Embed Size (px)
Citation preview

Midface Sculpting withAutologous Fat
Lesley A. Rabach, MDa,*, Robert A. Glasgold, MDb,c, Samuel M. Lam, MDd,Mark J. Glasgold, MDb,cKEYWORDS
� Fat grafting � Aging face � Volume loss � Midface
KEY POINTS
� There is currently a major paradigm shift from purely excision-based surgery to combined surgicaland volume enhancement.
� Because there is still no perfect facial filler, development of synthetic facial injectables continue toadvance at a remarkable pace.
� Each type of filler carries a specific characteristic that makes it more suitable for a certain clinicalapplication.
� The continuing change in facial fillers offers the possibility for volume augmentation procedureswith less downtime and without the need for harvesting fat.
� We predict that volume enhancement will continue to play an increasing role as both a complemen-tary procedure and as a stand-alone procedure in facial rejuvenation.
INTRODUCTION
Over the past several years, the role of volumerestoration with autologous fat has become anincreasingly recognized entity as a primary mech-anism by which to overcome the aging process.Facial fat grafting has assumed a renewed interestamong aesthetic surgeons owing to technical ad-vances that have been shown to be beneficialboth in achieving consistently excellent cosmeticresults and in limiting morbidity.1
The aging process can be understood with asimple analogy of the aging face: in youth, theface is like a grape, and as people age, volumedepletion causes the face to become like a raisin.When performing age-related surgeries, the re-dundant skin is lifted, pulled, and cut away sothat the remainder no longer resembles thegrape of youth but is more like a truncated pea.
Disclosures: The authors have no disclosures.a Private Practice, 224 Riverside Drive #3D, New York, NYRutgers University, New Brunswick, NJ, USA; c Private Prad Willow Bend Wellness Center, 6101 Chapel Hill Boulev* Corresponding author.E-mail address: [email protected]
Facial Plast Surg Clin N Am 23 (2015) 221–231http://dx.doi.org/10.1016/j.fsc.2015.01.0081064-7406/15/$ – see front matter � 2015 Elsevier Inc. All
This approach does not restore all the highlights,contours, and convexities of youth. Filling thedepressed facial zones helps restore a youthfulappearance more effectively. Note that this reduc-tionist philosophy does not reflect the authors’opinion entirely, because we recognize the com-plexity of the aging process that can comprisevolume loss, volume gain, gravitational descent,and dermatologic changes. In the past, the agingface was perceived as a change caused by gravityand skin redundancy and it is now interpreted asarising from tissue deflation, which can be cor-rected with facial fat grafting.2
The best approach for prospective patientswith aging faces seeking to restore a youthfulcountenance is to view old photographs from thepatient’s youth. Old photographs provide a frame-work for our goals and help the patient understandwhat combination of procedures will provide a
10025, USA; b Robert Wood Johnson Medical School,ctice, 31 River Road, Highland, Park, NJ 08904, USA;ard, Suite 101, Plano, TX 75093, USA
rights reserved. facialplastic.theclinics.com

Rabach et al222
natural and rejuvenated appearance. During theconsultation and evaluation, it is important tomaintain a global approach for optimal rejuvena-tion. The myriad of procedures may include fatgrafting, face-lifting, microliposuction/liposuction,blepharoplasty, and or skin therapies. The combi-nation approach toward fat grafting is not neces-sarily a stand-alone procedure in every case butan adjuvant to traditional procedures (Fig. 1).3
This integrated strategy allows the surgeon toselect the right combination of individually tailoredprocedures based on how that person lookedpreviously.The advent of disposable microcannulas for use
with office-based facial fillers, and the continueddevelopment of filler products intended for facialvolumization, has challenged fat grafting as thesole method for facial volumization. Fillers arenow a suitable alternative in patients who desirefat transfer or as an adjunct to fat transfer becausemicrocannulas can be used for advanced facialsculpting, which fat grafting alone was only ableto achieve a few years ago.3
This article proposes a systematic approachto facial fat enhancement of the midface empha-sizing simplicity, consistency, and safety, whichis the result of a decade of clinical experiencewith ongoing refinements in technique. Autolo-gous fat transfer plays a critical role in facialrejuvenation of the midface as a stand-alone
Fig. 1. (A, B) Combination approach to fat grafting. Uppefat transfer to the upper eyelid, lower eyelid, cheek, submagold, MD. Reprinted with permission from Glasgold Grou
procedure or in combination with traditionalage-related surgeries.4 Preoperative educationand counseling are emphasized.
TREATMENT GOALS AND PLANNEDOUTCOMES
There are several goals of facial fat grafting. Thesegoals include the achievement of a natural rejuve-nation and restoration of youth, the avoidance ofcomplications, and the attainment of long-lastingaesthetic benefit. In the modern era of facial fatgrafting, learning about autologous fat graftingrequires completely rethinking of the approachto the aging face. Clinicians must use a novelaesthetic appreciation of the aging process. Clini-cians also must use new operative techniques,including body harvesting and infiltration, andmust manage unique complications.5 The detailsof approach and technique are described later.Facial aesthetic surgeons must think about
autologous fat transfer in a different manner thana typical operative procedure. Specifically, typi-cally they strive for the ideal result; however,for autologous fat transfer, a more conservativeapproach is advocated.6 Surgeons must tapertheir expectations. In particular, as the limit of fattransfer is pushed by increasing volumes trans-ferred to obtain an ideal result, the associatedincreased recovery time and potential for
r and lower eyelid blepharoplasty was performed withlar and buccal regions. (Photo courtesy of Robert Glas-p Plastic Surgery, 2012.)

