Embed Size (px)
Citation preview

Ava i l ab l e on l i ne a t www.sc i enced i r ec t . com
Journal of Crohn's and Colitis (2013) 7, 590–593
SHORT REPORT
Mercaptopurine-induced hepatoportalsclerosis in a patient with Crohn's diseaseAna C. Tuyama a, Mark Krakauer b, Mohamed Alzaabi c, Maria Isabel Fiel d,Peter Legnani e, Thomas D. Schiano c,⁎
a Department of Medicine, Mount Sinai School of Medicine, New York, NY, United Statesb Department of Medical Education, Mount Sinai School of Medicine, New York, NY, United Statesc Division of Liver Diseases, Department of Medicine, Mount Sinai School of Medicine, New York, NY, United Statesd Department of Pathology, Mount Sinai School of Medicine, New York, NY, United Statese Division of Gastroenterology, Department of Medicine, Mount Sinai School of Medicine, New York, NY, United States
Received 21 March 2012; received in revised form 6 July 2012; accepted 6 July 2012
⁎ Corresponding author at: Division ofMedicine, Mount Sinai School of MedicinBox 1104, New York, NY 10029, Unitedfax: +1 212 241 2138.
E-mail address: thomas.schiano@m
1873-9946/$ - see front matter © 2012doi:10.1016/j.crohns.2012.07.006
KEYWORDSThiopurine toxicity;Hepatoportal sclerosis;Crohn's disease;Portal hypertension;Mercaptopurine
Abstract
Thiopurines play a pivotal role in the management of inflammatory bowel disease. Azathioprine andmercaptopurine have been associated with a number of liver abnormalities, including hepatitis,veno-occlusive disease, nodular regenerative hyperplasia, and peliosis hepatitis. Patients treatedwith azathioprine and mercaptopurine have their liver chemistry tests routinely checked due to thispotential for hepatotoxicity. Hepatoportal sclerosis is a cause of non-cirrhotic portal hypertension
that is increasingly being recognized; its etiopathogenesis is not well defined. We present the firstcase report of mercaptopurine-induced hepatoportal sclerosis leading to non-cirrhotic portalhypertension in a patient with Crohn's disease. He had been treated with mercaptopurine for fiveyears, and his liver chemistry tests were always within normal limits. This case underscores thepotential serious liver adverse events thatmay arise silently and go undetected during treatmentwithmercaptopurine, and should alert clinicians as to the potential need to discontinuemercaptopurine inthis setting.© 2012 European Crohn's and Colitis Organisation. Published by Elsevier B.V. All rights reserved.Liver Diseases, Department ofe, One Gustave L. Levy Place,States. Tel.: +1 212 659 8502;
ountsinai.org (T.D. Schiano).
European Crohn's and Colitis
Org1. Introduction
Thiopurines, such as azathioprine (AZA) and mercaptopurine(MP), are widely used in the treatment of inflammatory boweldisease (IBD).1 These effective and potent medications canhave significant toxicity, which aremajor obstacles to their longterm use. Liver toxicity is a well-recognized phenomenon that
anisation. Published by Elsevier B.V. All rights reserved.

591Mercaptopurine and Hepatoportal Sclerosis
can have variable presentations.2–4 Physicians often rely onliver chemistry testing in order to detect hepatotoxicity.However, some of these complications may occur withoutprior or ongoing laboratory abnormalities. We present acase of hepatoportal sclerosis (HPS) leading to non-cirrhoticportal hypertension in a patient with Crohn's disease who wastreated with MP for many years without having alterations inliver chemistry tests. HPS is a cause of non-cirrhotic portalhypertension that is being increasingly recognized in light of itsassociation with didanosine use in patients with HIV.5–8 Thiscase highlights a new serious complication of MP use, and alsosuggests for HPS a similar etiopathogenesis as nodular regener-ative hyperplasia (NRH).
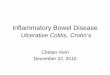
Figure 1 Needle liver biopsy. Photomicrograph of a repre-sentative portal tract and the surrounding periportal area. Notethe abnormally dilated vascular structures (asterisks) in theperiportal spaces representing either herniation of the portalvein branches or some probably representing markedly dilatedsinusoids. The area where the portal vein should be normallylocated is obliterated by fibrous tissue (arrow). (H&E, originalmagnification 40×.)
