Embed Size (px)
Citation preview
Medicare Shared Savings Program ACO Learning System
ACO Lessons Learned from GPRO Reporting
Wednesday, October 28, 20152:30-4:00 PM ET
Disclaimer
The comments made on this call are offered only for general informational and educational purposes. As always, the agency’s positions on matters may be subject to change. CMS’s comments are not offered as and do not constitute legal advice or legal opinions, and no statement made on this call will preclude the agency and/or its law enforcement partners from enforcing any and all applicable laws, rules and regulations. ACOs are responsible for ensuring that their actions fully comply with applicable laws, rules and regulations, and we encourage you to consult with your own legal counsel to ensure such compliance.
Furthermore, to the extent that we may seek to gather facts and information from you during this call, we intend to gather your individual input. CMS is not seeking group advice.
2
Past Webinar Materials
Interested in past Learning System events? Go to https://portal.cms.gov to access recordings and summaries of past webinars, including:• Advancing Primary Care – 11/14/14• Beneficiary Engagement – 10/22/14• Beneficiary Engagement and Annual Wellness Visits – 8/19/15 • Care Coordinator Roundtable – Session 1 – 9/30/15• Coordinating Care for Beneficiaries with Complex Care Needs –
6/24/15• Coordinating with Hospitals and Specialists – 12/15/14• Coordinating with Post Acute Care Providers – 11/21/14• Evidence-Based Medicine – 1/7/14 and 1/24/14
3
Past Webinar Materials (cont.)
• Internal Cost and Quality Reporting—4/17/14 and 5/22/14• Lessons from GPRO Reporting – 1/17/14 and 10/28/14• Lessons Learned from the Million Hearts Initiative – 7/29/15 • Provider Engagement– 9/9/14 and 10/1/14• Strategies of SSP ACOs Achieving Interim Savings – 4/4/14, 4/11/14,
5/2/14, 5/16/14• Strategies of SSP ACOs Achieving Shared Savings -- 4/15/15, 4/29/15,
5/12/15, 5/19/15• Using Data to Drive Performance – 6/8/15In the ACO portal, materials for these and other webinars are located in the Events Calendar, and Program Announcements section, under “Learning System Webinar Materials”
4
Webinar Agenda
• Housekeeping items• ACO Introductions• Roundtable discussion
• Data Collection and Reporting Process• Staff and Training• Technology and Other Resources• Strategies and Lessons Learned
• Q&A• Wrap-up
5
The widget menu located at the bottom of your event console provides access to various resources for a webcast. Should you accidentally minimize any of your widgets, you can open them again using the widget menu.
The Help widget provides immediate access to technical resources and information, like the system requirements and technical FAQs. In addition, you can test your system to see if you are meeting the minimal technical requirements.
The Q&A widget allows attendees to submit questions to the presenters – technical or content related – at any time.
The Slides widget is the presentation display area for the PowerPoint slides that are presented to the audience. It also displays any polling questions.
The Resource List widget contains documents related to this webcast.
The Closed Captioning widget opens a separate URL featuring the live closed captioning feed for the webcast.
The Survey widget contains a link to a survey, which you can use to submit feedback about the webcast.
