Embed Size (px)
Citation preview
Medicines Reconciliation Workshop
Medicines Reconciliation
Dr Gordon BlackClinical Lead SPSP Primary Care, NHS Lothian
Arlene CoulsonLead Clinical Pharmacist, NHS Tayside
Workshop Aims
•Learn about a framework for implementing Medicines Reconciliation
•Learn various tools to support practices to achieve reliability
•Share experiences, challenges and successes
Participants should prepare to leave with clear plans for further development and testing improvements in their local systems.
Workshop Aims
•Learn about a framework for implementing Medicines Reconciliation
•Learn various tools to support practices to achieve reliability
•Share experiences, challenges and successes
Participants should prepare to leave with clear plans for further development and testing improvements in their local systems.
What is Medicines Reconciliation?
It is defined as –
“the process of identifying the most accurate list of a patient’s current medicines –
including the
name, dosage, frequency and route – and comparing them to the current list in use,
recognizing any discrepancies, and documenting any changes, thus
resulting in a complete
list of medications, accurately communicated”.
(IHI 2005)
Why Medicines Reconciliation?
SGHD/CMO(2013)18
20th
September 2013Action
•
NHS Boards are required to be able to demonstrate compliance in discharging their clinical governance
responsibility around medicines reconciliation by ensuring implementation and monitoring of this
guidance.
NHS Boards are required to:
•
Have involvement of patients in safer medicines work
•
Ensuring medicines reconciliation is a core part of training for
all doctors
•
Clinical leadership is imperative in creating a culture in which
patient safety improvements can be
implemented and sustained
Meds Rec
Quiz
Spend 1-2 mins getting to know your table
Work as a team for the quiz – there is a prize!

A 1%
D 30%
B 4%
C 10%
Q What percentage of all hospital admissions may be due to preventable medicine related issues?
B 4%
£2,000
A £89 million
D £523 million
B £125 million
C £466 million
Q What is the estimated annual cost of preventable medicines related admissions in England?
C £466 million
£4,000
A 36%
D 70%
B 53%
C 65%
Q What percentage of practices report that discharge summaries were received in enough time to be useful either ‘all or most of the time’?
£8,000
B 53%
A 12%
D 48%
B 25%
C 39%
Q How often do late discharge summaries directly compromise patient safety?
C 39%
£16,000
A 50%
D 81%
B 63%
C 75%
Q How often, over a 12 month period, were details of prescribed medicines on discharge inaccurate or incomplete all or most of the time?
D 81%
£32,000
A 8%
D 25%
B 11%
C 18%
Q In UK General Medical Practice, what percentage of prescriptions is estimated to contain an error?
B 11%
£64,000
A Safety
D Effectiveness
B Efficiency
C Patient-centredness
Q Which of the following is the most important dimension of quality?
D Effectiveness
£1,000,000
C Patient-centredness
B EfficiencyA Safety
‘Framework for implementing Meds Rec’
What are you doing in your Board?
•
Spend 5 mins
discussing –
‐
Do you have an Enhanced Service?
‐
If you don’t have an ES, how are you implementing the work?
‐
What areas of harm have you focussed upon?
‐
What support have you to implement the Enhanced service?