2. Case report
A 23-year-old white male with a history of Crohn's disease wastransferred from an outside hospital for treatment of a partialsmall bowel obstruction in addition to an intra-abdominalabscess. The patient was diagnosed with Crohn's disease atage 12 and had ileo-colonic involvement with a spontaneousperforation (that was managed conservatively with intrave-nous antibiotics) in the remote past. He had been previouslytreated with aminosalicylates and was started on MP at age17, undergoing a prolonged period of remission. Eight monthsprior to the current admission, the patient developed epistaxisand was first found to have thrombocytopenia, splenomegalyand abnormal liver chemistries as follows: AP 164 μ/L, BR0.5 mg/dL, ALT 62 μ/L, AST 14 μ/L and platelet count 141×103/μL. At that time, MP was discontinued, and the liverenzyme abnormalities gradually returned to normal withinthree weeks. Of note, during the 5 year period that thepatient was treated with MP, he was regularly followed byhis gastroenterologist and had frequent liver chemistrytests that were always normal.
Two weeks prior to the current hospitalization, he wasadmitted to the hospital with a partial small bowel obstruction.This episode was medically managed, and he was treated withbowel rest, steroids and antibiotics. Upon resolution of theobstruction, he received a single dose of infliximab and wasdischarged home. His medical course was complicated by thedevelopment of severe abdominal pain, nausea and vomiting4 days after his hospital discharge. A CT scan of his abdomenwas significant for a partial small bowel obstruction, a 7 cmanterior intra-abdominal abscess, a small retroperitoneal fluidcollection, splenomegaly and ascites. He was then transferredto our hospital for further management. On admission, thepatient was noted to have significant abdominal distentionand tenderness, and pitting leg edema, although no cutaneousstigmata of chronic liver disease were observed on physicalexam. His labs were significant for leukocytosis, microcyticanemia, and a normal platelet count. The liver chemistry testswere significant only for a low albumin (3.0 g/dL) and aslightly prolonged prothrombin time (17.2 s). The patient wastreated with bowel rest and antibiotics. On hospital day 2, heunderwent CT-guided drainage of the anterior abdominalabscess, which yielded 90 mL of purulent material. Adiagnostic paracentesis was done as well, and analysis ofthe ascitic fluid was consistent with portal hypertension(serum ascites albumin gradient greater than 1.1 g/dL)and negative for spontaneous bacterial peritonitis.
During his hospital course, the patient underwent threelarge volume paracenteses and was started on diuretics forpersistent ascites. An extensive work up to establish theetiology of the portal hypertension was initiated. The patienthad no prior history or family history of liver disease. He deniedthe intake of alcohol or the use of recreational, over the counteror herbal drugs. An abdominal ultrasoundwith Doppler flowwasnegative for portal/hepatic/splenic vein thrombosis but showedportal hypertension and liver nodularity suggestive of cirrhosis.Subsequent testing for viral hepatitis, Wilson's disease, alpha-1antitrypsin deficiency, hemochromatosis, and autoimmunehepatitis were unrevealing. An MRCP to evaluate for sclerosingcholangitis showed normal bile ducts, a heterogeneous hepaticparenchyma and nodularity.
A trans-jugular liver biopsy was performed, and portalpressure measurements were consistent with portal hyper-tension. The biopsy showed HPS, with thickened, herniatedportal venules and capillarization of sinusoids (Fig. 1), with noevidence of cirrhosis, biliary obstruction or drug-induced liverinjury. The patient underwent a surveillance upper endoscopyfor varices and was found to have grade 1–2 distal esophagealvarices as well as gastric varices; he was started on nadolol.Sixteen months after the patient's discharge from the hospitalhis Crohn's disease has remained in remission and his liverchemistry tests have been normal with the ascites wellcontrolled with diuretics.
3. Discussion
Thiopurines are immunomodulators that have been widelyused in transplant medicine, cancer chemotherapy, and arecurrently an integral part in the treatment of IBD.1 AZA/MPare nucleotide metabolites incorporated into cellular nucleicacids leading to inhibition of de novo purine synthesis, whichexplains their cytotoxic and immunosuppressive properties.

592 A.C. Tuyama et al.
They have been shown to induce and maintain remission inIBD patients in whom corticosteroids cannot be tapered ordiscontinued. These drugs are recognized steroid-sparingagents, as they allow the withdrawal of steroids, thuspreventing the long term side effects of chronic steroiduse. However, there are many caveats to their use sincepatients tend to be treated for a prolonged period of time, asthe risk of recurrence increases once treatment is discontinuedand, the optimal duration of therapy has not been determined.A major drawback in using these drugs is related to theirsignificant toxicity profile.