6
Rocky Mountain Accountable Health Network
Carol BeamChief Executive Officer
7
Rocky Mountain Accountable Health Network
• RMAHN began January 1, 2014• We are a Track One ACO • Our primary service area is Montana (Yellowstone and
surrounding counties); we have a primary care practice in Cody, Wyoming that has attributed lives as well
• We are not an Advanced Payment ACO• Our participant list consists of the following (350 total providers
/18 TINs):– 1 hospital, its 80 employed primary care providers, its 215 employed
specialists and its DME company – 50 independent specialists– 1 independent ASC
• 10,000 +/- assigned beneficiaries • Close to 100% EHR penetration; 18 different platforms
8
ACO Formation, Culture and Background• RMAHN is an initiative of a Physician Hospital Organization affiliated
with St. Vincent Healthcare and its independent physicians (St. Vincent is one of 9 hospitals owned by SCL Health out of Denver, Colorado)– The PHO formed a wholly owned subsidiary for the specific purpose of
contracting with CMS– The ACO participants make up a subset of the membership of the PHO
• The ACO is in a geographic area that would be considered rural by most standards but for Montana it is considered urban (Billings, MT is the largest city in the state)
• Several key reasons for entering the MSSP realm:– The hospital’s employed physician network is committed to PCMH and
the MSSP fits well with this delivery model– The hospital and some PHO members are forward thinking and prefer
to be on the leading edge of initiatives– The SCL Health system recognized the need to transition the
organization from its current hospital centric model and Billings was farther ahead in its ambulatory development
9
Reporting Timeline – Before GPRO Tool Opened
We spent at least 3 months preparing for the delivery of our list from CMS We dedicated one person as the project leader Project leader became the expert on understanding
the criteria needed to satisfy the metric (documented in detail)
Project leader assembled a small team (project leader, PCMH director and the population health director) to research the primary care EMRs for the specific purpose of understanding where the data lived and how it could be extracted
10
Before GPRO Tool OpenedWhat we found: There was no consistency within the EMR Some providers would use the “notes” section to document;
others would use a defined field There was a lack of documentation to support a “plan” to
improve
Information from 2 years ago was not included in the current EMR (there was a change from IDX to Epic – nothing carried forward) This made reporting on colonoscopies the most challenging
11
Reporting Timeline – After GPRO Tool Opened
We were very prepared by the time reporting opened We moved to a new office and used the opportunity to set
up a computer lab in the conference room specifically for GPRO reporting
The project leader used her existing staff to complete various metrics Because of the work done up front, we knew which metrics could be
found in the primary care EMRs The project leader assigned these metrics to her team (i.e., fall risk)
For other metrics, the project leader used resources in IT to extract data when it was deemed available in discreet fields (Epic registries – tobacco use)
The project leader assigned the toughest metrics to herself and the PCMH director – IVD, heart failure and CAD
12
After GPRO Tool OpenedWhat we found: Preparing as much in advance was a significant
help Identifying a project leader with great project
management skills helped Having the luxury of an “all hands on deck”
atmosphere removed some of the stress Compiling the results to upload to CMS took
longer than planned Documenting the results is highly recommended
13
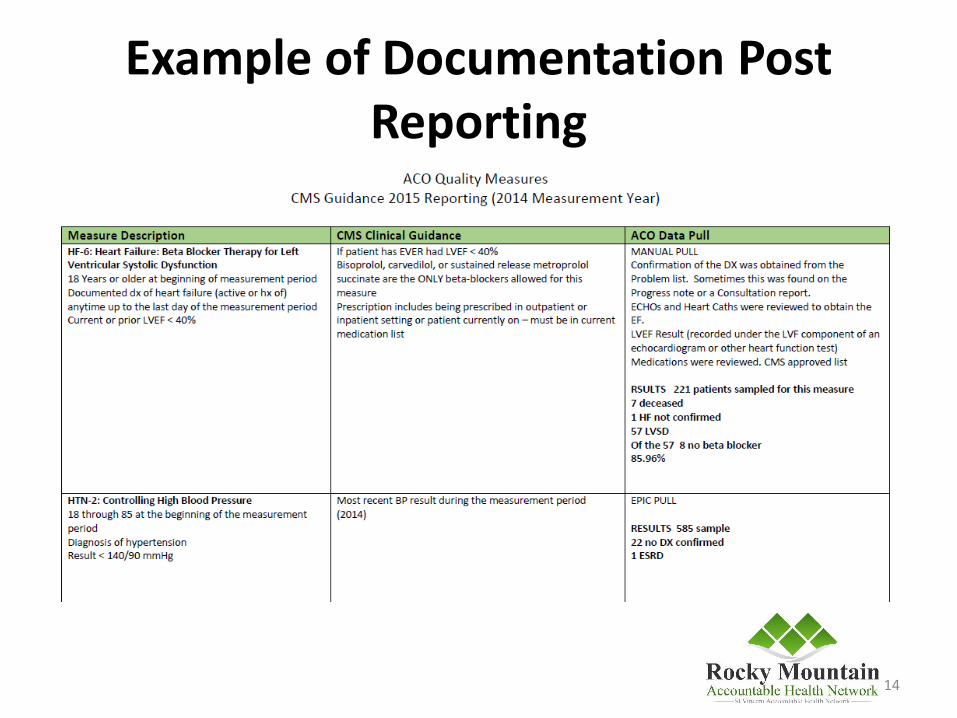
Example of Documentation Post Reporting
14
Data from Multiple Sources
RMAHN was fortunate enough to have direct access to the primary care EMR (Epic)
Because we are a PHO, we had the advantage of easier access to information outside Epic (if needed)• ACO providers are members of the PHO• ACO providers know us and we can reach out to
them for help• About the only group we needed to reach out to
was the cardiology group (non-Epic)
15
Contact Information
For further information please contact:
Carol A. Beam, CEO orDale Squires, CFO
Rocky Mountain Accountable Health NetworkBillings, MT
[email protected] or [email protected]
16

ProHEALTH Accountable Care Medical Group
Carole RomanoDirector, Accountable Care &
Regulatory Compliance
17
ProHEALTH Accountable CareMedical Group, PLLC
A subsidiary of the ACO’s single Participant, ProHEALTH Care Associates, LLP, a multi-specialty physician group.
