Embed Size (px)
Citation preview

Mechanical Venti lationand Bronchopulmonary
DysplasiaMartin Keszler, MDa,*, Guilherme Sant’Anna, MD, PhD, FRCPCb
KEYWORDS
� Mechanical ventilation � Bronchopulmonary dysplasia� Ventilator-associated lung injury � Volume-targeted ventilation� Lung-protective ventilation
KEY POINTS
� Mechanical ventilation (MV) is an important potentially modifiable risk factor for the devel-opment of bronchopulmonary dysplasia (BPD).
� Effective use of noninvasive respiratory support reduces the risk of lung injury.
� Lung volume recruitment and avoidance of excessive tidal volume (VT) are key elements oflung-protective ventilation strategies.
� Avoidance of oxidative stress, less invasive methods of surfactant administration, andhigh-frequency ventilation (HFV) are also important factors in lung injury prevention.
INTRODUCTION
MV is undoubtedly one of the key advances in neonatal care. Even in this era of nonin-vasive respiratory support, MV remains a mainstay of therapy in the extremely pretermpopulation. Data from the Neonatal Research Network show that 89% of extremelylow birth weight (ELBW) infants were treated with MV during the first day of life.1
Among survivors, almost 95% were invasively ventilated at some point during theirhospital stay. In the Surfactant, Positive Pressure, and Oxygenation Randomized Trial
Conflict of Interest Statement: Dr M. Keszler has been a consultant to Draeger Medical. He hasreceived honoraria for lectures and research grant support from the company. Dr M. Keszleralso chairs the scientific advisory board of Discovery Laboratories and the Data Safety Moni-toring Board of a clinical trial supported by Medipost America. None of the companies hadany input into the content of this article.a Department of Pediatrics, Women and Infants Hospital of Rhode Island, Alpert MedicalSchool of Brown University, 101 Dudley Street, Providence, RI 02905, USA; b Department of Pe-diatrics, Neonatal Division, Montreal Children’s Hospital, McGill University, 1001 Decarie Boule-vard, Room B05.2711, Montreal, Quebec H4A 3J1, Canada* Corresponding author.E-mail address: [email protected]
Clin Perinatol 42 (2015) 781–796http://dx.doi.org/10.1016/j.clp.2015.08.006 perinatology.theclinics.com0095-5108/15/$ – see front matter � 2015 Elsevier Inc. All rights reserved.
Keszler & Sant’Anna782
(SUPPORT), 83% of the ELBW infants initially assigned to noninvasive supportrequired endotracheal intubation and MV at some point.2 The CPAP or Intubation trialenrolled infants between 25 and 28 weeks of gestational age only if they had adequaterespiratory effort at birth, but even in this group, 46% of the infants assigned to nonin-vasive support required endotracheal intubation and MV.3
Although often lifesaving, MV has many untoward effects. Although this articlefocuses on the adverse effects of MV on the lungs, protracted MV is also stronglyassociated with adverse neurologic outcomes.1 In preterm baboons, 5 days of electiveMV resulted in greater degree of brain injury compared with ventilation for 1 day.4
Cohort data from the Neonatal Research Network show that each week of additionalMV is associated with a significant increase in the likelihood of neurodevelopmentalimpairment.1 Additionally, the endotracheal tube acts as a foreign body, quicklybecoming colonized and acting as a portal of entry for pathogens, increasing therisk of ventilator-associated pneumonia and late-onset sepsis.5 For these reasons,avoidance of MV in favor of noninvasive respiratory support is seen as perhaps themost important step in preventing neonatal morbidity.BPD was originally described by Northway and colleagues6 more than 45 years ago
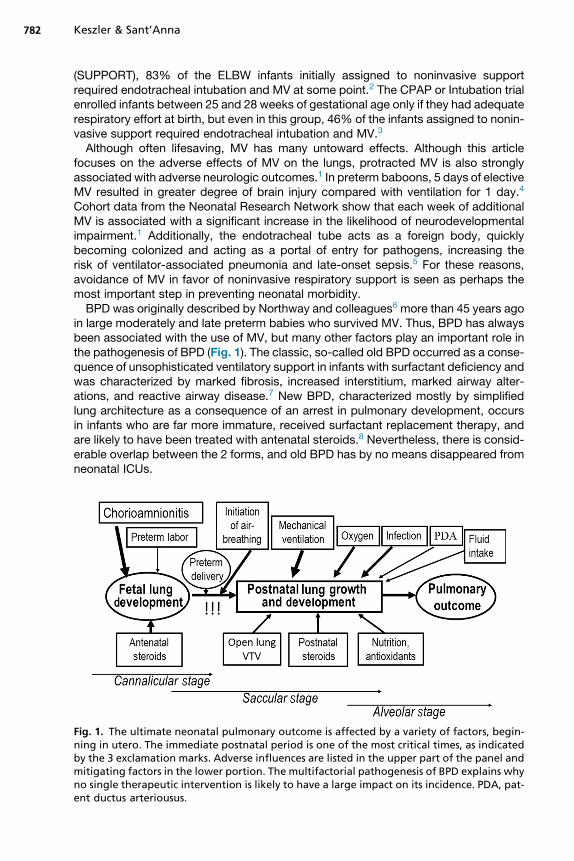
in large moderately and late preterm babies who survived MV. Thus, BPD has alwaysbeen associated with the use of MV, but many other factors play an important role inthe pathogenesis of BPD (Fig. 1). The classic, so-called old BPD occurred as a conse-quence of unsophisticated ventilatory support in infants with surfactant deficiency andwas characterized by marked fibrosis, increased interstitium, marked airway alter-ations, and reactive airway disease.7 New BPD, characterized mostly by simplifiedlung architecture as a consequence of an arrest in pulmonary development, occursin infants who are far more immature, received surfactant replacement therapy, andare likely to have been treated with antenatal steroids.8 Nevertheless, there is consid-erable overlap between the 2 forms, and old BPD has by no means disappeared fromneonatal ICUs.
Fig. 1. The ultimate neonatal pulmonary outcome is affected by a variety of factors, begin-ning in utero. The immediate postnatal period is one of the most critical times, as indicatedby the 3 exclamation marks. Adverse influences are listed in the upper part of the panel andmitigating factors in the lower portion. The multifactorial pathogenesis of BPD explains whyno single therapeutic intervention is likely to have a large impact on its incidence. PDA, pat-ent ductus arteriousus.
Ventilation and Bronchopulmonary Dysplasia 783
WHAT IS VENTILATOR-ASSOCIATED LUNG INJURY?
The huge number of articles published since the first description of ventilator-associated lung injury (VALI) highlights its importance and the incomplete understand-ing of this complex subject. The central role of MV and oxygen exposure in VALI andsubsequent development of BPD have been recognized since the early days ofneonatal medicine. In 1975, Alistair Philip described the etiology of BPD as “oxygenplus pressure plus time.”9 Although fundamentally this concept still holds, it has sincebeen refined by recognizing that excessive volume, rather than pressure, is the mostimportant factor that contributes to VALI, a concept that has been slow to gain com-plete acceptance, despite strong evidence in its favor.Many terms have been coined to describe the mechanism of lung injury in VALI.