‘Framework for implementing Meds Rec’ ‐
What we have done in NHS Lothian
•
2012‐2013 Introduced 1st
ES –
Better Warfarin Management•
2013‐2014 2nd
ES – Medicines Reconciliation (and ongoing Warfarin)
2013‐2014 Enhanced Service:‐
Process Mapping
‐
Patient involvement‐
Care Bundle
‐
PDSA ‐
Learning Set
2010-2011 7 practices 21 staff trained
NHS Lothian Spread
2012-2013 93 practices -
259 staff trained
NHS Lothian Spread
2013-2014 102 practices -
200 staff trained
NHS Lothian Spread
NHS Lothian Progress
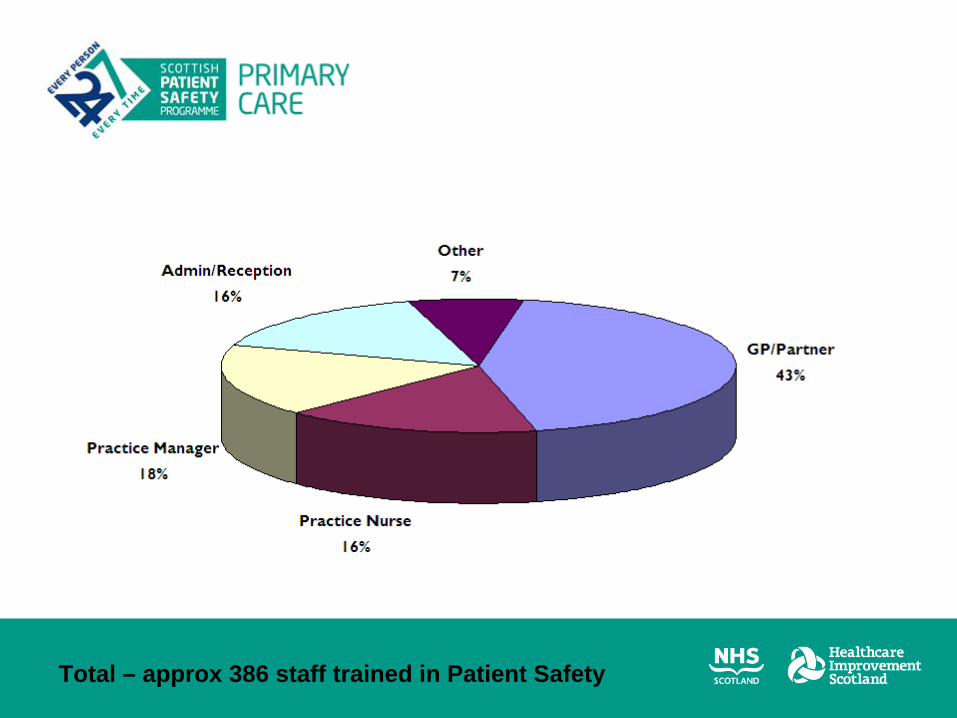
Total – approx 386 staff trained in Patient Safety
What are you doing with Data?
•
Spend ?5 mins
discussing –
‐
What are you currently doing with data?