MSSP Track 1, July 2012 starter. No interim payment election. 30K+ current beneficiaries. Shared savings programs with 4 commercial carriers.
Total patients in all programs is approximately 110K. 700+ physicians. (225+ adult primary care).
18
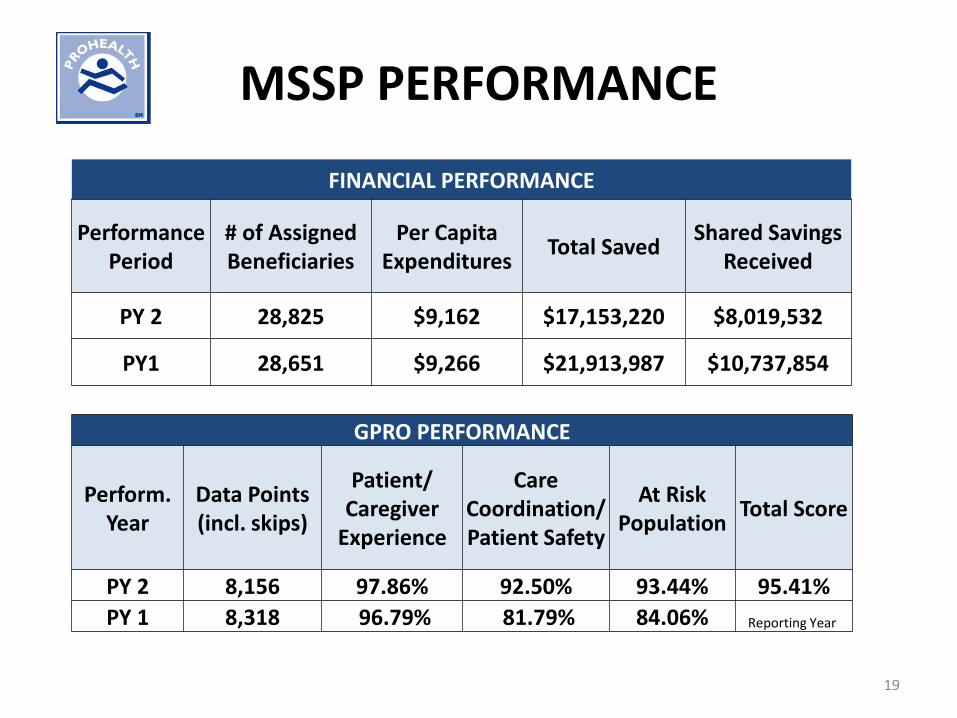
MSSP PERFORMANCE
FINANCIAL PERFORMANCE
Performance Period
# of Assigned Beneficiaries
Per Capita Expenditures Total Saved Shared Savings
Received
PY 2 28,825 $9,162 $17,153,220 $8,019,532
PY1 28,651 $9,266 $21,913,987 $10,737,854
GPRO PERFORMANCE
Perform.Year
Data Points (incl. skips)
Patient/ Caregiver
Experience
Care Coordination/Patient Safety
At Risk Population Total Score
PY 2 8,156 97.86% 92.50% 93.44% 95.41%PY 1 8,318 96.79% 81.79% 84.06% Reporting Year
19