Barotrauma refers to damage caused by pressure. The conviction that pressure isthe key determinant of lung injury has fostered a deeply ingrained “barophobia,”causing clinicians to focus on limiting inflation pressure, sometimes to the point ofprecluding adequate ventilation. There is convincing evidence, however, that highpressure by itself, without correspondingly high volume, does not result in lung injury.Rather, injury related to high inflation pressure is mediated through the tissue stretchresulting from excessive VT. Dreyfuss and colleagues10 demonstrated more than20 years ago that severe acute lung injury occurred in small animals ventilated withlarge VT, regardless of whether that volume was generated by positive or negativeinflation pressure. In contrast, animals exposed to the same high inflation pressurebut with an elastic bandage over the chest and abdomen to limit VT delivery experi-enced much less acute lung damage. Hernandez and colleagues11 similarly showedthat animals exposed to pressure as high as 45 cm H2O did not show evidence ofacute lung injury when their chest and abdomen were enclosed in a plaster cast.Volutrauma refers to injury caused by overdistention and excessive stretch of tissues,which leads to disruption of alveolar and small airway epithelium, resulting in acuteedema; outpouring of proteinaceous exudate; and release of proteases, cytokines,and chemokines, which in turn leads to activation of macrophages and invasion ofactivated neutrophils. Collectively, this complex process is referred to as biotrauma.Another important concept is that of atelectrauma, or lung damage caused by tidalventilation in the presence of atelectasis.12 Atelectrauma exerts lung injury via severalmechanisms. The portion of the lungs that remains atelectatic has increased surfac-tant turnover and high critical opening pressure. There are shear forces at the bound-ary between aerated and atelectatic parts of the lung, leading to structural damage.Ventilation of injured lungs using inadequate end-expiratory pressure results inrepeated alveolar collapse and expansion (RACE), which rapidly leads to lung injury.Perhaps most importantly, when a large portion of the lungs is atelectatic, whateverVT is entering the lungs preferentially enters the aerated portion of the lung, which ismore compliant than the atelectatic lung with its high critical opening pressure(Laplace’s law). This maldistribution of VT leads to overdistention of that portion ofthe lungs and regional volutrauma. Thus, it becomes clear that the risk of lung damagefrom MV is multifactorial and cannot be linked to any single variable.The key concept regarding VALI is that the initiating event is biophysical injury from
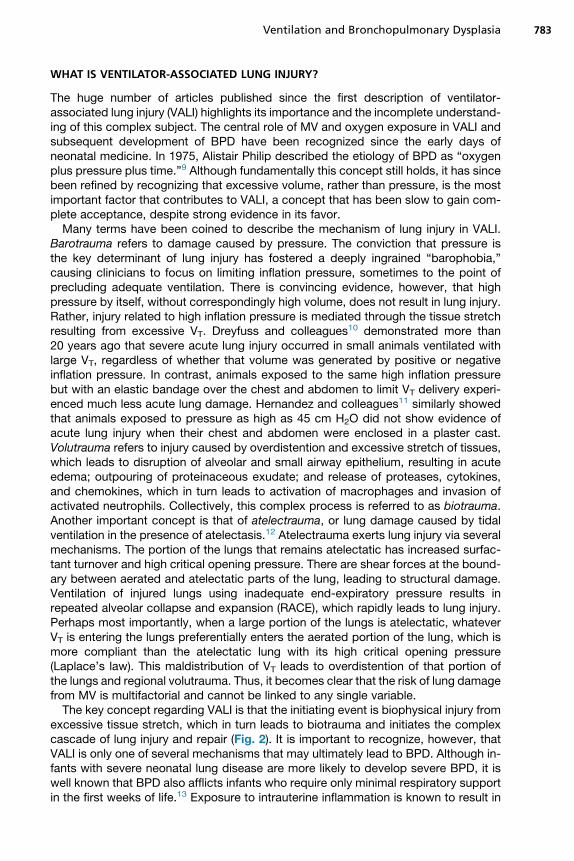
excessive tissue stretch, which in turn leads to biotrauma and initiates the complexcascade of lung injury and repair (Fig. 2). It is important to recognize, however, thatVALI is only one of several mechanisms that may ultimately lead to BPD. Although in-fants with severe neonatal lung disease are more likely to develop severe BPD, it iswell known that BPD also afflicts infants who require only minimal respiratory supportin the first weeks of life.13 Exposure to intrauterine inflammation is known to result in
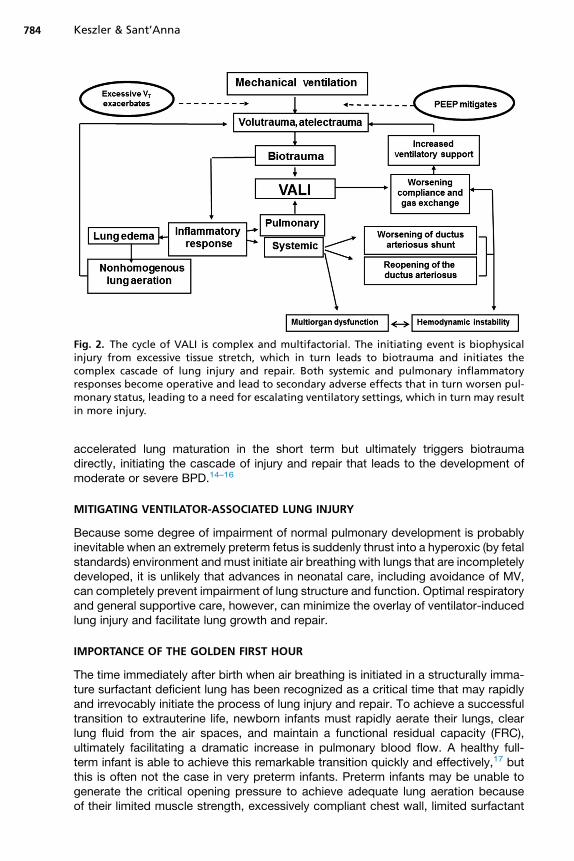
Fig. 2. The cycle of VALI is complex and multifactorial. The initiating event is biophysicalinjury from excessive tissue stretch, which in turn leads to biotrauma and initiates thecomplex cascade of lung injury and repair. Both systemic and pulmonary inflammatoryresponses become operative and lead to secondary adverse effects that in turn worsen pul-monary status, leading to a need for escalating ventilatory settings, which in turn may resultin more injury.
Keszler & Sant’Anna784
accelerated lung maturation in the short term but ultimately triggers biotraumadirectly, initiating the cascade of injury and repair that leads to the development ofmoderate or severe BPD.14–16
MITIGATING VENTILATOR-ASSOCIATED LUNG INJURY
Because some degree of impairment of normal pulmonary development is probablyinevitable when an extremely preterm fetus is suddenly thrust into a hyperoxic (by fetalstandards) environment andmust initiate air breathing with lungs that are incompletelydeveloped, it is unlikely that advances in neonatal care, including avoidance of MV,can completely prevent impairment of lung structure and function. Optimal respiratoryand general supportive care, however, can minimize the overlay of ventilator-inducedlung injury and facilitate lung growth and repair.
IMPORTANCE OF THE GOLDEN FIRST HOUR
The time immediately after birth when air breathing is initiated in a structurally imma-ture surfactant deficient lung has been recognized as a critical time that may rapidlyand irrevocably initiate the process of lung injury and repair. To achieve a successfultransition to extrauterine life, newborn infants must rapidly aerate their lungs, clearlung fluid from the air spaces, and maintain a functional residual capacity (FRC),ultimately facilitating a dramatic increase in pulmonary blood flow. A healthy full-term infant is able to achieve this remarkable transition quickly and effectively,17 butthis is often not the case in very preterm infants. Preterm infants may be unable togenerate the critical opening pressure to achieve adequate lung aeration becauseof their limited muscle strength, excessively compliant chest wall, limited surfactant
Ventilation and Bronchopulmonary Dysplasia 785
pool, and incomplete lung development. Additionally, their excessively compliantchest wall fails to sustain any lung aeration that may have been achieved spontane-ously or with positive pressure ventilation. They may also be unable to generatesufficient negative intrathoracic pressure to effectively move lung fluid from the airspaces to the interstitium, lymphatics and veins. Consequently, subsequent tidalbreathing, whether spontaneous or generated by positive pressure ventilation, takesplace in lungs that are still partially fluid filled and partially atelectatic. This situationleads to maldistribution of the VT to a fraction of the preterm lung, which leads tovolutrauma even when the VT is in a safe physiologic range.
