Embed Size (px)
Citation preview

Dr Keren received his BS, MS, and MD degrees from the University of Illinois, the latter in 1971. He completed his residency
training in Anatomic and Clinical Pathology and postdoctoral training in immunopathology and immunohematology at The Johns Hopkins Hospital from 1971-1976. From 1976-1978 he served as a Major in the United States Armed Forces at the Walter Reed Army Institute for Research in Washington, DC. He joined the Department of Pathology of the University of Michigan in 1978. From 1989 through 2011, he served as the Medical Director of Warde Medical Laboratory while continuing as an Adjunct Clinical Professor of Pathology at the University of Michigan.
Dr Keren has authored over 160 peer-reviewed articles and has written or edited 13 books. He has received several awards, including the Carl A Jolliff Award from the Clinical and Diagnostic Immunology Division of the American Association of Clinical Chemists, a Lifetime Achievement Award from the Michigan Society of Pathologists, the Israel Davidsohn Award, the Distinguished Service Award, and the Mastership Award from the American Society for Clinical Pathology. Dr Keren served as the President of the American Society for Clinical Pathology (2003) and as the President of the American Board of Pathology (2011). He is currently Professor of Pathology and Associate Director, Clinical Pathology Laboratories at the University of Michigan.

v
ISBN 978-089189-5916
Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xiv
CHAPTER 1: Protein Structure and Electrophoresis . . . . .1Protein Structure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Peptide Bonds and Polypeptides . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Primary Structure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Secondary Structure. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Tertiary Structure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Quaternary Structure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Posttranslational Modifications. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Glycosylation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Determinants of Electrical Charge of the Protein . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Electrophoretic Techniques in the Clinical Laboratory. . . . . . . . . . . . . . . . . . . . . . . . . . . . .4Moving Boundary Electrophoresis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4Zone Electrophoresis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Filter Paper Support . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Cellulose Acetate Support . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Agarose Support . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Capillary Electrophoresis (CE) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7Early Clinical Applications of Electrophoresis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8High-Resolution Techniques . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Contents

vi
CONTENTSPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
CHAPTER 2: Techniques for Protein Electrophoresis and Measurement of M-proteins . . . . . . . . . . . . . . . . . . . 12Principles of Protein Electrophoresis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Electrophoresis in Agarose. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Electrophoresis on Cellulosic Media. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Capillary Electrophoresis (CE) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15CE and M-proteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Interferences with Detection of M-proteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Interference by Chimeric and Humanized Monoclonal Antibody Therapies . . . . . . . 19
Pediatric Reference Ranges . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Measurement of Protein Fractions Densitometry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 205 or 6 Fractions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Densitometry vs Nephelometry to Measure M-proteins in Serum . . . . . . . . . . . . . . . . 21
Heavy-Light Chain Assay. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
CHAPTER 3: Identification of M-proteins: Immunoelectrophoresis, Immunofixation, Immunosubtraction, & Isoelectric Focusing . . . . . . . . . . . . . . 26Principles of Immunoprecipitation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Antibody-Antigen Interaction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Interpreting Antibody-Antigen Precipitation Reactions . . . . . . . . . . . . . . . . . . . . . . . . . 28Double Diffusion in 2 Directions (Ouchterlony Technique) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Combining Antibody-Antigen Interactions in Gel with Electrophoresis . . . . . . . . . . . . . . . . . . . . . 29
Immunoelectrophoresis (IEP) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Limitations of IEP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Immunofixation (IFE) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Immunosubtraction (ISUB) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Isoelectric Focusing (IEF) and Immunoblotting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40

ISBN 978-089189-5916
vii
CONTENTS
CHAPTER 4: Proteins Identified by Serum Protein Electrophoresis . . . . . . . . . . . . . . . . . 42Prealbumin and Albumin Regions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
Transthyretin (Prealbumin) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Albumin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Decreased Albumin. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
Bisalbuminemia or Alloalbuminemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
Analbuminemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
Increased Albumin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
α Region. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48α1-Lipoprotein . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48α1-Antitrypsin (αAT). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
Decreased αAT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
Strategies to Detect αAT Variants. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
Increased αAT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
α1-Fetoprotein (αFP) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54α1-Acid Glycoprotein (αAG) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54α1-Antichymotrypsin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55α2-Macroglobulin (α2M). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
Increased α2M . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Decreased α2M. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Haptoglobin. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56Decreased Haptoglobin. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
Increased Haptoglobin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
Ceruloplasmin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60Fibronectin (Cold Insoluble Globulin) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
β RegionTransferrin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
Transferrin Variants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
Increased Transferrin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
Decreased Transferrin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
C3 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62Decreased C3 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
Increased C3 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
C4 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64Fibrinogen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64

viii
CONTENTSPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
γ Region. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64C-Reactive Protein (CRP) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64Immunoglobulins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Immunoglobulin Structure. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
IgG . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
IgM. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
IgA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
IgE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
IgD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69

ISBN 978-089189-5916
ix
CONTENTS
CHAPTER 5: Pattern Interpretations in Serum . . . . . . . . . . 75Approach to Pattern Interpretation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
Initial Processing of the Sample . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
Overview of the Electrophoretic Strip . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
Interpretation of the Individual Sample. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78
Serum Pattern Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80Liver Disease Patterns. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
Cirrhosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
Hepatitis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
Biliary Obstruction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
Renal Disease Pattern . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83Gastrointestinal Protein Loss . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84Protein Loss through Thermal Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84Acute Phase Reaction Pattern . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85Protein Abnormalities in Autoimmune Disease. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86Protein Patterns in Hyperestrogen Effect . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87γ Globulin Patterns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87
Increased γ Globulin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .87
Restricted Polyclonal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88
Oligoclonal Bands . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91
Infections. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92
Lymphoproliferative Disease. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
Post-Stem Cell Transplantation Oligoclonal Responses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
Polyclonal Gammopathy in Neoplastic Diseases. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95Angioimmunoblastic T-Cell Lymphoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
Posttransplant Lymphoproliferative Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
Other Associations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
Decreased γ-Globulin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96Bruton X-Linked Agammaglobulinemia (XLA) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
Transient Hypogammaglobulinemia of Infancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
Common Variable Immunodeficiency Disease. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
X-Linked Lymphoproliferative syndromes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
Iatrogenic Hypogammaglobulinemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
Chronic B-Cell Lymphoproliferations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98

x
CONTENTSPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
CHAPTER 6: Conditions Associated with Monoclonal Gammopathies. . . . . . . . . . . . . . . . . . 105Differentiation of B Lymphocytes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
Maturation Prior to Activation by Antigen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105Maturation after Activation by Antigen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106
Conditions Associated with M-Proteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106Monoclonal Gammopathy of Undetermined Significance (MGUS) . . . . . . . . . . . . . . . . . . . . . . . . 108Smoldering Multiple Myeloma (SMM). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 109Multiple Myeloma (MM) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 110
Clinical Presentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 110
Epidemiological Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 110
MM Pathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 112
Staging and Prognosis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113
Immunoglobulin Isotypes in MM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113
Immunosuppression in MM and B-Cell Lymphoproliferative Disorders . . . . . . . . . . . . . . . . . . . 124Heavy Chain Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 125
Waldenström Macroglobulinemia (WM) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 128
M-proteins in Lymphoma and Leukemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 130
M-proteins Associated with Tissue Deposition: AL Amyloidosis and Light Chain Deposition Disease . . . . . 131
Solitary Plasmacytoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 133
M-proteins Not Associated with B Lymphoproliferative Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . 133
POEMS Syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 134M-proteins in Infectious Diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 134M-proteins in Immunodeficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 135Cryoglobulins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 136Bands Mistaken for M-proteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 140
Fibrinogen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 140
Genetic Variants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141
C-Reactive Protein (CRP) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141
Hemolysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141
Radiocontrast Dyes and Antibiotics. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141
Unusual Effects of M-proteins on Laboratory Tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141Electrophoretic Findings Following Chemotherapy and ASCT Therapy . . . . . . . . . . . . . . . . . . . . . . . . 142
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142

ISBN 978-089189-5916
xi
CONTENTS
CHAPTER 7: Examination of Urine for Proteinuria . . . . 155Urine Protein Composition. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155
Size and Amount of the Protein . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155Charge of the Protein . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155Hydrostatic Pressure. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155Glomerular Filtrate and Tubular Absorption . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155Protein in Normal Urine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 156
Measurement of Total Urine Protein . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 156
Concentration of Urine Samples . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 157
Proteinuria after Minor Injury. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 158
Overflow Proteinuria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 158
Glomerular Proteinuria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 159
Tubular Proteinuria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 161
Factitious Proteinuria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 162
Monoclonal Free Light Chains (MFLCs), alias Bence Jones Protein . . . . . . . . . . . . . . . 162
Renal Damage Due to MFLC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163
Detection and Measurement of MFLC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 164Detection of MFLC in Urine and Serum by Electrophoresis and IFE. . . . . . . . . . . . . . . . . . . . . . . . 164Optimizing Detection of MFLC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 166False Positive MFLC in Urine by Electrophoresis and IFE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 169
Urine Protein Electrophoresis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 169
Urine Immunofixation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 170
False Negatives by Urine Protein Electrophoresis and IFE. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171
Nephelometry to Measure κ and λ Light Chains. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 171Diagnostic Interval for rFLC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 174

xii
CONTENTSPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
CHAPTER 8: Approach to Pattern Interpretation in Cerebrospinal Fluid. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 179Early Electrophoretic Studies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 179
CSF Protein Composition. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 179Source of CSF Proteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 179
Electrophoretic Pattern of Normal CSF . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 180
Damaged Blood-CSF Barrier. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 182
Multiple Sclerosis and O-Bands. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 183Identifying O-Bands in CSF . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184
Isoelectric Focusing with IB or IFE vs Agarose Gels. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184
Interpretation of CSF Electrophoresis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 184
IgM O-Bands . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 188
Light Chain O-Bands. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 188
Other Conditions with CSF O-Bands. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 189Central Nervous System Involvement with Systemic Lupus Erythematosus (CNS Lupus) . 189
Calculation of CSF IgG Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 190
Detection of CSF Leakage in Nasal and Aural Fluid Following Head Trauma. . . . . . . . . . . . . . . 190Detection of β2-Transferrin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 190
Detection of β-Trace Protein . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192

ISBN 978-089189-5916
xiii
CONTENTS
CHAPTER 9: Laboratory Strategies for Diagnosing Monoclonal Gammopathies . . . . . . . . . . 197Guidelines for Clinical and Laboratory Evaluation of Monoclonal Gammopathies 197
Guideline 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 197Guideline 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 198Guideline 3 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 199Guideline 4 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202Guideline 5 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202Guideline 6 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203Guideline 7 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203Guideline 8 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 204Guideline 9 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 204
Algorithm for Detecting M-proteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 204Assumption about the Ordered Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 205Initial Testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 205Evaluation of Suspicious Findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 206
Maintain an Active File of all Monoclonal Proteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 209
Screening and Follow-up of MFLC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 209
Final Words. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 209
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 210

xiv
CONTENTSPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
CHAPTER 10: Interpretive Case Studies . . . . . . . . . . . . . . . . . 212Denaturation of serum protein artifact . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 212Normal variations in the α2 and β region. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 213Dealing with tiny γ restrictions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 214Patient safety—identification error . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 215Antibiotic (cephtriaxone) artifact on capillary electrophoresis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 216Antibiotic (sulfamethoxazole) artifact on capillary electrophoresis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 216Heparin artifact on gel electrophoresis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 217Analbuminemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 218Bisalbuminemia (alloalbuminemia) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 218Acute phase reaction and correction of electropherogram (densitometric) distortion. . . . . . . . . . . . . 219α1-antitrypsin deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 219α1-antitrypsin heterozygote . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220Dehydration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220Nephrotic pattern . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221Plasmapheresis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222Isolated hypogammaglobulinemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222Chronic active inflammation with small γ restriction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223Acute phase reaction with prominent oligoclonal bands . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 224Subtle serum oligoclonal bands . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 224Fibrinogen artifact . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 225Common variable immunodeficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 225C3 variant . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 226Normal serum immunofixation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 226Tiny γ restriction in light chain myeloma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 227Immunofixation pattern interpretations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 228Type II cryoglobulin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 229IgM M-protein requiring reduction for measurement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 230IgD M-protein. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 231IgE myeloma with 20-year survival . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 232Susupicious serum light chain M-protein turns out to be an IgE myeloma . . . . . . . . . . . . . . . . . . . . . . . . 233Polyclonal increase in IgM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 234Pattern resembling Wiskott-Aldrich syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 235Massive polyclonal increase in γ globulins with artifact on immunosubtraction . . . . . . . . . . . . . . . . . . 236Polyclonal and oligoclonal increase in γ globulins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 237β1-β2 bridging: IgA M-protein . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 238Polyclonal increase in IgG4 subclass . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 239Serum free light chain and light chain myeloma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 240Radiocontrast (Omnipaque) artifact as a false positive band on capillary electrophoresis . . . . . . . . . 241IgM M-spike in typical location . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 242IgM M-protein requring immunofixation for detection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 242IgA M-spike presents as “fuzzy band”. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 243Lymphoplasmacytic lymphoma with urine M-spike in pregnancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 244Acute phase pattern complicated by radiocontrast dye (Optiray) on capillary electrophoresis . . . . . 245Urine gel patterns with case of κ monoclonal free light chains . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 245Urine gel pattern in kidney-pancreas transplant. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 246CSF isoelectric focusing patterns for multiple sclerosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 247CSF leakage into nasal fluid—β2 transferrin test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 248

