Embed Size (px)
Citation preview

bs
A
The Journal of Emergency Medicine, Vol. 42, No. 1, pp. e19–e21, 2012Copyright © 2012 Elsevier Inc.
Printed in the USA. All rights reserved0736-4679/$–see front matter
doi:10.1016/j.jemermed.2009.08.014
Visual Diagnosisin Emergency Medicine
METASTATIC NEUROBLASTOMA: THE MIMICKER OF BASILAR SKULLFRACTURE IN CHILDREN
Antonio E. Muñiz, MD, FACEP, FAAP, FAAEM
Department of Emergency Medicine and Pediatrics, The University of Texas Health Science Center at Houston, Houston, TexasReprint Address: Antonio E. Muñiz, MD, FACEP, FAAP, FAAEM, Department of Emergency Medicine and Pediatrics, The University of Texas
Health Science Center at Houston, 6431 Fannin Street, JJL-451, Houston, TX 77030
ffp
CASE REPORTS
Patient 1
A 21-month-old Caucasian boy was seen at anotherhospital with a chief complaint of mild ecchymosis in theleft infraorbital region. The parents denied any knowntrauma or fall. His examination did not reveal any obvi-ous fracture and he was discharged with a presumeddiagnosis of facial contusion from a fall. Three days laterhe presented with worsening ecchymosis and markedbilateral periorbital swelling.
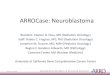
The child’s past medical history was unremarkable.He took no medications and had no allergies. Vital signswere normal. His facial examination showed markedswelling and periorbital ecchymosis with proptosis ofboth eyes. His ocular movements were decreased (Figure1). His pupils were 4 mm and reactive. His nasal pas-sages were obstructed with a small mass. He was lethar-gic but arousable. The remainder of his examination wasunremarkable.
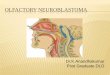
The computed tomography (CT) scan of his headshowed soft tissue mass in the orbital regions pushing theeyes forward and extensive bony erosions (Figures 2 and 3).
He was admitted to the pediatric intensive care unit. Aiopsy of the tissue revealed neuroblastoma. He wastarted on chemotherapy, but he developed neutropenic
RECEIVED: 28 February 2009; FINAL SUBMISSION RECEIVED:
CCEPTED: 23 August 2009e19
ever and acute respiratory distress syndrome and after aew days, life support treatment was withdrawn and theatient died.
ly 2009;
Figure 1. Periorbital ecchymosis and swelling caused bymetastatic neuroblastoma.
11 Ju

e20 A. E. Muñiz
Patient 2
A 30-month-old Caucasian boy presented with worsen-ing periorbital edema and distinctive ecchymosis. Theparents denied any known trauma. The child’s past med-ical history was unremarkable. He took no medicationsand had no allergies. Vital signs were normal. His facialexamination showed marked swelling and very darkperiorbital ecchymosis (Figure 4). His pupils were 3 mmand reactive. The remainder of his examination, includ-ing his neurologic examination, was unremarkable.
He was admitted to the pediatric floor. He had ele-vated urinary levels of the catecholamine metabolites,
Figure 2. Computed tomography (CT) scan of the headshowing extensive tumor invasion of the orbits and exten-sive bony erosions, as shown by the arrows.
Figure 3. Computed tomography (CT) scan of the headshowing extensive tumor invasion of the orbits and exten-
sive bony erosions.vanillylmandelic acid (VMA) and homovanillic acid(HVA). An abdominopelvic CT scan revealed an abdom-inal mass and the biopsy confirmed neuroblastoma. Hewas started on chemotherapy, but he died of sepsis a fewweeks later.
DISCUSSION
Periorbital ecchymosis in children is usually caused bytrauma to the anterior floor of the skull. Hemorrhagefrom the fracture infiltrates the periorbital tissues, caus-ing the periorbital ecchymosis. This can either be in-flicted or not. However, on occasion a metastatic neu-roblastoma can mimic these physical findings (1).Neuroblastoma is the most common extracranial solid tu-mor in children under the age of 5 years. Metastatic neu-roblastoma has a predilection to spread to the orbitalspaces, causing periorbital edema and ecchymosis (“rac-coon eyes”), which, on occasion, can be initially thoughtto occur from a basilar skull fracture (1–3). Ophthalmo-logic manifestations are a result of periorbital soft tissueinfiltration of tumor, producing proptosis and periorbitalhematoma or ecchymosis (4,5). There are a multitude ofdifferent diagnoses that could present with periorbitaledema and ecchymosis in children, such as lymphoma,bleeding disorders (hemophilia, thrombocytopenia), drug-induced coagulopathy (warfarin, heparin), amyloidosis,Kaposi’s sarcoma, infection of the soft tissue, or myx-
Figure 4. Periorbital ecchymosis and swelling cause by met-astatic neuroblastoma.
edema (2,3).

Tdmmsacom
Neuroblastoma e21
CONCLUSION
his case is presented to increase awareness of the broadifferential diagnosis associated with periorbital ecchy-osis and edema, as potential causes include both trau-atic and medical etiologies. The clinical evaluation
hould include appropriate imaging as well as laboratorynalysis based on clinical suspicion. Although both ac-idental and non-accidental trauma could be entertained,ur two cases highlight the importance of considering
edical causes as well.REFERENCES
1. Bohdiewicz PJ, Gallegos E, Fink-Bennett D. Raccoon eyes and theMIBG super scan: scintigraphic signs of neuroblastoma in a case ofsuspected child abuse. Pediatr Radiol 1995;25:S90–2.
2. Cliff JF, Newman L, Malone M, et al. Facial features of widespreadneuroblastoma: a case report. Int J Paediatr Dent 2001;11:215–20.
3. Gumus K. A child with raccoon eyes masquerading as trauma. IntOphthalmol 2007;27:379–81.
4. Belgaumi AF, Kauffman WM, Jenkins JJ, et al. Blindness in chil-dren with neuroblastoma. Cancer 1997;80:1997–2004.
5. Musarella MA, Chan HS, DeBoer G, et al. Ocular involvement in
neuroblastoma: prognostic implications. Ophthalmology 1984;91:936–40.