
⇒ C. S. – Charaka samhitha.
⇒ G. N. – Gada nigraha.
⇒ H. S. – Hareetha samhitha.
⇒ M. N. – Madhava nidana.
⇒ No. – Number.
⇒ Pt.’s – Patients.
⇒ Sl. – Serial number.
⇒ S. S. – Sushruta samhitha.
⇒ Su. – Sutrasthana.
⇒ V. S. – Vangasena samhitha.
⇒ Y. R. – Yogaratnakara.
⇒ Sk. D. – Shabdakalpadruma.
⇒ SKKG – Sukumaraka Kumaraka Ghrita.
iv
ABSTRACT
Obstruction at different levels in the urinary tract produces different effects.
Ayurveda too deals with the chapter of urinary obstruction under Mutraghata and also
principles of its managements. Here a sincere attempt is made to asses the efficacy of
Ayurvedic formulations in the conservative management of Vatashtila (BPH.)
Research begins with doubts and ends with facts, that serve as new data to be
verified again. Thus the process of research never ends, but at the end of it the researcher
would have become wiser with plans to counter newer challenges.
The present study is “A Comparative effect of Matrabasti and as Shamana
Snehapana with Sukumara Kumarak Ghrita in the management of Vatashtila
(BPH)”
MatraBasti is one the most important among the Panchakarmas. It has already
been proved that the “Basti” is the choice of treatment Vata pradanavyadisas the
Vatashtila is one of the Vata pradanana vyadi. And Shamana Snehapana is indicated in
mutrakrachar, it is having importance to alleviates disease quickly.
Sukumara Kumaraka Ghrita is the name itself indicates, it is recommended for
Sukumaras viz old age persons without any hesitation .The ingredients viz- Dashamula,
Laghupanchamoola, Punarnava etc are having properties like Rasayana, Balya,
Shoolahara and Vatahara.etc which helps in correcting the pathology of Vatashtila
(BPH). Hence this study has under taken.
iv
v
Objectives Of The Study:-
1) To evaluate the effect of Sukumara kumaraka ghrita Matrabasti in the
management of Vataashtila (BPH).
2) To evaluate the effect of Sukumara kumaraka ghrita as Shamana snehapana in
the management of Vatashtila (BPH).
3) To compare the effect of Sukumsr kumaraka ghrita Matrabasti and as shamana
snehapana in the management of Vatashtila (BPH).
Clinically this study deals with the management of patients of Vatashtila (Benign
Prostatic Hyperplasia.). It is a common problem in who is men over 50years of age;
Approximately one half of 50 years, by the age of 60 years 50 % of men have histological
evidence of BPH, and an estimated three fourths of all men over the age of 60
experiences such symptoms as difficulty in initiating urinations, Nocturia, and frequency.
As life expectancy increases, primary care physicians will likely see significantly more
male patients with this disorder.
Vatashtila (BPH) is characterized by both Obstructive and Irritative symptoms.
The main severity of symptom is not correlated with the size of the prostate. Many men
with enlarged prostate have no symptoms whereas others, some times with lesser
enlarged, experience severe symptoms. The management of BPH is divided into Non-
operative treatment, Conventional operative treatment and Minimally invasive treatment.
All these considerations provided a firm launch pad to make excursion into the
therapeutic alternatives, which could be provided by Ayurveda, the Mantra of
“NIRAMAYA” Therefore a set of therapeutic procedures was designed to assess its
efficacy on symptomatology of BPH.
v
vi
In this present work the schedule of treatment was as follows –
30 patients are selected and are randomly categorized into two groups.
Group 'A' – 15 patients with Matrabasti with Sukumara Kumarak Ghrita, 8 days
Matrabasti with 70ml of Ghrita, 16 days for pariharakala total study duration was 24
days.
Group 'B' – 15 patients with Shaman Snehapana with Sukumara Kumarak
Ghrita, 16 days Shaman Snehapana with 30ml Ghrita, divided dose twice Daly up to 16
days and 8 days for pariharakala total study duration was 24 days.
Subjective parameters:
Cardinal symptoms of Vatashtila (BPH).viz – Ashtila vatha Ghanam Ghranthi,
Mala, Mutra, Anila Sanga, Adhmana, Sashula yukta mutratyaga. And American
Urological Association Symptoms Index & (I-PSS).
Objective parameters:
Digital Rectal Examination and Ultrasonography.
Response of the treatment:
Subjective complaints were relieved significantly in the range of 38.88% patents from
good respond after the completion of Matrabasti in Group A, and 22.22% of patients are
from moderate respond, where as 22.22% of patients are from poor respond.
In the objective parameter 6.66% good respond, 26.66% poor respond. Comparing the
subjective and objective parameter, subjective parameter is having better effect.
In Group B the range of relief was observed from subjective parameter 55.55% is
poor respond, 11.11%is moderate respond. Where as objective parameter among 15
patients there is no any respond has seen. Comparing the subjective and objective
parameter, group-A and group-B, group-A (Matrabasti) is having better effect.
vi
viii
TABLE OF CONTENTS
Chapters Page No.
1. Introduction 1-4
2. Objectives 5-9
3. Review of literature 10-81
4. Methodology 82-104
5. Results 105-137
6. Discussion 138-168
7. Conclusion 169-171
8. Summary 172-173
9. Bibliography 1-16
10. Annexure 17-31
ix
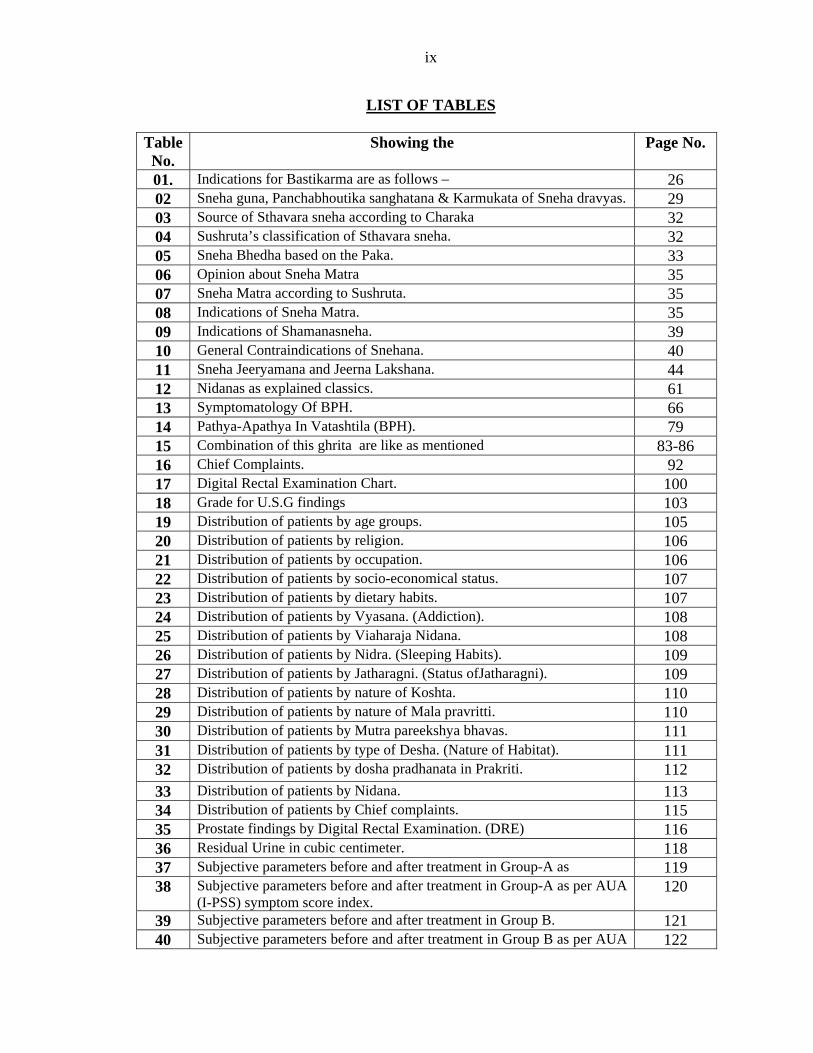
LIST OF TABLES
Table No.
Showing the Page No.
01. Indications for Bastikarma are as follows – 26 02 Sneha guna, Panchabhoutika sanghatana & Karmukata of Sneha dravyas. 29 03 Source of Sthavara sneha according to Charaka 32 04 Sushruta’s classification of Sthavara sneha. 32 05 Sneha Bhedha based on the Paka. 33 06 Opinion about Sneha Matra 35 07 Sneha Matra according to Sushruta. 35 08 Indications of Sneha Matra. 35 09 Indications of Shamanasneha. 39 10 General Contraindications of Snehana. 40 11 Sneha Jeeryamana and Jeerna Lakshana. 44 12 Nidanas as explained classics. 61 13 Symptomatology Of BPH. 66 14 Pathya-Apathya In Vatashtila (BPH). 79 15 Combination of this ghrita are like as mentioned 83-86 16 Chief Complaints. 92 17 Digital Rectal Examination Chart. 100 18 Grade for U.S.G findings 103 19 Distribution of patients by age groups. 105 20 Distribution of patients by religion. 106 21 Distribution of patients by occupation. 106 22 Distribution of patients by socio-economical status. 107 23 Distribution of patients by dietary habits. 107 24 Distribution of patients by Vyasana. (Addiction). 108 25 Distribution of patients by Viaharaja Nidana. 108 26 Distribution of patients by Nidra. (Sleeping Habits). 109 27 Distribution of patients by Jatharagni. (Status ofJatharagni). 109 28 Distribution of patients by nature of Koshta. 110 29 Distribution of patients by nature of Mala pravritti. 110 30 Distribution of patients by Mutra pareekshya bhavas. 111 31 Distribution of patients by type of Desha. (Nature of Habitat). 111 32 Distribution of patients by dosha pradhanata in Prakriti. 112 33 Distribution of patients by Nidana. 113 34 Distribution of patients by Chief complaints. 115 35 Prostate findings by Digital Rectal Examination. (DRE) 116 36 Residual Urine in cubic centimeter. 118 37 Subjective parameters before and after treatment in Group-A as 119 38 Subjective parameters before and after treatment in Group-A as per AUA
(I-PSS) symptom score index. 120
39 Subjective parameters before and after treatment in Group B. 121 40 Subjective parameters before and after treatment in Group B as per AUA 122
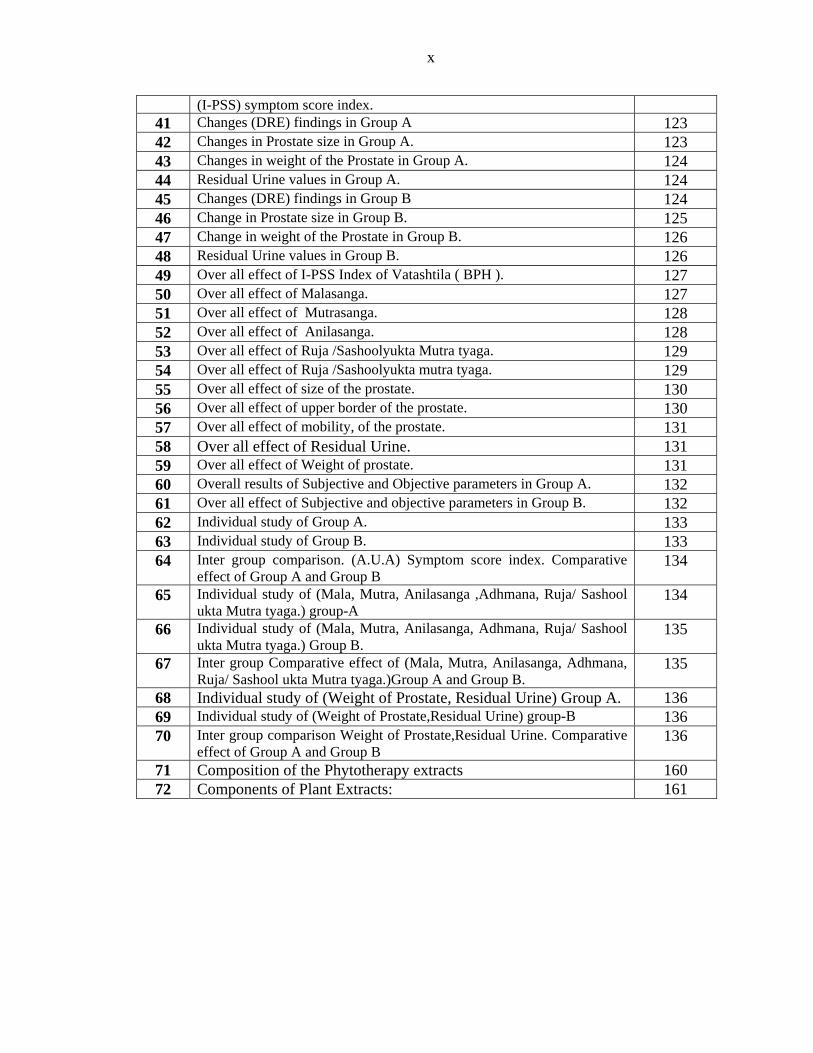
x
(I-PSS) symptom score index. 41 Changes (DRE) findings in Group A 123 42 Changes in Prostate size in Group A. 123 43 Changes in weight of the Prostate in Group A. 124 44 Residual Urine values in Group A. 124 45 Changes (DRE) findings in Group B 124 46 Change in Prostate size in Group B. 125 47 Change in weight of the Prostate in Group B. 126 48 Residual Urine values in Group B. 126 49 Over all effect of I-PSS Index of Vatashtila ( BPH ). 127 50 Over all effect of Malasanga. 127 51 Over all effect of Mutrasanga. 128 52 Over all effect of Anilasanga. 128 53 Over all effect of Ruja /Sashoolyukta Mutra tyaga. 129 54 Over all effect of Ruja /Sashoolyukta mutra tyaga. 129 55 Over all effect of size of the prostate. 130 56 Over all effect of upper border of the prostate. 130 57 Over all effect of mobility, of the prostate. 131 58 Over all effect of Residual Urine. 131 59 Over all effect of Weight of prostate. 131 60 Overall results of Subjective and Objective parameters in Group A. 132 61 Over all effect of Subjective and objective parameters in Group B. 132 62 Individual study of Group A. 133 63 Individual study of Group B. 133 64 Inter group comparison. (A.U.A) Symptom score index. Comparative
effect of Group A and Group B 134
65 Individual study of (Mala, Mutra, Anilasanga ,Adhmana, Ruja/ Sashool ukta Mutra tyaga.) group-A
134
66 Individual study of (Mala, Mutra, Anilasanga, Adhmana, Ruja/ Sashool ukta Mutra tyaga.) Group B.
135
67 Inter group Comparative effect of (Mala, Mutra, Anilasanga, Adhmana, Ruja/ Sashool ukta Mutra tyaga.)Group A and Group B.
135
68 Individual study of (Weight of Prostate, Residual Urine) Group A. 136 69 Individual study of (Weight of Prostate,Residual Urine) group-B 136 70 Inter group comparison Weight of Prostate,Residual Urine. Comparative
effect of Group A and Group B 136
71 Composition of the Phytotherapy extracts 160 72 Components of Plant Extracts: 161
xi
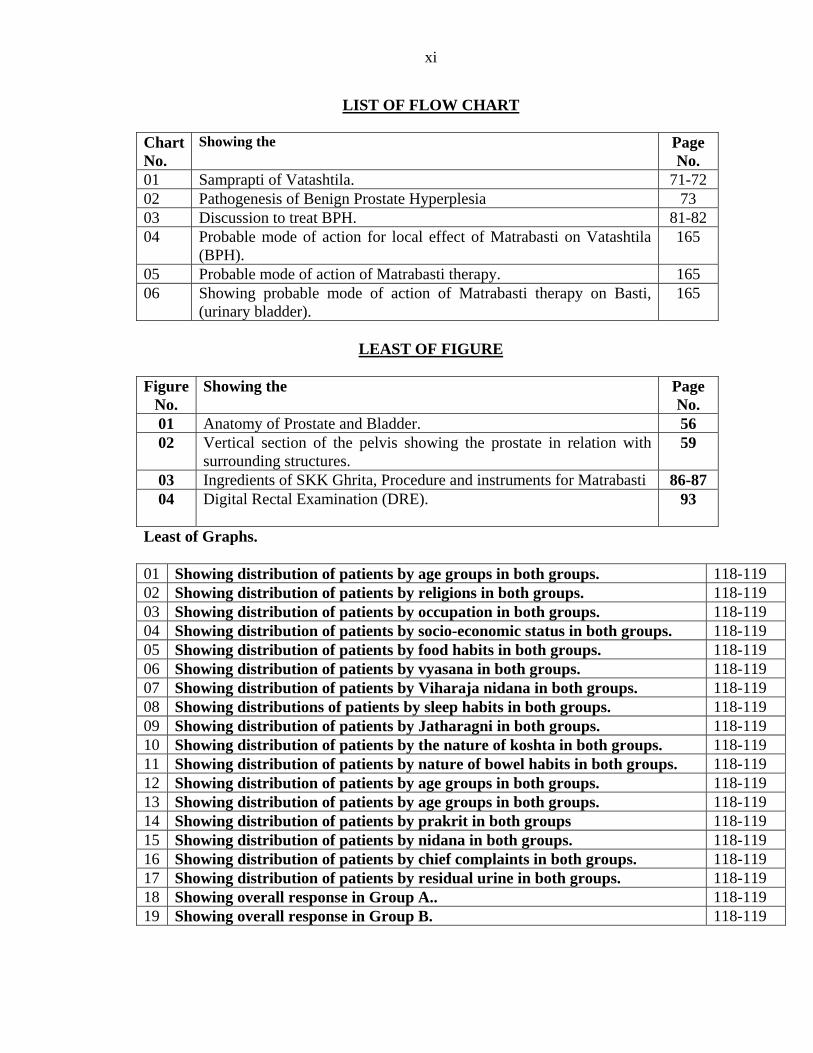
LIST OF FLOW CHART Chart No.
Showing the Page No.
01 Samprapti of Vatashtila. 71-72 02 Pathogenesis of Benign Prostate Hyperplesia 73 03 Discussion to treat BPH. 81-82 04 Probable mode of action for local effect of Matrabasti on Vatashtila
(BPH). 165
05 Probable mode of action of Matrabasti therapy. 165 06 Showing probable mode of action of Matrabasti therapy on Basti,
(urinary bladder). 165
LEAST OF FIGURE
Figure No.
Showing the Page No.
01 Anatomy of Prostate and Bladder. 56 02 Vertical section of the pelvis showing the prostate in relation with
surrounding structures. 59
03 Ingredients of SKK Ghrita, Procedure and instruments for Matrabasti 86-87 04 Digital Rectal Examination (DRE). 93
Least of Graphs. 01 Showing distribution of patients by age groups in both groups. 118-119 02 Showing distribution of patients by religions in both groups. 118-119 03 Showing distribution of patients by occupation in both groups. 118-119 04 Showing distribution of patients by socio-economic status in both groups. 118-119 05 Showing distribution of patients by food habits in both groups. 118-119 06 Showing distribution of patients by vyasana in both groups. 118-119 07 Showing distribution of patients by Viharaja nidana in both groups. 118-119 08 Showing distributions of patients by sleep habits in both groups. 118-119 09 Showing distribution of patients by Jatharagni in both groups. 118-119 10 Showing distribution of patients by the nature of koshta in both groups. 118-119 11 Showing distribution of patients by nature of bowel habits in both groups. 118-119 12 Showing distribution of patients by age groups in both groups. 118-119 13 Showing distribution of patients by age groups in both groups. 118-119 14 Showing distribution of patients by prakrit in both groups 118-119 15 Showing distribution of patients by nidana in both groups. 118-119 16 Showing distribution of patients by chief complaints in both groups. 118-119 17 Showing distribution of patients by residual urine in both groups. 118-119 18 Showing overall response in Group A.. 118-119 19 Showing overall response in Group B. 118-119
hen the hair becomes gray and scanty when speaks of earthy matter begin
to be deposited in the tunica of the artery and when white zone is formed at the margins
of cornea, at this same period the prostrate gland usually. I might perhaps say invariably
becomes increased in size. it is the statement of “SIR BENJAMIN BODIE”.
W
In Ayurveda, there are two main treatment principles explained i.e. (1) Shamana
(2) Shodhana. The Panchakarma comes under the Shodhana, because of their nature, i.e.
elimination or purification methods. It has been mentioned, the diseases which have been
treated with shodhana therapy, will alleviate the disease from its root cause Na-tesham
Punarudbhavaha. The panchakarma techniques have the prime importance in the
treatment, as well as in the two goals of Ayurveda i.e. Swasthasysa Oorjaskara and
Aturasya Roganut.
Ayurveda considered Jara chikitsa i.e. science of geriatrics as one of the eight
divisions of Asthanga Ayurveda. Ayurveda perceives ageing as a special entity and laid
down its own multidimensional treatment approach towards it, which stresses on Vata
pacification along with the nourishment of depleted Dhatus, by means of Rasayana and
Vajikarana. The phenomena of ageing is considered in an entirely new angle, by this
eternal science. Total life span is considered as hundred years by our Aacharys in their
classics.
Different stages of ayu are –
Balya avastha (before 16 years)
Madhyama avastha (16-60 years)
Vridha avastha (after 60 years)
Introduction 1
Last phase of life span is considered as jara, which is natural and inevitable
process as the age advances and is associated with its own disorders. During this period
naturally depletion in Dhatu, Indriya, Veerya, Bala And Ojus occurs, gradually. As age
advances loss of hairs, wrinkling on skin of whole body, senile cough, and short breath
appears.
As per Ayurveda Jaravastha is associated with vitiation of vatadosha and is more
prone to Vatavyadi’s. Vatashtila is one of the vata predominant disease, which succeeds
with old age. Acharyas susrhutha explained Vatashtila under vata vyadi nidana in first
chapter.
Ageing is defined as the “Sense of a progressive generalized impairment of function
resulting in a loss of adaptive response to stress and growing risk of age related diseases” is
expected that with the present rate, in early part of next century, we will be having around
25% of population in a geriatric group. Among the geriatric problems major systems
involved are central nervous system, cardio vascular system and third major is urinary
system. Common urinary diseases which affects elderly men is Benign Prostatic
Hyperplasia. (BPH)
Vatashtila is one of the Mutraghata which explained by all Brahatries and
Laghutries. Acharya Charaka has explained it in Siddhisthana 9th chapter of
“Thrimarmeeyasiddhi” and considered as one of the Bastigata vikara, but not as a type of
Mutraghata. Acharya Sushruta and others explained regarding Vatashtila, in the context of
Mutraghata. The diseases like Vatashtila, and Mutragranthi, which are having similar signs
and symptoms to that of BPH. Out of the two, the signs and symptoms of Vatashtila are in
resemblance to BPH. Vatashtila manifests mainly due to the derangement of Apanavata,
which is responsible for normal voiding of function. There by produces stone like swelling
“Ashteelavath Ghanam Granthi” which is firm, Sthira and Unnatha. Manifesting between the
Guda and basti pradesha, it leads to bahirmrga avarodini means obstruction of Mutra, Anila,
Purisha and Adhmana.
Introduction 2
NEED FOR STUDY
The long-term exposure to drug induced adverse events and the prohibitive costs are
the primary limitations of prevention therapy of BPH. In addition, effective medical and
surgical therapy exists when BPH ultimately does becomes clinically evident. Because there
is no clinically evidence, biochemical, or genetic predictors of BPH development or
progression. So every male is at risk. The ability to identify those individuals who are
predisposed to develop clinical BPH refractory to medical therapy would provide a more
compelling rational for prophylaxis. There is evidence that men with very large prostates are
at greater risk for developing urinary retention. (Jacobsen et al, 1997)
As the high incidence of disease Vatashtila (BPH) in elderly men, at the beginning of
the 4th decade of life, 8% of men have histopathological Benign Prostatic Hyperplasia. 50%
of men aged 51 to 60 yrs, and 90% of the men over the age of 80 yrs. Have histological
evidence of benign prostatic hyperplasia. Approximately 23 million men world wide suffer
from moderate to severe BPH.
In the management of Vatashtila (BPH), which is the out come of vitiated vata,
Acharyas gave importance to the Sneha as the choice of treatment. because Sneha is having
antagonistic properties to that of Vata. The Basti and Sneha are indicated in Mutrakricchra
and Mutraghata. In general Matrabasti is the major and effective treatment modality which is
easy to administer and can be given to old age persons without any complications. Shamana
snehapana is having the capacity to do the Shamana of the Vikaras, “Shigram”
Doshanukarshani, Sarvamarga i.e. Koshta, Sandi, Marma, Shaka, Sancharini and is
Balya, Punarnavikari, Sharira, Indriyachetasam, which is widely indicated in gulma,
Mutrakrichra, Gadhavarchas, etc. (Ch. Su. 13., Uttama Matra) (A. Hr. Su. 16/19) There
by these two remedies i.e. Matrabasti and Shamana snehapana are considered as the best
treatment options to treat Vatashtila (BPH).
Introduction 3
In contemporary system of medicine various surgical approaches have been practiced
to relieve this embarrassing disorder of BPH. because medicines are practically of no avail.
Even surgery is not supposed to be an ideal treatment owing to various complications
associated with operative problems, hemorrhage etc. Incontinence of urine is noted in several
of cases post-operatively, which is more frustrating than the disease itself. The patient
doesn’t want to be treated surgically in the first instance, rather he prefers non-invasive
therapy. Acharyas elaborated the different kinds of treatment modalities regarding the
treatment of various types of Mutravaha Srotovikaras, Mutravikaras. In the management
of Vatashtila Acharya Susrhuta mentioned, Swedana, Abhyanga, Basti Uttara basti, and
Kashaya, Kalka, and Sarpi. Susrhuta specifies treatment for Vatashtila in 5th chapter of
Chikitsa Sthana and he emphasizes to that of Gulma and Abhyantara Vidradivat Chikitsa
(5th Cha. Chi.) to be carried out with regards to Vatashtila.
Sukumara kumaraka ghrita is indicated in Mutrakricchra Chikitsa in the textbook
of Chakradutta and Bhaishajyaratnavali which is best Vatahara, Balya, Rasayana and
Vedana shyamaka. With regard to this Sukumara Kumaraka ghrita was considered for
this present clinical study as Matrabasthi and shamana Snehapaana in Vatasthila (BPH).
Introduction 4
To evaluate the effect of Sukumarakumaraka ghrita Matrabasti in the management of
Vatashtila (BPH).
To evaluate the effect of Sukumarakumaraka ghrita as Shamana snehapana in the
management of Vatashtila (BPH).
To compare the effect of Sukumsrkumaraka ghrita Matrabasti and as shamana
snehapana in the management of Vatashtila (BPH).
The goals of treatment for Vatashtila (BPH) include relieving – LUTS,
Decreasing BOO (Bladder Outflow Obstruction). (Mutra sanga)
Improving bladder emptying. (Mutra sanga)
Ameliorating destrusor instability.(Mutra sanga)
Reversing renal insufficiency.
Preventing future episodes of gross hematuria.
Urinary tract infection and Urinary retention. (Mutraghata)
Preventing future episodes of gross hematuria, (Raktha mutrata)
In our classics there is no explanation about anatomical structure of Vatashtila as
well as BPH but acharya Sushruta has mentioned the term Pourusha which can be
compared with Prostate gland.
In Ayurveda Vatashtila is closely resembles to the BPH according to its location
and signs and symptoms. Vatashtila is one of the Vata pradhna vyadhi, incidence
of both are in old age persons, obstruction induced changes in detrusor muscle
function, compounded by age related changes in both bladder and nervous system
function, lead to urinary frequency, urgency and nocturia. Old age which is
inevitable stage of life also acts as Nidana for Vatashtila which is one among
Vatavyadhi. (A. Hr. Su 1/8).
Objectives of the Study 5
In the classics there is no explanation about Sadhasadhyata for Vatashtila.
But by considering, in general Mutraghata are difficult to cure due to involvement
of Basti marma.
Where as in contemporary system of medicine, there is no satisfactory treatment
modalities in controlling the symptoms and preventing the complications of the
BPH. They include α blockers, androgen suppressants, aromatase inhibitors and
phytotheraphy, i.e. the plant extracts.
However surgical intervention is Prostectomy, even today it is the ultimate choice
of treatment, then also not recommendable. Because most of the patients in late
sixties and seventies, the risk for cardiovascular diseases, hypertension, diabetes
mellitus are high, serious post operative complications like hemorrhage, infective
processes such as Cystitis, and also delayed complications like urge or stress
urinary incontinence. Therefore by considering the contraindications of surgery,
risk of surgery and very less satisfactory results by the hormonal treatment. On
the aim of one should get rid of age related disorders like Vatashtila (BPH), here
an attempt has made with Panchakarma modalities to find a better solution to
maintain the normal life in old age also.
1) “To evaluate the effect of Sukumarakumaraka ghrita Matrabasti in the
management of Vatashtila (BPH)”.
Matrabasti is best treatment for old age persons, because of its less dose and
minimum complication. The drug of Matrabasti is sneha, as it is perfectly
antagonistic to the Vata and the disease Vatashtila is vatadosha pradhana vyadhi
(Apanavata).
Objectives of the Study 6
Matrabasti is selected, as the Apanavata is prime cause for the disease and the seat
of Apanavata is “Apano apanaga shroni basti medhrorugocharaha.” The
administered Basti dravya stays in Pakvashaya and it will reach to the affected
area quickly by the Anupravaranabhava of Sneha and the properties of ingredients
like Dashamoola, Laghupanchamoola, Punarnava, Ashwagandha etc, as the
affected area is near to the Pakvashaya.
Hypothetically the Matrabasti can bring vitiated doshas to balanced state, severity
of the signs and symptoms of the Vatashtila (BPH) may reduce.
2) To evaluate the effect of Sukumara kumaraka ghrita as Shamana
snehapana in the Management of Vatashtila (BPH).
Shamana snehapana, is having the capacity to (Ch. Su. 13 cha. Uttama
Matrasneha ) spared all over the body immediately and it can restore the normal
health.
Shamana snehapana is indicated in Gulma, Mutrakricchra etc, as the Sneha is the
best vatahara, it can be used for the treatment of Vatashtila (BPH).
By the virtue of active principles of Sukumara kumaraka ghrita it can spread all
over the body and reach the affected area, does the shamana of the disease.
3) To compare the effect of Sukumara kumaraka ghrita Matrabasti and as
Shamana snehapana in the management of Vatashtila (BPH).
Sukumara Kumaraka Ghrita is the name itself indicates, it is recommended for
Sukumaras viz old age persons without any hesitation. The ingredients viz.-
Dashamooula, Laghupanchamoola, Punarnava etc are having properties like
Rasayana, Balya, Shoolahara and Vatahara, etc., which helps in correcting the
pathology of Vatashtila. (BPH).
Objectives of the Study 7
As Basti is the prime treatment for the Vatavyadhies and Vatavyadhies are
generally correlated with Neurological disorders, by correcting the Apanavata
inturn it acts on the nervous system related to the prostate because normal
function of the Apanavata is the normal function of voiding.
This study has undertaken with the hypothesis that the Matrabasti is having better
results than the Shamana snehapana because as already mentioned the affected
area is near to the Pakvashaya.
This study has under taken to compare the effect of Sukumara kumaraka ghrita
Matrabasti and as Shamana Snehapana in the management of Vatashtila (BPH).
To evaluate the effect of two groups, among two which is best treatment by
assessing the before and after treatment datas of the study.
Ayurvedic preparations, which are having minimal side effects and no
complications, even in aged persons also can be given.
Acharya Susrhuta mentioned, Gulma and Abhyantara Vidradivat Chikitsa for
Vatashtila (BPH).
The main aim of the present study is not only reveals the symptoms of the
Vatashtila (BPH) but also induce reduction in size and weight of the prostate and
decreases the residual urine.
LIST OF FEW STUDIES CONDUCTED
The research papers published by Rashatriya Ayurveda Vidyapeetha in March, 2003.
1) Ashtila Vyadhi ka (Prostate enlargement) ayurvediya upachara. By Dr.
Prakashshraj Singh, Dr. Dayanandan Mana and Ach. Jyotirmita, Varanasi
2) Management of Benign Prostatic Hyperplasia (Vatashtila) in Panchakarma
theatre with reference to Vasti, By - Dr. Anand, Belgaum.
Objectives of the Study 8
3) Ayurvedic therapy in the management of Benign Prostatic Hyperplasia
By Dr. Shivji Gupta, Dr. Ramesha Bhat, and Dr. M. Sahu, Varanasi.
4) Role of Varunadi Kashaya in the management of Benign Prostatic Hyperplasia.
By Dr. Praveen Kumar, and Dr. K. K. Sijoria, Delhi.
5) Poursh granthi vriddhi ki Ayurvedic chikitsa - Ek aturia adhyayan.
By:- Dr. B. P. Gupta, Delhi.
6) A clinical study on Yavnalkshaya and Chandraprabhavati in Mutrasanga
(Retention of urine w.s.r.t. B.P.H. - Pundir R.K. (1984).
7) A clinical study on Mutraghata (Relation of urine w.s.r. to Mutraghata (B.P.H.) -
Raut S.Y. (1987)
8) Role of Punarnavadi compound in the management of Mutraghata w.s.r. to B.P.H.
Jagruti Joshi (1995)
9) Clinical evaluation of Kshara and Uttar Basti in the management of Mutraghata -
Akasha Kembhavi (1998)
10) Role of Mustadi Kalpa in the management of Mutraghata w.s.r. to B.P.H. - Dr.
Ashish B. Soni (1999)
11) A Clinical study on the role of Devdarayadi Kshaya and Dashmool Siddha Taila
Uttar basti in the management of Mutraghata w.s.r. to B.P.H. - Dr. N.H. Kulkarni
(2002).
12) Some of scholars in Contemporary system of medicine they tried Phytotherapy
(plant extracts) in BPH/LUTS. They have gained widespread usage since about
1990 among them (Plosker and Brogden, 1996), (Gormley et al, 1992),
(Disilverio et al, 1998), (Lowe and Fagelman1999).
Objectives of the Study 9
HISTORICAL REVIEW
Historical view is an essential part of the literature in which review is done about
the past events. Ayurveda starts since ancient period, before going to write any treatises
in Ayurveda. It would be a judicious to review the references of Vedas and Samhitas.
The Vedas are the first written documents of human civilization. Therefore the
available information can be formulated as follows –
A. Vedic Kala – 2500 B.C. – 1000 B.C.
B. Samhita Kala – 1000 B.C. – 100 A.D.
C. Sangrahakala – 100 A.D. – 800 A.D.
D. Aadhunika Kala – 17 A.D. – onwards.
Veda kala
There is so many reference we can get in Vedas especially Atharva Vada
explanation Basti, (1/3/7Ater) “Vishitam te Vastibilam . . . . . . this type of explanation
are available but there is no explanation regarding Vasti Karma in Vadas.1
Samhitas kala:-
All classical treatises of Ayurveda have emphasized the importance of Bastikarma
and Matrabasti as the most effective therapeutic measure than any other such methods
prescribed for various ailments especially in the diseases occurring due to Vatadosha.
Acharya Charaka has described the Bastikarma, its usage, dosage, advantages,
complications, and indications with different yogas, in Charaka samhitha Siddhisthana
(1stchap. 4,5,7,8,10,12.).2 Sushruta has elaborately described the Bastikarma procedures,
about Bastiyantra, types of Bastis, complications, management, in different chapters of
kalpasthana3 and Chkistasthana- (35,36,37chapters) Acharya Vagbhata has explained the
bastikarma in Ashtangasangraha and Ashtangahridaya like Avastha Anusrutabastis,
Prasrutikabastis and Vyapaths.4, 5, 6.
Historical Review 10
Madhyama kala
Sarngadharasamhita also has given much importance to Bastikarma with the
Brihatriyee’s methods of explanations in Uttarakhanda (5 to 7 chapters) including
Uttarabasti. Yogaratnakara, Bhavaparakasha dealt the bastikarma, and added newer
combinations to the Ayurvedic world for a better practice.7 Acharya Kashyapa equated
the Bastikarma as Amrutam in first chapter of Siddhisthana, because of its wide
applications even in both infants and old age.8
Later, modern authors in Ayurveda has also elaborately explained the Bastikarma,
modifications of Bastiyantra, converted the older measurements to the present day
measurements and made the things easier for the practitioners.
SNEHA
Veda Kala
In Rigveda description of many herbal plants and qualities of Tila Pinji Tilataila,
Sarshapa, are available. The Atharvana veda, gives plenty of references regarding the use
of Sneha therapeutically.9
Samhita Kala
In Charaka samhita references regarding the therapeutically use of Sneha in
various disorders. The author has devoted an entire chapter in the Sutra Sthana on
“Shadvidopakramas.”10 (Ch. Su. 22nd) Snehana as Pradhana karma is the most significant
therapeutic procedure. Among them Charaka has extensively dealt with the subject
“Snehana” and its Qualities, doses, time sedulous, advantages, complications, and
indications, separately in 13th chapter of Sutrasthana,11 and about Shodhananga snehana
in Charaka siddhisthana.12 Here he has described in detail the properties of Sneha
dravyas, basic sources of Sneha dravya, indication and contraindications of Snehana etc.
Historical Review 11
Acharya Sushruta has contributed separate chapter on “Sneha” in 31st chapter of
Chikitsasthana. Here he has classified Snehana on the basis of its Karmukata as
Shodhana, Shamana and Brumhana and explained the preparation of “Sneha” i.e. Ghrita
and Taila.13 Also we found that number of references regarding the uses of sneha in the
Shodhana and Shamana or alleviation of different diseases. Types and qualities of Ghrita
and Tailas, method of preparations of Aushadhisiddha ghritas and method of
administration have been mentioned in Sutrasthana and Chikitsasthana of Astanga
Hridaya.14
Kasyapa an eminent personality in Koumarabhritya has dealt in detail regarding
Snehana in 22nd chapter of his Sutrasthana and added use of different ghrita and taila in
managing various Balarogas.15 Bhela one of the six celebrated disciples of Atreya has
mentioned the use of different Sneha in treating different disorders.16 Qualities of each
taila their specific indications have been mentioned in 14th chapter in Harita samhita.17
Later others like Yogaratnakara18, Bhavamishraa19, Sharangadhara20, Vangasena
and Chakrapani they explained Paryayas, Swaroopa, Utpattisthana, Gunas of Ghrita and
Taila and their indications.
Adhunika Kala
Detailed explanation about uses of both animal product ghee and plant products
oils, in materia medica and added classification of fats, oils, properties and sources of oil
expression of oils, have been mentioned. Textbook of pharmacognocy, Teiz’s text book
of clinical Biochemistry, etc are the textbooks where literary review regarding the use of
sneha can be obtained clinically.21
Historical Review 12
VATASHTILA
Vedic period
In vedic period there is no explanation about Vatashtila, but we can get references
of Mutraghata. A comprehensive description regarding Mutraghata, and its treatment
with the use of “Loha Shalaka” this kind of references give as account of the knowledge
that our ancestors had with regards to the anatomical, physiological, pathological and
therapeutic aspects of the human body. (A.V.1-3-1 to 4 & 6 to 9).
Another one important references in treating the Mutraghata in Atharvaveda is
explained as “Mutramoochana.” Atharvana veda22 is treasure house of mantras and they
can be linked to nuclear energy, among the innumerable mantras. This type of
explanation we can get in Ayurveda also. i.e. Acharya Sushruta declares that student
desires of studying Ayurveda should be initiated into the regular practice of “Gayatri
Mantra” and Acharya Charaka also mentioned chanting of “Vishnusahasranama” in
Sannipataja jwara.
Samhita kala
This was the golden period of ayurveda and the two great works viz. Charaka
samhita and Sushruta samhita were written in this period. Acharya Charaka in 9th chapter
of Siddhisthana in the name of Trimarmeeyasiddhi adhyaya explained 13 types of Basti
sambhandi vyadhis among those Vatashtila is one of the mutravarodha janya vyadhi.23
Where as Sushrut explained 12 types of Mutraghata, Nidanapanchaka laxanas and
Chikitsa eloberately,24 particularly for Vatashtila in the 1st chapter of Vatavyadhi
Nidadana25 and also 5th chapter of Chikitsasthana.26 Ashtanga sangrahakara, Ashtanga
hridayakara including Kashyapa fallowed the same view of Charaka and Sushruta.27
Historical Review 13
Madhyama kala
The important work has been done in the text book of Chakradutta28 and
Bhishajyaratnavali29 have given more concentration over Chikitsa with different Yogas in
the context of Mutrakricchra and Mutraghata chikitsa. Other Acharyas Vangasena,
Yogaratnakara contributed over Mutraghata. The commentators of Chakrapani,
Gangadhara and Dalhana have fulfilled their commentary for the better understanding of
the Samhitas.
Historical Review 14
Yutpatti and Nirukti of Basti
The word Basti is derived form ‘vas + tich’ and is masculine gender.
“Vasu nivase”30 - Means residence.
“Vas-aachadane” - That which gives covering.
“Vas vasane surabhikarane” - That which gives fragrance.
“Vasti vaste aavrunothi muthram” - That which covers the urine.
“Nabheradhobhage mutradhare” - The position of Basti is just below nabhi
(umbilicus) and is the collecting organ of
urine in the body i.e. urinary bladder.
Paribhasha
In the context of Panchakarma the term Basti is used in different sense.
“Vastina deeyate iti vasti”31
“Vastibhir deeyate yasmat tasmat vastiriti smritha”32
“Vastina deeyate vastini va Purvamanyattavasto vasti” 33
The term Basti means bladder. It is used as a device for Bastikarma. Hence, the
term Basti is used as a name in Panchakarma therapy to designate the process. The
medicated decoctions, milk, oil, ghee, mamsarasa of prescribed quantities are taken in
Basti and introduced into Gudamarga by means of a device Bastinetra after proper
pretreatment procedures.
SNEHA NIRUKTI
The word ‘sneha’ is derived from the root “sniha” with “Lute” pratyaya
Vachaspathyam.34 In general speaking the process in which “Snigdhata” of the body is
brought about is called as Snehana.
Vyutpatti & Paribhasha 15
.
The word Sneha is masculine gender and is derived from “Snih” Dhatu by suffix
“Lyut” Pratyaya
The verb root “Snih” has two implications –
• Snih – Preetau. to render affection.
• Snih – Snehane. to render lubrication.
The term Sneha implies that a substance that brings oiliness or unctuousness.
Sneha literally means oiliness, unctuousness, fattiness, greasiness, lubricity, viscidity,
affection, love, kindness and tenderness.35
PARIBHASHA
“Snehanam - sneha vishyandha mardhava kledakarakam”.36
Achrya Charaka defines, the Sneha indicates Snighata, Vishadana reffers to
vilayana, or fluidit. Vishyando Vilayana Chakrapani. Mardavata indicates softness, and
Kleda is moistness, which signifies the increase in apya guna of body. It means the
Snehana is the process by which Snigdhata, Vishyandana, Mardavata and Kledana are
produced in the body. These measures are adopted to bring about snigdhata in the body is
known as snehana.
The word Sneha is used to describe application of Sneha dravyas in Ayurvedic
text. It is refers to internal administration as well as external use of Sneha. There are such
specific nomenclature used for external application of sneha i.e. Abhyanga, Lepa, etc for
internal administration Shodhana poorva snehapana, Shamansneha and Brimhana sneha
such are used.
Hence which does the Shaman or normalizes the aggravated doshas all over the
body is Shamanasneha.37
Vyutpatti & Paribhasha 16
NIRUKTI OF VATASHTILA
ASHTILA :- Ashtila Uttarapathe Deergha Vartula Pashana Vishesha.38
Ashtila means it is situated in just above the Guda pradesha and below the Basti.
It is elongated, round, apple and stony like structure.
It is a feminine gender.
Meaning of Ashtila
It is a round bulk, stone, ball or globe like structure.
It is a globular swelling. 39
Ashtila is a type of Mutraghata vyadhi.
Mutra + Aghata = Mutraghata
Enn + Dhanya + Add = Aghata 40
PARIBHASHA
Astilavat Ghanam Granti Urdhwa Ayata Unnatam 41- means Ashtila is the hard,
round, stone like structure which is situated in between Vasti and Guda and its structure
resemblance to Urdhwa, Ayata,Unnata.
01. Yen mootra kricchre mootram kricchrena vahit |
Mootraghate mootram shoshyate partihanyate va ||
(Cha. Chi. 26\43-44 Chakrapani)
Means which is cause for the difficulty in micturation, which will dries up the
mutra and leads to its obstruction is known a Mutraghata.42
2) Mutraghate Tu Vibhandho Balavan Kricchratva | (Vijayrakshita)
The one which causes the obstruction of mutra and leads to difficult in
micturation.
Vyutpatti & Paribhasha 17
Paryaya and Bheda of Basti
• On the basis of Adhisthana - Pakwashayagata, Grabhashayagata,
Vranagata, Mutrashayagata.
• On the basis of Dravya - Nirooha, Anuvasana, Sneha, Matra.
• On the basis of Karmukata - Shodhana, Lekhana, Snehana, etc.
• On the basis of Samkhya - Kala, Karma, Yoga.
• On the basis of Anushangi - Yapanabasti, Sidhabasti etc.
But Charaka has used the term Basti exclusively for Nirooha as per the
commentary of Chakrapani.43 Similarly the term Basti has also been referred to the
method of Shirobasti, Urobasti, Janubasti, etc.
Synonyms of Sneha
The synonyms mentioned for Snehana are Sneha, Snigdhata, Mritkshana,
Abhyanga and Abhyanjana.44
Bheda of Vatashtila “Ashtila and prathya ashtila”45
Vyutpatti & Paribhasha 18
IMPORTANCE OF BASTIKARMA
Different Acharyas appreciated this form of treatment considering the efficacy it
generates. No other elimination therapy is equal to Basti because it expels the vitiated
doshas rapidly and easily from the body and also reducing as well as nourishing the body
very fastly. Though emesis and purgation eliminate the vitiated doshas form the body,
the drugs used in these therapies contain Katurasa, Ushnaguna and Teekhsna gunas,
which cannot be taken easily by children or older people. But Basti can be given in all
age groups without any hesitation.46
Bastikarma is the best method of treatment in dealing with Vatavikaras and Vata
dominating other Vikaras as Vata being the chief controller among the causative forces of
disease.47 As per the fundamental principles of Ayurveda; vata is responsible for every
movements and activities in the body whether it is of constructive or of destructive
nature. On the other hand Vata is functionally required to co-ordinate with Pitta and
Kapha in order to accomplish various duties assigned to them in the organization of life.48
Pakwasaya is considered to the seat of Vata. Direct application of this kind of
treatment to Pakwasaya helps for the proper regulation and co-ordination of the functions
of Vatadosha not only in its own site but also control the related doshas which are
involved in the pathogenesis of disease.49 Hence, it is considered as one of the appropriate
treatment for Vata predominant disease and also called it as Ardhachikitsa by Vagbhata.50
Apart form this, Basti is considered as superior to the other therapeutic measures on
account of its varied actions like Samshodhana, Samshamana and Samgrahana of doshas
on this basis of drugs used in it.51
Review of Bastikarma 19
Basti is indicated for providing rejuvenation, happiness, longitivity, strength,
improving memory, voice, digestive power and complexion. It removes noxious matters
form the tissues, pacifies the doshas and rectifies the process of excretion. Consequently,
it affords stability and thus indirectly strengthens the reproductive capacity in man.52
Kashyapa equated the bastikarma as ‘Amrutam’, because of its wide application even in
both infants and in old age.53
Classification of Basti
Basti is an important method of therapy in Ayurveda. For better understanding it
can be classified in various ways. We cannot find uniformity in classification of basti
among the authors of classical texts. Generally, the term Basti has been used for all types
of Bastikarma, which includes Nirooha, Anuvasana, Uttarabasti etc. But Charaka has
used this term Basti exclusively for Nirooha as per the commentary of Chakrapani.54
Similarly the term Basti has also been referred to the method of Shirobasti, Urobasti,
Vrina basti etc. So a rational thinking on various aspects of Bastikarma has brought about
the following classification.55
Adhishtana bheda – The site of application.
Dravya bheda – The medicinal preparations used.
Karma bheda – The action it does.
Sankhya bheda – The number of bastis given.
Anushangika bheda – Always associated
Matra bheda – Based on amount used.
1. Adhishtana bheda
According to the site of application of basti it is classified into two types –
a. Internal b. External
Review of Bastikarma 20
a. Internal
i) Pakwasayagata basti – The administration of medicine via ano-rectal route to
Pakwasaya.
ii) Garbhasayagata basti – The administration of medicine via vaginal route to
Garbhasaya.
iii) Mutrasayagata basti – The administration of medicine via urethral route to
Mutrasaya.
iv) Vrinagata basti – The medicine administered through the Vrinamukha by
the process of Bastikarma.
b. External
In certain diseases the medicated oil is kept over the part of the body using a cap
or with flour paste for prescribed period of time and named after the site of application of
oil such as – Shirobasti, Katibasti, Urobasti, etc.
2. Dravya bheda
It is based on the major ingredients of Bastidravya - kwatha or sneha and
so classified into two types: -
i) Nirooha basti – The main ingredient is Kwatha and it is the important type of
Bastikarma having varied therapeutic effects. The Basti is able to eliminate doshas form
the body and so called Nirooha. Also called Asthapana, as it is Vaya and Aayusthapaka
the Vikalpa of Nirooha basti are synonyms.56 The effect of Nirooha will spread all over
the body even in the cellular level and helps to eliminate the vitiated doshas adhered in
Srotases and its action in the body is beyond the perception of physician.57
Review of Bastikarma 21
ii) Anuvasana basti – Sneha is the chief ingredient of Anuvasana. The term
Anuvasana is coined due to the unharmful effect of the Bastidravya even if it is retained
inside the Koshta. More over this type of Basti can be practiced daily without any serious
precautionary measure, as it is less complications than nirooha.58
3. Karma bheda
Sushruta and Vagbhata have made the following classification according to their
actions.59,60
Shodhana basti – Contains shodhana dravyas and removes doshas and
malas from the body. malas from the body.
Lekhana basti – Reduces medodhatu and produces lekhana in the body.
Sneha basti – Contains more of sneha and produces snehana in the
body. body. body. body.
Brumhana basti – Increases the rasadi dhathus and indirectly it helps in the
growth of the body. growth of the body.
Utkleshana basti – Causes utklesha of malas and doshas by increasing its
Pramana and causes dra Pramana and causes dravabhootha.
Doshahara basti – Purificatory or eliminating type.
Shamana basti – Produces shamana of doshas.
Sharangadhara added, shodhana basti to it also he has added lekhana, brimhana,
deepana and pachana types of bastis.61 Vataghna basti, Balavarnakrita basti, Snehaneeya
basti, Sukrakrit basti, Krimighna basti, Vrushatvakrit basti has been explained in various
contexts by Charaka.62
Review of Bastikarma 22
4. Sankhya bheda
It is stated that neither snehabasti nor niroohabasti can be applied alone63 So,
Charaka has made this classification based on the number of snehabastis and
niroohabastis in a treatment.64
a) Karma basti – There are 30 numbers of bastis in this group out of which
snehabastis and niroohabastis are 18 and 12 respectively. Prescribed in chronic diseases
of prolonged nature and particularly of vata predominant.65 First 1 snehabasti then
alternate sneha and kashaya- each 12 and 5 snehabastis in the end.
b) Kala basti – There are 16 numbers of bastis. First basti is anuvasana,
then 6 nirooha and 6 anuvasana must be given alternately and in the end 3 anuvasana.
Indicated in patients of madhyamabala and vatapitta predominant conditions.66 However,
a difference of opinion regarding the number of nirooha is also prevailing.
c) Yoga basti – There are 8 numbers of bastis. 5 snehabastis and 3
niroohabastis. First basti is anuvasana, then 3 nirooha and 3 anuvasana and last 1
snehabasti. Indicated in diseases where involvement of vata dosha is found less.67
5. Matra bheda
This classification of basti is based on the quantity of bastidravya prescribed. The
quantity may vary according to the age, strength of the patient and severity of the
disease.68
a) Dvadashaprasruta basti – In nirooha, the maximum dose or quantity of
bastidravya prescribed is dvadashaprasruta i.e. 24 palas.
b) Prasritayogika basti – Charaka has prescribed various types of nirooha
in different doses like 4,5,6,7,8,9, and 10 prasrutas, considering the strength of the patient
and condition of the disease.69
Review of Bastikarma 23
c) Padaheena basti – In this type of basti, 3 prasrutas i.e. ¼ of
dvadashaprasruta is less form from the total quantity of nirooha used i.e. 9 prasruthis.
Anuvasana is also classified into 3 according to the difference in the quantity of
sneha70used.
Sneha basti – 6 palas (¼of total quantity of nirooha)71
Matra basti – The sneha that will be digested in 6 hrs if taken orally.72
Anuvasana basti – ½ of the quantity of sneha basti.73
6. Anushangika bheda
01. Yapana basti – Enhances bala, shukra and mamsa. Mostly employed in treating
the vyapats produced by excessive coitus. It can be given during all the seasons of the
years. It increases life span. Charaka has explained 26 bastis of this type. Kukkutamamsa,
ksheera, eggs, kwatha, madhu, ghrita, mamsarasa are should be added to prepare this.74
02. Siddha basti – The basti creates bala, varna, prasanata and it purifies more than
100 diseases.75
03. Yuktaratha basti – Mainly indicated for travelers on horse, different types of
vehicles etc.76
04. Vaitarana basti – It is explained by both Vangasena and Chakradutta. It is mainly
concentrating on the elimination of doshas. It has got wide applications.77
05. Ksheera basti – Explained for shoolam, vitsangam, anaha, murakrirchha.78
06. Ardhamatrika nirooha basti – No need for sneha sweda pratikriya. Sarvaroga
nivarana in nature, mainly rajayakhsma, shoola krimi, vatarakta. It improves sukha and
ojus and has the nature of pumsavana.79
Review of Bastikarma 24
07. Pichha basti – It is given with a drug called as Shalmaliniryasa. It produces
sthamba (stoppage) of pichasrava and jeevashonita. It is also called as Sangrahibasti.80
08. Mutra basti – Gomutra is the main ingredient and it has the qualities of mridu
in nature, pacifies all doshas and it is harmless.81
09. Rakta basti – When there is severe blood loss from the body, acharya has
advised to perform raktabasti that which stops the further blood loss and initiates the
production.82
Importance of Matrabasti
Matra + Basti = Matrabasti. The word meaning of matra.
Arunadutta, states for the word meaning of matra, “Matra Shabdasthara
Pramanarthaha”. (A. Hr. Su 16/25).83
The term Matra conveys many meanings such as measurement, quantity, size,
duration, number, degree, unit of time and moment, but here in this context Matra refers
to measure i.e. quantity of Basti dravya as Ashtanga Hridaya states that Hhrusva matra it
means Alpamatra of sneha, which is given in the name of Matra basti.84
Sushruta states that Matrabasti is Vikalpa of Anuvasana basti it means it is the
type of Anuvasana vasti.85
As per Ashtanga hrudaya “Hrusvaya Sneha Panasya Matrayam” from the above
statement it is clearly understand that it can be given at any age viz. Bala, Vridha, etc
even for Alpagni person also. It is not having any complications due to its less quantity
of Sneha. Hemadri used the term Sukha which gives meaning of easy to handle.86
According to Charaka “Yethashta Ahara Chestashya Sarva Kalam Nirathaiyah”
this quotation gives more importance to Matrabasti. Because during the administration of
Matrabasti it does not require any regimen like ahara chesta.. There is no any particular
time schedule for it.87
Review of Bastikarma 25
Ashtanga Hridaya gives the terms like Nishparihara. Arunadutta added the word
Aniyantrana means, there is no any restriction for the day today activities and no Parihara
kala also as explained for other Bastis. No restrictions of time to follow other procedures
after the administration of Matrabasti.88
Ashtanga sangrahakar states that “Sevyaha Sada Cha Madutailikavat”, it can be
restored to always just as Madhutailika basti.89
Properties of Matrabasti
Acharya Charaka explained benefits of Matrabasti as, it increases strength of the
body (Balya), easily administrable (Sukhopacharya) and no much restrictions after
administration, makes easy evacuation of bowel (Shrishta purishakrita), best for
Vatavyadhies.90
Vagbhata opines the same as Charaka and added it can be given regularly, which
is indicated for Bala, Vriddha, and Alpagni person also it as Varnya, Doshaghna etc.91
Hemadri commenting on the term “Sukho-Vyapad Rahitha”, it is devoid of
complications.92
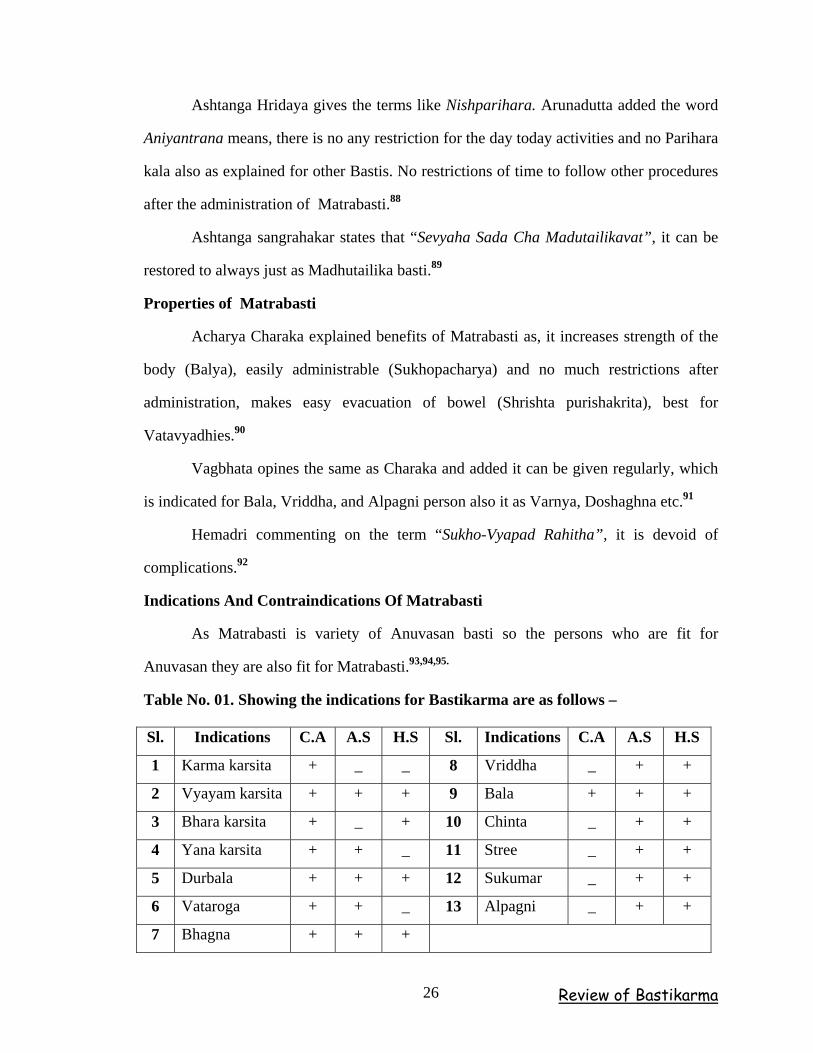
Indications And Contraindications Of Matrabasti
As Matrabasti is variety of Anuvasan basti so the persons who are fit for
Anuvasan they are also fit for Matrabasti.93,94,95.
Table No. 01. Showing the indications for Bastikarma are as follows –
Sl. Indications C.A A.S H.S Sl. Indications C.A A.S H.S
1 Karma karsita + _ _ 8 Vriddha _ + +
2 Vyayam karsita + + + 9 Bala + + +
3 Bhara karsita + _ + 10 Chinta _ + +
4 Yana karsita + + _ 11 Stree _ + +
5 Durbala + + + 12 Sukumar _ + +
6 Vataroga + + _ 13 Alpagni _ + +
7 Bhagna + + +
Review of Bastikarma 26
Contraindications for Matrabasti
No such particular contraindications for Matrabasti but Ashtanga sangrahakar
stated it should not be administered in case of Ajeerna and Diwaswapna.96
Matrabasti sevana kala and sevana vidhi
Acharya Charaka stated that it can be given regularly at any time and in all
seasons.97
Dosage of Matrabasti
Matrabasti, the term is popular because of its dose. Because Sneha is
administered in the Hriswa matra.
“Hraswaya snehapanasya matrayaha yojita samaha |” 98
So the dose of Matrabasti is equal to the quantity of Sneha which can digest
within 6 hours when taken orally. Acharya Dalhana mentioned the quantity of this as 11/2
phala i.e. 6 tola.99 Where as Kashyapa prescribed the quantity of Matrabasti as 2 palas as
Uttamamatra, 11\2 pala as Madhyama matra and 1 Prakuncha as Hriswa matra. He stated
that even half pala of Sneha can be given in Kaumara. (K. Khi. 8\104-105).100
Chakrapani stated pramana of Matrabasti as 11\2 pala. But whereas
Sharangandhara101 mentioned matra of Matrbasti as 2 palas. (i.e.8 tolas) (Su. U.5\5)102
Matrabasti Procedures
Poorvakarma (Pre-treatment procedure)
The mridu abyangha and swedana administered prior the pradhana karma. Then
advised to have alpha ahara a short walk. Patient must have passed natural urges. Then
made the patient laid on a cot comfortably, which is not very high and the head must be
at little lower level. Pillows should not be used. The patient should be in left lateral side
drawing up the right leg and straightening the left leg.103,104,105.
Review of Bastikarma 27
Pradhana karma (Treatment procedure)
The sneha prescribed for Matrabasti taken in the Bastiputaka and tied well placing
the Bastinetra in position. The entrapped air in Bastiyantra is expelled by gently pressing
the Bastiputaka. Then the anal region and the Netra should be smeared with oil. Gently
probe the anal orifice with the index finger of the left hand and introduce the Bastinetra
through it into the rectum up to first Karnika. Keeping in the same position press the
Bastiputaka with right hand with adequate and uniform force. Bastinetra should be
released carefully when a little quantity of sneha remained inside the Bastiputaka.106
Paschyata karma (Post-treatment procedures)
The patient is kept lying on his back as long as it would take to count up to
hundred. The patient should be gently struck three times on each of the soles and over the
buttocks by Vaidhya’s own hand. The distal part of the cot should be lifted thrice. Allow
him to lie for sometime in the same position. If he gets the urge for defecation he may do
it. But in the event of sneha passed immediately another Anuvasana basti should be
administered. After passing the motion with sneha in proper time the patient is allowed to
take light food if he feels hungry.107,108 There is no specific duration of retention of matra
basti so we can consider duration of sneha basti. i.e. 3 yamas it means 9 hours.
Review of Bastikarma 28
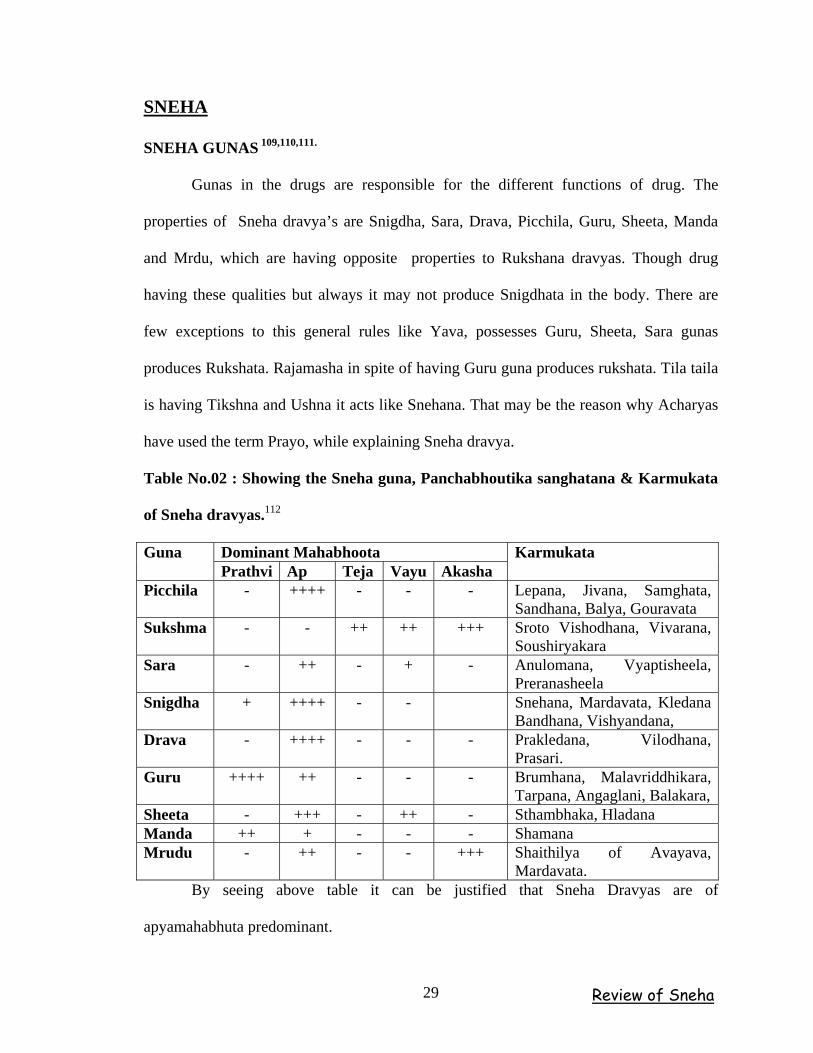
SNEHA
SNEHA GUNAS 109,110,111.