In most clinical trials, as many as 15% of patients had theirtreatment discontinued as a result of both the short term andlong term toxicities of AZA/MP. The adverse events can bedivided into those that are dose independent and those thatare dose-dependent.2,3 The drug-independent effects usuallydevelop within 2–4 weeks of treatment, and can present asallergic reactions, or idiosyncratic phenomena such as drug-induced pancreatitis. These toxicities cannot be reliablypredicted by monitoring blood counts or measuring metabo-lite concentrations. Among the dose-dependent toxicities,the most recognized and potentially lethal toxicity ismyelosuppression. Drug-induced hepatitis can result fromeither a hypersensitivity phenomena or a dose-dependenteffect. The use of 6-TGN in IBD patients is being increasingscrutinized for its presumed hepatotoxic profile, as it hasbeen linked to the development of NRH and non-cirrhoticportal hypertension.9,10
The incidence of hepatotoxicity was initially reported to beas low as 0.3% by Present et al.11 In a more recent systematicreview of the literature, Gisbert et al. estimated the incidenceof hepatotoxicity in IBD patients given AZA/MP to be approx-imately 1% per patient per year of treatment.12 Most of thesecases occurred during the first 6 months of treatment.However, there is significant variability among case series,which probably results from the lack of standardized defini-tions, and difficulties in diagnosis given the absence of specificmarkers or tests. Furthermore, these calculated rates areestimated from retrospective studies with relatively lownumbers of patients and limited follow up.
A number of liver abnormalities have been described inpatients taking AZA/MP. These range frommild and transientderangements of liver chemistry tests that resolve uponreduction or discontinuation of therapy, to more severeforms with variable prognoses. They can be divided into dose-independent hypersensitivity reactions such as acute hepati-tis and idiosyncratic cholestatic hepatitis, which are usuallyassociated with biochemical abnormalities of liver chemistrytests, and dose-dependent endothelial cell injury such asNRH, veno-occlusive disease, and peliosis hepatitis.13,14 HPShas previously been noted in patients taking AZA but not inMP. The main clinical manifestation of these vascular lesionsis portal hypertension. The diagnosis of thiopurine-inducedliver toxicity is usually made in the setting of liver chemistryabnormalities that arise with treatment and that resolveupon drug withdrawal, and with relapse upon re-introductionof the offending agent. However, these dose-dependentadverse events may occasionally present without prior liverenzyme abnormalities,15 making its diagnosis more difficult.
HPS has been documented in patients treated with azathi-oprine following renal transplantation.16 The current case is thefirst reported of HPS induced by MP in a patient with IBD. HPS is
a clinico-pathologic entity associated with non-cirrhotic portalhypertension. It was first described by Mikkelsen in 1965,17 andis also known as idiopathic portal hypertension in Japan, andnoncirrhotic portal fibrosis in India. The primary lesion consistsof fibrotic, sclerosed, and obliterated portal vein branches(phlebosclerosis), which are found in portal tracts, and areassociated with marked dilatation of sinusoids (megasinusoids).The diagnosis is based on the presence of portal hypertensionwith normal or near normal liver chemistry tests, a non-cirrhoticliver, and portal fibrosis without diffuse nodule formation onliver biopsy. Portal vein thrombosis can be seen in somepatients. Often the histological changes of HPS can be verysubtle and the liver biopsy may be read as being normal,especially in the absence of an adequately-sized specimen. It iscrucial for the clinician to communicate with the pathologistthe clinical suspicion of portal hypertension. Early changesdescribed in patients with HPS include lymphoid cell infiltrationof the portal tracts and sub-endothelial regions of portal veinbranches. Portal veins may be thickened to an extent thatthey start resembling the adjoining hepatic arterioles of thecorresponding portal tract. Patients usually present withcomplications of portal hypertension such as ascites, varicealbleeding, and splenomegaly with or without hypersplenism;treatment is symptomatic. However, recent reports haveshown that a subset of these patients may develop hepaticsynthetic compromise in addition to portal hypertension,necessitating liver transplantation.18,19 All patients inthese series were felt to have other etiologies for theirdecompensated liver disease; HPS was unrecognized priorto transplantation. None of these cases of HPS was directlyascribable to MP use.