POSITIVE END-EXPIRATORY PRESSURE IN THE DELIVERY ROOM
The use of positive end-expiratory pressure (PEEP)/continuous positive airway pres-sure (CPAP) during initial stabilization of preterm infants mitigates the effect of exces-sively compliant chest wall and surfactant deficiency by stabilizing alveoli during theexpiratory phase and has been shown to help establish FRC. Siew and colleagues18
demonstrated the beneficial effects of PEEP by using phase-contrast radiography inpreterm rabbits, showing that virtually no FRC was established after several minuteswhen PPV was delivered without PEEP. In contrast, FRC was rapidly establishedwhen 5 cm H2O of PEEP was applied.Both the Neonatal Resuscitation Program and International Liaison Committee on
Resuscitation guidelines state, “PEEP is likely to be beneficial during initial stabiliza-tion of apneic preterm infants and should be used if suitable equipment is avail-able.”19,20 The physiologic rationale and experimental evidence from preclinicalstudies is so persuasive that this practice has become the standard of care in muchof the developed world. Provision of end-expiratory pressure alone, however, maynot entirely address the inadequate muscle strength of the preterm infant or help clearlung fluid sufficiently rapidly to avoid regional volutrauma and atelectrauma, which canoccur in minutes.
SUSTAINED INFLATION
Because liquid hasmuch greater viscosity than air, resistance to moving liquid throughsmall airways is orders of magnitude higher than that for air, making the time constantsrequired to clear fluid from the airways much longer. Recognition of these factorssupports the concept that a prolonged (sustained) inflation applied soon after birthshould be more effective than short inflations in clearing lung fluid in the first minutesof life. Theoretically, ensuring effective lung recruitment with even distribution of VT
immediately after birth should reduce VALI.Despite a substantial body of evidence that supports the theoretic advantages of
sustained inflation in extremely preterm infants,21 the evidence that this measurecan substantially reduce VALI remains inconclusive.22–24 Additionally, the most appro-priate way to deliver an sustained inflation is unclear. Therefore, the procedure cannotcurrently be recommended outside of well-controlled clinical trials.
HYPEROXIC INJURY
Preterm infants have immature antioxidant defenses, making them more susceptibleto oxidative stress from relative or absolute hyperoxia. Several studies of early respi-ratory management in the delivery room evaluated whether reducing oxygen exposureresults in improved respiratory outcomes. A single-center randomized clinical trial(RCT) in infants born at 24 to 28 weeks’ gestation demonstrated less oxidative stress,
Keszler & Sant’Anna786
lower proinflammatory cytokine levels, and a lower incidence of BPD (15.4% vs31.7%; P<.05) in infants resuscitated with a fraction of inspired oxygen (FIO2) of0.30, compared with 0.90, and then titrated to achieve target oxygen saturation asmeasured by pulse oximetry (SpO2) levels.
25 Kapadia and colleagues26 comparedrates of BPD in infants with gestational age of 24 to 34 weeks randomized to receiveeither 21% or 100% oxygen, which was then titrated to achieve the Neonatal Resus-citation Program recommended SpO2 target of 85% to 94%. BPD rates were lower inthe infants initially resuscitated with room air (7% vs 25%; P<.04). In contrast, theRoom-Air Versus Oxygen Administration for Resuscitation of Preterm Infants studyfound no difference in BPD rates between preterm infants treated with room air,despite randomizing greater than 1000 infants.27 This may be in part because initiatingresuscitation with room air in very preterm infants often resulted in inadequateresponse and a rapid increase to 100% oxygen. Therefore, the best approach prob-ably is to initiate support with FIO2 of 0.30 and avoid an excessively rapid increase,recognizing that several minutes are needed for SpO2 to reach 90%.Although avoidance of oxidative stress is desirable, it has turned out to be a more
complicated issue than was initially thought. A series of RCTs that compared lowerversus higher SpO2 targets (SUPPORT, Canadian Oxygen Trial, and Benefits ofOxygen Saturation Targeting II) failed to show a significant reduction in BPD and,unexpectedly showed a higher mortality rate in the low SpO2 target group.28–30 Arecent meta-analysis of those trials confirmed a significant increase in mortality andnecrotizing enterocolitis and a decrease in the rate of severe retinopathy of prematu-rity in low compared with high oxygen saturation target infants.31 No differences inphysiologic BPD, brain injury, or patent ductus arteriosus were noted between thegroups. Based on these results, definitive recommendations regarding saturation tar-gets during continued care of preterm infants are difficult to make. Nevertheless, itseems prudent to target functional SpO2 at 90% to 95% in infants with gestationalage less than 28 weeks until 36 weeks’ postmenstrual age. Most NICUs have revisedtheir saturation targets to be close to this higher range, with alarm limits slightly wider,or approximately 88% to 97%. Anecdotally, this change has again increased the riskof significant retinopathy of prematurity.
NONINVASIVE RESPIRATORY SUPPORT
There is little doubt that avoiding MV reduces iatrogenic lung injury superimposed onthe inevitable arrest of pulmonary development. Although earlier cohort comparisonsof CPAP or MV suggested a large reduction in the risk of BPD,32 a series of morerecent RCTs showed a much more modest benefit of avoiding MV. A meta-analysisof 4 recent RCTs2,3,33,34 that enrolled nearly 2800 preterm infants showed that BPDrates were not significantly reduced by the use of different types of nasal CPAP(32.4% vs 34.0%).35 A modest benefit with the use of CPAP, however, was demon-strated for the combined outcome of death or BPD with a reduction of approximately10% (relative risk [RR] 0.91; 95% CI, 0.84–0.99); with 1 additional infant surviving to36 weeks without BPD for every 25 babies treated with nasal CPAP in the deliveryroom rather than being intubated. This latter finding is more important because deathand BPD are competing outcomes and, therefore, should be evaluated in combina-tion. There was also a significant decrease in the duration of MV and a nonsignificanttrend toward shorter duration of oxygen exposure with early CPAP in the 2 largesttrials.2,3
Nasal intermittent positive pressure ventilation may be able to augment an immatureinfant’s inadequate respiratory effort without the complications associated with
Ventilation and Bronchopulmonary Dysplasia 787
endotracheal intubation.36 In theory, this approach offers the benefit of avoiding theuse of an endotracheal tube, thus reducing the incidence of VALI and ventilator-associated pneumonia and avoiding the contribution of postnatal inflammatoryresponse to the development of BPD.37 Although a meta-analysis of several small sin-gle center studies concluded that nasal intermittent positive pressure ventilation wassuperior to CPAP,38 a recent large pragmatic multinational RCT in infants with birthweight less than 1000 g failed to substantiate these benefits, showing no reductionin BPD, mortality, or the combined outcome.39
LESS INVASIVE SURFACTANT ADMINISTRATION
Traditionally, the avoidance of intubation and MV and the use of noninvasive respira-tory support have meant a trade-off between the presumed benefits of this approachand the well documented benefits of surfactant replacement therapy. Early surfactanttrials suggested that prophylactic surfactant administration was superior to rescueuse40; thus, some clinicians still intubate very premature infants in the delivery roomfor the sole purpose of administering surfactant. It must be recognized, however,that most surfactant RCTs were done many years ago in a different population ofinfants and with a less sophisticated approach to delivery room stabilization. A recentmeta-analysis comparing prophylactic versus selective surfactant use in the modernera concluded that a prophylactic approach was associated with increased risk ofBPD (RR 1.13; 95% CI, 1.00–1.28).41
In recent years, a variety of approaches have been proposed to preserve thebenefits of avoiding delivery room intubation while still providing surfactant therapy.These include the intubation-surfactant-extubation approach (INSURE) and severalmethods of administering surfactant through small catheters under direct laryngo-scopic visualization.33,42–45 Although these techniques avoid endotracheal intubation,they still require direct laryngoscopy, typically without sedation and thus are still inva-sive. Administration of nebulized surfactant during CPAP is a potentially attractiveapproach that is currently under investigation.46
LUNG-PROTECTIVE STRATEGIES OF MECHANICAL VENTILATION
There are numerous modes and modalities of MV and little high-quality evidence toguide clinicians in selecting the optimal method. A detailed discussion of thesetechniques is beyond the scope of this article; interested readers are referred toseveral recent reviews of the topic.47,48 Key principles of lung-protective strategies,however, are outlined.