xv
ISBN 978-089189-5916
Preface
This text presents the use of protein electrophoresis of serum, urine and cerebrospinal fluid in clinical diagnosis. It is a
revision of three previous books on this subject with substantive changes. During the past decade, there have been major advances in our knowledge of and ability to detect protein abnormalities by electrophoresis and immunoassay.
Some techniques formerly limited to specialized or research laboratories now are available for incorporation into routine clinical laboratory testing. Isoelectric focusing with immunologic characterization is the standard for detecting oligoclonal bands (O-bands) in the cerebrospinal fluid of patients with multiple sclerosis. Some years ago, agarose gel electrophoresis was performed on cerebrospinal fluid that needed to be concentrated 80-fold. While research studies indiciated superiority of isoelectric focusing, that technique was too cumbersome for most clinical laboratories. Now, 2 FDA-approved commercially available instruments provide excellent results. Moreover, a consensus conference discussed in this book provides guidance for the use of this technique in diagnosis and on the interpretation of the patterns seen in cerebrospinal fluid.
Though described barely a decade ago, the serum free light chain (FLC) test has had a major impact in the diagnosis, prognosis and clinical follow-up of therapy for multiple myeloma, nonsecretory myeloma, smoldering multiple myeloma, AL amyloidosis, and monoclonal gammopathy of undetermined significance (MGUS). The serum FLC test has joined time-honored methods of characterizing and measuring M-proteins as part of the assessment recommended by the International Myeloma Working Group.
Capillary electrophoresis has become routine in many larger centers. With more extensive use of capillary electrophoresis, advantages and problems such as unusual bands produced by radiocontrast dyes, antibiotics and gelatin-based plasma substitutes have been described. The advantages and limitations of capillary electrophoresis is discussed and illustrated extensively in the present volume. Gel-based methods have been improved to where now almost all available techniques provide crisp separation of the β1 (transferrin) and β2 (C3) fractions. This improves the ability of the interpreter to detect subtle restrictions in the β region where many M-proteins may be found.
In addition to the advances in the initial detection and quantification of specific proteins, the techniques available to identify the M-proteins have improved. Immunosubtraction is routinely performed in laboratories using capillary electrophoresis. It is automated technology and highly efficient allowing characterization of straightforward M-proteins. But immunosubtraction has a lower sensitivity and less flexibility than immunofixation. Immunofixation is available as a semi-automated procedure with less technologist time and more reliable instrumentation than previously. In addition to increased sensitivity compared with immunosubtraction, immunofixation has a flexibility that allows the operator to use antisera other than those provided in a kit. For instance, one may use anti-IgD or anti-IgE when working up a serum with an M-spike, but no reactivity with anti-IgG, anti-IgA or anti-IgM. Alternatively, anti-fibrinogen may used with immunofixation in explaining a β-γ region restriction. The uses of both techniques are discussed along with many case examples.
A new test is now available that uses an immunoassay to separately measure IgG κ from IgG λ, IgA κ from IgA λ and IgM κ from IgM λ. In a few reports it has been shown to have utility in detecting and measuring M-proteins that may be obscured in the β region. However, just like the serum FLC test, its true importance will only be known with larger independent studies.
Beyond technical issues, we continue to fine-tune our utilization and interpretation of protein studies when searching for the presence of an M-protein. Consensus conferences and large studies have been reported that offer cogent advice on the most effective use of the five main techniques currently available: serum protein electrophoresis, urine protein electrophoresis, serum immunofixation (immunosubtraction), urine immunofixation, and serum FLC test. This information, discussed in Chapters 6 and 9, will help the reader streamline testing methods while improving detection.
I hope you enjoy this book, or at least find it useful. If this book has been improved it is largely due to comments and questions that readers of my previous work have sent to me. Please feel free to contact me at [email protected] with your questions, comments and interesting cases.
David F Keren, MDProfessor of PathologyThe University of Michigan Ann Arbor, Michigan

12
CHAPTER 2
Techniques for Protein Electrophoresis and Measurement of M-proteins
PRO
TEIN
ELE
CTR
OPH
ORE
SIS I
N C
LIN
ICA
L DIA
GN
OSI
S
CHAPTER 2
Techniques for Protein Electrophoresis and
Measurement of M-proteins
Principles of Protein Electrophoresis
When proteins migrate in an electrical field, the extent of their migration and the degree of the resolution of each band depend on
the following: isoelectric point (pI) of the protein, pH of the buffer, ionic strength of the buffer, temperature of the gel and the voltage applied.
The pI of any protein is constant and dependent on its amino acid composition and carbohydrate content. The net charge that a protein expresses is determined by the pH of the solution in which it is dissolved. For instance, fibrinogen has a pI of 5.5. In a buffer with a pH of 8.6, fibrinogen donates protons to the buffer and is left with a net negative charge. Conversely, in a solution with a pH of 4.0, fibrinogen accepts a proton resulting in a net positive charge.
High resolution of protein bands is achieved by optimizing the velocity of migration while minimizing passive diffusion and avoiding interactions of proteins with the support medium. Detailed reviews of these factors are available in Wieme, and Briere and Mull [Wieme 1965, Briere 1964].
The speed with which a protein migrates in an electric field (electrophoretic mobility) under defined conditions of pH, ionic strength, temperature, and voltage is characteristic for that protein. The formula which defines the relationships among the variables that determine the electrophoretic mobility ( ) of a protein is:
=d/Etwhere d is the distance traveled from the origin in centimeters, E is the strength of the electrical field in V/cm, and t is the duration of electrophoresis in seconds. As the strength of an electrical field is inversely proportional to its length, a shorter support medium permits faster separation of proteins.
Increasing the voltage results in a faster separation of proteins. Unfortunately, it also results in a greater generation of heat that increases passive diffusion and is deleterious to resolution of individual
bands. The amount of heat (in joules) generated when the electric current passes through the apparatus can be calculated by:
Heat generated = xE2/Awhere x is the specific conductance of the apparatus, E is the strength of the electric field in V/cm, and A is the mechanical heat equivalent. From this, it follows that heat production increases exponentially as the voltage is increased.
Excessive heat production plays havoc with good resolution of electrophoretic bands. One of the major effects of heat is to increase the thermal agitation, and as a result, the diffusion of the protein molecules also increases. Diffusion broadens the width of a band, thereby decreasing the resolution. Heat production can also decrease the viscosity of agarose. Although the decreased viscosity of the gel permits a more rapid electrophoretic migration ( ) of the proteins through the gel, it is more than counterbalanced by an even greater increase in diffusion with a resulting decrease in resolution. Before closed systems (where evaporation is eliminated) were common, the heat generated further complicated resolution by causing enough evaporation to change the ionic strength.
The ionic strength of the buffer is another important factor in achieving optimum resolution. As the concentration of the salt ions in a buffer increase, the velocity of electrophoretic protein migration decreases. Change in ionic strength does not, however, alter the relative migration of serum proteins. The effect is largely the result of interaction of the buffer ions with the surface charges on the protein.
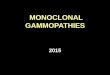
Consider a buffer in which one increases the concentration of NaCl. At the typical pH 8.6 of agar gel electrophoresis, human serum albumin has a negative surface charge. The positive sodium ions are attracted to the negative charges on albumin and diminish its effective net negative charge in the solution f2.1. Further, positively charged ions, in immediate proximity to the albumin, are attracted to the cathode during electrophoresis and tend to retard the progress

ISBN 978-089189-5916
13
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINS
of albumin toward the anode. This accumulation of positive charges in the buffer around the negatively charged albumin is known as the “diffuse double layer effect.” This is why it is important to control the concentration of ions in a buffer solution to provide consistent migration from one run to another [Wieme 1965]. If one notices a marked change in migration when a new lot of buffer is used, an incorrect ionic strength of the buffer would be one consideration in evaluating the problem.
Another factor limiting effective separation of protein bands is adsorption of molecules to the agar gel itself. Because of the negative charges possessed by the relatively purified agarose solutions used today, use of a buffer with a pH <5.0 is impractical. Below this pH, serum proteins have a net positive charge and can precipitate in the agar gel. This is why if a drop of acid fixative falls by accident onto the gel, proteins placed at this position will precipitate thus creating an artifact.
With close attention to buffer strength, voltage, heat dissipation, purity, and thickness of the agarose, currently available electrophoretic systems can display from 6 to as many as 12 protein bands. These encompass
>95% of the total mass of serum proteins [Laurell 1973]. A comparison of the resolutions generally available by commercially available instruments is shown in f2.2. Better resolution is an important part of detecting M-proteins.
To improve the detection of M-proteins, guidelines for the quality of resolution on protein electrophoresis have been created [Aguzzi 1986, Keren 1999a]. The Protein Commission of the Societa Italiana di Biochimica Clinica published guidelines for criteria for performance of sensitive electrophoresis procedures t2.1 [Ruggeri 2001].
For simplicity, I prefer to refer to systems that provide resolution sufficient to achieve a crisp separation of 1- (transferrin) from 2-globulin (C3) to improve detection of M-proteins [Keren 1999a, 1999b]. Detection of proteins present in concentrations smaller than 10 mg/dL require more sensitive immunoassay techniques.
Electrophoresis in AgaroseMost electrophoresis systems which achieve
high quality resolution are based on the method of Wieme as modified by Johansson [1972]. The latter used a 1% concentration of agarose in 0.075 M, pH 8.6 barbital buffer containing 2 mM calcium lactate. The calcium ions are especially helpful to improve resolution in the region. Commercially available agarose electrophoresis kits usually have a uniformly thin (about 1 mm) layer of agarose on an inert plastic support.
The specimen is applied to the agarose surface in a narrow band. Excessive moisture is removed from the surface of the gel by blotting (typically with filter paper). The blotting is needed to help the proteins diffuse into the gel and to prevent the formation of excessive lateral bands. Various mechanical devices such as a plastic template evenly apply or wick a few microliters of sample onto the gel. Consistency and attention to detail in sample application are extremely important to obtain good results. Occasional gel preparations have distortions due to their initial preparation, or to problems with storage f2.3.
f2.1 At the pH 8.6 of the typical SPE gel, albumin has a strong negative charge. The positive ions in the buffer, in this case sodium, are attracted to the negative charges on albumin and diminish its migration toward the anode.
f2.2 This composite figure illustrates the resolution of different samples
run on different commercial electrophoretic systems. Examining the β region bands (transferrin and C3) helps to evaluate the resolution avail-able with these techniques.
t2.1 Recommendations for Optimizing Detection of M-proteins
1. Transthyretin (prealbumin) should be seen in all healthy persons
2. 1-antitrypsin heterozygotes should be evident
3. Haptoglobin and 2-macroglobulin should be seen though not com-pletely separated from one another
4. Transferrin and C3 should be clearly resolved
5. M-proteins measuring 1 g/L (100 mg/dL) should be detectable in the
region

14
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINSPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
On the semiautomated, gel-based systems, application devices are used along with automated washing to streamline the technical process. The Sebia Hydragel
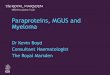
1- 2 15/30 and Helena Rep Unit methods provide serum and urine gel results with crisp separation of the 1- 2 region f2.4. Most electrophoretic systems would easily allow detection of the obvious M-proteins in samples 6, 8, 9, 11, 12, 20, 21, 25 and 26 in f2.4. The advantage of such crisp separation of 1 from the 2 region is in detecting more subtle bands such as the slightly darker, slightly more cathodal band in the 2 region of sample 19. Such suspicious bands deserve further study by immunofixation (IFE). In this case it was an IgAK M-protein.
Along with modern application techniques comes the possibility of misapplications. One contemporary tool is a device that facilitates application of serum or urine by having the operator place the liquid into a well. At the bottom of the well is a paper that allows the sampled to be “wicked” to the tip of the applicator f2.5. The sharp edge of the applicator places the sample on the gel for a uniform origin. However, the technologist needs to follow the manufacturer’s instructions to avoid problems from cells, crystals, or casts in urine and cryoprecipitating proteins in serum [Keren 2004]. These may clog the bottom of the well and interfere with the wicking effect of the
sample onto the gel f2.6. In these situations, the problem can be avoided by centrifugation of the urine and use of the supernatant as required by the instructions. With serum, IgM M-proteins may self-aggregate and interfere with wicking of the serum to the end of the applicator.
f2.4 Crisp resolution of the transferrin (β1) and C3 (β2) bands is evident in all but samples 29 and 30. The latter 2 were lyophilized normal and high controls where the relatively unstable C3 had been cleaved into smaller fragments. The resolution of this method allows detection of subtle suspicious bands such as the slightly darker, more cathodal β2 band in sample 19 (indicated) that was found to be an IgAK M-protein by IFE (Sebia β1-β2 gel).
f2.5 Applicator for serum and urine protein electrophoresis on Sebia β1-β2 gels
f2.6 2 gels used to evaluate the protein content of several urines are shown. The lack of detectable protein in the second urine from the top on the left was not consistent with the total protein detected in that patient. The next day it was rerun with other samples after removing cellular material by centrifugation. On the second run, several protein bands are obvious in the same urine (indicated), some of which were suspicious for the presence of monoclonal free light chain (Sebia β1-β2 gel).
f2.3 The bowing distortion of all the samples with a broadened albumin band at the bottom while the middle albumin bands are smaller indicates a problem with the initial gel preparation (Panagel SPE2).