‐
What might you do differently with your data?
‐
How do you support practices with data?
What have we done with Data?
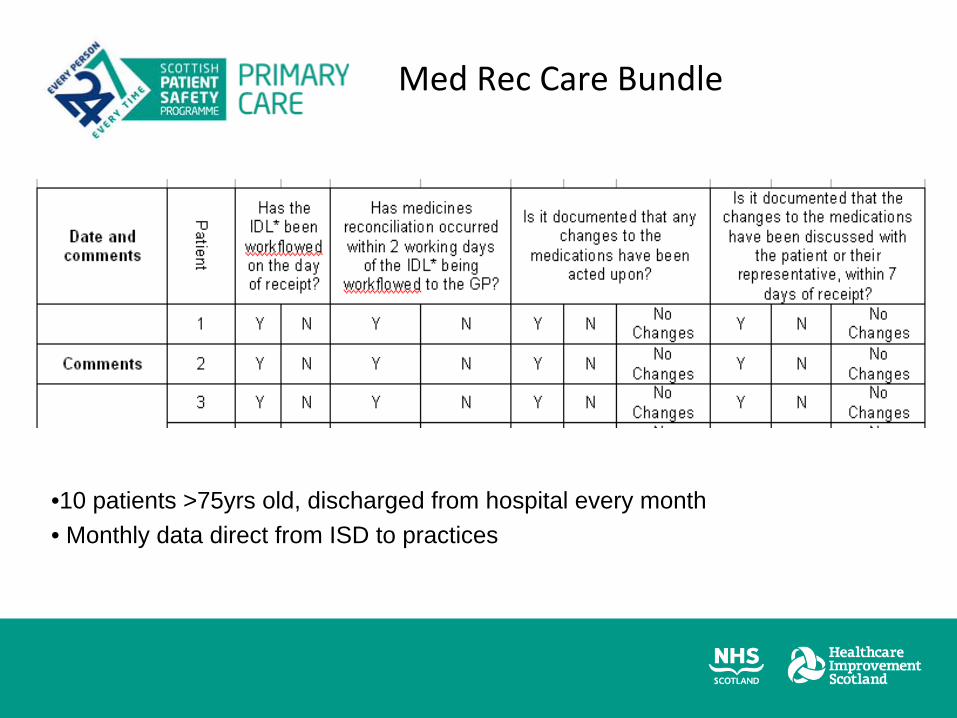
Med Rec
Care Bundle
•10 patients >75yrs old, discharged from hospital every month• Monthly data direct from ISD to practices
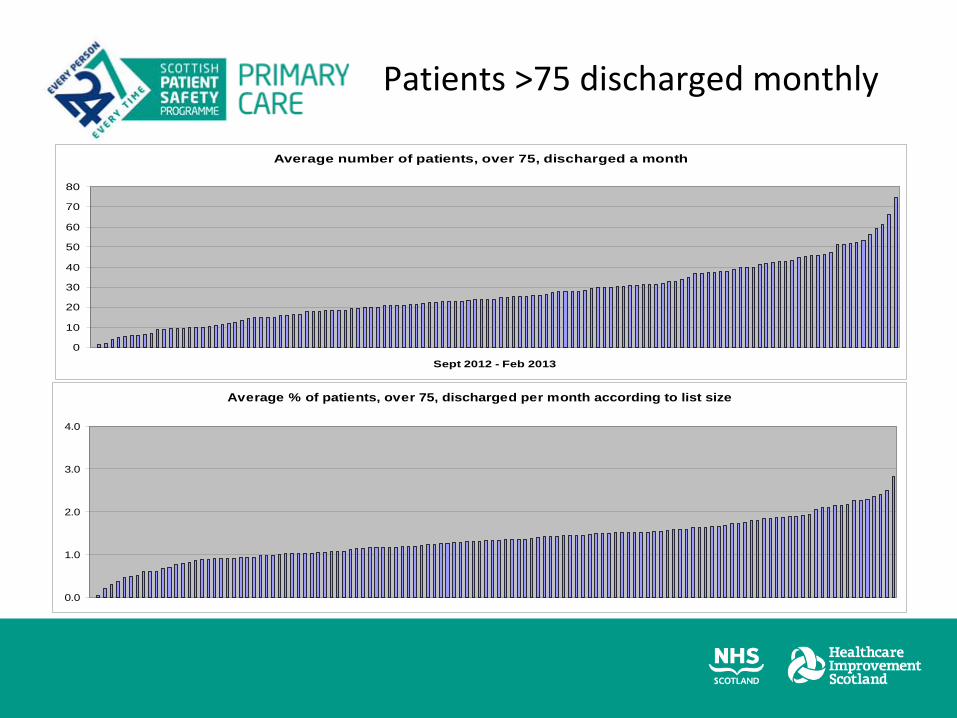
Average number of patients, over 75, discharged a month
0
10
20
30
40
50
60
70
80
Sept 2012 - Feb 2013
Average % of patients, over 75, discharged per month according to list size
0.0
1.0
2.0
3.0
4.0
Patients >75 discharged monthly
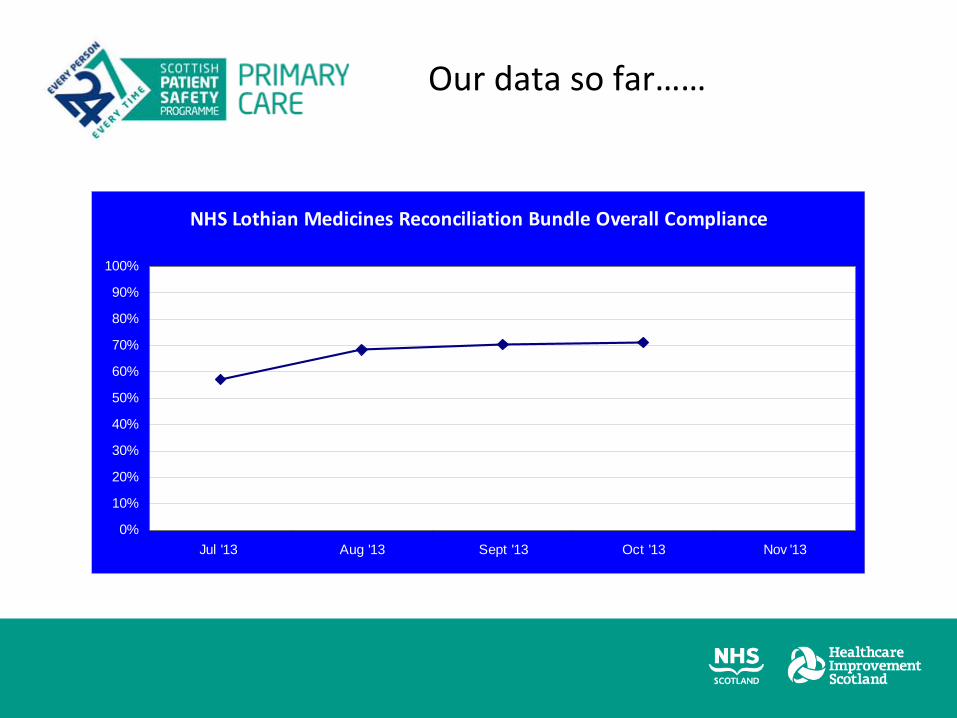
NHS Lothian Medicines Reconciliation Bundle Overall Compliance