Volume-targeted Ventilation
Pressure-controlled ventilation (PCV) became the standard mode of ventilation in ne-onates because early attempts at volume-controlled ventilation proved ineffective insmall preterm infants using equipment available at the time. PCV remains theacceptedmode of ventilation in neonatal ICUs because of its simplicity, ability to venti-late despite a large endotracheal tube leak, and improved intrapulmonary gas distribu-tion due to the decelerating gas flow pattern.49,50 Perhaps most importantly, clinicianscontinue to hold onto the belief that directly controlling peak inflation pressure isimportant. The danger of using PCV is that VT varies with changes in lung compliance.Rapid improvement in compliance may occur rapidly in the immediate postnatalperiod as a result of resorption of lung fluid, recruitment of optimal lung volume, andsurfactant replacement therapy, leading to hyperventilation and volutrauma fromexcessively large VT. Insufficient VT may develop because of decreasing lung
Keszler & Sant’Anna788
compliance, increasing airway resistance, airway obstruction, air-trapping, and/ordecreased spontaneous respiratory effort. Inadequate VT leads to hypercapnia,tachypnea, increased work of breathing and oxygen consumption, agitation, fatigue,atelectasis/atelectrauma, and possibly increased risk of intraventricular hemorrhage(IVH) and thus should also be avoided. Low VT also leads to inefficient gas exchangedue to an increased dead space:VT ratio. These factors suggest that tight control of VT
delivery during MV is highly desirable and are the reason volume-controlled ventilationremains the standard of care in adult and pediatric respiratory support.There are many ways to regulate VT delivery during MV. Although there are impor-
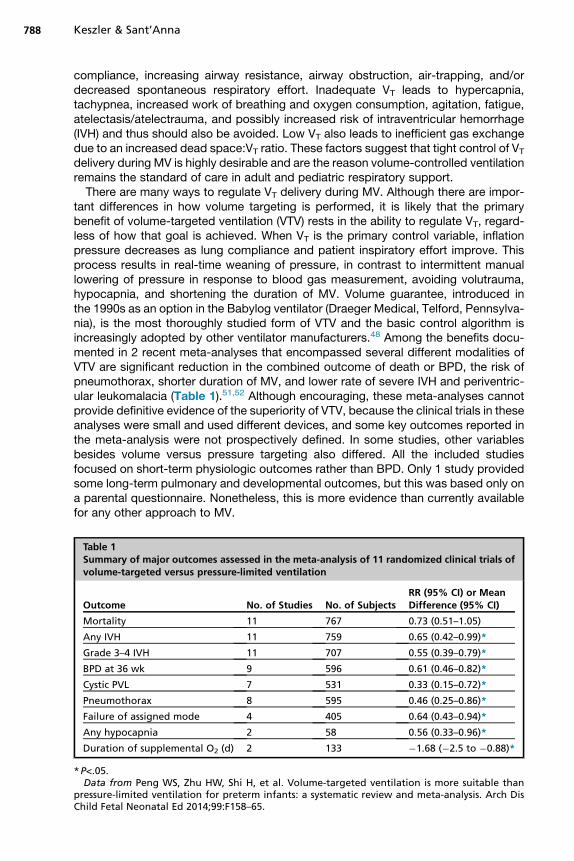
tant differences in how volume targeting is performed, it is likely that the primarybenefit of volume-targeted ventilation (VTV) rests in the ability to regulate VT, regard-less of how that goal is achieved. When VT is the primary control variable, inflationpressure decreases as lung compliance and patient inspiratory effort improve. Thisprocess results in real-time weaning of pressure, in contrast to intermittent manuallowering of pressure in response to blood gas measurement, avoiding volutrauma,hypocapnia, and shortening the duration of MV. Volume guarantee, introduced inthe 1990s as an option in the Babylog ventilator (Draeger Medical, Telford, Pennsylva-nia), is the most thoroughly studied form of VTV and the basic control algorithm isincreasingly adopted by other ventilator manufacturers.48 Among the benefits docu-mented in 2 recent meta-analyses that encompassed several different modalities ofVTV are significant reduction in the combined outcome of death or BPD, the risk ofpneumothorax, shorter duration of MV, and lower rate of severe IVH and periventric-ular leukomalacia (Table 1).51,52 Although encouraging, these meta-analyses cannotprovide definitive evidence of the superiority of VTV, because the clinical trials in theseanalyses were small and used different devices, and some key outcomes reported inthe meta-analysis were not prospectively defined. In some studies, other variablesbesides volume versus pressure targeting also differed. All the included studiesfocused on short-term physiologic outcomes rather than BPD. Only 1 study providedsome long-term pulmonary and developmental outcomes, but this was based only ona parental questionnaire. Nonetheless, this is more evidence than currently availablefor any other approach to MV.
Table 1Summary of major outcomes assessed in the meta-analysis of 11 randomized clinical trials ofvolume-targeted versus pressure-limited ventilation
Outcome No. of Studies No. of SubjectsRR (95% CI) or MeanDifference (95% CI)
Mortality 11 767 0.73 (0.51–1.05)
Any IVH 11 759 0.65 (0.42–0.99)*
Grade 3–4 IVH 11 707 0.55 (0.39–0.79)*
BPD at 36 wk 9 596 0.61 (0.46–0.82)*
Cystic PVL 7 531 0.33 (0.15–0.72)*
Pneumothorax 8 595 0.46 (0.25–0.86)*
Failure of assigned mode 4 405 0.64 (0.43–0.94)*
Any hypocapnia 2 58 0.56 (0.33–0.96)*
Duration of supplemental O2 (d) 2 133 �1.68 (�2.5 to �0.88)*
*P<.05.Data from Peng WS, Zhu HW, Shi H, et al. Volume-targeted ventilation is more suitable than
pressure-limited ventilation for preterm infants: a systematic review and meta-analysis. Arch DisChild Fetal Neonatal Ed 2014;99:F158–65.