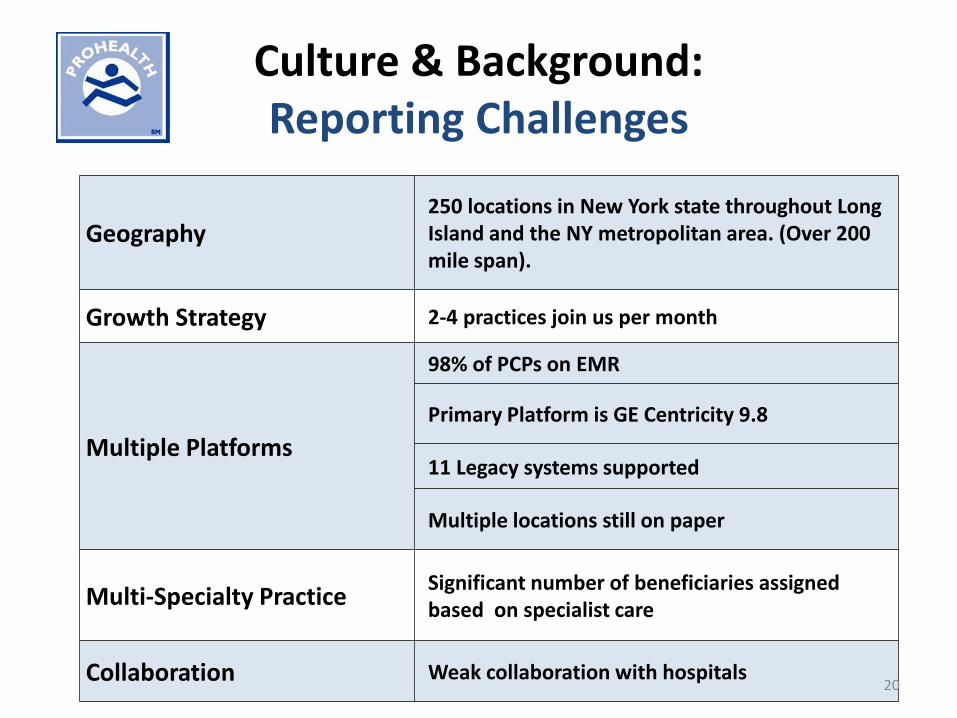
Culture & Background: Reporting Challenges
Geography250 locations in New York state throughout Long Island and the NY metropolitan area. (Over 200 mile span).
Growth Strategy 2-4 practices join us per month
Multiple Platforms
98% of PCPs on EMR
Primary Platform is GE Centricity 9.8
11 Legacy systems supported
Multiple locations still on paper
Multi-Specialty Practice Significant number of beneficiaries assigned based on specialist care
Collaboration Weak collaboration with hospitals20
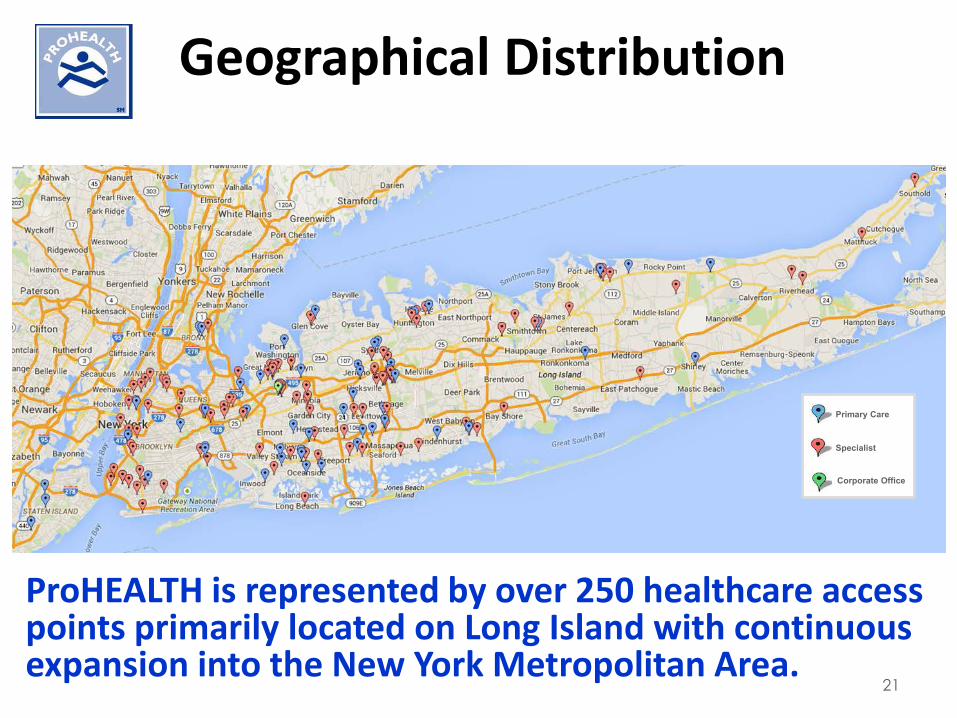
Geographical Distribution
ProHEALTH is represented by over 250 healthcare access points primarily located on Long Island with continuous expansion into the New York Metropolitan Area.