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Jul '13 Aug '13 Sept '13 Oct '13 Nov '13
Our data so far……
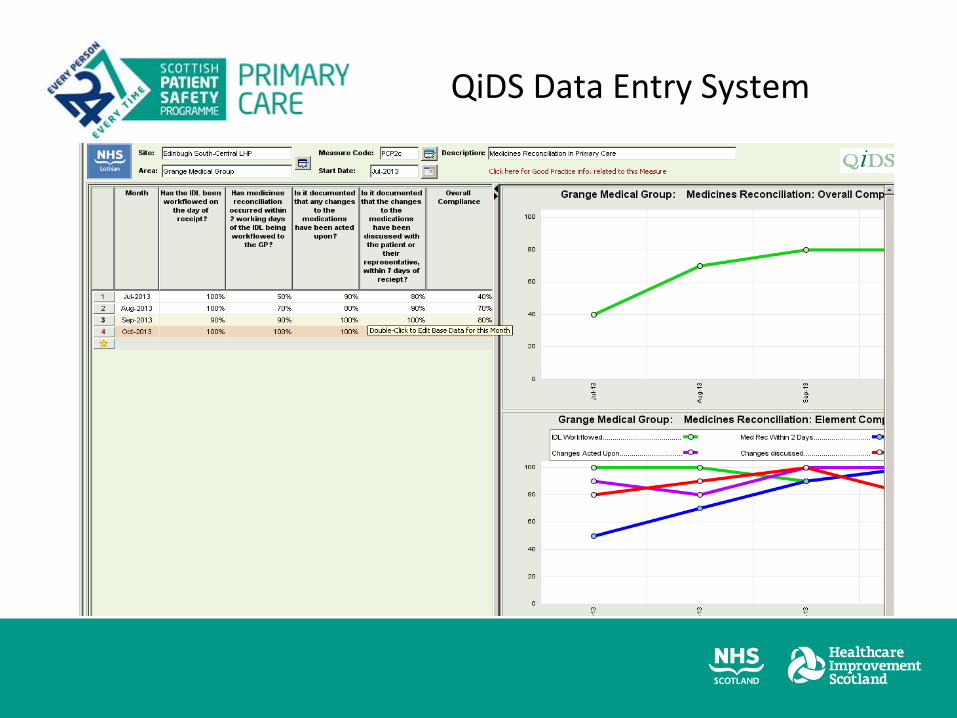
QiDS
Data Entry System

Data entry screen
Are you involving patients and if so how?
•
Spend ?5 mins
discussing –
‐
How are your practice teams involving patients?
‐
How could you support your practices with patient involvement?

•
Public Partner – Isobel Miller
•
Integral part of our ES – all practices must do some form of patient involvement
•
Examples –
Focus groups
Questionnaires – central supported or practice based
3 simple questions: What went well?
What didn’t?
What would you change?
How have we involved patients?