Ventilation and Bronchopulmonary Dysplasia 789
Importance of the Open Lung Strategy
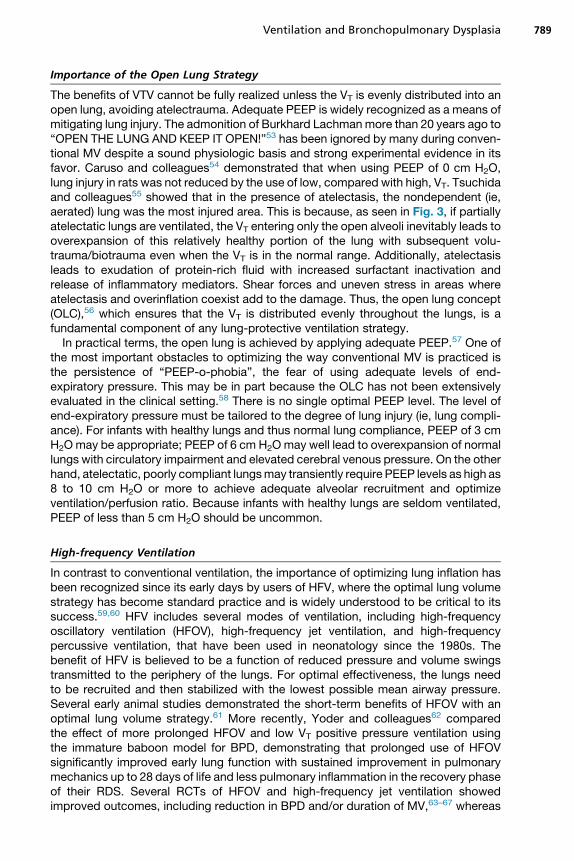
The benefits of VTV cannot be fully realized unless the VT is evenly distributed into anopen lung, avoiding atelectrauma. Adequate PEEP is widely recognized as a means ofmitigating lung injury. The admonition of Burkhard Lachmanmore than 20 years ago to“OPEN THE LUNG AND KEEP IT OPEN!”53 has been ignored by many during conven-tional MV despite a sound physiologic basis and strong experimental evidence in itsfavor. Caruso and colleagues54 demonstrated that when using PEEP of 0 cm H2O,lung injury in rats was not reduced by the use of low, compared with high, VT. Tsuchidaand colleagues55 showed that in the presence of atelectasis, the nondependent (ie,aerated) lung was the most injured area. This is because, as seen in Fig. 3, if partiallyatelectatic lungs are ventilated, the VT entering only the open alveoli inevitably leads tooverexpansion of this relatively healthy portion of the lung with subsequent volu-trauma/biotrauma even when the VT is in the normal range. Additionally, atelectasisleads to exudation of protein-rich fluid with increased surfactant inactivation andrelease of inflammatory mediators. Shear forces and uneven stress in areas whereatelectasis and overinflation coexist add to the damage. Thus, the open lung concept(OLC),56 which ensures that the VT is distributed evenly throughout the lungs, is afundamental component of any lung-protective ventilation strategy.In practical terms, the open lung is achieved by applying adequate PEEP.57 One of
the most important obstacles to optimizing the way conventional MV is practiced isthe persistence of “PEEP-o-phobia”, the fear of using adequate levels of end-expiratory pressure. This may be in part because the OLC has not been extensivelyevaluated in the clinical setting.58 There is no single optimal PEEP level. The level ofend-expiratory pressure must be tailored to the degree of lung injury (ie, lung compli-ance). For infants with healthy lungs and thus normal lung compliance, PEEP of 3 cmH2Omay be appropriate; PEEP of 6 cm H2Omay well lead to overexpansion of normallungs with circulatory impairment and elevated cerebral venous pressure. On the otherhand, atelectatic, poorly compliant lungsmay transiently require PEEP levels as high as8 to 10 cm H2O or more to achieve adequate alveolar recruitment and optimizeventilation/perfusion ratio. Because infants with healthy lungs are seldom ventilated,PEEP of less than 5 cm H2O should be uncommon.
High-frequency Ventilation
In contrast to conventional ventilation, the importance of optimizing lung inflation hasbeen recognized since its early days by users of HFV, where the optimal lung volumestrategy has become standard practice and is widely understood to be critical to itssuccess.59,60 HFV includes several modes of ventilation, including high-frequencyoscillatory ventilation (HFOV), high-frequency jet ventilation, and high-frequencypercussive ventilation, that have been used in neonatology since the 1980s. Thebenefit of HFV is believed to be a function of reduced pressure and volume swingstransmitted to the periphery of the lungs. For optimal effectiveness, the lungs needto be recruited and then stabilized with the lowest possible mean airway pressure.Several early animal studies demonstrated the short-term benefits of HFOV with anoptimal lung volume strategy.61 More recently, Yoder and colleagues62 comparedthe effect of more prolonged HFOV and low VT positive pressure ventilation usingthe immature baboon model for BPD, demonstrating that prolonged use of HFOVsignificantly improved early lung function with sustained improvement in pulmonarymechanics up to 28 days of life and less pulmonary inflammation in the recovery phaseof their RDS. Several RCTs of HFOV and high-frequency jet ventilation showedimproved outcomes, including reduction in BPD and/or duration of MV,63–67 whereas
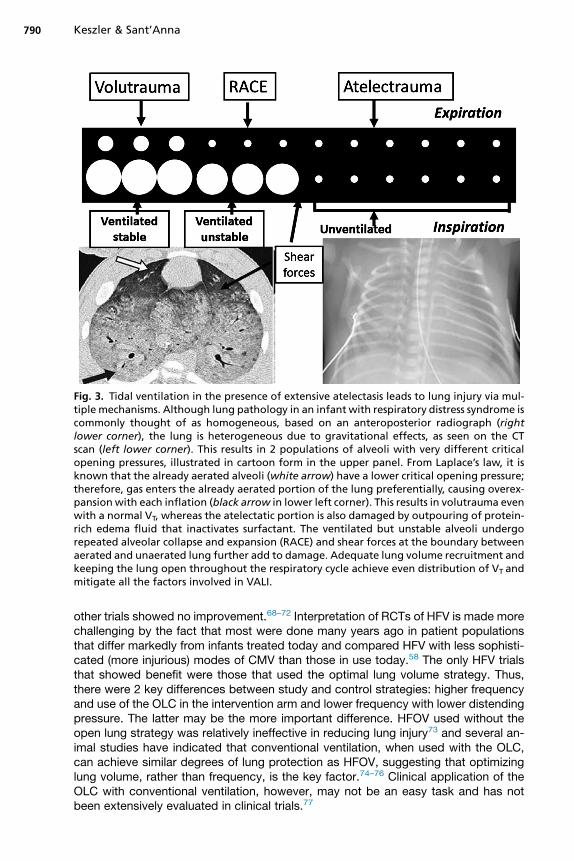
Fig. 3. Tidal ventilation in the presence of extensive atelectasis leads to lung injury via mul-tiple mechanisms. Although lung pathology in an infant with respiratory distress syndrome iscommonly thought of as homogeneous, based on an anteroposterior radiograph (rightlower corner), the lung is heterogeneous due to gravitational effects, as seen on the CTscan (left lower corner). This results in 2 populations of alveoli with very different criticalopening pressures, illustrated in cartoon form in the upper panel. From Laplace’s law, it isknown that the already aerated alveoli (white arrow) have a lower critical opening pressure;therefore, gas enters the already aerated portion of the lung preferentially, causing overex-pansionwith each inflation (black arrow in lower left corner). This results in volutrauma evenwith a normal VT, whereas the atelectatic portion is also damaged by outpouring of protein-rich edema fluid that inactivates surfactant. The ventilated but unstable alveoli undergorepeated alveolar collapse and expansion (RACE) and shear forces at the boundary betweenaerated and unaerated lung further add to damage. Adequate lung volume recruitment andkeeping the lung open throughout the respiratory cycle achieve even distribution of VT andmitigate all the factors involved in VALI.