Gunas in the drugs are responsible for the different functions of drug. The
properties of Sneha dravya’s are Snigdha, Sara, Drava, Picchila, Guru, Sheeta, Manda
and Mrdu, which are having opposite properties to Rukshana dravyas. Though drug
having these qualities but always it may not produce Snigdhata in the body. There are
few exceptions to this general rules like Yava, possesses Guru, Sheeta, Sara gunas
produces Rukshata. Rajamasha in spite of having Guru guna produces rukshata. Tila taila
is having Tikshna and Ushna it acts like Snehana. That may be the reason why Acharyas
have used the term Prayo, while explaining Sneha dravya.
Table No.02 : Showing the Sneha guna, Panchabhoutika sanghatana & Karmukata
of Sneha dravyas.112
Dominant Mahabhoota Guna Prathvi Ap Teja Vayu Akasha
Karmukata
Picchila - ++++ - - - Lepana, Jivana, Samghata, Sandhana, Balya, Gouravata
Sukshma - - ++ ++ +++ Sroto Vishodhana, Vivarana, Soushiryakara
Sara - ++ - + - Anulomana, Vyaptisheela, Preranasheela
Snigdha + ++++ - - Snehana, Mardavata, Kledana Bandhana, Vishyandana,
Drava - ++++ - - - Prakledana, Vilodhana, Prasari.
Guru ++++ ++ - - - Brumhana, Malavriddhikara, Tarpana, Angaglani, Balakara,
Sheeta - +++ - ++ - Sthambhaka, Hladana Manda ++ + - - - Shamana Mrudu - ++ - - +++ Shaithilya of Avayava,
Mardavata. By seeing above table it can be justified that Sneha Dravyas are of
apyamahabhuta predominant.
Review of Sneha 29
PROPERTIES OF CHATURVIDHA SNEHAS
1. Ghrita
Rasa – Madhura.
Guna – Snigdha, Mrdu, Guru, Manda.
Veerya – Sheeta.
Vipaka – Madhura.
Prabhava – Agnideepaka.
Karma – Pitta-vatahara, Svara Lavanyab and Tejobalakara,
Chakshushya, Medhya, Increases Rasa, Shukra and Ojas, Vayasthapaka,
Dahashamaka, Alpaabhishyandi, Vrishya, Rasayana, and best agnideepaka.
Seasonal indication – Sharad Ritu.
Suitable condition for Ghrita application
Following are the conditions in whcih the ghrit can be used efficiently –
Vata-pitta Prakrti persons, Vata-pitta pradhana Vikratis, those desirer of longevity, Bala,
Varna, Swara, Pushti, Smriti, Medha, Dhee, and the some oft the conditions like
Dahapeedita, Shastra peedita,Visha Pidita.etc 113,114,115,116
2: Properties of Taila
Rasa – Madhura.
Anu rasa – Tikta, Kashaya.
Guna – Snigdha, Guru, Teekshna, Vikasi, Sara gunas.
Veerya – Sheeta
Vipaka – Madhura.
Review of Sneha 30
Karma – Vata-kaphahara, Pittakara, Balakara, Varnya, Twacha
mardavakara, Krimighna, Garbhashaya Shodhaka, Bhagna Sandhanakara ,
Subsides Yoni shoola and Yoni vyapats.
Seasonal indication – Pravrita (Sheeta Kala)
Suitable condition for Tilataila Snehana
Vata Prakriti, Shleshma pradhana vyadhis, Taila Satmya, Vatavyadhi, Nadivrina,
Bhagandara, Krura Koshta, and along with those desires of Bala, Tanutva, Laghuta,
Drdhata and Sthiragatrata. 113,114,115,116
3. Vasa
Properties – These are similar with the Mamsa of animals from which they are obtained.
Seasonal indication – Madhava Kala.
Suitable Condition for Vasa Prayoga 113,114,115,116
Due to vast origin and qualities of Vasa, it is indicated for the Mahat agnibala
persons along with those who are capable of bearing klantata of ruksha Vayu and Atapa,
karshatwa due to carrying of excess weights and it is found much beneficial in the vikritis
found in Asthi-Sandhi-Marma-Koshta ruja and Avarana like conditions.
4. Majja
Properties – Properties should be understood based on its source.
Seasonal Indication – Madhava Ritu.
Suitable condition for Majja Prayoga
This is the most heaviest sneha dravya. Hence, indicated in persons having
Diptagni, able to bear Klesha, having Krura Koshta and habituated to Sneha. 113,114,115,116
So Majja prayoga is indicated in those who desire of Bala-Shukra-Majja-Asthi Vardhana
and Snehana quickly.
Review of Sneha 31
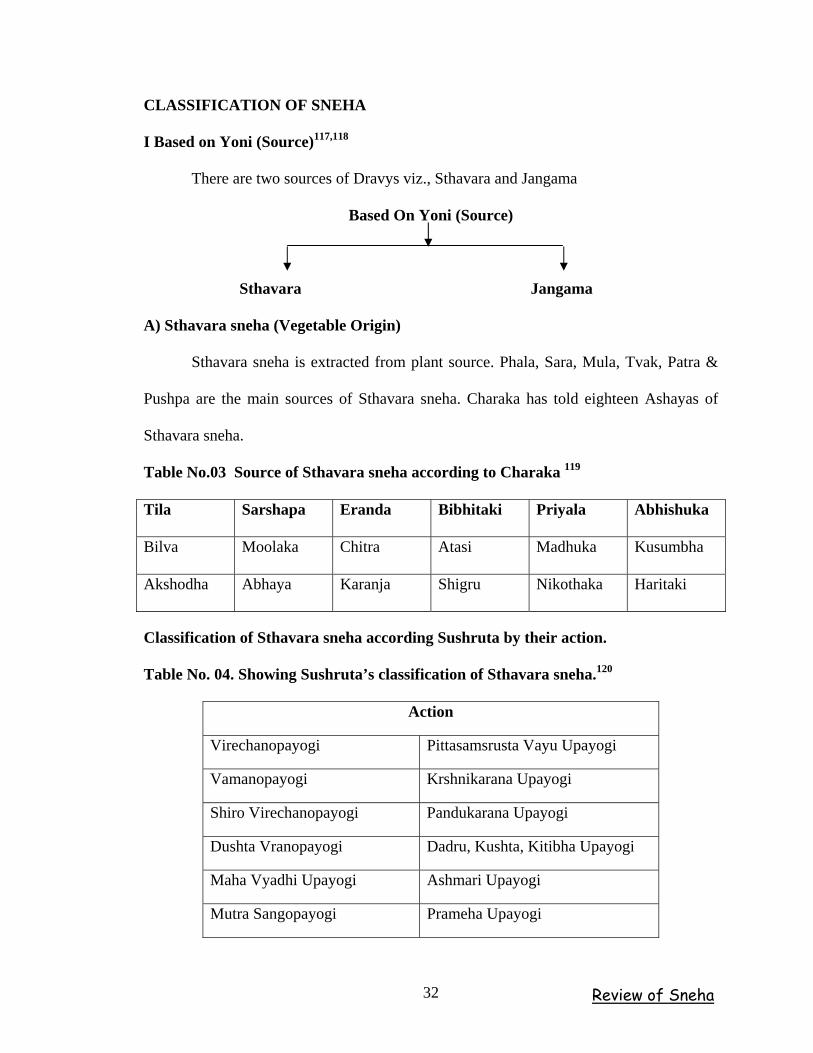
CLASSIFICATION OF SNEHA
I Based on Yoni (Source)117,118
There are two sources of Dravys viz., Sthavara and Jangama
Based On Yoni (Source)
Sthavara Jangama
A) Sthavara sneha (Vegetable Origin)
Sthavara sneha is extracted from plant source. Phala, Sara, Mula, Tvak, Patra &
Pushpa are the main sources of Sthavara sneha. Charaka has told eighteen Ashayas of
Sthavara sneha.
Table No.03 Source of Sthavara sneha according to Charaka 119
Tila Sarshapa Eranda Bibhitaki Priyala Abhishuka
Bilva Moolaka Chitra Atasi Madhuka Kusumbha
Akshodha Abhaya Karanja Shigru Nikothaka Haritaki
Classification of Sthavara sneha according Sushruta by their action.
Table No. 04. Showing Sushruta’s classification of Sthavara sneha.120
Action
Virechanopayogi Pittasamsrusta Vayu Upayogi
Vamanopayogi Krshnikarana Upayogi
Shiro Virechanopayogi Pandukarana Upayogi
Dushta Vranopayogi Dadru, Kushta, Kitibha Upayogi
Maha Vyadhi Upayogi Ashmari Upayogi
Mutra Sangopayogi Prameha Upayogi
Review of Sneha 32
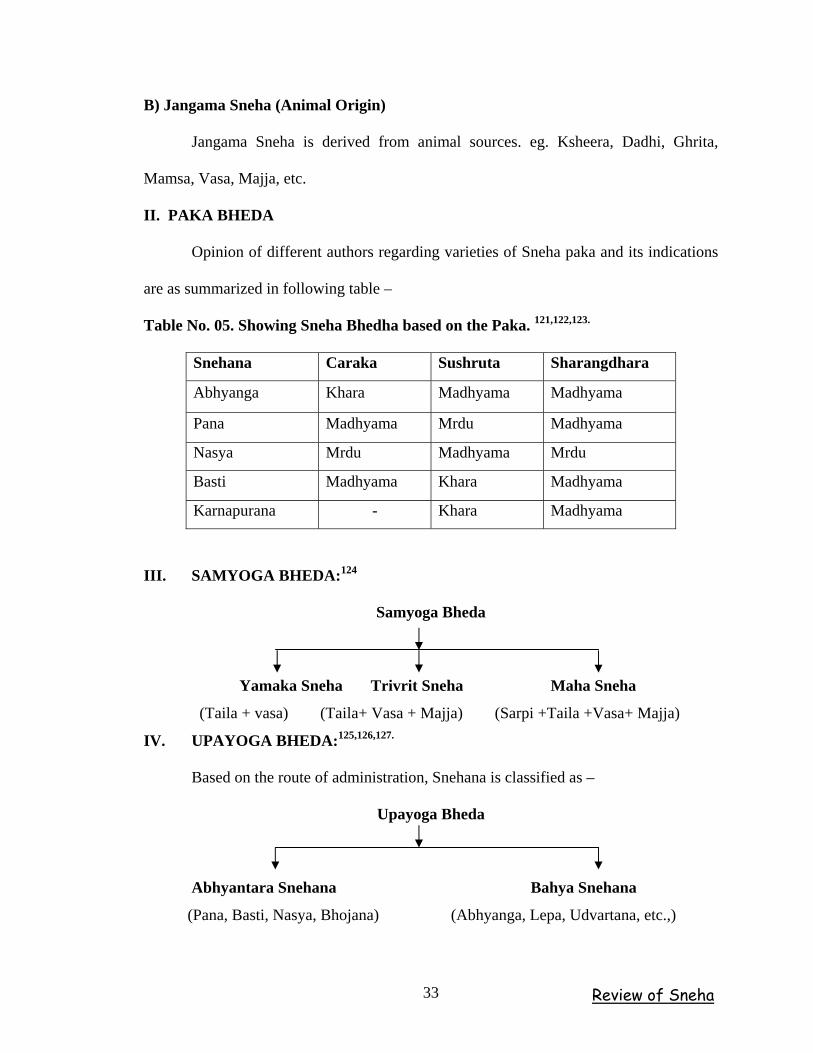
B) Jangama Sneha (Animal Origin)
Jangama Sneha is derived from animal sources. eg. Ksheera, Dadhi, Ghrita,
Mamsa, Vasa, Majja, etc.
II. PAKA BHEDA
Opinion of different authors regarding varieties of Sneha paka and its indications
are as summarized in following table –
Table No. 05. Showing Sneha Bhedha based on the Paka. 121,122,123.
Snehana Caraka Sushruta Sharangdhara
Abhyanga Khara Madhyama Madhyama
Pana Madhyama Mrdu Madhyama
Nasya Mrdu Madhyama Mrdu
Basti Madhyama Khara Madhyama
Karnapurana - Khara Madhyama
III. SAMYOGA BHEDA:124
Samyoga Bheda
Yamaka Sneha Trivrit Sneha Maha Sneha
(Taila + vasa) (Taila+ Vasa + Majja) (Sarpi +Taila +Vasa+ Majja)
IV. UPAYOGA BHEDA:125,126,127.
Based on the route of administration, Snehana is classified as –
Upayoga Bheda
Abhyantara Snehana Bahya Snehana
(Pana, Basti, Nasya, Bhojana) (Abhyanga, Lepa, Udvartana, etc.,)
Review of Sneha 33
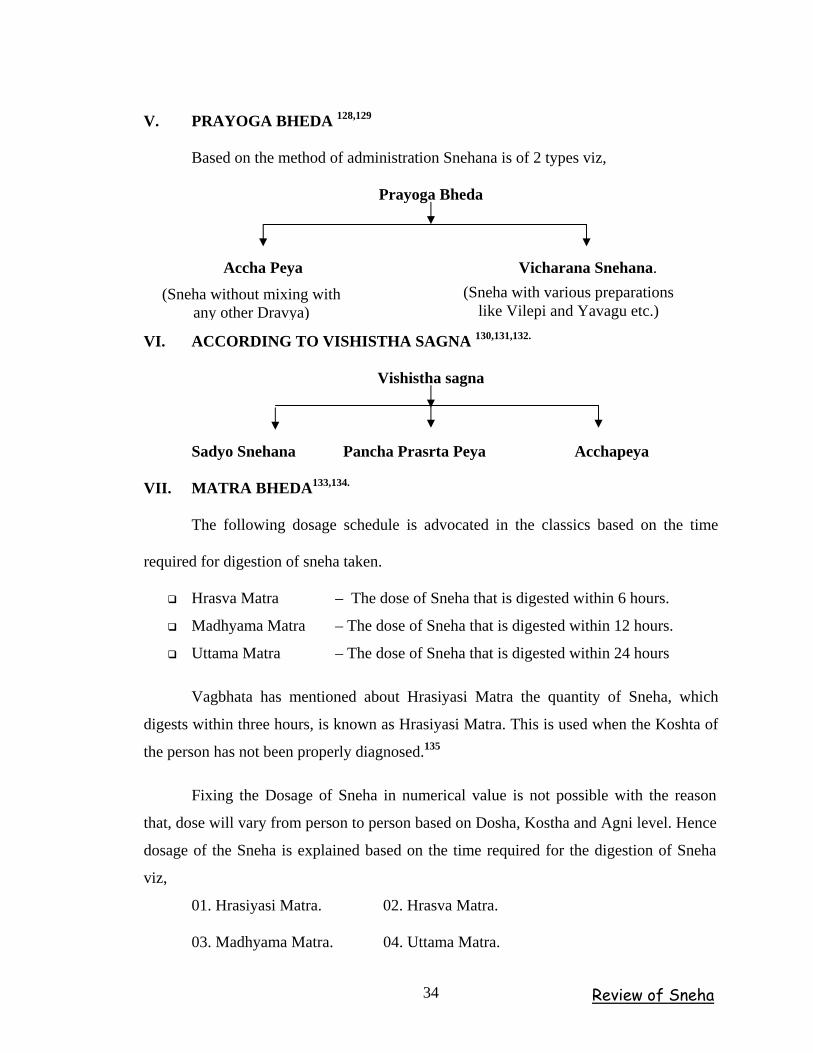
V. PRAYOGA BHEDA 128,129
Based on the method of administration Snehana is of 2 types viz,
Prayoga Bheda
Accha Peya Vicharana Snehana. (Sneha with various preparations
like Vilepi and Yavagu etc.) (Sneha without mixing with
any other Dravya)
VI. ACCORDING TO VISHISTHA SAGNA 130,131,132.
Vishistha sagna
Sadyo Snehana Pancha Prasrta Peya Acchapeya
VII. MATRA BHEDA133,134.
The following dosage schedule is advocated in the classics based on the time
required for digestion of sneha taken.
Hrasva Matra – The dose of Sneha that is digested within 6 hours.
Madhyama Matra – The dose of Sneha that is digested within 12 hours.
Uttama Matra – The dose of Sneha that is digested within 24 hours
Vagbhata has mentioned about Hrasiyasi Matra the quantity of Sneha, which
digests within three hours, is known as Hrasiyasi Matra. This is used when the Koshta of
the person has not been properly diagnosed.135
Fixing the Dosage of Sneha in numerical value is not possible with the reason
that, dose will vary from person to person based on Dosha, Kostha and Agni level. Hence
dosage of the Sneha is explained based on the time required for the digestion of Sneha
viz,
01. Hrasiyasi Matra. 02. Hrasva Matra.
03. Madhyama Matra. 04. Uttama Matra.
Review of Sneha 34
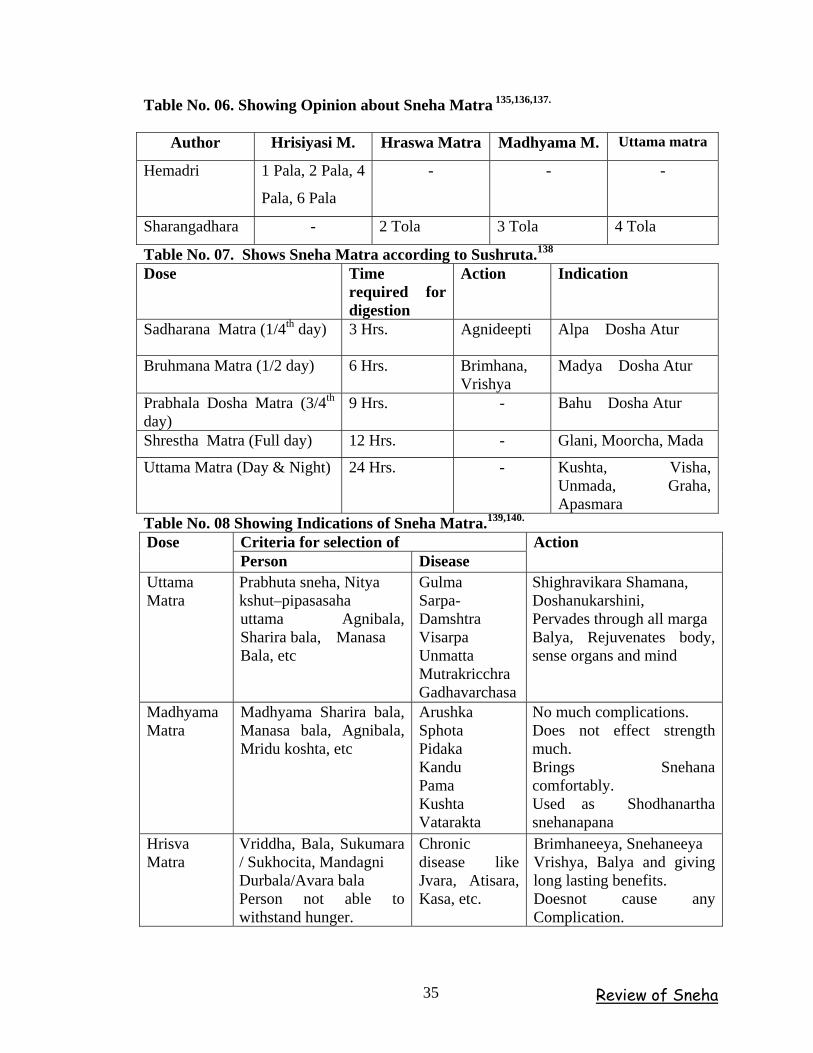
Table No. 06. Showing Opinion about Sneha Matra 135,136,137.
Author Hrisiyasi M. Hraswa Matra Madhyama M. Uttama matra
Hemadri 1 Pala, 2 Pala, 4
Pala, 6 Pala
- - -
Sharangadhara - 2 Tola 3 Tola 4 Tola
Table No. 07. Shows Sneha Matra according to Sushruta.138
Dose Time required for digestion
Action Indication
Sadharana Matra (1/4th day) 3 Hrs. Agnideepti Alpa Dosha Atur
Bruhmana Matra (1/2 day) 6 Hrs. Brimhana, Vrishya
Madya Dosha Atur
Prabhala Dosha Matra (3/4th day)
9 Hrs. - Bahu Dosha Atur
Shrestha Matra (Full day) 12 Hrs. - Glani, Moorcha, Mada
Uttama Matra (Day & Night) 24 Hrs. - Kushta, Visha, Unmada, Graha, Apasmara
Table No. 08 Showing Indications of Sneha Matra.139,140.
Criteria for selection of Dose Person Disease
Action
Uttama Matra
Prabhuta sneha, Nitya kshut–pipasasaha uttama Agnibala, Sharira bala, Manasa Bala, etc
Gulma Sarpa-Damshtra Visarpa Unmatta Mutrakricchra Gadhavarchasa
Shighravikara Shamana, Doshanukarshini, Pervades through all marga Balya, Rejuvenates body, sense organs and mind
Madhyama Matra
Madhyama Sharira bala, Manasa bala, Agnibala, Mridu koshta, etc
Arushka Sphota Pidaka Kandu Pama Kushta Vatarakta
No much complications. Does not effect strength much. Brings Snehana comfortably. Used as Shodhanartha snehanapana
Hrisva Matra
Vriddha, Bala, Sukumara / Sukhocita, Mandagni Durbala/Avara bala Person not able to withstand hunger.
Chronic disease like Jvara, Atisara, Kasa, etc.
Brimhaneeya, Snehaneeya Vrishya, Balya and giving long lasting benefits. Doesnot cause any Complication.
Review of Sneha 35
Hrasiyasi Matra is a trail dose, which is administered on the first day of
Snehapana.
Shamana sneha in Hrisva matra acts as Brimhana. Chakrapani mentions that,
Uttama matra should be used for Shamana and not for Shodhana poorva snehana. So
doubt may arise regarding usage of Uttama and Hrisva matra as Shodhana poorva
snehapana.
VIII. Karmukata Bheda
Based on the Karmukata of Sneha it has been divided into 3 types viz.
(i) Shamana Snehana
(ii) Brumhana Snehana
(iii) Shodhana Snehana
(i) Shamana sneha
Shamana sneha is a procedure of administration of Madhyama matra of Accha
sneha during Annakala when one feels hungry without taking the meal.141,142. Hemadri
defines Shamana snehana is one which normalizes the aggravated doshas without
expelling them and disturbing the normal doshas 143.
(ii) Brimhana sneha
The sneha used for Brimhana is called as ‘Bhrimhana sneha’. The administration
of Sneha along with Mamsa rasa, Madya, Ksheera etc., are known as Brimhana
snehana.144 If, Brimhana sneha is given before food, it will cures Adhobhaga rogas, if
given in the middle of food cures Madhyamabhaga rogas and if given after food cures
Urdhwabhaga rogas and strengthens the body.145 But, here the dose of Sneha should be
Alpa or even less than quantity of Hrisiyasi Matra.146
Review of Sneha 36
(iii) Shodhana sneha
The Uttama matra of Accha Sneha is administered in morning hours when
preceding evening food has been digested but individual have shown less hunger is called
as Shodhana sneha.147,148,149.
Shodhana snehana is carried out through Matranusara or Arohana or
Pravicharana. Matranusara and Pravicharana snehapana were already explained.
IMPORTANCE OF SHAMANA SNEHA PANA
Though the Acharyas explained about Shamana sneha but they did not defined it
clearly. But Arunadutta, the commentator of Ashtanga Hridaya stated that “Rogascha
Shamana Yopa Yuchyate Sneha” which normalizes the aggravated doshas all over the
body is called Shamana sneha.150
Charaka has explained Uttama matra of sneha for the person who is having
Uttama koshtaagni and bala, who can withstand thirst, hunger and fatigue (kshut,
pipasa). If we administered properly, it can does the shamana of the sarva shareeravyapi
doshas immediately, “Vikaran Shamayati Tesham, Shigram, Dhoshanukarshani,
Sarvamarga-Koshta, Sandi, Marma, ShakaSancharini. Balya, Punarnavikari, Shareera,
Indriyachetasam. (Ch. Su. 13 Uttama Matrasneha) and (A. Hr. Su. 16/19) and it has the
capacity to spread in to sarva shareera like entering into Marma, Asthi and Sandhi. It
cures the vyadhis like Gulma, Sarpadamshtra, Visrpa, Mutrakricchra, and it evacuates the
bowel easily. It enhances the Bala, Indriya and Manaprasannata. Arunadatta states that it
should administered when doshas are in relay to kupitavastha.151
Brihatrayee’s explained after Shamasneha, Peyadi krama should be followed
“Sneha Viriktavat” after the digestion of sneha. (Ah. S. 16/19, Ch. Su. 13/81) Because
Chkrapani said that after Dhoomapana is cotra-indication.152,153,154.
Review of Sneha 37
MATRA OF SHAMANA SNEHA
Regarding the posology of Shamana snehapana there is quite controversy between
Acharya Charaka and Vagbata. Charaka while describing the dose schedule for sneha,
says that Uttamamatra or optimum dose of sneha which gets digested with in 24 hours is
the more suitable dose for Shamana sneha.155 Vagbhat opines that the Madhyama matra
sneha which gets digest within 12 hours is the more suitable dose for Shamana sneha.
Where as Ashtanga Hridya added that for Shodana purpose Matra should Bahu, but for
Shamana purpose Madhyama matra should be used,156 It seems to be the time which is
taken for the digestion of Sneha dravya is one and same, but there is no contradictory
explanation by Charaka. Because Uttamamathra sneha will digest within 24 hours
Madyama matra will digest within 12 hours and Hrisvamatra will digest within 6
hours.157 , 157 (a)
Shrangadhara relatively more recent author has determined the dose depending
upon the digestive capacity of a person. Sneha for person of good digestive capacity is
one phala, for the person of medium digestive capacity is 3 karsha, and person of poor
capacity will be 2 karsha, which are considered as pradhana, madhyama, and hrisva matra
respectively.158 A close and critical analysis of the edition of the samhitas would appear
that, there is a gradual decreases in the dose of shamana sneha with the evidence of age.
This may be due to the decrease in the strength and power of digestion of the people with
advancement of age.159,160
The validity and applicability of Uttama and Madyama matra are Shamanasneha
matra according to Charaka and Vagbhat respectively. In the present day the person can
not withstand such a high dose of sneha. Hence it is favor to adopt the principal of
Sharangadhara that the dose of sneha should be decided as Heena, Madhyama, or Uttama
matra depending on the condition of Dosha, Kala, Agni, and Vyadhi of the patient. Even
the Chakrapani while commenting on Charaka opines that there is no fixed dosage of
drugs, but the dose is to be prescribed by considering the state of Doshas, Agni balabala
and nature of disease.
Review of Sneha 38
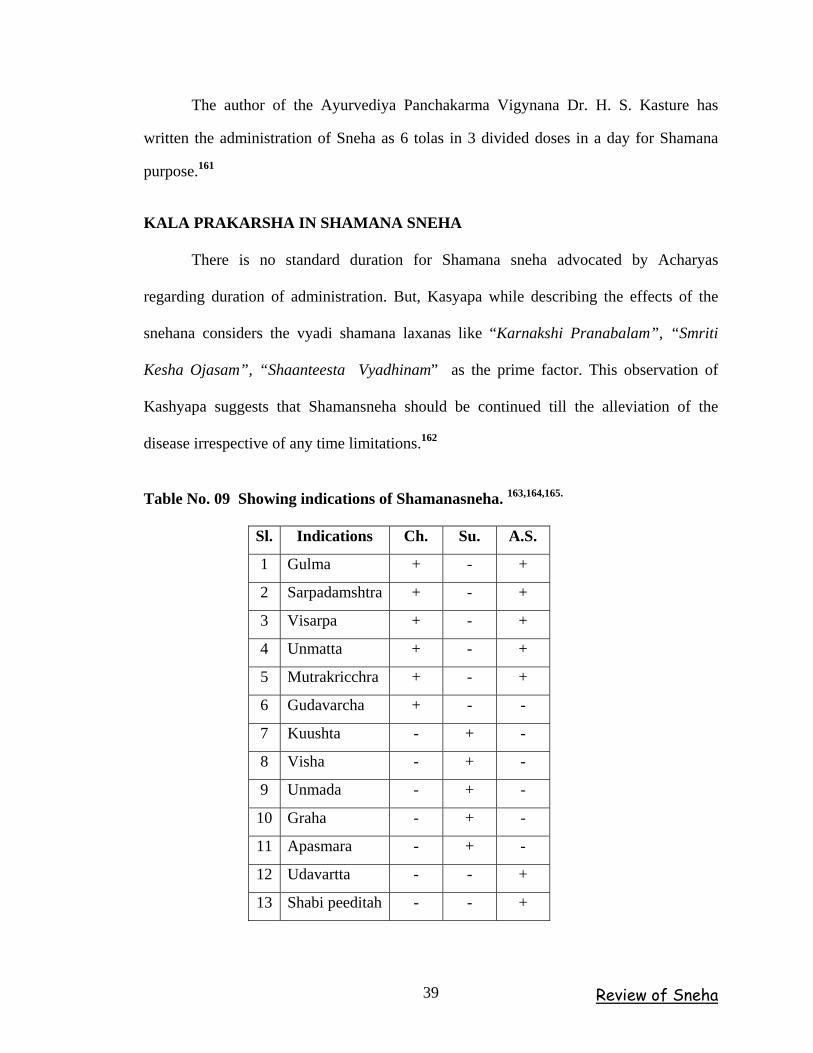
The author of the Ayurvediya Panchakarma Vigynana Dr. H. S. Kasture has
written the administration of Sneha as 6 tolas in 3 divided doses in a day for Shamana
purpose.161
KALA PRAKARSHA IN SHAMANA SNEHA
There is no standard duration for Shamana sneha advocated by Acharyas
regarding duration of administration. But, Kasyapa while describing the effects of the
snehana considers the vyadi shamana laxanas like “Karnakshi Pranabalam”, “Smriti
Kesha Ojasam”, “Shaanteesta Vyadhinam” as the prime factor. This observation of
Kashyapa suggests that Shamansneha should be continued till the alleviation of the
disease irrespective of any time limitations.162
Table No. 09 Showing indications of Shamanasneha. 163,164,165.
Sl. Indications Ch. Su. A.S.
1 Gulma + - +
2 Sarpadamshtra + - +
3 Visarpa + - +
4 Unmatta + - +
5 Mutrakricchra + - +
6 Gudavarcha + - -
7 Kuushta - + -
8 Visha - + -
9 Unmada - + -
10 Graha - + -
11 Apasmara - + -
12 Udavartta - - +
13 Shabi peeditah - - +
Review of Sneha 39
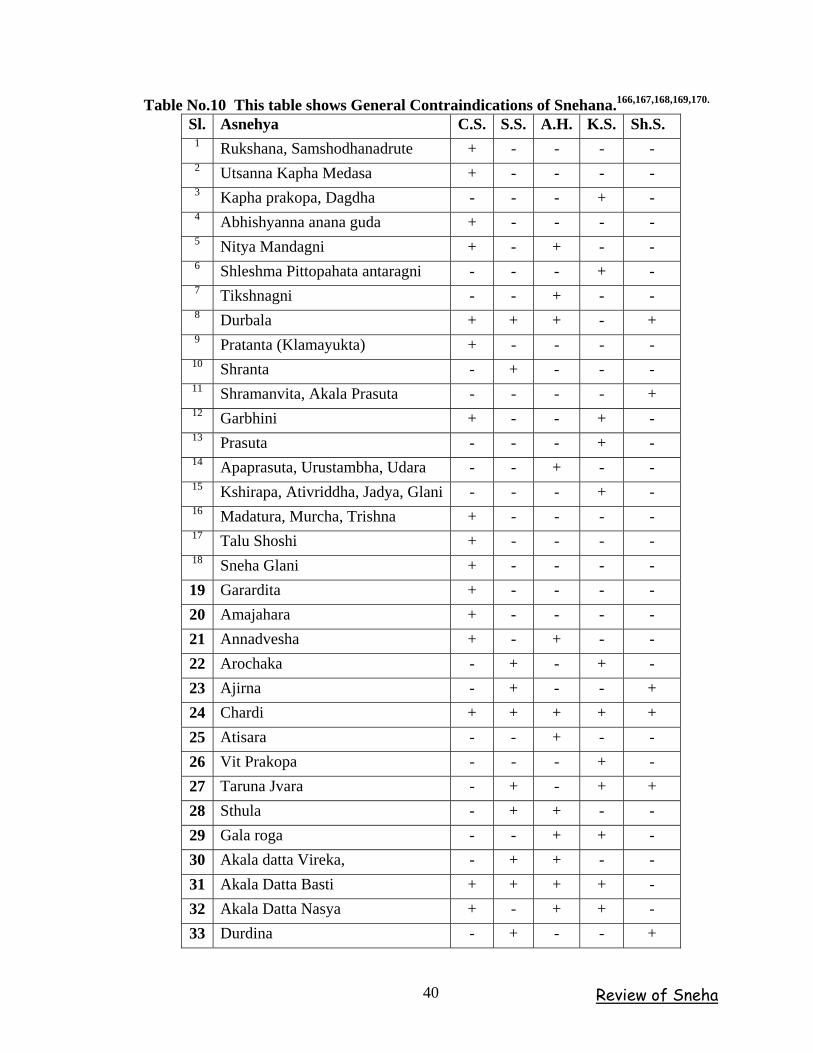
Table No.10 This table shows General Contraindications of Snehana.166,167,168,169,170.
Sl. Asnehya C.S. S.S. A.H. K.S. Sh.S. 1 Rukshana, Samshodhanadrute + - - - - 2 Utsanna Kapha Medasa + - - - - 3 Kapha prakopa, Dagdha - - - + - 4 Abhishyanna anana guda + - - - - 5 Nitya Mandagni + - + - - 6 Shleshma Pittopahata antaragni - - - + - 7 Tikshnagni - - + - - 8 Durbala + + + - + 9 Pratanta (Klamayukta) + - - - - 10 Shranta - + - - - 11 Shramanvita, Akala Prasuta - - - - + 12 Garbhini + - - + - 13 Prasuta - - - + - 14 Apaprasuta, Urustambha, Udara - - + - - 15 Kshirapa, Ativriddha, Jadya, Glani - - - + - 16 Madatura, Murcha, Trishna + - - - - 17 Talu Shoshi + - - - - 18 Sneha Glani + - - - - 19 Garardita + - - - - 20 Amajahara + - - - - 21 Annadvesha + - + - - 22 Arochaka - + - + - 23 Ajirna - + - - + 24 Chardi + + + + + 25 Atisara - - + - - 26 Vit Prakopa - - - + - 27 Taruna Jvara - + - + + 28 Sthula - + + - - 29 Gala roga - - + + - 30 Akala datta Vireka, - + + - - 31 Akala Datta Basti + + + + - 32 Akala Datta Nasya + - + + - 33 Durdina - + - - +
Review of Sneha 40
SUITABLE RITUS FOR SNEHA
Oil is to be used in Pravrut (First rainy season)
Ghee at the end of Varsha (Season of heavy rain)
Vasa and majja during maadhava (Vasant , spring )
These are when the doshas are in the normal state (in a healthy person) 171
ACCORDING TO DOSHA
When there is Kapha associated with Vata or Kapha alone Sneha has to be
administered in day time.
When the aggravation of Pitta and Vata, Pitta associated with Vata or Pitta
associated with Kapha sneha should be given at night.172
SHAMANA SNEHA PANA VIDHI
The administration of sneha in three different stages (1) Poorvakarma (2)
Pradhana karma and (3) Pachyat karma
Poorvakarma
Athura siddatata
For Shamananga snehapana is no specific preparatory regimens are needed. But
care should to be taken about Sama and Niramavastha of the patient before giving
Shamana sneha. In Samavastha Snehapana is contraindicated. Doshas have permeated
through out the dhatus of the body such an attempt seldom gives the desired effect.
Shamana sneha should be administered when the doshas are in Paripakwa avastha
“Paripakweshu, Dhosheshu, Sarpihi, Panam Yataambrutum.”173Ch. Su. 13/72) Ashtanga
samgraha and Hridayakara advised mridu bhojana prior night of Shamana snehapana.
Because his previous food should digest completely and should feel hunger (bubbukshita)
then only he is fits for Shamana snehapana. When the patient is not having proper
appetite the administered sneha will not be able do its desired effect and may leads to
doshotklesha. So one must be very particular about the appetite while administering
Shamana sneha.174,175
Review of Sneha 41
Pradhanakarma
“Pibet Samshamanam Sneham Anna Kale Prakakshitaha |”176
The Shamana sneha should be administered during the anna kala, when the
patient feels hungry, advise to take Snehapana by praying the God and devoting respect
to the elders.177
Pashatkarma
The physician should take care of three things in Paschyata karma viz.
i. Anupana.
ii. Peyadi krama. (Sneha viriktavat)
iii. Pathya pathyha.
Anupana 178,179,180.
Particular Anupana should selected and given along with the Snehadravya.
Because it helps in breakdown, softening, digestion, proper assimilation and instant
diffusion. It energies the patient and gives sense of pleasure.
Charaka has mentioned particular type of Anuapna dravyas in respect with sneha
dravyas viz.
Ushna jala – For Ghrita
Yusha – For Taila
Manda – For Vasa and Majja,
Sheetala Jala – For Bhallataka and Tuvaraka Taila
In the non availability of particular Anupana dravya Ushnajala can be used except
in case of Tuvaraka and Bhallataka Taila. The dosage of the Anupana should be decided
on the basis of Agnibalabala or according to the pharmaceutical process involved.
Review of Sneha 42
Peyadi Krama (Sneha viriktavat)
After the digestion of sneha patient should follow sequence of regimens as a part
of post-operative care –
Ushna yavagu, Saklinna alpatandula, Krita yavagu, Krita vilepi with alpa ghrita.
Arunadatta has commented over (A.Hr.16/19) Upacharsthu Shamanae Karyah
Snehae Virikthava.181,182,183
Pathya Pathyha
Pathya 184,185,186,187.
Ushna Jalapana – Ushna Jala is having Balya, Deepana-pachana and
Vatanulomana properties. Hence helps in Snehapachana process.
Bramhacharya – Helps in Sneha process.
Kaphashaya – As day sleep and Ratri jagarana aggravates Kapha and
Vata dosha respectively. Hence, only night sleep is advised.
Apathya
Vyayama – Exercise
Uccha Vacana – Loud speech
Vega Samrodha – Suppression of Urges
Shoka, Krodha – Anger, anxiety.
Hima, Atapa – Mist, Sunlight.
Pravata – Open breeze
Atyasana – Sitting at a place for long time.
Nicha/Uccha Upadhana – Usage of too low or too high pillows.
Pathya-apathya is to be followed strictly during the course of therapy.
Review of Sneha 43
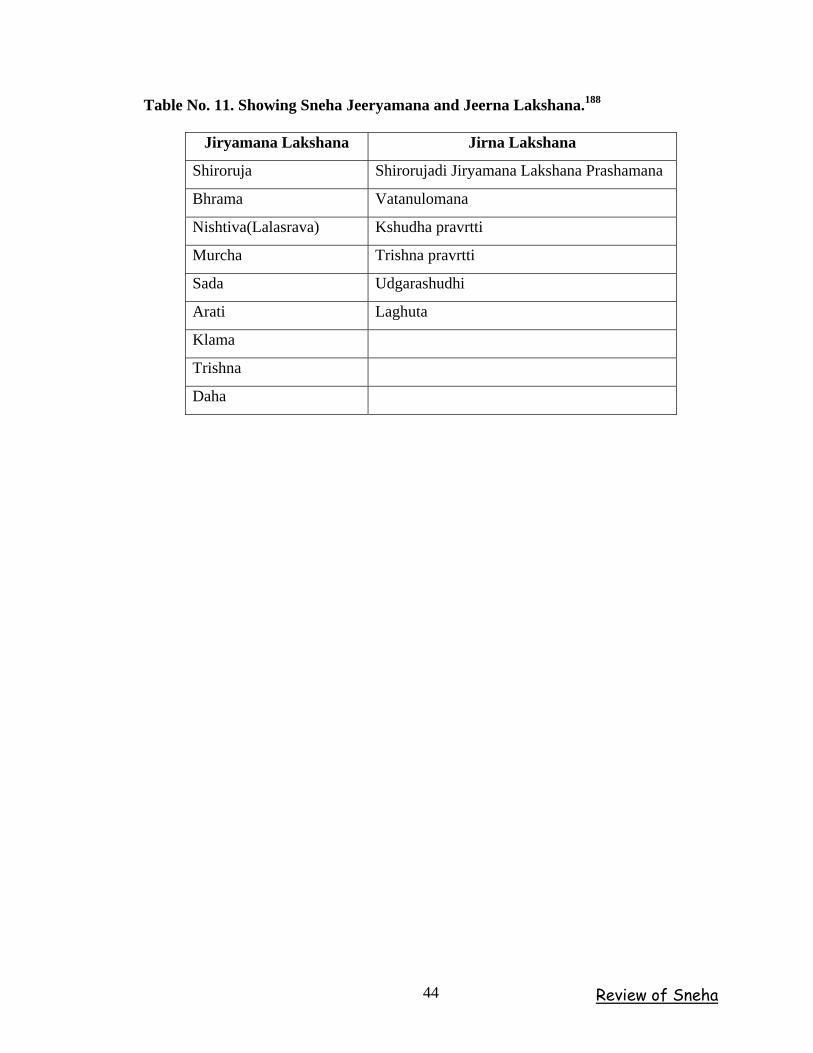
Table No. 11. Showing Sneha Jeeryamana and Jeerna Lakshana.188
Jiryamana Lakshana Jirna Lakshana
Shiroruja Shirorujadi Jiryamana Lakshana Prashamana
Bhrama Vatanulomana
Nishtiva(Lalasrava) Kshudha pravrtti
Murcha Trishna pravrtti
Sada Udgarashudhi
Arati Laghuta
Klama
Trishna
Daha
Review of Sneha 44
SHARRERA OF ASHTILA Ashtila is the hard, round, stony like structure . Acharya sushruta explained very
clearly about structure and its location in the body.189 It is located in Shakrunmarga i.e.
it lies in between the Basti and guda Pradesha.190
STRUCTURE OF ASHTILA
01. Deerghavartula pashana visheshaha191 – It means elongated, round, apple and
stony like structure.192
02. Charmakarinam – Means it is very hard mass which feels like metallic one i.e.
(loha, bhandi).
03. Ayata – Means to arrive, to adhere. Here Ayata means Granthi, which is like
Ayatakara. It can be compare with prostate when it enlarges with right and left lateral
lobes.193
04. Urdhwa – It means perhaps raised, tending upwards or raised elevated. It can be
compared with upper border of prostate.194
05. Ghana – Means solid material, hard, thick.195
It can’t be compared with hyperplesia of the prostate, because it composed of
smooth muscle cells and granular epithelial tissue, but it can be compared with prostatic
cancer.
06. Unnata – It means bent, turned upwards, elevated little up or prominent
projective. It can be compared with anterior lobe of the prostate.196
07. Achala \ Eshacchala – Means fixed or partial movable. In case of prostatic
hyperplasia there will be partial movement, where as in prostatic cancer it will be fixed
one.197
Shareera 45
RECTUM / GUDA
Sushruta has explained about the anatomical structure of Guda while describing
Arsharoga. Guda is a part, which is the extension of sthoolantra with 4½ angula in length.
It has got 3 valis (parts) named as Gudavalitrayam.200
Pravahini – That which does pravahana.
Visarjini – That which does viasrajana.
Samvarani – That which does samvarana.
There is another structure called as Gudostha, which is about a distance of 1½
yavapramana. The first vali samvarani starts at a distance of 1 angula from gudostha. The
width of each vali will be 1 angula and resembles the colour of elephant’s palate.201
Charaka when described about the Koshatagni has considered Uttaraguda and
Adharaguda. The modern commentators consider them as rectum and anus
respectively.202
All Acharyas have considered Guda as one among the Dashajeevita dhamanis and
also one among the Bahyasrotas. 203,204,205.
The rectum forms the last 15 cm of digestive tract and is an expandable organ for
the temporary storage of fecal material. Movement of fecal material into the rectum
triggers the urge to defecate.
The last portion of the rectum, the ano-rectal canal, contains small longitudinal
folds, the rectal columns. The distal margins of rectal columns are joined by transverse
folds that marks the boundary between columnar epithelium of the proximal rectum and a
stratified squamous epithelium like that in the oral cavity. Very close to the anus or anal
orifice, the epidermis becomes keratinized and identical to the surface of the skin.
Shareera 46
There is a network of veins in the lamina propria and submucosa of the ano-rectal
canal. The circular muscle layer of the muscular is extern in the region forms the internal
sphincter and are not under voluntary control. The external anal sphincter guards the anus
and is under voluntary control. Pudental nerves carry the motor commands.206
BASTI
Nirukti - The term Basti is derived from the root ‘Vas nivase’ which is suffixed
by ‘Tich' or ‘Ktin' gives the meaning of reservoir or hoarded or covered. In addition, it
has been told as ‘Vas acchadane'.
According to Shabdastomamahanidhi -
‘Baste Avrunoti Mutram’
‘Nabheradho bhage Mutradhare Sthane’,
It means, the organ, which acts as receptacle or lodges or hoarded or covers the
urine, which is situated in the lower part of Nabhi.
According to Medini commentator of Namalinganushasana “Vasati mutramatra”
the organ where Mutra stays or resides or in other words Basti acts as a reservoir of urine.
Synonyms - The terms such as Mutrabasti (Su. Sha.9), Mutradhara (Ch.Si.9),
Mutrashaya (Su. Ni.3), Basti (Su. Ni.3), and Basti puta (Vijayarakshita on Ma. Ni.31).207
Uthpatti - The essence part of the Rakta and Kapha after being digested by Pitta
along with Vayu forms the Basti, Antra and Guda (Su. Sha.4).208 Further in this context
Sushruta explains that the hollow shape is formed when the essence parts are inflated by
the repeated action of Vayu (Su. Sha.4).208 Charaka has not explained about the
embryological origin but has encounters it in Matruja Avayava (Ca. Sha.3).
Shareera 47
Number, Location, Relations - Basti is only one and is one of the Koshthanga
(Ch. Sha.7, Su. Sha.5, Su. Chi.2, A. Hr. Sha.3), Saptashaya (Su. Sha.5) and Dasha
pranayatana (A. S. Sha.5).
Regarding the location, Sushruta and Vagbhata opines that the Basti lies between
the Nabhi, Prushtha, Kati, Vrishana (Mushka), Guda, Vankshana and Shepha
(Medhra/Linga). The Basti, Bastishira, Pourusha, Kati, Vrishana and Guda are all related
to one another and situated within Gudasthivivara (Cavity of rectal bone/Pelvic cavity).
Further in the chapter of Ashmari Nidana,209 Sushruta and also Vagbhata states that in
females the Urinary bladder is situated very near and side to the Uterus (Su. Chi.7, A. S.
Chi. 13, A. Hr.Chi.11).
Acharya Charaka mentions that Basti is located in the midest of Sthula Guda,
Mushka, Sevani, Shukravaha and Mutravaha Nadi, is the receptacle of urine into which
all the channels of the body carrying liquid elements converge as all the rivers on the
earth flow into the ocean (Ch. Si. 9). Further Chakrapani commenting on the same verse
explains that Basti is the resort (Ashraya) of all the surrounding organs and it is the
resting place of Ambuvaha srotas. The channels connected to their moola which are
Marma and which provide nourishment to them because of which even these channels are
called as Marma. Bhavamishra and Sharangadhara have mentioned that the Basti is
located below the Malashaya (Sha. Pu. Kha.5). Amarasimha mentions it to be situated
below the Nabhi.
Size - Acharya Sushruta mentioned that the size or pramana of Basti marma is
equal to the pit of one’s own palm (Su.Sha.6).
Shareera 48
Shape - The shape of the Basti is similar to Alabu (Gourd) (Su. Ni.3), whereas
Acharya Vagbhata says that it has a shape of Dhanurvakra - a bent bow - (A. H. Sha.4).
Adhamalla commenting on Sha. Pu. Kha.5 mentions that it is having resemblance (with
the shape) of a bag of leather.
Structure - It is hollow viscera (Ashaya) (Su. Sha.5), having thin walled (Tanu
Twak) and a single outlet directed downwards, which is fixed on all sides by the Sira and
Snayu (Su. Ni.3, Su. Sha.5, Su. Sha.5). Here Snayu are of Sushira variety. Structurally it
is composed of very less Mamsa and Rakta dhatu (A. H. Sha.4, A. S. Sha.7). Basti is
devoid of Mamsa and Meda dhatu (Dal. on Su.Ni.9) Basti is counted under Sadya
Pranahara marma and Snayu marma having vital area of about 4 Angulas (Su. Sha.6) and
it also consists of Dhamani according to Vriddha Vagbhata (A.S.Sha.6).
Synonyms - Mutra Praseka (Su. Chi.7), Mutra patha (Ch. Chi.26), Mutra vahi
Srotas (Dal - Su. Ut.58), Mutra Seka (Su. Chi.7), Mutra Marga (Ch. Si.9, Su. Chi.7, Su.
Ut. 58), Mutra Srota (Su. Ni.13, A. Hr. Ni.9), Mutrayanam (Madhukosha - Ma. Ni.27).
Mutrapraseka -
There are no direct references available regarding the size, shape and other
specific anatomical details of Mutra Praseka but some relevant and cross references in
Uttara Basti chapter gives a superficial idea about the length of Mutra praseka. Wherein
the Uttara Basti (Pushpa) netra pramana is said to be of 12 or 14 angula in male and 10
angula in female (Ch. Si.9, Su. Chi.37) Further it has been explained that in males it
should be administered up to half of its length i.e. 6 to 7 angula or up to Madhya karnika.
Therefore the length of Mutra praseka in male is about 6 to 7 angula. In female it has to
be introduced up to 2 angula, hence the length of Mutra praseka in female is about 2
angula. Acharyas opinion about Mutra praseka is identical to that of "Urethra".
Shareera 49
Applied aspect - While explaining the surgical approach to Ashmari Sushruta has
said to prevent Mutra praseka from any injury, otherwise dribbling of urine will become
continuously (Su. Chi.7). Sushruta describes that below the opening of the urinary
bladder (Bastidwarasya chapyadhah - internal urinary meatus) and two fingers on the
right side (Dwayangule Dakshine parshwe), the Shukra enters and flows out through the
urinary passage (urethra) of the man (Su. Sha.4, A. S. Sha.5). It also opens from left side
at the same level, which can be practically appreciable (Pratyaksha Shareera).
Suppression of urge of urine during sexual intercourse leads to Shopha and Ruja of the
Mutrashaya, Guda, Mushka and leads to retention of urine. Urologists are also of same
opinion that due to aforesaid cause retrograde ejaculation occurs in consequence to the
relaxation of bladder internal sphincter. It is also related to testes. This is further
substantiated by the lakshana mentioned in Shukrashmari (Ca.Chi.26).
Prakrita Mutra Pramana -
4 Anjali. (Ch. Sha.7) 1 Anjali is nearly about 4 ounces. So 4 Anjali is nearly about
16 ounces, (480 ml) which clearly indicates that Acharyas considered 4 Anjali only
because of the storage capacity of Basti. In 24 hours 1500 ml of urine is excreted out
which can be considered. 1500 ml cannot be stored in bladder at normal physiological
instances.
The urinary bladder performs the function of Dharana (storage) and poshana
(release) of urine. The example of a ''taut bow" in relation to Basti signifies the
functioning of the urinary bladder in the light of modem physiology.
Applied aspect - When Mutravaha srotas is vitiated it manifests the lakshanas
like Atisrushta (Increased Quantity or Frequency), Atibaddha (Obstructed or Retention of
Urine), Prakupita (Provoked), Alpalpam (Scanty), Abhikshnam (Dribbling), Bahalam
(Thick urine or abundant urine) and Sashoolam (With pain or Dysuria) (Ch. Vi.5).
Shareera 50
Any injury to Mutravaha srotas leads to the Anaddha basti (Distention of urinary
bladder), Mutranirodha (Retention of urine) and Stabdha Medhra (Stiffness of the penis)
(Su. Sha.9).
ANATOMY OF PROSTATE
Fundamental to a complete understanding of the pathophysiology and therefore
the symptoms of BPH is a through comprehension of the normal and pathologic anatomy
of the structures involved.
Graphically the prostrate gland can be conceived of as an apple with the core
entirely removed. The hole thus produced through the center of the apple is the prostatic
urethra, which is contiguous with the bladder neck superiorly and the membranous
urethra inferiorly. This analogy with the apple can be carried further by thinking of the
skin of the apple representing the gland itself, which consists of fibrous, muscular and
glandular elements. The entire prostrate gland in a young, healthy adult man weighs
about 20gm is about the size of a large chestnut. Stephen N, Rous Textbook of Urology.)
The Prostate is located in the pelvis and is surrounded by the rectum, bladder,
dorsal and periprostatic venous complexes, musculature of the pelvic sidewall, the
urethral sphincter (responsible for passive urinary control), the pelvic plexus, and
cavernous nerves (which innervate the pelvic organs and corpora cavernosa). Sushruta
and Charaka explained the Sthana of Basti in the similar fashion.
The Prostate is a firm, partly glandular, partly fibro muscular body, surrounding
the beginning of the male urethra. Being somewhat conical, it presents: above - a base or
vesicle aspect, below - an apex and also posterior, an anterior and two inferolateral
surfaces.
Shareera 51
The base is largely contiguous with the neck of the bladder above it; the urethra
enters here, nearer its anterior border. The apex is inferior and in contact with the fascia
on the superior aspects of the sphincter urethra and transversi perinei profundi. The
posterior surface, transversely flat and vertically convex, is separated from the rectum by
the Prostatic sheath and loose connective tissue external to the sheath. Near its superior
(Juxta vesical) border is a depression where the ejaculatory ducts penetrate the gland,
dividing this surface into a superior and an inferior, larger part. The superior part is
variable in size and usually regarded as the external aspect of the median lobe; the
inferior part shows a shallow, median sulcus, usually considered to mark a partial
separation into right and left lateral lobes, forming the main Prostatic mass and
continuous behind the urethra. A band of fibro muscular tissue, ventral to the urethra,
joins these lobes together and is often referred to as the anterior lobe; it contains less
glandular tissue than the rest of the gland. The anterior surface, transversely narrow and
convex, extends from the apex to the base, about 2 cm behind the pubic symphisis from
which it is separated by a venous plexus and loose adipose tissue. Near its superior limit
it is connected to the pubic bones by the puboprostatic ligaments. The urethra emerges
from this surface anterosuperior to the apex of the gland. The inferolateral surfaces are
related to the anterior parts of the lavatories ani, which are separated from them by a
plexus of veins embedded in the fibrous Prostatic sheath.
The Prostatic base measures about 4 cm transversely, the gland being about 2 cm
in anteroposterior and 3 cm in its vertical diameters. It weighs about 20 gms. It has a
fibrous sheath, partly vascular; on each side this consists fibrous tissue containing the
prostatic venous plexus; anteriorly it blends with the puboprostatic ligaments and
inferiorly with fascia on the deep surfaces of the sphincter urethra, the deep transverse
Shareera 52
perineal muscles and with the perineal body. Posteriorly the sheath has a different origin
and is a vascular. In male fetuses, at the forth month, the rectovesical peritoneal pouch
descends to the pelvic floor, separating prostate from rectum; its lower part is obliterated
and the fused peritoneal layers here form the posterior prostatic sheath, sometimes termed
the rectovesical fascia. Traces of its separate layers persist as a plane cleavage. Above, it
descends over the posterior aspects of the seminal vesicles and deferent ducts and is
connected to the floor of the rectovesical pouch; on each side, it joins with the posterior
vesicle ligament. Below, adherent to the prostate, it joins with the perineal body. The
anterior parts of the lavatories ani pass back from the pubis around the prostate as
levatores prostatae.
The prostate is traversed by the urethra and ejaculatory ducts, and contains the
prostatic utricle. The urethra usually passes between its anterior and middle thirds. The
ejaculatory ducts pass antero-inferiorly through its posterior region to open into the
prostatic urethra.
It is divided into a peripheral zone, a central zone, and a transition zone. The
anterior surface is covered by the fibro muscular stroma. Most cancers develop in the
peripheral zone, while nonmalignant proliferation occurs predominantly in the transition
zone. The functional unit is the glandular acinus, which consists of an epithelial
compartment including epithelial, basal - neuroendocrine cells - and a stromal
compartment including fibroblasts and smooth muscle cells.
These compartments are separated by a basement membrane. PSA and prostate
specific acid phosphatase are produced in the epithelial cells. Both stromal and epithelial
cells express androgen receptors and depend on androgens for growth. Additional growth
regulatory signals occur via paracrine signaling between the two compartments. In
cancer, the relationship between stromal and epithelial elements contributes to growth
Shareera 53
both in the primary and metastatic sites. The major circulating androgens in the blood are
Testosterone, which is converted to dihydrotestosterone (DHT), the active form, by 5-α
reductase. Changes in prostate size occur during two distinct periods –
01. Diffuse enlargement during puberty
02. In focal regions in the periurethral area after the age of 55. (Harrison's-I )210
The contemporary classification of the prostate into different zones was based on
the work of Mc Neal. He showed that it is divided into: the peripheral zone which lies
mainly posteriorly and from which many carcinomas arise, and a central zone which lies
posterior to the urethral lumen and above the ejaculatory ducts as they pass through the
Prostate; the two zones are rather like an egg in its egg cup. There is also a periurethral
transitional zone from which most Benign Prostatic Hyperplasia (BPH) arises. Smooth
muscle cells are found through the prostate, but in the upper part of the Prostate and
bladder neck (the internal sphincter) these sub serve a sexual function, closing during
ejaculation. Resection of this tissue during Prostatectomy is responsible for retrograde
ejaculation.
Sushruta explained the condition like Mutra shukra, which resembles to above
said explanation. The distal striated urethral sphincter muscle is found at the junction of
the prostate and the membranous urethra, it is horseshoe shaped with the bulk lying
anteriorly; it is quite distinct from the muscle of the pelvic floor.
The glands of the peripheral zone, lined by columnar epithelium, lie in the fibro
muscular stroma and their ducts, which are long and branched, open into posterolateral
grooves on either side of the verumontanum. The glands of the transitional zones are
shorter and unbranched. All these ducts, the common ejaculatory ducts and the prostatic
ducts, open into the Prostatic urethra. No wonder that infection of the prostatic urethra is
difficult to eradicate.
Shareera 54
Benign Prostatic Hyperplasia starts in the periurethral transitional zone and, as it
increases in size, it compresses the outer peripheral zone of the Prostate, which becomes
the false capsule. There is also the outer true fibrous anatomical capsule, and external to
this lie condensations of endopelvic fascia known as the periprostatic sheath of
endopelvic fascia. Between the anatomical capsule and the prostatic sheath lays the
abundant prostatic venous plexus. The prostatic sheath is contiguous with the strong
fascia of Denonvilliers' that separate the prostate and its coverings from the rectum. The
neurovascular bundles supplying anatomic innervations to the corpora of the penis are in
very close relationship to the posterolateral aspect of the prostatic capsule and are at risk
of damage during radical cystoprostatectomy and radical Prostatectomy; inadvertent
diathermy to these nerves may be the cause of erectile impotence after Transurethral
Prostatectomy. (Bailey and love) 211 Vagbhata and Sushruta had considered this as Abhighata to
Shukravaha srotas that leads to Klaibya or Marana as explained during the operative
procedure of Ashmari.
The peripheral and central zone of the prostate are divided according to newer
anatomical studies.
A dorsocranially located central zone with wide lumina and a high cylindrical
epithelium. The glands show papillary folding. The cellular cytoplasm is light and
granular. The stroma is loose. A transition zone, located mediolateral of the urethra.
Narrow glands and a very tight stroma characterize this zone. A peripheral zone with
loose stroma and glands such as are seen in the transition zone. In all three zones
glandular acini and ducts with basal and secretary cells are found.
Shareera 55
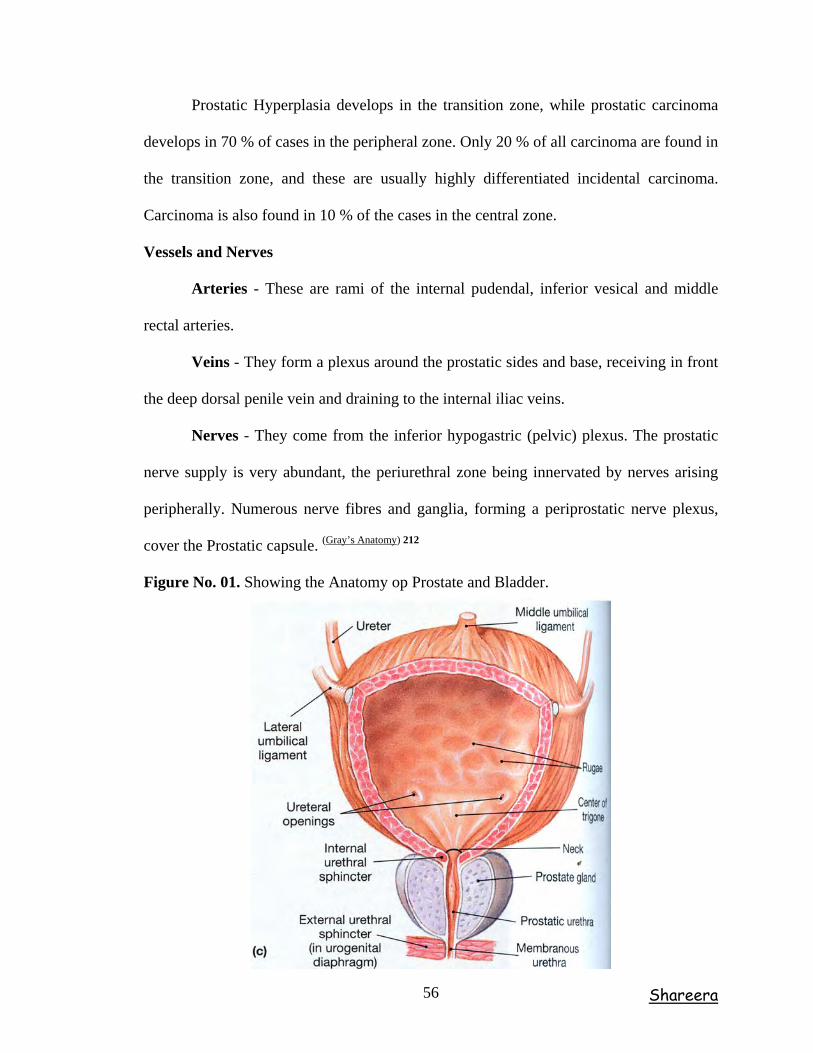
Prostatic Hyperplasia develops in the transition zone, while prostatic carcinoma
develops in 70 % of cases in the peripheral zone. Only 20 % of all carcinoma are found in
the transition zone, and these are usually highly differentiated incidental carcinoma.
Carcinoma is also found in 10 % of the cases in the central zone.
Vessels and Nerves
Arteries - These are rami of the internal pudendal, inferior vesical and middle
rectal arteries.
Veins - They form a plexus around the prostatic sides and base, receiving in front
the deep dorsal penile vein and draining to the internal iliac veins.
Nerves - They come from the inferior hypogastric (pelvic) plexus. The prostatic
nerve supply is very abundant, the periurethral zone being innervated by nerves arising
peripherally. Numerous nerve fibres and ganglia, forming a periprostatic nerve plexus,
cover the Prostatic capsule. (Gray’s Anatomy) 212
Figure No. 01. Showing the Anatomy op Prostate and Bladder.
Shareera 56
PHYSIOLOGY OF PROSTATE
The prostate has a purely sexual function and in animals that have a seasonal
sexual life, it is rudimentary except during the rutting season. The normal adult Prostate
undergoes atrophy after castration.
The glands of the Prostate consist of many follicle-like spaces leading into ducts.
The epithelium of the follicles secretes the prostatic fluid, which is thin and opalescent
and gives the semen its characteristic odor.
Prostatic Fluid – The seminal vesicles produce their own seminal fluid, which
nourishes and gives volume to the sperm. During sexual excitement the seminal vesicles
empty their contents into the prostate, which, in turn, adds its own prostatic fluid to this
mixture. Some prostatic fluid precedes ejaculation, but most of the released fluid is added
to the sperm and seminal fluid to constitute the semen. Only about 5% of the final
mixture comprising the ejaculate is composed of actual sperm. Prostatic fluid is both a
lubricant and a carrier of sperm and constitutes about 20% of the volume of the semen.
The muscles of the prostate are very active in the expulsion of semen from the body at
sexual climax. The stimulation of the prostate that activates ejaculation is responsible for
much of the intense pleasure that immediately precedes ejaculation. This fluid in man is
slightly acid in reaction (pH = 6.4). It is rich in calcium (30 mEq/ltr) and citrate (150
mEq/ltr) and in the enzyme fibrinolysin (Plasmin) and Acid Phosphatase. The low zinc
status of most men who suffer from BPH abets chronic low-level infection because free
zinc is the most active antibacterial agent found in prostatic fluids.
Shareera 57
Systemic hormonal influence (endocrine) and local growth factors (paracrine and
autocrine) were seen on prostate. Many local and systemic hormones whose exact
functions are not yet known govern the growth of the Prostate. The main hormone acting
on the Prostate is testosterone, which is secreted by the Leydig cells of the testes under
the control of luteinising hormone (LH), which is secreted from the anterior pituitary
under the control of hypothalamic luteinising hormone releasing hormone (LHRH).