Pilot Meds Rec
Questionnaire results
Medicines Reconciliation SPSP Primary Care Learning Session 2
Arlene Coulson, Lead Clinical Pharmacist, Surgery
NHS Tayside

Twitter #SPT2013
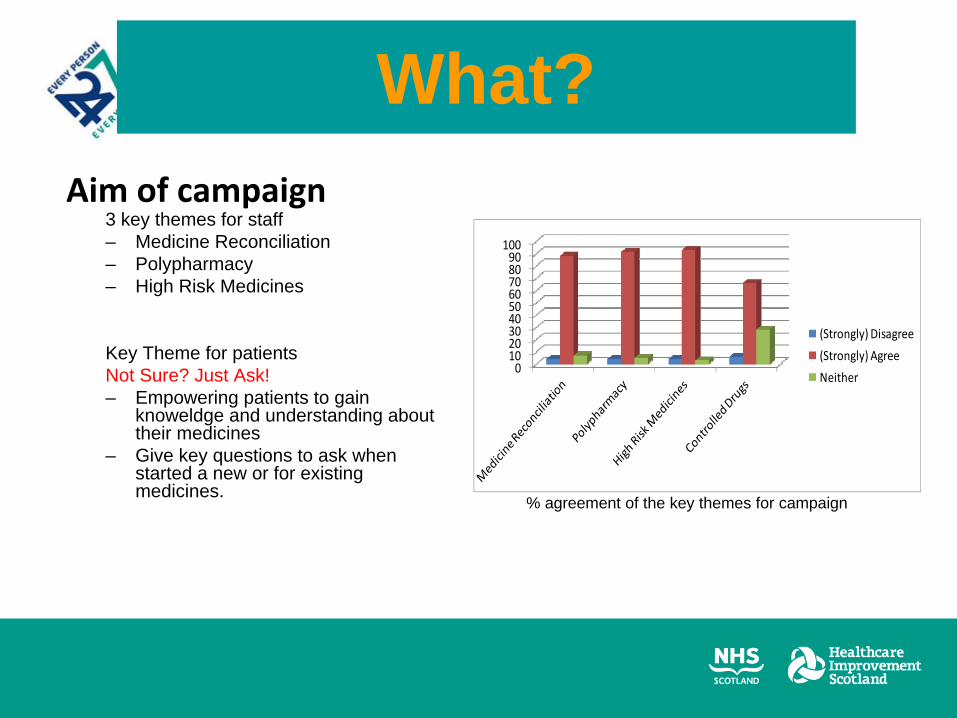
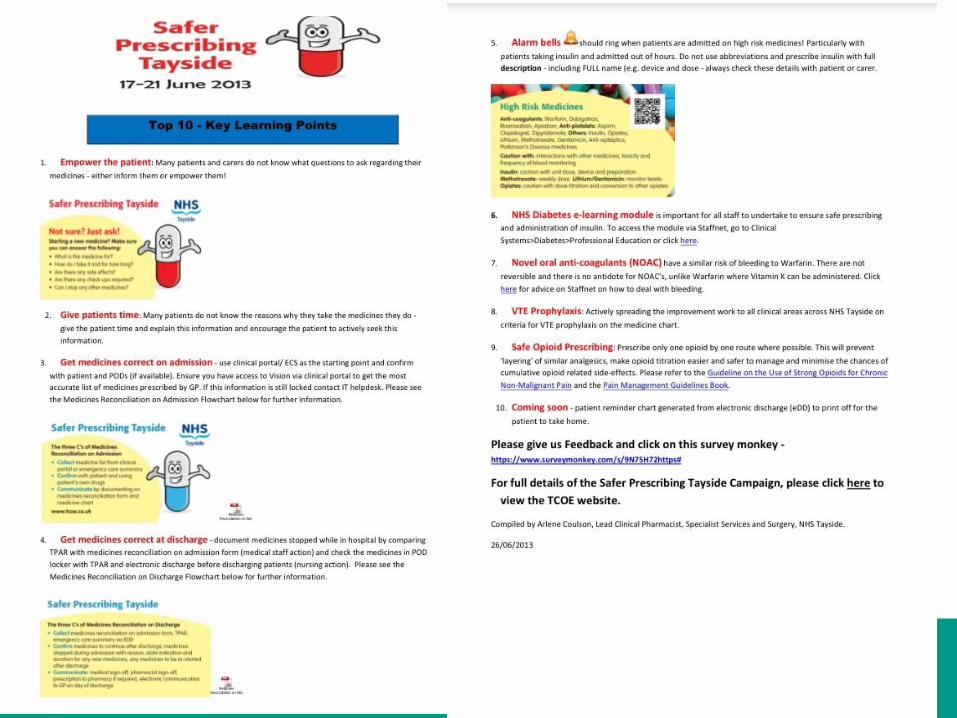
Aim of campaign3 key themes for staff– Medicine Reconciliation– Polypharmacy– High Risk Medicines
Key Theme for patientsNot Sure? Just Ask!– Empowering patients to gain
knoweldge and understanding about their medicines
– Give key questions to ask when started a new or for existing medicines.