KEYPrimary Care
Specialist
Corporate Office
21
REPORTING TIMELINE
SETTING OURSELVES UP FOR SUCCESS: Customized EMR forms with hard stops; Paper quality measure flow sheet with supportive
documentation pages (i.e., plans of care, PHQ9 scoring, etc.); ACO training for every provider and every staff member; Quality measure training for every internal medicine provider
and all medical specialists, as well as their staff; Strong Accountable Care department with staff members
available to support departments throughout the year; Strong physician leadership; Our own regular patient satisfaction surveys and Patient
Advocacy department.22
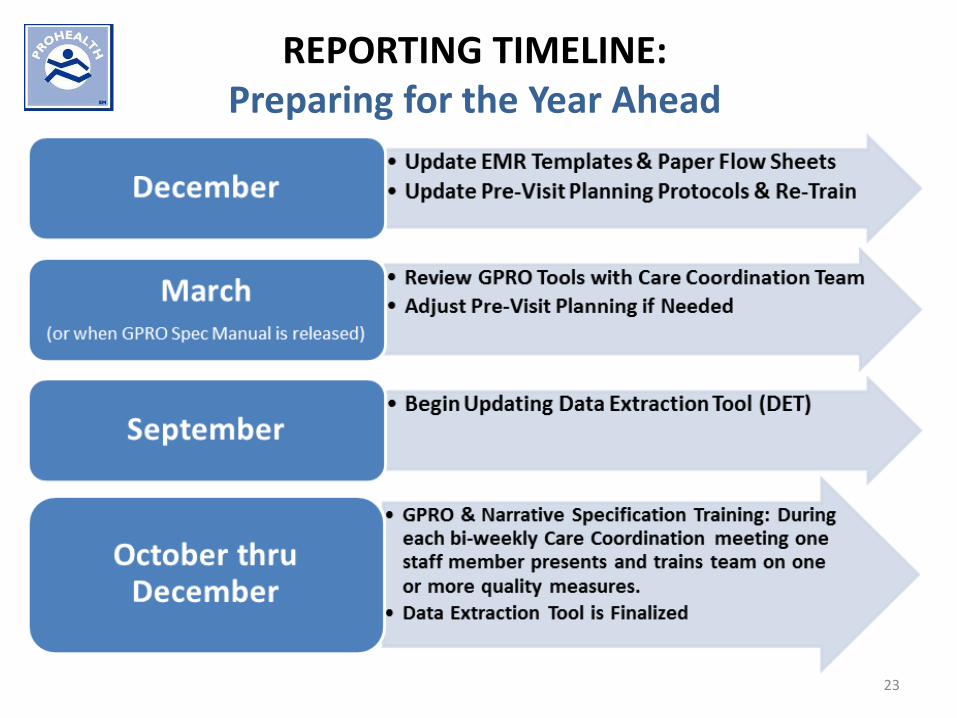
REPORTING TIMELINE:Preparing for the Year Ahead
23
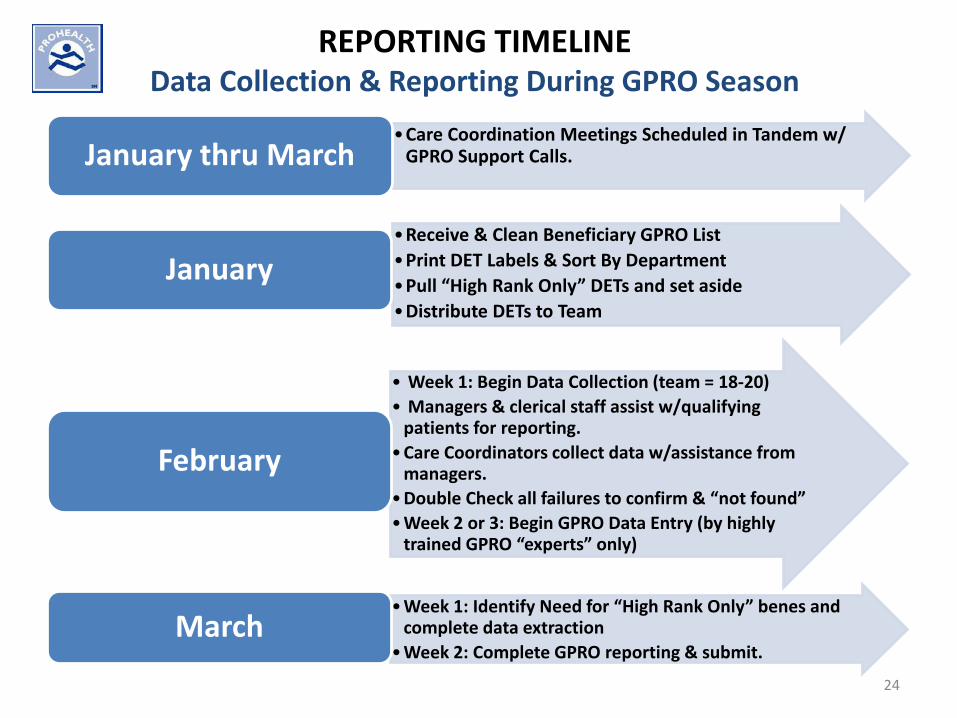
REPORTING TIMELINEData Collection & Reporting During GPRO Season
•Care Coordination Meetings Scheduled in Tandem w/ GPRO Support Calls.January thru March
•Receive & Clean Beneficiary GPRO List•Print DET Labels & Sort By Department•Pull “High Rank Only” DETs and set aside•Distribute DETs to Team
January
• Week 1: Begin Data Collection (team = 18-20)• Managers & clerical staff assist w/qualifying
patients for reporting.•Care Coordinators collect data w/assistance from
managers.•Double Check all failures to confirm & “not found”•Week 2 or 3: Begin GPRO Data Entry (by highly
trained GPRO “experts” only)
February