ISBN 978-089189-5916
15
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINS
For self-aggregating IgM M-proteins treatment with a reducing agent (2-mercaptoethanol, penicillamine or dithiothreitol) can prevent some electrophoretic problems on both gel and CE techniques [Keren 2001, Zetterberg 2004]. Because of these issues, I recommend comparing the total protein of the serum or urine to the electrophoretic pattern to be sure that the sample is adequately applied. If the total serum or urine protein does not agree with what one sees on the gel, consider a sample application problem.
Modern gel-based systems typically use conditions that complete the electrophoretic run in 20-30 minutes. When electrophoresis has been completed, the proteins are fixed with an acid fixative. After fixing the proteins, the gel is dried and stained with any of a variety of protein dyes: Amido black, Ponceau S, Coomassie blue, and several proprietary mixtures.
Electrophoresis on Cellulosic MediaCellulose acetate has been available as a supporting
medium for protein electrophoresis since the late 1950s [Cawley 1962, 1965a, 1965b, Kohn 1957]. Due to the relatively poor resolution in most commercially available cellulose acetate systems used in the United States, <1% of laboratories reporting results on the 2011 CAP electrophoresis surveys used this technique [CAP 2011]. However, the rapid electrophoresis time and clarity of its background made cellulose acetate a considerable improvement over filter paper. Cellulose acetate has the advantage of uniform porosity. The membrane is obtained by dissolving in a volatile organic solvent the product of mixing carbonic anyhydride with cellulose. The resulting membranes provide consistent 5-band resolution.
The resolution possible from cellulose can be improved. By using gelification to prevent the membranes from drying, the creation of gelled cellulose acetate
improved the resolution of protein bands [Destro-Bisol 1995]. Preparations of gelled cellulose acetate, Cellogel (Cellogel Electrophoresis Co, Milan, Italy), were shown to separate serum proteins into the same fractions seen with the higher resolution agarose methods [Aguzzi 1981, Janik 1985, Ojala 1980,
Merlini 1981]. Unlike agarose electrophoresis, cooling is not required to provide optimal resolution. Furthermore, IFE analysis may also be performed on Cellogel. Under certain circumstances, Cellogel strips have been reused [Destro-Bisol 1993]. Bienvenu et al reported good correlation between CE and Cellogel for 2, , and regions, though higher results are found by CE in the 1 region, likely due to better detection of 1 acid glycoprotein by CE (see below) [Bienvenu 1998].
Capillary Electrophoresis (CE)Available capillary electrophoresis (CE) systems
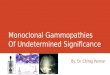
provide automated, high-quality electrophoretic separation of proteins with excellent resolution of transferrin and C3 f2.7. In addition to providing an electropherogram (similar in appearance to gel-based densitometric tracings), CE systems can convert the electropherograms into virtual gel images f2.7, f2.8 [Jolliff 1997, Keren 1998]. The assay is performed at 35oC, which may prevent the precipitation of cryoglobulins.
With CE systems, the electropherogram displays the basic information while the virtual gel image is generated from that data. This is the opposite of gel-based electrophoresis where the stained gel is the basic information and the densitometric scan is a line drawing generated from the gel. Both systems provide high-quality electrophoresis with minimal investment of technologist time. In the serum protein electrophoresis (SPE) mode, currently available instruments can have a throughput as high as 80 samples per hour. Automated immunosubtraction (ISUB) (see Chapter 3) is alternatively termed “immunotyping” by the Sebia and “immunodetection” by the Helena instruments due to patent issues.
f2.7 Electropherogram from the monitor on the Sebia Capillarys. The electropherogram displays serum proteins in a manner similar to densitometric scans of gels. Above, below, and to the right of the electropherogram are boxes that when clicked allow the operator to adjust the image for optimal viewing. In addition, to the right of the electropherogram, a virtual gel image of the proteins is presented.
f2.8 Virtual gel images have been combined to allow comparison of the results from 8 capillaries on 1 run. 1 M-spike is apparent in sample 2 while at least 2 and possibly a 3rd (overlying the C3 band) are present in sample 6. The prealbumin (transthyretin) bands are faint, but detectable. And in sample number 3, a band slightly anodal to the transthyretin band is due to the presence of the antibiotic ceftriaxone. Such nonprotein molecules in serum are detected with CE due to their absorbance at the wavelength used in this technique.

16
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINSPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
To perform electrophoresis, serum is placed into a barcoded test tube. Software controls both the physical operation of the instrument as well as the display and output of results [Bienvenu 1998]. The apparatus uses pressure injection to sample neat serum from the sector. By use of a buffer that has a lower ionic strength to carry the sample than the ionic strength of the running buffer, a stacking effect (like airplanes queuing up) is produced [Klein 1993]. The individual samples travel into 1 of several (the number of capillaries varies from instrument type and manufacturer) approximately 20-cm-long uncoated fused silica capillaries (inner diameter 25 microns). At the alkaline pH of the buffer systems used (approximately pH
10.0), an endosmotic flow is created by high voltage and the narrow bore of the strongly negatively charged silica capillary. This propels the proteins toward the cathode where an ultraviolet light (approximately 215 nm) is used to detect the peptide bonds [Keren 1998].
Separation of the proteins results from the individual pI, tertiary structure, and charge of the proteins under the conditions of the electrophoresis (Chapter 1). The software delimits the 5 (or 6 if one chooses to measure separately
1 and 2 regions) major protein fractions, however, the operator can readjust these as needed. The operator also can define limits of M-proteins for measurement f2.9. The software also permits one to zoom in on specific areas of interest in the electropherogram. This has been especially useful in examining small distortions such as an
1-antitrypsin variant f2.10 [Bossuyt 2003a]. The current version of the Sebia Capillarys II system includes the lipoproteins with the albumin fraction [Lichtinghagen 2010].
Bossuyt et al compared the reference intervals for the major serum protein fractions by cellulose acetate, agarose, and CE [Bossuyt 1998a]. They found significant differences in the ranges for all fractions other than the -globulins t2.2. Similar to the Bienvenu et al report, Bossuyt et al found that the 1-globulin fraction for CE had lower and upper ranges that were twice those based on either agarose or cellulose gels, whereas the 2- and -globulin fractions for CE were just slightly lower than those from the gel-based systems. Similar results were reported when Katzmann et al compared CE with agarose gel electrophoresis [Katzmann 1998]. In the latter study, there was a 46% increase in the 1-globulin fraction in CE compared to agarose with a 36% decrease in
2 and a 10% decrease in the -globulin fractions with CE.The higher concentrations of 1-globulin reflect
the fact that CE is better able to detect both 1-lipoprotein and 1-acid glycoprotein (orosomucoid). The high sialic
f2.9 Measurement of a γ-migrating M-spike on a Sebia Capillarys II electropherogram is illustrated. The area measured under the peak is determined by the operator.
f2.10 a The red box outlines a suspicious area in the α region of this electropherogram (Sebia Capillarys II). b The designated area was expanded to allow a better visualization of the α region. The 2 small equal peaks in the α1 region are most consistent with a carrier of an α1-antitrypsin variant (see Chapter 4). With such cases, we recommend phenotype studies to confirm this impression and genetic counseling due to implications for the family (Sebia Capillarys II).
a b

ISBN 978-089189-5916
17
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINS
acid content of 1-acid glycoprotein and the lipid content of 1 lipoprotein interfere with the binding of protein dyes, whereas CE detects the proteins via peptide bond absorbance which is not influenced by these factors [Bossyut 1998b, Dati 1996].
In contrast to the Bossuyt et al study, however, Katzmann et al noted that -globulin by CE was 21% lower than seen in their agarose gel-based assays [Katzmann 1998]. This difference may relate to the use of different protein stains by the agarose commercial procedures, since the CE instrument used was the same in both studies. Despite minor differences in the fractions from CE to gel-based techniques, Petrini et al found good agreement between interpretation of results when they compared CE to a high-resolution cellulose electrophoresis [Petrini 1999].
CE and M-proteinsThe crisp resolution of CE has proven to be an excellent
technique to detect M-proteins [Arranz-Peña 2000, Clark 1998, Jenkins 1995, 1997,
1999, Litwin 1999, Mussap 2006a, 2006b, Roudiere 2006]. In studies by Katzmann et al and Bossuyt et al, the sensitivity of CE to detect M-proteins was 93% and 95% respectively [Katzmann 1998, Bossyut 1998a]. In contrast, the same studies detected M-proteins in only 86% and 91% of their samples by the agarose techniques they used. It should be noted, however, that the gel-based techniques
used were of relatively low resolution 5 band patterns that did not separate region transferrin and C3.
A more recent study comparing CE to gel techniques found some inconsistency among several observers when evaluating M-proteins by the CE technique. However, it was not clear whether this was due to inexperience of some of the observers with the newer CE technique since there was a great variability of M-protein detection between observers [McCudden 2008].
In addition, CE has been reported to have limitations in the detection of small or unusual M-proteins [Bossyut 2001a,
Henskens 1998, Jenkins 1996, Keren 2001, Zetterberg 2004]. CE failed to detect IgA, IgD, and IgM M-proteins that were present in concentrations <3.2 g/L (0.32 g/dL) in the study by Bossuyt et al [2001a]. In early work, Jenkins and Guerin found that 6 M-proteins with high pI values (between 6.9 and 8.3 for IgM and >8.5 for IgG M-proteins) and extreme cathodal migration could not be detected [Jenkins 1996]. By increasing the ionic strength of the boric acid buffer they used from 50 mmol pH 9.7 to 75 mmol pH 10.3, they were able to detect all of these problem M-proteins. Henskens reported a similar occurrence with an IgM M-protein [Henskens 1998]. In 2 similar cases, a reducing agent (2-mercaptoethanol or penicillamine) pretreatment was needed before the concentration of an IgM M-protein could be accurately determined by CE f2.11 [Keren 2001, Zetterberg 2004].
t2.2 Serum Protein Reference Intervals in Men*
Region Cellulose Agarose CEAlbumin 4.20-5.31† 4.19-5.36 4.17-5.23
1 0.12-0.25 0.13-0.27 0.26-0.45
2 0.38-0.67 0.38-0.70 0.34-0.64
0.61-1.00 0.65-1.14 0.58-0.95
0.53-1.30 0.49-1.21 0.53-1.32*Data modified from [Bossuyt 1998]†Range in mg/dL for all 3 instruments expressed as 95% confidence intervals
Serum Protein Reference Intervals in Women*
Fraction Cellulose Agarose CEAlbumin 3.94-4.96 4.01-5.11 3.74-4.98
1 0.14-0.26 0.14-0.28 0.26-0.51
2 0.44-0.69 0.41-0.69 0.39-0.64
1 0.55-0.95 0.65-1.00 0.55-0.87
0.53-1.30 0.49-1.21 0.53-1.32*Data modified from [Bossuyt 1998]†Range in mg/dL for all 3 instruments expressed as 95% confidence intervals
f2.11 a This electropherogram demonstrates a small fast γ region spike (indicated in black). The amount of the spike was inconsistent with the initial nephelometric measurement of IgM as being >2,500 mg/dL. (Sebia Capillarys) b Immunofixation of this sample demonstrates a large IgMK M-protein. (Sebia IFE) c Electropherogram of the same sample after treatment with 2-mercaptoethanol. The M-spike is now consistent with the IgM measurement and the immunofixation results. (Sebia Capillarys)
a b c