What?
0102030405060708090100
(Strongly) Disagree
(Strongly) Agree
Neither
% agreement of the key themes for campaign
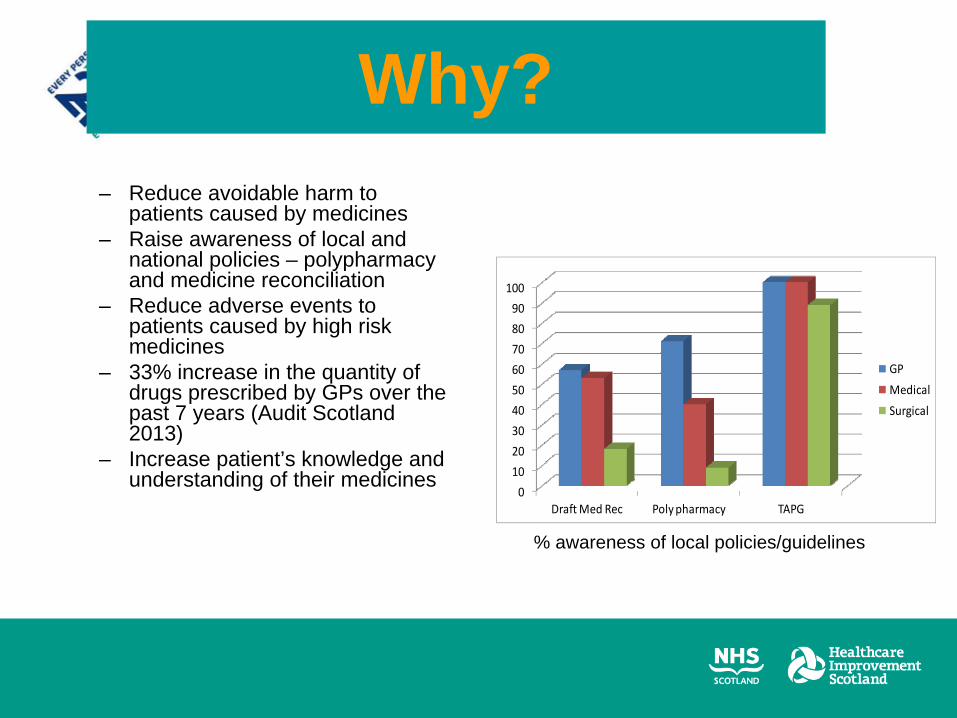
– Reduce avoidable harm to patients caused by medicines
– Raise awareness of local and national policies – polypharmacy and medicine reconciliation
– Reduce adverse events to patients caused by high risk medicines
– 33% increase in the quantity of drugs prescribed by GPs over the past 7 years (Audit Scotland 2013)
– Increase patient’s knowledge and understanding of their medicines
0
10
20
30
40
50
60
70
80
90
100
Draft Med Rec Poly pharmacy TAPG
GP
Medical
Surgical
Why?
% awareness of local policies/guidelines
“Pleased I was taken off some medication that perhaps I didn’t need anymore (with no ill
effects)”
“I often wonder if you can take this whole pile
of pills altogether or not?”
Patient Quotes
“I would really like to know more about my
medicines. I think I would find that most useful”
“When starting a new medicine I wish
someone would take time to speak to me
about what it is for and any problems to watch
for”.