Testosterone is converted to 5 di-hydrotestosterone (DHT) by the enzyme 5-α-reductase
that is found in high concentrations in the prostate and the perigenital skin. Other
androgens are secreted by the adrenal cortex but their effects are minimal. Estrogenic
steroids are also secreted by the adrenal cortex and, in the ageing male, may play part in
disrupting the delicate balance between DHT and local peptide growth factors and hence
increase the risk of BPH. Increased levels of serum estrogens, by acting on the
hypothalamus, decrease the secretion of LRHR (and hence LH) and thereby decrease
serum testosterone levels. Therefore, pharmacological doses of estrogens cause atrophy
of the testes and Prostate by means of reduction in testosterone.
The prostatic epithelium and mesenchymal stromal cells in response to steroid
hormones secrete other locally acting peptides. These include epidermal growth factor,
insulin-like growth factor, basic fibroblast growth factor, and transforming growth factors
alpha and beta. These undoubtedly play a part in normal and abnormal Prostatic growth
but, as yet, their functions are unclear.
Shareera 58
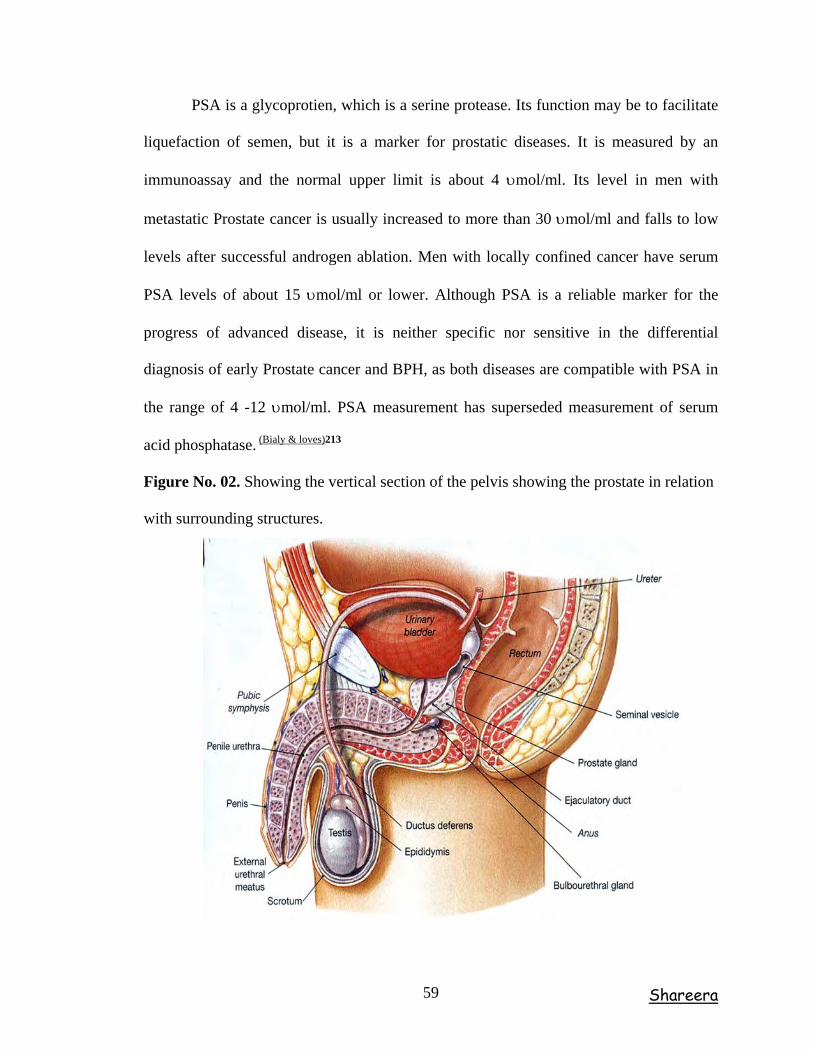
PSA is a glycoprotien, which is a serine protease. Its function may be to facilitate
liquefaction of semen, but it is a marker for prostatic diseases. It is measured by an
immunoassay and the normal upper limit is about 4 υmol/ml. Its level in men with
metastatic Prostate cancer is usually increased to more than 30 υmol/ml and falls to low
levels after successful androgen ablation. Men with locally confined cancer have serum
PSA levels of about 15 υmol/ml or lower. Although PSA is a reliable marker for the
progress of advanced disease, it is neither specific nor sensitive in the differential
diagnosis of early Prostate cancer and BPH, as both diseases are compatible with PSA in
the range of 4 -12 υmol/ml. PSA measurement has superseded measurement of serum
acid phosphatase. (Bialy & loves)213
Figure No. 02. Showing the vertical section of the pelvis showing the prostate in relation
with surrounding structures.
Shareera 59
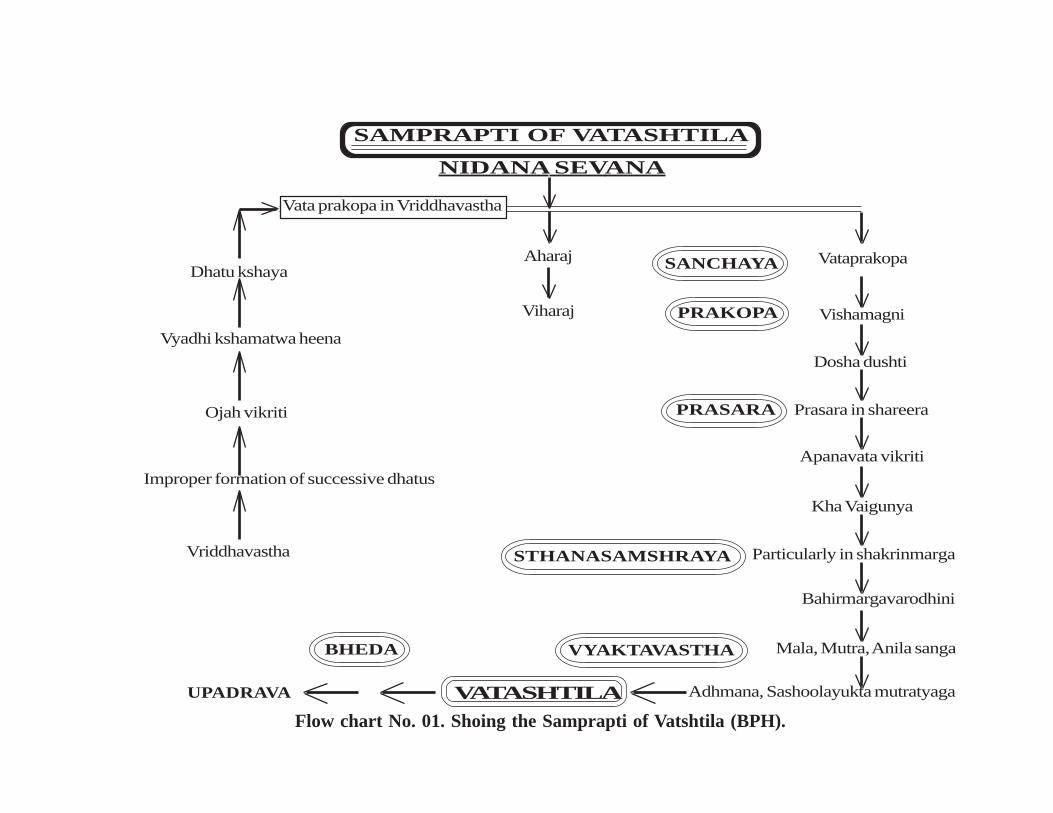
NIDANA SEVANA
Dhatu kshaya
Vyadhi kshamatwa heena
Ojah vikriti
Improper formation of successive dhatus
Vriddhavastha
Aharaj
Viharaj
SAMPRAPTI OF VATASHTILA
Vata prakopa in Vriddhavastha
Vataprakopa
Vishamagni
Dosha dushti
Prasara in shareera
Apanavata vikriti
Kha Vaigunya
Particularly in shakrinmarga
Bahirmargavarodhini
Mala, Mutra, Anila sanga
Adhmana, Sashoolayukta mutratyagaVATASHTILA
BHEDA
UPADRAVA
VYAKTAVASTHA
STHANASAMSHRAYA
PRASARA
PRAKOPA
SANCHAYA
Flow chart No. 01. Shoing the Samprapti of Vatshtila (BPH).
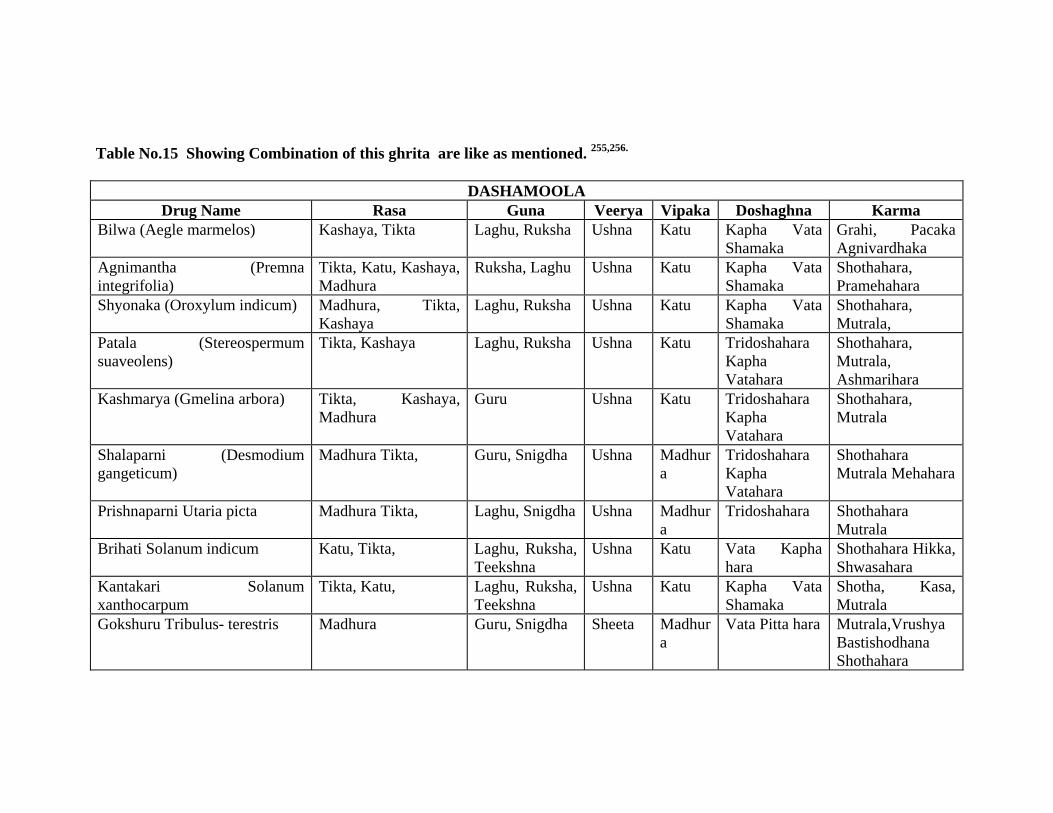
Table No.15 Showing Combination of this ghrita are like as mentioned. 255,256.
DASHAMOOLA Drug Name Rasa Guna Veerya Vipaka Doshaghna Karma
Bilwa (Aegle marmelos) Kashaya, Tikta Laghu, Ruksha Ushna Katu Kapha Vata Shamaka
Grahi, Pacaka Agnivardhaka
Agnimantha (Premna integrifolia)
Tikta, Katu, Kashaya, Madhura
Ruksha, Laghu Ushna Katu Kapha Vata Shamaka
Shothahara, Pramehahara
Shyonaka (Oroxylum indicum) Madhura, Tikta, Kashaya
Laghu, Ruksha Ushna Katu Kapha Vata Shamaka
Shothahara, Mutrala,
Patala (Stereospermum suaveolens)
Tikta, Kashaya Laghu, Ruksha Ushna Katu Tridoshahara Kapha Vatahara
Shothahara, Mutrala, Ashmarihara
Kashmarya (Gmelina arbora) Tikta, Kashaya, Madhura
Guru Ushna Katu Tridoshahara Kapha Vatahara
Shothahara, Mutrala
Shalaparni (Desmodium gangeticum)
Madhura Tikta, Guru, Snigdha Ushna Madhura
Tridoshahara Kapha Vatahara
Shothahara Mutrala Mehahara
Prishnaparni Utaria picta Madhura Tikta, Laghu, Snigdha Ushna Madhura
Tridoshahara Shothahara Mutrala
Brihati Solanum indicum Katu, Tikta, Laghu, Ruksha, Teekshna
Ushna Katu Vata Kapha hara
Shothahara Hikka, Shwasahara
Kantakari Solanum xanthocarpum
Tikta, Katu, Laghu, Ruksha, Teekshna
Ushna Katu Kapha Vata Shamaka
Shotha, Kasa, Mutrala
Gokshuru Tribulus- terestris Madhura Guru, Snigdha Sheeta Madhura
Vata Pitta hara Mutrala,Vrushya Bastishodhana Shothahara
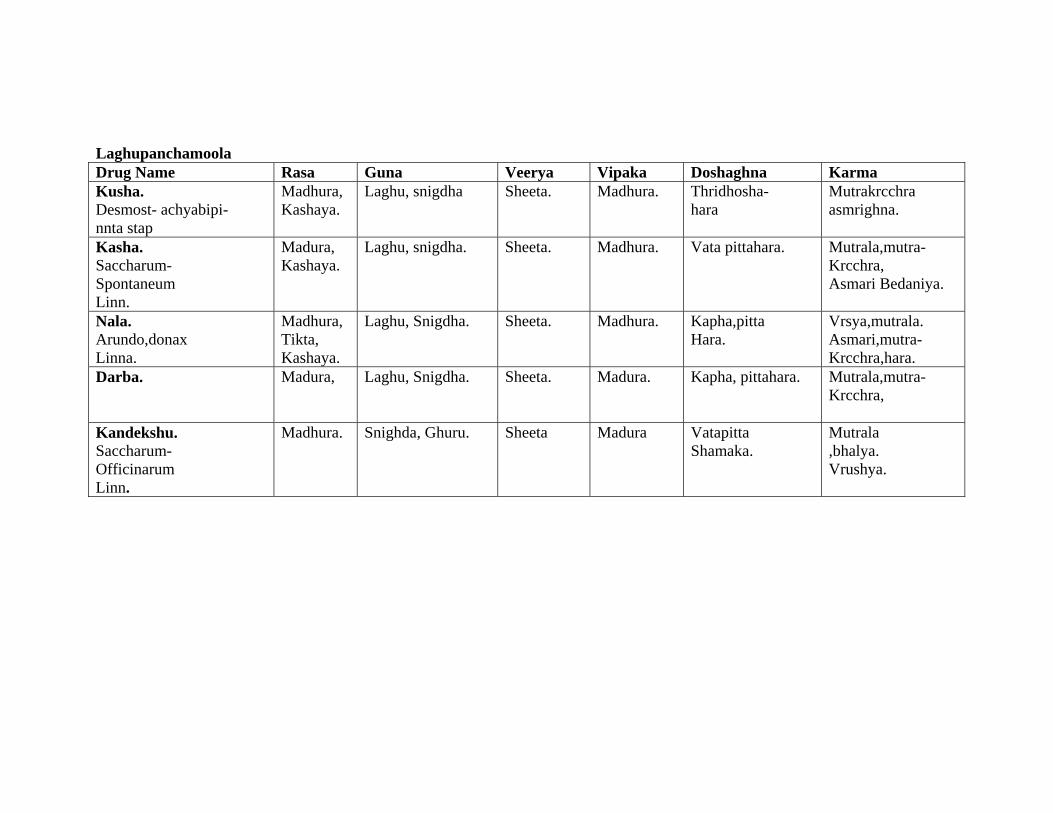
Laghupanchamoola Drug Name Rasa Guna Veerya Vipaka Doshaghna Karma Kusha. Desmost- achyabipi- nnta stap
Madhura, Kashaya.
Laghu, snigdha Sheeta. Madhura. Thridhosha- hara
Mutrakrcchra asmrighna.
Kasha. Saccharum- Spontaneum Linn.
Madura, Kashaya.
Laghu, snigdha.
Sheeta. Madhura. Vata pittahara. Mutrala,mutra- Krcchra, Asmari Bedaniya.
Nala. Arundo,donax Linna.
Madhura, Tikta, Kashaya.
Laghu, Snigdha. Sheeta. Madhura. Kapha,pitta Hara.
Vrsya,mutrala. Asmari,mutra- Krcchra,hara.
Darba.
Madura,
Laghu, Snigdha. Sheeta. Madura. Kapha, pittahara. Mutrala,mutra- Krcchra,
Kandekshu. Saccharum- Officinarum Linn.
Madhura.
Snighda, Ghuru. Sheeta Madura Vatapitta Shamaka.
Mutrala ,bhalya. Vrushya.
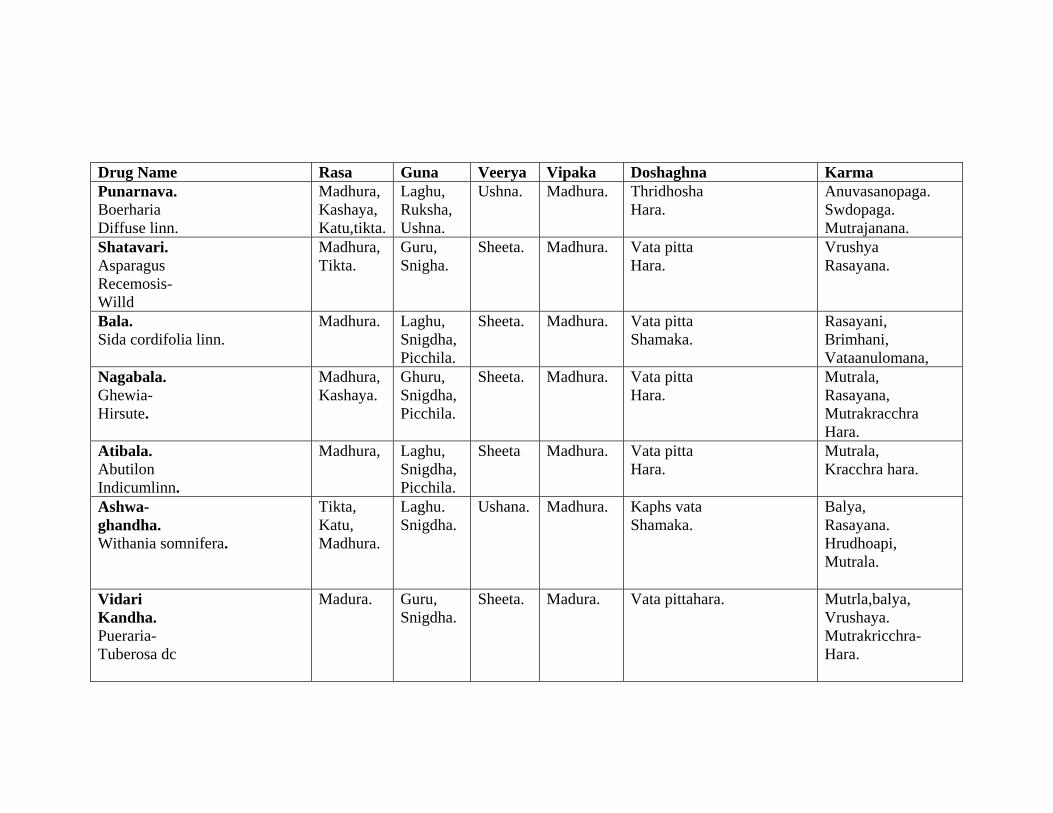
Drug Name Rasa Guna Veerya Vipaka Doshaghna Karma Punarnava. Boerharia Diffuse linn.
Madhura, Kashaya, Katu,tikta.
Laghu, Ruksha, Ushna.
Ushna. Madhura. Thridhosha Hara.
Anuvasanopaga. Swdopaga. Mutrajanana.
Shatavari. Asparagus Recemosis- Willd
Madhura, Tikta.
Guru, Snigha.
Sheeta. Madhura. Vata pitta Hara.
Vrushya Rasayana.
Bala. Sida cordifolia linn.
Madhura. Laghu, Snigdha, Picchila.
Sheeta. Madhura. Vata pitta Shamaka.
Rasayani, Brimhani, Vataanulomana,
Nagabala. Ghewia- Hirsute.
Madhura, Kashaya.
Ghuru, Snigdha, Picchila.
Sheeta. Madhura. Vata pitta Hara.
Mutrala, Rasayana, Mutrakracchra Hara.
Atibala. Abutilon Indicumlinn.
Madhura,
Laghu, Snigdha, Picchila.
Sheeta Madhura. Vata pitta Hara.
Mutrala, Kracchra hara.
Ashwa- ghandha. Withania somnifera.
Tikta, Katu, Madhura.
Laghu. Snigdha.
Ushana. Madhura.
Kaphs vata Shamaka.
Balya, Rasayana. Hrudhoapi, Mutrala.
Vidari Kandha. Pueraria- Tuberosa dc
Madura. Guru, Snigdha.
Sheeta. Madura. Vata pittahara. Mutrla,balya, Vrushaya. Mutrakricchra- Hara.
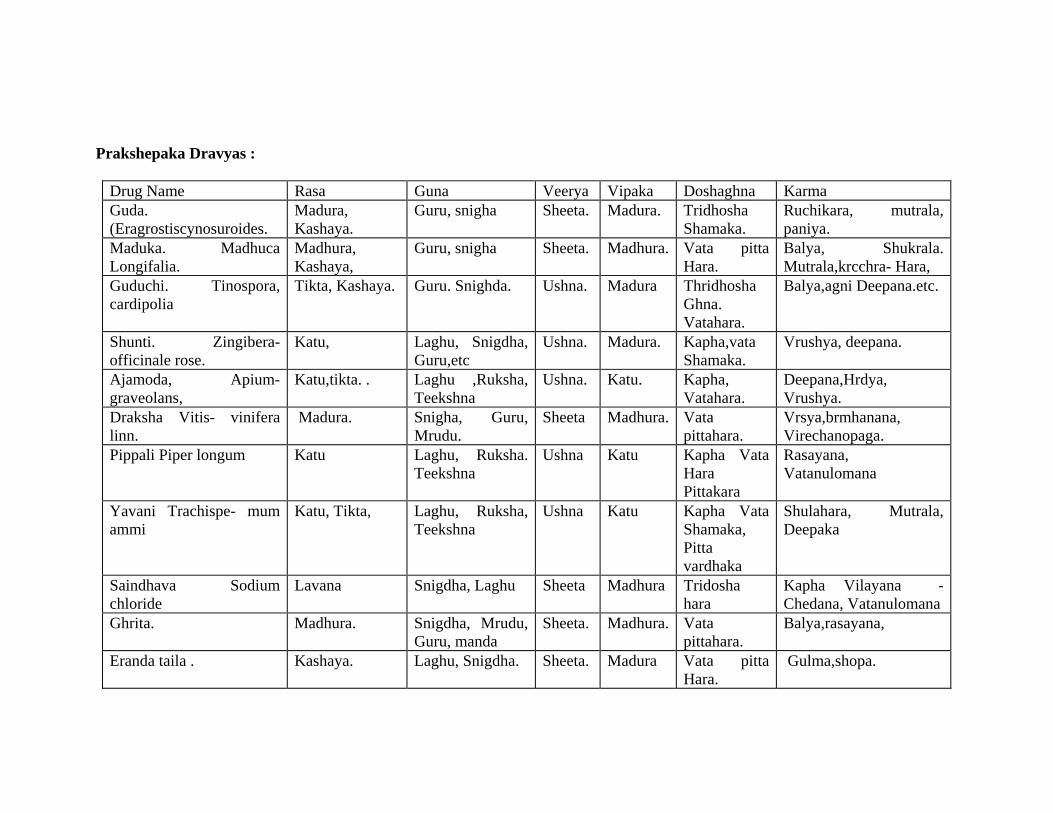
Prakshepaka Dravyas :
Drug Name Rasa Guna Veerya Vipaka Doshaghna Karma Guda. (Eragrostiscynosuroides.
Madura, Kashaya.
Guru, snigha Sheeta. Madura. Tridhosha Shamaka.
Ruchikara, mutrala, paniya.
Maduka. Madhuca Longifalia.
Madhura, Kashaya,
Guru, snigha Sheeta. Madhura. Vata pitta Hara.
Balya, Shukrala. Mutrala,krcchra- Hara,
Guduchi. Tinospora, cardipolia
Tikta, Kashaya. Guru. Snighda. Ushna. Madura Thridhosha Ghna. Vatahara.
Balya,agni Deepana.etc.
Shunti. Zingibera- officinale rose.
Katu, Laghu, Snigdha, Guru,etc
Ushna. Madura. Kapha,vata Shamaka.
Vrushya, deepana.
Ajamoda, Apium- graveolans,
Katu,tikta. . Laghu ,Ruksha, Teekshna
Ushna. Katu. Kapha, Vatahara.
Deepana,Hrdya, Vrushya.
Draksha Vitis- vinifera linn.
Madura. Snigha, Guru, Mrudu.
Sheeta Madhura. Vata pittahara.
Vrsya,brmhanana, Virechanopaga.
Pippali Piper longum Katu Laghu, Ruksha. Teekshna
Ushna Katu Kapha Vata Hara Pittakara
Rasayana, Vatanulomana
Yavani Trachispe- mum ammi
Katu, Tikta, Laghu, Ruksha, Teekshna
Ushna Katu Kapha Vata Shamaka, Pitta vardhaka
Shulahara, Mutrala, Deepaka
Saindhava Sodium chloride
Lavana Snigdha, Laghu Sheeta Madhura Tridosha hara
Kapha Vilayana - Chedana, Vatanulomana
Ghrita. Madhura. Snigdha, Mrudu, Guru, manda
Sheeta. Madhura. Vata pittahara.
Balya,rasayana,
Eranda taila . Kashaya. Laghu, Snigdha. Sheeta. Madura Vata pitta Hara.
Gulma,shopa.
VATASHTILA CHIKITSA
Chikitsa means, a combined operation of all the four factors, viz. the Physician
and the other three factors of commendable qualities, with the object of engendering the
concordance of dhatu when pathological changes have occurred in them due to different
Nidana. (Ch. Su.9)238
There is no specific treatment mentioned in classics for Vatashtila (BPH). But,
Mutraghata and Mutrashmari chikista can be used as it is a type of Mutraghata. Sushruta
has mentioneda special treatment i.e. “Gulma Abyantara Vidradivat”239 for Vatashtila
(BPH). But in Mutraghata chikitsa the chikitsoprakamas are depending upon the extend
of vitiation and direction of movement of vayu.240,241(Ch.Chi.28). Basti is one among the
Trividha sadyopranahara marma, so Basti marma paripalana must be kept in mind while
treating.242 To Precautions to be taken to prevent damage to Marma and to maintain the
hygienic measures routinly (Nityam Svasth vrutta auvartanam) (Ch.Si.9)243 Treatment
should be aimed at establishing proper nutrients to Basti marma. So those structures of
Basti receives nourishment only when the nutrient supplying channels are cleared and
Apanavayu made its sanchalana. Basti karma is well appreciated in Charaka samhita
siddhisthana. (ChSi.9/49).244
Avagaha Swedana that alleviate Apana Vata from its main place and removes
obstruction of Mutravaha Srotas and leads to normal voiding of Mutra. Abhyanga due to
its Mardava, Snigdha, Manda, and Guru quality alleviate Vata Dosha. All three types of
Basti are indicated i.e. Niruha, Anuvasana and Uttara Basti (Ch.Su.7, Ch.Chi.28). These
directly act on Vyadhi Udbhava and Adhishthana pradesha (Pakwashaya and Basti) and
disintegrate the Vatashtila pathology. Mutra Virechaneeya medicines and Uttara Basti
can be administered (Ch.Chi.28). Charaka also suggests the utility of Avapeedaka
Sneha.245
Chikitsa 75
Hence at a outstretch the aim of treatment is -
Nidana Parivarjana.
Apanavata Anulomana246
Increasing the stability of Mutravaha Srotas and particularly of Basti.
Removing the Sanga (Obstruction).
Reducing the Ghanatwa of Granthi.
Protecting the Basti marma.
Making proper flow of Urine with Mutrala and Basti Shodhaka drugs.
Following Proper Diet And Regimen
A concise outline can be drawn to manage the problem of Vatashtila (Mutraghata)
according to classics. i.e.
Nidana Parivarjana.
Shodhana.
Shamana.
Shastra Pranidhana.
Rasayana.
Pathya-Apathya.
1. Nidana Parivarjana – It may be further classified as under -
Ahara – Excessive use of Ruksha, Madya, Teekshna ahara and to avoid fasting for
long time.
Vihara – Suppressing the natural urge particularly of Mutra. Performing sexual
intercourse while under the urge of micturition. Excessive exercise, speedy
walking, sitting under the direct sun light continuously etc.
Anya – Avoiding the Teekshna oushadha and psychological depression etc.
Chikitsa 76
2. Shodhana – When Doshas are increased extremely Shodhana Chikitsa become
necessary. While describing the Mutraghata chikitsasutra Sushruta says that in case of
Mutraghata snigdha virechana, Basti and Uttarabasti should be administered according to
the condition of Dosha. Further more he advised to undertake Poorvakarma such as
Snehapana, Snehana/Abhyanga and Swedana followed by Virechana till the Dosha are
eliminated out of the body and then Uttarabasti is advocated. (Su.Ut.58).247 In addition to
this he suggests the Prayoga of Asthapanabasti too. (Su.Chi.35).
Charaka suggests the usage of Trividha basti Karma in Mutra Roga (Ch.Su.7,
Ch.Si.9).248 He also suggests Mutrala drugs, Swedana - especially Avagaha swedana,
Abhyanga, Sarpipana and Uttara Basti (Ch.Chi.28), (Ch.Chi.28/99) & (Ch.Su.7).
Avapeedaka sneha prayoga is a special type of Sneha administered as
Jeernantikamatra.249 After the digestion of Sneha food is given and followed by Sneha
once again. Here giving excessive dosage of Sneha makes Peedana of Dosha and there by
palliate the aggravated Dosha. Acharya Vagbhata advises Tailvaka ghrita for
Virechanartha, Basti karma and especially for Uttarabasti. (A.H.Chi.11, A.S.Chi.13).
3. Shamana – While describing the Mutraghata Chikitsa Acharya Sushruta says
to administer various types of Kashaya, Kalka, Ghrita, Modaka, Avaleha, Dugdha,
Kshara, Asava etc. (Su. Ut.58). Further he says to administer Ashmari hara and Mutra
Udavartahara yogas (Su.Ut.58). Whereas Acharya Charaka states that after diagnosing
the predominance of morbid Dosha, these conditions should be prepared by the measures
curative of Mutrakricchra hara (ChSi.9/49). Acharya Vagbhata has devoted one full
chapter namely Mutraghata chikitsa adhyaya (A. Hr.Chi.11).
Chikitsa 77
4. Shastra Pranidhana Chikitsa – It is further classified into two groups as
under Shalya chikitsa. On going through all the classics it seems to be that no operative
procedures were mentioned for the treatment of Mutraghata.
5. Anu Shalya Chikitsa – Reference of Para-surgical intervention, in the form of
urethral catheterization to drain the bladder in retention of urine, can be traced back to the
Vedic period (A.V.1/1-3). Acharya Sushruta has included Mutra vishodhani Shalaka.
About its function, he has said that it does Marga vishodhana (Su. Su.7). In this context
Dalhana says that Margavishodhana is to be performed during the conditions of Mutra
Sanga and Pureesha sanga (Dal - Su.Su.7).
6. Rasayana – Acharya Vagbhata said to prepare Shilajatu by giving the bhavana
of Veerataradi gana dravya and then it should be given to the patients of Mutraghata.
(A.H.Chi.11/39). It is mainly used for Rasayana purpose. Rasayana chikitsa plays very
important role in Vatashtila / BPH as it is seen in elderly patients where Vata dosha is
predominant and it is also a stage of degeneration of the body.
PATHYA-APATHYA
The entire Ayurvedic system of healing is based on two major principles that is
"Maintaining The Health Of Healthy Persons And Curing The Ailments Of The Patients".
Healthy living is the most important aspect of Ayurveda but unfortunately this has been
the most neglected part. This can be achieved only by the Pathya ahara, which can
nourish both body and mind. Importance of Pathya is to increase the digestive power
there by proper production of optimum quality of Ahara Rasa that nourishes the Dhatu
through these Srotas.
Chikitsa 78
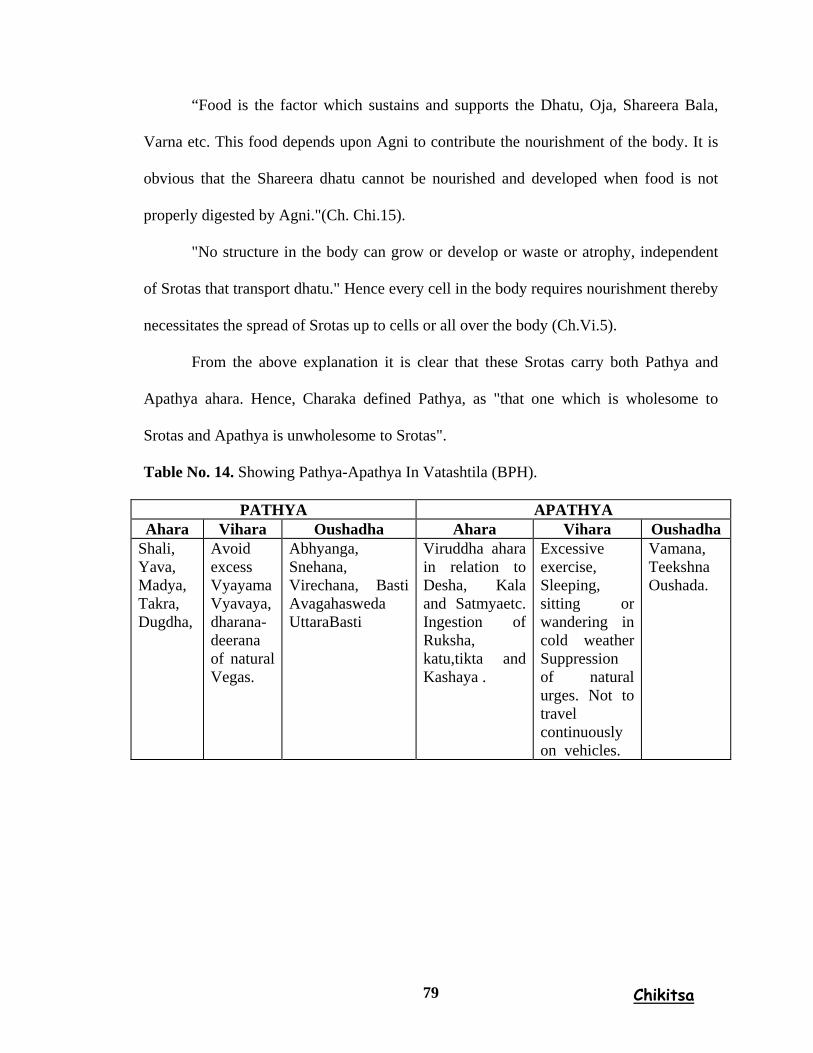
“Food is the factor which sustains and supports the Dhatu, Oja, Shareera Bala,
Varna etc. This food depends upon Agni to contribute the nourishment of the body. It is
obvious that the Shareera dhatu cannot be nourished and developed when food is not
properly digested by Agni."(Ch. Chi.15).
"No structure in the body can grow or develop or waste or atrophy, independent
of Srotas that transport dhatu." Hence every cell in the body requires nourishment thereby
necessitates the spread of Srotas up to cells or all over the body (Ch.Vi.5).
From the above explanation it is clear that these Srotas carry both Pathya and
Apathya ahara. Hence, Charaka defined Pathya, as "that one which is wholesome to
Srotas and Apathya is unwholesome to Srotas".
Table No. 14. Showing Pathya-Apathya In Vatashtila (BPH).
PATHYA APATHYA Ahara Vihara Oushadha Ahara Vihara Oushadha
Shali, Yava, Madya, Takra, Dugdha,
Avoid excess Vyayama Vyavaya, dharana-deerana of natural Vegas.
Abhyanga, Snehana, Virechana, Basti Avagahasweda UttaraBasti
Viruddha ahara in relation to Desha, Kala and Satmyaetc. Ingestion of Ruksha, katu,tikta and Kashaya .
Excessive exercise, Sleeping, sitting or wandering in cold weather Suppression of natural urges. Not to travel continuously on vehicles.
Vamana, Teekshna Oushada.
Chikitsa 79
MANAGEMENT OF BPH
1. Non operative treatment –
The treatment of any disease depends on the magnitude of the clinical effect and
the incidence and severity of treatment related morbidity, assessing the effectiveness of
treatment related morbidity, assessing the effectiveness of medical therapies for BPH.
A. Conservative – 'watchful waiting' - general advice about fluid intake i.e. less intake of
fluid after evening, avoiding caffeinated and alcoholic beverages, and smoking.250
B. Pharmacological treatment – α-blockers, Terazosin, Prazosin, Phenoxybenzymine,
Alfuzosin, Indoramine etc.251
C. Testosterone Ablation Agents – Diethyle stilbestrol, Flutamide, GnRh Analogues,
Progesterone derivatives etc.
D. 5-α reductase inhibitors – Finasteride, Epristeride, Combined agents, Hormonal
manipulation with Antiandrogens. In addition aromatase inhibitors are also used.252
2. Conventional operative treatment –
Trans Urethral Resection of Prostate (TURP)
Bladder neck incision for the small prostate (under 20 gm)
Open Prostatectomy for the big gland (around 80 -100 or more)
Suprapubic Transvesical Prostatectomy.
Simple Retropubic Prostatectomy.
Perineal Prostatectomy.
Trans Urethral Incision of the Prostate (TUIP).
Chikitsa 80
3. Minimally invasive methods –
Intraprostatic Stents.
Contact Laser of the Prostate.
Trans Urethral Microwave Therapy.
Trans Urethral Laser Ablation of the Prostate (TULAP).
Trans Urethral Vaporization of Prostate (TUVP).
Trans Urethral Needle Ablation of the Prostate (TUNA).
Diode Laser.
4. Clinical Endpoints –
The clinical consequences of BPH include LUTS; detrusor dysfunction
characterized by detrusor acontractility, detrusor instability, and detrusor fibrosis;
incomplete bladder emptying; acute and chronic renal retention; urinary tract infection;
renal insufficiency; and haematuria.
The goals of treatment for BPH include -
Relieving LUTS,
Decreasing BOO,
Improving bladder emptying,
Ameliorating detrusor instability,
Reversing renal insufficiency,
Preventing future episodes of gross haematuria,
Urinary tract infection, Urinary retention.
The treatment of any disease depends on the magnitude of the clinical effect and
the incidence and severity of treatment related morbidity, assessing the effectiveness of
treatment related morbidity, assessing the effectiveness of medical therapies for BPH.
Chikitsa 81
DRUG REVIEW
The main motto of this study is to assess the comparative effect of Matrabasti and
as Shamana snehapana with sukumarakumara ghrita. 253
In Ayurveda the success of Chikitsa depends totally upon Chikitsa Chatushpadas.
Among these four basic factors of treatment, Dravya has been awarded the second place.
The selection of a proper drug in the management of disease is very important. Therefore
sufficient attention should be given for selecting the drug. Ghrita, Taila, Vasa, Majja are
the best Sneha dravyas among all snehas. Out of these four, Ghrita is the best Sneha
Dravya for par excellence because of its power to assimilate the properties of the
substance.
Sukumara Kumaraka Ghrita is mentioned by textbook of Chakradutta253 and
Bhaishajyaratnavali in Mutrakricchra chikitsa.254 They have mentioned number of Yogas,
pertaining to Mutrakricchra and Mutraghata. Sukumara Kumaraka Ghrita, the name itself
indicates it is recommended for Sukumaras i.e. old aged persons without any hesitation.
The ingredients viz- Dashamula, Laghupanchamoola, Punarnava etc are having
properties like Balya, Rasayana, sheetam and sukumarakam. This is Indicated in
mootrakricchra, gulma, vataroga, etc. which helps in correcting the pathology of
Vatashtila (BPH).
Methodology 82
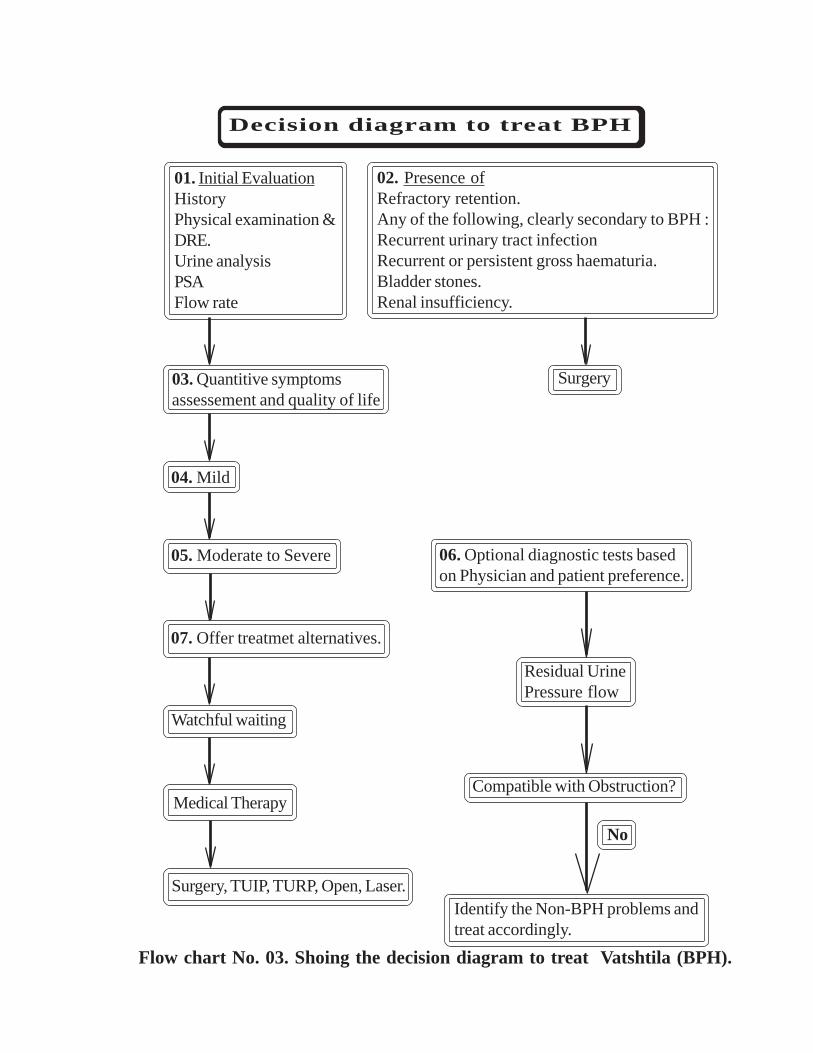
01. Initial EvaluationHistoryPhysical examination &DRE.Urine analysisPSAFlow rate
02. Presence ofRefractory retention.Any of the following, clearly secondary to BPH :Recurrent urinary tract infectionRecurrent or persistent gross haematuria.Bladder stones.Renal insufficiency.
03. Quantitive symptomsassessement and quality of life
04. Mild
05. Moderate to Severe 06. Optional diagnostic tests basedon Physician and patient preference.
07. Offer treatmet alternatives.
Watchful waiting
Residual UrinePressure flow
Compatible with Obstruction?
Identify the Non-BPH problems andtreat accordingly.
Surgery
No
Surgery, TUIP, TURP, Open, Laser.
Medical Therapy
Decision diagram to treat BPH
Flow chart No. 03. Shoing the decision diagram to treat Vatshtila (BPH).
CLINICAL STUDY
Methodological approach is the backbone of research. Utmost care is taken in
designing a methodology for conducting this research. Clinical trial is a way of research
and it is the best method to evaluate any drug or line of treatment. It involves the
experimentation of a drug or therapy on a population and recording the feedback based
on which postulations are made regarding the usefulness of the drug or therapy in the
disease. Hence, this trial is a carefully designed experiment with the aim of solving
problems conducted on scientific lines.
Research Approach
The present clinical study is powerful research, with an objective to evaluate
comparative effect of Matrabasti and as Shamana snehapana with Sukumara kumaraka
ghrita in the management of Vatashtila (BPH). The effect is to be determined by finding
out the difference between the base line data before and after treatment.
Study Design
The study design selected for the present study was prospective comparative
clinical trial. Here, Matrabasti, group of patients are compared with the Shamana sneha
group of patients. Demographic data and disease-specific data are collected according to
the case record proforma given in the appendix.
Reasons For Selection Of The Study Design
The results and conclusions of a clinical trial depends on the study design. The
aim of this study was to find out the effect of Matrabasti, and Shamana sneha, in the
management of Vatashtila (BPH). Therefore, two groups were made and the results
obtained in both the individual groups were compared.
Methodology 87
Source of Data
Patients suffering from Vatashtila (BPH) were selected from the P.G.R.S & R
(Panchakarma) OPD & IPD of Shri. D. G. Melmalagi Ayurvedic Medical College
Hospital, Gadag.
Sample Size and Grouping
The sample size for the present study was 30, patients suffering from Vatashtila as
per the selection criteria. Patients were randomly distributed to both the groups of equal
size. In group A, 15 patients received Matrabasti and in group B, 15 patients received
Shamanasneha.
Selection Criteria
The cases were selected strictly as per the preset inclusion and exclusion criteria.
A) Inclusion Criteria
1 Patients who were aged above50years and below 70years.
2 Patients fit for Matrabasti and Shamana sneha.
3 Patients with the clinical features of Vatashtila (BPH) (I-PSS Index)
4 Digital rectal examination findings i.e. (enlargement of prostate) Vatashtila (BPH)
5 Ultrasonography findings suggestive of Vatashtila (BPH).
B) Exclusion Criteria
1 Patients below 50 years and above 70 years of the age.
2 Patients with other systemic and metabolic disorders viz:- urethral stricture,
calculus, prostatitis carcinoma of the prostate and bladder instability.
Duration of The Study
The total study duration was 24 days i.e.
Group A -(8 days Matrabasti, and 16 days Parihara kala.
Group B -(16 days Shamana sneha, and 8 days parihara kala.
Methodology 88
Data Collection
Patients were thoroughly examined both subjectively and objectively. Detailed
history pertaining to the mode of onset, previous ailment, previous treatment history,
family history, habits, Ashtavidhapareeksha and Dashavidhapareeksha and physical
examination findings were noted. Routine investigations were done to exclude other
pathologies.
Examination of the patient
History – History taking of patient is very important to diagnose the diseases
specially benign prostate hyperplasia. When medical history focusing on the urinary tract,
specific things to discussed when taking the history of a man with BPH symptoms
include a history of hematuria, UTI, tuberculosis, diabetes, etc.
Inspection – In case of BPH, the abdomen and genitalia should be examined by
inspection. We can observe the abnormalities in genital organs, etc. if residual urine in
excess of 500 ml, usually produces a visibly distended bladder.
Palpation – Should be accurate to identify any organomegaly, asymmetry,
tenderness, or Mass in the area of abdomen and pelvic reign.
Percussion – It is to understand the gas, watery or any mass. The bladder must
contain at least 150 ml of fluid to allow its detection by percussion. It can be used to
identify the Adhmana and Anilasanga.
Auscultation – It is helpful to elicit the Adhmana and Anilasanga by hearing the
sound like (gudu gudu).
Methodology 89
TREATMENT SCHEDULE
Group A - Matrabasti
Poorvakarma – Patient was given the Sthanika mridu abhyanga and swedana
prior to the pradhanakarma. The abhyanga was done with Murcchita Tila taila. Then
advised to have alpa ahara and made to take a short walk. Encourage to pass his natural
urges previously, and asked the patient to lay down on table of suitable to his height, in
left lateral position.
Pradhanakarma – Matrabasti was administered to using sterilized 100 ml of
glicerine syringe. A quantity of 70 ml Ghrita was injected through the rectum in a luke
warm temperature, after the proper preparation of Dravya as per the classical method
discussed in drug review. The method of administration of bastidravya was strictly
followed as per classics. After the basti, the patient was made to lie on supine posture just
after (5 to 10 min) and gentle tapping was made on his buttocks, legs were lifted up, hips
were tapped thrice and made pressure over abdomen. Asked to wet for 10min in supine
posture, the same procedure was repeated for 8 days and it was conducted in a time
between 9.30 to 10.30 am. The time of administration, the time of retention and any
complications present were `recorded in case sheet proforma.
Pariharakala of 16 days was advised and reported asked the patient to report on
24th day counting from the day of initiation of treatment protocol and observation done
on 24th day.
Methodology 90
Group B – Shamana snehapana
Poorvakarma – Patients were advised to take mridu bhojana at night prior to
shamana Snehapana. Because on the day of Snehapana, the food of the previous day must
have to undergo digestion and patient must feel hunger (i.e. Bubhukshita). Then only the
patient is prepared for shamana snehapana.
Pradanakarma – Next day morning i.e. on the day of Shamana snehapana after
elimination of routine urges, jeerna ahara lakshana should be assessed. Then the 15 ml of
Sukumaraka kumaraka ghrita should be taken with a fresh mind, enthusiasm, courage, by
praying God. Same procedure should be follow twice daily for 16 days.
Paschat karma – Ushnajala should be given as Anupana. The patient is kept
under keen observation till the “Sneha jeerna lakshanas” appears. The patients were
advised to follow strictly the rules and regulations of Pathyapathya as explained in
Snehapana vidhi adhyaya. Followed with Pariharakala of 8 days, patients is asked to
report on 24th day from the day of commencing the treatment protocol.
Diagnostic Criteria
The diagnosis of Vatashtila (BPH) was made according to the signs and
symptoms of the classics and modern science explantion, also with objective parameters.
Signs and symptomatology of Vatashtila (BPH) are mentioned for its diagnosis, but those
may not be sufficient for the diagnose of this disease. Hence, for better understanding of
the diseases, and purpose of the adaptation of resent advancement of for the appropriate
diagnosing the disease, laboratory investigations are essential.
Methodology 91
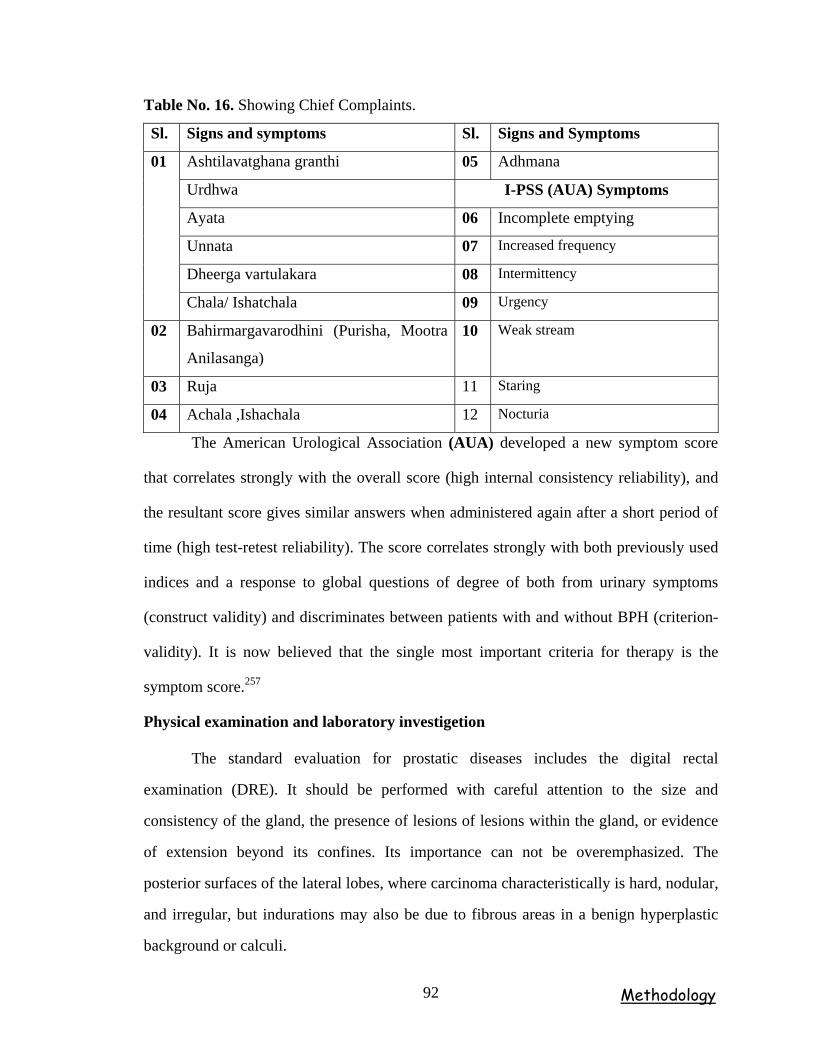
Table No. 16. Showing Chief Complaints.
Sl. Signs and symptoms Sl. Signs and Symptoms
Ashtilavatghana granthi 05 Adhmana
Urdhwa I-PSS (AUA) Symptoms
Ayata 06 Incomplete emptying
Unnata 07 Increased frequency
Dheerga vartulakara 08 Intermittency
01
Chala/ Ishatchala 09 Urgency
02 Bahirmargavarodhini (Purisha, Mootra
Anilasanga)
10 Weak stream
03 Ruja 11 Staring
04 Achala ,Ishachala 12 Nocturia
The American Urological Association (AUA) developed a new symptom score
that correlates strongly with the overall score (high internal consistency reliability), and
the resultant score gives similar answers when administered again after a short period of
time (high test-retest reliability). The score correlates strongly with both previously used
indices and a response to global questions of degree of both from urinary symptoms
(construct validity) and discriminates between patients with and without BPH (criterion-
validity). It is now believed that the single most important criteria for therapy is the
symptom score.257
Physical examination and laboratory investigetion
The standard evaluation for prostatic diseases includes the digital rectal
examination (DRE). It should be performed with careful attention to the size and
consistency of the gland, the presence of lesions of lesions within the gland, or evidence
of extension beyond its confines. Its importance can not be overemphasized. The
posterior surfaces of the lateral lobes, where carcinoma characteristically is hard, nodular,
and irregular, but indurations may also be due to fibrous areas in a benign hyperplastic
background or calculi.
Methodology 92
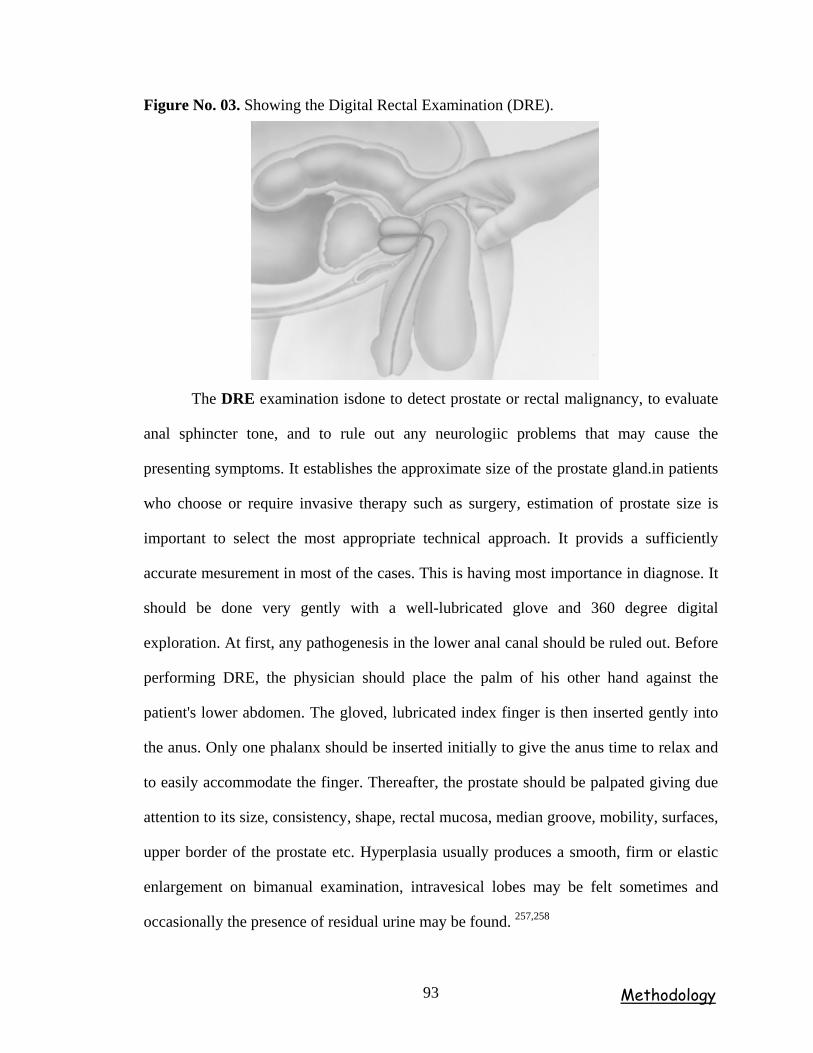
Figure No. 03. Showing the Digital Rectal Examination (DRE).
The DRE examination isdone to detect prostate or rectal malignancy, to evaluate
anal sphincter tone, and to rule out any neurologiic problems that may cause the
presenting symptoms. It establishes the approximate size of the prostate gland.in patients
who choose or require invasive therapy such as surgery, estimation of prostate size is
important to select the most appropriate technical approach. It provids a sufficiently
accurate mesurement in most of the cases. This is having most importance in diagnose. It
should be done very gently with a well-lubricated glove and 360 degree digital
exploration. At first, any pathogenesis in the lower anal canal should be ruled out. Before
performing DRE, the physician should place the palm of his other hand against the
patient's lower abdomen. The gloved, lubricated index finger is then inserted gently into
the anus. Only one phalanx should be inserted initially to give the anus time to relax and
to easily accommodate the finger. Thereafter, the prostate should be palpated giving due
attention to its size, consistency, shape, rectal mucosa, median groove, mobility, surfaces,
upper border of the prostate etc. Hyperplasia usually produces a smooth, firm or elastic
enlargement on bimanual examination, intravesical lobes may be felt sometimes and
occasionally the presence of residual urine may be found. 257,258
Methodology 93
Ultrasonography
A detailed USG of both abdomen and pelvis was carried out before and after the
treatment in relation to the bladder wall thickness, trabacular pattern, residual urine,
prostate volume, prostate size and kidneys in general.
The most common method is ultrasound to determination of the size (i.e.height,
width, length) and approximate weight of the prostate, and further important is post voide
residual urine volume measurement, i.e. PVR urine is the volume of fluid remaining in
the bladder immediately after the completion of miturition. The studies indicate that
residual urine normally ranges from 0.09 to 2.24 ml, with the men being 0.53ml (Hinman
and Cox, 1967). 78% of normal men have PVR’s of less then 5ml, and 100% have
volumes of less than 12ml by (Di mare et al, 1963). Ultrasound is the standard diagnostic
instrument for the BPH. The size of prostate is estimated approximately by the
Ultrasonography and made 1 to 4 grading for diagnose the severity of BPH.
Score chart for size of prostate.
Grade 1 – 20 to 25 gms.
Grade 2 – 26 to 50 gms.
Grade 3 – 51 to 75 gms.
Grade 4 – above 75 gms.
Methodology 94
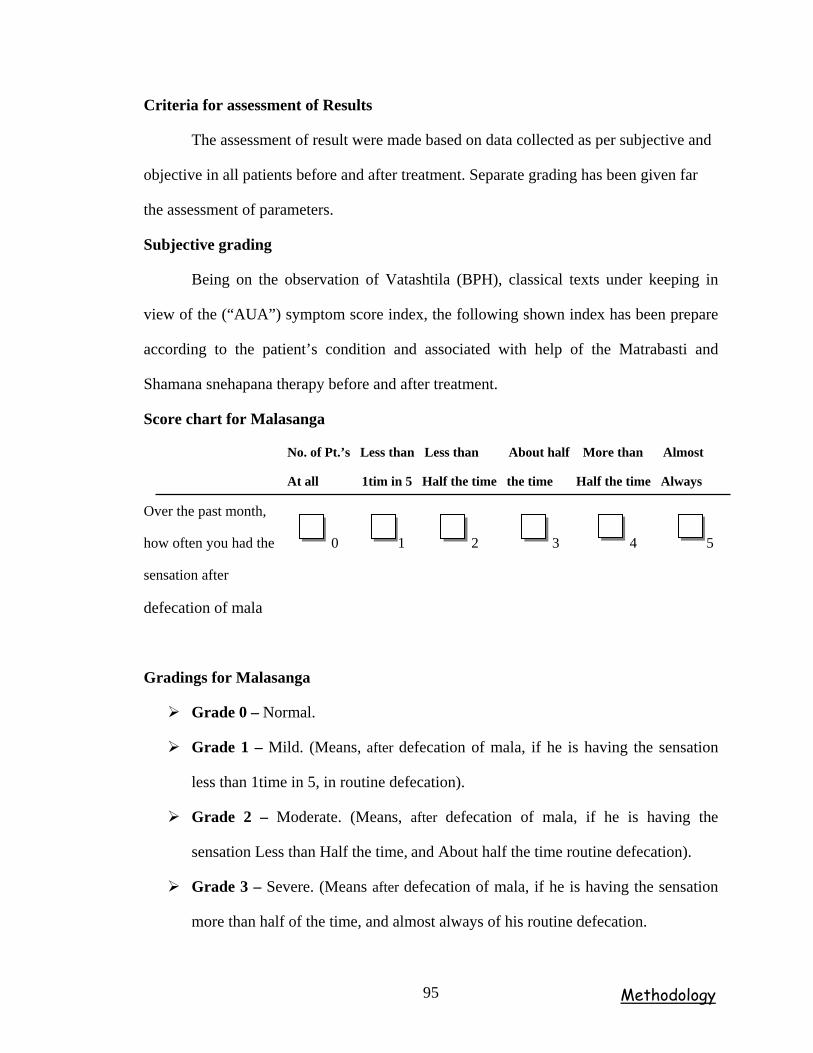
Criteria for assessment of Results
The assessment of result were made based on data collected as per subjective and
objective in all patients before and after treatment. Separate grading has been given far
the assessment of parameters.
Subjective grading
Being on the observation of Vatashtila (BPH), classical texts under keeping in
view of the (“AUA”) symptom score index, the following shown index has been prepare
according to the patient’s condition and associated with help of the Matrabasti and
Shamana snehapana therapy before and after treatment.
Score chart for Malasanga
No. of Pt.’s Less than Less than About half More than Almost
At all 1tim in 5 Half the time the time Half the time Always
Over the past month,
how often you had the 0 1 2 3 4 5
sensation after
defecation of mala
Gradings for Malasanga
Grade 0 – Normal.
Grade 1 – Mild. (Means, after defecation of mala, if he is having the sensation
less than 1time in 5, in routine defecation).
Grade 2 – Moderate. (Means, after defecation of mala, if he is having the
sensation Less than Half the time, and About half the time routine defecation).
Grade 3 – Severe. (Means after defecation of mala, if he is having the sensation
more than half of the time, and almost always of his routine defecation.
Methodology 95
Overall Response Assessment Criteria for Malasanga
Poor response – Means, if severity is reduced by grade 1, then it is considered as
poor response to the treatment.
Moderately response – Means, if severity is reduced by grade 2, then it is
considered as Moderate response of treatment.
Good response – Means, if severity is reduced to grade 0, then it is considered as
Good response of treatment. If the bowel habit returns to grade 0, then that will
be considered as Good response.
Not responded – Means, if severity is not reduced or increase, then it is
considered as Not respond from the treatment.
Score chart for Mutra sanga
Grade- 0 - 500-2500ml. Per day.
Grade -1 - 400-500ml. Per day.
Grade -2 - 300-400ml. Per day.
Grade -3 - 200-300ml. Per day.
Overall Response Assessment Criteria for Mutrasanga
Poor response – Means, (If there is increase in micturation by 100ml and severity
is reduced by grade 1, then it is considered as poor response of treatment.
Moderately response – Means, (If there is increase in micturation by 200ml to
300ml severity is reduced by grade 2, then it is considered as Moderate response
of treatment.
Good response – Means (If there is increase in micturation by 400ml to 500ml
severity is reduced to grade 0, then it is considered as Good response of
treatment. If the severity is reduced from any other to grade 0, then it is
considered as Good response.
Not respond – Means (If severity is neither reduced nor increased, then it is
considered as No response to the treatment.
Methodology 96
Score chart for Anilasanga (By percussion and auscultation)
Sounds heard Grade 1 + Means – Mild
Sounds heard Grade 2 ++ Means – Moderate
Sounds heard Grade 3 +++ Means – Sever
All sounds Absent Grade 0 Means – Normal
Overall Response Assessment Criteria for Anilasanga
Poor response – Means if Severity is reduced by grade 1, then it is considered as
poor response to the treatment.
Moderately response – Means if Severity is reduced by grade 2, then it is
considered as Moderate response to the treatment.
Good response – Means if Severity is reduced to grade 0, then it is considered as
Good response to the treatment. If the Severity is reduced from any other to grade
0, that is considered as Good response to the treatment.
Not respond – Means if Severity is neither reduced nor increased, then it is
considered as No response to the treatment.