Keszler & Sant’Anna790
other trials showed no improvement.68–72 Interpretation of RCTs of HFV is made morechallenging by the fact that most were done many years ago in patient populationsthat differ markedly from infants treated today and compared HFV with less sophisti-cated (more injurious) modes of CMV than those in use today.58 The only HFV trialsthat showed benefit were those that used the optimal lung volume strategy. Thus,there were 2 key differences between study and control strategies: higher frequencyand use of the OLC in the intervention arm and lower frequency with lower distendingpressure. The latter may be the more important difference. HFOV used without theopen lung strategy was relatively ineffective in reducing lung injury73 and several an-imal studies have indicated that conventional ventilation, when used with the OLC,can achieve similar degrees of lung protection as HFOV, suggesting that optimizinglung volume, rather than frequency, is the key factor.74–76 Clinical application of theOLC with conventional ventilation, however, may not be an easy task and has notbeen extensively evaluated in clinical trials.77
Ventilation and Bronchopulmonary Dysplasia 791
With the inclusion of more recent clinical trials that reflect advances in conventionalventilation strategies, the protective effect of HFOV is less clear than earlier studies sug-gested.78 A recent meta-analysis of individual patient data from several RCTs did notdemonstrate any superiority of HFOV over conventional ventilatory strategies.79 Theanalysis also did not support the selection of a specific subgroup of preterm infantswho might uniquely benefit from HFOV on the basis of gestational age, birth weight forgestation, initial lung disease severity, or exposure to antenatal corticosteroids. Thelong-term pulmonary follow-up from the United Kingdom Oscillation Study, however,which demonstrated less severe long-term pulmonary abnormalities in the HFOV group,suggests that the dichotomous outcome of BPD versus No BPD is too blunt a tool toassess possible benefits of lung-protective ventilation strategies.80
PUTTING IT ALL TOGETHER
Based on the key concepts discussed previously, certain general guidelines for theuse of MV can be formulated. The overarching goal is to support adequate gasexchange with the minimum of adverse effects on the infant’s lungs, hemodynamics,and brain. Longer duration of ventilation is associated with increased likelihood ofchronic lung disease, late-onset sepsis, and neurodevelopmental impairment; there-fore, successful extubation at the earliest possible time is desirable. Ventilationstrategies should be individualized to address each patient’s specific condition, butoptimizing lung volume and preventing atelectasis, which improve lung compliance,minimize oxygen requirement, avoid surfactant inactivation and achieve even VT dis-tribution, remain fundamental imperatives. The second key element of lung-protectivestrategy is to avoid excessively large VT, whichminimizes volutrauma and hypocapnia,2 potentially preventable elements of lung and brain injury. This is best accomplishedby the use of one of the volume-targeted modes available on most widely used ven-tilators. When high distending and inflation pressures are needed to achieve thesegoals, HFV is a reasonable option.Mild permissive hypercapnia and minimal FIO2 to achieve adequate oxygen satura-
tion are generally considered appropriate, but PCO2 greater than 60 mm Hg shouldbe avoided in the first 3 days of life due to increased risk of IVH. There is no evidenceto support the routine use of sedation and, therefore, infants should be allowed tobreathe spontaneously. Routine suctioning should be avoided, because it leads toderecruitment, transient hypoxemia, and perturbation of cerebral hemodynamics.Only when secretions are detected by auscultation or by perturbation of the flowwaveform is gentle rapid suctioning without instillation of normal saline indicated.In the absence of definitive evidence from RCTs, the choice of synchronized inter-
mittent mandatory ventilation (SIMV) or assist/control (A/C) remains a matter of per-sonal preference and practice style. There is little difference between the two in theacute phase of respiratory failure or in a patient who has little or no respiratory effortbut becomes more pronounced during weaning, especially in the smallest infants withnarrow endotracheal tubes. Prolonged ventilation with low SIMV rates should beavoided in these infants, because of the mechanical inflations it imposes an undesir-ably high work of breathing. SIMV also results in larger VT compared with A/C,because small preterm infants typically do not generate adequate spontaneous VT
resulting in a high dead space:VT ratio. To a significant degree, this problem may beovercome by adding pressure support ventilation (PS) to the spontaneous breathsduring SIMV.81 Although this approach is effective, it adds complexity and does notseem to have any advantage over A/C or PS used alone as long as atelectasis isavoided by using adequate level of PEEP. Additionally, it is important to recognize
Keszler & Sant’Anna792
that volume targeting is only applied to the SIMV inflations when using SIMV with PSand volume guarantee.
SUMMARY
Although even with optimized respiratory care it is likely that some degree of lunginjury is inevitable in ELBW infants, the wide variation in the risk-adjusted incidenceof BPD among the academic medical centers that comprise the Neonatal ResearchNetwork suggests that MV and other clinical practices are potentially modifiable riskfactors.82,83 Although the evidence to guide respiratory support strategies remainsincomplete, the key concepts outlined in this review are based on the best availableevidence and physiologic rationale and may provide an opportunity to minimizeadverse respiratory outcomes in ELBW infants requiring respiratory support.
REFERENCES
1. Walsh MC, Morris BH, Wrage LA, et al. Extremely low birthweight neonates withprotracted ventilation: mortality and 18-month neurodevelopmental outcomes.J Pediatr 2005;146(6):798–804.
2. NICHD Neonatal Research Network, Support Study Group of the Eunice KennedyShriver. Early CPAP versus surfactant in extremely preterm infants. N Engl J Med2010;362:1970–9.
3. Morley CJ, Davis PG, Doyle LW, et al. Nasal CPAP or intubation at birth for verypreterm infants. N Engl J Med 2008;358(7):700–8.
4. Loeliger M, Inder T, Cain S, et al. Cerebral outcomes in a preterm baboon modelof early versus delayed nasal continuous positive airway pressure. Pediatrics2006;118(4):1640–53.
5. Garland JS. Strategies to prevent ventilator-associated pneumonia in neonates.Clin Perinatol 2010;37(3):629–43.
6. Northway WH Jr, Rosan RC, Porter DY. Pulmonary disease following respiratortherapy of hyaline-membrane disease. Bronchopulmonary dysplasia. N Engl JMed 1967;276(7):357–68.
7. Northway WH Jr, Rosan RC. Radiographic features of pulmonary oxygen toxicityin the newborn: bronchopulmonary dysplasia. Radiology 1968;91(1):49–58.
8. Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med2001;163(7):1723–9.
9. Philip AG. Oxygen plus pressure plus time: the etiology of bronchopulmonarydysplasia. Pediatrics 1975;55(1):44–50.
10. Dreyfuss D, Soler P, Basset G, et al. High inflation pressure pulmonary edema.Respective effects of high airway pressure, high tidal volume, and positiveend-expiratory pressure. Am Rev Respir Dis 1988;137(5):1159–64.
11. Hernandez LA, Peevy KJ, Moise AA, et al. Chest wall restriction limits high airwaypressure-induced lung injury in young rabbits. J Appl Physiol (1985) 1989;66(5):2364–8.
12. Mols G, Priebe HJ, Guttmann J. Alveolar recruitment in acute lung injury. Br JAnaesth 2006;96(2):156–66.
13. Laughon M, Bose C, Allred EN, et al. Antecedents of chronic lung diseasefollowing three patterns of early respiratory disease in preterm infants. Arch DisChild Fetal Neonatal Ed 2011;96(2):F114–20.