“I don’t know what half of my tablets are for but if I don’t’ take
them I feel awful”
Aim of campaign
• Focus groups – junior doctors and patients• Survey monkey sent to all medical staff for initial input to define campaign
and for formal feedback after campaign. • Stands at Ninewells concourse (patients, public, carers)• Stands on level 5 outside doctors mess (staff)• Programme of daily lunchtime presentations in lecture theatres at Ninewells
Hospital and Perth Royal Infirmary• Communications Plan – media coverage (radio and newspaper), Facebook,
Twitter intranet, extranet, inbox, spectra, patient/staff cards, daily newsletters• TCOE website – hosted all the information
http://www.t-coe.org.uk/_page.php?id=296
How?

•
Patients, Public and Carers
•
Public & Carer Representative
•
Primary and Secondary Care
•
Clinicians/GP’s
•
Community/Locality Pharmacists
•
Multi‐disciplinary Teams
•
Senior managers
•
Executives
Engage across the whole system


"As my memory starts to fail this will make sure I don't forget an important question“
“Yes it reminds you to do the right thing
by asking”
“I never would have thought to ask what
medicines I can stop” Patient Feedback
"There are questions on the card that I wouldn't have
thought of asking”
“Great because there is usually something you
forget to ask”
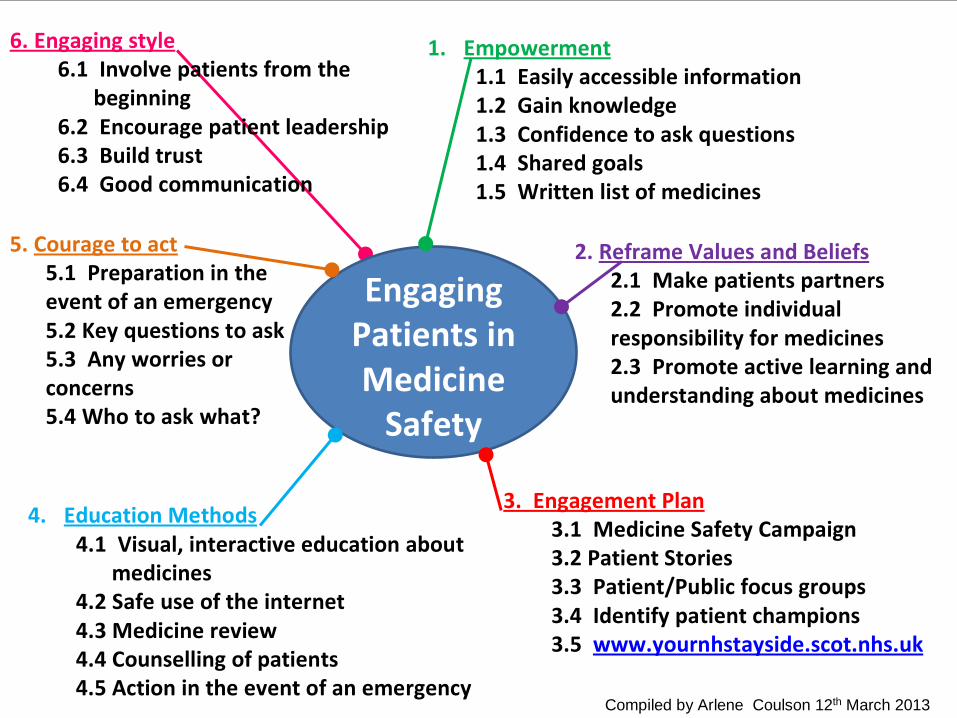
Engaging Patients in Medicine Safety
1. Empowerment1.1 Easily accessible information1.2 Gain knowledge1.3 Confidence to ask questions1.4 Shared goals1.5 Written list of medicines
2. Reframe Values and Beliefs2.1 Make patients partners2.2 Promote individual responsibility for medicines2.3 Promote active learning and understanding about medicines
3. Engagement Plan3.1 Medicine Safety Campaign3.2 Patient Stories3.3 Patient/Public focus groups3.4 Identify patient champions3.5 www.yournhstayside.scot.nhs.uk
4. Education Methods4.1 Visual, interactive education about
medicines4.2 Safe use of the internet4.3 Medicine review4.4 Counselling of patients4.5 Action in the event of an emergency
5. Courage to act5.1 Preparation in the event of an emergency5.2 Key questions to ask 5.3 Any worries or concerns5.4 Who to ask what?