This case highlights the potential severe and irreversibleadverse events that can result from prolonged treatmentwith AZA/MP. In the renal transplant literature, most of thecases of dose-dependent hepatotoxicity induced by azathio-prine occurred after many years of treatment (4–6 years),which reinforces a probable dose- and time-dependenteffect.20–23 However, as mentioned above, most of theliterature in the IBD population is based on retrospectivestudies with very short follow up. There has been oneprospective study assessing the rate and risk factors associat-ed with thiopurine-induced liver injury in IBD patients.24 Thisstudy followed a cohort of 161 IBD patients withmedian followup of 271 days, and found that liver chemistry abnormalitieswere present in 13% of patients, and hepatotoxicity defined byelevation of liver enzymes above pre-determined parameters,was present in 10% of their cohort, necessitating treatmentwithdrawal in 75% of them. A percentage of patients were ableto continue optimal doses of AZA/MP after dose adjustmentand monitoring of liver chemistries. However, this strategymay be problematic and risky, as the long term cumulativeeffect of these drugs has not been well defined, especially inpatients who present with liver chemistry abnormalities,suggesting an underlying susceptibility to the toxic effects ofAZA/MP.
The current case also raises the question of how to bestpredict and prevent liver damage in patients treated with AZA/MP. It is recommended to check liver enzymes regularly duringthe treatment course, and to either decrease or discontinuethese medications if abnormalities arise. This common practiceallows for early detection of dose-independent hypersensitivityreactions. However, as demonstrated by this case report, dose-

593Mercaptopurine and Hepatoportal Sclerosis
dependent toxicities such as HPS may develop silently withoutabnormalities in liver chemistries, highlighting the importanceof determining better methods for early detection of thesepotential severe and irreversible toxicities. It is yet to bedetermined if genetic testing or monitoring drug levels willhave an impact on these type of events. It is also important todetermine when and in which circumstances these patientsshould undergo liver biopsy. There are no guidelines forsurveillance of the development of portal hypertension inpatients receiving long-term MP use. Periodic Doppler ultraso-nography will detect established portal hypertension but maymiss the gradual development of elevated portal pressures.Detection of portal vein thrombosis or increasing spleen sizemay be helpful for early detection. When available, serialtransient elastography measurements (Fibroscan) might detectthe interval development of fibrosis suggestive of HPS or NRH.25
This is the first case report of MP induced HPS leading toportal hypertension in an IBD patient. It thus seems that HPSmay have a similar etiopathogenesis as NRH, which is also acause of drug-induced liver injury due to a hepatic vascularendothelial insult. Both can be seen concurrently within thesame liver biopsy and both have been associated withdidanosine use in patients with HIV.5,6,26 A recent report of apatient developing HPS in paired liver biopsies showing portalvenule endotheliitis and central venulitis that progressed towell established portal venopathy despite resolution of theacute endothelial injury, suggests that in some cases HPS maynot be reversible.
Conflict of interest
None of the authors have a conflict of interest with theproduction of this manuscript.
All the authors contributed in caring for the patients and inwriting and reviewing this manuscript.
References
1. Siegel CA, Sands BE. Review article: practical management ofinflammatory bowel disease patients taking immunomodulators.Aliment Pharmacol Ther 2005;22:1–16.
2. de Jong DJ, Derijks LJJ, Naber AHJ, Hooymans PM, Mulder CJJ.Safety of thiopurines in the treatment of inflammatory boweldisease. Scand J Gastroenterol 2003;38:69–72.
3. Derijks LJJ, Gilissen LPL, Hooymans PM, Hommes DW. Reviewarticle: thiopurines in inflammatory bowel disease. AlimentPharmacol Ther 2006;24:715–29.
4. Al Hadithy AFY, de Boer NKH, Derijks LJJ, Escher JC, Mulder CJJ,Brouwers JRBJ. Thiopurines in inflammatory bowel disease:pharmacogenetics, therapeutic drug monitoring and clinical rec-ommendations. Dig Liver Dis 2005;37:282–97.
5. Schiano TD, Uriel A, Dieterich DT, Fiel MI. The development ofhepatoportal sclerosis and portal hypertension due to didano-sine use in HIV. Virchows Arch 2011;458:231–5.
6. Schiano TD, Kotler DP, Ferran E, Fiel MI. Hepatoportal sclerosisas a cause of noncirrhotic portal hypertension in patients withHIV. Am J Gastroenterol 2007;102:2536–40.
7. Saifee S, Joelson D, Braude J, Shrestha R, Johnson M, Sellers M,et al. Noncirrhotic portal hypertension in patients with humanimmunodeficiency virus-1 infection. Clin Gastroenterol Hepatol2008;6:1167–9.