•Week 1: Identify Need for “High Rank Only” benes and complete data extraction
•Week 2: Complete GPRO reporting & submit.March
24

GPRO COMPLETED!
25
REPORTING: Reference Materials
DATA EXTRACTION FILE:• Blank DET• Ranking Guide (High Rank only DETs set aside for use as
needed. For all others, data is collected on ALL measures, even if some of those measures are high ranking)
• Medications List by Measure• CPT Codes by Measure• ICD Codes by Measure (ICD-9 & ICD-10)• Guide to Qualifying Patient for Sample
GPRO SPECIFICATIONS MANUAL DRUGS.COM PHYSICIAN LEADER
26
MANAGING DATAFROM MULTIPLE SOURCES
INTERNAL DATA SOURCES: Manual Extraction from All Data Sources: EMR, legacy systems; Care Coordinators all trained in our primary EMR and individual staff
receive EMR training in the many legacy systems; Care Coordinators deployed to all paper departments and to those with
legacy systems for data extraction at the site; Manager Support: Chart pull, translation of handwriting, some data
extraction supervised by Care Coordinator; On site physician presence at all paper chart locations.
NON-ACO DATA SOURCES: HIE/RHIO: Hospital/ER notifications and individual patient record access; Call, email and/or send paper mail requests to physicians outside ACO.
(Requests must beHIPAA compliant. A copy of the patient registration or chart note may be used to demonstrate provider relationship with the patient).