Score chart for Adhmana (By percussion and auscultation)
Sounds heard Grade 1 + Means – Mild
Sounds heard Grade 2 ++ Means – Moderate
Sounds heard Grade 3 +++ Means – Sever
All sounds Absent Grade 0 Means – Normal
Overall Response Assessment Criteria for Adhmana
Poor response – Means, if Saatopa (Gudaguda sound in abdomen) is reduced by
grade 1, then it is considered as poor response to the treatment.
Methodology 97
Moderately response – Means, if Saatopa (Bearable Ruja in Pakvashaya) is
reduced by grade 2, then it is considered as Moderate response to the treatment.
Good response – Means, if Atyugra ruja, and complete distinction in abdomen is
reduced to grade 0, and If the Severity is reduced from any other grade to 0, then
it is considered as Good response to the treatment.
Not respond – Means, if Severity is neither reduced nor increased, then it is
considered as No response to the treatment.
Score chart for Ruja/ Sasholaukta Mootratyaga
No symptoms Grade 0 – Normal.
Bearable Grade 1 – Mild.
Unbearable Grade 2 – Severe.
Overall Response Assessment Criteria for Ruja / Sashoolayukta mutratyaga.
Poor response – Means, if Ruja / Sasholaukta Mootratyaga is reduced up to
bearable stage i.e. grade 1, then it is as poor response to the treatment.
Good response – Means if Ruja/ Sasholaukta Mootratyaga is reduced to Normal
stage i.e. grade 0, and If the Severity is reduced from any other grade to grade 0,
then it is considered as Good response.
Not respond – Means, if Severity is neither reduced nor increased, then it is
considered as No response to the treatment.
Effect over (AUA) I-PSS Index for Vatashtila (BPH)
The international prostate symptom score (I-PSS) which is identical to the AUA
symptom index, is recommended as the symptom scoring instrument, and it was to
provide a universally accepted instrument to quantify the impact of BPH therapies
(Cockettet al, 19992). The I-PSS was developed by the Measurement Committee of the
AUA. This is an integral part of virtually every epidemiologic study as treatment studies
in the field.
Methodology 98
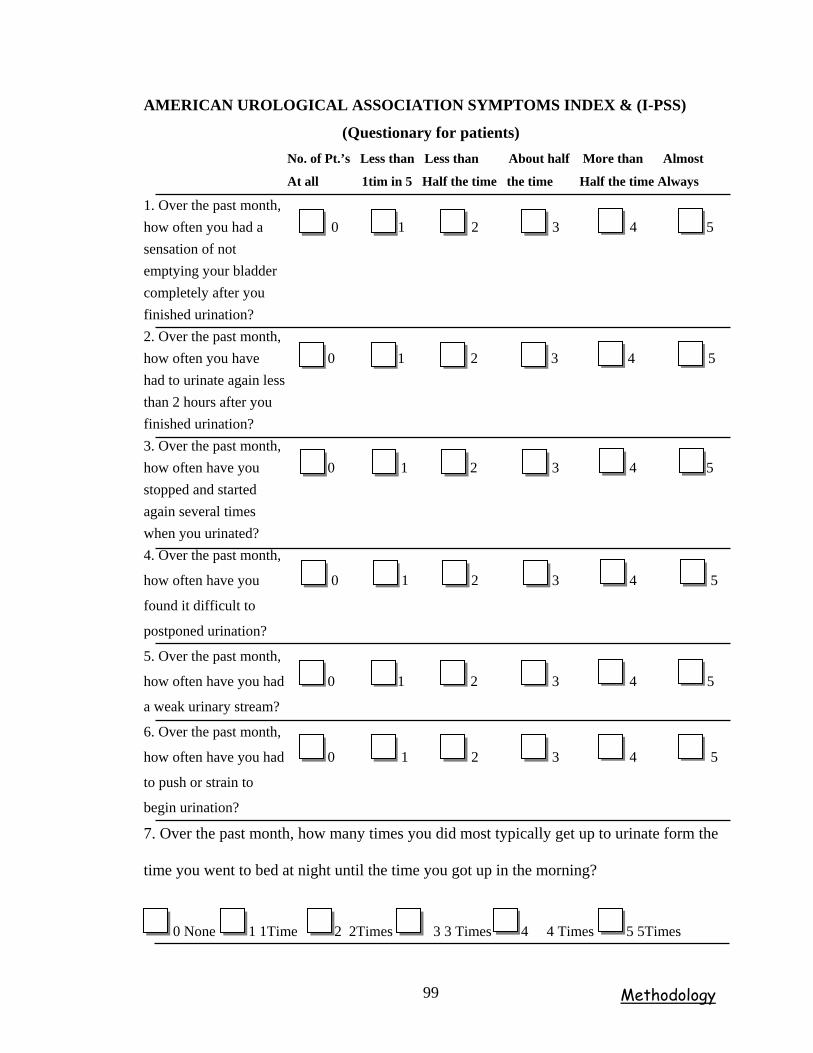
AMERICAN UROLOGICAL ASSOCIATION SYMPTOMS INDEX & (I-PSS)
(Questionary for patients) No. of Pt.’s Less than Less than About half More than Almost
At all 1tim in 5 Half the time the time Half the time Always
1. Over the past month, how often you had a 0 1 2 3 4 5 sensation of not emptying your bladder completely after you finished urination? 2. Over the past month, how often you have 0 1 2 3 4 5 had to urinate again less than 2 hours after you finished urination? 3. Over the past month, how often have you 0 1 2 3 4 5 stopped and started again several times when you urinated? 4. Over the past month,
how often have you 0 1 2 3 4 5
found it difficult to
postponed urination?
5. Over the past month,
how often have you had 0 1 2 3 4 5
a weak urinary stream?
6. Over the past month,
how often have you had 0 1 2 3 4 5
to push or strain to
begin urination?
7. Over the past month, how many times you did most typically get up to urinate form the
time you went to bed at night until the time you got up in the morning?
0 None 1 1Time 2 2Times 3 3 Times 4 4 Times 5 5Times
Methodology 99
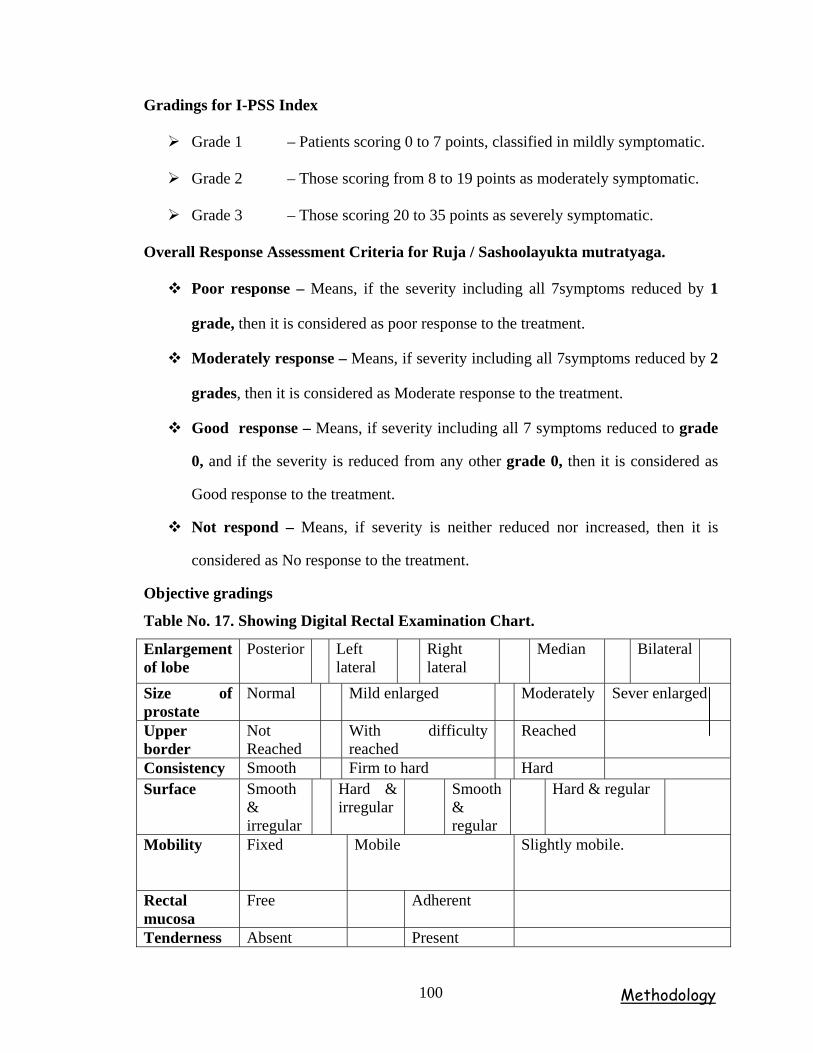
Gradings for I-PSS Index
Grade 1 – Patients scoring 0 to 7 points, classified in mildly symptomatic.
Grade 2 – Those scoring from 8 to 19 points as moderately symptomatic.
Grade 3 – Those scoring 20 to 35 points as severely symptomatic.
Overall Response Assessment Criteria for Ruja / Sashoolayukta mutratyaga.
Poor response – Means, if the severity including all 7symptoms reduced by 1
grade, then it is considered as poor response to the treatment.
Moderately response – Means, if severity including all 7symptoms reduced by 2
grades, then it is considered as Moderate response to the treatment.
Good response – Means, if severity including all 7 symptoms reduced to grade
0, and if the severity is reduced from any other grade 0, then it is considered as
Good response to the treatment.
Not respond – Means, if severity is neither reduced nor increased, then it is
considered as No response to the treatment.
Objective gradings
Table No. 17. Showing Digital Rectal Examination Chart.
Enlargement of lobe
Posterior Left lateral
Right lateral
Median Bilateral
Size of prostate
Normal Mild enlarged Moderately Sever enlarged
Upper border
Not Reached
With difficulty reached
Reached
Consistency Smooth Firm to hard Hard Surface Smooth
& irregular
Hard & irregular
Smooth & regular
Hard & regular
Mobility Fixed Mobile Slightly mobile.
Rectal mucosa
Free Adherent
Tenderness Absent Present
Methodology 100
The DRE findings assessed by a above chart made score chart, and most of the
findings assessed by putting present and absent according before and after treatment.
Score chart for size of prostate.
Grade 0 – Normal.
Grade 1 – Mild enlargement
Grade 2 – Moderate enlargement
Grade 3 – Sever enlargement
Overall Response Assessment Criteria for size of Prostate.
Poor response – Means, if the size of prostate is reduced by grade 1, then it is
considered poor response to the treatment.
Moderately response – Means, if the size of prostate is reduced by grade 2, then
it is considered poor response to the treatment.
Good response – Means, if the size of prostate is reduced to grade 0, and if the
Severity is reduced from any other grade to grade 0, then it is considered as Good
response to the treatment.
No response – Means, if there is neither increase nor decrease in the size of
prostate, then it is called as No response to the treatment.
Score chart for upper border of the prostate.
Grade 0 – Not reached
Grade 1 – With difficulty reached.
Grade 2– Reached.
Overall Response Assessment Criteria for upper border of Prostate.
Methodology 101
Overall Response Assessment Criteria for Upper border of Prostate.
Poor response – Means if by feeling the Upper border of prostate is turns by
grade 1, and, then it is considered as poor response to the treatment.
Good response – Means if by feeling the Upper border of prostate is turns by
grade 0, If the Severity is reduced from any other grade to 0, it is considered it is
as Good response.
No response – Means, if there is neither increase nor decrease in the upper border
of prostate, then it is called as No response to the treatment.
Score chart for of mobility prostate.
Grade 1 – Fixed.
Grade 2 – Slightly mobile.
Grade 3 – Mobile
Overall Response Assessment Criteria for mobility of Prostate
Moderately response – Means if by feeling the mobility of prostate is terns to by
grade 1, and , then it is considered as Moderate response to the treatment.
Good response – Means if by feeling the mobility of prostate is terns to Grade 0,
If the Severity is reduced from any other grade to 0, it is considered it is as Good
response.
Not response --. Means, if there is neither increase nor decrease in the mobility
of prostate, then it is called as No response to the treatment.
Methodology 102
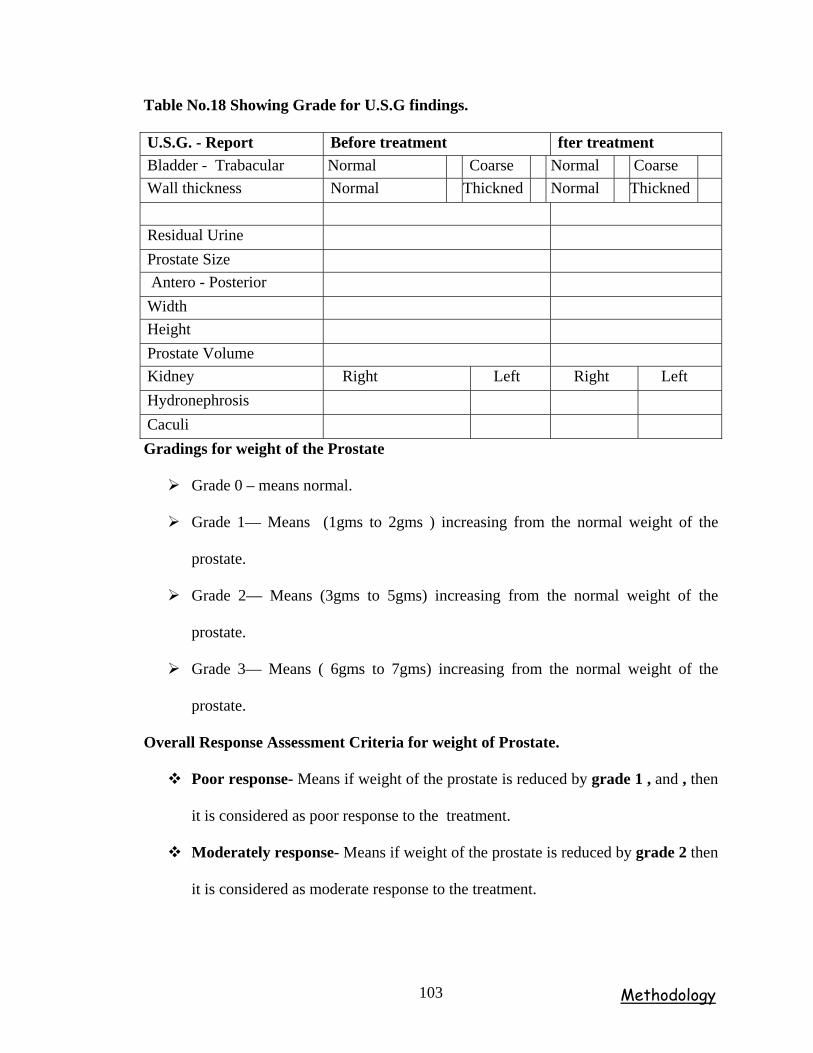
Table No.18 Showing Grade for U.S.G findings.
U.S.G. - Report Before treatment fter treatment Bladder - Trabacular Normal Coarse Normal Coarse Wall thickness Normal Thickned Normal Thickned Residual Urine Prostate Size Antero - Posterior Width Height Prostate Volume Kidney Right Left Right Left Hydronephrosis Caculi Gradings for weight of the Prostate
Grade 0 – means normal.
Grade 1— Means (1gms to 2gms ) increasing from the normal weight of the
prostate.
Grade 2— Means (3gms to 5gms) increasing from the normal weight of the
prostate.
Grade 3— Means ( 6gms to 7gms) increasing from the normal weight of the
prostate.
Overall Response Assessment Criteria for weight of Prostate.
Poor response- Means if weight of the prostate is reduced by grade 1 , and , then
it is considered as poor response to the treatment.
Moderately response- Means if weight of the prostate is reduced by grade 2 then
it is considered as moderate response to the treatment.
Methodology 103
Good response- Means if weight of the prostate is reduced to grade 0. and If the
weight of the prostate is reduced from any other grade to 0, it is considered it is as
Good response.
Not respond-. Means, if there is neither increase nor decrease in the weight of
prostate, then it is called as no response to the treatment.
Score chart for residual urine flow
Grade 0 – Below 10cc normal
Grade 1 – 10 to 50cc.
Grade 2 – 51 to 100cc.
Grade 3 – 101 to 200cc.
Grade 4 – 201 and above.
Overall Response Assessment Criteria for Residual urine flow.
Poor response- Means if residual urine volume is reduced by grade 1, and then
it is considered as poor response to the treatment.
Moderately response- Means if residual urine volume is reduced by grade 2,
(51cc to100cc) as and then is considered as moderate response to the treatment.
Good response- Means if residual urine volume is reduced to grade 0. and If the
is residual urine volume is reduced from any other grade to 0, it is considered as
Good response.
Not respond-. Means, if there is neither increase nor decrease in the residual
urine volume then it is called as No response to the treatment.
Methodology 104
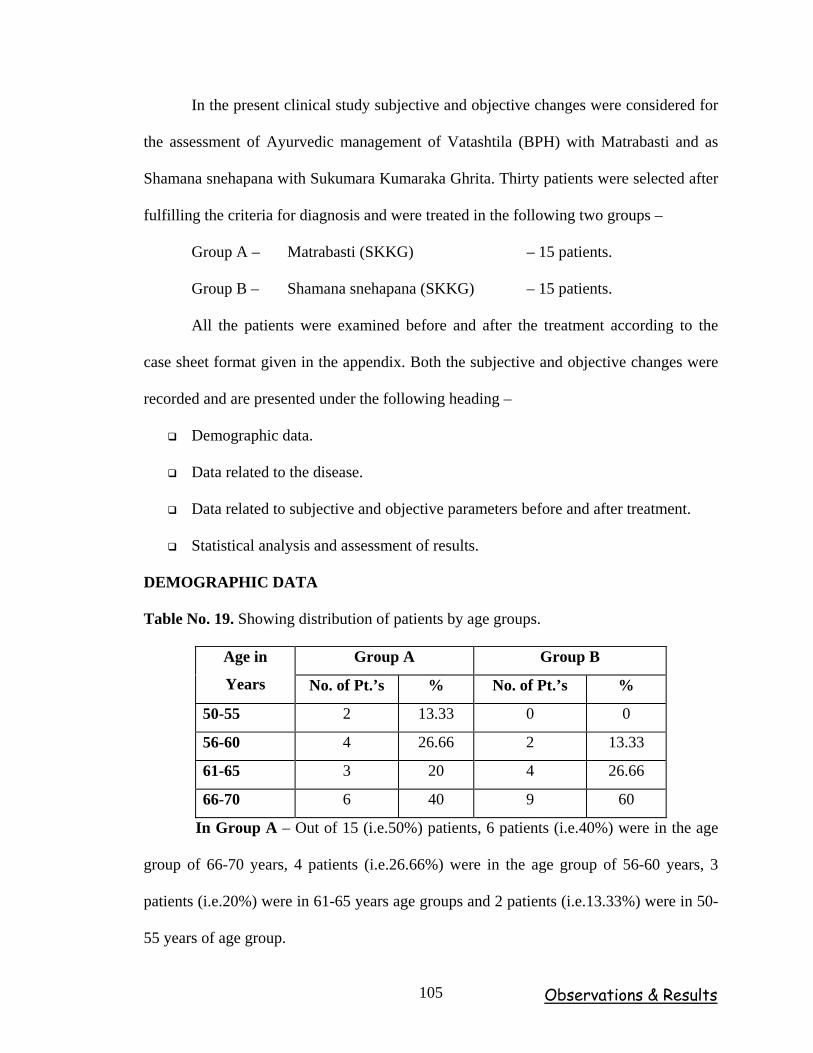
Observations & Results 105
In the present clinical study subjective and objective changes were considered for
the assessment of Ayurvedic management of Vatashtila (BPH) with Matrabasti and as
Shamana snehapana with Sukumara Kumaraka Ghrita. Thirty patients were selected after
fulfilling the criteria for diagnosis and were treated in the following two groups –
Group A – Matrabasti (SKKG) – 15 patients.
Group B – Shamana snehapana (SKKG) – 15 patients.
All the patients were examined before and after the treatment according to the
case sheet format given in the appendix. Both the subjective and objective changes were
recorded and are presented under the following heading –
Demographic data.
Data related to the disease.
Data related to subjective and objective parameters before and after treatment.
Statistical analysis and assessment of results.
DEMOGRAPHIC DATA
Table No. 19. Showing distribution of patients by age groups.
Group A Group B Age in
Years No. of Pt.’s % No. of Pt.’s %
50-55 2 13.33 0 0
56-60 4 26.66 2 13.33
61-65 3 20 4 26.66
66-70 6 40 9 60
In Group A – Out of 15 (i.e.50%) patients, 6 patients (i.e.40%) were in the age
group of 66-70 years, 4 patients (i.e.26.66%) were in the age group of 56-60 years, 3
patients (i.e.20%) were in 61-65 years age groups and 2 patients (i.e.13.33%) were in 50-
55 years of age group.
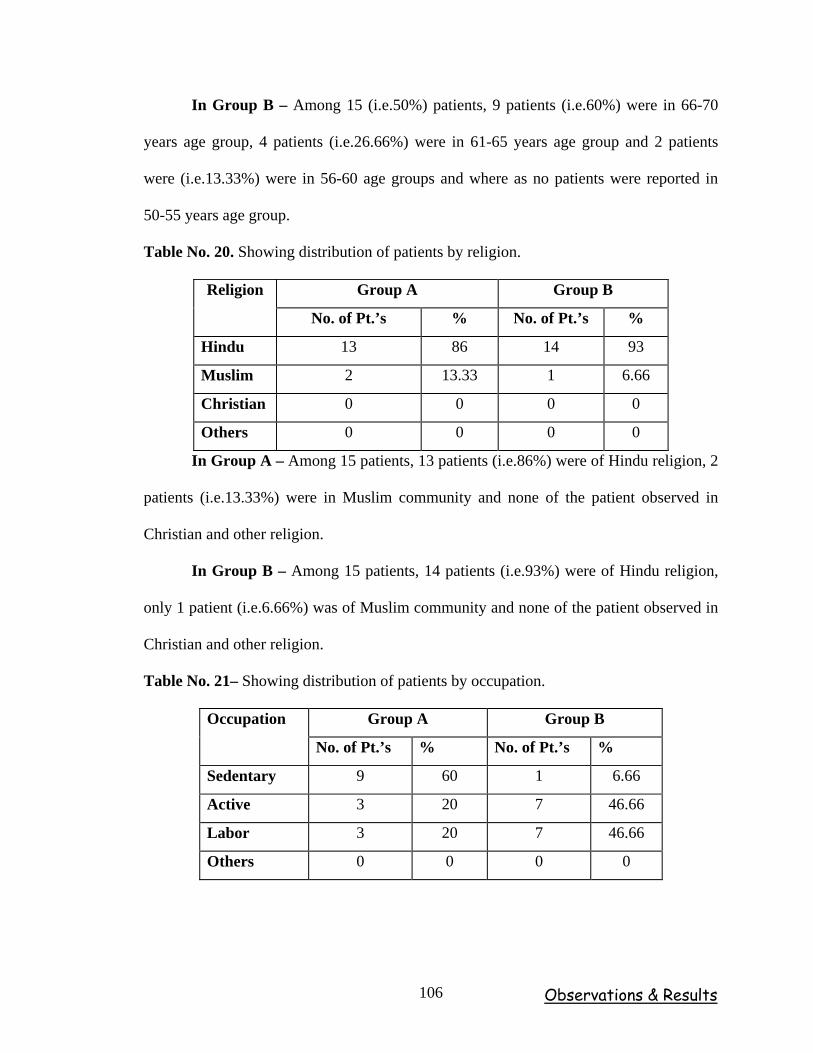
Observations & Results 106
In Group B – Among 15 (i.e.50%) patients, 9 patients (i.e.60%) were in 66-70
years age group, 4 patients (i.e.26.66%) were in 61-65 years age group and 2 patients
were (i.e.13.33%) were in 56-60 age groups and where as no patients were reported in
50-55 years age group.
Table No. 20. Showing distribution of patients by religion.
Group A Group B Religion
No. of Pt.’s % No. of Pt.’s %
Hindu 13 86 14 93
Muslim 2 13.33 1 6.66
Christian 0 0 0 0
Others 0 0 0 0
In Group A – Among 15 patients, 13 patients (i.e.86%) were of Hindu religion, 2
patients (i.e.13.33%) were in Muslim community and none of the patient observed in
Christian and other religion.
In Group B – Among 15 patients, 14 patients (i.e.93%) were of Hindu religion,
only 1 patient (i.e.6.66%) was of Muslim community and none of the patient observed in
Christian and other religion.
Table No. 21– Showing distribution of patients by occupation.
Group A Group B Occupation
No. of Pt.’s % No. of Pt.’s %
Sedentary 9 60 1 6.66
Active 3 20 7 46.66
Labor 3 20 7 46.66
Others 0 0 0 0
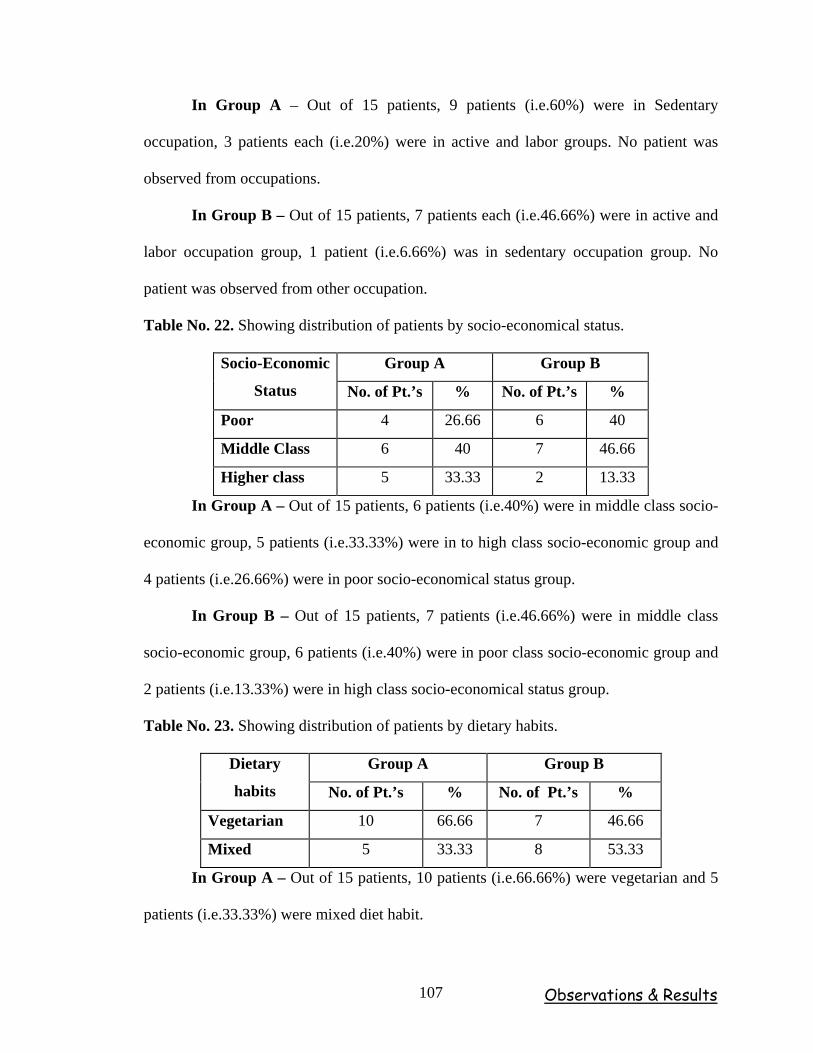
Observations & Results 107
In Group A – Out of 15 patients, 9 patients (i.e.60%) were in Sedentary
occupation, 3 patients each (i.e.20%) were in active and labor groups. No patient was
observed from occupations.
In Group B – Out of 15 patients, 7 patients each (i.e.46.66%) were in active and
labor occupation group, 1 patient (i.e.6.66%) was in sedentary occupation group. No
patient was observed from other occupation.
Table No. 22. Showing distribution of patients by socio-economical status.
Group A Group B Socio-Economic
Status No. of Pt.’s % No. of Pt.’s %
Poor 4 26.66 6 40
Middle Class 6 40 7 46.66
Higher class 5 33.33 2 13.33
In Group A – Out of 15 patients, 6 patients (i.e.40%) were in middle class socio-
economic group, 5 patients (i.e.33.33%) were in to high class socio-economic group and
4 patients (i.e.26.66%) were in poor socio-economical status group.
In Group B – Out of 15 patients, 7 patients (i.e.46.66%) were in middle class
socio-economic group, 6 patients (i.e.40%) were in poor class socio-economic group and
2 patients (i.e.13.33%) were in high class socio-economical status group.
Table No. 23. Showing distribution of patients by dietary habits.
Group A Group B Dietary
habits No. of Pt.’s % No. of Pt.’s %
Vegetarian 10 66.66 7 46.66
Mixed 5 33.33 8 53.33
In Group A – Out of 15 patients, 10 patients (i.e.66.66%) were vegetarian and 5
patients (i.e.33.33%) were mixed diet habit.
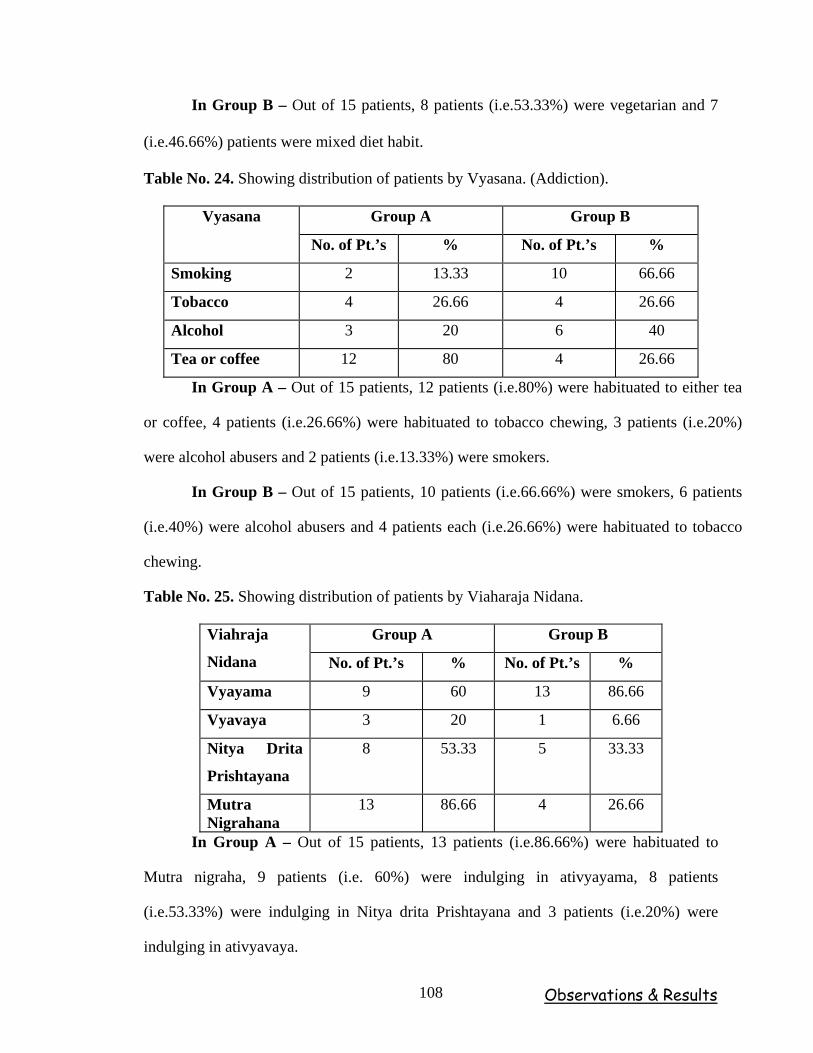
Observations & Results 108
In Group B – Out of 15 patients, 8 patients (i.e.53.33%) were vegetarian and 7
(i.e.46.66%) patients were mixed diet habit.
Table No. 24. Showing distribution of patients by Vyasana. (Addiction).
Group A Group B Vyasana
No. of Pt.’s % No. of Pt.’s %
Smoking 2 13.33 10 66.66
Tobacco 4 26.66 4 26.66
Alcohol 3 20 6 40
Tea or coffee 12 80 4 26.66
In Group A – Out of 15 patients, 12 patients (i.e.80%) were habituated to either tea
or coffee, 4 patients (i.e.26.66%) were habituated to tobacco chewing, 3 patients (i.e.20%)
were alcohol abusers and 2 patients (i.e.13.33%) were smokers.
In Group B – Out of 15 patients, 10 patients (i.e.66.66%) were smokers, 6 patients
(i.e.40%) were alcohol abusers and 4 patients each (i.e.26.66%) were habituated to tobacco
chewing.
Table No. 25. Showing distribution of patients by Viaharaja Nidana.
Group A Group B Viahraja
Nidana No. of Pt.’s % No. of Pt.’s %
Vyayama 9 60 13 86.66
Vyavaya 3 20 1 6.66
Nitya Drita
Prishtayana
8 53.33 5 33.33
Mutra Nigrahana
13 86.66 4 26.66
In Group A – Out of 15 patients, 13 patients (i.e.86.66%) were habituated to
Mutra nigraha, 9 patients (i.e. 60%) were indulging in ativyayama, 8 patients
(i.e.53.33%) were indulging in Nitya drita Prishtayana and 3 patients (i.e.20%) were
indulging in ativyavaya.
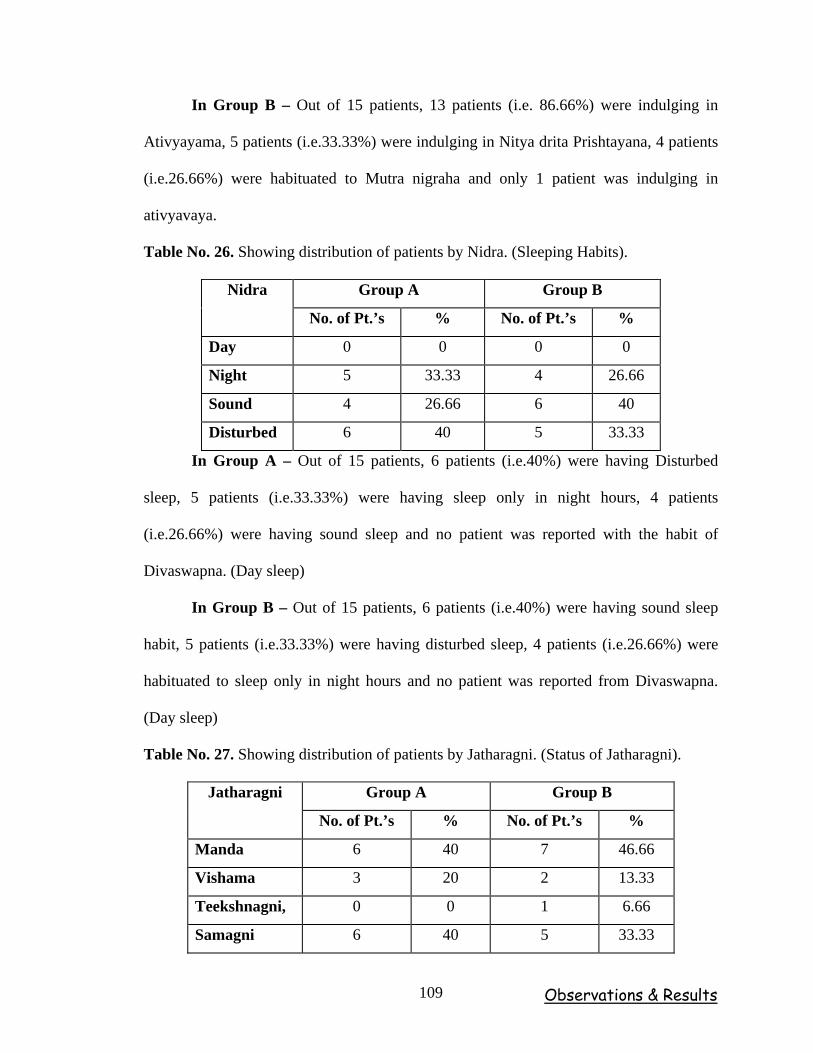
Observations & Results 109
In Group B – Out of 15 patients, 13 patients (i.e. 86.66%) were indulging in
Ativyayama, 5 patients (i.e.33.33%) were indulging in Nitya drita Prishtayana, 4 patients
(i.e.26.66%) were habituated to Mutra nigraha and only 1 patient was indulging in
ativyavaya.
Table No. 26. Showing distribution of patients by Nidra. (Sleeping Habits).
Group A Group B Nidra
No. of Pt.’s % No. of Pt.’s %
Day 0 0 0 0
Night 5 33.33 4 26.66
Sound 4 26.66 6 40
Disturbed 6 40 5 33.33
In Group A – Out of 15 patients, 6 patients (i.e.40%) were having Disturbed
sleep, 5 patients (i.e.33.33%) were having sleep only in night hours, 4 patients
(i.e.26.66%) were having sound sleep and no patient was reported with the habit of
Divaswapna. (Day sleep)
In Group B – Out of 15 patients, 6 patients (i.e.40%) were having sound sleep
habit, 5 patients (i.e.33.33%) were having disturbed sleep, 4 patients (i.e.26.66%) were
habituated to sleep only in night hours and no patient was reported from Divaswapna.
(Day sleep)
Table No. 27. Showing distribution of patients by Jatharagni. (Status of Jatharagni).
Group A Group B Jatharagni
No. of Pt.’s % No. of Pt.’s %
Manda 6 40 7 46.66
Vishama 3 20 2 13.33
Teekshnagni, 0 0 1 6.66
Samagni 6 40 5 33.33
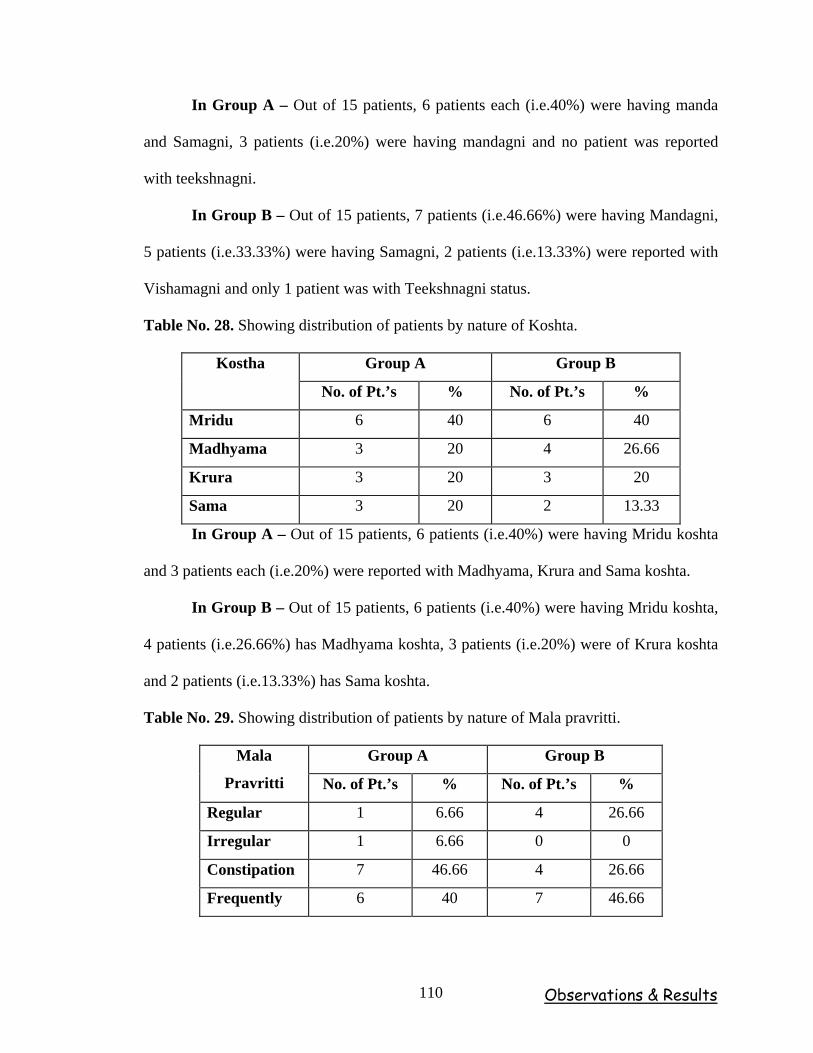
Observations & Results 110
In Group A – Out of 15 patients, 6 patients each (i.e.40%) were having manda
and Samagni, 3 patients (i.e.20%) were having mandagni and no patient was reported
with teekshnagni.
In Group B – Out of 15 patients, 7 patients (i.e.46.66%) were having Mandagni,
5 patients (i.e.33.33%) were having Samagni, 2 patients (i.e.13.33%) were reported with
Vishamagni and only 1 patient was with Teekshnagni status.
Table No. 28. Showing distribution of patients by nature of Koshta.
Group A Group B Kostha
No. of Pt.’s % No. of Pt.’s %
Mridu 6 40 6 40
Madhyama 3 20 4 26.66
Krura 3 20 3 20
Sama 3 20 2 13.33
In Group A – Out of 15 patients, 6 patients (i.e.40%) were having Mridu koshta
and 3 patients each (i.e.20%) were reported with Madhyama, Krura and Sama koshta.
In Group B – Out of 15 patients, 6 patients (i.e.40%) were having Mridu koshta,
4 patients (i.e.26.66%) has Madhyama koshta, 3 patients (i.e.20%) were of Krura koshta
and 2 patients (i.e.13.33%) has Sama koshta.
Table No. 29. Showing distribution of patients by nature of Mala pravritti.
Group A Group B Mala
Pravritti No. of Pt.’s % No. of Pt.’s %
Regular 1 6.66 4 26.66
Irregular 1 6.66 0 0
Constipation 7 46.66 4 26.66
Frequently 6 40 7 46.66
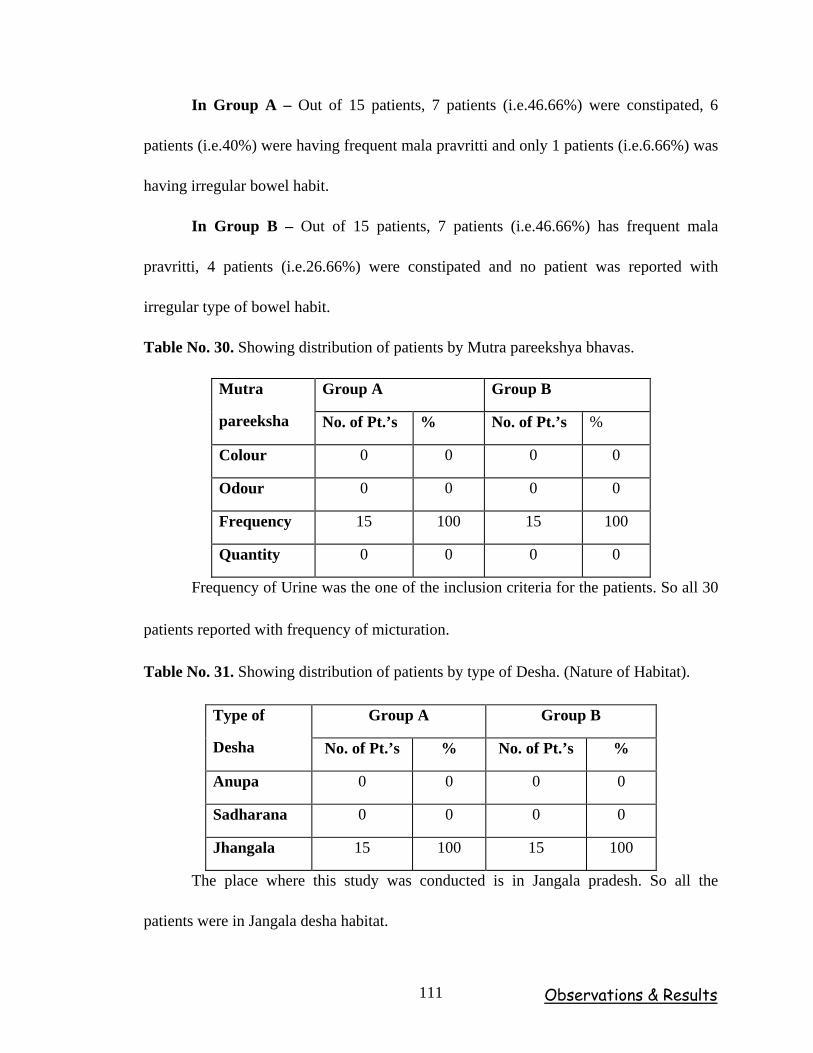
Observations & Results 111
In Group A – Out of 15 patients, 7 patients (i.e.46.66%) were constipated, 6
patients (i.e.40%) were having frequent mala pravritti and only 1 patients (i.e.6.66%) was
having irregular bowel habit.
In Group B – Out of 15 patients, 7 patients (i.e.46.66%) has frequent mala
pravritti, 4 patients (i.e.26.66%) were constipated and no patient was reported with
irregular type of bowel habit.
Table No. 30. Showing distribution of patients by Mutra pareekshya bhavas.
Group A Group B Mutra
pareeksha No. of Pt.’s % No. of Pt.’s %
Colour 0 0 0 0
Odour 0 0 0 0
Frequency 15 100 15 100
Quantity 0 0 0 0
Frequency of Urine was the one of the inclusion criteria for the patients. So all 30
patients reported with frequency of micturation.
Table No. 31. Showing distribution of patients by type of Desha. (Nature of Habitat).
Group A Group B Type of
Desha No. of Pt.’s % No. of Pt.’s %
Anupa 0 0 0 0
Sadharana 0 0 0 0
Jhangala 15 100 15 100
The place where this study was conducted is in Jangala pradesh. So all the
patients were in Jangala desha habitat.
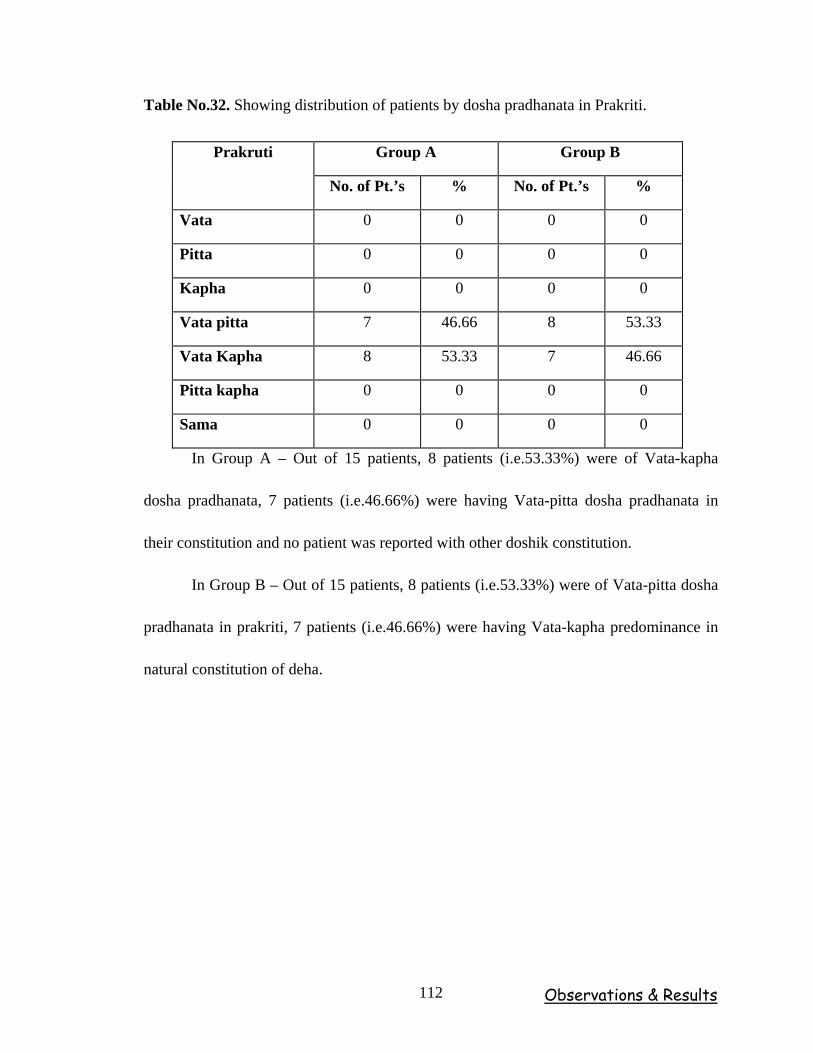
Observations & Results 112
Table No.32. Showing distribution of patients by dosha pradhanata in Prakriti.
Group A Group B Prakruti
No. of Pt.’s % No. of Pt.’s %
Vata 0 0 0 0
Pitta 0 0 0 0
Kapha 0 0 0 0
Vata pitta 7 46.66 8 53.33
Vata Kapha 8 53.33 7 46.66
Pitta kapha 0 0 0 0
Sama 0 0 0 0
In Group A – Out of 15 patients, 8 patients (i.e.53.33%) were of Vata-kapha
dosha pradhanata, 7 patients (i.e.46.66%) were having Vata-pitta dosha pradhanata in
their constitution and no patient was reported with other doshik constitution.
In Group B – Out of 15 patients, 8 patients (i.e.53.33%) were of Vata-pitta dosha
pradhanata in prakriti, 7 patients (i.e.46.66%) were having Vata-kapha predominance in
natural constitution of deha.
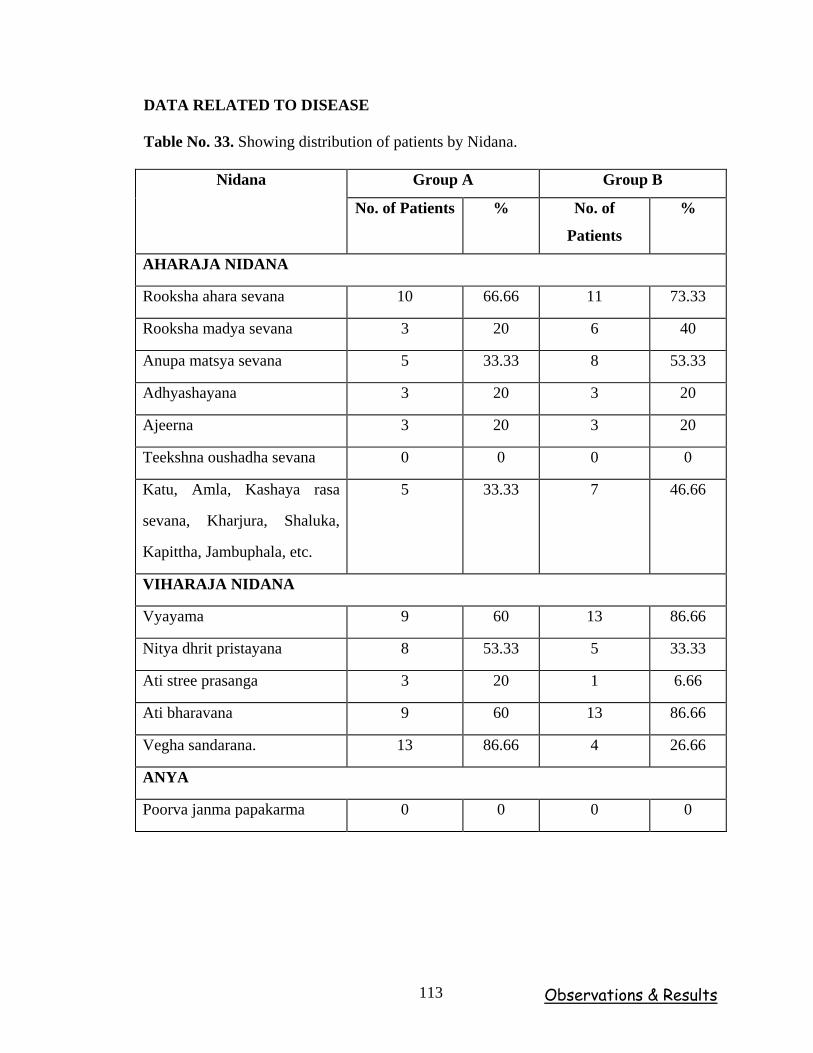
Observations & Results 113
DATA RELATED TO DISEASE
Table No. 33. Showing distribution of patients by Nidana.
Group A Group B Nidana
No. of Patients % No. of
Patients
%
AHARAJA NIDANA
Rooksha ahara sevana 10 66.66 11 73.33
Rooksha madya sevana 3 20 6 40
Anupa matsya sevana 5 33.33 8 53.33
Adhyashayana 3 20 3 20
Ajeerna 3 20 3 20
Teekshna oushadha sevana 0 0 0 0
Katu, Amla, Kashaya rasa
sevana, Kharjura, Shaluka,
Kapittha, Jambuphala, etc.
5 33.33 7 46.66
VIHARAJA NIDANA
Vyayama 9 60 13 86.66
Nitya dhrit pristayana 8 53.33 5 33.33
Ati stree prasanga 3 20 1 6.66
Ati bharavana 9 60 13 86.66
Vegha sandarana. 13 86.66 4 26.66
ANYA
Poorva janma papakarma 0 0 0 0
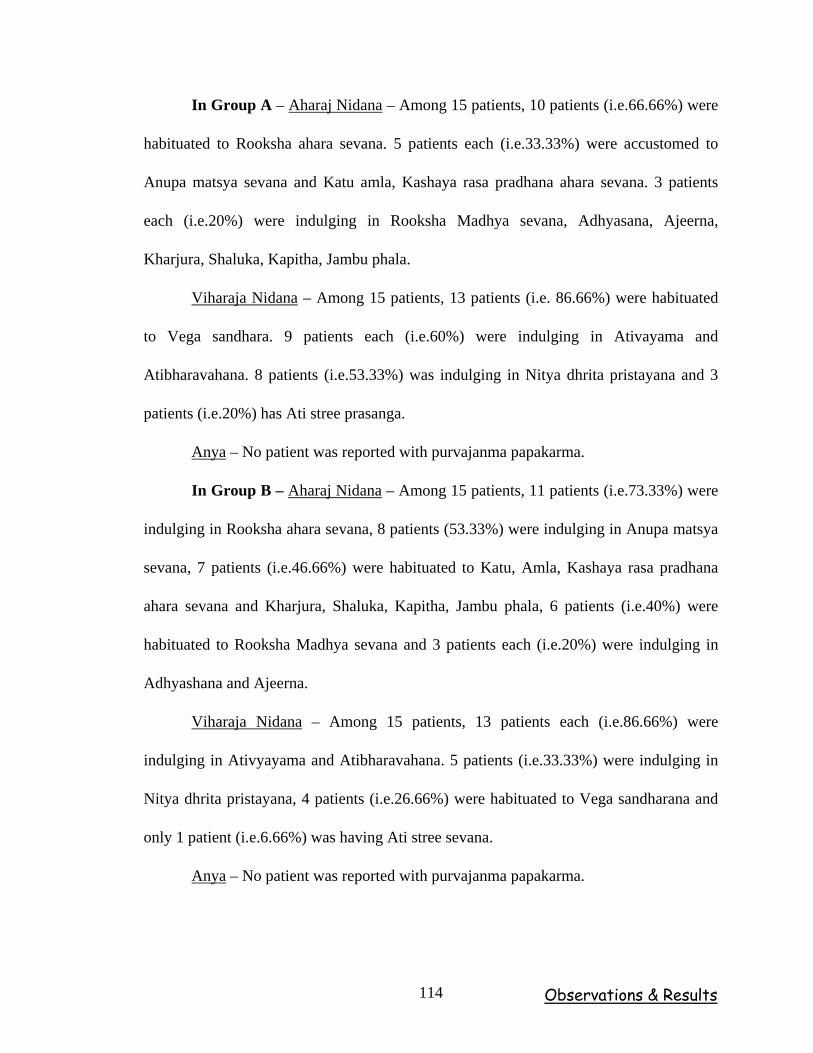
Observations & Results 114
In Group A – Aharaj Nidana – Among 15 patients, 10 patients (i.e.66.66%) were
habituated to Rooksha ahara sevana. 5 patients each (i.e.33.33%) were accustomed to
Anupa matsya sevana and Katu amla, Kashaya rasa pradhana ahara sevana. 3 patients
each (i.e.20%) were indulging in Rooksha Madhya sevana, Adhyasana, Ajeerna,
Kharjura, Shaluka, Kapitha, Jambu phala.
Viharaja Nidana – Among 15 patients, 13 patients (i.e. 86.66%) were habituated
to Vega sandhara. 9 patients each (i.e.60%) were indulging in Ativayama and
Atibharavahana. 8 patients (i.e.53.33%) was indulging in Nitya dhrita pristayana and 3
patients (i.e.20%) has Ati stree prasanga.
Anya – No patient was reported with purvajanma papakarma.
In Group B – Aharaj Nidana – Among 15 patients, 11 patients (i.e.73.33%) were
indulging in Rooksha ahara sevana, 8 patients (53.33%) were indulging in Anupa matsya
sevana, 7 patients (i.e.46.66%) were habituated to Katu, Amla, Kashaya rasa pradhana
ahara sevana and Kharjura, Shaluka, Kapitha, Jambu phala, 6 patients (i.e.40%) were
habituated to Rooksha Madhya sevana and 3 patients each (i.e.20%) were indulging in
Adhyashana and Ajeerna.
Viharaja Nidana – Among 15 patients, 13 patients each (i.e.86.66%) were
indulging in Ativyayama and Atibharavahana. 5 patients (i.e.33.33%) were indulging in
Nitya dhrita pristayana, 4 patients (i.e.26.66%) were habituated to Vega sandharana and
only 1 patient (i.e.6.66%) was having Ati stree sevana.
Anya – No patient was reported with purvajanma papakarma.
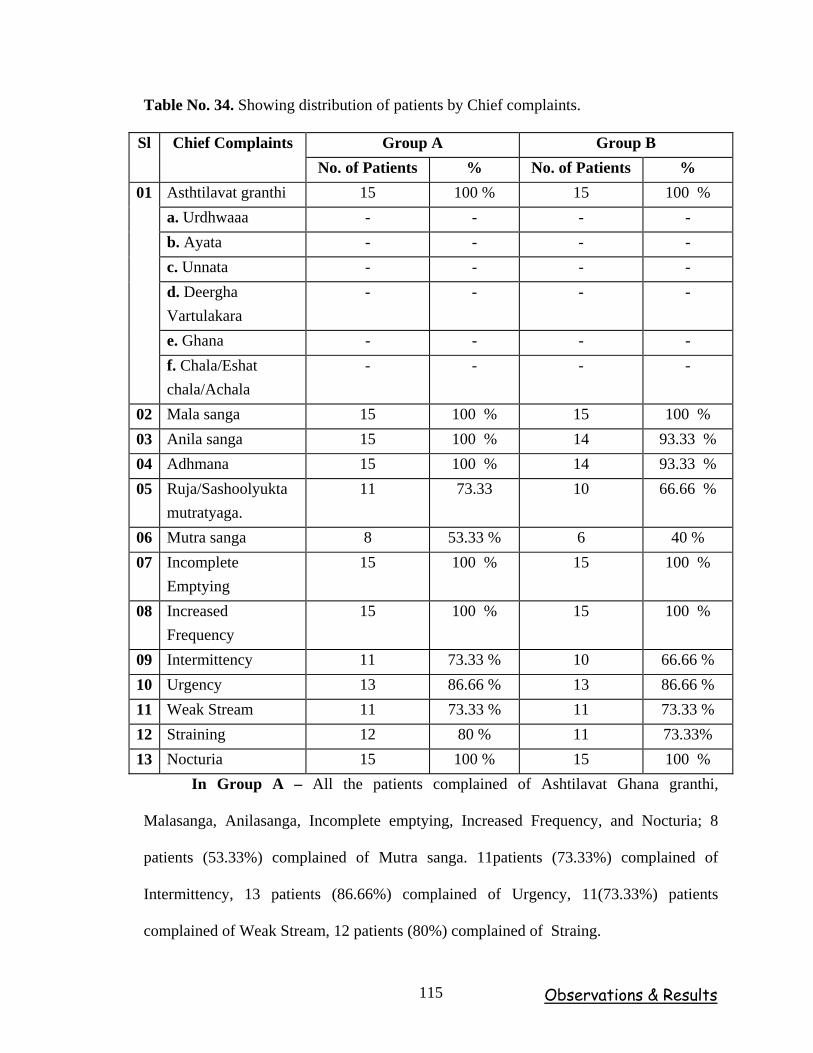
Observations & Results 115
Table No. 34. Showing distribution of patients by Chief complaints.
Group A Group B Sl Chief Complaints No. of Patients % No. of Patients %
Asthtilavat granthi 15 100 % 15 100 % a. Urdhwaaa - - - - b. Ayata - - - - c. Unnata - - - - d. Deergha Vartulakara
- - - -
e. Ghana - - - -
01
f. Chala/Eshat chala/Achala
- - - -
02 Mala sanga 15 100 % 15 100 % 03 Anila sanga 15 100 % 14 93.33 % 04 Adhmana 15 100 % 14 93.33 % 05 Ruja/Sashoolyukta
mutratyaga. 11 73.33 10 66.66 %
06 Mutra sanga 8 53.33 % 6 40 % 07 Incomplete
Emptying 15 100 % 15 100 %
08 Increased Frequency
15 100 % 15 100 %
09 Intermittency 11 73.33 % 10 66.66 % 10 Urgency 13 86.66 % 13 86.66 % 11 Weak Stream 11 73.33 % 11 73.33 % 12 Straining 12 80 % 11 73.33% 13 Nocturia 15 100 % 15 100 %
In Group A – All the patients complained of Ashtilavat Ghana granthi,
Malasanga, Anilasanga, Incomplete emptying, Increased Frequency, and Nocturia; 8
patients (53.33%) complained of Mutra sanga. 11patients (73.33%) complained of
Intermittency, 13 patients (86.66%) complained of Urgency, 11(73.33%) patients
complained of Weak Stream, 12 patients (80%) complained of Straing.
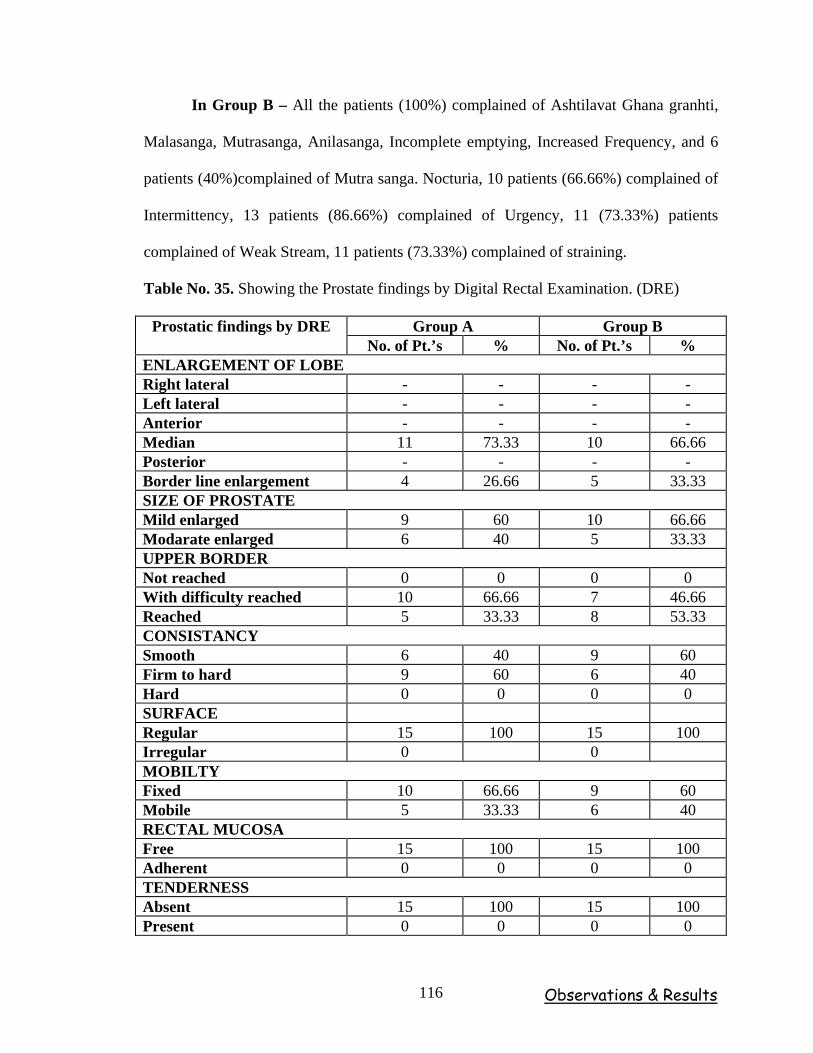
Observations & Results 116
In Group B – All the patients (100%) complained of Ashtilavat Ghana granhti,
Malasanga, Mutrasanga, Anilasanga, Incomplete emptying, Increased Frequency, and 6
patients (40%)complained of Mutra sanga. Nocturia, 10 patients (66.66%) complained of
Intermittency, 13 patients (86.66%) complained of Urgency, 11 (73.33%) patients
complained of Weak Stream, 11 patients (73.33%) complained of straining.