18
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINSPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
As with gel electrophoresis, the most difficult M-proteins to detect are those that are of relatively low concentration and those that migrate in the region. Transferrin and C3 may obscure these small M-proteins.
Bienvenu et al reported that the detection limit for an M-protein by CE was <0.5 g/L (50 mg/dL) [Bienvenu 1998]. A similar sensitivity for the detection limit of M-proteins with CE has been reported by Smalley et al [2000]. These limitations reflect the fact that although a M-protein may be present, the actual restriction, the M-spike, may be too small to be reproducibly detected.
Although Katzmann et al found good comparison of M-spikes on CE vs cellulose acetate [Henskens 1998], there was not a linear correlation between M-proteins measured by agarose gel-based methods compared to CE. Bergon et al observed an overestimation of the M-proteins that inversely correlated to concentrations below 15 g/L (1,500 mg/dL) [Bergon 2005]. Mussap et al found a concentration-related bias with densitometry on agarose gels giving higher values with M-proteins <20 g/L (2,000 mg/dL) and CE giving higher values with M-proteins greater than 20 g/L (2,000 mg/dL) [Bergon 2008]. Because of such differences, I recommend not switching from one method to another in following individual patient values.
Interferences with Detection of M-proteinsAs with gel electrophoresis, plasma specimens and
sera that are hemolyzed or lipemic interfere with the analysis for the presence of an M-protein. But, unique to CE technique, small molecules that absorb ultraviolet light
around 200 nm create confusing peaks. Radiocontrast dyes and antibiotics have been the most bothersome with peaks that cannot be visually distinguished from a true M-spike. They may appear in several locations from the transthyretin (prealbumin) to the -globulin region [Arranz-Peña 2000, Bossyut 1999, Brouwers 2007]. Because of this, any restriction suggestive of an M-protein that has not previously been characterized, must be proven to be an M-protein by IFE or ISUB before reporting it as such.
Blessum et al successfully removed an artifactual 2 region peak caused by sodium meglumin ioxitalamate
(Telebrix) by desalting the sample f2.12 [Blessum 1999]. They used D-Salt Dextran plastic desalting columns, 5 kDa cutoff from Pierce. However, Arranz-Peña et al reported obstruction in some of their capillaries after trying that procedure [Arranz-Peña 2000]. The latter group removed the interference by adding 0.2 g of activated charcoal to 1 mL of serum, vortexing for 20 seconds, and centrifuging at 200 g for 5-10 minutes at room temperature. In t2.3 is a list of radiocontrast dyes and antibiotics complete with the region where the false positives are known to occur [Arranz-Peña 2000, Bossuyt 2002, 2003a, Brouwers 2007].
As shown in f2.13a, the electropherogram cannot distinguish between this artifact and a true M-spike. The complete IFE shown in f2.13b can rule out an M-protein. An alternative method that may be a bit more efficient to distinguish small discrete nonprotein bands from M-proteins is to perform an IFE with a pentameric antibody reagent (anti-G, A, M, K, and L in the same antiserum) on suspicious cases (see Chapter 3). With either technique, IFE will be negative for contrast dyes and other nonimmunoglobulin protein bands.
In addition to radiocontrast dyes, other molecules that absorb around 200 nm can create unusual patterns on CE. Bossuyt et al reported that
f2.12 Electropherograms of serum before (a) and after (b) desalting. Figure from Blessum et al [1999]. The suspicious area in the slow α2 region (Omnipaque) is removed by the desalting. Used with permission from Clinical Chemistry (Paragon CZE 2000).
t2.3 Location of Radioopaque Media and Antibiotics on Capillary Electrophoresis
Location Compound Anodal to prealbumin Ceftriaxone sodium
Prealbumin Bilisegrol (meglumine iotroxate)
Albumin (anodal edge) Sulfamethoxazole
2 (anodal) Gastrografin and urograffin (sodium-meglumine amidotrizoate)Uroangiografin (meglumine amido-trizoate)
2 (middle) Telebrix (ioxitaalamic acid)Xenetix (iobitridol)
2 (cathodal) Iopamiro (iopamidol) Omnitrast and Omnipaque (iohexol) Ultravist (iopromide)
1 (anodal) Piperacillin-taxobactam (tazocin)
2 (anodal) Hexabrix (sodium-meglumine ioxaglate)
2 (middle) Optiray (ioversol) Iomeron (iomeprol)
[Arranz-Peña 2000, Bossuyt 2002, 2003, Brouwers 2007]
a
b

ISBN 978-089189-5916
19
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINS
the antibiotic piperacillin-tazobactam (Tazocin Wyeth Lederle) produced a small peak in the -globulin region. Sulfamethoxazole produces a small peak at the anodal edge of albumin [Bossyut 2002, 2003b]. Brouwers also reported an even more anodal peak with ceftriaxone [Brouwers 2007] f2.14.
A more problematic interference, however, has been reported by Gijbels et al [2004].They found that gelatin-based plasma substitutes produced a polyclonal-like increase in the and regions mainly in CE techniques, and to a lesser extent in gel-based procedures. This type of - bridging and polyclonal increase in -globulins produces patterns that one cannot distinguish from chronic inflammation and liver disease f2.15. Since SPE is never a stat procedure, for laboratories using CE as their main screening technique a good rule of thumb would be to wait 24 hours after infusion of gelatin-based plasma substitutes and to delay
ordering a SPE for several days after a patient has received a radiocontrast dye [Arranz-Peña 2000, Gijbels 2004].
Interference by Chimeric and Humanized Monoclonal Antibody Therapies
In the past decade, the use of chimeric and humanized monoclonal antibodies have become commonplace. These drugs contain a variable region from a mouse monoclonal antibody and the Fc portion derived from human IgG. Many such reagents are routinely used to treat autoimmune
f2.14 Ceftriaxone produces a small artifactual band (arrows in A, D, E, and F) anodal to the transthyretin band when studied by CE [Brouwers 2007]. Used with permission from Clin Chim Acta.
f2.15 Normal serum mixed with phosphate-buffered saline (A and B) or Geloplasma (I and J), or Gelofusine (K and L). Note the β-γ bridging and increase in γ-globulins in samples with the gelatin-based plasma substitutes. Figure modified from Gijbels et al to show the most prominent changes. The reader is encouraged to see the original more detailed figure [Gijbels 2004]. (Paragon CZE200 for samples on the left-A, I, and K, Sebia Capillarys for samples on the right-B, J, and L). Used with permission from Clinical Chemistry.
f2.13 a Electropherogram from patient who had received a radiocontrast dye (Omnipaque). The arrow indicates the position of the suspicious peak at the cathodal end of the α2 region. The size of the dye peak depends on the dose and the time since it was given (Sebia Capillarys II). b IFE on serum from patient who had received the radiocontrast dye Omnipaque. No restriction is seen either in the SPE lane or any anti-immunoglobulin lane since the radiocontrast dye will not precipitate with acid nor stain with a protein dye. (Beckman SPE2 IFE gel).
a
b

20
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINSPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
diseases and malignancies including multiple myeloma. In therapeutic doses, these reagents can reach levels as high as 60 mg/dL. Such levels will produce small restrictions in the region on protein electrophoresis as well as confirmatory positive results by IFE [McCudden 2010].
McCudden et al reported finding a subtle restriction on serum protein electrophoresis of a patient treated with siltuximab (Centocor) [McCudden 2010]. As shown in f2.16 they found a discrete tenting in the mid-gamma region of the CE electropherogram performed on a patient who had had a previously identified IgD κ M-protein. Further studies on that and other patients receiving siltuximab indicated that routine IFE detects a small IgG κ M-spike in many patients receiving siltuximab.
In addition to these findings, McCudden et al tested other patients at the time of the mean peak serum drug levels for rituximab (Rituxan), trastuzumab (Herceptin), bevacizumab (Avastin), inf liximab (Remicade), cetuximab (Erbitu), and adalimumab (Humira). IFE on all of these samples produced a detectable IgG κ spike in the region. They noted that rituximab and trastuzumab were located in the cathodal end of the region while the rest were mid-gamma. They found that IFE on 11 of 13 patients with multiple myeloma who were being treated with siltuximab had an IgG κ M-spike consistent with this drug. Preincubation of siltuximab with anti-siltuximab was able to shift its migration to allow one to distinguish between the drug and an endogenous M-protein. In terms of duration, McCudden et al noted that siltuximab was no longer detected after about 3 months following discontinuation of the therapy [McCudden 2010].
Pediatric Reference RangesReference ranges for the 5 major protein fractions
in a pediatric population were established by Bossuyt et al t2.4 [Bossyut 2001b] . They divided the population studied into 4 groups by ages: 1-2 years, 3-4 years, 5-9 years, and 10-14 years. No differences were found between boys and girls for any of these age groups in any of the protein fractions. The 2-globulin fraction values were lower in the older children (5-14 years) than the younger children (1-4 years) due to higher values of 2-macroglobulin in the latter group [Bossyut 2001b]. Not surprisingly, the -globulin fraction was higher in the older groups than the younger ones due to the increased amount of IgG in older children. Even in the 3-4 year group, the -globulin fraction was higher than in the 1-2 year group.
Measurement of Protein Fractions Densitometry
When electrophoresis is performed on gel-based systems, the fractions can be examined by direct visualization. This allows comparison of one sample to
t2.4 Pediatric Reference Ranges for Capillary Electrophoresis (Paragon CZE 2000)
Age (yrs) N Albumin* α1 α2 β γ1-2 33 63.5
(54.7-70.4)6.3 (4.2-8.5)
10.8 (7-15.6)
9.4 (7.5-11.6)
10.1 (4.7-16.0)
3-4 44 61.5 (53.9-70.4)
6.4 (4.8-8.1)
10.4 (7.6-15.2)
9.5 (7.4-11.6)
11.6 (7.1-17.8)
5-9 70 62.2 (52.6-66.3)
6.2 (4.2-7.6)
9.9 (7.4-13.5)
9.4 (7.9-11.3)
12.2 (8.5-18.7)
10-14 48 61.2 (54.1-69.1)
5.9 (4.4-8.0)
8.9 (6.8-11.4)
9.7 (8.5-12.9)
13.7 (8.8-17.6)
*Results expressed as fraction percentages as median, 95% confidence limits in parenthesis [Bossuyt 2001b]
f2.16 Top image shows an overlay of a reference serum (black) on the pattern of a serum from a patient receiving siltuximab (red). The arrow indicates the discrete restriction caused by the drug. Middle left is the IFE pattern of siltuximab spiked into saline showing a small mid-gamma re-striction that is identified as IgG and κ. Middle right and bottom samples are from patients with other M-proteins who also have a small siltuximab restriction (red arrows). Used with permission from Clinical Chemistry.

ISBN 978-089189-5916
21
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINS
another and comparison to controls run on the same gel. Although direct examination can detect subtleties in migration such as 1-antitrypsin heterozygotes or oligoclonal bands (Chapter 4), differences in the density of staining of each protein fraction are objectively recorded by the densitometer [Aguzzi 1986, Kremers 1967, Mosser 1968]. Such objective information about differences in protein fractions helps to draw the attention of the interpreter to subtle quantitative abnormalities that otherwise might have been missed. Unfortunately, the sensitivity of densitometry is hindered by its dependence on the ability of the protein dye to stain a given protein. The precision of densitometry has been less than optimal in all fractions t2.5 [Kahn 1986]. Because of this, some consider densitometry of protein electrophoresis fractions to be a semiquantitative procedure [Kahn 1986].
To obtain reproducible measurements from densitometry of electrophoretic gels requires rigid standardization of the conditions of the assay. The values obtained will differ depending on the dilution of the sample, the densitometer settings, and the electrophoretic system used for analysis. The upper and lower limits of linearity should be established for each electrophoretic system use [Keren 1986]. The type of dye used affects the concentration recorded for albumin [Mendler 1999]. When using densitometry, our laboratory found linearity superior with Amido black than with Coomassie blue or crystal violet, although the latter 2 are more sensitive than Amido black. Sun noted that Amido black is also superior to Ponceau S for estimating the major protein fractions [Sun 1992]. Silver stain, though very sensitive, does not provide the linearity of more conventional stains. In addition to albumin, Amido black provides a reasonable estimate of serum transferrin and -globulin [Uriel 1958]. Yet, depending on the type of immunoglobulin being measured, variability has been noted. When measuring -migrating M-proteins, we found excellent agreement between the densitometric scans and nephelometric measurements of IgG f2.17 [Keren 1986].
5 or 6 FractionsOur laboratory performs densitometric scanning
on 1- 2 agarose gel-based serum patterns. Even though gels with crisp resolution of the 1 and 2 regions allow for a 6-band pattern, we use a standard 5-fraction pattern for serum. Partly, this reflects the familiarity of clinicians with these patterns but also the instability of the main
2-globulin protein C3. Using a 5-band measurement helps deal with the variability in the conditions of the specimen; it may not have been assayed for a few days due to transportation, weekends, or holidays.
Densitometry vs Nephelometry to Measure M-proteins in Serum
The M-protein is a convenient marker for the tumor burden. Most laboratories and recent guidelines have used a densitometric scan of the M-spike in the serum or urine to monitor patients with M-proteins [Dispenzieri 2008, Durie 2003,
Katzmann 1997, Sinclair 1990, Smith 2006, Stemerman 1989, Tichy 1985, Zak 1978]. The ability to perform ISUB on CE (Chapter 3) allows one to more precisely estimate an M-spike even in the 2 region of the CE electropherogram f2.18. Nonetheless, concerns about problems with M-protein measurement by densitometry (or electropherograms for CE) have been reported [Bergon 2005,
Chang 1997, Keren 2001, Mussap 2006b, Schreiber 1992, Shin 2008]. Some of the problems in using densitometry
involve the combined complexity of the several methods involved in obtaining a gravimetric amount. For instance, one needs to perform a total protein measurement. Several methods for such protein measurements will provide differing results. Electrophoresis provides an M-spike. However, the standard dilution used may not be optimal for measuring a large one. Staining the gel with a protein dye may not give linear results (due to saturation) in the range of the M-protein. Further, the densitometric scan has its own issues with linearity [Artiss 1986, Murray 2009,
Snozek 2007, Zak 1978]. Consequently, the dilution of the sample is particularly important when estimating the concentration of an M-spike by densitometry. When the M-protein is present in high concentration, the staining by the dye is saturated and the result moves off linearity for the proteins in the highest concentration [Bergon 2005, Chang 1997, Keren 1986, Mussap 2006b].
t2.5 Precision of Densitometric Quantification*
Fraction Mean CV% CV% RangeAlbumin 2.9 1.3-5.1
α1 9.5 4.4-20.2
α2 5.1 1.8-9.2
β 5.3 1.6-14.0
γ 6.7 2.5-27.2
*Data from using 10 measurements of the relative concentration in 30 samples [Kahn 1986]
f2.17 Correlation of γ region concentration, as determined by densito-metric scans of SPE gels, with total IgG as determined by nephelometry on sera with known γ-migrating IgG M-proteins. With β-migrating monoclonal proteins, however, transferrin, β1-lipoprotein and C3 may interfere with this measurement.