8. Kovari H, Ledergerber B, Peter U, Flepp M, Jost J, Schmid P, et al.Swiss H.I.V. cohort study. Association of noncirrhotic portal
hypertension in HIV-infected persons and antiretroviral therapywith didanosine: a nested case–control study. Clin Infect Dis2009;49:626–35.
9. Dubinsky MC, Lamothe S, Yang HY, Targan SR, Sinnett D, ThéorêtY, et al. Pharmacogenomics and metabolite measurement formercaptopurine therapy in inflammatory bowel disease. Gastro-enterology 2000;118:705–13.
10. Dubinsky MC, Vasiliauskas EA, Singh H, Abreu MT, Papadakis KA,Tran T, et al. 6-Thioguanine can cause serious liver injury ininflammatory bowel disease patients.Gastroenterology 2003;125:298–303.
11. Present DH, Meltzer SJ, Krumholz MP, Wolke A, Korelitz BI.Mercaptopurine in themanagement of inflammatory bowel disease:short- and long-term toxicity. Ann Intern Med 1989;111:641–9.
12. Gisbert JP, Gonzalez-Lama Y, Mate J. Thiopurine-induced liverinjury in patients with inflammatory bowel disease: a systematicreview. Am J Gastroenterol 2007;102:1518–27.
13. de Boer NK, Mulder CJ, van Bodegraven AA. Myelotoxicity andhepatotoxicity during azathioprine therapy. Neth J Med 2005;63:444–6.
14. Mion F, Napoleon B, Berger F, Chevallier M, Bonvoisin S, Descos L.Azathioprine induced liver disease: nodular regenerative hyper-plasia of the liver and perivenous fibrosis in a patient treated formultiple sclerosis. Gut 1991;32:715–7.
15. Arnott ID, Ghosh S. Portal hypertension in the presence ofminimal liver damage in Crohn's disease on long-term azathio-prine: possible endothelial cell injury. Eur J GastroenterolHepatol 2000;12:569–73.
16. Roland S, Delwaide J, Cornet G, Mahieu P, Jacquet N, BelaicheJ. Clinical case of the month. Hepatoportal sclerosis in a patienttreated with azathioprine. Rev Med Liege 1998;53:450–3.
17. Mikkelsen WP, Edmondson HA, Peters RL, Redeker AG, ReynoldsTB. Extra- and intrahepatic portal hypertension without cirrhosis(hepatoportal sclerosis). Ann Surg 1965;162:602–20.
18. Isabel Fiel M, Thung SN, Hytiroglou P, Emre S, Schiano TD. Liverfailure and need for liver transplantation in patients withadvanced hepatoportal sclerosis. Am J Surg Pathol 2007;31:607–14.
19. Krasinskas AM, Eghtesad B, Kamath PS, Demetris AJ, AbrahamSC. Liver transplantation for severe intrahepatic noncirrhoticportal hypertension. Liver Transpl 2005;11:627–34.
20. Haboubi NY, Ali HH, Whitwell HL, Ackrill P. Role of endothelial cellinjury in the spectrum of azathioprine-induced liver disease afterrenal transplant: light microscopy and ultrastructural observations.Am J Gastroenterol 1988;83:256–61.
21. Olsen TS, Fjeldborg O, Hansen HE. Portal hypertension withoutliver cirrhosis in renal transplant recipients. APMIS Suppl 1991;23:13–20.
22. Yoshimura N, Oka T, Ohmori Y, Yasumura T, Kohnosu H, KobashiT. Idiopathic portal hypertension in renal transplant recipients:report of two cases. Surg Today 1994;24:1111–4.
23. Nataf C, Feldmann G, Lebrec D, Degott C, Descamps JM, Rueff B,et al. Idiopathic portal hypertension (perisinusoidal fibrosis) afterrenal transplantation. Gut 1979;20:531–7.
24. Bastida G, Nos P, Aguas M, Beltrán B, Rubín A, Dasí F, et al.Incidence, risk factors and clinical course of thiopurine-inducedliver injury in patients with inflammatory bowel disease. AlimentPharmacol Ther 2005;22:775–82.
25. Scourfield A, Waters L, Holmes P, Panos G, Randell P, Jackson A,et al. Non-cirrhotic portal hypertension in HIV-infected individ-uals. Int J STD AIDS 2011;22:324–8.
26. Mallet VO, Varthaman A, Lasne D, Viard JP, Gouya H, Borgel D,et al. Acquired protein S deficiency leads to obliterative portalvenopathy and to compensatory nodular regenerative hyperplasiain HIV-infected patients. AIDS 2009;23:1511–8.