Table No. 35. Showing the Prostate findings by Digital Rectal Examination. (DRE)
Group A Group B Prostatic findings by DRE No. of Pt.’s % No. of Pt.’s %
ENLARGEMENT OF LOBE Right lateral - - - - Left lateral - - - - Anterior - - - - Median 11 73.33 10 66.66 Posterior - - - - Border line enlargement 4 26.66 5 33.33 SIZE OF PROSTATE Mild enlarged 9 60 10 66.66 Modarate enlarged 6 40 5 33.33 UPPER BORDER Not reached 0 0 0 0 With difficulty reached 10 66.66 7 46.66 Reached 5 33.33 8 53.33 CONSISTANCY Smooth 6 40 9 60 Firm to hard 9 60 6 40 Hard 0 0 0 0 SURFACE Regular 15 100 15 100 Irregular 0 0 MOBILTY Fixed 10 66.66 9 60 Mobile 5 33.33 6 40 RECTAL MUCOSA Free 15 100 15 100 Adherent 0 0 0 0 TENDERNESS Absent 15 100 15 100 Present 0 0 0 0
Observations & Results 117
In Group A – Enlargement of lobe – Among 15 patients, 11 patients
(i.e.73.33%) were noticed with median lobe enlargement, 4 patients (i.e.26.66%) were
noticed with border line enlargement.
Size of prostate – Among 15 patients, 9 patients (i.e.60%) were noticed with
mild enlargement and 6 patients (i.e.40%) were noticed with moderate enlargement of
prostate.
Upper border – Among 15 patient, in 10 patients (i.e.66.66%) the upper border of
prostate was reached with difficulty, 5 patients (i.e.33.33%) were noticed with the easy
palpation of upper border of the prostate and no patient was reported with palpation of
upper border of prostate.
Consistency – Among 15 patients, 9 patients (i.e.60%) were noticed with smooth
consistency, 9 patients (i.e.40%) were noticed firm to hard consistency of prostate and no
patient was observed with hard consistency of prostate.
Surface – All patients were observed with regular surface of prostate.
Mobility – Among 15 patients, in 10 patients (i.e.66.66%) the prostate was fixed
and in 5 patients (i.e.33.33%) the prostate was mobile.
Rectal mucosa – All patients the prostate was found free of rectal mucosa.
Tenderness – No patient was noticed with tender prostate.
In Group B – Enlargement of lobe – Among 15 patients, 10 patients
(i.e.66.66%) were noticed with median lobe enlargement, 5 (33.33%) noticed with border
line enlargement of prostate.
Size of prostate – Among 15 patients, 10 patients (i.e.66.66%) were noticed with
mild enlargement of prostate and 5 patients (i.e.33.33%) were noticed with moderate
enlargement.
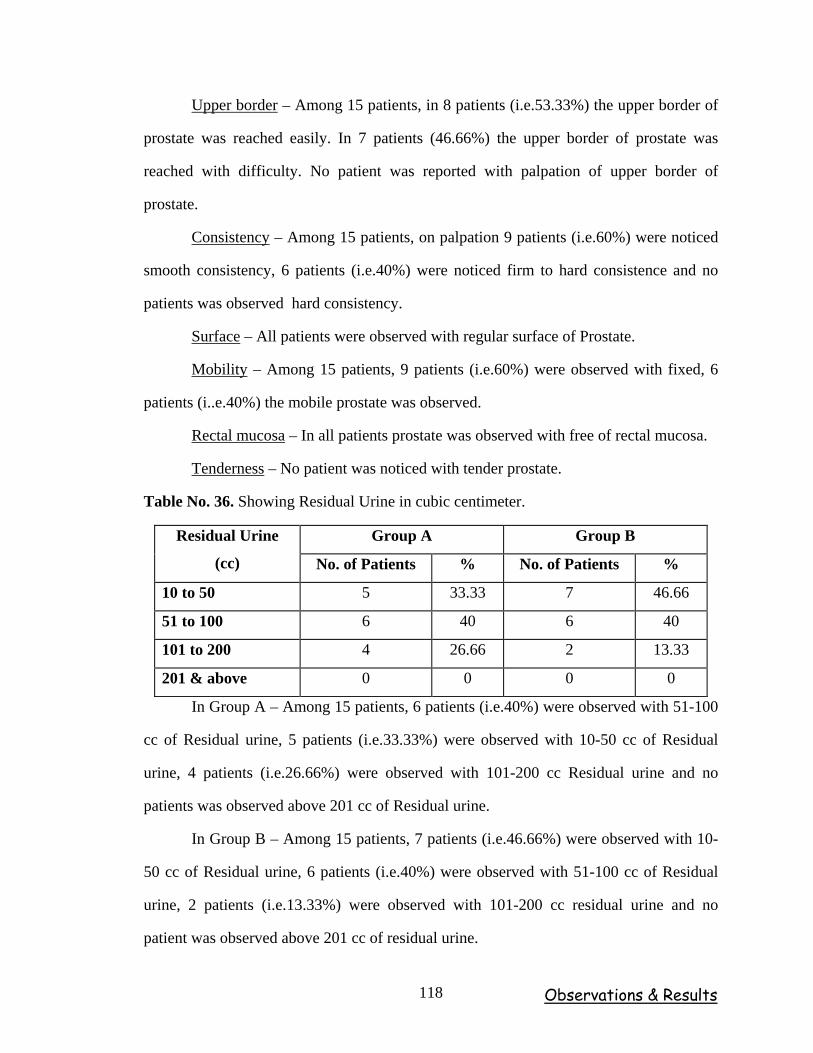
Observations & Results 118
Upper border – Among 15 patients, in 8 patients (i.e.53.33%) the upper border of
prostate was reached easily. In 7 patients (46.66%) the upper border of prostate was
reached with difficulty. No patient was reported with palpation of upper border of
prostate.
Consistency – Among 15 patients, on palpation 9 patients (i.e.60%) were noticed
smooth consistency, 6 patients (i.e.40%) were noticed firm to hard consistence and no
patients was observed hard consistency.
Surface – All patients were observed with regular surface of Prostate.
Mobility – Among 15 patients, 9 patients (i.e.60%) were observed with fixed, 6
patients (i..e.40%) the mobile prostate was observed.
Rectal mucosa – In all patients prostate was observed with free of rectal mucosa.
Tenderness – No patient was noticed with tender prostate.
Table No. 36. Showing Residual Urine in cubic centimeter.
Group A Group B Residual Urine
(cc) No. of Patients % No. of Patients %
10 to 50 5 33.33 7 46.66
51 to 100 6 40 6 40
101 to 200 4 26.66 2 13.33
201 & above 0 0 0 0
In Group A – Among 15 patients, 6 patients (i.e.40%) were observed with 51-100
cc of Residual urine, 5 patients (i.e.33.33%) were observed with 10-50 cc of Residual
urine, 4 patients (i.e.26.66%) were observed with 101-200 cc Residual urine and no
patients was observed above 201 cc of Residual urine.
In Group B – Among 15 patients, 7 patients (i.e.46.66%) were observed with 10-
50 cc of Residual urine, 6 patients (i.e.40%) were observed with 51-100 cc of Residual
urine, 2 patients (i.e.13.33%) were observed with 101-200 cc residual urine and no
patient was observed above 201 cc of residual urine.
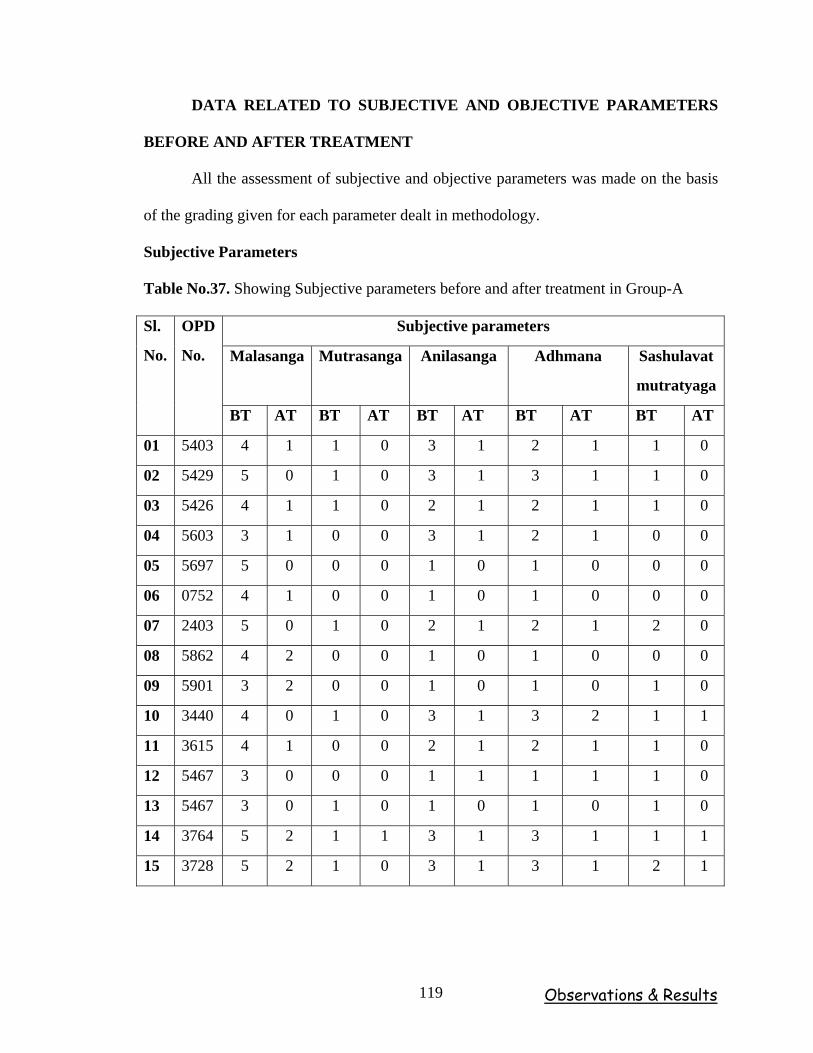
Observations & Results 119
DATA RELATED TO SUBJECTIVE AND OBJECTIVE PARAMETERS
BEFORE AND AFTER TREATMENT
All the assessment of subjective and objective parameters was made on the basis
of the grading given for each parameter dealt in methodology.
Subjective Parameters
Table No.37. Showing Subjective parameters before and after treatment in Group-A
Subjective parameters
Malasanga Mutrasanga Anilasanga Adhmana Sashulavat
mutratyaga
Sl.
No.
OPD
No.
BT AT BT AT BT AT BT AT BT AT
01 5403 4 1 1 0 3 1 2 1 1 0
02 5429 5 0 1 0 3 1 3 1 1 0
03 5426 4 1 1 0 2 1 2 1 1 0
04 5603 3 1 0 0 3 1 2 1 0 0
05 5697 5 0 0 0 1 0 1 0 0 0
06 0752 4 1 0 0 1 0 1 0 0 0
07 2403 5 0 1 0 2 1 2 1 2 0
08 5862 4 2 0 0 1 0 1 0 0 0
09 5901 3 2 0 0 1 0 1 0 1 0
10 3440 4 0 1 0 3 1 3 2 1 1
11 3615 4 1 0 0 2 1 2 1 1 0
12 5467 3 0 0 0 1 1 1 1 1 0
13 5467 3 0 1 0 1 0 1 0 1 0
14 3764 5 2 1 1 3 1 3 1 1 1
15 3728 5 2 1 0 3 1 3 1 2 1
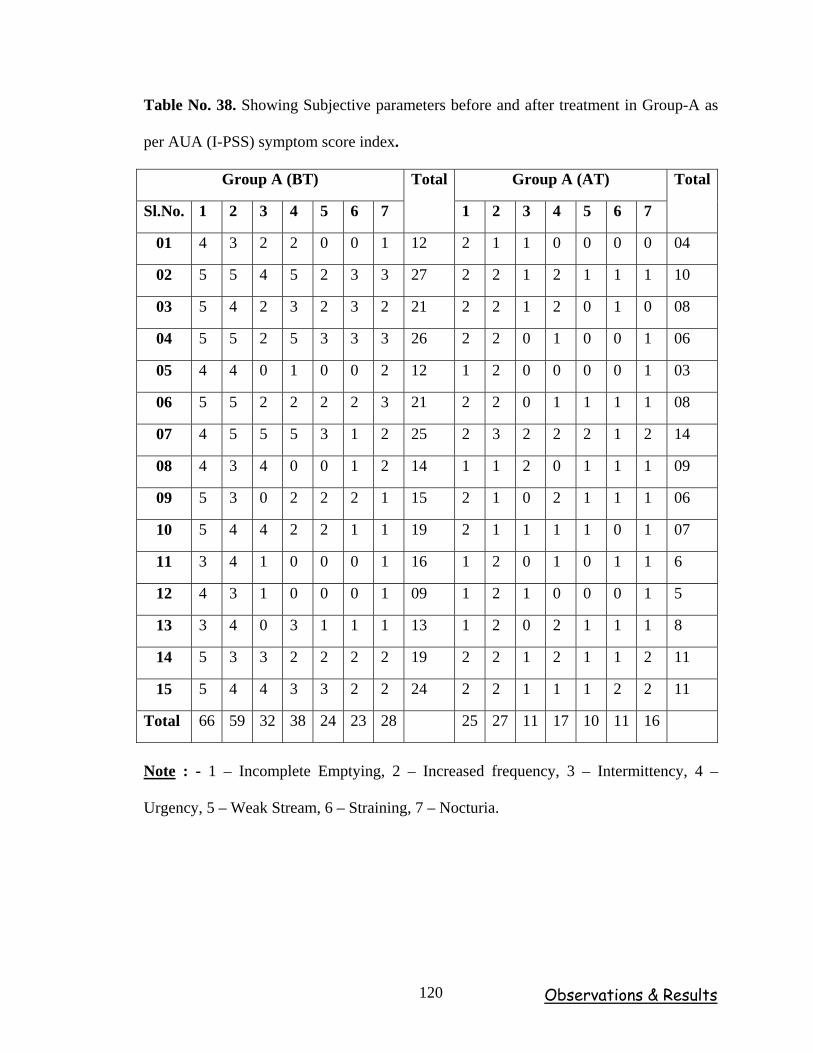
Observations & Results 120
Table No. 38. Showing Subjective parameters before and after treatment in Group-A as
per AUA (I-PSS) symptom score index.
Group A (BT) Group A (AT)
Sl.No. 1 2 3 4 5 6 7
Total
1 2 3 4 5 6 7
Total
01 4 3 2 2 0 0 1 12 2 1 1 0 0 0 0 04
02 5 5 4 5 2 3 3 27 2 2 1 2 1 1 1 10
03 5 4 2 3 2 3 2 21 2 2 1 2 0 1 0 08
04 5 5 2 5 3 3 3 26 2 2 0 1 0 0 1 06
05 4 4 0 1 0 0 2 12 1 2 0 0 0 0 1 03
06 5 5 2 2 2 2 3 21 2 2 0 1 1 1 1 08
07 4 5 5 5 3 1 2 25 2 3 2 2 2 1 2 14
08 4 3 4 0 0 1 2 14 1 1 2 0 1 1 1 09
09 5 3 0 2 2 2 1 15 2 1 0 2 1 1 1 06
10 5 4 4 2 2 1 1 19 2 1 1 1 1 0 1 07
11 3 4 1 0 0 0 1 16 1 2 0 1 0 1 1 6
12 4 3 1 0 0 0 1 09 1 2 1 0 0 0 1 5
13 3 4 0 3 1 1 1 13 1 2 0 2 1 1 1 8
14 5 3 3 2 2 2 2 19 2 2 1 2 1 1 2 11
15 5 4 4 3 3 2 2 24 2 2 1 1 1 2 2 11
Total 66 59 32 38 24 23 28 25 27 11 17 10 11 16
Note : - 1 – Incomplete Emptying, 2 – Increased frequency, 3 – Intermittency, 4 –
Urgency, 5 – Weak Stream, 6 – Straining, 7 – Nocturia.
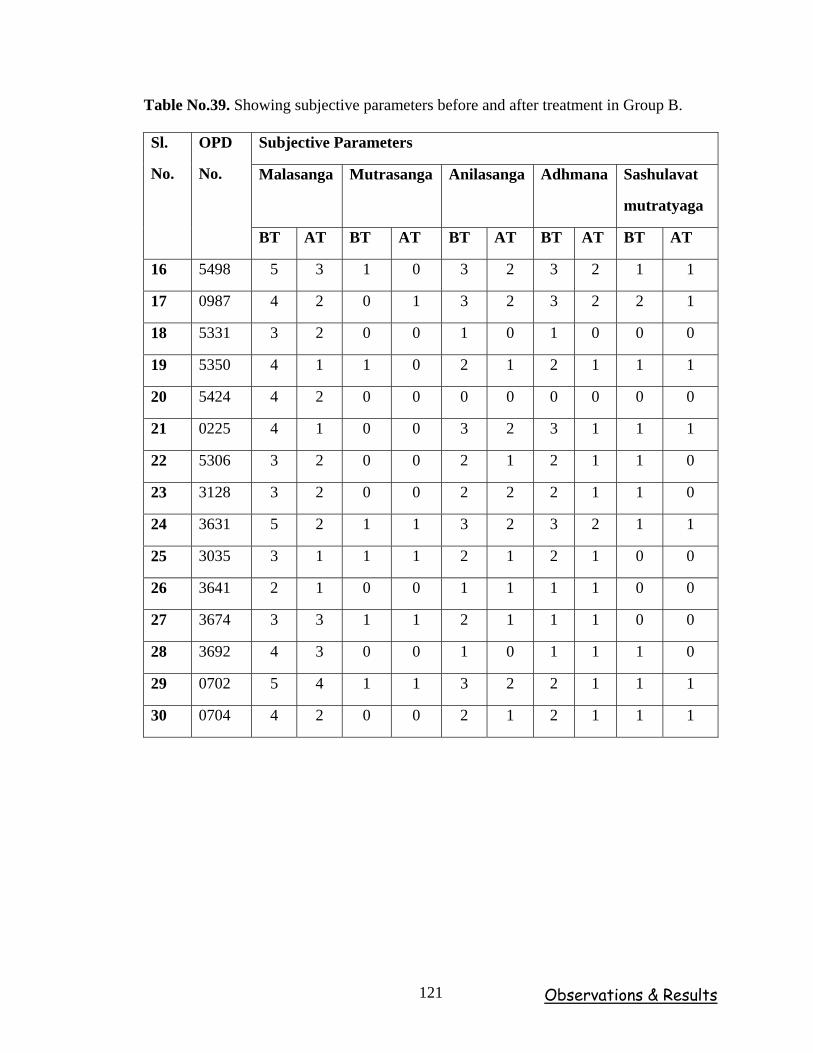
Observations & Results 121
Table No.39. Showing subjective parameters before and after treatment in Group B.
Subjective Parameters
Malasanga Mutrasanga Anilasanga Adhmana Sashulavat
mutratyaga
Sl.
No.
OPD
No.
BT AT BT AT BT AT BT AT BT AT
16 5498 5 3 1 0 3 2 3 2 1 1
17 0987 4 2 0 1 3 2 3 2 2 1
18 5331 3 2 0 0 1 0 1 0 0 0
19 5350 4 1 1 0 2 1 2 1 1 1
20 5424 4 2 0 0 0 0 0 0 0 0
21 0225 4 1 0 0 3 2 3 1 1 1
22 5306 3 2 0 0 2 1 2 1 1 0
23 3128 3 2 0 0 2 2 2 1 1 0
24 3631 5 2 1 1 3 2 3 2 1 1
25 3035 3 1 1 1 2 1 2 1 0 0
26 3641 2 1 0 0 1 1 1 1 0 0
27 3674 3 3 1 1 2 1 1 1 0 0
28 3692 4 3 0 0 1 0 1 1 1 0
29 0702 5 4 1 1 3 2 2 1 1 1
30 0704 4 2 0 0 2 1 2 1 1 1
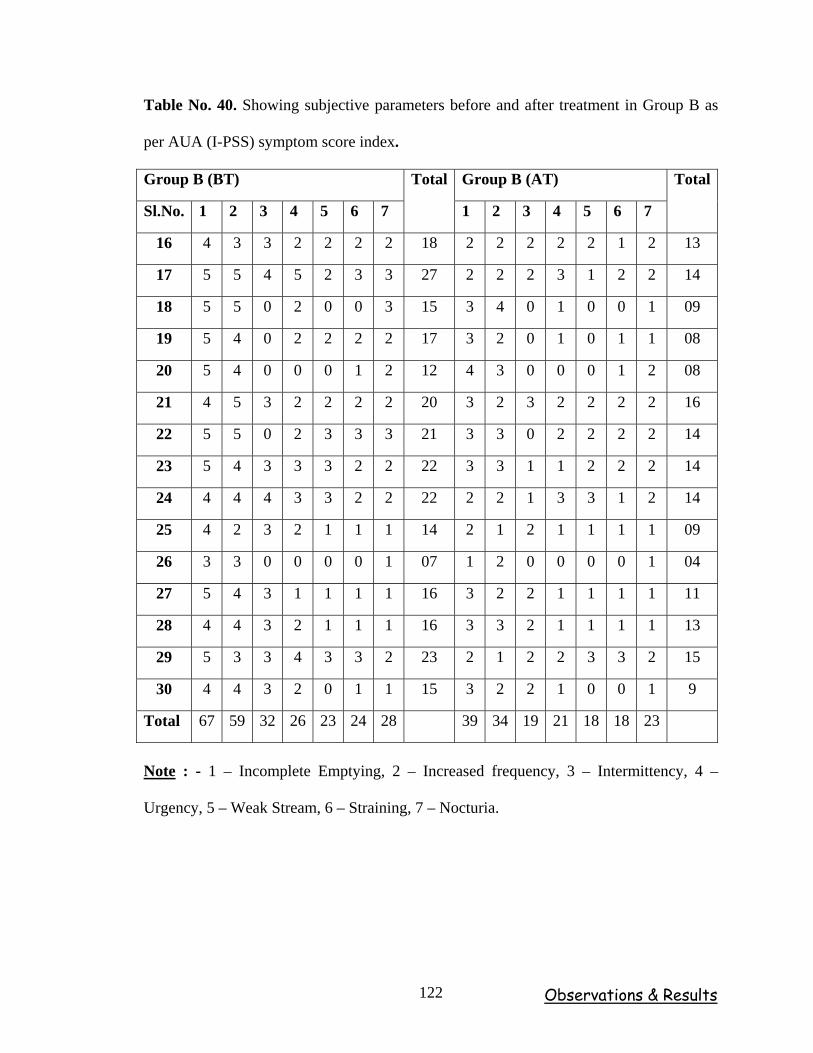
Observations & Results 122
Table No. 40. Showing subjective parameters before and after treatment in Group B as
per AUA (I-PSS) symptom score index.
Group B (BT) Group B (AT)
Sl.No. 1 2 3 4 5 6 7
Total
1 2 3 4 5 6 7
Total
16 4 3 3 2 2 2 2 18 2 2 2 2 2 1 2 13
17 5 5 4 5 2 3 3 27 2 2 2 3 1 2 2 14
18 5 5 0 2 0 0 3 15 3 4 0 1 0 0 1 09
19 5 4 0 2 2 2 2 17 3 2 0 1 0 1 1 08
20 5 4 0 0 0 1 2 12 4 3 0 0 0 1 2 08
21 4 5 3 2 2 2 2 20 3 2 3 2 2 2 2 16
22 5 5 0 2 3 3 3 21 3 3 0 2 2 2 2 14
23 5 4 3 3 3 2 2 22 3 3 1 1 2 2 2 14
24 4 4 4 3 3 2 2 22 2 2 1 3 3 1 2 14
25 4 2 3 2 1 1 1 14 2 1 2 1 1 1 1 09
26 3 3 0 0 0 0 1 07 1 2 0 0 0 0 1 04
27 5 4 3 1 1 1 1 16 3 2 2 1 1 1 1 11
28 4 4 3 2 1 1 1 16 3 3 2 1 1 1 1 13
29 5 3 3 4 3 3 2 23 2 1 2 2 3 3 2 15
30 4 4 3 2 0 1 1 15 3 2 2 1 0 0 1 9
Total 67 59 32 26 23 24 28 39 34 19 21 18 18 23
Note : - 1 – Incomplete Emptying, 2 – Increased frequency, 3 – Intermittency, 4 –
Urgency, 5 – Weak Stream, 6 – Straining, 7 – Nocturia.
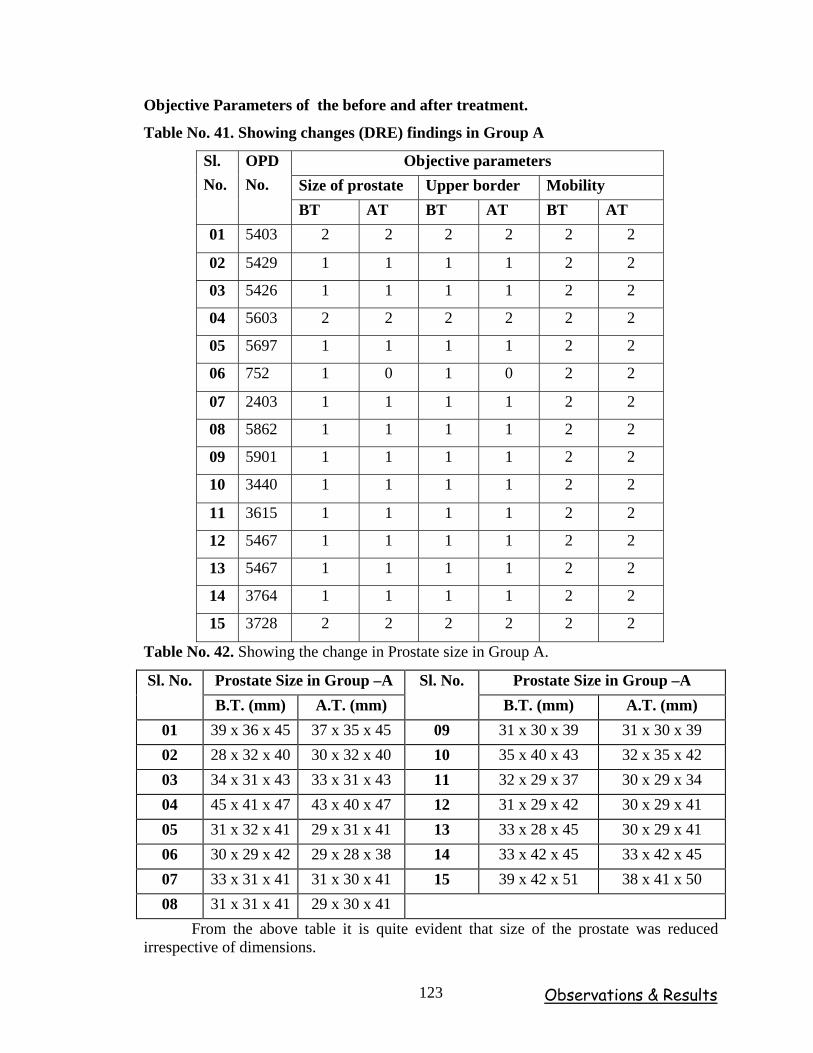
Observations & Results 123
Objective Parameters of the before and after treatment.
Table No. 41. Showing changes (DRE) findings in Group A
Objective parameters Size of prostate Upper border Mobility
Sl. No.
OPD No.
BT AT BT AT BT AT 01 5403 2 2 2 2 2 2
02 5429 1 1 1 1 2 2
03 5426 1 1 1 1 2 2
04 5603 2 2 2 2 2 2
05 5697 1 1 1 1 2 2
06 752 1 0 1 0 2 2
07 2403 1 1 1 1 2 2
08 5862 1 1 1 1 2 2
09 5901 1 1 1 1 2 2
10 3440 1 1 1 1 2 2
11 3615 1 1 1 1 2 2
12 5467 1 1 1 1 2 2
13 5467 1 1 1 1 2 2
14 3764 1 1 1 1 2 2
15 3728 2 2 2 2 2 2
Table No. 42. Showing the change in Prostate size in Group A.
Prostate Size in Group –A Prostate Size in Group –A Sl. No. B.T. (mm) A.T. (mm)
Sl. No. B.T. (mm) A.T. (mm)
01 39 x 36 x 45 37 x 35 x 45 09 31 x 30 x 39 31 x 30 x 39 02 28 x 32 x 40 30 x 32 x 40 10 35 x 40 x 43 32 x 35 x 42 03 34 x 31 x 43 33 x 31 x 43 11 32 x 29 x 37 30 x 29 x 34 04 45 x 41 x 47 43 x 40 x 47 12 31 x 29 x 42 30 x 29 x 41 05 31 x 32 x 41 29 x 31 x 41 13 33 x 28 x 45 30 x 29 x 41 06 30 x 29 x 42 29 x 28 x 38 14 33 x 42 x 45 33 x 42 x 45 07 33 x 31 x 41 31 x 30 x 41 15 39 x 42 x 51 38 x 41 x 50 08 31 x 31 x 41 29 x 30 x 41
From the above table it is quite evident that size of the prostate was reduced irrespective of dimensions.
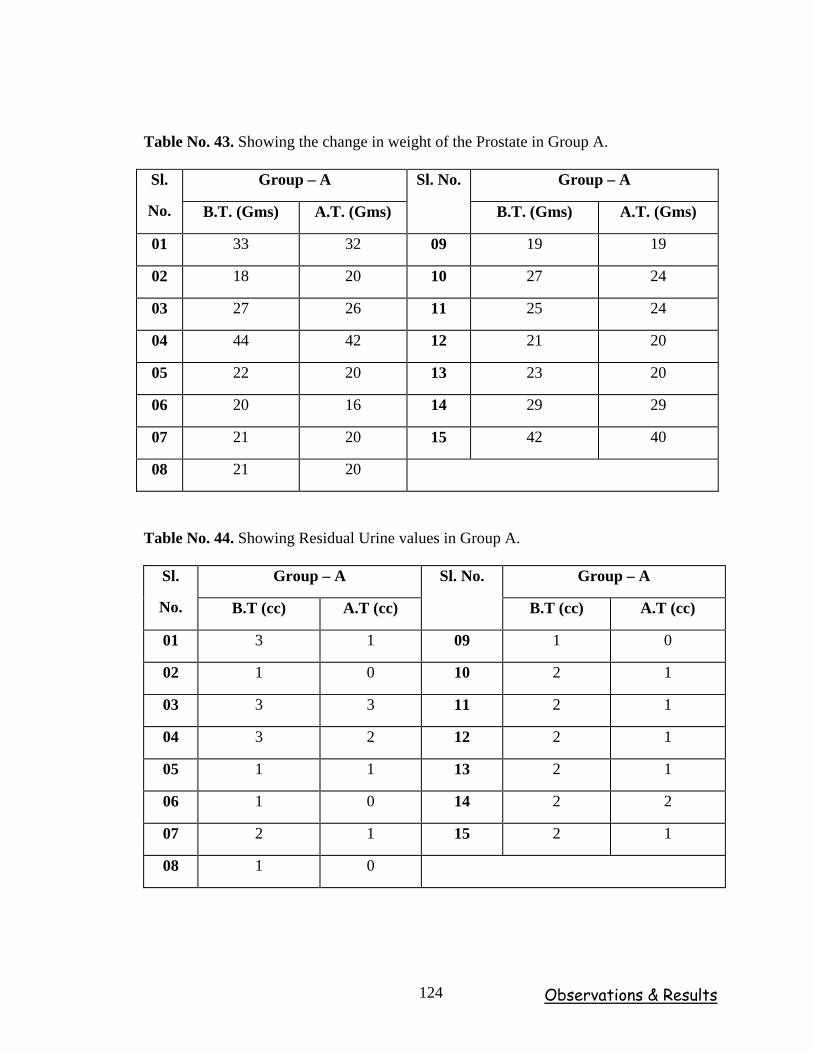
Observations & Results 124
Table No. 43. Showing the change in weight of the Prostate in Group A.
Group – A Group – A Sl.
No. B.T. (Gms) A.T. (Gms)
Sl. No.
B.T. (Gms) A.T. (Gms)
01 33 32 09 19 19
02 18 20 10 27 24
03 27 26 11 25 24
04 44 42 12 21 20
05 22 20 13 23 20
06 20 16 14 29 29
07 21 20 15 42 40
08 21 20
Table No. 44. Showing Residual Urine values in Group A.
Group – A Group – A Sl.
No. B.T (cc) A.T (cc)
Sl. No.
B.T (cc) A.T (cc)
01 3 1 09 1 0
02 1 0 10 2 1
03 3 3 11 2 1
04 3 2 12 2 1
05 1 1 13 2 1
06 1 0 14 2 2
07 2 1 15 2 1
08 1 0
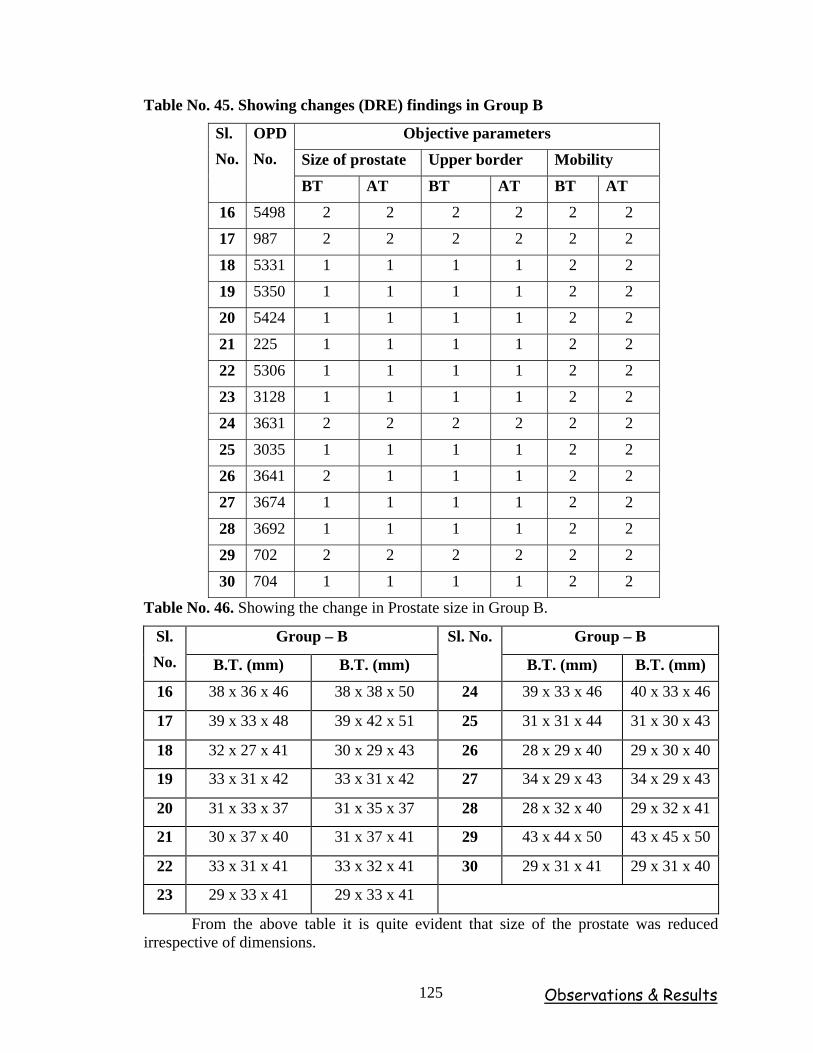
Observations & Results 125
Table No. 45. Showing changes (DRE) findings in Group B
Objective parameters
Size of prostate Upper border Mobility
Sl. No.
OPD No.
BT AT BT AT BT AT
16 5498 2 2 2 2 2 2
17 987 2 2 2 2 2 2
18 5331 1 1 1 1 2 2
19 5350 1 1 1 1 2 2
20 5424 1 1 1 1 2 2
21 225 1 1 1 1 2 2
22 5306 1 1 1 1 2 2
23 3128 1 1 1 1 2 2
24 3631 2 2 2 2 2 2
25 3035 1 1 1 1 2 2
26 3641 2 1 1 1 2 2
27 3674 1 1 1 1 2 2
28 3692 1 1 1 1 2 2
29 702 2 2 2 2 2 2
30 704 1 1 1 1 2 2
Table No. 46. Showing the change in Prostate size in Group B.
Group – B Group – B Sl. No. B.T. (mm) B.T. (mm)
Sl. No.
B.T. (mm) B.T. (mm)
16 38 x 36 x 46 38 x 38 x 50 24 39 x 33 x 46 40 x 33 x 46
17 39 x 33 x 48 39 x 42 x 51 25 31 x 31 x 44 31 x 30 x 43
18 32 x 27 x 41 30 x 29 x 43 26 28 x 29 x 40 29 x 30 x 40
19 33 x 31 x 42 33 x 31 x 42 27 34 x 29 x 43 34 x 29 x 43
20 31 x 33 x 37 31 x 35 x 37 28 28 x 32 x 40 29 x 32 x 41
21 30 x 37 x 40 31 x 37 x 41 29 43 x 44 x 50 43 x 45 x 50
22 33 x 31 x 41 33 x 32 x 41 30 29 x 31 x 41 29 x 31 x 40
23 29 x 33 x 41 29 x 33 x 41
From the above table it is quite evident that size of the prostate was reduced irrespective of dimensions.

Observations & Results 126
Table No. 47. Showing the change in weight of the Prostate in Group B.
Group – B Group – B Sl.
No. B.T. (Gms) A.T. (Gms)
Sl. No.
B.T. (Gms) A.T. (Gms)
16 37 37 24 32 32
17 33 44 25 21 22
18 20 22 26 18 19
19 23 23 27 23 23
20 20 20 28 19 20
21 25 25 29 49 49
22 21 22 30 21 20
23 22 22
Table No.48. Showing Residual Urine values in Group B.
Group – B Group – B Sl.
No. B.T (cc) A.T (cc)
Sl. No.
B.T (cc) A.T (cc)
16 2 1 24 2 2
17 2 2 25 1 1
18 2 1 26 1 1
19 1 1 27 2 1
20 1 1 28 1 1
21 2 1 29 2 2
22 1 1 30 2 1
23 1 1
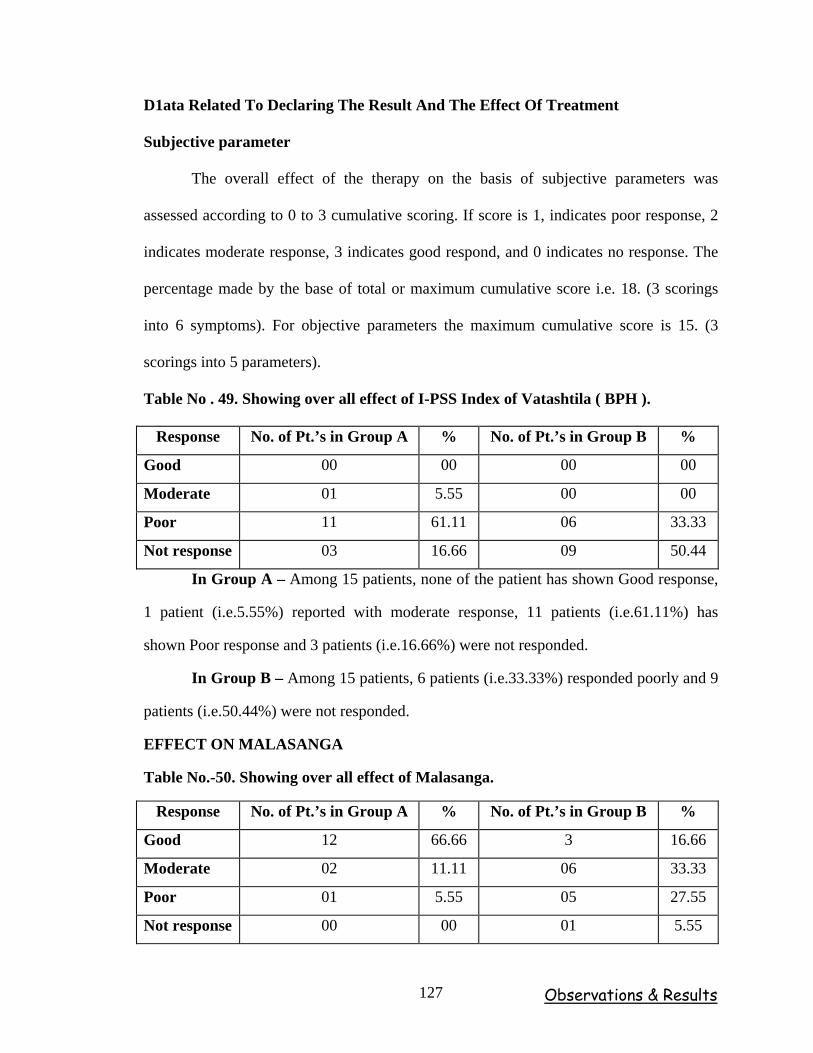
Observations & Results 127
D1ata Related To Declaring The Result And The Effect Of Treatment
Subjective parameter
The overall effect of the therapy on the basis of subjective parameters was
assessed according to 0 to 3 cumulative scoring. If score is 1, indicates poor response, 2
indicates moderate response, 3 indicates good respond, and 0 indicates no response. The
percentage made by the base of total or maximum cumulative score i.e. 18. (3 scorings
into 6 symptoms). For objective parameters the maximum cumulative score is 15. (3
scorings into 5 parameters).
Table No . 49. Showing over all effect of I-PSS Index of Vatashtila ( BPH ).
Response No. of Pt.’s in Group A % No. of Pt.’s in Group B %
Good 00 00 00 00
Moderate 01 5.55 00 00
Poor 11 61.11 06 33.33
Not response 03 16.66 09 50.44
In Group A – Among 15 patients, none of the patient has shown Good response,
1 patient (i.e.5.55%) reported with moderate response, 11 patients (i.e.61.11%) has
shown Poor response and 3 patients (i.e.16.66%) were not responded.
In Group B – Among 15 patients, 6 patients (i.e.33.33%) responded poorly and 9
patients (i.e.50.44%) were not responded.
EFFECT ON MALASANGA
Table No.-50. Showing over all effect of Malasanga.
Response No. of Pt.’s in Group A % No. of Pt.’s in Group B %
Good 12 66.66 3 16.66
Moderate 02 11.11 06 33.33
Poor 01 5.55 05 27.55
Not response 00 00 01 5.55
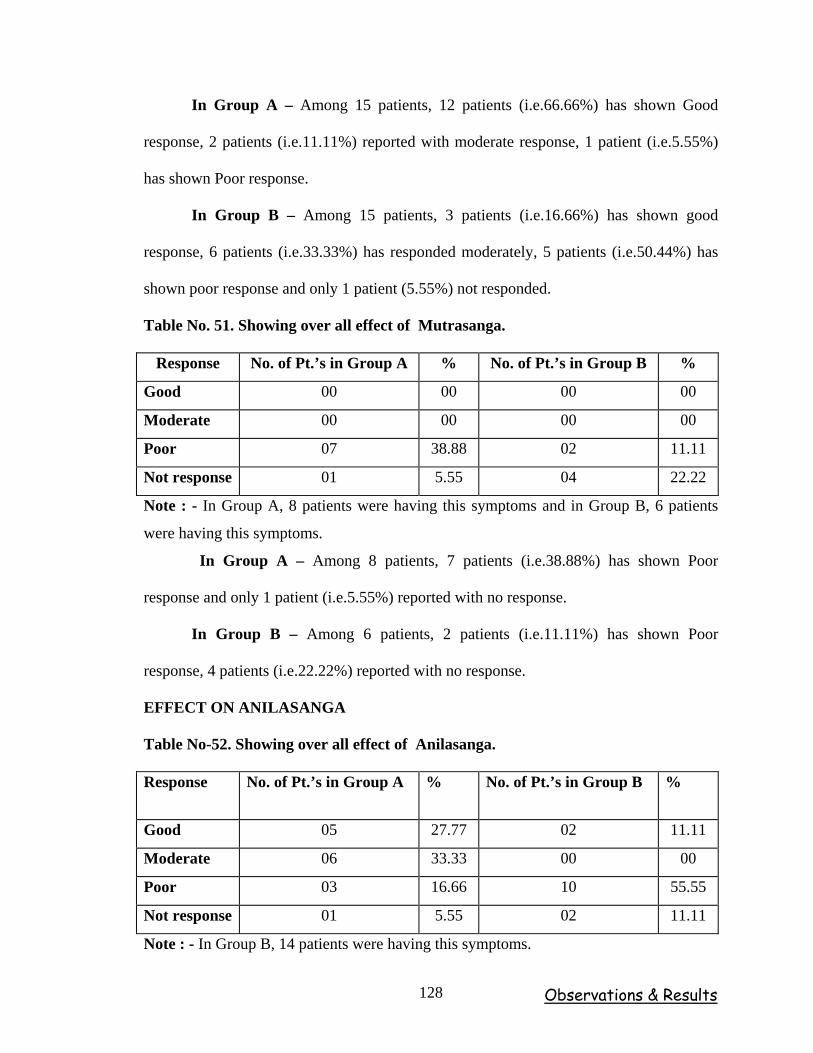
Observations & Results 128
In Group A – Among 15 patients, 12 patients (i.e.66.66%) has shown Good
response, 2 patients (i.e.11.11%) reported with moderate response, 1 patient (i.e.5.55%)
has shown Poor response.
In Group B – Among 15 patients, 3 patients (i.e.16.66%) has shown good
response, 6 patients (i.e.33.33%) has responded moderately, 5 patients (i.e.50.44%) has
shown poor response and only 1 patient (5.55%) not responded.
Table No. 51. Showing over all effect of Mutrasanga.
Response No. of Pt.’s in Group A % No. of Pt.’s in Group B %
Good 00 00 00 00
Moderate 00 00 00 00
Poor 07 38.88 02 11.11
Not response 01 5.55 04 22.22
Note : - In Group A, 8 patients were having this symptoms and in Group B, 6 patients
were having this symptoms.
In Group A – Among 8 patients, 7 patients (i.e.38.88%) has shown Poor
response and only 1 patient (i.e.5.55%) reported with no response.
In Group B – Among 6 patients, 2 patients (i.e.11.11%) has shown Poor
response, 4 patients (i.e.22.22%) reported with no response.
EFFECT ON ANILASANGA
Table No-52. Showing over all effect of Anilasanga.
Response No. of Pt.’s in Group A % No. of Pt.’s in Group B %
Good 05 27.77 02 11.11
Moderate 06 33.33 00 00
Poor 03 16.66 10 55.55
Not response 01 5.55 02 11.11
Note : - In Group B, 14 patients were having this symptoms.
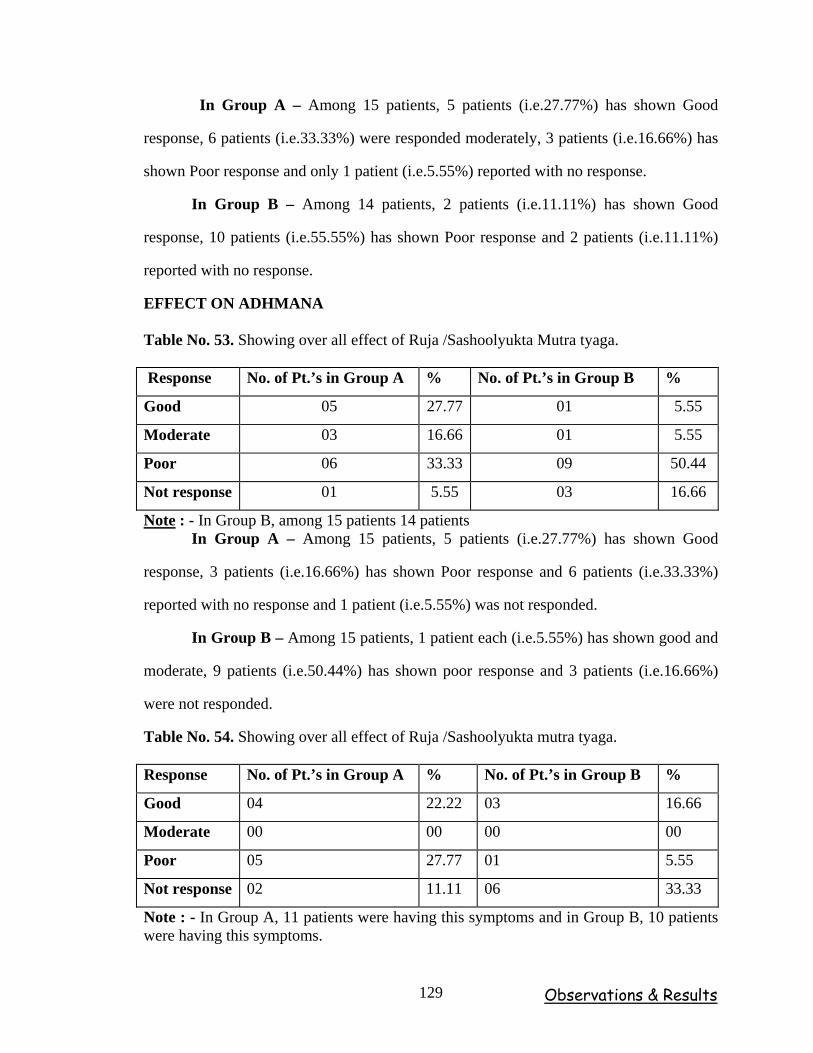
Observations & Results 129
In Group A – Among 15 patients, 5 patients (i.e.27.77%) has shown Good
response, 6 patients (i.e.33.33%) were responded moderately, 3 patients (i.e.16.66%) has
shown Poor response and only 1 patient (i.e.5.55%) reported with no response.
In Group B – Among 14 patients, 2 patients (i.e.11.11%) has shown Good
response, 10 patients (i.e.55.55%) has shown Poor response and 2 patients (i.e.11.11%)
reported with no response.
EFFECT ON ADHMANA
Table No. 53. Showing over all effect of Ruja /Sashoolyukta Mutra tyaga.
Response No. of Pt.’s in Group A % No. of Pt.’s in Group B %
Good 05 27.77 01 5.55
Moderate 03 16.66 01 5.55
Poor 06 33.33 09 50.44
Not response 01 5.55 03 16.66
Note : - In Group B, among 15 patients 14 patients In Group A – Among 15 patients, 5 patients (i.e.27.77%) has shown Good
response, 3 patients (i.e.16.66%) has shown Poor response and 6 patients (i.e.33.33%)
reported with no response and 1 patient (i.e.5.55%) was not responded.
In Group B – Among 15 patients, 1 patient each (i.e.5.55%) has shown good and
moderate, 9 patients (i.e.50.44%) has shown poor response and 3 patients (i.e.16.66%)
were not responded.
Table No. 54. Showing over all effect of Ruja /Sashoolyukta mutra tyaga.
Response No. of Pt.’s in Group A % No. of Pt.’s in Group B %
Good 04 22.22 03 16.66
Moderate 00 00 00 00
Poor 05 27.77 01 5.55
Not response 02 11.11 06 33.33
Note : - In Group A, 11 patients were having this symptoms and in Group B, 10 patients were having this symptoms.
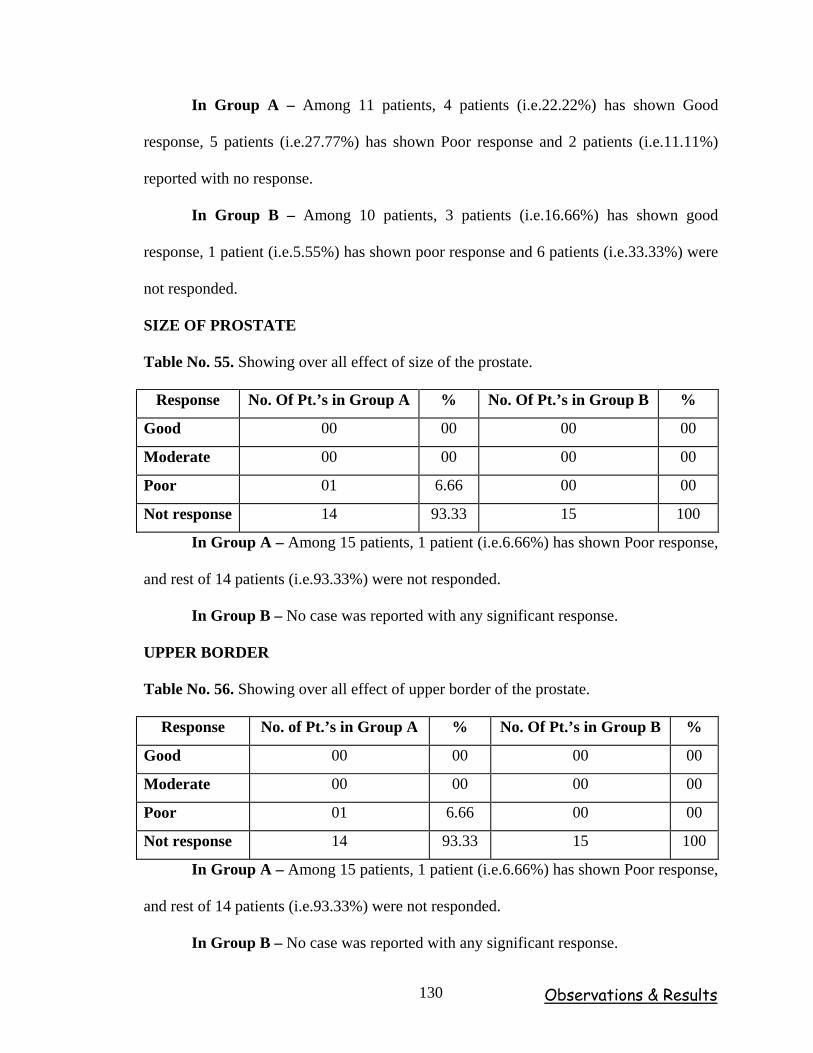
Observations & Results 130
In Group A – Among 11 patients, 4 patients (i.e.22.22%) has shown Good
response, 5 patients (i.e.27.77%) has shown Poor response and 2 patients (i.e.11.11%)
reported with no response.
In Group B – Among 10 patients, 3 patients (i.e.16.66%) has shown good
response, 1 patient (i.e.5.55%) has shown poor response and 6 patients (i.e.33.33%) were
not responded.
SIZE OF PROSTATE
Table No. 55. Showing over all effect of size of the prostate.
Response No. Of Pt.’s in Group A % No. Of Pt.’s in Group B %
Good 00 00 00 00
Moderate 00 00 00 00
Poor 01 6.66 00 00
Not response 14 93.33 15 100
In Group A – Among 15 patients, 1 patient (i.e.6.66%) has shown Poor response,
and rest of 14 patients (i.e.93.33%) were not responded.
In Group B – No case was reported with any significant response.
UPPER BORDER
Table No. 56. Showing over all effect of upper border of the prostate.
Response No. of Pt.’s in Group A % No. Of Pt.’s in Group B %
Good 00 00 00 00
Moderate 00 00 00 00
Poor 01 6.66 00 00
Not response 14 93.33 15 100
In Group A – Among 15 patients, 1 patient (i.e.6.66%) has shown Poor response,
and rest of 14 patients (i.e.93.33%) were not responded.
In Group B – No case was reported with any significant response.
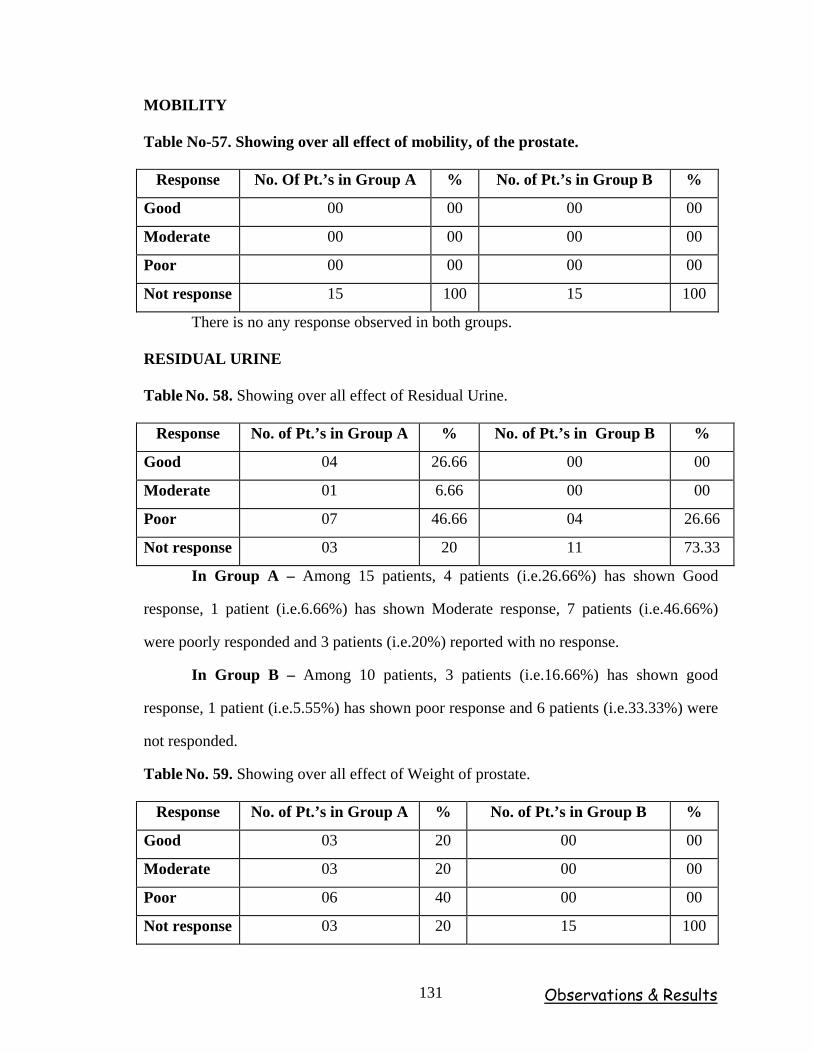
Observations & Results 131
MOBILITY
Table No-57. Showing over all effect of mobility, of the prostate.
Response No. Of Pt.’s in Group A % No. of Pt.’s in Group B %
Good 00 00 00 00
Moderate 00 00 00 00
Poor 00 00 00 00
Not response 15 100 15 100
There is no any response observed in both groups.
RESIDUAL URINE
Table No. 58. Showing over all effect of Residual Urine.
Response No. of Pt.’s in Group A % No. of Pt.’s in Group B %
Good 04 26.66 00 00
Moderate 01 6.66 00 00
Poor 07 46.66 04 26.66
Not response 03 20 11 73.33
In Group A – Among 15 patients, 4 patients (i.e.26.66%) has shown Good
response, 1 patient (i.e.6.66%) has shown Moderate response, 7 patients (i.e.46.66%)
were poorly responded and 3 patients (i.e.20%) reported with no response.
In Group B – Among 10 patients, 3 patients (i.e.16.66%) has shown good
response, 1 patient (i.e.5.55%) has shown poor response and 6 patients (i.e.33.33%) were
not responded.
Table No. 59. Showing over all effect of Weight of prostate.
Response No. of Pt.’s in Group A % No. of Pt.’s in Group B %
Good 03 20 00 00
Moderate 03 20 00 00
Poor 06 40 00 00
Not response 03 20 15 100
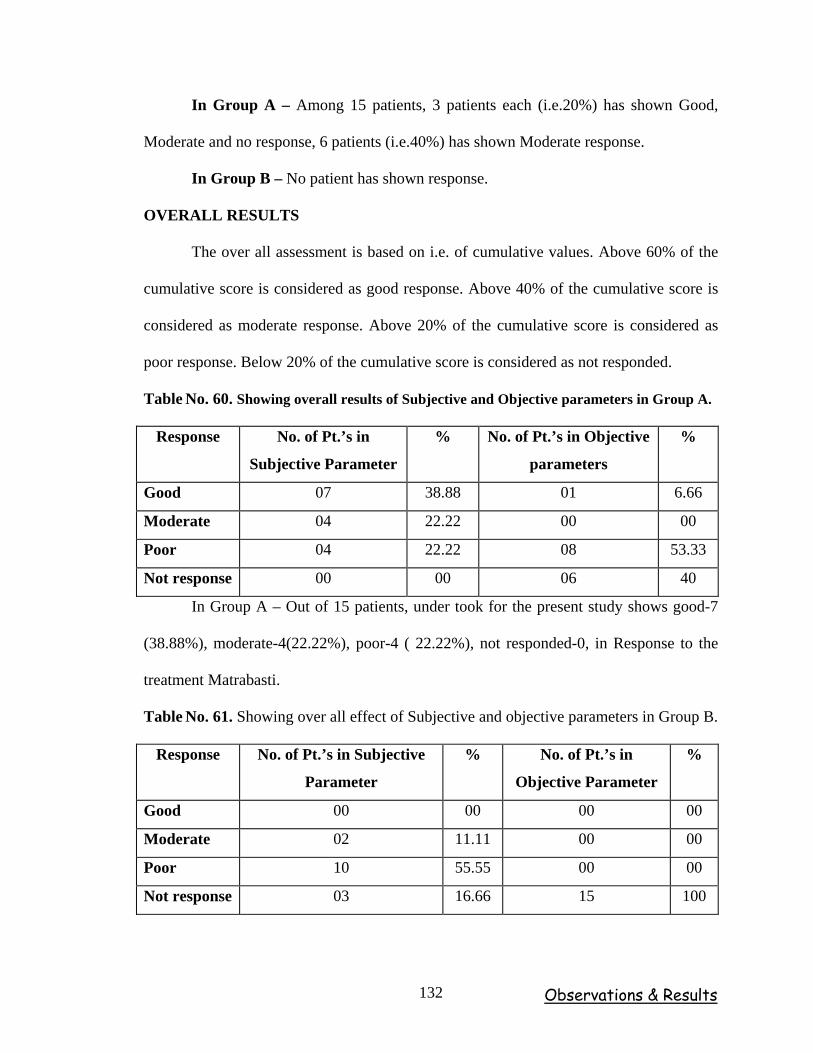
Observations & Results 132
In Group A – Among 15 patients, 3 patients each (i.e.20%) has shown Good,
Moderate and no response, 6 patients (i.e.40%) has shown Moderate response.
In Group B – No patient has shown response.
OVERALL RESULTS
The over all assessment is based on i.e. of cumulative values. Above 60% of the
cumulative score is considered as good response. Above 40% of the cumulative score is
considered as moderate response. Above 20% of the cumulative score is considered as
poor response. Below 20% of the cumulative score is considered as not responded.
Table No. 60. Showing overall results of Subjective and Objective parameters in Group A.
Response No. of Pt.’s in
Subjective Parameter
% No. of Pt.’s in Objective
parameters
%
Good 07 38.88 01 6.66
Moderate 04 22.22 00 00
Poor 04 22.22 08 53.33
Not response 00 00 06 40
In Group A – Out of 15 patients, under took for the present study shows good-7
(38.88%), moderate-4(22.22%), poor-4 ( 22.22%), not responded-0, in Response to the
treatment Matrabasti.
Table No. 61. Showing over all effect of Subjective and objective parameters in Group B.
Response No. of Pt.’s in Subjective
Parameter
% No. of Pt.’s in
Objective Parameter
%
Good 00 00 00 00
Moderate 02 11.11 00 00
Poor 10 55.55 00 00
Not response 03 16.66 15 100
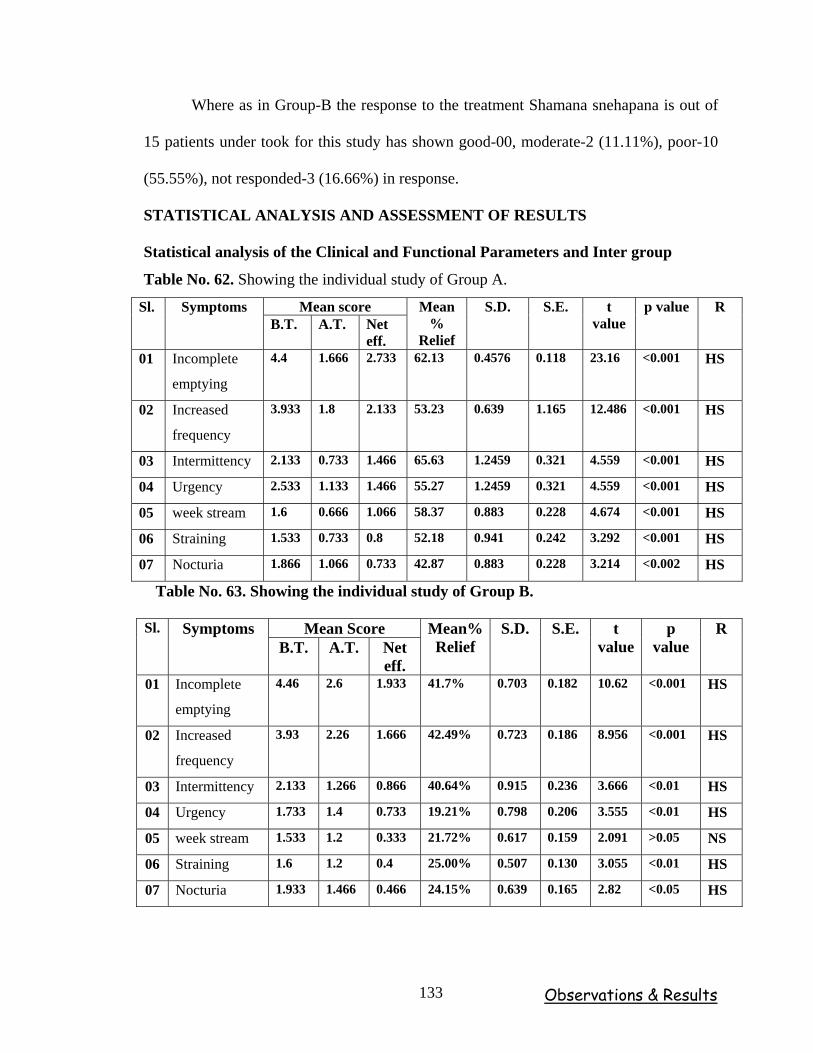
Observations & Results 133
Where as in Group-B the response to the treatment Shamana snehapana is out of
15 patients under took for this study has shown good-00, moderate-2 (11.11%), poor-10
(55.55%), not responded-3 (16.66%) in response.