6. Engaging style6.1 Involve patients from the
beginning6.2 Encourage patient leadership6.3 Build trust 6.4 Good communication
Compiled by Arlene Coulson 12th March 2013

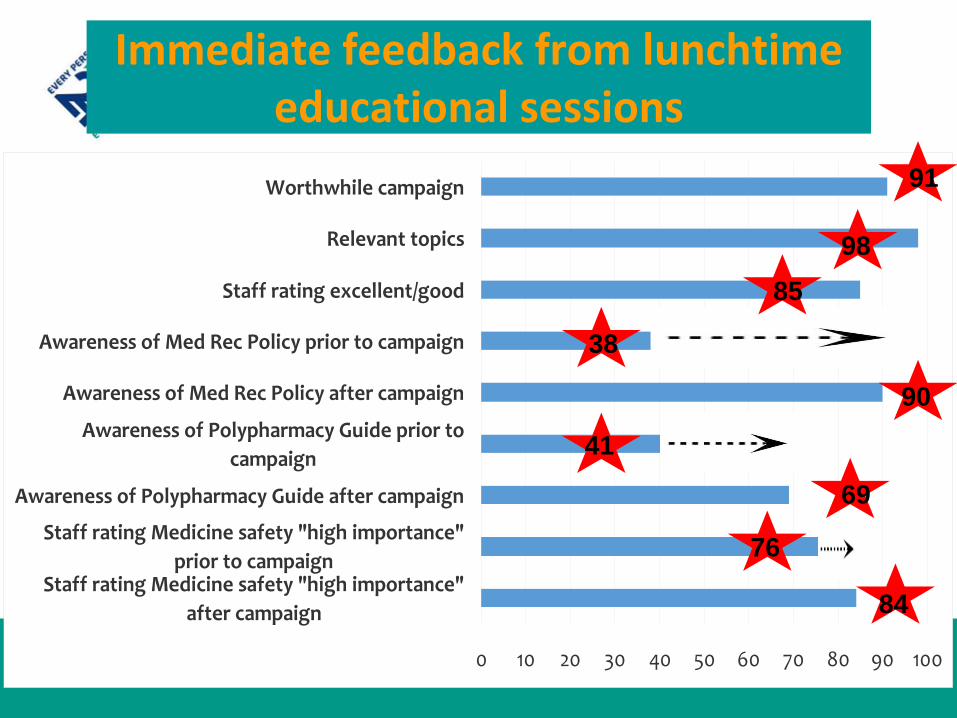
0 10 20 30 40 50 60 70 80 90 100
Staff rating Medicine safety "high importance"after campaign
Staff rating Medicine safety "high importance"prior to campaign
Awareness of Polypharmacy Guide after campaign
Awareness of Polypharmacy Guide prior tocampaign
Awareness of Med Rec Policy after campaign
Awareness of Med Rec Policy prior to campaign
Staff rating excellent/good
Relevant topics
Worthwhile campaign
Immediate feedback from lunchtime educational sessions
91
9885
38
90
41
69
76
84
Future: Patient at centre
What next.....?
Top 10 improvement
ideas
Explore processes for
common themes of medicine
errors
Test and spread these priorities
locally Start planning for next year
How do you provide support for the practices?
•
Spend ?5 mins
discussing –
‐
How do you support practices day to day?
‐
How do you support practices to share their learning?
Initial learning set
CGRMST – see photo
Dashboard
Telephone support
E mail support
Practice visits – targeted or requested
Monthly e mails
Quarterly Newsletter
What support do we provide to practices?
Moving forward – what plans do you have?
•
Spend ?5 mins
discussing –
‐
Have you had a 2nd learning set?
‐
What feedback have you had from practices?
‐
What are your plans for next year?
‐
How do you ensure support from your Health Board/GP colleagues/LMC?
Warfarin SESP Evaluation (89 practices – 55 returned)
•
Does your team feel that improving patient safety within your practice is a priority?
96% said Strongly agree / agree
•
Has the Patient Safety ES made a positive difference to patient safety in your practice?
84% YES
•
Would your practice sign up again in the future if another patient safety ES was offered?
84% YES

What next in NHS Lothian?
•
Executive Walkrounds
in Primary Care
•
Proposed ES –
Handling Outpatient Communication
•
Development of Drug Users Care Bundle
2013‐2014