22
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINSPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
Using a laser densitometer on high-resolution agarose gel electrophoresis, Stemerman and Papdeao found a loss of linearity above 60 g/L requiring dilution to measure larger M-proteins. They presented a handy table to aid the interpreter in determining if a change in the quantity of an M-protein is significant t2.6.
In addition to the analytical variability, there is individual biologic variability in measurement of M-spikes in serum and urine that limit one’s ability to reproducibly claim a significant decline of an M-spike in response to therapy [Katzmann 2011]. Because of such variability, the international guidelines for monitoring patients with MM require a measurable M-spike to be ≥ 1 g/dL in serum and ≥ 200 mg/24 h in urine [Durie 2006, Smith 2006]. They recommend a decline of at least 25% in the serum M-spike and at least 50% in the urine M-spike to document a minimal response to therapy. These guidelines are confirmed by Katzmann et al in a study of the biologic and analytic variability of measurement of M-spikes in serum and urine [Katzmann 2011] (see Chapter 9).
Because of the problems measuring M-proteins by densitometry, immunoassays have been used to quantify the specific immunoglobulin isotype [Nutman 2001]. Immunoassays, however, cannot quantify the M-protein alone. They measure all of the heavy or light chain isotype class to which they are directed. Thus, if there is normal amount of polyclonal IgG in a patient who also has a small IgG M-spike, the immunoassay of total IgG will considerably overestimate the M-protein f2.19 In addition to dealing with the polyclonal issue, when there are large amounts of M-protein in the sample nephelometric techniques may provide misleading information due to antigen excess effects as well as the characteristics of antisera used in the measurement [Bush 1992, Hawkins 2008, Sinclair 1990].
Some workers have found acceptable agreement between the densitometric scans and nephelometric measurements of IgG using serum from patients who
t2.6 Minimal Differences in Paraprotein Measurement That Indicate True Changes between Sera*
Initial Paraprotein Concentration (g/L)
85% Probability of a True Difference (g/L)
95% Probability of a True Difference (g/L)
0 1.1 1.8
10 1.6 2.5
20 2.0 3.3
30 2.4 4.0
40 2.9 4.7
50 3.3 5.4
60 3.7 6.1
70 7.2 6.8
80 4.6 7.5*Data modified from [Stemerman 1989]
f2.18 a This electropherogram demonstrates a slow α2 region M-spike (Sebia Capillarys). b The ISUB shows that the spike is subtracted by antisera against IgG and κ. This also outlines the extent of the M-spike. c Measurement of the M-spike approximated from the ISUB information.
a
b
c

ISBN 978-089189-5916
23
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINS
had region migrating IgG M-proteins [Keren 1986, Vuorinen 1989]. However, in studies of all 3 major immunoglobulin classes, the correlation between polyclonal immunoglobulin concentrations determined by nephelometry vs densitometry is variable [Chang 1997, Murray 2009, Schreiber 1992]. Schreiber et al compared the concentration of -globulins to the sum of nephelometric measurements of IgG, IgM, and 1/2 of IgA (they assumed that about 1/2 of the IgA migrated in the region of their system) [Schreiber 1992]. Although the correlation between the 2 techniques was good (average correlation coefficient of 0.95, the densitometric technique had a consistently low bias compared to nephelometry. This discrepancy became more pronounced at higher immunoglobulin concentrations. Similar results were reported by Chang et al who recommended diluting sera according to the protein concentration to improve the linearity [Chang 1997]. Sera with total protein from 9.1-11.4 g/dL required a 1:10 dilution, while sera with >11.5 g/dL of total protein were diluted 1:20. A unique solution was offered by Bergon et al [2008]. They subtracted the estimated polyclonal portion of the isotype of the M-protein from the total isotype amount obtained by nephelometry. They estimated the polyclonal fraction by using the uninvolved polyclonal isotypes and their light chains.
More recently, Murray et al performed an in-depth review of data from 2,845 patients with a -migrating M-protein as well as nephelometric measurement of the involved immunoglobulin [Murray 2009]. They found that the correlation differed for each of the 3 major isotypes. IgG M-proteins <19.2 g/L had a linear region with a slope of 0.83, but higher concentrations had a second linear region with a slope of 1.47. IgM had a systematic bias of higher
values by nephelometry, while IgA had reasonably good correlation with densitometry f2.20.
The overall recommendation from these studies is for clinicians not to alternate between nephelometry and densitometric or electropherogram measurements. Further, when data from one method does not correlate with other data, the laboratorian needs to aggressively pursue the clinical history to offer appropriate guidance to the clinician. For instance, in the case of a patient with a low IgM level by electropherogram measurement but with a high serum viscosity, further evaluation of the sample after treatment with a reducing agent such as 2-mercaptoethanol or penicillamine can be helpful f2.11 [Keren 2001].
Heavy-Light Chain AssayA unique approach to the problem of measuring
M-proteins has been offered in the form of the Hevylite assay (The Binding Site Inc, San Diego). This nephelometric immunoassay can measure separately IgG from IgG , IgA from IgA and IgM from IgM [Bradwell 2009]. This assay does not separate the IgG M-protein molecules from the IgG polyclonal molecules. Nonetheless, it may be useful in following cases where the M-protein is relatively subtle and present in the or regions f2.21 [Keren 2009].
Studies on Waldenström macroglobulinemia indicate that the measurement of IgMK and IgML separately might provide better quantitative information about the M-protein spike than that from densitometric or electrophoretogram studies [Leleu 2011]. Further a recent case report by Donato et al demonstrated the utility of the IgAK/IgAL ratio in following a patient with an IgAK M-protein [Donato 2011]. Broader use of this technique may follow from larger independent studies.
f2.19 A small IgG M-spike is seen atop the normal amount of polyclonal immunoglobulins in the γ region. Total IgG measurement in this case will reflect more of the normal IgG more than the IgG M-protein.
f2.20 Comparison of the measurement of a 294 IgA M-proteins, b 2,095 IgG M-proteins, and c 456 IgM M-proteins by electrophoresis (SPEP) and nephelometry (NEPH). Each curve demonstrates the line of equality (dashed line) and of best fit (solid line) [Murray 2009]. Used with permission from Clinical Chemistry.

24
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINSPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
ReferencesAguzzi F, et al [1981] Electrophoresis: cellulose acetate vs agarose gel,
visual inspection vs densitometry. Clin Chem 27(11):1944-5.Aguzzi F, et al [1986] Densitometry of serum protein electrophoreto-
grams. Clin Chem 32:2004-2005.Arranz-Peña ML, et al [2000] Interference of iodinated contrast media in
serum capillary zone electrophoresis. Clin Chem 46(5):736-7.Artiss JD, et al [1986] Potential problems in serum protein electrophoresis.
Clin Lab Med 6(3):427-40.Bergon E, Miranda I, Miravalles E [2005] Linearity and detection limit in
the measurement of serum M-protein with the capillary zone electro-phoresis system Capillarys. Clin Chem Lab Med 43(7):721-3.
Bergon E, Miravalles E [2008] Estimation of serum M-protein concen-tration from polyclonal immunoglobulins: an alternative to serum protein electrophoresis and standard immunochemical procedures. Clin Chem Lab Med 46(8):1156-62.
Bienvenu J, et al [1998] Multicenter evaluation of the Paragon CZE 2000 capillary zone electrophoresis system for serum protein electropho-resis and monoclonal component typing. Clin Chem 44(3):599-605.
Blessum CR, Khatter N, Alter SC [1999] Technique to remove interfer-ence caused by radio-opaque agents in clinical capillary zone electro-phoresis. Clin Chem 45(8 Pt 1):1313.
Bossuyt X, et al [1998a] Detection and classification of paraproteins by capillary immunofixation/subtraction. Clin Chem 44(4):760-4.
Bossuyt X, et al [1998b] Serum protein electrophoresis by CZE 2000 clinical capillary electrophoresis system. Clin Chem 44(4):749-59.
Bossuyt X, Mewis A, Blanckaert N [1999] Interference of radio-opaque agents in clinical capillary zone electrophoresis. Clin Chem 45(1):129-31.
Bossuyt X, Marien G [2001a] False-negative results in detection of mono-clonal proteins by capillary zone electrophoresis: a prospective study. Clin Chem 47(8):1477-9.
Bossuyt X, et al [2001b] Reference values for the five electrophoretic serum protein fractions in Caucasian children by capillary zone elec-trophoresis. Clin Chem Lab Med 39(10):970-2.
Bossuyt X, Peetermans WE [2002] Effect of piperacillin-tazobactam on clinical capillary zone electrophoresis of serum proteins. Clin Chem 48(1):204-5.
Bossuyt X, et al [2003a] Automated serum protein electrophoresis by Capillarys. Clin Chem Lab Med 41:704-710.
Bossuyt X, et al [2003b] Effect of sulfamethoxazole on clinical capillary zone electrophoresis of serum proteins. Clin Chem 49(2):340-1.
Bradwell AR, et al [2009] Assessment of monoclonal gammopathies by nephelometric measurement of individual immunoglobulin kappa/lambda ratios. Clin Chem 55(9):1646-55.
Briere RO, Mull JD [1964] Electrophoresis of serum protein with cellu-lose acetate. A method for quantitation. Am J Clin Pathol 34:547-551.
Brouwers A, et al [2007] Interference of ceftriaxone on capillary zone elec-trophoresis. Clin Chim Acta 376(1-2):255-6.
Bush D, Keren DF [1992] Over- and underestimation of monoclonal gammopathies by quantification of kappa- and lambda-containing immunoglobulins in serum. Clin Chem 38(2):315-6.
CAP [2011] Electrophoresis Survey.Cawley LP, et al [1965a] A simple semi-automated method of immuno-
electrophoresis. Clin Chim Acta 12(1):105-10.Cawley LP, Eberhardt L, Schneider D [1965b] Simplified gel electro-
phoresis. II. Application of immunoelectrophoresis. J Lab Clin Med 65:342-54.
Cawley LP, Eberhardtl [1962] Simplified gel electrophoresis. I. Rapid technic applicable to the clinical laboratory. Tech Bull Regist Med Technol 32:165-73.
Chang CY, et al [1997] Underestimation of monoclonal proteins by agarose serum protein electrophoresis. Ann Clin Lab Sci 27(2):123-9.
Clark R, et al [1998] Differential diagnosis of gammopathies by capil-lary electrophoresis and immunosubtraction: analysis of serum samples problematic by agarose gel electrophoresis. Electrophoresis 19(14):2479-84.
Dati F, et al [1996] Consensus of a group of professional societies and diagnostic companies on guidelines for interim reference ranges for 14 proteins in serum based on the standardization against the IFCC/BCR/CAP Reference Material (CRM 470). International Federation of Clinical Chemistry. Community Bureau of Reference of the Commission of the European Communities. College of American Pathologists. Eur J Clin Chem Clin Biochem 34(6):517-20.
Destro-Bisol G [1993] Reusing Cellogel strips after visualization of elec-trophoretically separated isozymes. Electrophoresis 14:238-239.
Destro-Bisol G, Santini SA [1995] Electrophoresis on cellulose acetate and Cellogel: current status and perspectives. J Chromatogr A 698:33-40.
Dispenzieri A, et al [2008] Appraisal of immunoglobulin free light chain as a marker of response. Blood 111(10):4908-15.
Donato L, et al [2011] A 71-year-old woman with multiple myeloma status after stem cell transplantation. Clin Chem 57(12):1645-1648.
Durie BG, et al [2003] Myeloma management guidelines: a consensus report from the Scientific Advisors of the International Myeloma Foundation. Hematol J 4(6):379-98.
Durie BG, et al [2006] International uniform response criteria for multiple myeloma. Leukemia 20(9):1467-73.
Gijbels K, De Coster J, Bossuyt X [2004] Interference by gelatin-based plasma substitutes in capillary zone electrophoresis. Clin Chem 50(8):1473-5.
Hawkins RC, Lee LK [2008] Immunoglobulin G paraprotein cross-reactivity with immunoglobulin M measurement. Ann Clin Biochem 45(Pt 4):431-3.
Henskens Y, et al [1998] Detection and identification of monoclonal gammopathies by capillary electrophoresis. Clin Chem 44(6 Pt 1):1184-90.
Janik B [1985] High Resolution Electrophoresis and Immunofixation of Serum Proteins on Cellulosic Media Ann Arbor: Gelman Sciences.
Jenkins MA et al [1995] Evaluation of serum protein separation by capillary electrophoresis: prospective analysis of 1000 specimens. J Chromatogr B Biomed Appl 672(2):241-51.
Jenkins MA, Guerin MD [1996] Optimization of serum protein separa-tion by capillary electrophoresis. Clin Chem 42(11):1886.
Jenkins MA, Guerin MD [1997] Capillary electrophoresis procedures for serum protein analysis: comparison with established techniques. J Chromatogr B Biomed Sci Appl 699(1-2):257-68.
Jenkins MA, Ratnaike S [1999] Five unusual serum protein presentations found by capillary electrophoresis in the clinical laboratory. J Biochem Biophys Methods 41(1):31-47.
Johansson BG [1972] Agarose gel electrophoresis. Scand J Clin Lab Invest Suppl 124:7-19.
f2.21 Use of the ratio of IgAK/IgAL to detect M-proteins. The 95% refer-ence interval is indicated within the parallel diagonal lines [Bradwell 2009]. Used with permission from Clinical Chemistry.