STATISTICAL ANALYSIS AND ASSESSMENT OF RESULTS
Statistical analysis of the Clinical and Functional Parameters and Inter group
Table No. 62. Showing the individual study of Group A.
Mean score Sl. Symptoms B.T. A.T. Net
eff.
Mean%
Relief
S.D. S.E. t value
p value R
01 Incomplete
emptying
4.4 1.666 2.733 62.13 0.4576 0.118 23.16 <0.001 HS
02 Increased
frequency
3.933 1.8 2.133 53.23 0.639 1.165 12.486 <0.001 HS
03 Intermittency 2.133 0.733 1.466 65.63 1.2459 0.321 4.559 <0.001 HS
04 Urgency 2.533 1.133 1.466 55.27 1.2459 0.321 4.559 <0.001 HS
05 week stream 1.6 0.666 1.066 58.37 0.883 0.228 4.674 <0.001 HS
06 Straining 1.533 0.733 0.8 52.18 0.941 0.242 3.292 <0.001 HS
07 Nocturia 1.866 1.066 0.733 42.87 0.883 0.228 3.214 <0.002 HS
Table No. 63. Showing the individual study of Group B.
Mean Score Sl. Symptoms B.T. A.T. Net
eff.
Mean%Relief
S.D. S.E. t value
p value
R
01 Incomplete
emptying
4.46 2.6 1.933 41.7% 0.703 0.182 10.62 <0.001 HS
02 Increased
frequency
3.93 2.26 1.666 42.49% 0.723 0.186 8.956 <0.001 HS
03 Intermittency 2.133 1.266 0.866 40.64% 0.915 0.236 3.666 <0.01 HS
04 Urgency 1.733 1.4 0.733 19.21% 0.798 0.206 3.555 <0.01 HS
05 week stream 1.533 1.2 0.333 21.72% 0.617 0.159 2.091 >0.05 NS
06 Straining 1.6 1.2 0.4 25.00% 0.507 0.130 3.055 <0.01 HS
07 Nocturia 1.933 1.466 0.466 24.15% 0.639 0.165 2.82 <0.05 HS
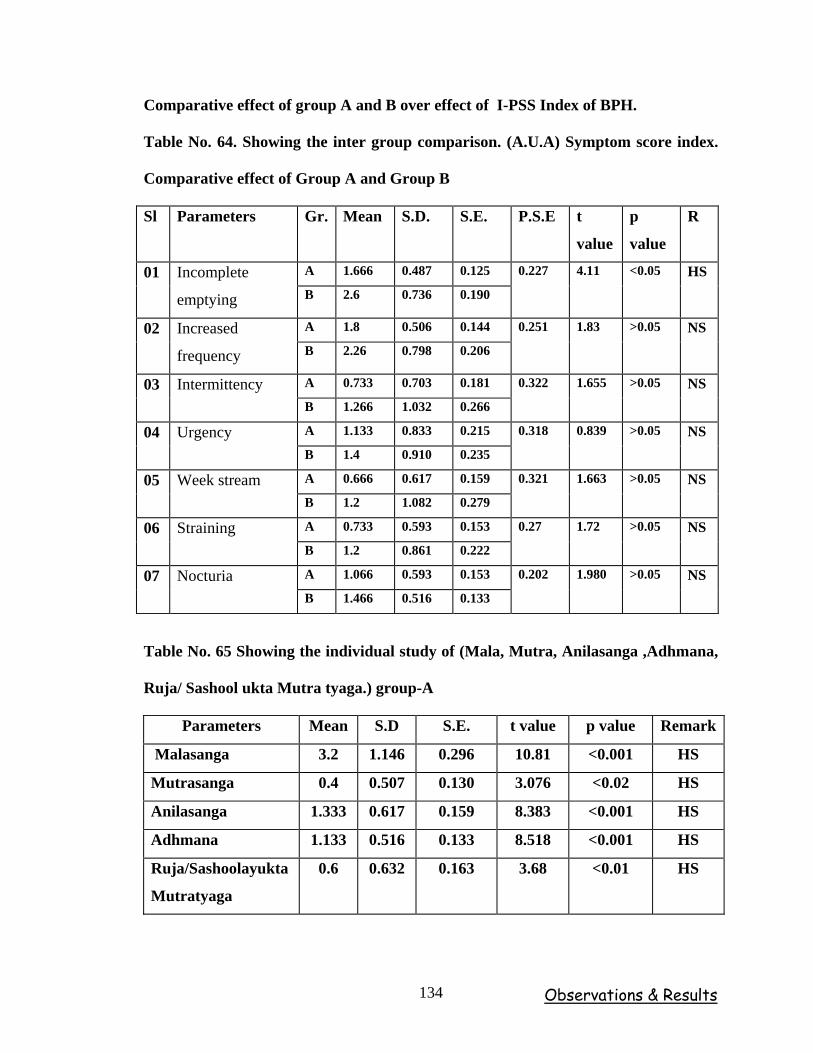
Observations & Results 134
Comparative effect of group A and B over effect of I-PSS Index of BPH.
Table No. 64. Showing the inter group comparison. (A.U.A) Symptom score index.
Comparative effect of Group A and Group B
Sl Parameters Gr. Mean S.D. S.E. P.S.E t
value
p
value
R
A 1.666 0.487 0.125 01 Incomplete
emptying B 2.6 0.736 0.190
0.227 4.11 <0.05 HS
A 1.8 0.506 0.144 02 Increased
frequency B 2.26 0.798 0.206
0.251 1.83 >0.05 NS
A 0.733 0.703 0.181 03 Intermittency B 1.266 1.032 0.266
0.322 1.655 >0.05 NS
A 1.133 0.833 0.215 04 Urgency B 1.4 0.910 0.235
0.318 0.839 >0.05 NS
A 0.666 0.617 0.159 05 Week stream B 1.2 1.082 0.279
0.321 1.663 >0.05 NS
A 0.733 0.593 0.153 06 Straining B 1.2 0.861 0.222
0.27 1.72 >0.05 NS
A 1.066 0.593 0.153 07 Nocturia B 1.466 0.516 0.133
0.202 1.980 >0.05 NS
Table No. 65 Showing the individual study of (Mala, Mutra, Anilasanga ,Adhmana,
Ruja/ Sashool ukta Mutra tyaga.) group-A
Parameters Mean S.D S.E. t value p value Remark
Malasanga 3.2 1.146 0.296 10.81 <0.001 HS
Mutrasanga 0.4 0.507 0.130 3.076 <0.02 HS
Anilasanga 1.333 0.617 0.159 8.383 <0.001 HS
Adhmana 1.133 0.516 0.133 8.518 <0.001 HS
Ruja/Sashoolayukta
Mutratyaga
0.6 0.632 0.163 3.68 <0.01 HS
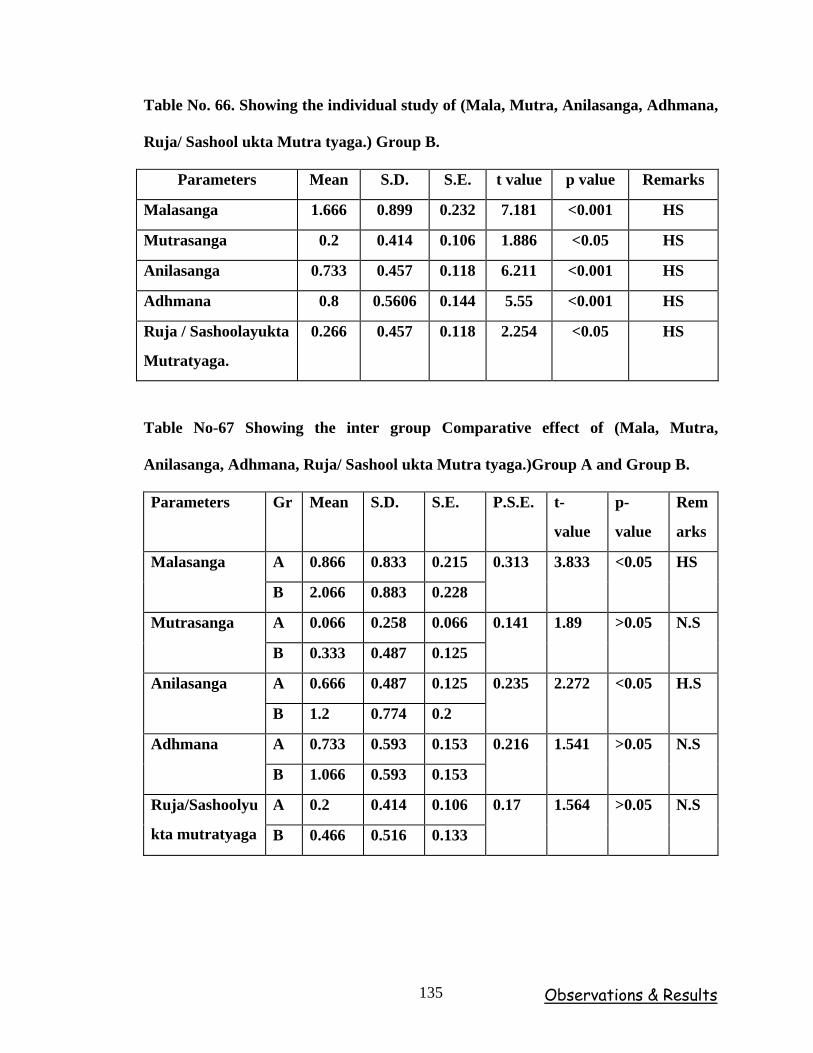
Observations & Results 135
Table No. 66. Showing the individual study of (Mala, Mutra, Anilasanga, Adhmana,
Ruja/ Sashool ukta Mutra tyaga.) Group B.
Parameters Mean S.D. S.E. t value p value Remarks
Malasanga 1.666 0.899 0.232 7.181 <0.001 HS
Mutrasanga 0.2 0.414 0.106 1.886 <0.05 HS
Anilasanga 0.733 0.457 0.118 6.211 <0.001 HS
Adhmana 0.8 0.5606 0.144 5.55 <0.001 HS
Ruja / Sashoolayukta
Mutratyaga.
0.266 0.457 0.118 2.254 <0.05 HS
Table No-67 Showing the inter group Comparative effect of (Mala, Mutra,
Anilasanga, Adhmana, Ruja/ Sashool ukta Mutra tyaga.)Group A and Group B.
Parameters Gr Mean S.D. S.E. P.S.E. t-
value
p-
value
Rem
arks
A 0.866 0.833 0.215 Malasanga
B 2.066 0.883 0.228
0.313 3.833 <0.05 HS
A 0.066 0.258 0.066 Mutrasanga
B 0.333 0.487 0.125
0.141 1.89 >0.05 N.S
A 0.666 0.487 0.125 Anilasanga
B 1.2 0.774 0.2
0.235 2.272 <0.05 H.S
A 0.733 0.593 0.153 Adhmana
B 1.066 0.593 0.153
0.216 1.541 >0.05 N.S
A 0.2 0.414 0.106 Ruja/Sashoolyu
kta mutratyaga B 0.466 0.516 0.133
0.17 1.564 >0.05 N.S
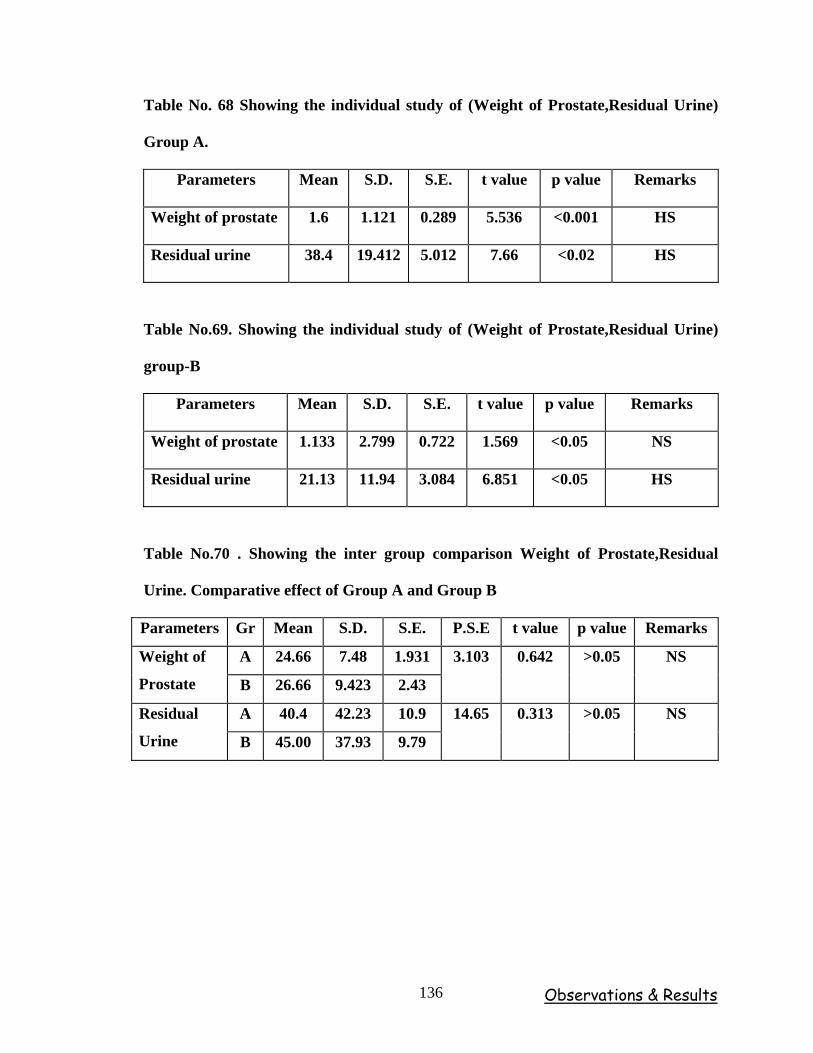
Observations & Results 136
Table No. 68 Showing the individual study of (Weight of Prostate,Residual Urine)
Group A.
Parameters Mean S.D. S.E. t value p value Remarks
Weight of prostate 1.6 1.121 0.289 5.536 <0.001 HS
Residual urine 38.4 19.412 5.012 7.66 <0.02 HS
Table No.69. Showing the individual study of (Weight of Prostate,Residual Urine)
group-B
Parameters Mean S.D. S.E. t value p value Remarks
Weight of prostate 1.133 2.799 0.722 1.569 <0.05 NS
Residual urine 21.13 11.94 3.084 6.851 <0.05 HS
Table No.70 . Showing the inter group comparison Weight of Prostate,Residual
Urine. Comparative effect of Group A and Group B
Parameters Gr Mean S.D. S.E. P.S.E t value p value Remarks
A 24.66 7.48 1.931 Weight of
Prostate B 26.66 9.423 2.43
3.103 0.642 >0.05 NS
A 40.4 42.23 10.9 Residual
Urine B 45.00 37.93 9.79
14.65 0.313 >0.05 NS
Observations & Results 137
STATISTICAL CONCLUSION
When the two groups are compared, except in the parameter incomplete emptying
rest of the parameters shows non-significant i.e. the mean effect incomplete emptying is
not same in the two groups after the treatment (p<0.05 ). But individually the
performance of Group A is more effective in the all the parameters (by comparing p
value). The parameter incomplete emptying, urgency, straining, and nocturia, shows
more significant in Group A than in Group B (by comparing t value). The parameter
weak stream shows non-significant in Group B (p>0.05). In Group B, the mean effect
after the treatment is more than Group A, but the in Group A the variation of the S.D is
very less in the parameter. There is uniform effect in all the parameter on the patient. We
can also observe the mean net effect of Group A is more than Group B before and after
the treatment. Hence, Group A is more effective (by comparing mean, variance, and co-
efficient of variation.)
In the parameter except Malasanga and Anilasanga Adhmana, Sashulayukta mutra
tyaga, shows not-significant. When the mean effect of the two groups. But, the individual
groups shows significance in the above said parameters. The but the objective parameters
weight of the prostate and residual urine shows non-significant in the mean effect of the
two groups after the treatment individually the Group A shows more significant than
Group B in the parameter of weight of the prostate and residual urine, but the parameter
weight of the prostate is not-significant in Group B.
Human beings have developed two characteristics since the ages – the urge to
impart his knowledge to other members and the desire to record the life and needs.
Because of these characteristics, lots of inventions have been enlightened in the field of
scientific explanation. Ayurveda is a simple, practical science of life, whose principles
are universally applicable to each individual’s daily existence. Ayurveda speaks of every
element and facet of human life, offering guidance that who seeks greater harmony,
peace and longevity.
Discussion part is divided into five sections.
1. Discussion on Vatashtila (BPH).
2. Discussion on clinical study.
3. Discussion on role of Sukumara Kumaraka Ghrita in Vatashtila (BPH).
4. Discussion on probable mode of action of Matrabasti and Shamana Snehapana
with Sukumara Kumaraka Ghrita in Vatashtila (BPH).
DISCUSSION ON VATASHTILA (BPH)
Ashtila is the hard, round, stony structure. Acharya Sushruta explained very
clearly about its structure and location in the body. It is located in Shakrunmarga i.e. in
between Guda and Basti pradesha. Acharya has explained different types of anatomical
structures with lot of similes for the Ashtila which are elaborated in literary part.
Vatashtila is the condition where in complete or partial obstruction due to
“Ashtilavat Ghana Granthi”, which leads to Mala, Mutra, Aanilasanga and Adhmana, etc
is seen.
Discussion 138
VATASHTILA vis-à-vis PROSTATE
It is one of the great job being an Ayurvedist, with regards to find the description
of prostate gland and the interpretation of its related explantion in Ayurveda. There is no
direct reference regarding this entity in the existent Ayurvedic literature. There by it is
our prime duty to give an appropriate conclusion related to prostate gland in Ayurvedic
terms.
But some scholars concluded that Basti shiras as prostate gland. Where as
Dalhanas comments on Su. Ni. 3\5 and emphasis as “Basti Shiraha Mutrashayopari
Tanobagaha”. It means basti shiras lies in the upper part of the bladder.
As our Acharyas dealt even about the minute structures of the body, no doubt they
may have mentioned about the prostate. Acharya Sushruta mentioned about the organs,
which lies around the Basti, while explaining Mutra utpatti, he emphasized on location of
the Basti, and mentioned the terms like Pourusham, Vrishanou and Guda. (Su. Ni 3\19).
Here, Pourusha can be safely concluded as prostate because, many scholars and
authors have followed the same view. Following are the some of the references –
Pourusha Granthi Vriddhi Ki Ayurveda Chikitsa – By – Dr. P. B. Gupta (New
Delhi)
Shareera Rachanatmaka Ve Kriyatmaka Drishtise Vasti, Vankshana,
Mutrashaya Ve Vrikka Aadi Ka Vivechanatamaka Adhyayana – By Dr. Suman
Rawat & Dr. Umashankar (New Delhi).
A Text Book of Sachitra Hindi Pratyakshika Shareera – By – Kaviraj Gananath
Sena.
Discussion 139
Acharya Sushruta while explaining the location of Vatashtila, mentioned the
terms like “Shakrun Marga” on this regard Dalhana comments that Guda and Basti as
“Shakrun Marga” and in this place Vatashtila is situated which is “Deergha Varthula
Akara,”. within this area there is no other organ which is “Deergha Varthula Akara,”
other than prostate. By this we can concluded that Vatashtila is none other than prostate
which is situated in the inferior aspect of the bladder. (Located at the point at which the
bladder gives rise to the urethra) (Ref-Bailey & Love’s)
Mutra praseka
There is no direct reference regarding the length of Mutra praseka but with the
help of Uttara Basti netra pramana it can be summed that, the length of Mutra praseka in
males is 6 - 7 angula.
Pourusha
Prostate being purely a reproductive gland and if we consider "Pourusha" as
Shukravaha Nadi which extends from Vrushana and opens in Mutra praseka just 2 angula
below Bastidwara then we can infer that probably Acharyas were included such an organ
in between Medhra mula pradesha and Basti dwara, which resembles that of Prostate
gland but. Pourusha Granthi the term already considered as a prostate gland by some
experts. I too agree with that “Pourusha” can be correlated with prostate, but when it
turns to Benign Prostate Hyperplasia it can be correlate with Vatashtila on the basis of
structure, location, signs and symptoms as already explained.
Discussion 140
Prostate
The function of prostate and its vulnerabilities arise from its place in male
anatomy. The prostate is a walnut sized chestnut shaped gland which is strategically
located at the point at which the bladder gives rise to the urethra, the outlet for urine. In
an adult male, the prostate usually weighs about 20 grams. Almost all of this mass
develops during puberty in response to hormonal changes associated with maturation.
The prostate literally doubles in size during puberty. In some of the men prostate
never changes in size. But, unfortunately 60% of elder population (i.e. age group of 50-60
years) is in progressive stage of BPH. Usually this remains asymptomatic till the age of
50, by the age of 80, however 90% of men suffer from one or more symptoms of BPH.
Female Prostate
The term some times applied to the periurethral glands in the upper part of urethra
in the female. This is from “Stadman’s Dictionary” But it cannot be taken into
consideration because we cannot found appropriate literature about it.
NIDANA
In our classics Vardhakyajanita rogas are mentioned along with their preventive
measures viz. Vatavyadi, Vriddhakyajanya klibya, etc. Arunadutta states that,
Vriddhavastha is Vata prokopakala. (A.Hr.Su.1/8) Creation, maintenance and destruction
of our body is under the control of Vata and it is responsible for Arogya and Anarogyata
of our body. In Vriddhavastha Ojovikriti occurs and leads to Vyadhikshamatwa heenata
intern causes Dhatukshaya. Persistent nidana sevana makes the Prakupita vata to attain
Prasaradi avasthas.
Vatasthila is one of the Vatadosha pradana vyadhi. Vriddhavastha may be the one
of Anubandi karana for Vatashtila. Frequency of micturition, difficulty in micturition,
partial or complete obstruction of urine and constipation, etc generally follows with old
age.
Discussion 141
AHARAJA NIDANA
Teekshnoushadhi, Ruksha madya sevana causes vitiation of Mutrvaha Shrotas,
Most of the pharmacological agents like higher antibiotics, α–sympathomimetic,
Antidepressants, Bronchodilators, Anticholinergic agents, α-andrenergic agents and
psychotropic drugs causes LUTS and BPH. In one or the other aspect they disturb the
functional as well as structural integrity of Mutravaha srotas by their Teekshna, Ushna
guna.
Anupa matsya sevana, Adhyashayana and Ajeerna
Anupadesha matsya is having the qualities like Snigdha, Bahudoshakara, Guru,
Madhura, Pavana nashaka. It is responsible for excessive Kledatva in Dosha, Dhatu, Mala
and Srotas. Thus, producing favorable conditions in the body for various diseases
(Ch.Su.27, Su.Su.46). Excessive Kledatva is imparted to Mutra, there by allowing the
vitiated Dosha to be lodged in it and results in various conditions of Mutraghata where
Kleda or Kapha is predominant compared to Vata dosha.
Consuming foodstuffs before ingested food gets digested is known as
Adhyashana. Due to this Ajeerna and Agnimandya takes place and ultimately resulting
into Ama formation. Further it can result into the formation of unmetabolized end
products and reaches to Mutravaha srotas, where they cause different Mutra rogas
including Vatashtila.
Discussion 142
VIHARAJA NIDANA
Mutravega sandarana
It is mentioned as one of the most important causative factor in Vatasthila (BPH).
Because Apanavayu is responsible for normal evacuation of urine, is deranged by
voluntary suppression of the urge of micturition if a person indulges for a long period of
time. This brings about vitiation of Vata to the extent that it results in Vatashtila. The
concept of Vata is analogus to that of nervous system in its functional aspect and is
presented in the study with respect to reflex mechanisms and functioning of the bladder.
The bladder is influenced by conditions that alter the membrane threshold and can
predispose it to either hypoactivity or hyperactivity, and it is tempting to speculate that
the propensity for spontaneous activity contributes in part to detrusor muscle instability
or Hyperreflexia. Suppression of urges routinely disturbs normal biochemical and
biophysical properties of body cells. Aggravated vata due to its suppression infiltrates
inside the Sushira Snayu, Sira and Dhamani of Basti and make them loose so that they
cannot contract during the urge of Mutra and thus urine cannot be voided out.
Nitya druta Prushtha yana, Ati Stree sevana
Continuously sitting over vehicles or continuously traveling over the vehicles
induces the mechanical pressure over the prostate and bladder and moreover those
persons tend to suppress the urge of urine there by vitiate Mutravaha Srotas. During the
urge of urine if a person involves in intake of food or drink or indulging in sexual
intercourse (Mutritasya Udaka, Bhakshya) it may loosen the bladder sphincter and
leads to production of Irritative symptoms. It will produce retrograde ejaculation (Mutra
Shukra), which indicates the Karmatah Viparyaya of Apana Vata.
Discussion 143
Ati vyayama , chankramana, and baravahana
Excessive Vyayamadi leads Datu, Ojah khsaya, because one should have do half
of his body strength other voice it will Vataprakopa result of Datu-kshaya etc.
Poorva janma papas
This is by Astrological if horoscope shows Shani (Saturn) and Rahu in seventh
house, the person is likely to suffer from dysuria, it is very difficult to correlate this
nidana in the manifestation of disease as such there are no psychological reasons
observed for the development of the disease.
Etiological Factor For BPH
Excessive increase of body weight by the accumulation of adipose tissue. This
adipose tissue is the main source of aromatization of testosterone to estrogen and this
estrogen is abundantly found in hyperplastic prostatic cells. Hence obese persons are
more risky to develop BPH. Beef, higher milk consumption and lower consumption of
green and yellow vegetables, NIDDM, Hypertension, Tallness, Obesity, and high insulin
and low HDL cholesterol levels are risk factors for BPH. The etiological factors of BPH
are uncertain even though intense research on various histological, hormonal and age
related changes were going on. Androgens, Estrogens, stromal-epithelial interactions,
growth factors and neurotransmitters may play a role, either singly or in combination, in
the etiology of the hyperplastic process.
Testosterone, the male hormone, is at its peak during adolescence. It decreases
thereafter, and the rate of decrease sharpens by about age 50. This in some ways is the
male equivalent of menopause. The decline in testosterone production typically calls into
play the compensatory release of other hormones, which are stimulants to testosterone
Discussion 144
production. These cannot prevent the decline in testosterone levels, but they can lead to
an elevated rate of transformation of testosterone into di-hydrotestosterone (DHT) and/or
to the increased binding and/or to the decreased clearance of DHT from prostate
cells. This reminds us about the Acharya's view about the depletion in the Shukra dhatu
(Androgens) of aged individuals. Ayurvedic virtuoso have explained completely about
the etiological factors but it is need of the hour to explore these factors with justifiable
and correct reasoning.
In this clinical trial most of the patients had given the history of Mutravega
dharana, Constipation, Teekshna ahara, Nitya Druta Prushta Yana. Some patients have
given the history of Ati Vyayama, Ajeerna, and Alcohol-Tobacco-Tea/Coffee intake.
Samprapti and Etiopathogenesis of Vatashtila (BPH)
Age factor and Nidana are the causes for the deformity (i.e.Khavaigunya) and
restrain Shaithilya in the structures of Basti i.e. Sira, Snayu and Mansa and at another
facet it aggravates Vata dosha. This aggravated Vayu i.e. Apanavayu settles in vitiated
structures of Guda and Basti and interacts with them. Finally the obstruction occurs by
Deergha varthulakara granthi, which causes the Bahirmargavarodha and it leads to
manifestation of lakshanas.
In case of Ashthila, manifestation of an enlarged mass is seen in between the
bladder and the rectum, giving rise to obstruction to urine, feces, and flatus. It is
important to note that, a stony hard mass is found in the carcinoma of prostate. As per my
hypothesis Vatashtila is not having hard consistency. But, in early stage it soft in future
when it becomes hard in consistency may leads to carcinoma of prostate.
Discussion 145
SYMPTOMS
Ashtilavat ghana granthi, Malasanga, Mutrasanga, Anilasanga, Adhmana.
Sashulayoukti Mutratyaga, Incomplete emptying, Increased frequency, Intermittency,
Urgency, Weak stream, Staring Nocturia are the symptoms found in Vatashtila.
BPH mainly consists with the symptoms like incomplete emptying, increased
frequency, intermittency, weak stream, staining, and Nocturia. Hence, there is much
similarity in symptomatology of BPH & Vatashtila. The other symptoms like Adhmana,
(Distention of abdomen) Malasanga, (Constipation) Anilsanga (Obstruction to the Flatus)
are because of Margavarodha by Ashtilavath Ghana granti.
The obstruction induced changes in detrusor function, compounded by age related
changes in both bladder function and nervous system function, lead to urinary frequency,
urgency and nocturia, the most bothersome BPH related complaints.
AYURVEDIC LINE OF MANAGEMENT
Treatments modalities mentioned for Mutrakricchra, Udavarta, Ashmari can be
used to treat Mutraghata. Avapeedaka sneha prayoga, Snigdha virechana, Trividha basti,
Avagaha Swedana, etc are explained. Rasayana and Vajeekara treatments are indicated.
Especially Vrishya drugs have to be advised in the management of BPH as because of
Prostate belongs to reproductive system. There is decrease in androgen level leads to the
proliferation of stromal and epithelial cells of the prostate. Shatavari, Gokshuru, Shilajatu
are some of the drugs which are extensively explained in the management of Mutraghata
that suggests the role of Vrishya and Rasayana drugs. Trivanga is also very useful. Food
is the main cause for both 'ease' and 'disease'. These foodstuffs need proper conversion
(Agni) to their elemental form for nourishment of dhatus for which a media is required
which is called as Srotas. Pathya is that one which is wholesome to body and Apathya is
unwholesome to Srotas. Hence detailed Pathyapathya is explained.
Discussion 146
MODERN LINE OF MANAGEMENT
Treatment should be always concentrating on relieving LUTS, Decreasing BOO,
Improving bladder emptying, Ameliorating detrusor instability, Reversing renal
insufficiency, Preventing future episodes of gross haematuria, Urinary tract infection, and
Urinary retention.
Medical therapies investigated for BPH include α−adrenergic blockers, androgen
suppression, aromatase inhibitors, and plant extracts, which are also reviewed. Because
these agents are widely used in some parts of the world despite the lack of properly
designed clinical trials. Because plant extracts are not classified as drugs, the marketing
and claims are not critically scrutinized by regulatory agencies.
The enthusiasm for medical therapy has been supported in part by the limitations
of Prostectomy, which include the morbidity of the surgical procedure, failure to
consistently achieve a successful outcome, necessity for re-treatment, and the suggestion
that prostatectomy increase the risk of delayed life-threatening cardiac events (Lepor,
1993). Because the indication for intervention in the overwhelming majority of patients
with BPH is to improve quality of life by reliving symptoms (Mebust et al, 1989), the
lower morbidity of medical therapy is of paramount importance in patient driven
treatment decisions.
Acharyas suggested to Avoid the causative factors, increasing the power of
digestion and metabolism, Apanavata anulomana, increasing the stability of Mutravaha
Srotas and particularly of Basti, removes the Sanga (Obstruction), Reducing the Vriddhi,
Protects the Basti marma and makes proper flow of Urine, following proper diet and
regimens may be the 10 principle to manage the Vatashtila (BPH). These principles
supersedes in the management of BPH more than modern medical science.
Discussion 147
DISCUSSION ON CLINICAL STUDY
The patients were selected from the medical camps conducted in the premises of
Shri. D. G. Melmalagi Ayurvedic Medical College and Hospital Gadag. Vatashtila
patients were diagnosed and selected for the clinical study between the age groups 50 to
70 years for the purpose of administration of Matrabasti and shamana Snehapana.
All the patients for the study are randomly selected and categorized in to two
groups. In Group A Matrabasti and Shamana Snehapana in Group B the yoga selected is
Sukumara Kumara Ghrita i.e. for both groups. Matrabasti with 70 ml of Sukumara
Kumara Ghrita was given for 8 days and 16 days was for follow up, where as for
Shamana Snehapana 16 days with same Ghrita was given and 8 days follow up. Total 24
days was the study duration.
DISCUSSION ON OBSERVATIONS
Age – Higher incidence of BPH was found in the age group of 66–70 years (15
patients i.e.50%) followed by 7 patients (i.e.23.33) in 61-65 years of age, 6 patients
(i.e.20%) were belonging to the 56-60 years of age group and remaining 2 patients
(i.e.6.66%) were in to age group of 50-55 years.
This reveals that the disease, which afflicts the aged males, supports the view of
an increasing agglomeration of 5-α−reductase due to an age related shift in Prostatic
androgen metabolism. Age play an important role in the manifestation of BPH and
according to Ayurveda, Vata dominates in this period and hence elders are more likely to
suffer from Vatashtila (BPH).
Religion – In this study maximum number of patients (27 patients i.e.90%)
belonged to Hindu religion an remaining 3 patients (i.e.10%) were in Muslim
community.
Discussion 148
This reflects the geographical preponderance of this particular region rather than
any specific affinity of the disease with religion.
Occupation – The equal incidence of occupation observed during this study. This
shows that the Vatashtila (BPH) patients are obtained from those vicinity of works where
they tend to suppress the urge of micturition or continuously sitting in one place as well.
Dietetic habit – Maximum number of 17 patients (i.e.56.66%) were vegetarian
and 13 patients (i.e.43.33%) were with mixed diet habit.
Chyou and associates 1993 examined 33 food items in relationship to
Prostectomy associated. Araki and Coworkers (1983) reported increased clinical
diagnosis of BPH in men with higher milk consumption and lower consumption of green
and yellow vegetables. Overall, there is no convincing evidence for any dietic factors to
play a major role in the development of LUTS /BPH.
Vyasana – More incidence of the disease was found in the patients with Tea or
Coffee addiction (12 patients i.e.80%). Followed with smokers (12 patients i.e.40%). 9
patients (i.e.30%) were alcohol abusers and 6 patients (i.e.26.66%) were habituated to
Tobacco chewing.
Caffine present in Tea-coffee and Nicotin present in cigarettes appears to increase
both testosterone and estrogen levels. Alcohol is also the causative factors for BPH by
increasing the plasma testosterone level (Chopra et al, 1973). However in this study all
most all patients were found with habituated to some of habits. Because of small sample
size and stipulated nature of study definite relation of habits can not be taken out.
Viharaja nidanas – 22 patients (i.e.73.33%) were exposed to Ativyayama, 17
patients (i.e.56.66%) were indulging in Mutra nigrahana, 13 patients (i.e.43.33%) were
habituated in Nitya drita pristayana and 4 patients (i.e.20%) were indulging Ativyavaya.
Discussion 149
Vata is the nearest cause for Vatashtila and the present study supports the view.
Because of most of the patients were indulging in Ashukari vata vridhhikara bhavas like
Vegavidharana, etc. Because, suppression of urges routinely disturbs normal biochemical
and biophysical properties of body cells. Nitya Drutaprushta Yana (Continuously sitting
and traveling over vehicles and horses, etc) leads to fatigue and exertion thus vitiates
Vata. Indulging in Ativyayama and Ativyavaya leads to dhatu kshaya and extreme
vitiation of Vata. Ekman suggested that the increase in the fibromuscular stroma is a
result of sexual activity (Ekman,1989). The decrease in sexual ability and frequency of
sexual activity with advancing age, exactly when the prevalence of BPH increases, in fact
might suggest a reverse relationship, namely, a causative effect of BPH on sexual
function (Altwein and Keuler, 1992). These are all the favorable conditions for the
Vatashtila. (BPH)
Nidra – 11 patients (i.e.36.66%) were having disturbed sleep, 10 patients
(i.e.33.33%) were having sound sleep, 9 patients (i.e.30%) patients were habituated to
sleep only at night hours and no patient was accustomed to day sleep.
Nidra Ardha Rogahari, Kshudha Sarva Roga Hari | This famous quotation was
well appreciated in this study. Disturbed sleep habits hampers the metabolic processes
and intern causes dhatukshaya and ultimately results in Vatavriddhi. Apart form this the
majority of the patients were of old age group, hence because of this the sleep habitat is
already affected.
Jataragni – Maximum number of the patients 13 (i.e.43.33%) were having
Mandagni, 11 patients (i.e.36.66%) were having Samagni, 5 patients (i.e.16.66%) were
afflicted with Vishamagni and no patients was observed with Teekshnagni.
Discussion 150
Sarve Roga Api Mandagni Eva Karanam | The famous quotation form Charaka
has been well appreciated in present clinical study. Decreased and disturbed nature of
Jathargni indicates that the patients are having pre-existed state of vikrita doshas and
further it hampers the Bhutagni, Dhatwagni vyapara and altimately results in
malformation of dhatus. Dhatu kshaya strongly reflects in terms of Vata dosha vriddhi.
Vriddhavastha and vikrita avastha of Jathargni makes the more favorable place for
Vatashtila.
Mala Mutra pravritti (Bowel movement) – 13 patients (i.e.43.33%) were
having frequent mala pravritti, 11 patients (i.e.36.66%) were constipated, 5 patients
(i.e.16.66%) patients were having normal bowel movements and only 1 patient
(i.e.3.33%) was having irregular bowel habits. Frequency of Mutra is the criteria for
diagnosis which was present in all patients.
Due to disturbed pattern of mala pravritti shows the pre-existence of vikrit vayu
and it may be due to more enlarged prostate, which causes obstruction to feces.
Prakruti – Equal incidence of Vata-pitta and Vata-kapha prakriti was observed.
This suggests that incidence of BPH may be high in these Prakruti purushas and which
also confirms the predominance of Vatadosha in natural constitution of prakriti itself.
DISCUSSION ON DATA RELATED TO DISEASE
Chief Complaints
The maximum symptoms were present in the age group of 66 to 70 age group and
60 to 65 age group. It seams to be as per incidence of BPH, common problem in who is
men over 50 years of age. Approximately the incidence of BPH is more in fifth decade of
men’s life.
Discussion 151
Prostatic findings – The present clinical study assessed through DRE. Most of
the patients were having median lobe enlargement and border line enlargement and free
from rectal mucosa and tenderness was absent.
Residual Urine – 12 patients each (i.e. 40%) were reported in 10 to 50 cc and 51
to 100 cc of residual urine. 2 patients (i.e.20%) were having 101-200 cc of residual urine.
Whereas, no patient was observed with residual urine above 201 cc.
This is due to fatigue of the altered detrusor during prolonged voiding at higher
than normal pressures and reduced flow. Towards the end of the urination, the detrusor
can no longer maintain sufficient contraction to force the urine, to keep the bladder neck
and prostatic urethra open. Due to the contraction and leaving residual urine in the
bladder. This again dependent upon the Chronicity of the disease.
Size and weight of the prostate
In the present clinical study it was observed that, size and weight of the prostate is
first and second degree.
DISCUSSION ON RESULTS
The results were assessed on the basis of subjective and objective parameters with
individual gradings and discussed as follows –
Subjective Parameter
Effect on I-PSS Index of Vatashtila ( BPH)
Group A – The AUA or I-PSS is having 7 symptoms, all the seven symptoms
were given according to age interval. In the age interval of 50 to 55, among two patients
in one patient observed good response and one patient was poor respond. Where as 56 to
60 age interval among 4 patients, all three patient were observed poor respond. And age
61 to 65 among 3 patients, one patient was not responded, where in rest of two patients
responded poorly. As the age interval of 66 to 70, among 6 patients in only 2 patients has
seen poor respond remaining 4 patients were not responded.
Discussion 152
Group B – In the age interval of 50 to 55, there was no any patients were
reported. Where as 56 to 60 age interval among 2 patients, only one patient was observed
good response and another 1 was patient not responded. And age 61 to 65 among 4
patients one patient was not responded, where in rest of 3 patients responded poorly. Age
interval of 66 to 70, among 6 patients in 3 patients has seen poor respond remaining 3
patients were not responded.
EFFECT ON MALASANGA
Group A – Malasanga was found 2 patients in the age interval of 50 to 55, and
shown good response. 4 patients were in age interval of 56 to 60 years. Among these, 3
patients shown good response and 1 patient was not responded. 3 patients were observed
in the age group of 61 to 65 years. All has shown good response. 4 patients were in the
age interval of 66 to 70 years. Among 6 these 4 patients has shown good response,
remaining 2 patients has shown moderate and poorly response respectively.
Group B – No patient was reported in the age interval of 50 to 55 years. 2
patients were in age interval of 56 to 60 years. Among these 1 patient has shown good
response and another patient was not responded. 4 patients were in the age interval of 61
to 65 years. Among these 2 patients responded good and remaining patients were
responded moderately and poorly respectively. 6 patients were in the age interval of 66 to
70 years. Among these 3 patients each has shown moderate and poor response
respectively.
Discussion 153
EFFECT ON MUTRASANGA
Note : - In Group A, 8 patients were having this symptoms and in Group B, 6 patients were having this symptoms.
Group A – The symptom Mutrasanga in the age interval of 50 to 55, one patient
observed and shown good response. In the age interval of 56 to 60, among 2 patients both
patients shown good respond. In age interval 61 to 65 in among 2 patients one patient
was observed very good response and 1, patient was not responded. As interval of 66 to
70, among 3 patients, 2 patients has seen good responded, one was not responded.
Group B – In the age interval of 50 to 55, there was no any patients are reported.
In the age interval of 56 to 60, among 2 patients, only one patient shown good response,
and another patient was not responded. In the age interval of 61 to 65, among 4 patients 1
patient was responded poorly, and rest of the patients were not responded. In rest other
age interval patients were not reported.
EFFECT ON ANILA SANGA
Note : - In Group B, 14 patients were having this symptoms.
Group A – Symptom Anilasanga in the age interval of 50 to 55, among 2 patients
one patient was responded good, and another one was moderately responded. In the age
interval of 56 to 60, among 4 patients, 3 patients shown good response and 1 patient was
not responded. In the age interval of 61 to 65 in 2 patients 1 was moderately and 1 was
poorly responded. In the age interval of 66 to 70, among 6 patients in 3 patients has seen
good respond, 2 patients were moderately responded and 1 patient was not responded.
Group B – In the age interval of 50 to 55, there is no patients were reported. In
the age interval of 56 to 60 interval among 2 patients, both patient has shown poor
response. In the age interval of 61 to 65, among 4 patients all patients responded poorly.
In the age interval of 66 to 70, among 8 patients in 1 patients has seen good respond, 5
patients responded poorly and 2 patients were not responded.
Discussion 154
EFFECT ON ADHMANA
Note : - In Group B, among 15 patients 14 patients In Group A – Symptom Adhmana in the age interval of 50 to 55, among 2
patients each patient has shown good and poorly response. In the age interval of 56 to 60,
among 4 patients, 2 patients has shown good response and 2 patients are poorly
responded and in the age interval of 61 to 65, 2 patients responded poorly. In the age
interval of 66 to 70, among 6 patients 2 patients has shown good response and 1 patients
has seen moderate respond and 2 patients were poorly responded and only 1 patient was
not responded.
Group B – In the age interval of 50 to 55, there was no any patients are reported.
In the age interval of 56 to 60, among 2 patients each patient has shown poor and
moderate response. In the age interval of 61 to 65, among 4 patients 3 patients were
poorly responded, 1 patient has shown good response. In the age interval of 66 to 70,
among 8 patients in 5 patients are poorly responded and 3 patients were not responded.
EFFECT ON RUJA/SASHOOLYUKTA MUTRA TYAGA
Note : - In Group A, 11 patients were having this symptoms and in Group B, 10 patients were having this symptoms.
Group A – The Symptom Ruja / Sashoolyukta mutra tyaga, in the age interval of 50
to 55, 1 patient observed and shown good response. In the age interval of 56 to 60, among
3 patients 2 were patients observed good response and 1 was poorly responded. In the age
interval of 61 to 65, among 2 patients 1 patient was observed good response and 1 patient
was poorly responded. As interval of 66 to 70, among 5 patients in 3 patient has shown
poor response and other 2 patients were not responded.
Group B – In the age interval of 50 to 55, there is no any patients are reported. In
the age interval of 56 to 60, among 2 patients, both are not responded. Where age 61 to
65, among 2 patients no one has responded, In the age interval of 66 to 70, among 6
patients 3 patients were good responded and 1 is poorly responded rest of other 2 patients
were not responded.
Discussion 155
OBJECTIVE PARAMETER
SIZE OF PROSTATE
Group A – There was no response observed except age interval of 66 to 70, only
1 patient was observed and responded good.
Group B – There was no response observed in Group B.
UPPER BORDER
Group A – There is no response observed except age interval of 66 to 70, only 1
patient was observed and responded good.
Group B – There was no response observed in Group B.
MOBILITY
There was no response observed in Group A and B.
RESIDUAL URINE
In Group A – In the age interval of 50 to 55, among 3 patients only 1 patient was
responded moderately and 2 patients were not responded. In the age interval of 56 to 60,
among 4 patients, 1 patient has responded good, 2 patients were poorly respond and 1
patient was not responded. In the age interval of 61to 65, among 3 patient 1 patient was
responded good, 2 patients were poorly responded. In the age interval of 66 to 70, among
5 patients only 2 patient good respond, 3 patients were poorly responded.
In Group B – In the age interval of 50 to 55 there was no patients reported. 56 to
60, among 3 patients 1 patient was responded good. In the age interval of 61to 65 among
5 patients 2 patient were responded and 2 patients were not responded. In the age interval
of 66 to 70, among 7 patients only 1 patient poorly responded, remaining all patients
were not responded.
Discussion 156
WEIGHT OF PROSTATE
In Group A – In the age interval of 50 to 55, among 2 patients only 1 patient was
responded moderately and 1 patients was not responded. In the age interval of 56 to 60,
among 4 patients 1 patient responded good, 3 patients were poorly respond. In the age
interval of 61 to 6, among 3 patient, 1 patient was responded good, 2 patients were
moderately responded. In the age interval of 66 to 70, among 4 patients, 2 patients each
responded good and poor.
In Group B – No patient was responded.
STATISTICAL DISCUSSION
In statistical analysis by comparing the two groups, only incomplete emptying of
bladder was significant i.e. the mean effect of incomplete emptying is not same in the two
groups after the treatment (i.e. p value is <0.05). But individually the performance of
Group A is more effective in the all the parameters (by comparing p values). The
parameters incomplete emptying, urgency, straining, and nocturia, were more significant
in Group A then Group B (by comparing t value). The parameter weak stream was not
significant in Group B (i.e. p value is >0.05). In Group B, the mean effect after the
treatment is more than Group A, but in the Group A the variation or the S.D. is very less
in all the parameters. There is no uniform effect in the all the parameter of both Groups.
We can also observe the mean net effect of Group A is more than Group B before and
after the treatment. Hence, Group A is more effective, (by comparing mean, variance, and
co-efficient of variation).
Discussion 157
In the subjective parameter except Malasanga and Anilasanga shows not-
significant. When the mean effect of the two groups, but the objective parameters weight
of the prostate and residual urine shows non-significant in the mean effect of the two
groups after the treatment individually the Group A shows more significant then Group B
in the parameter of weight of the prostate and residual urine, but the parameter weight of
the prostate is not-significant in Group B.
Overall Response to the treatment
Assessment of response was done on the basis of subjective and objective
parameters after recording the baseline pre and post treatment data of Mala, Mutra,
Anilasanga, Adhmana, Sashoolayukta mutratyaga and AUA symptom score index in
gradings. (Mentioned in methodology). The statistical analyses of the subjective and
objective parameters were made for overall result assessment.
The role of Sukumara Kumaraka Ghrita, in Vatashtila (BPH)
Sukumara Kumaraka Ghrita has been selected for the clinical study because of the
direct indication of the yoga towards Mutrakricchra in the textbook of Chakradutta and
Bhaishajya ratnavali.
It contains Dashamoola, Trinapanchamoola, Punarnava, Vidarikanda, Nagabala
and Atibala are having properties like Mutrala, Mutrakricchrahara, Ashmari bhedana,
Shothahara, Shoolahara and Vata-kaphahara.
Dashamoola is having Ushna veerya and hence Vata-kapha shamaka. It is very
good Vedana sthapaka, normalizes the obstructed Gati of Vata dosha by other Dosha or
by Mala. It is used in Shwayathu. It is more beneficial in Apanavata vaigunya.
Discussion 158
Shatavari, Bala, Ashwagandha, and Ghrita are having properties like Mutrala,
Vata-pittahara, Vatanulomana, mainly Vrushya, Balya, Rasayana, Vatanulomana.
Ashwagandha is specially indicated in Vridda. (Aged person)
Pippali, Ajamoda, Shunti, Yavani are having Agnideepana, Vatanulomana
Shoolahara.
Saindhavalavana increases the Vishyandana property of Bastidravya there by
enhances the absorption rate and alleviates Vatadosha. Eranda taila is Mridu virechaka
and Vatanulomaka. The name itself indicates, it is recommended for Sukumaras viz. old
age persons without any hesitation.
Gokshura is having the 5-α reductase inhibitory, α−andrenergic, antagonistic
activity and reduction in the weight of the testosterone induced prostate. It is also noticed
that it inhibits the stromal proliferation and controls the epithelial height. (Sundaram. R,
and Co; R&D Centre; The Himalaya Drug Co. Bangalore, 1999). It is one of the safe and
famous mutrala dravyas mentioned in classical texts.
Shatavari is known for inhibitory activity of 5-α reductase enzyme, there by
checks the proliferation of prostatic cells. It is Mutrala hence reduces residual urine. Its
Rasayana property increases the stability of Basti and Mutravaha srotas. Madhura rasa
and Vipaka, Sheeta veerya alleviates Pittadosha hence useful in burning micturition.
Sukumara Kumaraka Ghrita indicated in various disease Gulma, Mutrakricchra,
and Shoola etc. It is the best vatahara. (i.e. Apanavata) It can be claimed that it helps in
correcting the pathology of Vatashtila (BPH).
Discussion 159
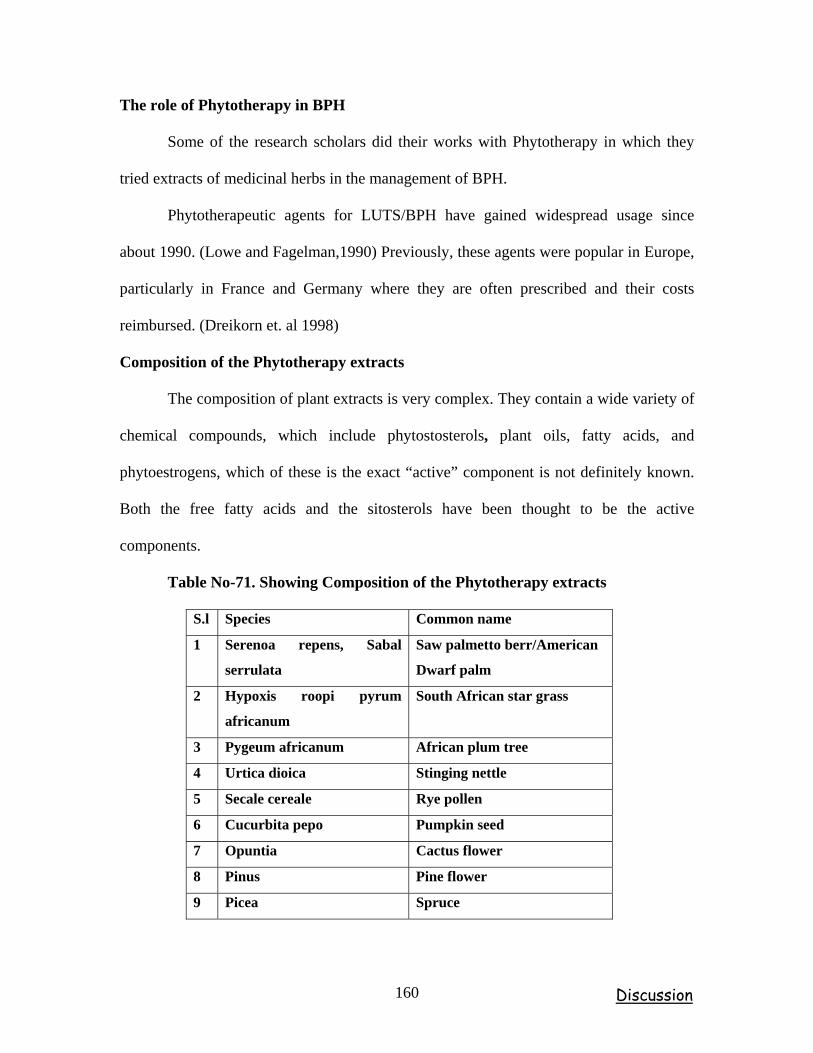
The role of Phytotherapy in BPH
Some of the research scholars did their works with Phytotherapy in which they
tried extracts of medicinal herbs in the management of BPH.
Phytotherapeutic agents for LUTS/BPH have gained widespread usage since
about 1990. (Lowe and Fagelman,1990) Previously, these agents were popular in Europe,
particularly in France and Germany where they are often prescribed and their costs
reimbursed. (Dreikorn et. al 1998)
Composition of the Phytotherapy extracts
The composition of plant extracts is very complex. They contain a wide variety of
chemical compounds, which include phytostosterols, plant oils, fatty acids, and
phytoestrogens, which of these is the exact “active” component is not definitely known.
Both the free fatty acids and the sitosterols have been thought to be the active
components.
Table No-71. Showing Composition of the Phytotherapy extracts
S.l Species Common name
1 Serenoa repens, Sabal
serrulata
Saw palmetto berr/American
Dwarf palm
2 Hypoxis roopi pyrum
africanum
South African star grass
3 Pygeum africanum African plum tree
4 Urtica dioica Stinging nettle
5 Secale cereale Rye pollen
6 Cucurbita pepo Pumpkin seed
7 Opuntia Cactus flower
8 Pinus Pine flower
9 Picea Spruce
Discussion 160
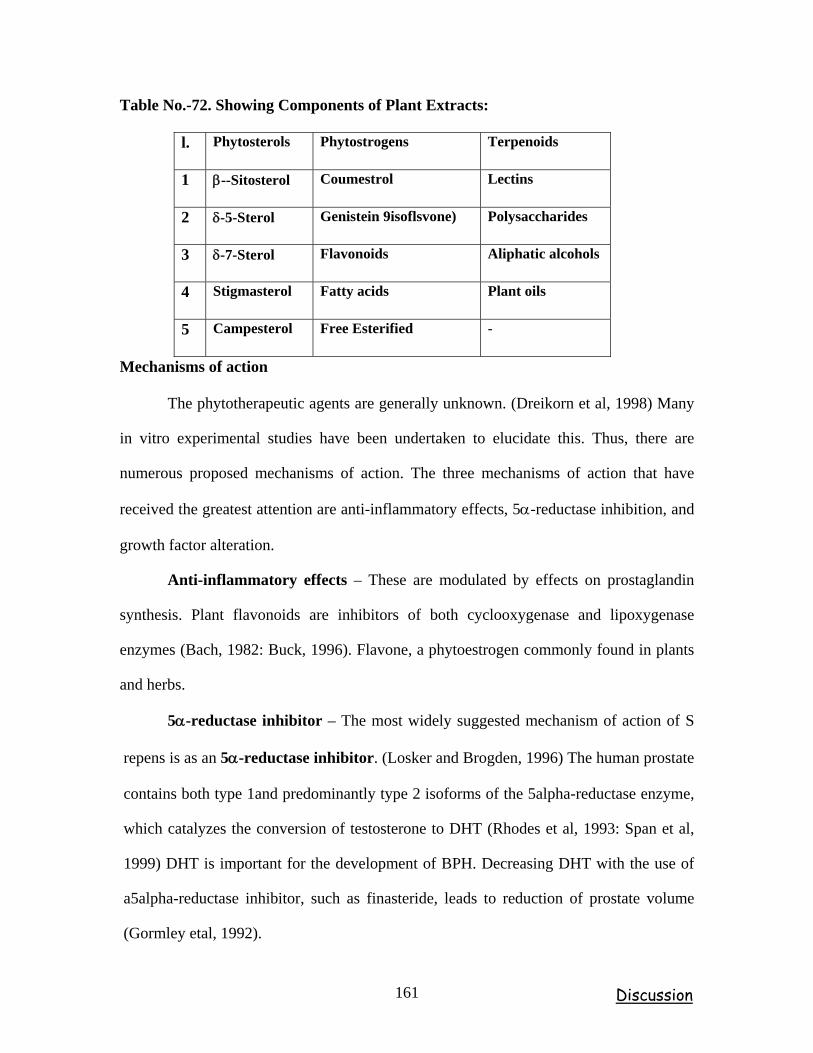
Table No.-72. Showing Components of Plant Extracts:
l. Phytosterols Phytostrogens Terpenoids
1 β--Sitosterol Coumestrol Lectins
2 δ-5-Sterol Genistein 9isoflsvone) Polysaccharides
3 δ-7-Sterol Flavonoids Aliphatic alcohols
4 Stigmasterol Fatty acids Plant oils
5 Campesterol Free Esterified -
Mechanisms of action
The phytotherapeutic agents are generally unknown. (Dreikorn et al, 1998) Many
in vitro experimental studies have been undertaken to elucidate this. Thus, there are
numerous proposed mechanisms of action. The three mechanisms of action that have
received the greatest attention are anti-inflammatory effects, 5α-reductase inhibition, and
growth factor alteration.
Anti-inflammatory effects – These are modulated by effects on prostaglandin
synthesis. Plant flavonoids are inhibitors of both cyclooxygenase and lipoxygenase
enzymes (Bach, 1982: Buck, 1996). Flavone, a phytoestrogen commonly found in plants
and herbs.
5α-reductase inhibitor – The most widely suggested mechanism of action of S
repens is as an 5α-reductase inhibitor. (Losker and Brogden, 1996) The human prostate
contains both type 1and predominantly type 2 isoforms of the 5alpha-reductase enzyme,
which catalyzes the conversion of testosterone to DHT (Rhodes et al, 1993: Span et al,
1999) DHT is important for the development of BPH. Decreasing DHT with the use of
a5alpha-reductase inhibitor, such as finasteride, leads to reduction of prostate volume
(Gormley etal, 1992).
Discussion 161
Growth factor alteration – These are also thought to act by altering growth
factor-induced growth and proliferation. Although experimental data have suggested
numerous possible mechanisms of actions for the phytotherapeutic agents, it is uncertain
which, if any, of these proposed mechanisms is uncertain which, if any, of these
proposed mechanisms is responsible for the clinical responses.
Observations of Matrabasti Procedure
The treatment given to Group A i.e. Matrabasti patients with Sthanika mridu
abhyanga with Murcchita Tila taila and Sthanika swedana was done prior to Matrabasti.
Patient was advised to take alpa ahara before Matrabasti karma. The procedure is
followed consecutively for 8 days.
In severely constipated patients Tab Anuloma DS was given for 2 to 3 days. No
complications were observed in all the patients during and after the Matrabasti procedure.
Basti was administered in between 9 to 10.30am. In 13 patients retention of bastidravya
was up to 5 to 9 hours and in 2 patients it was retained for 2 to3 hours. Basti pranidhana
and Pratyagamana kala were recorded properly. During the course of therapy some
patients showed improvement in both obstructive and irritative symptoms i.e. incomplete
emptying of the bladder, increased frequency and urgency. Some patients showed marked
improvement during and after the treatment which was recorded in proforma of I-PSS
Index. Other symptoms like Constipation, were relieved in most of the patients. Addition
to that patients were relived from Durbalata and body aches, attained Indriya prasannata,
Chaitannya, even.
Discussion 162
Mode of Action Matrabasti
Vatashtila, a clinical entity wherein there is extreme vitiation of Vata
especially the Apanavata, which being sheltered in the Basti and Medhra leads to
obstruction to the outflow of urine due to its Vimargagamana and Margavarodha.
Therefore, the main principle of management should be Margashodhana and
Vatanulomana in order to restore the normal functioning of Apanavata. The ingredients
of Sukumarakumar Ghrita are well known for their Kapha-vatahara, Vatanulomana,
Shothahara, Bastishodhana, Balya and Rasayana effects.
Matrabasti is best treatment for old age persons, because of its less dose and
minimum complications. The drug of Matrabasti is sneha, it is perfectly antagonistic to
the Vata, as the disease Vatashtila is vata pradana vyadhi (Apanavata). Apanavata is
prime cause for the disease, as Moola of Vata is Pakvashaya (apanavata) the Sanchara
Sthana of Apanavata is Apano apanaga shroni basti medhrorugocharaha. The
administered Basti dravya stays in pakvashaya and it will reach to the affected area
quickly by the Anupravaranabhava. In the disease Vatashtila, structurally Affected area
is Guda and Basti pradesha which is near to the Pakvashaya.
The Srotases of a Ruksha and Klanta persons (old aged Vatapradhana person) are
emaciated therefore there will be natural obstructio and n to the movement of Vata to
bring about normal functions. As explained earlier, the Sneha brings about
Srotomardavatwa and Vatashamana actions thereby causes Srotoprasadana and helps for
proper movement of Vata.
Discussion 163
From the foregoing description it may be inferred that on per-rectal
administration, the medicaments are absorbed through the villi of the rectal mucosa and
then come into the vein and then into circulation after proper metabolism. This rectal
route is also mentioned in allopathic system of medicine as the important systemic route
of administration for some drug in the form of retention enema. Drugs, absorbed into
external haemorrhoidal veins (about 50%), bypass the liver, while the drugs, absorbed
into internal haemorrhoidal veins come into portal circulation.
As the Matrabasti quantity is less, it can stay 5 to 9 hours in Pakvashaya, and
may acts locally or systemically after absorption of active principles from Basti dravya.
Guda is pradhana marma and the moola of Siras, that nourishes the body.
The rectum has rich blood supply and drugs can cross the rectal mucosa like other
lipid membranes. Thus unionized and lipid soluble substances are readily absorbed from
the rectum and from rectal venous plexus. The concentration gradient of Basti dravya is
more inside the lumen of intestine as compared to rectal venous plexus, which facilitates
the absorption. This rectal venous plexus further divided into internal venous plexus and
external venous plexus. Internal venous plexus, situated in the submocosal layer of anal
canal and carries into superior rectal vein and to external venous plexus.
Basti dravya is also absorbed from external venous plexus in three parts, i.e. in
lower part through inferior rectal veins and drained into internal pudendal vein, in middle
part through middle rectal vein which is having tributaries, those drains from bladder,
prostate and seminal vesicle into internal iliac vein, in upper part through superior rectal
vein into inferior mesenteric vein a tributary of portal vein.
Discussion 164
Basti dravya is also absorbed from the upper rectal mucosa, and is carried by the
Superior mesenteric vein into the portal circulation and enters into Liver. Secondly, the
portion absorbed from the lower rectum enters directly into systemic circulation via
middle and inferior hemorrhoidal veins. This indicates that due to more vascularity in this
area absorption rate is high. Acharyas also said that Guda (Uttara Guda) is the moola of
Sira.
From above it is clear that Basti dravya is absorbed through rectal mucosa either
by chemically altered or un-altered and carried throughout the general circulation and
gives systemic effect along with local effects like Vatanulomana, Mutravirajaneeya and
Shoolahara, etc. The ingredients of Sukumara Kumaraka Ghrita acts on Rakta dhatu
and helps to provide proper nourishment to Sira, Snayu as they are its Upadhatu. Ushna
veerya and Madhura rasa alleviate Apanavayu.
Basti mainly acts on Pakvashaya the Mula sthana of Vata, it subsides vitiated
Vata, By means of its Katu vipaka, Ushna veerya it reduces the size and volume of the
prostate there by decreases the obstruction to flow of urine.
Basti dravya posses Basti vishodhana drugs, it improves the stability and also
compliance of detrusor muscle of the bladder. When Basti dravya reaches in general
circulation it may act on androgens (testosterone) directly or through pituitary there by
controlling leutenising hormone to stimulate Leydig’s cells present in testes and may
reduce the more production or more conversion of testosterone into DHT by inhibiting 5-
alpha reductase enzyme.
Discussion 165
By these factors Basti is responsible for the relief in the signs and symptoms of
the disease. So these observations suggests that this therapy not only attains symptomatic
relief but can also control it quite effectively.
Vatavyadhies are generally correlated with Neurological disorders. Basti acts on
nervous system related to the prostate (Apanavayu) and brings the normal function of the
Apanavata i.e. voiding of urine (micturation process).
By looking in to pathology of BPH, obstruction induced changes in neck of the
bladder function, compounded by age related changes in both bladder and nervous
system, leads to urinary frequency, urgency, and nocturia, which are the most bothersome
BPH related complaints. Matrabasti may act on nervous system (Apanavayu related), and
restores the normal function of the Apanavata i.e. voiding of urine.
It can be Hypothetically concluded that Matrabasti is an effective management for
Vatashtila (BPH) as the present clinical work reveals not only symptomatic relief but
there is also reduction in size and weight of prostate and decrease in the residual urine
and there is decrease in the level of free serum testosterone.
Discussion 166
Observations of Shamana Snehapana Procedure
Group-B was taken for Shamana Snehapana. Patients were advised to take, mridu
bhojana, before night prior to Shamana snehapana. Which is to be taken when the patient
gets hunger i.e. “Anannaha” (morning Tiffin time). Patients were advised to take 15ml of
Sukumarakumara ghrita with Ushnajala as Anupana twice daily for 16th day followed by
Mridu ahara and other Pathyapathya as explained in Snehapana vidhi adhyaya. A
pariharakala of 8 days was given.