14. Jobe AH. Effects of chorioamnionitis on the fetal lung. Clin Perinatol 2012;39(3):441–57.
Ventilation and Bronchopulmonary Dysplasia 793
15. Hendson L, Russell L, Robertson CMT, et al. Neonatal and neurodevelopmentaloutcomes of very low birth weight infants with histologic chorioamnionitis.J Pediatr 2011;158(3):397–402.
16. Speer CP. Chorioamnionitis, postnatal factors and proinflammatory response inthe pathogenetic sequence of bronchopulmonary dysplasia. Neonatology2009;95(4):353–61.
17. Mortola JP, Fisher JT, Smith JB, et al. Onset of respiration in infants delivered bycesarean section. J Appl Physiol Respir Environ Exerc Physiol 1982;52(3):716.
18. Siew ML, Te Pas AB, Wallace MJ, et al. Positive end-expiratory pressure en-hances development of a functional residual capacity in preterm rabbits venti-lated from birth. J Appl Physiol (1985) 2009;106:1487–93.
19. Kattwinkel J, Perlman JM, Aziz K, et al. Neonatal Resuscitation: 2010 Americanheart association guidelines for cardiopulmonary resuscitation and emergencycardiovascular care. Pediatrics 2010;126(5):e1400–13.
20. Perlman JM, Wyllie J, Kattwinkel J, et al. Neonatal resuscitation: 2010 internationalconsensus on cardiopulmonary resuscitation and emergency cardiovascularcare science with treatment recommendations. Pediatrics 2010;126(5):e1319–44.
21. Keszler M. Sustained inflation during neonatal resuscitation. Curr Opin Pediatr2015;27(2):145–51.
22. Hillman NH, Kemp MW, Miura Y, et al. Sustained inflation at birth did not alter lunginjury from mechanical ventilation in surfactant-treated fetal lambs. PLoS One2014;9(11):e113473.
23. Hillman NH, Kemp MW, Noble PB, et al. Sustained inflation at birth did not protectpreterm fetal sheep from lung injury. Am J Physiol Lung Cell Mol Physiol 2013;305(6):L446–53.
24. Schmolzer GM, Kumar M, Aziz K, et al. Sustained inflation versus positive pres-sure ventilation at birth - a systematic review and meta-analysis. Arch Dis ChildFetal Neonatal Ed 2015;100(4):F361–8.
25. Vento M, Moro M, Escrig R, et al. Preterm resuscitation with low oxygen causesless oxidative stress, inflammation, and chronic lung disease. Pediatrics 2009;124(3):e439–49.
26. Kapadia VS, Chalak LF, Sparks JE, et al. Resuscitation of preterm neonates withlimited versus high oxygen strategy. Pediatrics 2013;132(6):e1488–96.
27. Rabi Y, Singhal N, Nettel-Aguirre A. Room-air versus oxygen administration forresuscitation of preterm infants: the ROAR study. Pediatrics 2011;128(2):e374–81.
28. SUPPORT Study Group of the Eunice Kennedy Shriver NICHD NeonatalResearch Network. Target ranges of oxygen saturation in extremely preterminfants. N Engl J Med 2010;362(21):1970–9.
29. Stenson BJ, Tarnow-Mordi WO, Darlow BA, et al. Oxygen saturation and out-comes in preterm infants. N Engl J Med 2013;368(22):2094–104.
30. Schmidt B, Whyte RK, Asztalos EV, et al. Effects of targeting higher vs lower arte-rial oxygen saturations on death or disability in extremely preterm infants: a ran-domized clinical trial. JAMA 2013;309(20):2111–20.
31. Saugstad OD, Aune D. Optimal oxygenation of extremely low birth weight infants:a meta-analysis and systematic review of the oxygen saturation target studies.Neonatology 2014;105(1):55–63.
32. Van Marter LJ, Allred EN, Pagano M, et al. Do clinical markers of barotrauma andoxygen toxicity explain interhospital variation in rates of chronic lung disease?The Neonatology Committee for the Developmental Network. Pediatrics 2000;105:1194–201.
Keszler & Sant’Anna794
33. Sandri F, Plavka R, Ancora G, et al. Prophylactic or early selective surfactantcombined with nCPAP in very preterm infants. Pediatrics 2010;125(6):e1402–9.
34. Dunn MS, Kaempf J, de Klerk A, et al. Randomized trial comparing 3 approachesto the initial respiratory management of preterm neonates. Pediatrics 2011;128(5):e1069–76.
35. Schmolzer GM, Kumar M, Pichler G, et al. Non-invasive versus invasive respira-tory support in preterm infants at birth: systematic review and meta-analysis. BMJ2013;347:f5980.
36. Moretti C, Gizzi C, Papoff P, et al. Comparing the effects of nasal synchronizedintermittent positive pressure ventilation (nSIPPV) and nasal continuous positiveairway pressure (nCPAP) after extubation in very low birth weight infants. EarlyHum Dev 1999;56(2–3):167–77.
37. Davis PG, Morley CJ, Owen LS. Non-invasive respiratory support of preterm neo-nates with respiratory distress: continuous positive airway pressure and nasal inter-mittent positive pressure ventilation. Semin Fetal Neonatal Med 2009;14(1):14–20.
38. Meneses J, Bhandari V, Alves JG. Nasal intermittent positive-pressure ventilationvs nasal continuous positive airway pressure for preterm infants with respiratorydistress syndrome: a systematic review and meta-analysis. Arch Pediatr AdolescMed 2012;166(4):372–6.
39. Kirpalani H, Millar D, Lemyre B, et al. A trial comparing noninvasive ventilationstrategies in preterm infants. N Engl J Med 2013;369(7):611–20.
40. BahadueFL, Soll R. Early versusdelayed selective surfactant treatment for neonatalrespiratory distress syndrome. Cochrane Database Syst Rev 2012;(11):CD001456.
41. Rojas-Reyes MX, Morley CJ, Soll R. Prophylactic versus selective use of surfac-tant in preventing morbidity and mortality in preterm infants. Cochrane DatabaseSyst Rev 2012;(3):CD000510.
42. Dargaville PA, Aiyappan A, Cornelius A, et al. Preliminary evaluation of a newtechnique of minimally invasive surfactant therapy. Arch Dis Child Fetal NeonatalEd 2011;96(4):F243–8.
43. Kribs A, Hartel C, Kattner E, et al. Surfactant without intubation in preterm infantswith respiratory distress: first multicenter data. Klin Padiatr 2010;222(1):13–7.
44. Dargaville PA, Aiyappan A, De Paoli AG, et al. Minimally-invasive surfactant ther-apy in preterm infants on continuous positive airway pressure. Arch Dis ChildFetal Neonatal Ed 2013;98(2):F122–6.
45. More K, Sakhuja P, Shah PS. Minimally invasive surfactant administration in pre-term infants: a meta-narrative review. JAMA Pediatr 2014;168(10):901–8.
46. Finer N, Merritt T, Bernstein G, et al. A multicenter pilot study of Aerosurf deliveredvia nasal continuous positive airway pressure (nCPAP) to prevent respiratorydistress syndrome in preterm neonates. J Aerosol Med Pulm Drug Deliv 2010;23(5):303–9.
47. Keszler M. State of the art in conventional mechanical ventilation. J Perinatol2009;29(4):262–75.
48. Morley CJ. Volume-limited and volume-targeted ventilation. Clin Perinatol 2012;39(3):513–23.
49. Dani C, Bresci C, Lista G, et al. Neonatal respiratory support strategies in theintensive care unit: an Italian survey. Eur J Pediatr 2013;172(3):331–6.