ISBN 978-089189-5916
25
2: TECHNIQUES FOR PROTEIN ELECTROPHORESIS AND MEASUREMENT OF M-PROTEINS
Jolliff CR, Blessum CR [1997] Comparison of serum protein electro-phoresis by agarose gel and capillary zone electrophoresis in a clinical setting. Electrophoresis 18(10):1781-4.
Kahn SN, Strony LP [1986] Imprecision of quantification of serum protein fractions by electrophoresis on cellulose acetate. Clin Chem 32(2):356-7.
Katzmann JA, et al [1997] Identification of monoclonal proteins in serum: a quantitative comparison of acetate agarose gel and capillary electro-phoresis. Electrophoresis 18(10):1775-80.
Katzmann JA, et al [1998] Prospective study of serum protein capillary zone electrophoresis and immunotyping of monoclonal proteins by immunosubtraction. Am J Clin Pathol 110(4):503-9.
Katzmann JA, et al [2011] Long-term biological variation of serum protein electrophoresis m-spike urine m-spike and monoclonal serum free light chain quantification: implications for monitoring monoclonal gammopathies. Clin Chem 57(12):1687-92.
Keren DF, Di Sante AC, Bordine SL [1986] Densitometric scanning of high-resolution electrophoresis of serum: methodology and clinical application. Am J Clin Pathol 85(3):348-52.
Keren DF [1998] Capillary zone electrophoresis in the evaluation of serum protein abnormalities. Am J Clin Pathol 110(2):248-52.
Keren DF, et al [1999a] Guidelines for clinical and laboratory evaluation patients with monoclonal gammopathies. Arch Pathol Lab Med 123(2):106-7.
Keren DF [1999b] Procedures for the evaluation of monoclonal immu-noglobulins. Arch Pathol Lab Med 123(2):126-32.
Keren DF, et al [2001] 2-Mercaptoethanol treatment improves measure-ment of an IgMkappa M- protein by capillary electrophoresis. Clin Chem 47(7):1326-7.
Keren DF, Gulbranson R, Ebrom SJ [2004] False-negative urine protein electrophoresis by semiautomated gel electrophoresis. Clin Chem 50(5):933-4.
Keren DF [2009] Heavy/light-chain analysis of monoclonal gammopa-thies. Clin Chem 55(9):1606-8.
Klein GL, Jolliff CR [1993] Chapter 16. Capillary electrophoresis for the routine clinical laboratory. In: Handbook of Capillary Electrophoresis, Landers JP, ed. Boca Raton, FL: CRC Press; 419-57.
Kohn J [1957] A cellulose acetate supporting medium for zone electro-phoresis. Clin Chim Acta 2:297-304.
Kremers B, Briere RO, Batsakis JG [1967] Reflectance densitometry of cellulose acetate protein electrophoresis. Am J Med Technol 33(1):28-34.
Laurell CB [1973] Electrophoresis, specific protein assays or both in measurement of plasma proteins. Clin Chem 19:99-102.
Leleu X, et al [2011] Novel M-component based biomarkers in Waldenstrom’s macroglobulinemia. Clin Lymphoma Myeloma Leuk 11(1):164-7.
Lichtinghagen R, Pietsch D, Brand K [2010] Evaluation of an automated capillary electrophoresis system for serum protein electrophoresis with the determination of gender-specific reference values. Clin Lab 56(3-4):119-26.
Litwin CM, et al [1999] Comparison of capillary zone and immunosub-traction with agarose gel and immunofixation electrophoresis for detecting and identifying monoclonal gammopathies. Am J Clin Pathol 112(3):411-7.
McCudden CR, et al [2010] Interference of monoclonal antibody therapies with serum protein electrophoresis tests. Clin Chem 56(12):1897-8
McCudden CR, et al [2008] Performance comparison of capillary and agarose gel electrophoresis for the identification and characterization of monoclonal immunoglobulins. Am J Clin Pathol 129(3):451-8.
Mendler MH, et al [1999] In patients with cirrhosis serum albumin determination should be carried out by immunonephelometry rather than by protein electrophoresis. Eur J Gastroenterol Hepatol 11(12):1405-11.
Merlini G, et al [1981] Detection and identification of monoclonal components: immunoelectrophoresis on agarose gel and immuno-fixation on cellulose acetate compared. Clin Chem 27(11):1862-5.
Mosser EL, Clark DA [1968] Estimation of serum proteins by quan-titative densitometry after gel electrophoresis. SAM-TR-68-133. [Technical report] Tech Rep SAM-TR 1-9.
Murray DL, et al [2009] Quantitation of serum monoclonal proteins: relationship between agarose gel electrophoresis and immunoneph-elometry. Clin Chem 55(8):1523-9.
Mussap M, et al [2006a] Evaluation of a new capillary zone electropho-resis system for the identification and typing of Bence Jones Protein. Clin Biochem 39(2):152-9.
Mussap M, et al [2006b] Measurement of serum monoclonal compo-nents: comparison between densitometry and capillary zone electro-phoresis. Clin Chem Lab Med 44(5):609-11.
Nutman TB [2001] Measurement of polyclonal immunoglobulin synthesis using ELISA. In: Current Protocols in Immunology, Coligan JE, ed, Chapter 7:Unit 7 12.
Ojala K, Weber TH [1980] Some alternatives to the proposed selected method for “agarose gel electrophoresis”. Clin Chem 26(12):1754-5.
Petrini C, et al [1999] Serum proteins by capillary zone electrophoresis: approaches to the definition of reference values. Clin Chem Lab Med 37(10):975-80.
Roudiere L, et al [2006] Evaluation of a capillary zone electrophoresis system vs a conventional agarose gel system for routine serum protein separation and monoclonal component typing. Clin Lab 52(1-2):19-27.
Ruggeri M, et al [2001] Linee guida per la diagnostica ed il montoraggio delle gammapatie monoclonali. Riv Med Lab-JLM 2(S1):68-71.
Schreiber WE, Chiang E, Tse SS [1992] Electrophoresis underestimates the concentration of polyclonal immunoglobulins in serum. Am J Clin Pathol 97(5):610-3.
Shin JW, Park R, Choi TY [2008] [A case of multiple myeloma showing marked differences in serum IgG levels between protein electropho-resis and turbidimetry]. Korean J Lab Med 28(4):282-5.
Sinclair D, et al [1990] Estimation of paraproteins by immunoturbidim-etry and electrophoresis followed by scanning densitometry. Ann Clin Biochem 27(Pt 4):335-7.
Smalley DL, Mayer RP, Bugg MF [2000] Capillary zone electrophoresis compared with agarose gel and immunofixation electrophoresis. Am J Clin Pathol 114(3):487-8.
Smith A, Wisloff F, Samson D [2006] Guidelines on the diagnosis and management of multiple myeloma 2005. Br J Haematol 132(4):410-51.
Snozek CL, et al [2007] Comparison of bromcresol green and agarose protein electrophoresis for quantitation of serum albumin in multiple myeloma. Clin Chem 53(6):1099-103.
Stemerman D, et al [1989] Precision and reliability of paraprotein deter-minations by high- resolution agarose gel electrophoresis. Am J Clin Pathol 91(4):435-40.
Sun T [1992] Interpretation of Protein and Isoenzyme Patterns in Body Fluids. New York, Tokyo: Igaku-Shoin; 81.
Tichy M [1985] A comparison of methods of monoclonal immuno-globulin quantitation. Neoplasma 32(1):31-6.
Uriel L [1958] Interpretation quantitative des resultats spres electropho-rese en gelose 1. Considerations generales application a l’etude de constituants proteiques isoles. Clin Chim Acta 3:234-238.
Vuorinen PI, et al [1989] Evaluation of the new Behring Nephelometer in the measurement of M proteins. American Journal of Clinical Pathology 92(1):93-6.
Wieme R [1965] Agar Gel Electrophoresis. Amsterdam: Elsevier.Zak B, Baginski ES, Epstein E [1978] Associated problems of protein elec-
trophoresis staining and densitometry. Ann Clin Lab Sci 8(5):385-95.
Zetterberg H, Nilsson-Ehle H [2004] False-negative result in the detection of an IgM monoclonal protein by capillary zone electrophoresis. Clin Chem 50(10):1878-80.

26
CHAPTER 3
Identification of M-proteins: Immunoelectrophoresis, Immunofixation, Immunosubtraction, and Isoelect
PRO
TEIN
ELE
CTR
OPH
ORE
SIS I
N C
LIN
ICA
L DIA
GN
OSI
S
CHAPTER 3
Identification of M-proteins: Immunoelectrophoresis,
Immunofixation, Immunosubtraction, & Isoelectric Focusing
Whereas one can use protein electrophoresis to detect suspicious bands in serum, urine, and cerebrospinal fluid, it cannot
definitively identify such restrictions as an M-protein. For that, immunochemical methods, often together with electrophoresis, must be employed.
Today, to identify a restriction as an M-protein, most laboratories using gel-based techniques perform immunofixation (IFE), while those using capillary electrophoresis (CE) perform immunosubtraction (ISUB). In addition, nephelometric techniques are available that can suggest the presence of an either an intact immunoglobulin M-protein or a monoclonal free light chain (MFLC).
An older technology, immunoelectrophoresis (IEP) is still used by a few laboratories. However, it has largely been abandoned because it is slow, lacks sensitiv-ity and is more difficult to interpret than IFE.
Principles of ImmunoprecipitationWhether one is performing IFE, ISUB, or IEP, the
basic principles of the precipitin reaction are applicable to all 3 methods. A detailed understanding of the precipitin reaction is critically important to making the correct interpretation of a given sample. Immunoprecipitation is the interaction of antibody molecules with antigen in either a gel or liquid matrix in which the molecules are free to diffuse. The key to precipitation is the multivalent nature of both the antigens and antibodies (each has 2 or more sites with which they can interact) [Remaley 2006].
In most chemical reactions, when substance A is mixed with substance B to form a product C the reaction can be expressed as
A + B CAs shown in f3.1, as one increases the amount of
substance A while maintaining the amount of substance B constant, the amount of precipitate C increases up to a point. Then, further addition of A does not result in an increase in C because all of the available substance B has been exhausted.
Similarly, in immunologic reactions, a precipitate (the product in this case) will form when antibody is added to its antigen. Unlike the chemical reaction shown in f3.1, however, a decrease in the amount of precipitate occurs when excess antibody is added to a constant amount of antigen f3.2. Therefore, there is something about the interaction of antibodies with antigens that differs from the simple chemical reaction shown before.
f3.1 As substance B is used up, no more product C is formed by the addition of substance A.
f3.2 This classic immunoprecipitin curve shows that the amount of precipitate (antigen-antibody complex) decreases with the addition of excessive amounts of antibody.