The patients asked to report on 24th day counting from the day of commencement
of the treatment. In some of the patients marked improvement observed in chief
complaints during and after the course of therapy, which was recorded as per proforma of
I-PSS Index. Other symptoms like Constipation were relieved in most of the patients. In
addition to that, patients were relived from Agnimandya, Durbalata, body aches and
attained Indriya prasannata, Chaitannya, even.
MODE OF ACTION OF SHAMAN SNEHAPANA
Shamana snehapana, is capable of effective pacification of vikaras, mitigation of
vitiated doshas, balya, revitalizing tendency of shareera and indriya by reaching to
Koshta, Shakha, Sandhi, Marmas quickly. (Ch. Su 13., A.Hr.Su.16/19) Its effect depends
upon the basis of method of administration and ingredients of the dravya being used.
By method of administration - As we are giving Shamana Snehanapana in the
“Anannaha” means without food, when patient is having hunger. In this condition Shrotas
will not be enveloped with kapha, and Sneha will get digested completely, as the
digestive enzymes are strong when the person is in hunger. And spreads all over the body
Immediately. Acts locally or systemically after absorption, by the virtue of active
principles of Sukumara kumaraka ghrita..
Discussion 167
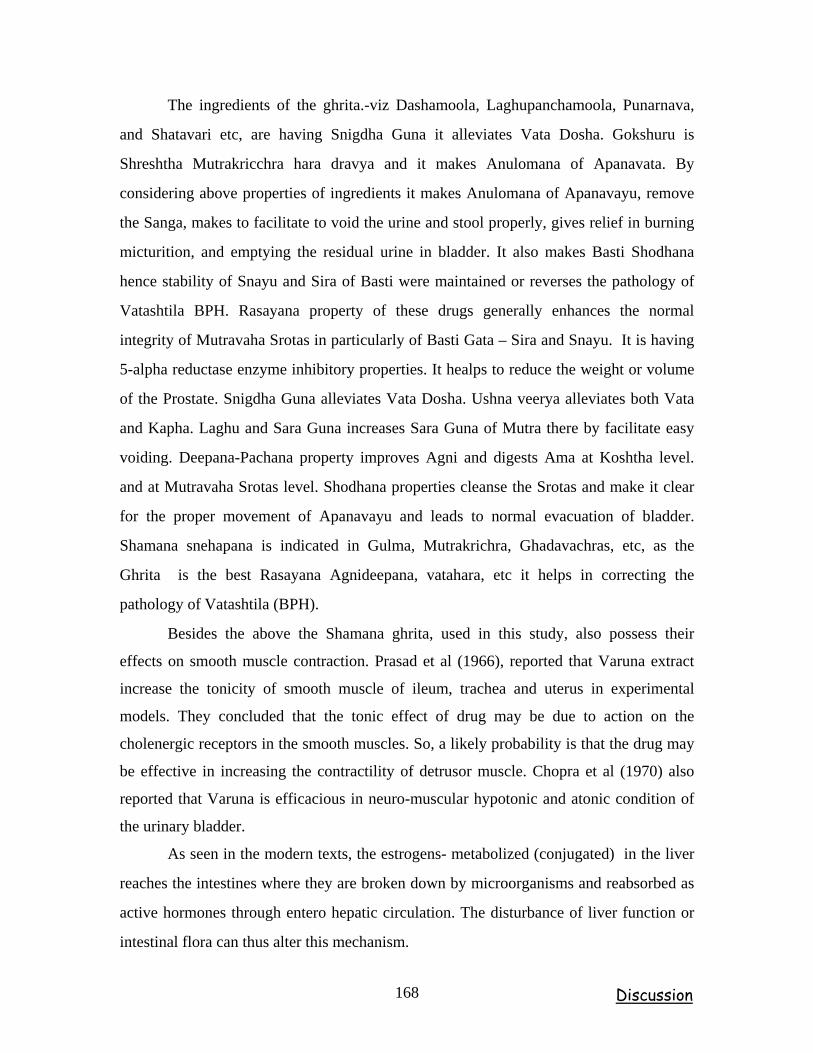
The ingredients of the ghrita.-viz Dashamoola, Laghupanchamoola, Punarnava,
and Shatavari etc, are having Snigdha Guna it alleviates Vata Dosha. Gokshuru is
Shreshtha Mutrakricchra hara dravya and it makes Anulomana of Apanavata. By
considering above properties of ingredients it makes Anulomana of Apanavayu, remove
the Sanga, makes to facilitate to void the urine and stool properly, gives relief in burning
micturition, and emptying the residual urine in bladder. It also makes Basti Shodhana
hence stability of Snayu and Sira of Basti were maintained or reverses the pathology of
Vatashtila BPH. Rasayana property of these drugs generally enhances the normal
integrity of Mutravaha Srotas in particularly of Basti Gata – Sira and Snayu. It is having
5-alpha reductase enzyme inhibitory properties. It healps to reduce the weight or volume
of the Prostate. Snigdha Guna alleviates Vata Dosha. Ushna veerya alleviates both Vata
and Kapha. Laghu and Sara Guna increases Sara Guna of Mutra there by facilitate easy
voiding. Deepana-Pachana property improves Agni and digests Ama at Koshtha level.
and at Mutravaha Srotas level. Shodhana properties cleanse the Srotas and make it clear
for the proper movement of Apanavayu and leads to normal evacuation of bladder.
Shamana snehapana is indicated in Gulma, Mutrakrichra, Ghadavachras, etc, as the
Ghrita is the best Rasayana Agnideepana, vatahara, etc it helps in correcting the
pathology of Vatashtila (BPH).
Besides the above the Shamana ghrita, used in this study, also possess their
effects on smooth muscle contraction. Prasad et al (1966), reported that Varuna extract
increase the tonicity of smooth muscle of ileum, trachea and uterus in experimental
models. They concluded that the tonic effect of drug may be due to action on the
cholenergic receptors in the smooth muscles. So, a likely probability is that the drug may
be effective in increasing the contractility of detrusor muscle. Chopra et al (1970) also
reported that Varuna is efficacious in neuro-muscular hypotonic and atonic condition of
the urinary bladder.
As seen in the modern texts, the estrogens- metabolized (conjugated) in the liver
reaches the intestines where they are broken down by microorganisms and reabsorbed as
active hormones through entero hepatic circulation. The disturbance of liver function or
intestinal flora can thus alter this mechanism.
Discussion 168
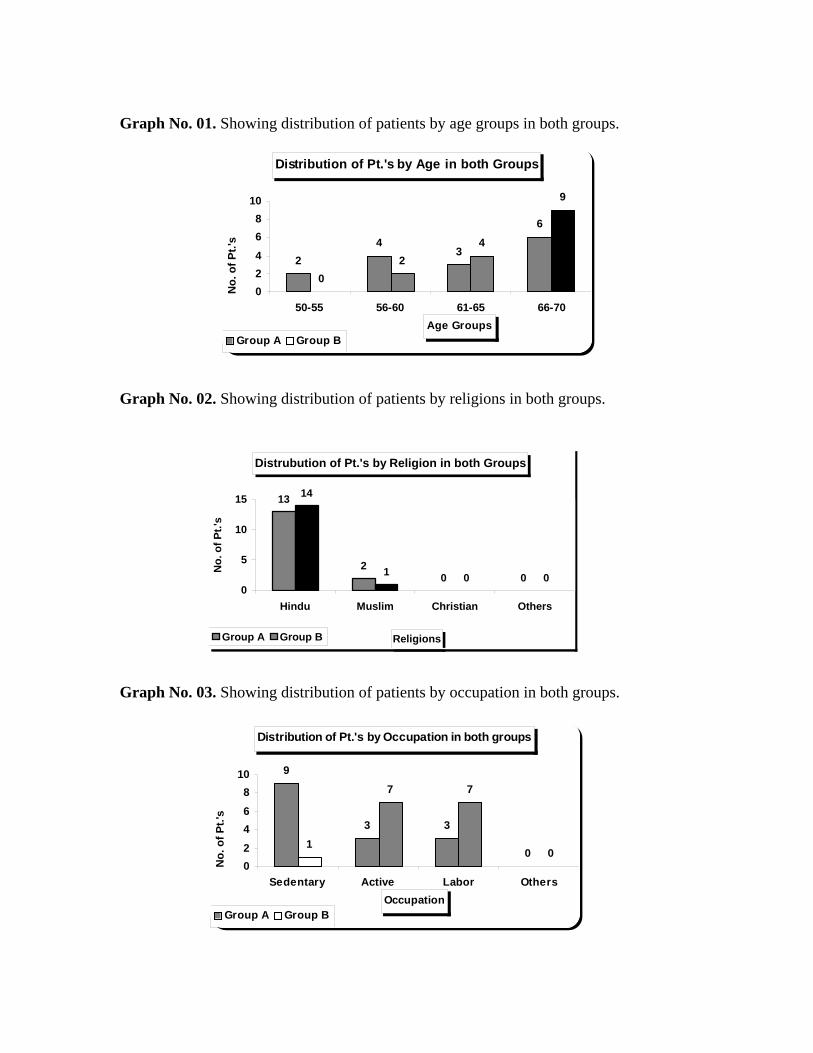
Graph No. 01. Showing distribution of patients by age groups in both groups.
Distribution of Pt.'s by Age in both Groups
24
3
6
02
4
9
02468
10
50-55 56-60 61-65 66-70Age Groups
No.
of P
t.'s
Group A Group B
Graph No. 02. Showing distribution of patients by religions in both groups. Distrubution of Pt.'s by Religion in both Groups
13
20 0
14
1 0 00
5
10
15
Hindu Muslim Christian Others
Religions
No.
of P
t.'s
Group A Group B
Graph No. 03. Showing distribution of patients by occupation in both groups. Distribution of Pt.'s by Occupation in both groups
9
3 3
01
7 7
002468
10
Sedentary Active Labor OthersOccupation
No.
of P
t.'s
Group A Group B
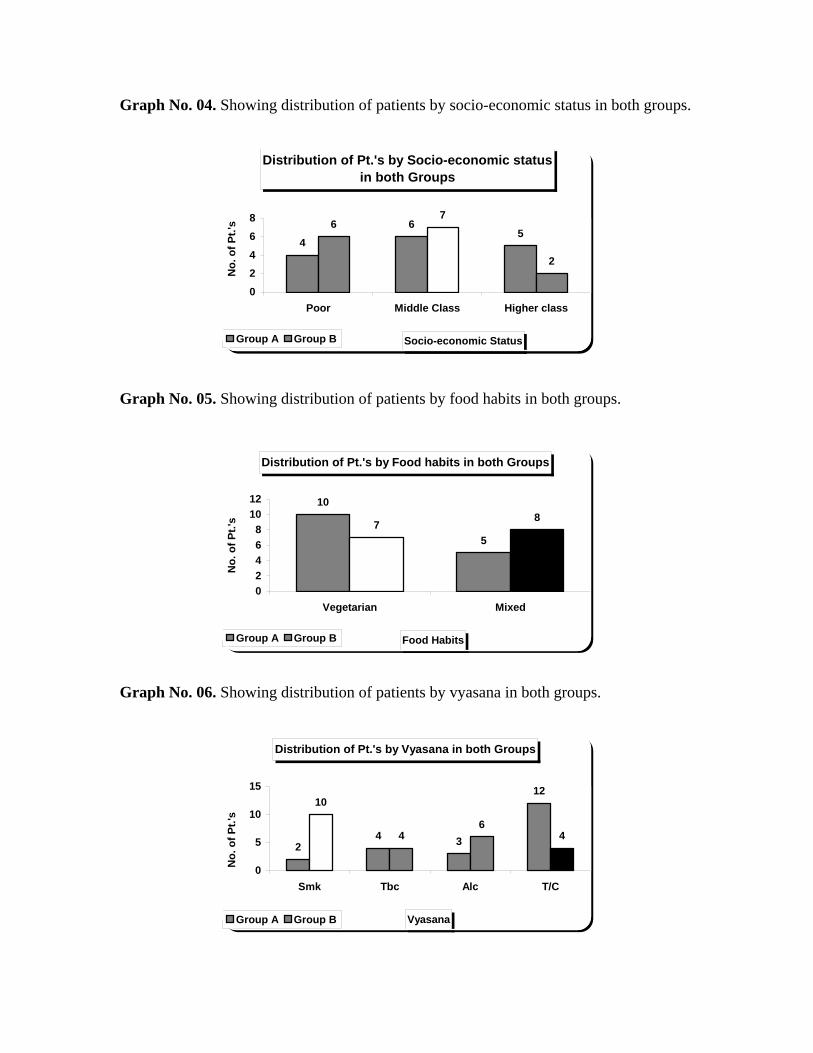
Graph No. 04. Showing distribution of patients by socio-economic status in both groups.
Distribution of Pt.'s by Socio-economic status in both Groups
46
56
7
2
02468
Poor Middle Class Higher class
Socio-economic Status
No.
of P
t.'s
Group A Group B
Graph No. 05. Showing distribution of patients by food habits in both groups. Distribution of Pt.'s by Food habits in both Groups
10
57
8
02468
1012
Vegetarian Mixed
Food Habits
No.
of P
t.'s
Group A Group B
Graph No. 06. Showing distribution of patients by vyasana in both groups.
Distribution of Pt.'s by Vyasana in both Groups
24 3
1210
46
4
0
5
10
15
Smk Tbc Alc T/C
Vyasana
No.
of P
t.'s
Group A Group B
Graph No. 07. Showing distribution of patients by Viharaja nidana in both groups. Distribution of Pt.'s by Viharaja Nidana in both Groups
9
3
8
1313
1
54
0
2
4
6
8
10
12
14
Vy a y Vy a v Dr i t P M u N i
Viharaja Nidana
No.
of P
t.'s
Group A Group B
Graph No. 08. Showing distribution of patients by sleep habits in both groups. Distribution of Pt.'s by Sleep Habits in both Groups
0
54
6
0
4
65
0
2
4
6
8
Day Night Sound Disturbed
Sleep Habits
No.
of P
t.'s
Group A Group B
Graph No. 09. Showing distribution of patients by Jatharagni in both groups.
Distribution of pt.'s by Nature of Jatharagni in both Groups
6
3
0
67
21
5
012345678
M.A. V.A. Tk.A. S.A.
Nature of Jatharagni
No.
of P
t.'s
Group A Group B
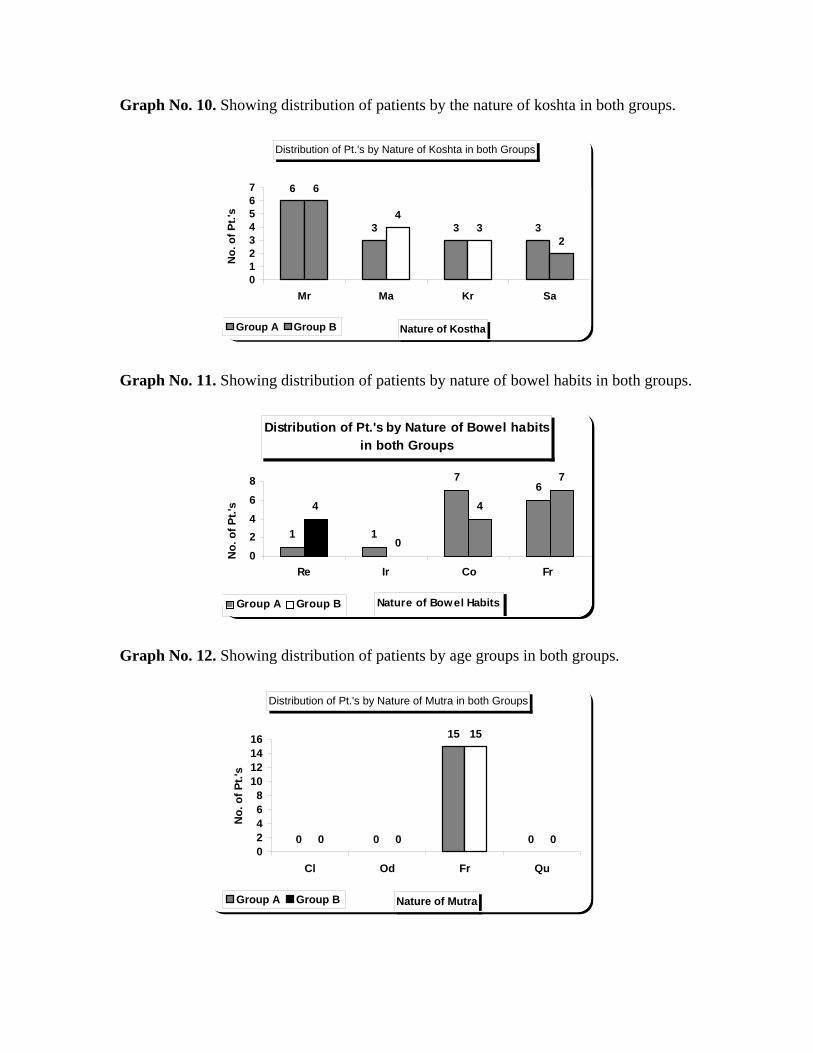
Graph No. 10. Showing distribution of patients by the nature of koshta in both groups. Distribution of Pt.'s by Nature of Koshta in both Groups
6
3 3 3
6
43
2
01234567
Mr Ma Kr Sa
Nature of Kostha
No.
of P
t.'s
Group A Group B
Graph No. 11. Showing distribution of patients by nature of bowel habits in both groups.
Distribution of Pt.'s by Nature of Bowel habits in both Groups
1 1
76
4
0
4
7
02468
Re Ir Co Fr
Nature of Bowel Habits
No.
of P
t.'s
Group A Group B
Graph No. 12. Showing distribution of patients by age groups in both groups. Distribution of Pt.'s by Nature of Mutra in both Groups
0 0
15
00 0
15
002468
10121416
Cl Od Fr Qu
Nature of Mutra
No.
of P
t.'s
Group A Group B
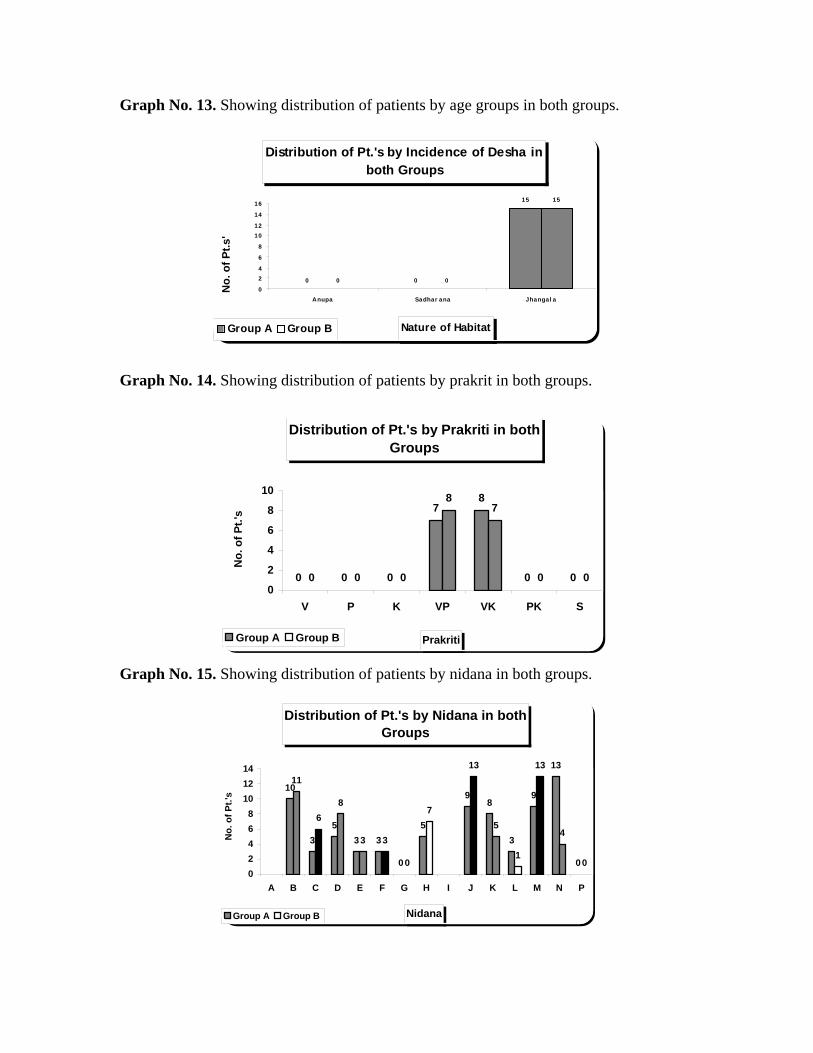
Graph No. 13. Showing distribution of patients by age groups in both groups.
Distribution of Pt.'s by Incidence of Desha in both Groups
0 0
15
0 0
15
0
24
6
8
1012
14
16
Anupa Sadhar ana Jhangal a
Nature of Habitat
No.
of P
t.s'
Group A Group B
Graph No. 14. Showing distribution of patients by prakrit in both groups.
Distribution of Pt.'s by Prakriti in both Groups
0 0 0
78
0 00 0 0
87
0 00
2
4
6
8
10
V P K VP VK PK S
Prakriti
No.
of P
t.'s
Group A Group B
Graph No. 15. Showing distribution of patients by nidana in both groups. Distribution of Pt.'s by Nidana in both
Groups
10
35
3 3
0
5
98
3
9
13
0
11
68
3 3
0
7
13
5
1
13
4
002468
101214
A B C D E F G H I J K L M N P
Nidana
No.
of P
t.'s
Group A Group B
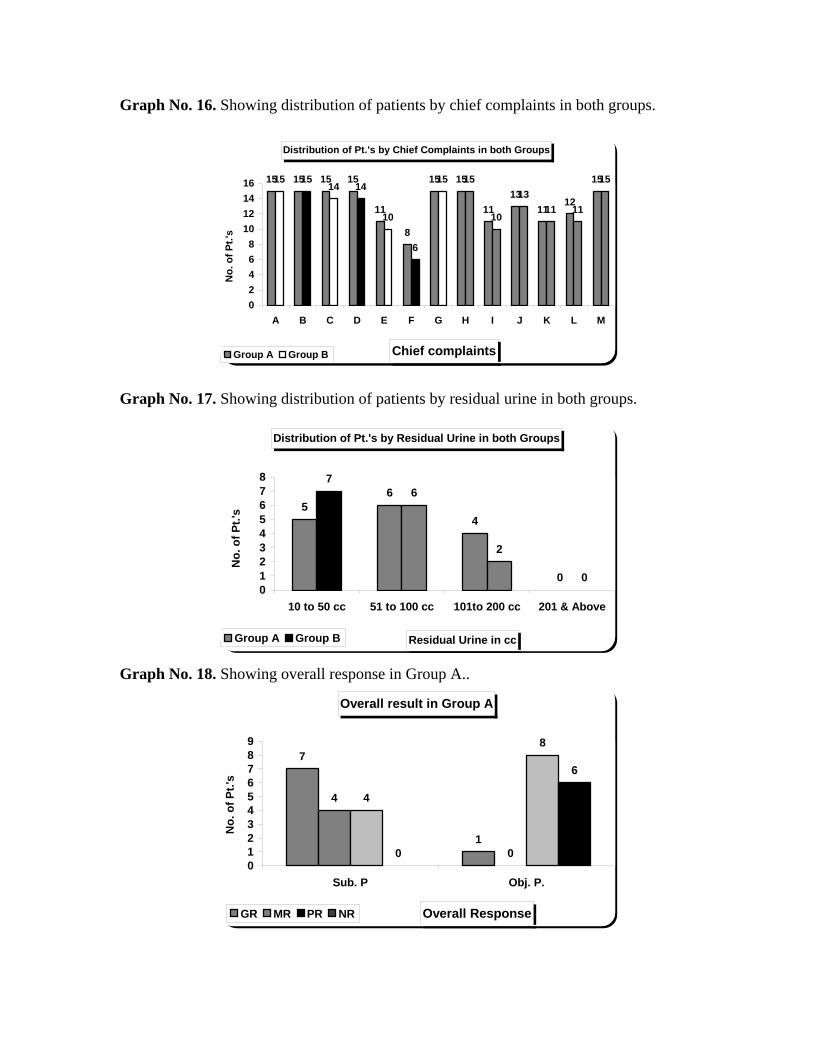
Graph No. 16. Showing distribution of patients by chief complaints in both groups. Distribution of Pt.'s by Chief Complaints in both Groups
15 15 15 15
11
8
15 15
1113
1112
1515 1514 14
10
6
15 15
10
1311 11
15
02468
10121416
A B C D E F G H I J K L M
Chief complaints
No.
of P
t.'s
Group A Group B
Graph No. 17. Showing distribution of patients by residual urine in both groups.
Distribution of Pt.'s by Residual Urine in both Groups
56
4
0
76
2
0012345678
10 to 50 cc 51 to 100 cc 101to 200 cc 201 & Above
Residual Urine in cc
No.
of P
t.'s
Group A Group B
Graph No. 18. Showing overall response in Group A..
Overall result in Group A
7
1
4
0
4
8
0
6
0123456789
Sub. P Obj. P.
Overall Response
No.
of P
t.'s
GR MR PR NR
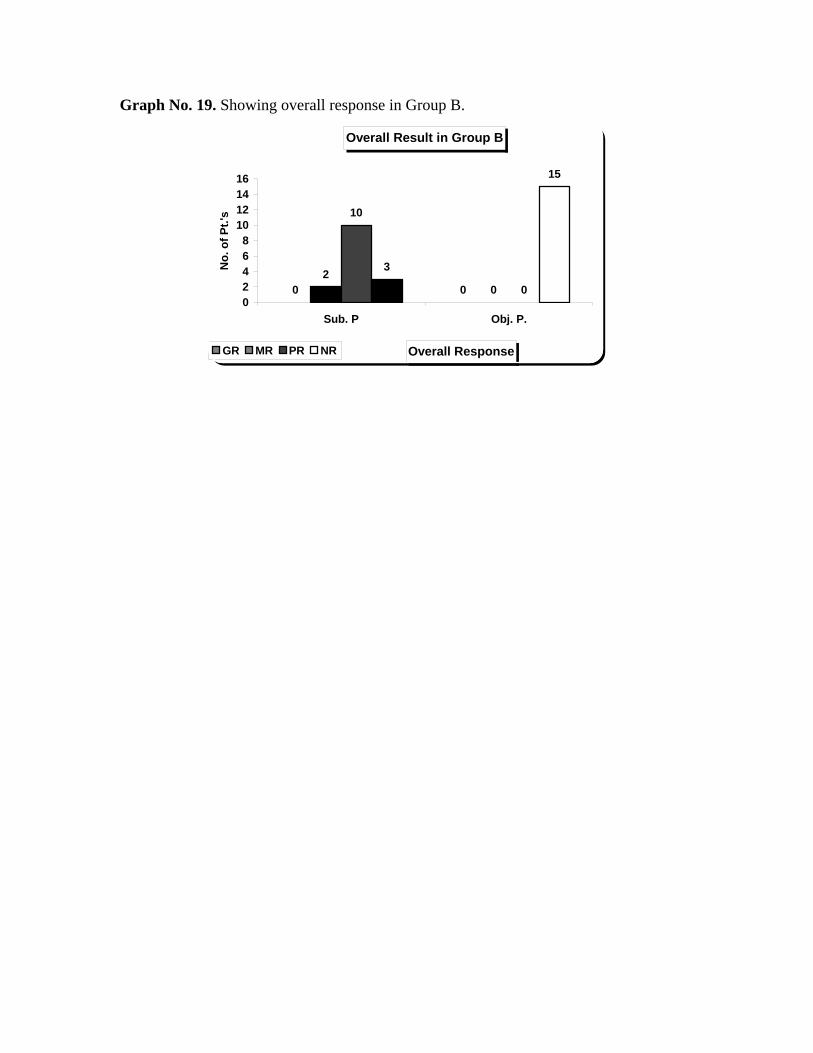
Graph No. 19. Showing overall response in Group B.
Overall Result in Group B
0 02
0
10
0
3
15
02468
10121416
Sub. P Obj. P.
Overall Response
No.
of P
t.'s
GR MR PR NR
CONCLUSION
The long-term exposure to drug induced adverse events and the prohibitive costs
are the primary limitations of prevention therapy.
As there are no clinical, biochemical, or genetic predictors of Vatashtila (BPH)
development or progression, every male is at risk.
A potential role of medical therapy is to prevent the development of Vatashtila
(BPH) or its progression.
The ability to identify those individuals who are predisposed to develop clinical
Vatashtila (BPH) refractory to medical therapy would provide a more compelling
rationale for prophylaxis.
Acute urinary retention is often considered as an absolute indication for medical
intervention, which is related to age, severity of symptoms, and size of prostate
gland. Because urinary retention is a relatively uncommon event, a study designed
to determine whether medical therapy prevents urinary retention would require
large number of patients followed for a long interval of time.
Aim of this therapy is to prevent a relapse of a second episode of urinary retention
after a successful voiding trial. To test the efficacy of the drug therapy for this
indication, patients successfully completing a voiding trial after an episode of
urinary retention would be randomized to active treatment.
The role of treatment for any disease process depends on the magnitude of the
clinical effect and the incidence and severity of treatment related morbidity.
As evident from the present clinical study Vatashtila (BPH) is an ailment of the
ageing male, and is with multifaceted etiology i.e. Vatakara- ahara, vihara, Nithya
Druta Prusta Yana (excess riding /traveling) Mutranigraha, Teekshna oushada and
habits are alcohol consuming, smoking, etc.
The digital rectal examination and neurological examination are done to detect
prostate or rectal malignancy, to evaluate anal sphincter tone, and to rule out any
neurological problems that may cause the presenting symptoms.
I PSS is an ideal instrument to grade baseline symptom severity, and is helpful to
assess the response to the therapy adopted. Which, as a parameter is useful to
Conclusion 168
detect symptom progression in those men managed by watchful waiting. It is not
only meant for the diagnosis of Vatashtila (BPH), but also helpful for the
assessment of a variety of lower urinary tract disorders (e.g. Infection, tumor,
neurogenic bladder disease) in both men and women.
The basic principles of Ayurveda affirms that, the humor Vata dominates with
age by its un unctuousness ( Rukshaguna ), manifestation of Vatashtila (BPH)
will be more. Vata pitta prakruti, Vata kapha prakruti persons are more
susceptible to Vatashtila (BPH) as per the observation of the present study, and
Muslim community is least effected, as these people are with mixed food habits
and when compared with Hindus the extent of dhatu kshaya is not so severe.
After the main treatment (Basti) the follow up the patients are asked to take
Varunnadi kashaya, Shilajatu vati.
It is interesting to detect a reference in “Stadmans Dictionary” regarding female
prostate, and explanation about Para urethral glands in female. asthis reference
makes us to think if any vitiation or derangement of the urethral glands by either
structurally or functionally, it can leads to diseases like urethritis, bulbo urethritis,
where as it is interesting to have thought then “Ashtila or pourusha granthi”
(prostate ) afflictation will take place in female too. In Ayurvedic classics there
is no explanation about female prostate as well as “Ashtila” it needs further
exploration by the scholars of the Ayurveda.
Phytotherapeutic products are also used in modern science’s those are plant
extracts, derived from either the roots, the seeds, the bark, or the fruits of various
plants used. The composition of plant extracts is very complex. They contain a
wide variety of chemical compounds, which include phytostosterols, plant oils,
fatty scids, and phyto-estrogens. which of these is the exact “active” component is
not definitely known. Both the free fatty acids and the sitosterols have been
thought to be the active components.
Statistical enumerations has shown, among all the parameters except incomplete
emptying, are non significant, i.e. comparative effect ( P= <0.05 ). Where as the
objective parameters i.e. weight of prostate, residual urine volume are non
significant, in the comparative effect of two groups. Over all observation of the
Conclusion 169

subjective and objective parameters before and after the treatment, It is evident
even though group-A (Matrabasti) is more significant comparing to group –B
(Shamana.), a satisfactory evaluation of the treatment is possible, if research is
designed with both Shodana and Shamana therapy combined together. And over
all the results observed during the study is encouraging but it needs further
adaptations, diagnostic techniques viz –Prostate specific antigen test, Transrectal
ultra sound, biopsy (to know benign or malignant changes so as to rule out the
malignancy) and hormonal ease, are the standard parameters for the diagnosis as
well as the assessment of Vatashtila (BPH). The taken samples, study duration
and selected criteria for present clinical study may not be sufficient enough for the
better evaluation and treatment of Vatashtila (BPH).
It is observed from this study that, Sukumarakumaraka Ghrita by virtue of its
Balya, Rasayana, Vatahara, Vedanashamaka properties is having a definite role in
the management of Vatashtila (BPH).
I believe that several factors such as aging, the hormonal milieu, nonurologic
diseases, and prostatic growth milieu, nonurologic diseases, and prostatic growth
affect bladder morphometry, neurologic innervations, BOO, and renal function,
and that these factors collectively contribute to clinical BPH. Our present
understanding of the pathophysicalogy of clinical BPH is rudimentary. It is,
therefore, imperative to develop a more comprehensive understanding of the
pathophysiology of symptoms. This knowledge will result in more effective use
of existing therapies and will provide the rationale for the next generation of
therapeutic modalities.
Conclusion 170
SUMMARY
“A Comparative effect of Matrabasti and as Shamana Snehapana with
Sukumara Kumarak Ghrita in the management of Vatashtila (BPH)”
1) Introduction.
2) Review of literature.
3) Methodology.
4) Results.
5) Discussion.
6) Conclusion.
Interest in diseases of Vatashtila (BPH) has always been considerable. In the last
two decades of the 20th century, the interest reached such levels that many important and
valuable studies into this field were carried out, but it was without question the changes
that took place in the treatment of Vatashtila (BPH) that made this work to proceed with
ideal interventional treatment for BPH. The very fact that in the name of “Ashtila or
Pourusha granthi (prostate gland)” has been dealt in such details, in our texts proves
the importance and antiquity of this study. Various measurements for its management
have been advised which only highlights the extent to which this condition was recorded.
Introduction: It has been highlights on panchakarmas, Matrabasti, Shamana
Snehapana, disease of Vatashtila (BPH), Shukumara Kumaraka Ghrita which trial drug of
the study. and incidence, need for study, role of age factor in Vatashtila (BPH).
Objectives of the study: This has explained purpose of the study and objectives
of the study.
Summary 171
Review of literature: This part is described historical review, vyutpatti and
nirukthi of both bastikarma and Sneha, Vatashtila (BPH) The shareera part deals with
both anatomy and physiology related to the Vatashtila (BPH). In the review Basti, the
procedure, types indications and contraindications etc of nirooha, anuvasana etc are
elaborated.
Methodology: This part deals with the administration of Matrabasti and Shamana
Snehapana, ingredients of Shukumara Kumaraka Ghrita and its properties. The study
design, subjective and objective parameters with their gradings and diagnostic criteria,
and criteria for assessment of the parameters are explained.
Observations and Results: This part is dealt in the result section. The
demographic data, response to treatment and overall response are also dealt. Results are
given in the form of tables along with a short description. The improvements in selected
parameters are statistically analyzed and presented in the form of tables and graphs.
Discussion: This part is divided into five sections. Four section entitled- The first
sections discussion on Sharira comparison with prostate gland and disease of Vatashtila
(BPH).The second section discuss about the discussion on analysis of clinical response to
the treatment with logical interpretation study. The third section deals discussion on role
of Sukumara Kumaraka Ghrita in Vatashtila (BPH). Forth section discuss about the
probable mode of action and probable mechanism of Matrabasti and Shamana Snehapana
with Sukumara Kumaraka Ghrita in Vatashtila (BPH).
Summary 172
i
1) Vidhya Ramagopal Shastri,.Vedon me Ayurveda, Chapter 50. Madan mohanlal editor Varanasi : Vishwabharati Anusandhana Parishadh ; 1956. p. 305, 117, 2) Agnivesa, Charakasamhitha Siddhisthana chapter 1-5, 7, 8, 10-12. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. P.No 680-703, 709-715, 734-738. (Kasi Sanskrit series 228). 3) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 35, 36, 37, 38. Varanasi: Krishnadas Academy; 1980. p. 525-548. (Krishnadas Ayurveda series 51). 4) Ashtangasangraha Suthrasthana chapter 28 - Kalpasthana chapters 4, 5, 6, Prof. K.R.Shrikhantamurthy, editor. Varanasi: Chaukhambha Orientalia; 1996. P No. 485, 579-606. (Jaikrishnadas Ayurvedic series 79). 5) Vagbhata, Ashtangahridaya Suthrasthana chapter 19 – Kalpasiddhi chapter 4, 5. Varanasi: Krishnadas Academy; 1982. P No. 270, 753, 763. (Krishnadas Academic series 6) Sharangadhara, Sarngadharasamhitha Utharakhanda chapter 5, 6, 7. 3rd ed. Varanasi: Chaukhambha Orientalia; 1983. p. 318-338. (Jaikrishnadas Ayurveda Granthamala 53). 7) Vangasena, Vangasenasamhitha Bastikarmaadhikara. Jain Sankarlalji Vaidya, editor. Mumbai: Khemnath Srikrishnadas publishers; 1996. p. 952. 8) Vrudhajeevaka, Kashyapasamhita Khilasthana chapter 8 sloka 54. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1988. p. 289. (Kasi Sanskrit series 154).
9) Kapildev Divedi, Vedon me Ayurveda, Chapter 12. 1st edn. Varanasi : Vishwabharati Anusandhana Parishadh ; 1993. p.no- 252-273 and 121.
10) Agnivesha, Charaka samhita, Sutrasthana, Chapter 22. Shloka 4. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 288-295.
11) Agnivesha, Charaka samhita, Sutrasthana, Chapter 13. Shloka 1-100. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 180-196.
12) Agnivesha, Charaka samhita, Siddisthana, Chapter 1. Shloka 6-10. Edited by Kashinath Shastry, 4th edn. Varanasi : Choukambha Bharathi Academy; 1994. p. 960-961.
13) Sushruta, Sushruta samhita, Chikitsasthana, Chapter 31, Shloka 1-57. Edited by Kaviraj Ambikadatta Shastry, 6th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1987. p. 132-138.
14) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, Shloka 1- 46. Edited by Kaviraj Atridev Gupta, 10th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1992. p. 108-111.
15) Vriddha Jeevaka, Kashyap Samhita, Sutrasthana, Chapter 22, Shloka 1-56. Edited by Hemaraj Sharma, 3rd edn. Varanasi : Choukambha Sanskrit Series ; p.16-24.
16) Bhela, Bhela samhita., Chapter 14 Chikstha Prabhutiya Adhyaya, Shloka 3-4, Edited by Girija Dayalu Shukla 1st edn. Varanasi : Choukambha Vidhya Bhavana ; 1959. p. 26.
ii
17) Atreya Maharshi, Hareeta Samhita, 1st edn. Mumbai: Pub. Khemaraj Shri. Krishndas; 1849. p. 80 – 86.
18) Laxmipati Shastry, Yogaratnakara, Chapter 1. 5th edn. Varanasi : Shri Gokul Mudranalaya ; 1993. p. 107-108
19) Ganga Sahaye Pande Chunekar, Bhavaprakash Nigantu, 10th edn. Varanasi : Choukambha Bharathi Academy ; 1995. p. 779-782
20) Sharangadhara, Sharangadhara Samhita, Uttar Khanda, Chapter 1, Shloka 1-33. Edited by Dr. Smt. Shailaja Srivatsava, 3rd edn. Varanasi : Choukambha Orientalia ; 2003. p. 316-323.
21) Herald varley, Alan H. Gowen lock, Mourice Bell, Practical Clinical Chemistry, Vol II, 6th Chapter, 5th edn. New Delhi: CBS publishers and distributors; 1991. p. 215 – 256. 22) Dr. Shantala priyadarshini,mysore, research paper published by Rashtriya Ayuveda vidyapeeth at 26-27,March,2003 p .65to 68, 23) Agnivesa, Charakasamhitha Shiddisthana chapter 9th sloka 32.to 48,edition ; reprint,2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 719. 24) Sushrutha, Sushruthasamhitha uttaratantra chapter 58th, sloka 3 to 4, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 787. 25) Sushrutha, Sushruthasamhitha Nidanasthana, chapter 1st, sloka 90, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 270 26) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 5th, sloka 27, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 429. 27) Vagbhata, Astanga Hridaya, Nidanasthana, Chapter 9, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 498. 28) Chakrapanidatta, Chakradatta chapter 32 edited by- Bhishagrathna Shribrahama Shankara Mishra Varanasi: Chaukhambha Publishers; 1998. p no-279. 29) Govindadasa, Bhaishajya Ratnavali edited by Ambikadatta Shastri, chapter 34, 2ed edition ; Publishers; Chaukhambha Sanskrit Sansthan; p no-497. 30) Williams Monier Monier Sir, Sanskrit English Dictionary cognate Indo-European languages. New Delhi: Motilal Banarasi Das; 1970. p no-139. 31) Arunadatta, Ashtangahridaya Suthrasthana chapter 19 sloka 1. Varanasi: Krishnadas Academy; 1982. p. 270. (Krishnadas academic series 4) 32) Ashtangasangraha Suthrasthana chapter 28 sloka 2. Prof.K.R.Shrikhantamurthy, editor. Varanasi: Chaukhambha Orientalia; 1996. p. 485. (Jaikrishnadas Ayurvedic series 79). 33) Agnivesa, Charakasamhitha Chikitsasthana chapter 28 sloka 56. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 619. (Kasi Sanskrit series 228).
iii
34)Williams Monier Monier Sir, Sanskrit English Dictionary cognate Indo-European languages. New Delhi: Motilal Banarasi Das; 1970. p no-66. 35) Williams Monier Monier Sir, Sanskrit English Dictionary cognate Indo-European languages. New Delhi: Motilal Banarasi Das; 1970.
36) Agnivesha, Charaka samhita, Sutrasthana, Chapter 22. Shloka 10. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 289.
37) Agnivesa, Charakasamhitha Sutrasthana chapter 13th sloka 33. edition; reprint,2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 83. 37)(a) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, sloka 19, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 247. 38) Sushrutha, Sushruthasamhitha Nidanasthana, “Dalhana” comentry, chapter 1st, sloka 90, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 270
39) Shri Monier, Williams “Sanskrita English Dictionary” first Publiser oxford university 1899, edition; reprent 1993 at delhi. p no-117. 40) Shabda Kalpadrum, Raja Raha kantadeva 3th fart third edition 1967, Varanasi: Publiser Chaukhambha Sanskrit Sansthan, p no- 757. 41) Sushrutha, Sushruthasamhitha Nidanasthana, and “Dalhana” comentry, chapter 1st, sloka 90, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 270 42) Agnivesa, Charakasamhitha Chikishtasthana “Chakrapani” chapter 26th sloka 43 to 44,edition ; reprint,2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 600. 43) Agnivesa, Charakasamhitha Siddhisthana chapter 7 sloka 1. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 709. (Kasi Sanskrit series 228).
44) Pandit Narahari’s Rajanighantu, Ksheera varga , Shloka-5. Edited by Indradeva Tripathi, 1th edn. Varanasi : Krishnadasa Academy ; 1982. p.504. 45) Sushrutha, Sushruthasamhitha Nidanasthana, and “Dalhana” comentry, chapter 1st, sloka 90, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 270 46) Agnivesa, Charakasamhitha Siddhisthana chapter 10 sloka 5-6. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 724. (Kasi Sanskrit series 228). 47) Vagbhata, Ashtangahridaya Suthrasthana chapter 19 sloka 1. Varanasi: Krishnadas Academy; 1982. p. 270. (Krishnadas academic series 4).
iv
48) Vagbhata, Ashtangahridaya Suthrasthana chapter 19 sloka 86. Varanasi: Krishnadas Academy; 1982. p. 285. (Krishnadas academic series 4). 49) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 36 sloka 6. Varanasi: Krishnadas Academy; 1980. p. 529. (Krishnadas Ayurveda series 51). 50) Vagbhata, Ashtangahridaya Suthrasthana chapter 19 sloka 87. Varanasi: Krishnadas Academy; 1982. p. 286. (Krishnadas academic series 4). 51) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 35 sloka 3. Varanasi: Krishnadas Academy; 1980. p. 525. (Krishnadas Ayurveda series 51). 52) Agnivesa, Charakasamhitha Siddhisthana chapter 1 sloka 27-28. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 682. (Kasi Sanskrit series 228). 53) Vrudhajeevaka, Kashyapasamhita Khilasthana chapter 8 sloka 54. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1988. p. 289. (Kasi Sanskrit series 154). 54) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 35 sloka 18. Varanasi: Krishnadas Academy; 1980. p. 526. (Krishnadas Ayurveda series 51). 55) Kasture VG, Ayurvediyapanchakarmavigyan chapter 6. 6th ed. Nagpur: Shree Baidyanath Ayurved Bhavan Ltd.; 1998. p. 373. 56) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 35 sloka 18. Varanasi: Krishnadas Academy; 1980. p. 526. (Krishnadas Ayurveda series 51). 57) Ashtangasangraha Suthrasthana chapter 28 sloka 4. Prof.K.R.Shrikhantamurthy, editor. Varanasi: Chaukhambha Orientalia; 1996. p. 485. (Jaikrishnadas Ayurvedic series 79). 58) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 35 sloka 17. Varanasi: Krishnadas Academy; 1980. p. 526. (Krishnadas Ayurveda series 51). 59) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 35 sloka 19. Varanasi: Krishnadas Academy; 1980. p. 526. (Krishnadas Ayurveda series 51). 60) Vagbhata, Ashtangahridaya Suthrasthana chapter 19 sloka 61. Varanasi: Krishnadas Academy; 1982. p. 282. (Krishnadas academic series 4). 61) Sharangadhara, Sarngadharasamhitha Utharakhanda chapter 5 sloka 19-22. 3rd ed. Varanasi: Chaukhambha Orientalia; 1983. p. 323. (Jaikrishnadas Ayu. Granthamala 53). 62) Agnivesa, Charakasamhitha Siddhisthana chapter 8. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 713-715. (Kasi Sanskrit series 228). 63) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 37 sloka 77. Varanasi: Krishnadas Academy; 1980. p. 536. (Krishnadas Ayurveda series 51). 64) Agnivesa, Charakasamhitha Siddhisthana chapter 1 sloka 47-48. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 684. (Kasi Sanskrit series 228).
v
65) Vrudhajeevaka, Kashyapasamhita Khilasthana chapter 8 sloka 7. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1988. p. 277. (Kasi Sanskrit series 154). 66) Vrudhajeevaka, Kashyapasamhita Khilasthana chapter 8 sloka 8. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1988. p. 277. (Kasi Sanskrit series 154). 67) Vrudhajeevaka, Kashyapasamhita Khilasthana chapter 8 sloka 9. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1988. p. 277. (Kasi Sanskrit series 154). 68) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 37 sloka 39. Varanasi: Krishnadas Academy; 1980. p. 533. (Krishnadas Ayurveda series 51). 69) Agnivesa, Charakasamhitha Siddhisthana chapter 8 sloka 2-14. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 713. (Kasi Sanskrit series 228). 70) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 38 sloka 118. Varanasi: Krishnadas Academy; 1980. p. 548. (Krishnadas Ayurveda series 51). 71) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 36 sloka 3. Varanasi: (research - Krishnadas Academy; 1980. p. 528. (Krishnadas Ayurveda series 51). 72) Agnivesa, Charakasamhitha Siddhisthana chapter 4 sloka 53. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 701. (Kasi Sanskrit series 228). 73) Agnivesa, Charakasamhitha Siddhisthana chapter 4 sloka 54. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 701. (Kasi Sanskrit series 228). 74) Agnivesa, Charakasamhitha Siddhisthana chapter 12 sloka 15. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 731. (Kasi Sanskrit series 228). 75) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 38 sloka 116. Varanasi: Krishnadas Academy; 1980. p. 548. (Krishnadas Ayurveda series 51). 76) Vangasena, Vangasenasamhitha Bastikarmaadhikara sloka 170. Jain Sankarlalji Vaidya editor. Mumbai: Khemnath Srikrishnadas publishers; 1996. p. 999. 77) Vangasena, Vangasenasamhitha Bastikarmaadhikara sloka 186-190. Jain Sankarlalji Vaidya editor. Mumbai: Khemnath Srikrishnadas publishers; 1996. p. 1000. 78) Chakrapanidatta, Chakradatta chapter 73 sloka 29-31. 2nd ed. P.V.Sharma editor. Varanasi: Chaukhambha Publishers; 1998. p. 628. (Kasi Ayurveda series 17). 79) Chakrapanidatta, Chakradatta chapter 73 sloka 23-26. 2nd ed. P.V.Sharma editor. Varanasi: Chaukhambha Publishers; 1998. p. 627-628. (Kasi Ayurveda series 17). 80) Vagbhata, Ashtangahridaya Chikitsasthana chapter 9 sloka 72-76. Varanasi: Krishnadas Academy; 1982. p. 661. (Krishnadas Academic series 4).
81) Agnivesa, Charakasamhitha Siddhisthana chapter 6 sloka 83. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 708. (Kasi Sanskrit series 228).
vi
82) Vangasena, Vangasenasamhitha Bastikarmaadhikara sloka 182-185. Jain Sankarlalji Vaidya editor. Mumbai: Khemnath Srikrishnadas publishers; 1996. p. 999. 83) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, sloka 25, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 248. 84) Agnivesa, Charakasamhitha Shiddisthana chapter 4th sloka 52.to 53,edition ; reprint,2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 701. 85) Sushrutha, Sushruthasamhitha chikishtasthana chapter 35th, sloka 18, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 527. 86)Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 19, sloka 68 to 69, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 283. 87) Agnivesa, Charakasamhitha Shiddisthana chapter 4th sloka 52.to 53,edition ; reprint,2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 701.
88) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 19, sloka 68 to 69, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 283.
89) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 28, Shloka 9. Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p.no- 487. 90) Agnivesa, Charakasamhitha Shiddisthana chapter 4th sloka 54,edition ; reprint,2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 701.
91) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 19, sloka 68 to 69, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 283.
92) Vagbhata, Astanga Hridaya, Sutrasthana, “Hemadri Commentary,” Chapter 19, sloka 68 to 69, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 283. 93) Agnivesa, Charakasamhitha Shiddisthana chapter 4th sloka 52.to 53,edition ; reprint,2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 701. 94) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 28, Shloka 8,9. Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p.no- 487-488. 95) Vagbhata, Astanga Hridaya, Sutrasthana, “Hemadri Commentary,” Chapter 19, sloka 69, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 283.
vii
96) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 28, Shloka 8,9. Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p.no- 487-488. 97) Agnivesa, Charakasamhitha Shiddisthana chapter 4th sloka 53. Edition ; reprint,2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 701. 98) Vagbhata, Astanga Hridaya, Sutrasthana, “Hemadri Commentary,” Chapter 19, sloka 67, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 283. 99) Sushrutha, Sushruthasamhitha chikishtasthana chapter 35th, sloka 18, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 527. 100) Vriddha Jeevaka, Kashyapa Samhita, Khilasthana, 8th chapter, shloka 104-105, Edited by Pandita Hemaraj Sharma, Varanasi: Chaukhamaba Sanskrit Samsthana, 4th Editon 1988.p.285. 101) Agnivesa, Charakasamhitha Shiddisthana chapter 4th sloka 52-54. Edition ; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no.285. 102) Pandita Sharangadhara Acharya, Sharangadhara Samhita, Uttara khanda, chapter 5, shloks 5, Edited By Pandita Parashuram Shastei Vidyasagar, 3rd Edition, 1983.p.320. 103) Vagbhata, Ashtangahridaya Suthrasthana chapter 19 sloka 22-23. Varanasi: Krishnadas Academy; 1982. p. 275. (Krishnadas Academic series 4). 104) Agnivesa, Charakasamhitha Siddhisthana chapter 3 sloka 27. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 694. (Kasi Sanskrit series 228). 105) Sushrutha, Sushruthasamhitha Chikitsasthana chapter 38 sloka 1-6. Varanasi: Krishnadas Academy; 1980. p. 539-540. (Krishnadas Ayurveda series 51). 106) Vagbhata, Ashtangahridaya Suthrasthana chapter 19 sloka 24-26. Varanasi: Krishnadas Academy; 1982. p. 276. (Krishnadas Academic series 4). 107) Vagbhata, Ashtangahridaya Suthrasthana chapter 19 sloka 26-30. Varanasi: Krishnadas Academy; 1982. p. 276-277. (Krishnadas Academic series 4). 108) Agnivesa, Charakasamhitha Siddhisthana chapter 3 sloka 28-29. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 694. (Kasi Sanskrit series 228).
109) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, Shloka 1. Edited by Kaviraj Atridev Gupta, 10th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1992. p. 108.
110) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 25, Shloka 3. Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p. 446.
111) Agnivesha, Charaka samhita, Sutrasthana, Chapter 22. Shloka 15. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 290.
viii
112) Sushruta, Sushruta samhita, Sutrasthana, Chapter 41, Shloka 14-15. Edited by Kaviraj Ambikadatta Shastry, 6th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1987. P No.155. 113) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, sloka 25, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 243,to245..
114) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 25, Shloka 10,to13, Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p.no- 434.
115) Agnivesha, Charaka samhita, Sutrasthana, Chapter 13. Shloka 13,to18,44to49. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p,no-83,84.
116) Sharangadhara, Sharangadhara Samhita, Uttara Khanda, Chapter 1, Shloka 15-18. Edited by Dr. Smt. Shailaja Srivatsava, 3rd edn. Varanasi : Choukambha Orientalia ; 2003. p.no-288,289.
117) Agnivesha, Charaka samhita, Sutrasthana, Chapter 13. Shloka 09. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 181.
118) Sushruta, Sushruta samhita, Chikitsasthana, Chapter 31, Shloka 4. Edited by Kaviraj Ambikadatta Shastry, 6th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1987. p.no- 133.
119) Agnivesha, Charaka samhita, Sutrasthana, Chapter 13. Shloka 10. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. no-181.
120) Sushruta, Sushruta samhita, Chikitsasthana, Chapter 31, Shloka 5. Edited by Kaviraj Ambikadatta Shastry, 6th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1987. p. no-133.
121) Agnivesha, Charaka samhita, Kalpasthana, Chapter 12. Shloka 103-104. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. no-957
122) Sushruta, Sushruta samhita, Chikitsasthana, Chapter 31, Shloka 11. Edited by Kaviraj Ambikadatta Shastry, 6th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1987. p. 134.
123) Sharangadhara, Sharangadhara Samhita, Madhyama Khanda, Chapter 9, Shloka 15-18. Edited by Dr. Smt. Shailaja Srivatsava, 3rd edn. Varanasi : Choukambha Orientalia ; 2003. p.217.
124) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, Shloka 04. Edited by Kaviraj Atridev Gupta, 10th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1992. p. 108.
125) Agnivesha, Charaka samhita, Sutrasthana, Chapter 1. Shloka 87. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 35.
126) Sushruta, Sushruta samhita, Dalhana commentary, Chikitsasthana, Chapter 31, Shloka 11. Edited by Kaviraj Ambikadatta Shastry, 4th edn. Varanasi : Choukambha orientalia ; 1980. p. 509.
127) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, Shloka 14. Edited by Kaviraj Atridev Gupta, 10th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1992. p. 109.
ix
128) Agnivesha, Charaka samhita, Sutrasthana, Chapter 13. Shloka 23-28. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 185.
129) Dalhana, Sushruta samhita, Nibandha Sangraha commentary, Chikitsasthana, Chapter 31, Shloka 19,21. 4th edn. Varanasi : Choukambha orientalia ; 1980. p. 510.
130) Agnivesha, Charaka samhita, Sutrasthana, Chapter 13. Shloka 89. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 194.
140) Dalhana Sushruta samhita, Nibandha Sangraha commentary, Chikitsasthana, Chapter 31, Shloka 38-44. 4th edn. Varanasi : Choukambha orientalia ; 1980. p. 511.
141) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, Shloka 42. Edited by Kaviraj Atridev Gupta, 10th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1992. p. 111.
142) Agnivesha, Charaka samhita, Sutrasthana, Chapter 13. Shloka 29. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 185.
143) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 25, Shloka 22-23. Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p. 452.
144) Arunadutta, Astanga Hridaya, Sarvanga sundhari commentary, Chapter 16, Shloka 18. Edited by Pt. Harisadashiva Shatry Paradakara Bhisagacharya, 6th edn. Varanasi : Choukambha Surabharati prakashana ;1997. p. 246-247.
145) Sharangadhara, Sharangadhara Samhita, Uttara Khanda, Chapter 1, Shloka 7-8. Edited by Dr. Smt. Shailaja Srivatsava, 3rd edn. Varanasi : Choukambha Orientalia ; 2003. p.318.
146) Chakradatta, Snehapanadhikar, Chapter 67, Shloka 13, 14. Edited by Jagadeeshwar Prasad Tripati, 5th edn. Varanasi : Choukambha Sanskrit Office; 1983. p. 580.
147) Sushruta, Sushruta samhita, Chikitsasthana, Chapter 31, Shloka 25-29. Edited by Kaviraj Ambikadatta Shastry, 6th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1987. P No. 136.
148) Agnivesha, Charaka samhita, Sutrasthana, Chapter 13. Shloka 61. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 190
149) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 25, Shloka 24-28. Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p. 452-453. 150) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, sloka 19, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 246. 151) Agnivesa, Charakasamhitha Sutrasthana chapter 13th sloka 29-40, edition ; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 83-84.
x
152) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, sloka 19, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 246 to 248. 153) Agnivesa, Charakasamhitha Sutrasthana chapter 13th sloka 81, edition ; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 86. 154) Sushrutha, Sushruthasamhitha chikishtasthana chapter 31th, sloka 34, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 511. 155) Agnivesa, Charakasamhitha Sutrasthana chapter 13th sloka 29-40, edition ; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 83. 156) Vagbhata, Astanga Hridaya, Sutrasthana, Arunadatta, Chapter 16, sloka 19, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 247. 157) Agnivesa, Charakasamhitha Sutrasthana “Chakrapani”chapter 13th sloka 29-40, edition ; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 83.
157) (a) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 25, Shloka 24, to 25 Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p.no- 437, 438. 158) Pandita Sharangadhara Acharya, Sharangadhara Samhita, Uttara khanda, chapter 1, shloks 4 to 10, Edited By Pandita Parashuram Shastei Vidyasagar, 3rd Edition, 1983.p.no-286 to 288. 159) Pandita Sharangadhara Acharya, Sharangadhara Samhita, Uttara khanda, chapter 1, shloks 4 to 10, Edited By Pandita Parashuram Shastei Vidyasagar, 3rd Edition, 1983.p.no-286to 288, 160) Pandita Sharangadhara Acharya, Sharangadhara Samhita, Uttara khanda, chapter 1, shloks 4 to 5, Edited By Pandita Parashuram Shastei Vidyasagar, 3rd Edition, 1983.p.no-286, 161) Dr. H. S. Kasture.Shri; Ayurvediya Panchakarma Vijynana, Chapter 2ed Bidhyanatha Ayurveda bavana publications editer Vidhya Haridas Shridara Kasture. P no-93. 162) Vriddha Jeevaka, Kashyapa Samhita, Sutrasthana, 22th chapter, shloka 46, Edited by Pandita Hemaraj Sharma, Varanasi: Chaukhamaba Sanskrit Samsthana, 4th Editon 1988.p.23. 163) Agnivesa, Charakasamhitha Sutrasthana chapter 13th sloka 29-40, edition ; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 83 to 84. 164) Sushrutha, Sushruthasamhitha chikishtasthana chapter 31th, sloka 29, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 511.
165) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 25, Shloka 24, to 25 Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p.no- 437, 438.
xi
166) Agnivesha, Charaka samhita, Sutrasthana, Chapter 13. Shloka 53-56. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 189.
167) Sushruta, Sushruta samhita, Chikitsasthana, Chapter 31, Shloka 46-48. Edited by Kaviraj Ambikadatta Shastry, 6th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1987. p. 137.
168) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, Shloka 6-7. Edited by Kaviraj Atridev Gupta, 10th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1992. p. 108.
169) Vriddha Jeevaka, Kashyap Samhita, Sutrasthana, Chapter 22, Shloka 30-32. Edited by Hemaraj Sharma, 3rd edn. Varanasi : Choukambha Sanskrit Series ; p. 20.
170) Sharangadhara, Sharangadhara Samhita, Uttara Khanda, Chapter 1, Shloka 26, Edited by Dr. Smt. Shailaja Srivatsava, 3rd edn. Varanasi : Choukambha Orientalia ; 2003. p.322.
171) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 25, Shloka 13, Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p.no- 434, 435.
172) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 25, Shloka 13, Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p.no- 434, 435. 173) Agnivesa, Charakasamhitha Sutrasthana “Chkrapani” chapter 13th sloka 70to78, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 86. 174) Arunadutta, Astanga Hridaya, Sarvanga sundhari, commentary, Chapter 16, Shloka 19. Edited by Pt. Harisadashiva Shatry Paradakara Bhisagacharya, 6th edn. Varanasi : Choukambha Surabharati prakashana ;1997. p. 246-247. 175) Agnivesa, Charakasamhitha Sutrasthana “Chkrapani” chapter 13th sloka 61, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 85. 176) Agnivesa, Charakasamhitha Sutrasthana “Chkrapani” chapter 13th sloka 61, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 85.
177) Sushruta, Sushruta samhita, Chikitsasthana, Chapter 31, Shloka 14. Edited by Kaviraj Ambikadatta Shastry, 6th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1987. p. 510.
178) Agnivesha, Charaka samhita, Sutrasthana, Chapter 13. Shloka 22. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 184.
179) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, Shloka 23-24. Edited by Kaviraj Atridev Gupta, 10th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1992. p. 110.
180) Sharangadhara, Sharangadhara Samhita, Uttara Khanda, Chapter 1, Shloka 19, Edited by Dr. Smt. Shailaja Srivatsava, 3rd edn. Varanasi : Choukambha Orientalia ; 2003. p.320.
xii
181) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, sloka 19, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 247 to 248. 182) Agnivesa, Charakasamhitha Sutrasthana “Chkrapani” chapter 13th sloka 81, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 86.
183) Sushruta, Sushruta samhita, Chikitsasthana, Chapter 31, Shloka 14. Edited by Kaviraj Ambikadatta Shastry, 6th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1987. p.no- 511.
184) Agnivesha, Charaka samhita, Sutrasthana, Chapter 13. Shloka 62-64. Edited by Rajeshwaradatta Shastry, 4th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1994. p. 190.
185) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 16, Shloka 26-27. Edited by Kaviraj Atridev Gupta, 10th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1992. p. 110.
186) Sushruta, Sushruta samhita, Chikitsasthana, Chapter 31, Shloka 34-35. Edited by Kaviraj Ambikadatta Shastry, 6th edn. Varanasi : Choukambha Sanskrit Sansthan ; 1987. p. 137.
187) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 25, Shloka 41-43. Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p. 459.
188) Shrimad Vriddha Vagbhata, Astanga Sangraha, Sutrasthana, Chapter 25, Shloka 37-38. Edited by Ravidatta Tripathi, 10th edn. Varanasi : Choukambha Sanskrit Pratisansthana ; 1996. p. 456.
189) Shri Monier, Williams “Sanskrita English Dictionary” first Publiser oxford university 1899, edition; reprent 1993 at delhi. p no-117. 190) Sushrutha, Sushruthasamhitha Uttaratantra, chapter 58th, shloka 7 to 8, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 527.
191) Sushrutha, Sushruthasamhitha Uttaratantra, chapter 58th, shloka 7 to 8, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 527.
192) Shri Monier, Williams “Sanskrita English Dictionary” first Publiser oxford university 1899, edition; reprent 1993 at delhi.
193) Shri Monier, Williams “Sanskrita English Dictionary” first Publiser oxford university 1899, edition; reprent 1993 at delhi. p no-148.
194) Shri Monier, Williams “Sanskrita English Dictionary” first Publiser oxford university 1899, edition; reprent 1993 at delhi. p no-222.
195) Shri Monier, Williams “Sanskrita English Dictionary” first Publiser oxford university 1899, edition; reprent 1993 at delhi.
xiii
196) Shri Monier, Williams “Sanskrita English Dictionary” first Publiser oxford university 1899, edition; reprent 1993 at delhi. p no-193.
197) Shri Monier, Williams “Sanskrita English Dictionary” first Publiser oxford university 1899, edition; reprent 1993 at delhi. 198) Sushrutha, Sushruthasamhitha Nidanasthana chapter 3th, sloka 5, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no.277. 199) Sushrutha, Sushruthasamhitha Nidanasthana chapter 3th, shloka 19, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no.279. 200) Sushrutha, Sushruthasamhitha Nidanasthana chapter 2 sloka 5. Varanasi: Krishnadas Academy; 1980. p. 272. (Krishnadas Ayurveda series 51). 201)Sushrutha, Sushruthasamhitha Nidanasthana chapter 2 sloka 6-7. Varanasi: Krishnadas Academy; 1980. p. 272. (Krishnadas Ayurveda series 51). 202)Agnivesa, Charakasamhitha Shareerasthana chapter 7 sloka 10. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 338. (Kasi Sanskrit series 228). 203)Vagbhata, Ashtangahridaya Shareerasthana chapter 3 sloka 13. Varanasi: Krishnadas Academy; 1982. p. 388. (Krishnadas academic series 4). 204)Agnivesa, Charakasamhitha Shareerasthana chapter 7 sloka 9. 4th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1994. p. 338. (Kasi Sanskrit series 228). 205) Sushrutha, Sushruthasamhitha Shareerasthana chapter 5 sloka 10. Varanasi: Krishnadas Academy; 1980. p. 364. (Krishnadas Ayurveda series 51). 206)Martini.F.H, Fundamentals of Anatomy and Physiology chapter 24. 4th ed. New Jersey: Prentice Hall Inc. Simon & Schuster; 1998. p. 899.