50. van Kaam AH, Rimensberger PC, Borensztajn D, et al. Ventilation practices in theneonatal intensive care unit: a cross-sectional study. J Pediatr 2010;157(5):767–71.
51. Wheeler K, Klingenberg C, McCallion N, et al. Volume-targeted versuspressure-limited ventilation in the neonate. Cochrane Database Syst Rev2010;(11):CD003666.
Ventilation and Bronchopulmonary Dysplasia 795
52. Peng WS, Zhu HW, Shi H, et al. Volume-targeted ventilation is more suitable thanpressure-limited ventilation for preterm infants: a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed 2014;99:F158–65.
53. Lachmann B. Open up the lung and keep the lung open. Intensive Care Med1992;18(6):319–21.
54. Caruso P, Meireles SI, Reis LFL, et al. Low tidal volume ventilation induces proin-flammatory and profibrogenic response in lungs of rats. Intensive Care Med2003;29:1808–11.
55. Tsuchida S, Engelberts D, Peltekova V, et al. Atelectasis causes alveolar injuryin nonatelectatic lung regions. Am J Respir Crit Care Med 2006;174(3):279–89.
56. Rimensberger PC, Cox PN, Frndova H, et al. The open lung during small tidal vol-ume ventilation: concepts of recruitment and “optimal” positive end-expiratorypressure. Crit Care Med 1999;27:1946–52.
57. Castoldi F, Daniele I, Fontana P, et al. Lung recruitment maneuver during volumeguarantee ventilation of preterm infants with acute respiratory distress syndrome.Am J Perinatol 2011;28:521–8.
58. van Kaam AH, Rimensberger PC. Lung-protective ventilation strategies in neona-tology: what do we know - what do we need to know? Crit Care Med 2007;35:925–31.
59. Bryan AC. The oscillations of HFO. Am J Respir Crit Care Med 2001;163(4):816–7.
60. Froese AB. Role of lung volume in lung injury: HFO in the atelectasis-prone lung.Acta Anaesthesiol Scand 1989;90:126.
61. Keszler M, Durand D. High-frequency ventilation. Clin Perinatol 2001;28(3):579–607.
62. Yoder BA, Siler-Khodr T, Winter VT, et al. High-frequency oscillatory ventilation:effects on lung function, mechanics, and airway cytokines in the immaturebaboon model for neonatal chronic lung disease. Am J Respir Crit Care Med2000;162:1867–76.
63. Clark RH, Gertsmann DR, Null DM, et al. Prospective randomized comparison ofhigh-frequency oscillatory and conventional ventilation in respiratory distresssyndrome. Pediatrics 1992;89:5–12.
64. Gerstmann DR, Minton SD, Stoddard RA, et al. The Provo multicenter early highfrequency oscillatory ventilation trial: improved pulmonary and clinical outcome inrespiratory distress syndrome. Pediatrics 1996;98:1044–57.
65. Keszler M, Modanlou HD, Brudno DS, et al. Multi-center controlled clinical trial ofhigh-frequency jet ventilation in preterm infants with uncomplicated respiratorydistress syndrome. Pediatrics 1997;100:593–9.
66. Plavka R, Kopecky P, Sebron V, et al. A prospective randomized comparison ofconventional mechanical ventilation and very early high-frequency oscillatoryventilation in extremely premature newborns with respiratory distress syndrome.Intensive Care Med 1999;25:68–75.
67. Courtney SE, Durand DJ, Asselin JM, et al, The Neonatal Ventilation Study Group.High-frequency oscillatory ventilation versus conventional mechanical ventilationfor very-low-birth-weight infants. N Engl J Med 2002;347:643–52.
68. Wiswell TE, Graziani LJ, Kornhauser MS, et al. High-frequency jet ventilation inthe early management of respiratory distress syndrome is associated with agreater risk for adverse outcomes. Pediatrics 1996;98:1035–43.
69. Rettwitz-Volk W, Veldman A, Roth B, et al. A prospective, randomized, multicentertrial of high-frequencyoscillatory ventilation comparedwith conventional ventilation
Keszler & Sant’Anna796
in preterm infantswith respiratory distress syndrome receiving surfactant. J Pediatr1998;132:249–54.
70. Moriette G, Paris-Llado J, Walti H, et al. Prospective randomized multicenter com-parison of high-frequency oscillatory ventilation and conventional ventilation inpreterm infants of less than 30 weeks with respiratory distress syndrome. Pediat-rics 2001;107:363–72.
71. Johnson AH, Peacock JL, Greenough A, et al. High-frequency oscillatory ventila-tion for the prevention of chronic lung disease of prematurity. N Engl J Med 2002;347:633–42.
72. Van Reempts P, Borstlap C, Laroche S, et al. Early use of high frequency ventila-tion in the premature neonate. Eur J Pediatr 2003;162:219–26.
73. McCulloch PR, Forkert PG, Froese AB. Lung volume maintenance prevents lunginjury during high-frequency oscillatory ventilation in surfactant deficient rabbits.Am Rev Respir Dis 1988;137:1185–92.
74. Gommers D, Hartog A, Schnabel R, et al. High-frequency oscillatory ventilation isnot superior to conventional mechanical ventilation in surfactant-treated rabbitswith lung injury. Eur Respir J 1999;14:738–44.
75. Vazquez de Anda GF, Hartog A, Verbrugge SJ, et al. The open lung concept:pressure-controlled ventilation is as effective as high-frequency oscillatory venti-lation in improving gas exchange and lung mechanics in surfactant-deficientanimals. Intensive Care Med 1999;25:990–6.
76. Vazquez de Anda GF, Gommers D, Verbrugge SJ, et al. Mechanical ventilationwith high positive end-expiratory pressure and small driving pressure amplitudeis as effective as high-frequency oscillatory ventilation to preserve the function ofexogenous surfactant in lung-lavaged rats. Crit Care Med 2000;28:2921–5.
77. Jobe AH. Lung recruitment for ventilation: does it work, and is it safe? J Pediatr2009;154(5):635–6.
78. Cools F, Henderson-Smart DJ, Offringa M, et al. Elective high frequency oscilla-tory ventilation versus conventional ventilation for acute pulmonary dysfunction inpreterm infants. Cochrane Database Syst Rev 2009;(3):CD000104.
79. Cools F, Askie LM, Offringa M, et al, PreVILIG Collaboration. Elective high-frequency oscillatory versus conventional ventilation in preterm infants: a system-atic review and meta-analysis of individual patients’ data. Lancet 2010;375(9731):2082–91.
80. Zivanovic S, Peacock J, Alcazar-Paris M, et al. Late outcomes of a randomizedtrial of high-frequency oscillation in neonates. N Engl J Med 2014;370(12):1121–30.
81. Osorio W, Claure N, D’Ugard C, et al. Effects of pressure support during an acutereduction of synchronized intermittent mandatory ventilation in preterm infants.J Perinatol 2005;25(6):412–6.
82. Laughon MM, Langer JC, Bose CL, et al. Prediction of bronchopulmonarydysplasia by postnatal age in extremely premature infants. Am J Respir CritCare Med 2011;183(12):1715–22.
83. Ambalavanan N, Walsh M, Bobashev G, et al. Intercenter differences in broncho-pulmonary dysplasia or death among very low birth weight infants. Pediatrics2011;127(1):e106–16.





