ISBN 978-089189-5916
27
3: IDENTIFICATION OF M-PROTEINS: IMMUNOELECTROPHORESIS, IMMUNOFIXATION, IMMUNOSUBTRACTION, & ISOELECTRIC FOCUSING
Antibody-antigen interactions are highly complex because of the many variables involved. First, a given antigen molecule usually possesses many different specific sites to which antibodies may bind. These sites are called antigenic determinants or epitopes f3.3. Antibodies against each antigenic determinant are produced by several clones of plasma cells. And each plasma cell clone’s product will have unique binding strength for that particular determi-nant. This strength of binding of an antibody to a particu-lar determinant is referred to as the antibody’s “avidity.”
The binding of antibody molecules to antigenic determinants depends on 4 types of noncovalent interac-tions. The forces involved are:
1. Coulombic forces that result from the attraction of oppositely charged polar groups such as –NH3
+ and –COO–
2. Hydrogen bonding that results from the attraction of a hydrogen atom closely linked to an electronegative atom (such as oxygen), with another electronegative atom
3. Hydrophobic bonding that is analogous to the observation of oil in water. Even when dispersed, oil will coalesce, excluding the intervening water molecules. Hydrophobic bonding occurs due to the preference of apolar groups for self-association
4. Van der Waals forces that are interactions occurring in the outer electrons of the reactants. These relatively weak forces gain considerably in strength as the distance between antigen and antibody molecules decrease
None of these interactions has the strength of cova-lent bonding; therefore, antibody-antigen interactions are readily reversible. The strength of the attraction of a partic-ular antibody for a particular antigenic determinant (affin-ity) depends on the number and strength of the combined 4 types of bonds described above. Optimal formation of
antibody-antigen interactions occurs when the 2 compo-nents are at equivalent concentration.
Understanding the immune precipitin reaction and the need to consider the concentration of the antibody and antigen is critically important to optimize IFE, ISUB, isoelectric focusing (IEF) and nephelometric techniques. Although the following concepts are quite basic, commer-cial products whose instructions try to simplify the tech-nique occasionally minimize these basic principles and may lead to false negative results. Before launching into a discus-sion of the chemistry involved, a case example may help to illustrate the relevance of this point.
In f3.4, the cathodal end of the serum protein electrophoresis (SPE) lane reveals a small restriction (band) that strongly suggests the presence of an M-protein.
f3.3 Most antigens are complex molecules with many surface epitopes to which antibodies will form. In turn, several different B-cell clones may respond to each epitope, creating a diverse array of antibody specificities with a variety of binding strengths in the reagent antisera that we use.
f3.4 a IFE of a serum referred to us from another laboratory. Specific anti-sera were added to the lanes as indicated by the immunoglobulin labels. The dilutions used were not provided. The anode is on the top. Note the sharp band at the extreme cathodal end of the SPE lane (arrow). Why are the bands in the IgG and Κ lanes so broad? Why is there no sharp band at the cathodal end? Did the technologist add the sample to the lanes labeled IgA, IgM, and λ? (Beckman Paragon system, anode at the top) b The top sample is from the case shown in f3.4a. The distinctive γ region band is also seen in our gel (arrow). The bottom sample is not from the present case but shows a striking M-spike. (Paragon SPE2 system) c IFE in our laboratory demonstrates the IgG κ M-protein. No IgM was run on this gel. Instead 2 concentrations of κ were used to see if the slow γ band became weaker at greater concentrations. Note that IgA and λ are visible, because the dilutions used were optimized to precipitate the normal polyclonal IgA and λ that were present. Note that the IgA is migrating in the correct posi-tion for polyclonal IgA, the β region. (Beckman Paragon system)
a
b
c

28
3: IDENTIFICATION OF M-PROTEINS: IMMUNOELECTROPHORESIS, IMMUNOFIXATION, IMMUNOSUBTRACTION, & ISOELECTRIC FOCUSINGPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
However, the IFE showed broad reactivity with antisera against IgG, and and no precipitation in the area of the restriction in the SPE lane. When we repeated the IFE using dilutions to better optimize the amount of antigen (M-protein) and antibody, an obvious IgG M-protein was confirmed.
The problem demonstrated here is an antigen excess effect. When we performed the repeat immunofixation at 2 concentrations, 1:10 and 1:20, both gave interpretable but slightly different results. This example demonstrates that adjusting the concentration to better approach equivalence may be important to correlate IFE findings with the SPE.
In this case, the dilutions of the serum on the first IFE gel resulted in antigen excess effect. Note also that the lanes shown where the patient’s serum was reacted with anti-IgA and anti- had no precipitate at all in f3.4a. Was the sample or the reagent antiserum omitted from these lanes, or was the dilution of serum used too large, resulting in a precipitate too small to be seen? I don’t know. This is another problem with using a standard dilution that doesn’t attempt to equate concentration of the antibodies in the serum with the concentration of reagent antiserum.
Why were broad precipitates of IgG and on the first IFE anodal to the major band in the slow region? This represented lower concentrations of the M-protein that had migrated behind the major M-spike. The broad migration may have reflected some self-aggregation, heavy glycosylation, or the known microheterogeneity of M proteins [Harrison 1991]. It stained well, however, because the concentration of the M-protein in this region was considerably less than that at the slow region where the complexes formed were small (antigen excess) and as a consequence did not precipitate, but were removed during the washing that occurs after the precipitation reaction (see below).
Antibody-Antigen Interaction In the immune precipitin reaction, the interaction
of multivalent antigen and antibody molecules results in formation of a lattice f3.5. In the zone of antigen excess, the large amount of antigen present increases the likelihood that relatively small immune complexes form. At the extreme, the formula of this antigen excess complex would be:
Ab(1)Ag(2)These molecules are too small to precipitate
under the conditions of this assay and are discarded with antigenically unrelated protein molecules during the washing step.
As more antibody is added to the system, a precipitate (large antibody-antigen latticework) begins to form until the optimal precipitate is created at the zone of equivalence with a formula of
Ab(1)Ag(1)With the addition of still more antibody, the
antigenic determinants on the surface of the antigen become saturated with antibody molecules and few are available for reaction with other antibodies to cross-link the molecules. Here the formula is
Ab(x)Ag(1)where x equals the number of antigenic determinants expressed on the surface of a particular antigen.
For optimal IFE, a large cross-liked precipitate is needed. Smaller immune complexes usually formed at antigen excess can result in false negative results as shown in f3.4.
Interpreting Antibody-Antigen Precipitation ReactionsDouble Diffusion in 2 Directions (Ouchterlony Technique)
Ouchterlony devised a simple way to use the immunoprecipitation reaction to determine antibody reactivity and to identify unknown antigens [Ouchterlony 1966]. Cawley also experimented with double immunodiffusion in agar [Cawley 1965a]. They cut wells in an agarose gel and put antibody in one well and antigen in a nearby well. These were placed in a high-humidity chamber (to prevent the gel from drying) and with time (typically overnight) molecules diffused radially out of the wells f3.6.
As they diffuse away from the center of the well, the concentrations of antigen and antibody decreases logarithmically. A precipitin band forms somewhere between the 2 wells at the point at which the concentrations of the reactants are equivalent. If the precipitate was closer to the antigen well, it indicated that the antibody was more concentrated than the antigen in the preparations because the antibodies
f3.5 Multivalency of antibody and antigens is responsible for the classic immunoprecipitin curve.

ISBN 978-089189-5916
29
3: IDENTIFICATION OF M-PROTEINS: IMMUNOELECTROPHORESIS, IMMUNOFIXATION, IMMUNOSUBTRACTION, & ISOELECTRIC FOCUSING
needed to diffuse further (thereby becoming more dilute) before the precipitate could be seen.
Other factors, such as the size of the molecules and interactions that the molecules may have with the gel, also affect this reaction. The beauty of the antibody-antigen interactions was that the concentrations automatically adjusted to form the precipitate by the diffusion.
Ouchterlony also found that by placing an antigen of known reactivity (call it “A”) in one well, an antiserum of known reactivity for 2 antigens (A and B) in another well, and an unknown solution in a third well, he could determine whether the unknown solution contained one or both of these antigens f3.7. If the unknown solution contained antigen B, 2 precipitate bands formed that crossed each other. This pattern of reactivity was termed “nonidentity.” It results because the antibodies against antigen B do not react with anything in the lattice and are free to pass through it until they meet antigen B and form a precipitate with that antigen.
If the unknown solution contained antigen A, 2 precipitate bands formed and met but did not cross,
and it was termed “identity.” The lines do not cross, because antibodies against antigen A are “removed” by reacting in the precipitate.
If the unknown solution contained a chemically similar antigen but one that lacked one of several antigenic determinants found on antigen A, 2 lines again form, but there is a “spur” due to antibodies that react with the determinants on A that are not present and, therefore, could not be removed by A. This pattern is termed “partial identity.”
Combining Antibody-Antigen Interactions in Gel with ElectrophoresisImmunoelectrophoresis (IEP)
A logical outgrowth of the immune precipitin reaction was to combine it with electrophoresis to achieve separation by charge and then identification of the molecules by immunologic techniques [Cawley 1965c]. For many years, IEP was the mainstay of this technology. Some early systems even automated portions of the technique [Cawley 1965b].
IEP is performed by placing the patient’s serum in a series of wells in an agarose gel. At the same time, a control serum is placed in alternative wells in the gel f3.8, f3.9.
The sample is electrophoresed to separate the major serum proteins by their charge f3.8. After electrophoresis, the gel is removed from the
f3.6 In Ouchterlony gels, as antibody and antigen diffuse from the well, their concentrations decrease logarithmically. The precipitin line forms where the concentrations are equivalent.
f3.7 Ouchterlony plate demonstrating nonidentity, identity, and partial identity. (See text)
f3.8 IEP takes advantage of the principles of electrophoresis, gel diffusion (which adjusts concentrations during diffusion), and antibody-antigen precipitin reactions to identify specific proteins. In the example shown, only IgG is precipitated and present after the wash step. The closer IgG is to the antiserum trough, the greater is its concentration. Large molecules such as pentameric IgM can be difficult to examine by this technique because they diffuse slowly through the agarose. Small quantities of monoclonal proteins are also difficult to identify because this technique does not offer good resolution of individual proteins.

30
3: IDENTIFICATION OF M-PROTEINS: IMMUNOELECTROPHORESIS, IMMUNOFIXATION, IMMUNOSUBTRACTION, & ISOELECTRIC FOCUSINGPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
electrophoretic apparatus and the troughs are filled with antisera to various specific components of interest.
Anti-pentavalent antisera (anti-IgG, IgA, IgM, & )Anti-IgGAnti-IgAAnti-IgMAnti-Anti-
The samples are then placed in a high-humidity chamber overnight (typically) to allow the antigens and antibodies to diffuse as shown in f3.8.
The precipitin bands that forms with the patient’s serum are compared with the control serum across each trough. A normal reaction is a smooth broad arc that looks similar to the control in terms of migration. However, the distance to the trough often differs from the control depending on the concentration of the specific antigen in each serum. The greater the concentration of the antigen, the closer it migrates toward the trough. If the patient has a strong polyclonal increase in IgG (for instance), it might even migrate partially into the trough.
If the patient has an M-protein, there is a relatively high concentration of the antigen in the region of that protein’s electrophoretic mobility, while the rest of the patient’s antigen of that type is present in either normal or decreased concentration f3.9. This results in a distortion of the arc that is referred to as “restricted mobility.” Finding restricted mobility in one heavy chain type and one light chain type that both migrated to the same electrophoretic location on the gel is the sine qua non for identifying an M-protein.
IEP was a significant advance in the identification of M-proteins associated with multiple myeloma (MM) and Waldenström macroglobulinemia (WM). Unlike the antigen excess problem with IFE discussed above, IEP is not as profoundly affected by the antigen excess. When the antigen diffuses into the agarose, its concentration decreases greatly, allowing the system to automatically adjust to antigen-antibody equivalence and a precipitin arc to be formed. When M-proteins are present in large quantities, IEP is usually able to detect the condition properly because of this diffusion effect [Penn 1978]. The larger quantity of antigen in such circumstances diffuse further from the well towards the trough to decrease its concentration and will often have its precipitin arc restricted and close to the trough. Because of the antigen excess effect, the precipitate could almost disappear in the center of the arc. As with a polyclonal increase in IgG, an M-protein in large quantity diffuses into the trough f3.10. Except in extreme cases, the diagnosis readily can be made without diluting the serum
Similarly, IEP can detect a second M-protein that results from the presence of an MFLC simultaneously with an M-protein that is an intact immunoglobulin
molecule. The MFLC has a different isoelectric point (pI), has a much smaller molecular weight, and is usually present at a different concentration from the intact immunoglobulin M-protein. Because of this, the MFLC can be distinguished because of its unique migration and position relative to the well or origin and the distance it diffused toward the trough before precipitating.
Free light chains also express certain antigenic determinants that are not expressed by light chains that are attached to intact immunoglobulin molecules. These “hidden determinants” will react with commercial antisera against light chains f3.11. Indeed specific antibodies against these determinants are now available and are the basis for the nephelometric assay for serum free light chains (see below). Consequently, as with the Ouchterlony patterns of partial identity discussed above,
f3.9 This IEP shows a large IgG λ M-protein. Note that control (c) serum alternates with patient (p) serum. Antisera with Pentavalent (PV) reactiv-ity (against IgG, IgA, IgM, κ and λ in one reagent) and individually specific antisera with reactivity for IgG (G), IgA (A), IgM (M), κ (K), and λ (L) were placed in the troughs. A large arc with excessive anodal migration is seen in the PV reagent, IgG, and λ areas of the patient’s sample (indicated in all 3 locations). The λ arc stains weakly, which is the prozone phenomenon often seen with λ reagents. Diagnosis of such large M-spikes is relatively easy by IEP.
f3.10 IEP of urine shows a large λ monoclonal free light chain (Bence Jones) protein. Note that control (c) is serum so that we can see the position of normal IgG, IgA, and IgM. Normal urine would have too little im-munoglobulin to detect with this method. The patient’s urine (p) has so much of the λ M-protein that it has substantially diffused into the trough before reaching “equivalence” and forming a precipitate with the anti-PV and anti-L reagents (indicated). Note that the PV reaction is quite weak. It is typical for PV reagents
to have relatively weak anti-λ reactivity. Compare this to f3.9 (symbols are same), in which the dense reaction in the PV reagent is due to the anti-IgG (G) in the PV reagent.