27
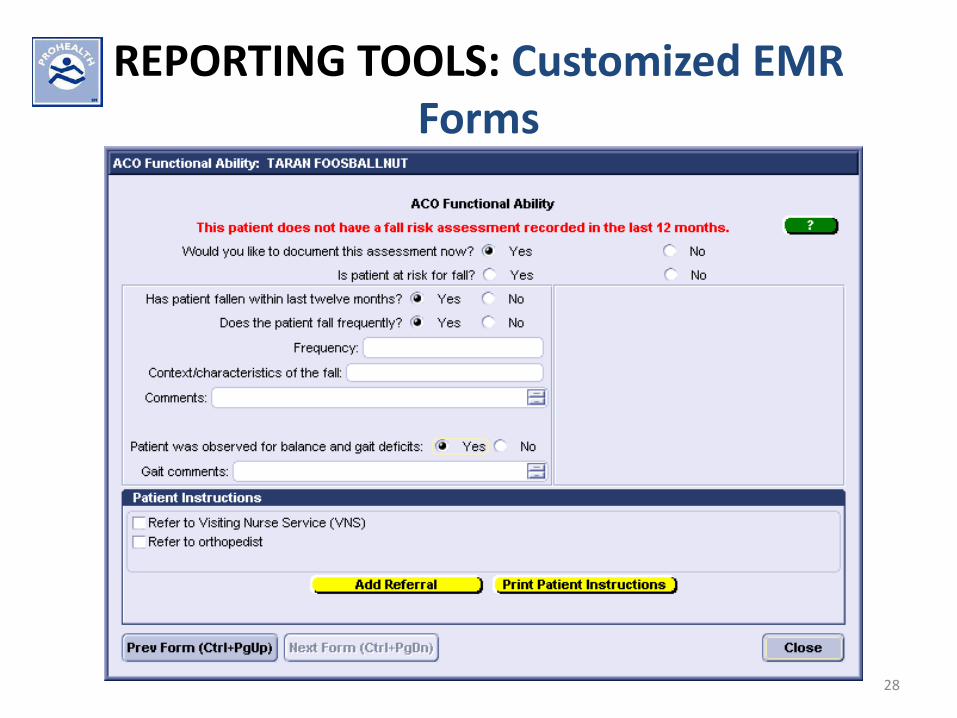
REPORTING TOOLS: Customized EMRForms
28
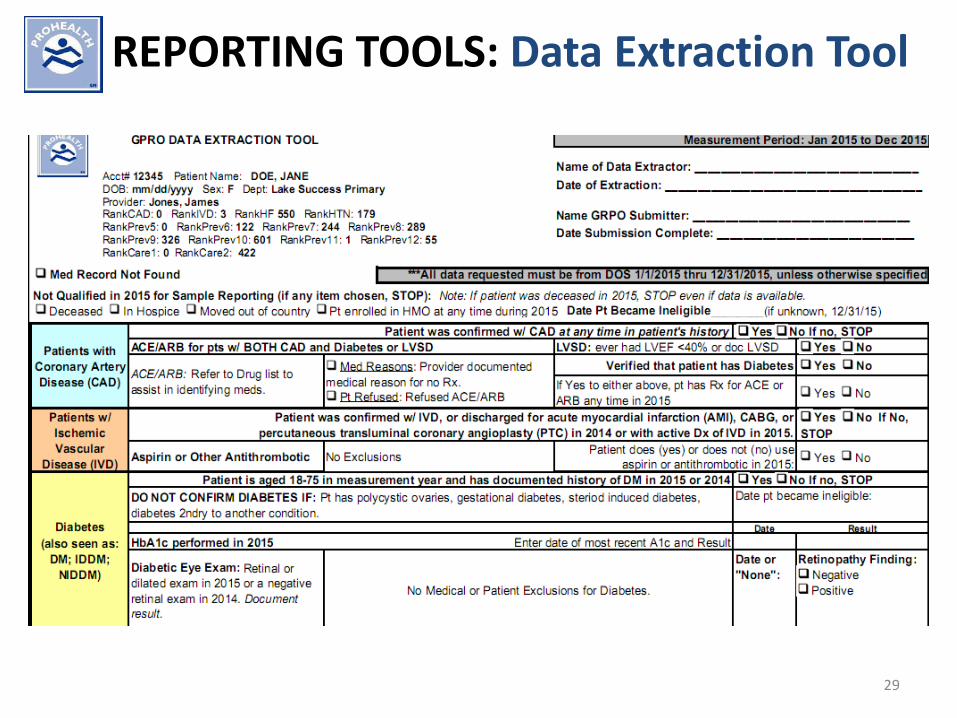
REPORTING TOOLS: Data Extraction Tool
29
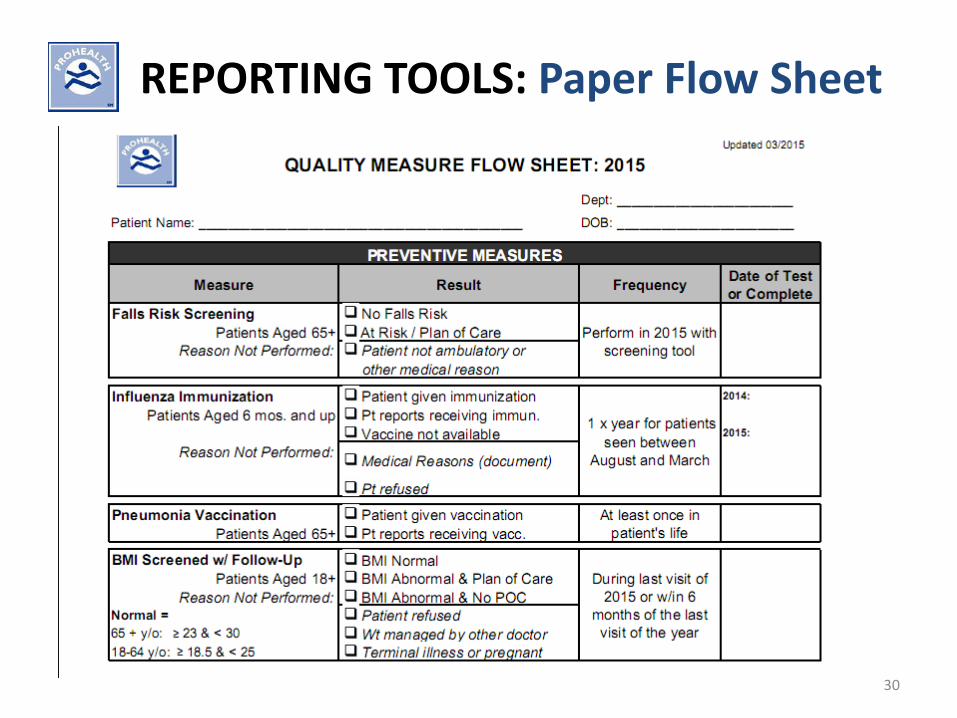
REPORTING TOOLS: Paper Flow Sheet
30
CONTACT INFORMATION
Carole RomanoDirector of Accountable Care and Regulatory ComplianceProHEALTH Medical Management, LLC2800 Marcus AvenueLake Success, NY [email protected]
31
Have Questions About Reporting Quality?
• For questions related to quality reporting, including quality sampling and measures specifications, use of the Web Interface, and EIDM accounts, contact the QualityNet help desk by email at [email protected], phone: 866-288-8912, TTY: 1-877-715-6222, or Fax: 888-329-7377. Help desk hours are Monday-Friday, 7am-7pm CT
• For questions about the CAHPS for ACOs survey, email [email protected]
32
Roundtable Discussion:Data Collection and Reporting Process
• Can you describe your data collection/reporting process? Was it effective, and/or what changes or adjustments have you made to the process for this year?
• In your opinion, what is the single most important thing for other ACOs to keep in mind when working with multiple EHRs/paper records?
33
Roundtable Discussion:Staff and Training
• Who was involved in collecting data for GPRO reporting? How many people, and in what roles?
• What training did you provide in order to prepare for GPRO? Who received training and how? What adjustments to training did you find were needed?
34
Roundtable Discussion:Technology and Other Resources
• How did you use technology (e.g., EHRs, analytic programs, tracking tools) in this process?
• Did you use any other resources that have not already been discussed?
• What additional resources do you anticipate needing for the next reporting based on your experience?
35
Roundtable Discussion:Strategies and Lessons Learned
• Are there any other strategies you used or lessons you learned that you would like to share? In what ways do you think you will need to adjust your strategies going forward?
• What did you find interesting or surprising about the process or challenges you faced?
• What “pearls of wisdom” would you share with ACOs that are new to the quality reporting process?
36
Questions & Answers
• Please submit questions through the Q&A panel/ widget
• Documents for this session are in the Resource List widget below, and will be posted to the ACO portlet.
37
Please give us your feedback!
Open the survey widget located in the widget menu at the bottom of your event console.
38
Thank you!
• Slides and a link to the webinar recording will be posted to the ACO portlet. A recording will also be available tomorrow from the audience link you used to attend.
• Please complete the webinar evaluation
• Feel free to send questions, comments, and suggestions for future topics to [email protected]
39





