207) Sushrutha, Sushruthasamhitha Nidanasthana chapter 3th, shloka 5 to 6, fourth edition ;1980. Edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 277.
208) Sushrutha, Sushruthasamhitha Shariraasthana chapter 4th, shloka 26 to 27. fourth edition; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 357.
209) Sushrutha, Sushruthasamhitha Nidanaasthana chapter 3th, sloka 18 to 19, fourth edition; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 279.
210) T. R. Harrisons. Harrison.s; Principles of Internal Medicine, Editor-T . R. Harrisons, Chapter 95, International edition-2003, 15th edition. P, no-608,609.
211) Bailey and love, Short practice of surgery. Chapter 66, Edited by- R. c. c. Russell, Norman .s. Williams. 23ed edition, P no 1237 to 1238.
xiv
212) Grays Anatomy CHURCHIL LIVINGSTONE, Chairman of the editorial board, 13th edition, reprinted, 2000 P. No.1859.
213) Bailey and love, Short practice of surgery. Chapter 66, Edited by- R. c. c. Russell, Norman .s. Williams. 23ed edition, P no 1238.
214) Prof. Krishnamurty K. R, English translation of Ashtanga Hridaya Samhita, 4th edition 1999, vol 1, Sutra stana, Ayushkameeya adhyaya, 1” chapter, Verse no. 8, P. no. 6,7.
215) Shasthri Kashinath, Charaka Samhita with vidyotthini Teeka, 4th Edition, 1994, part 1 Rogabhishagjateeya adhyaya, 8th chapter, Verse 122, P, no, 672.
216) Srivastav Shailaja, Sharangadhara Samhita with Hindi commentary, 1st edition, Poorvakhanda, Aharadigati adhyaya, 6th capter, Verse 19, P, no, 54.
217) Kirkwood T.B.L, Evolution of theory and the mechanism of aging in Brontology, Tallis R,C,. et.al. 5th edition 1998, chapter no,4, P, no, 45.
218) Sushrutha, Sushruthasamhitha Nidanaasthana chapter 1th, shloka 90, fourth edition; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 270.
219) Sushrutha, Sushruthasamhitha Uttaratantra, “Dhalhana” chapter 58th, shloka 7 to 8, fourth edition; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no-787. 220) Agnivesa, Charakasamhitha Chikisthasthana chapter 26th shloka 32,edition; reprint,2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 599. 221) Agnivesa, Charakasamhitha Vimanathasthana chapter 5th shloka 20, edition; reprint,2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 251.
222) Sushrutha, Sushruthasamhitha Uttaratantra, “Dhalhana” chapter 59th, shloka 8 to 9, fourth edition; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no-792. 223) Bhavamishra, Bhavaprakasha Poorvakhanda chapter 5 sloka 123. 5th ed. Varanasi: Chaukhambha Orientalia; 1988. (Chaukhambha Sanskrit series 130).
224) Sri Vaidya Shodala, Gada nigraha edited by Indradeva tripathi 1st edition, delhi; Chaukhambha Sanskrit Sansthan; 1969, chapter 27, shloka 1-2, P, no-625
225) Sushrutha, Sushruthasamhitha Sharirasthana, “Dhalhana” chapter 6th, shloka 25, fourth edition; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no-373. 226) Agnivesa, Charakasamhitha Chikisthasthana chapter 25th shloka 15, edition; reprint,2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 592. 227) Nigantu Ratnakara, Bastisharira and kriyavijnyana. By Vasant Balaji Athavale, Mutrakrachra prakarna, P,no-1029.
xv
228) Sushrutha, Sushruthasamhitha Uttaratantra, chapter 58th, shloka 7 to 8, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 787 229) Agnivesa, Charakasamhitha Siddisthana “Chkrapani” chapter 9th shloka 36, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 719 230) John D, et.al. Epidemiology, etiology, pathophysiology and diagnosis of Benign Prostatic Hyperplasia in Campbells, Urology by Patrick C, Walsh, et al, 7th edition, 1998, Vol 2, section 8, chapter 39, P.no- 1340. 231) Vagbhata, Astanga Hridaya, Sutrasthana, Chapter 1, sloka 8, Edited by Bhishagacharya Harishasashtri ParadakaraVaidya 7th edn. 1982. Varanasi : Choukambha Sanskrit Sansthan ; p. no- 07. 232) Sushrutha, Sushruthasamhitha Uttaratantra, chapter 58th, shloka 7 to 8, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 787 233) Sushrutha, Sushruthasamhitha Sutrasthana, chapter 21th, shloka 33, fourth edition;1980. Edited by vaidya jaadavaji trikamji acharya, Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 105,106. 234) Sushrutha, Sushruthasamhitha Sutrasthana, chapter 21th, shloka 30, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 105. 235) Sushrutha, Sushruthasamhitha Uttaratantra, chapter 58th, shloka 7 to 8, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 787 236) Bailey and love, Short practice of surgery. Chapter 66, Edited by- R. c. c. Russell, Norman .s. Williams. 23ed edition, P no 1238. 237) John D, et.al. Epidemiology, etiology, pathophysiology and diagnosis of Benign Prostatic Hyperplasia in Campbells, Urology by Patrick C, Walsh, et al, 7th edition, 1998, Vol, 2, section 8, chapter 39, P.no- 1348. 238) Agnivesa, Charakasamhitha Siddisthana “Chkrapani” chapter 9th shloka 49, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 720. 239) Sushrutha, Sushruthasamhitha, Chikisthasthana chapter 5th, shloka 27, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 429. 240) Agnivesa, Charakasamhitha Chikisthasthana chapter 28th shloka 212, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no, 625,. 241) Agnivesa, Charakasamhitha Chikisthasthana “Chakrapani,” chapter 28th shloka 85, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no, 620. 242)Agnivesa, Charakasamhitha Siddisthana “Chkrapani” chapter 9th shloka 11, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 719.
xvi
243) Agnivesa, Charakasamhitha Siddisthana “Chkrapani” chapter 9th shloka 49, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 720. 244) Sushrutha, Sushruthasamhitha Uttaratantra, chapter 58th, shloka 27, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 789. 245) Agnivesa, Charakasamhitha Sutrasthana with “Chkrapani” chapter 7th shloka 8, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 49. 246) Agnivesa, Charakasamhitha Sutrasthana with “Chkrapani” chapter 7th shloka 13, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 49,50. 247) Sushrutha, Sushruthasamhitha Uttaratantra, chapter 58th, shloka 27, fourth edition ; 1980. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 789. 248)Agnivesa, Charakasamhitha Siddisthana “Chkrapani” chapter 9th shloka 49, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 720. 249) Agnivesa, Charakasamhitha Sutrasthana with “Chkrapani” chapter 7th shloka 8, edition; reprint, 2004. edited by vaidya jaadavaji trikamji acharya,Varanasi: Chaukhambha Sanskrit Sansthan; p.no. 49. 250) John D, et.al. Epidemiology, etiology, pathophysiology and diagnosis of Benign Prostatic Hyperplasia in Campbells, Urology by Patrick C, Walsh, et al, 7th edition, 1998, Vol, 2, section 8, chapter 38, P.no- 1312. 251) John D, et.al. Epidemiology, etiology, pathophysiology and diagnosis of Benign Prostatic Hyperplasia in Campbells, Urology by Patrick C, Walsh, et al, 7th edition, 1998, Vol, 2, section 8, chapter 39, P.no- 1347. 252) I-PSS (AUA) Guidelines on benign prostatic Hyperplasia, P,no-250, (pub med, or googul.)
253) Chakrapanidatta, Chakradatta chapter 32, sloka 29-33 2nd ed. EditorBhishagratna Shibrahama Shankara mishra. Varanasi: Chaukhambha Publishers; 1998. p. 279. (Kasi Ayurveda series 17).
254) Govindadasa, Bhaishajya Ratnavali edited by Ambikadatta Shastri, chapter 34, shloka 59-65, 2ed edition ; Publishers; Chaukhambha Sanskrit Sansthan; p no-497. 255) J ,L ,N Shastri ,Drvyaguna Vijnana Vol,- 2, edition;2004, Publishers; Chaukhambha Sanskrit Sansthan; P no-1040,1042,1044,673,266,524. 256) P. V .Sharma , ,Drvyaguna Vijnana Vol,- 2, edition 12th -1989, Publishers; Chaukhambha Sanskrit Sansthan; P no-630, 761, 763, 332, 813,634,636, 638,736. 257) John D, et.al. Epidemiology, etiology, pathophysiology and diagnosis of Benign Prostatic Hyperplasia in Campbells, Urology by Patrick C, Walsh, et al, 7th edition, 1998, Vol, 2, section 8, chapter 39, P.no- 1340. 258) T.R. Harrisons. Harrison.s; Principles of Internal Medicine, Editor-T.R. Harrisons, Chapter 95, International edition-2003, 15th edition.p.-609.
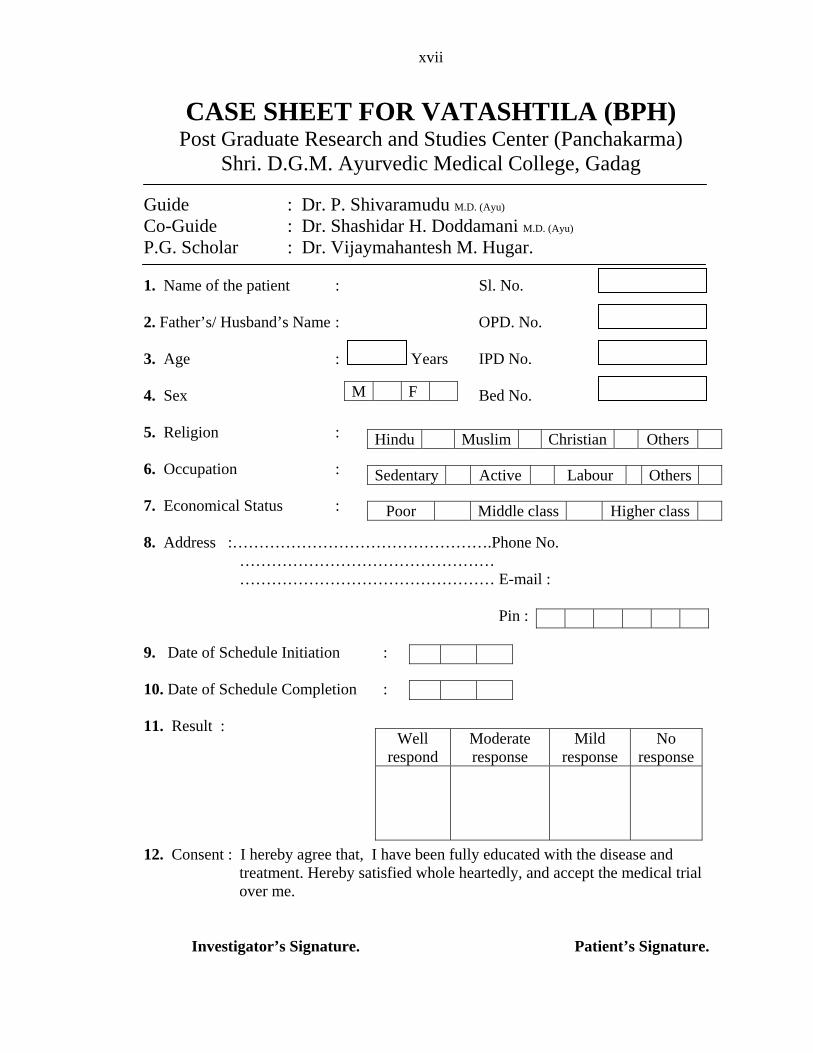
xvii
CASE SHEET FOR VATASHTILA (BPH) Post Graduate Research and Studies Center (Panchakarma)
Shri. D.G.M. Ayurvedic Medical College, Gadag Guide : Dr. P. Shivaramudu M.D. (Ayu) Co-Guide : Dr. Shashidar H. Doddamani M.D. (Ayu) P.G. Scholar : Dr. Vijaymahantesh M. Hugar. 1. Name of the patient : Sl. No. 2. Father’s/ Husband’s Name : OPD. No. 3. Age : Years IPD No. 4. Sex Bed No. M F 5. Religion : Hindu Muslim Christian Others 6. Occupation : Sedentary Active Labour Others 7. Economical Status : Poor Middle class Higher class 8. Address :………………………………………….Phone No. ………………………………………… ………………………………………… E-mail : Pin : 9. Date of Schedule Initiation : 10. Date of Schedule Completion : 11. Result :
Well respond
Moderate response
Mild response
No response
12. Consent : I hereby agree that, I have been fully educated with the disease and treatment. Hereby satisfied whole heartedly, and accept the medical trial
over me.
Investigator’s Signature. Patient’s Signature.
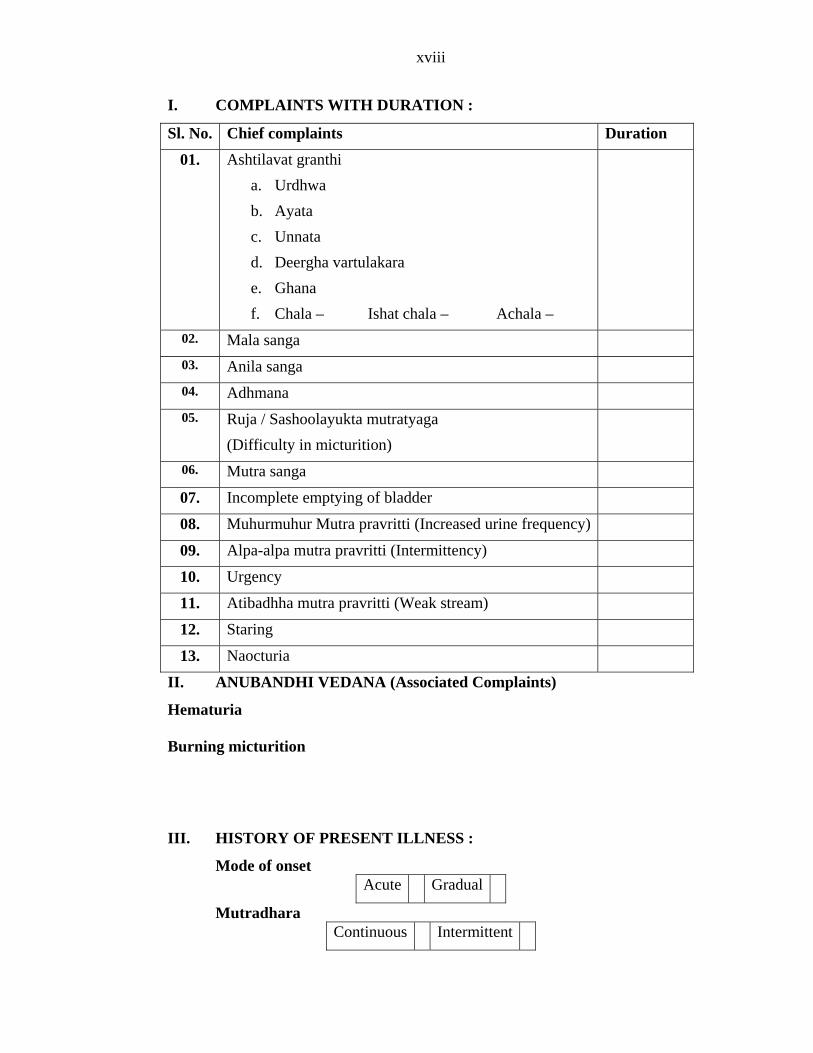
xviii
I. COMPLAINTS WITH DURATION :
Sl. No. Chief complaints Duration
01. Ashtilavat granthi a. Urdhwa b. Ayata c. Unnata d. Deergha vartulakara e. Ghana f. Chala – Ishat chala – Achala –
02. Mala sanga 03. Anila sanga 04. Adhmana 05. Ruja / Sashoolayukta mutratyaga
(Difficulty in micturition)
06. Mutra sanga
07. Incomplete emptying of bladder
08. Muhurmuhur Mutra pravritti (Increased urine frequency)
09. Alpa-alpa mutra pravritti (Intermittency)
10. Urgency
11. Atibadhha mutra pravritti (Weak stream)
12. Staring
13. Naocturia
II. ANUBANDHI VEDANA (Associated Complaints)
Hematuria
Burning micturition
III. HISTORY OF PRESENT ILLNESS :
Mode of onset Acute Gradual
Mutradhara Continuous Intermittent
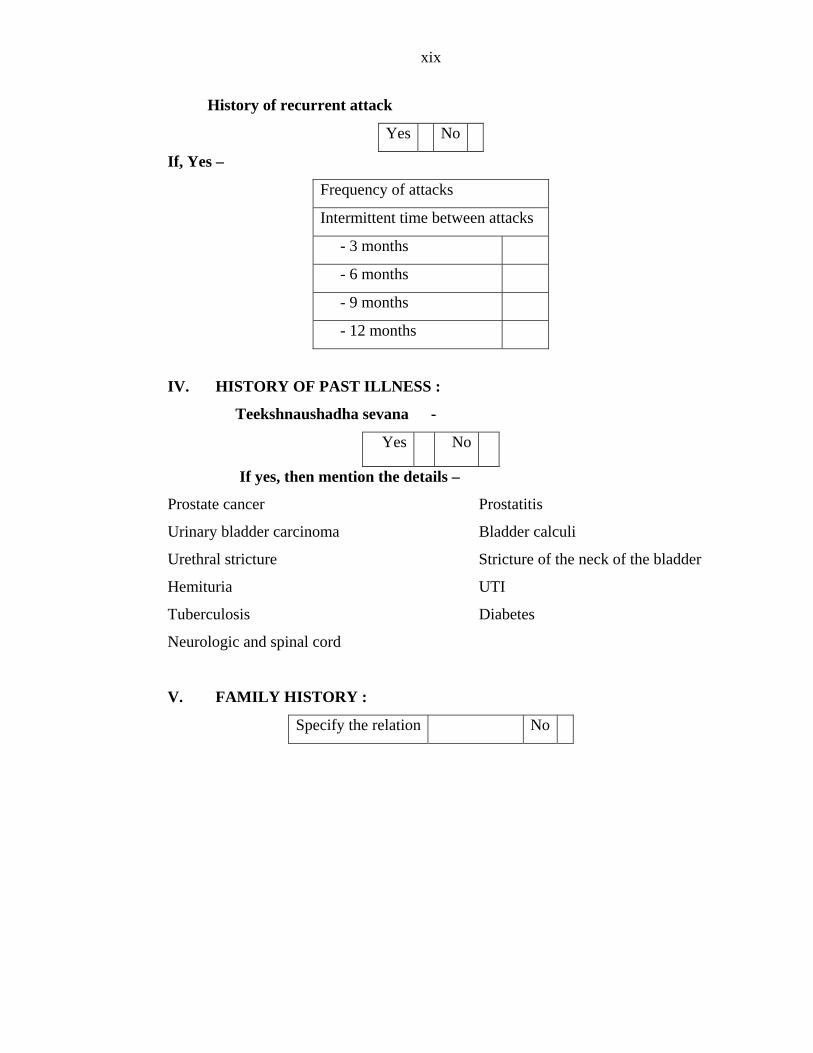
xix
History of recurrent attack
Yes No
If, Yes –
Frequency of attacks
Intermittent time between attacks
- 3 months
- 6 months
- 9 months
- 12 months
IV. HISTORY OF PAST ILLNESS :
Teekshnaushadha sevana -
Yes No
If yes, then mention the details –
Prostate cancer Prostatitis
Urinary bladder carcinoma Bladder calculi
Urethral stricture Stricture of the neck of the bladder
Hemituria UTI
Tuberculosis Diabetes
Neurologic and spinal cord
V. FAMILY HISTORY :
Specify the relation No
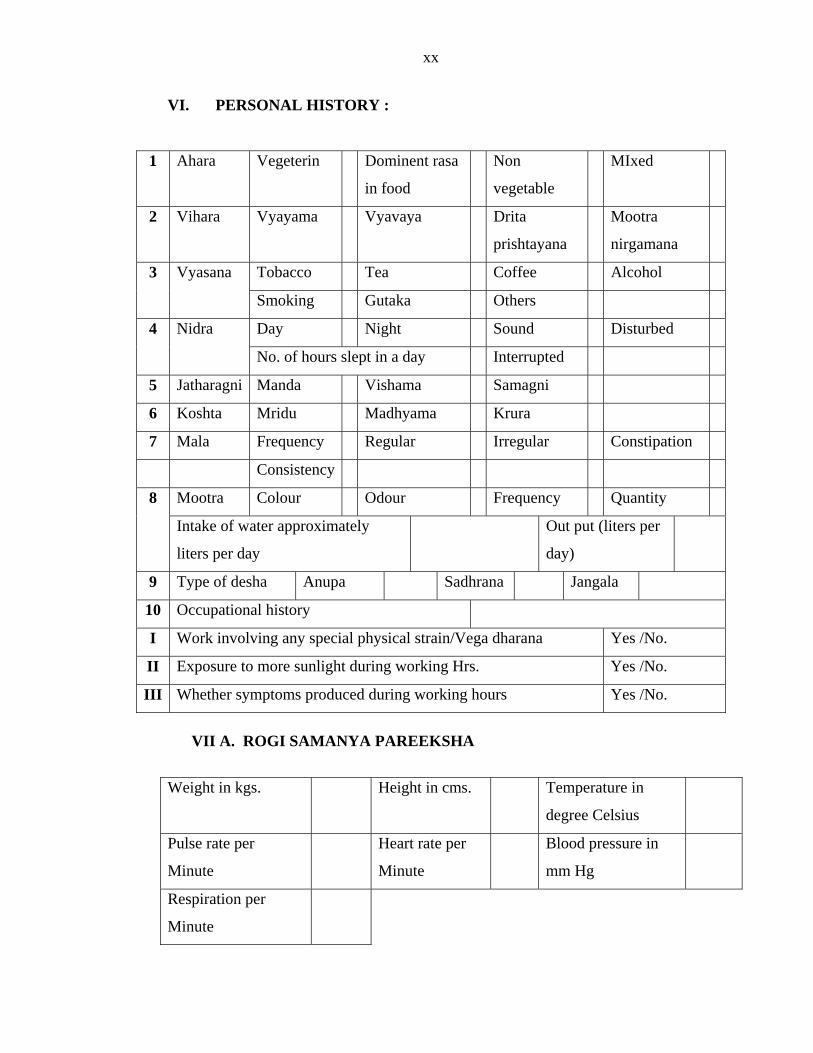
xx
VI. PERSONAL HISTORY :
1 Ahara Vegeterin Dominent rasa
in food
Non
vege
I
table
M xed
2 Vihara Vyayama Vyavaya Drita
prishtayana
Mootra
ir
n gamana
Tobacco Tea Coff Alc ee ohol 3 Vyasana
ka Othe Smoking Guta rs
Day Night Soun Disturbed d 4 Nidra
f hours s p ay Interrupted No. o le t in a d
5 Jatharagni Sam Manda Vishama agni
6 Koshta Mridu Madhyama Krur a
7 Mala Frequency Irreg Constipation Regular ular
Consistency
Mootra dour Frequency Quantity Colour O8
Intake of wa xima l (l rter appro te y
liters per day
Out put ite s per
day)
9 a Sadhrana Jangala Type of desha Anup
10 pational history Occu
I Work involving any p ysical strain/Vega dharana . special h Yes /No
II Exposure to more sunlight during working rs. Yes /No. H
III YeWhether symptoms produced during working hours s /No.
VII A. ROGI SAMANYA PAREEKSHA
We Temperature in
degree Celsius
ight in kgs. Height in cms.
Pulse rate per
Minute Minute
n Heart rate per Blood pressure i
mm Hg
Respiration per
Minute
xxi
B. ASTAST
1. N
HANA PAREEKSHA
adee :
Dosha
Gati
Poornata
Spandana
Kathinya
2. Mutra :
VIII. DASHAVIDHAPAREEKSHA
PK SAMA
3. Mala :
4. Jihwa :
5. Shabda :
6. Sparsha :
7. Druk :
8. Aakruthi :
A. PRAKRITI
V P K VP VK
B. VIKRITI
Dosha Desa
Dushya Kaala
Bala Linga
xxii
C. SAARA Pravara Madhyama Avara
D. SAMHANANA mhatha Madhyama samhatha Asamhatha Susa
E. PRAMANA Sama Heena Adhika
F. SATMYEkarasa
A Sarvarasa
Rookshasaatmya Snigdhasaatmya
G. SATVA Pravara Madhya Avara
H. AHARASHAKAbhyavahaara Pravara Madhyama Avara
THI
Jaranasak ra a a Avara thi P v ra M dhyama I. VYAYAMASHAKTHI
a h a raPravar Mad y ma Ava J. VAYAHA
Madhya Vrudha
IX. SROTOPAREEKObserved laxana Yes No
SHA Srotas
Atisrishta Atibaddha - Alpaalpa - Bahala - Sashoolayukta
Stabdha medhrata
a srotas
Mootravah
Mutra nirodha Krichhra and alpa-alpata Sashabda Shoolayukta Atidrava Atighrathita Atibahu
Durgandhata
Purishavaha srotas
xxiii
Anya srotas pariksha
Srotas Observed Lakshana
Pranavaha
Annavaha
Udakavaha
Rasavaha
Rakthavaha
Mamsavaha
Medovaha
Asthivaha
Majjavaha
Sukravaha
Swedovaha
X. SYSTEMIC EXAMINATION
A. Urinary system –
s lar system –
Yes No
B. Cardiova cu
C. Respiratory system –
D. Per-abdominal examination –
E. Central nervous system –
F. Musculoskleletal system –
X1. NIDANAPAREEKSHA
Sl. Nidana
Aharaja nidana
1. Rooksha ahara atisevana
2. Rooksha madya atisevana
3. Anupamamsa atisevana
4. Matsya atisevana
5. Adhyashana
6. Ajeerna
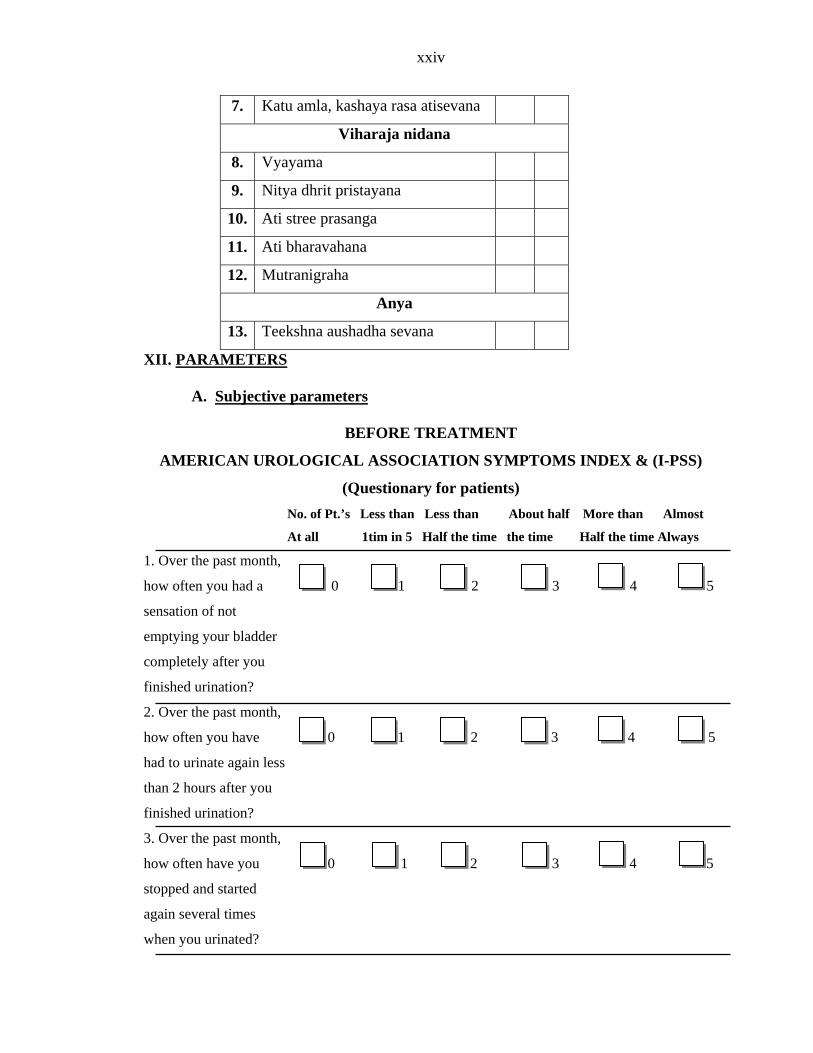
xxiv
7. Katu amla, kashaya rasa atisevana
Viharaja nidana
8. Vyayama
9. Nitya dhrit pristayana
10. Ati stree prasanga
11. Ati bharava hana
12. Mutranigraha
Anya
13. Teekshna aushadha sevana
XII. PARAM EET RS
A. Subjective parameters
ATMEN
OGICAL ASSOCIATION SYMPTOMS INDEX & (I-PSS)
(Questionary for patients) an Less than About half More than Almost
At all time Half the time Always
1. Over the past
how often 5
sensation of not
emptying your bladder
onth,
0 1 2 3 4 5
ou
0 1 2 3 4 5
BEFORE TRE T
AMERICAN UROL
No. of Pt.’s Less th
1tim in 5 Half the time the
month,
you had a 0 1 2 3 4
completely after you
finished urination?
2. Over the past m
how often you have
had to urinate again less
than 2 hours after y
finished urination?
3. Over the past month,
how often have you
stopped and started
again several times
when you urinated?
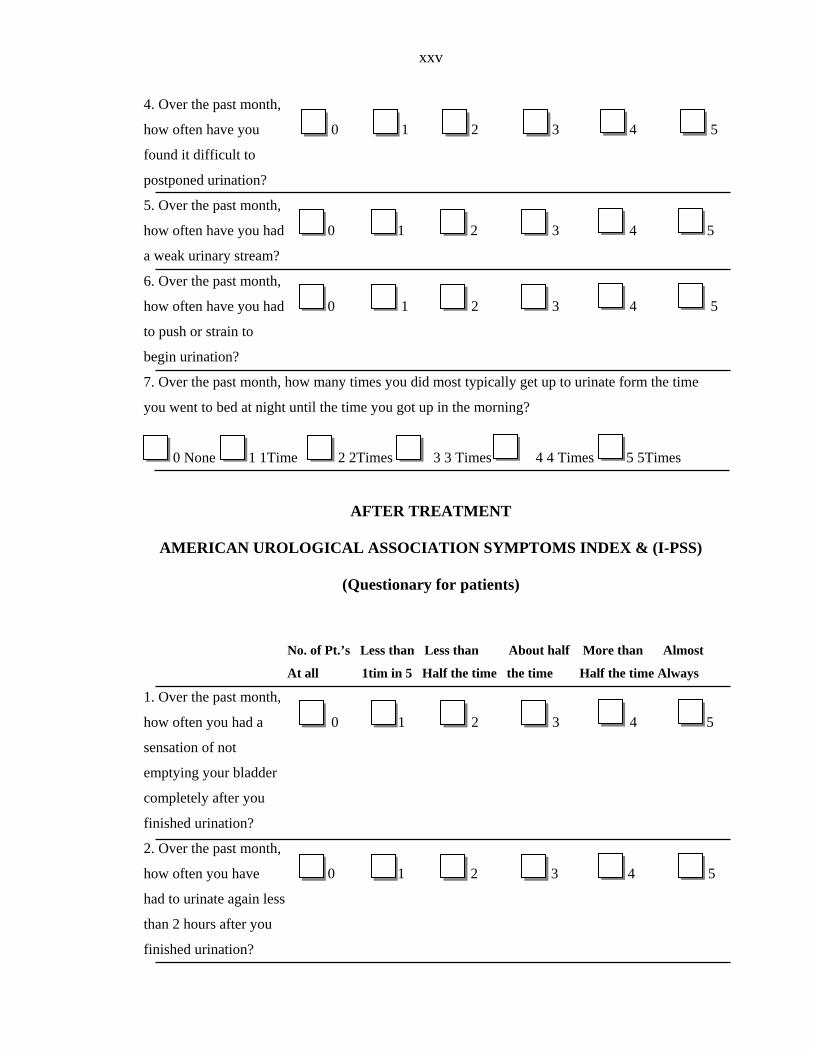
xxv
4. Over the past month,
how often have you 0 1 2 3 4 5
found it difficult to
postponed urination?
h,
0 1 2 3 4 5
?
th,
d 0 1 2 3 4 5
ow many times you did most typically get up to urinate form the time
until the time you got up in the morning?
Time 2 2Times 3 3 Times 4 4 Times 5 5Times
GICAL ASSOCIATION SYMPTOMS INDEX & (I-PSS)
No. of Pt.’s out half More than Almost
1. Over the past month,
how often you had a 0 3 4 5
sensation of not
emptying your bladder
ompletely after you
,
e 0 1 2 3 4 5
5. Over the past mont
how often have you had
a weak urinary stream
6. Over the past mon
how often have you ha
to push or strain to
begin urination?
7. Over the past month, h
you went to bed at night
0 None 1 1
AFTER TREATMENT
AMERICAN UROLO
(Questionary for patients)
Less than Less than Ab
At all 1tim in 5 Half the time the time Half the time Always
1 2
c
finished urination?
2. Over the past month
how often you hav
had to urinate again less
than 2 hours after you
finished urination?
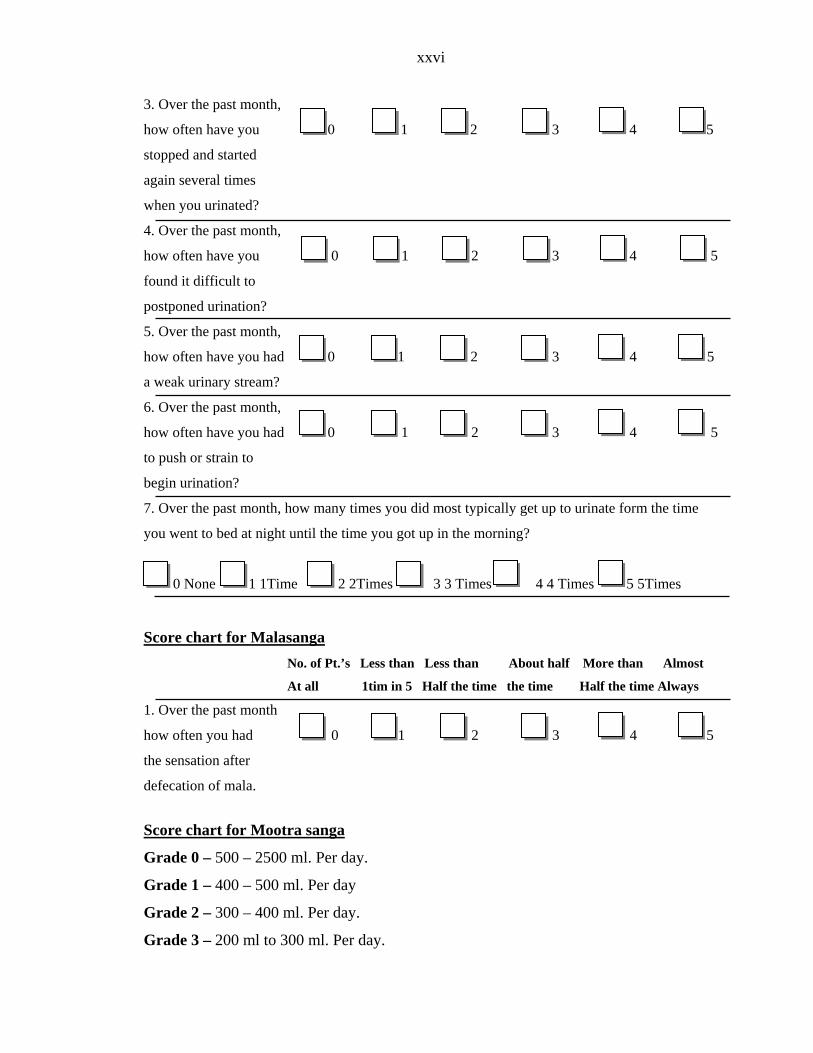
xxvi
3. Over the past month,
how often have you 0 1 2 3 4 5
stopped and started
again several times
when you urinated?
h,
2 3 4 5
?
th,
d 3 4 5
ow many times you did most typically get up to urinate form the time
until the time you got up in the morning?
Time 2 Tim 4 4 Time 5 5Times
4. Over the past month,
how often have you 0 1 2 3 4 5
found it difficult to
postponed urination?
5. Over the past mont
how often have you had 0 1
a weak urinary stream
6. Over the past mon
how often have you ha 0 1 2
to push or strain to
begin urination?
7. Over the past month, h
you went to bed at night
0 None 1 1 2Times 3 3 es s
Score chart for Malasanga No. of Pt.’s Less than Less than About half More than Almost
At all 1tim in 5 Half the time the time Half the time Always
ow often you had 2 3 4 5
defecation of mala.
a sanga
1. Over the past month
h 0 1
the sensation after
Score chart for Mootr
00 ay. 00 ml. Per day
00 ml. Per day.
Grade 3 – 200 ml to 300 ml. Per day.
Grade 0 – 500 – 25 ml. Per d
Grade 1 – 400 – 5
Grade 2 – 300 – 4
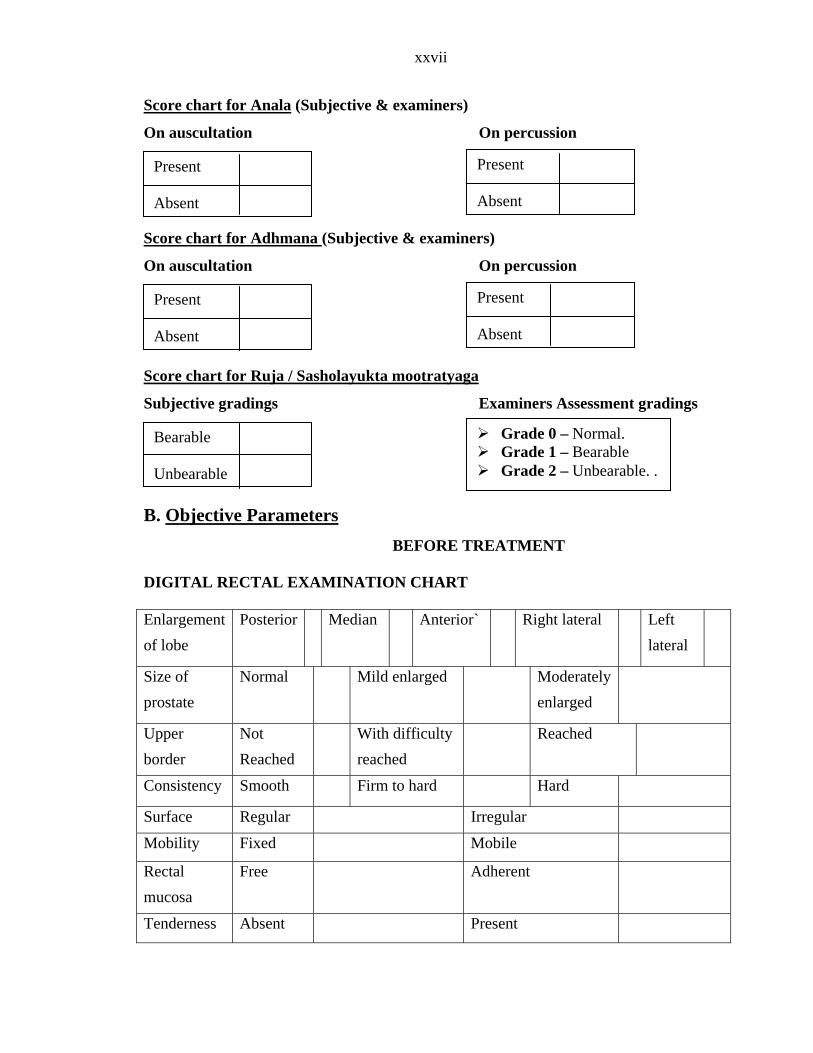
xxvii
Score chart for Anala (Subjective & examiners)
On percussion On auscultation
Score chart for Adhmana (Subjective & examiners)
On percussion
core chart for Ruja / Sasholayukta mootratyaga
On auscultation
S
miners Assessment gradings
Objective Parameters
Subjective gradings Exa
B.
ECTAL EXAMINATION CHART
f lobe Posterior Median ft
lateral
BEFORE TREATMENT DIGITAL R Enlargement o
Anterior` Right lateral Le
Size of Normal prostate
Mild enlarged Moderately ed
enlarg
Upper Not With difficulty Reached border Reached reached
Consistency Smooth t hFirm o ard Hard
Surface Regular Irregular
Mobility obile Fixed M
Rectal mucosa
Free Adherent
Tenderness Present Absent
Present Absent
Present Absent
Present
bsent A
Present Absent
Grade 0 – Normal. Bearable Unbearable
Grade – Bearable 1 Grade 2 – Unbearable. .
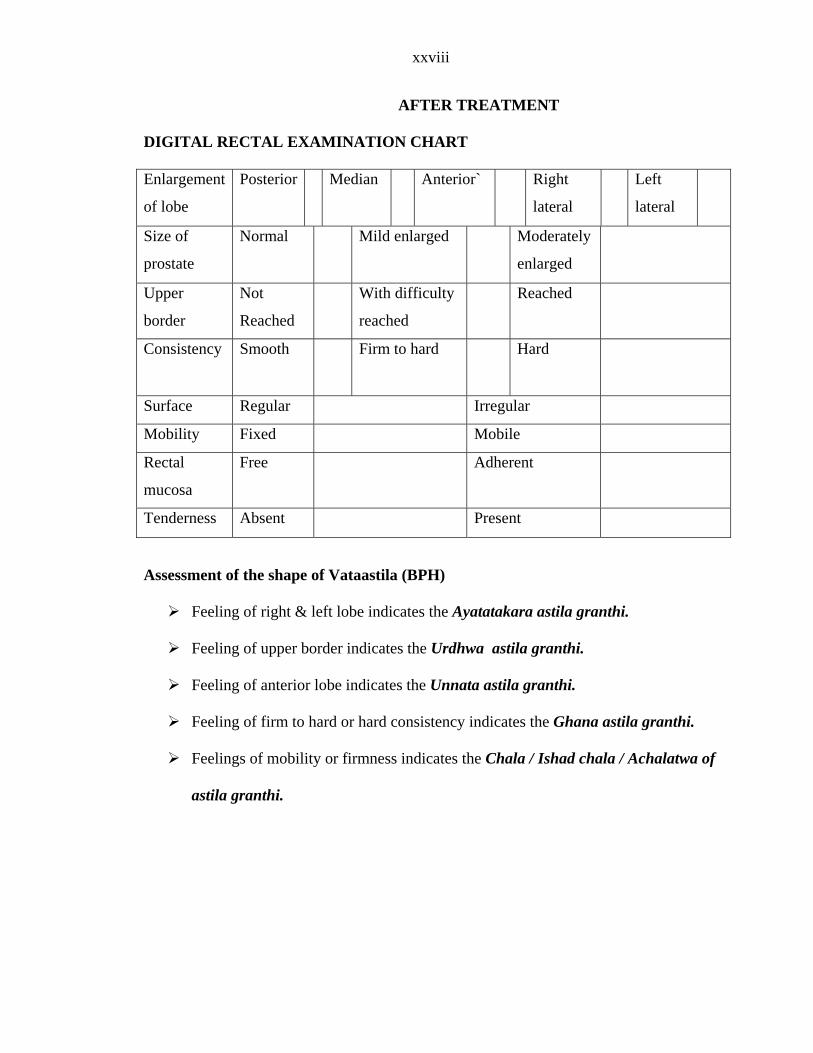
xxviii
AFTER T EATME
RE XAMINATION CHART
ent Median Anterior`
lateral
Left
lateral
R NT DIGITAL CTAL E Enlargem
of lobe
Posterior Right
Size of
prostate
Mild enlarged oderately
Normal M
enlarged
Upper Not With difficulty Reached
border Reached reached
Consistency Smooth h HFirm to ard ard
Surface reguRegular Ir lar
Mobility Fixed Mobil e
Rectal
mucosa
dherFree A ent
Tenderness Absent Present
nt of e of Vataastila (BPH)
ling t & le t lobe indicates the Ayatatakara astila granthi.
eeling of upper border indicates the Urdhwa astila granthi.
ng ior lobe indicates the Unnata astila granthi.
Feeling of firm to hard or hard consistency indicates the Ghana astila granthi.
Feelings of mobility or firmness indicates the Chala / Ishad chala / Achalatwa of
astila granthi.
Assessme the shap
Fee of righ f
F
Feeli of anter
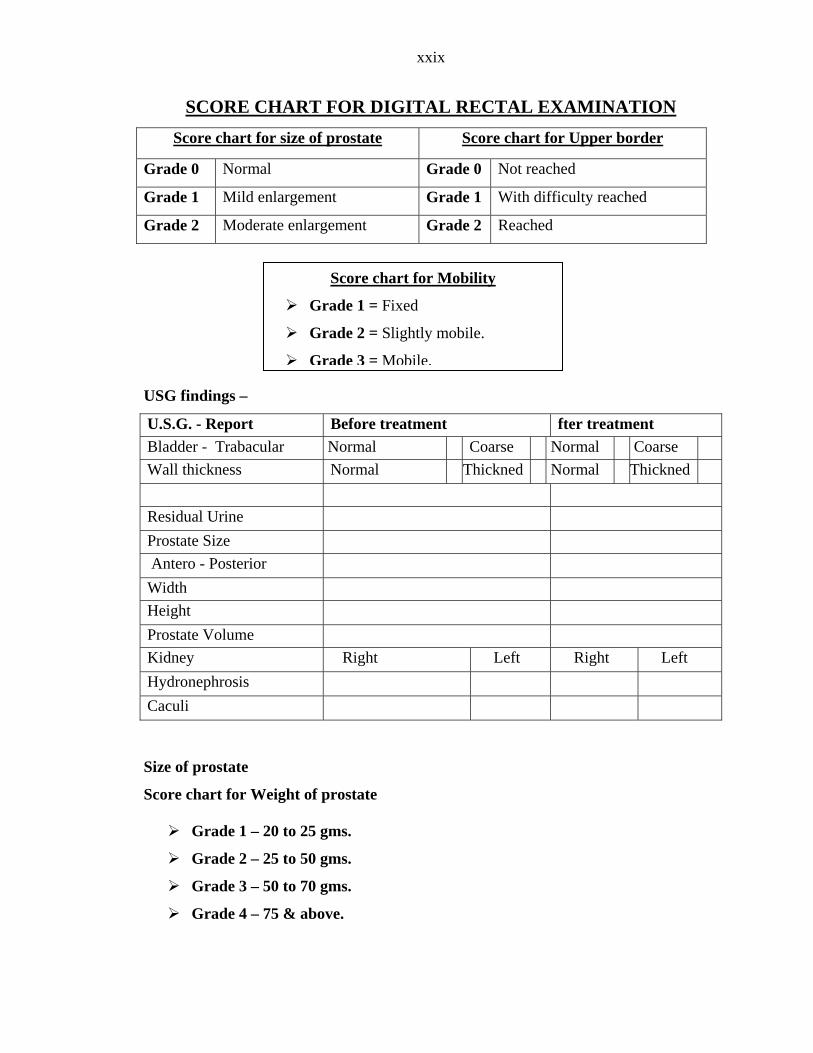
xxix
SCORE CHART FOR DIGITAL RECTAL EXAMINATION Score chart for size of prostate Score chart for Upper border
Grade 0 Normal Grade 0 Not reached
Grade 1 Mild enlargement Grade 1 With difficulty reached
Grade 2 Moderate enlargement Grade 2 Reached
USG findings –
U.S.G. - Report Before treatment fter treatment
Score chart for Mobility
Grade 1 = Fixed
Grade 2 = Slightly mobile.
Grade 3 = Mobile.
Bladder - Trabacular Normal Coarse Normal Coarse Wall thickness Normal Thickned Normal Thickned Residual Urine Prostate Size Antero - Posterior Width Height Prostate Volume Kidney Right Left Right Left Hydronephrosis Caculi Size of prostate
Score chart for Weight of prostate
Grade 1 – 20 to 25 gms.
Grade 2 – 25 to 50 gms.
Grade 3 – 50 to 70 gms.
Grade 4 – 75 & above.
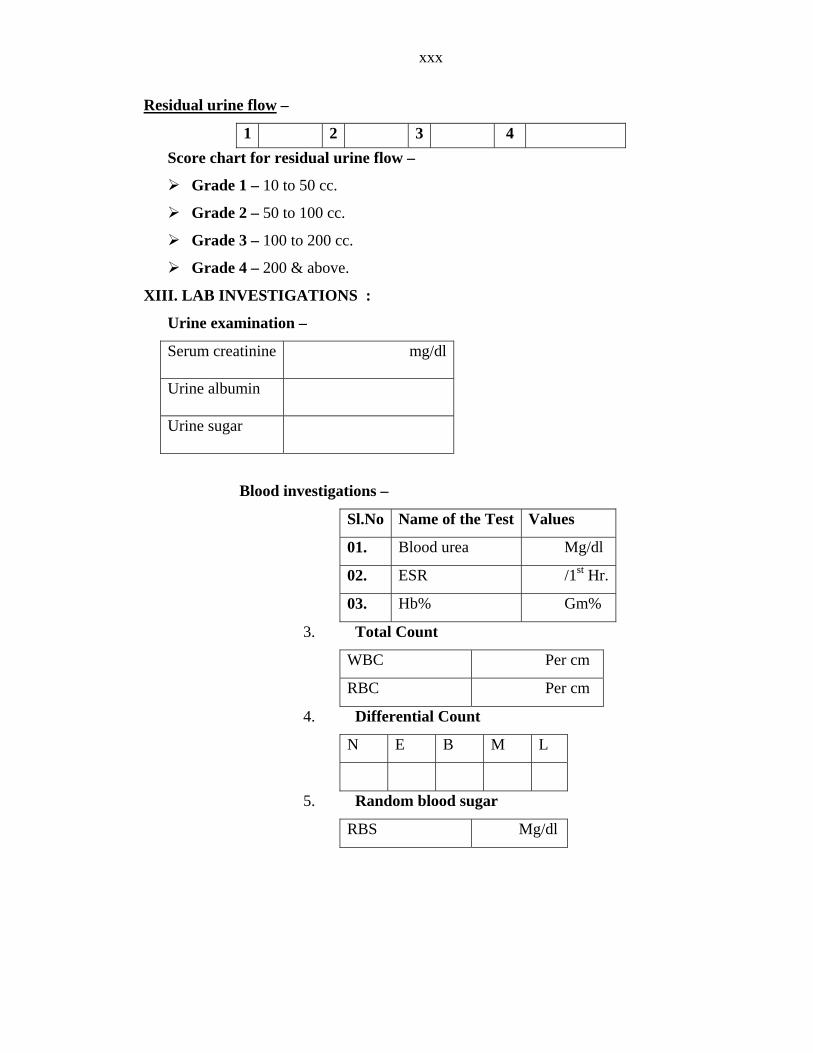
xxx
Residual urine flow –
1 2 3 4 Score ch esidual urine flow –
ad
Grade 3 – 100 to 200 cc.
Grade 4 – 200 & abo
III. LAB IN
Urine exa
Serum creatinine dl
art for r
Gr e 1 – 10 to 50 cc.
Grade 2 – 50 to 100 cc.
ve.
X VESTIGATIONS :
mination –
Dsf df skasdflk asmg/
Urine albumin
Urine sugar
Blood investigations –
Sl.No Name of the Test Values
01. Blood urea Mg/dl
02. ESR /1st Hr.
03. Hb% Gm%
3. Total Count
PWBC er cm
RBC Per cm
4. Differential Coun
N E B M L
t
5. Random blood sugar
S Mg/dl RB
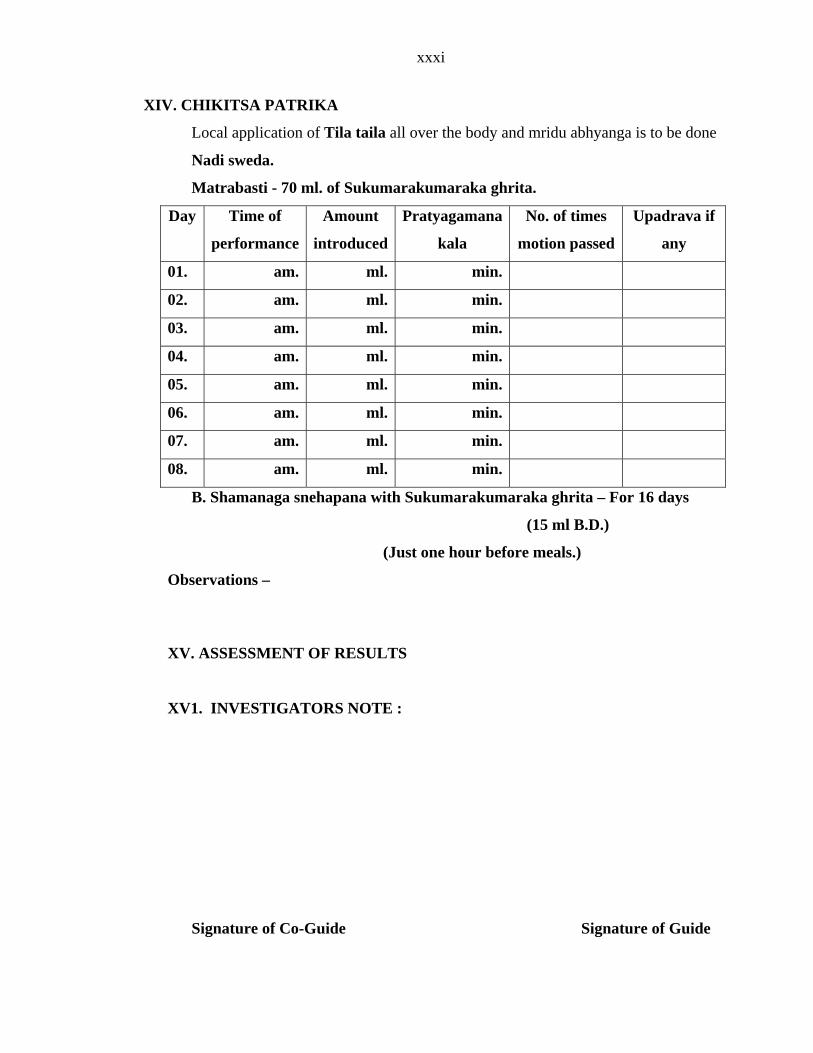
xxxi
XIV. CHIKITSA PATRIKA
Local application of Tila taila all over the body and mridu abhyanga is to be done
Sukumarakumaraka ghrita.
unt
ced
Pratyagamana
kala
No. of times
motion passed
Upadrava if
any
Nadi sweda.
Matrabasti - 70 ml. of
Day Time of Amo
performance introdu
01. am. ml. min.
02. am. ml. min.
03. am. ml. min.
04. am. ml. min.
05. am ml. min. .
06. am. ml. min.
07. am. ml. min.
08. am. ml. min.
B. Sha Sukumarakumaraka ghrita – For 16 days
.D.)
(J before
Observations – XV. ASSESSMENT OF R S
XV1. INVES
Signature of Co-Guide Signature of Guide
managa snehapana with
(15 ml B
ust one hour meals.)
ESULT
TIGATORS NOTE :
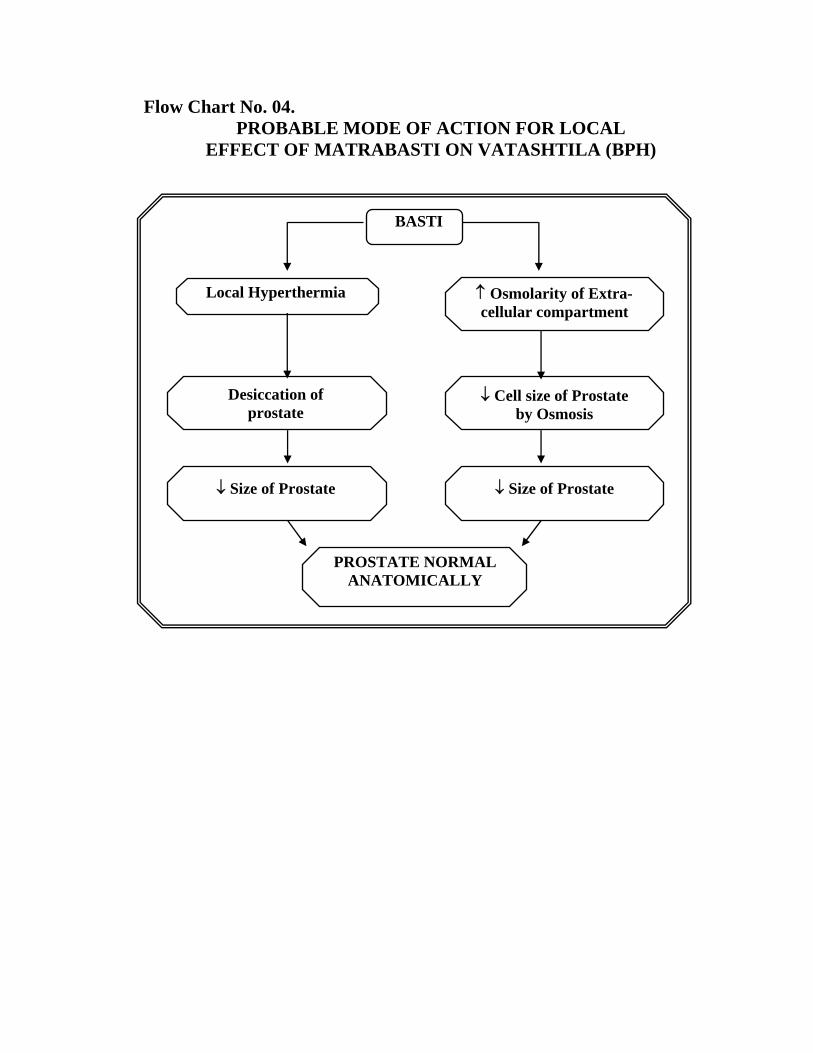
Flow Chart No. 04. PROBABLE MODE OF ACTION FOR LOCAL
EFFECT OF MATRABASTI ON VATASHTILA (BPH)
BASTI
Local Hyperthermia
↑ Osmolarity of Extra- cellular compartment
Desiccation of prostate
↓ Cell size of Prostate by Osmosis
↓ Size of Prostate
↓ Size of Prostate
PROSTATE NORMAL
ANATOMICALLY
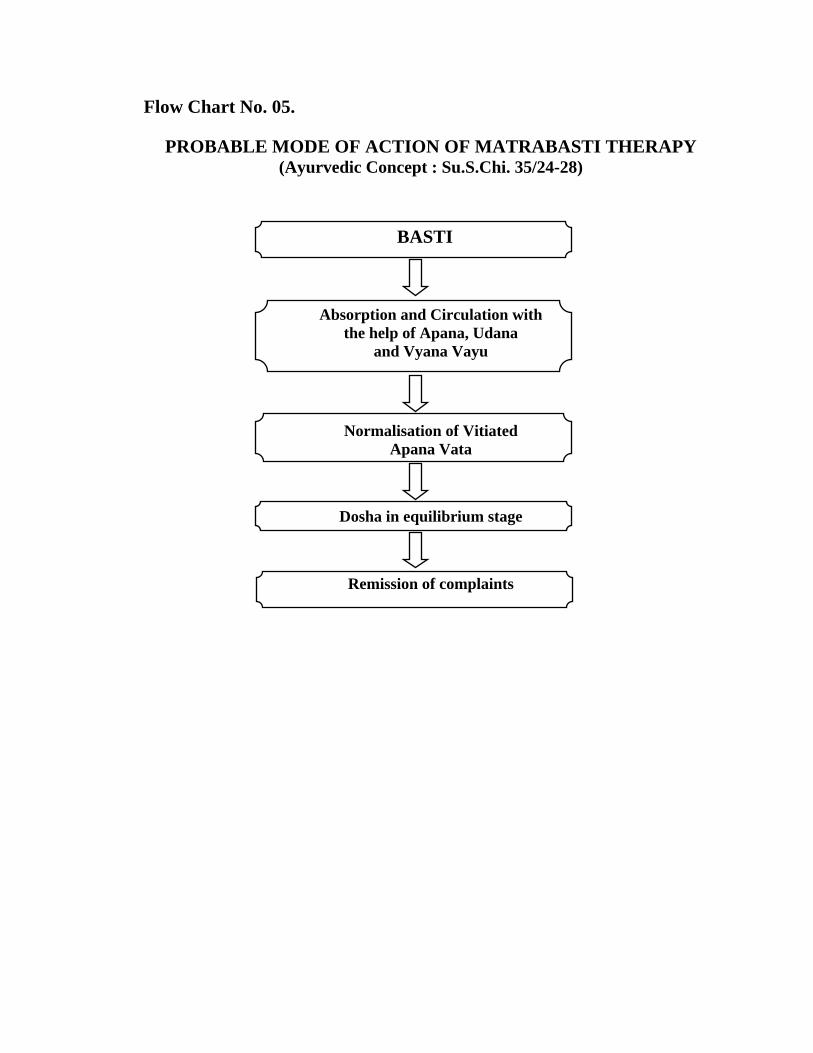
Flow Chart No. 05.
PROBABLE MODE OF ACTION OF MATRABASTI THERAPY (Ayurvedic Concept : Su.S.Chi. 35/24-28)
BASTI
Absorption and Circulation with the help of Apana, Udana
and Vyana Vayu
Normalisation of Vitiated Apana Vata
Dosha in equilibrium stage
Remission of complaints
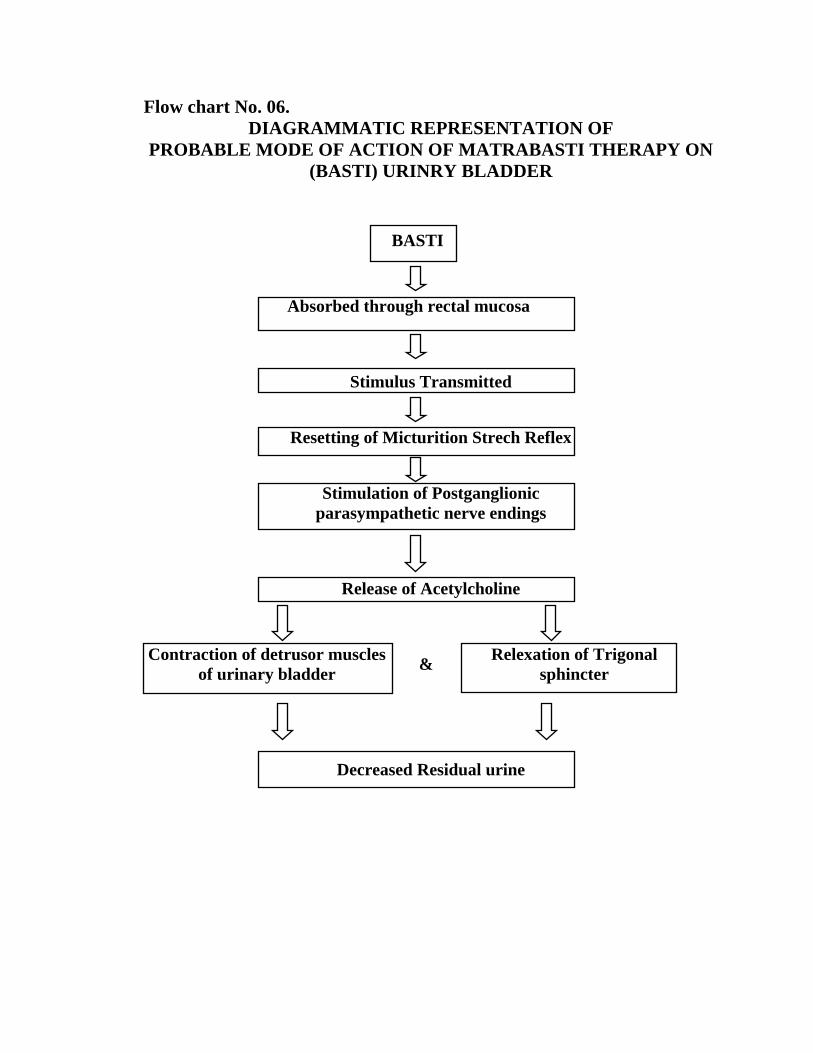
Flow chart No. 06. DIAGRAMMATIC REPRESENTATION OF
PROBABLE MODE OF ACTION OF MATRABASTI THERAPY ON (BASTI) URINRY BLADDER
BASTI
Absorbed through rectal mucosa
Stimulus Transmitted
Resetting of Micturition Strech Reflex
Stimulation of Postganglionic
parasympathetic nerve endings
Release of Acetylcholine
Contraction of detrusor muscles of urinary bladder
&
Relexation of Trigonal
sphincter
Decreased Residual urine





