ISBN 978-089189-5916
31
3: IDENTIFICATION OF M-PROTEINS: IMMUNOELECTROPHORESIS, IMMUNOFIXATION, IMMUNOSUBTRACTION, & ISOELECTRIC FOCUSING
when the intact immunoglobulin molecule reacts with the antiserum it cannot remove antibodies to these hidden determinants. The latter antibodies continue through the precipitin band to react with the free light chain.
Limitations of IEP
There are several limitations with IEP that resulted in its replacement by the more sensitive IFE and more facile ISUB techniques for the identification of M-proteins. IEP is very slow, requiring 18 to 24 hours or more to complete. Due to the architecture of the precipitin bands, it is inherently more difficult to interpret than IFE. Lastly, it is much less sensitive than IFE in detecting small M-proteins [Aguzzi 1984, Chowdhury 2002, Pudek 1982, Reichert 1982, Ritchie 1976c, Smith 1980, Whicher 1984].
The case shown in f3.12 is a typical example of the “umbrella effect.” The patient has an IgM M-protein where the IgM by nephelometry measured over 1.3 g/dL, yet the light chain type of the M-protein could not be identified by the IEP. Monoclonality could not be determined because the patient had a normal concentration of IgG. The lower molecular weight of IgG (160 kDa) compared to IgM (1,000 kDa) allows the IgG to diffuse more quickly than the large IgM thorough the agarose. By reaching the antisera against light chains first, the polyclonal IgG binds to the anti-K and anti-L antisera, which prevents reaction of anti-light chain antisera with the bulkier IgM that is closer to the origin. This shielding of an IgM M-protein by normal polyclonal IgG molecules is called the “umbrella effect” [Kahn 1988, Lane 1985, Normansell 1985, Sun 1979]. Despite these limitations, when relatively low quantities of polyclonal IgG was present, IEP could detect classic cases of WM and even unusual conditions such as monoclonal IgM in a child with ataxia-telangiectasia [Cawley 1970].
To improve detection of some IgM M-proteins, laboratories needed to reduce the IgM into monomers by using 2-mercaptoethanol (2-ME) to break the disulfide
bonds. To perform the procedure, we recommend using 5 microliters of 0.1M 2-ME in 1.0 ml of the serum. This is incubated for 1 hour at 37°C. This technique, or deploying penicillamine as the reducing agent, usually allows good visualization of IgM M-spike [Capel 1980, Herrlinger 1976,
Lane 1985, Normansell 1985, Orr 1979, Prokesova 1969, Sorenson 1988]. If the reduction is not successful, one may resort to a sizing column to separate IgM from IgG and then repeat the IEP on the separated fraction.
These methods are laborious, costly, and their slowness delays the diagnosis. With IFE or ISUB, one obtains the correct result in a couple of hours. Further, we have found that less than half of the costly reagent antisera is needed with IFE. Also, newer techniques are semiautomated, dramatically cutting down on technologist time. The IFE from the serum from this same case of IgM WM is easily interpreted without further study f3.13.
f3.11 An IEP from a serum is shown containing an IgG λ M-protein and a monoclonal free λ free light chain. The free λ M-protein is detected by the PV reagent where the extra arc due to the anti-free λ is indicated. The same area is indicated in the anti-L reaction with the patient’s serum in the bottom trough. This area is not seen with the anti-IgG reagent. Once again, the anti-L reagent gives a weak reactivity.
f3.12 Nondiagnostic IEP in a patient with 4-fold increase in IgM and an obvious γ spike on the serum protein electrophoresis (shown on the top of f3.13. Most of the patient’s pentameric IgM is barely able to migrate out of the well, forming diffuse hazy area indicated near the origin. With the anti-IgM reagent, there is a slight cathodal restriction. However, the normal K and L arcs once again represent the patient’s normal serum IgG and do not reflect his monoclonal protein (so-called “umbrella effect”).
f3.13 Immunofixation of serum from f3.12. Top sample is the SPE of the patient’s serum run at same time as IFE (anode at left). The interpretation of the IgM κ M-protein is obvious. Note that the M-protein has the same electrophoretic migra-tion in the reaction with anti-IgM and anti-K. Also, by using the serum at the proper dilution (see text), one has a built-in control for the antisera. IgA reacts as a broad β region band where IgA normally migrates. Similarly,
anti-IgG and anti-L reagents show proper reactivity. (Dilutions used: IgG 1:10, IgA 1:2, IgM 1:13, K 1:14, L 1:4; Panagel system)

32
3: IDENTIFICATION OF M-PROTEINS: IMMUNOELECTROPHORESIS, IMMUNOFIXATION, IMMUNOSUBTRACTION, & ISOELECTRIC FOCUSINGPR
OTE
IN E
LEC
TRO
PHO
RESI
S IN
CLI
NIC
AL D
IAG
NO
SIS
Immunofixation (IFE)
IFE brought a dramatic improvement to the identification of M-proteins in the clinical laboratory [Cawley 1976, Janik 1981, Ritchie 1976a, 1976b, 1976c, Sun 1979]. With modern semiautomated methods, IFE can now be performed simultaneously on several samples at once in about 2 hours with minimal technologist time f3.14. IFE is not subject to the umbrella effect, can readily detect small quantities of M-proteins, is easier to interpret than IEP, uses less than half the antisera as IEP, and requires the same equipment as that needed for commercially available protein electrophoresis methods.
Selection of the Dilution of Patient’s SerumOne advantage that IEP had over IFE was the
self-adjustment of the concentration of the M-protein to that of the reagent antisera that was achieved by the slow diffusion step. This step in IEP allowed the antigen and antibody to adjust to equivalence for maximal precipitation. And it avoided most problems of antigen excess that occur with IFE if the sample is not properly diluted. In IFE, the reaction occurs more rapidly than with IEP because reagent antiserum placed directly on the gel eliminates the diffusion step.
To achieve optimum sensitivity and to avoid the antigen excess effect, it is helpful to use a dilution of the serum that places it close to the equivalence range for the immunoprecipitation reaction. There is considerable variation in the strength and specificity of commercial antisera. Monos et al compared several commercial sera with the same M-proteins and found variable detection of the M-proteins [Monos 1989]. They also noted that an M-protein present at a concentration of 700 mg/dL could be missed if the incorrect dilution of the patient’s serum was used with a commercial antiserum with poor reactivity for that particular protein.
There are several ways to determine which dilution of serum to use. The first is to use a standard dilution. While this simplifies the assay, it presents problems in cases with very high or very low concentrations of M-proteins. Monos et al reported the following dilutions of serum could identify the M-protein in most cases: 1:10 for IgG, 1:5 for IgA, IgM, and , and 1:2 for
[Monos 1989]. They cautioned, however, that if equivocal results are obtained using these standard dilutions of reagent antiserum, the analysis should be repeated using a different antiserum (or different dilution of the patient’s serum).
Fortunately, because of the broad range of the equivalence zone for the immunoprecipitation reaction, there is usually considerable leeway with the dilutions used. As shown in f3.15, the M-proteins are detected by a variety of dilutions around the equivalence region. But, because reactivity does vary from one M-protein to another and from one antiserum to another, occasionally a significant M-protein will be missed via the “one set of dilutions fits all” strategy.
When possible, it is a great advantage to know the concentrations of the IgG, IgA, and IgM when setting up the IFE. Hadler et al recommended that the optimum concentration of antigen for detection of M-proteins in the system they used was 28-35 mg/dL [Hadler 1995]. In our laboratory, when using most commercial antisera for the first time, a concentration of the antigens (IgG, IgA, IgM, or ) of about 100 mg/dL works well. Antisera against tend to give weaker reactions that vary from one reagent to another, sometimes requiring unique dilutions.
An example of the weakness of anti- reagents is shown in f3.16. The SPE gel shows a prominent slow -migrating M-spike. By nephelometry, the IgA measured an improbable 14,400 mg/dL. Yet with a
f3.14 Semiautomated IFE gel from Sebia that demonstrates 9 monoclo-nal proteins with minimal technologist time. The application, wash, and staining steps are performed by the instrument.
f3.15 IFE of serum from patient with an IgG κ M-protein. The concentra-tion of the IgG was 1,740 mg/dL. The monoclonal band is readily seen at the 1:20, 1:40, and 1:80 dilutions. At 1:10 the band is visible, but is considerably obscured by the amount of polyclonal IgG present. At 1:5, there is a slight indentation at the junction of the band with the cathodal end of the polyclonal IgG (arrow). However, I believe that this would have been missed. With the IgG undiluted (left lane), the band is not detect-able. (Paragon system, anode at the top)

ISBN 978-089189-5916
33
3: IDENTIFICATION OF M-PROTEINS: IMMUNOELECTROPHORESIS, IMMUNOFIXATION, IMMUNOSUBTRACTION, & ISOELECTRIC FOCUSING
1:10 dilution of IgA, the M-protein stained strongly, perhaps obscuring the possible second IgA band (likely a multimer of the major band). At a 1:100 dilution, both the major band and the second band are seen to advantage with the anti-IgA reagent. Note that there was less reactivity with the anti- reagent. At a 1:10 dilution, an antigen excess effect is seen. The center of the major precipitate has been washed away due to insufficient cross-linking. Even at a 1:50 dilution the center of the precipitate has begun to wash away. With most antigen excess effects, one can still make the diagnosis of the type of M-protein present, but this varies from case to case. When in doubt, rerun the sample at other dilutions or with other antisera.
Most manufacturers recognize the need to adjust the concentration of serum to account for extremely high and low levels of antigen. For instance, the Sebia Hydragel system recommends different dilutions of the serum depending on the total immunoglobulin
concentration. When using homebrew IFE or with kits where no suggestion is provided for diluting, adjustment for concentration of an M-protein may be accomplished in one of several ways. One may first quantify IgG, IgA and IgM by an immunoassay (nephelometry, turbidimetry, ELISA or radial immunodiffusion) and then use these values to estimate the optimal dilution as shown in t3.1. If the laboratory does not perform immunoglobulin measurements before performing immunofixation, one may use the region protein estimation from either the densitometric scan (for gel-based systems) or from the electropherogram (for capillary electrophoresis). The globulin region provides a rough estimate of IgG. With most -migrating IgG M-proteins, there is a reasonable correlation between the region measurement and the IgG determined by immunologic methods [Keren 1986,
Schreiber 1992, Uriel 1958].Once one knows the approximate value for IgG,
about 2/3 of those molecules will be and 1/3 . Both IgA and IgM usually are present in relatively low concentrations (<300 mg/dL in individuals with normal SPE patterns). As a result, I recommend using a 1:2 dilution of the serum for the IgA and IgM immunofixation. It is unusual that a dilution of serum greater than 1:4 dilution will be needed to avoid extreme antigen excess for IgA and IgM when there is no abnormality in the or - region of the SPE.
Since we perform IFE after SPE, the presence of a suspicious band, along with its size, alerts us to the occasional need to increase the dilution of serum for the IFE. Occasionally, there will be a discrepancy between the densitometric scan of the gel or the electropherogram of the CE and the nephelometric measurement of the serum immunoglobulins. We have found this to be a problem most often with IgM M-proteins. By treating the serum with 2-mercaptoethanol (2-ME) thereby breaking the IgM pentamers into monomers, the problem is
f3.16 a SPE gel where the bottom lane contains a massive M-spike in the slow β region. The serum immediately above this sample has a small M-spike in the β-γ and a tiny restriction in the slow γ region. Since the monoclonal band in the bottom lane stains as dense as the albumin bands on this gel and is considerably broader, one can estimate that it will have about twice as much protein as albumin (about 8 grams/dL) (Paragon SPE2 system). b IFE of the sample from the bottom lane of f3.16a using the indicated dilutions of patient’s serum. Note that the SPE lane did not fix the albumin band. This may have resulted if the acid fixa-tive was not properly applied. A large IgA M-spike is readily seen at the 1:10 and 1:100 dilutions, but a second IgA band is somewhat obscured by the adjacent large IgA band at 1:10, but stands out nicely (arrow) at the 1:100 dilution. The center of the λ precipitate has washed away at the 1:10 (XS arrow) dilution and even to some extent at the 1:100 dilution. A diffuse (polyclonal) κ band is seen using the 1:20 dilution. It indicates the presence of this patient’s normal κ-containing immunoglobulins. (Paragon system, anode at the top)
a
b
t3.1 Calculation of Dilution of Serum to Use with Home Brew Immunofixation
ImmunoglobulinConcentration (mg/dL) Dilution*
IgG 1,434 1:14
IgA 241 1:2
IgM 126 1:2†
-containing 1,047 1:10
-containing 683 1:7‡
*In this example, dilution is based on closest approximation to 100 mg/dL. If antigen excess effect is seen, a greater dilution of serum will be needed for your system. If no precipitate is seen, a more concentrated patient sample may be needed. Adjustment needs to be made against controls with each new lot of antisera.†Dilute at least 1:2 to minimize the origin artifact‡Antisera against λ-containing immunoglobulins tend to give weak precipitates, adjustment of the dilution of patient’s sample may be necessary