Midface Fat Sculpting 223
complications increase dramatically. If the sur-geon or patient thinks that they is undercorrected,reharvest and transfer of additional fat is an easytask compared with the difficulty of correcting acomplication such as a visible contour irregularityor reduction of an overcorrected face. Thus, con-servatism should be the rule, especially for sur-geons inexperienced with facial fat grafting.
The aesthetic of volume enhancement em-bodied by facial fat grafting mandates a differentapproach to patients. The goal of facial fat transferis to return patients back to their own youthful ap-pearances. Many aesthetic surgeons now eval-uate a patient during consultation and attempt todefine what areas of the face require improvementwithout reference to how the patient lookedwhen younger. Patients are encouraged to bringin young photographs, which help the surgeonevaluate the patient’s youthful appearance andhelp the patient understand the importance of vol-ume loss in the aging process and the need toreplace it. The patient must help guide the desiredaesthetic outcome. Regardless, patients’ pastphotographs are reviewed to help the patients un-derstand the role of fat grafting. Past photographsalso help surgeons to conceptualize the optimal fatgrafting plan.
Fig. 2. (A, B) Fat grafting to the upper eyelid, lower eyelidand upper and lower eyelid blepharoplasty. (Photo courtefrom Glasgold Group Plastic Surgery, 2012.)
Our vision for facial rejuvenation does not insistthat autologous fat transfer is the only possiblemethod by which facial enhancement is achieved.Fat grafting is a complementary role in our clinicalpractice. We think that a patient’s aesthetic resultcan be greatly enhanced by the use of a combina-tion of approaches; for example, fat grafting, face-lifting, and blepharoplasty (Fig. 2). Patients areconsiderably more pleased when each procedureadds to the tally of aesthetic improvement. Tradi-tional procedures and fat transfer need not beexclusive of one another. Two ideologies canbe embraced: volume enhancement for volumedepletion and lifting procedures for gravitationaldescent. Judicious use of fat grafting with selectlifting procedures can constitute a potent mixturefor correcting specific flaws of aging. Combiningprocedures can also diminish the risk of morbidity.With ongoing clinical experience, surgeons willbegin to perceive the role that volume enhance-ment can play in the armamentarium of facialrejuvenation.
ANATOMY
As the face matures, soft tissue loss is accentu-ated by the presence of facial retaining ligaments
, and cheek, performed in combination with face-lift,sy of Robert Glasgold, MD. Reprinted with permission

Fig. 3. The anterior cheek separating with a lineardepression. (From Lam SM, Glasgold MJ, Glasgold RA.Complementary fat grafting. Philadelphia: LippincottWilliams & Wilkins, 2007; with permission.)
Rabach et al224
that create unfavorable shadows. The anatomy forfat grafting does not relate so much to an intimateknowledge of specific underlying anatomic struc-tures but rather to understanding the hills and val-leys across the surface of the face that can betransformed into a more uniformly convexity freeof unwanted depressions.7
The easiest way to categorize the face foranatomic understanding is into thirds: the upperthird comprises the brow and temple area; themid-dle third comprises the cheek andmidface; and thelower third comprises the prejowl, jowl, and lateralmandible. This systematic approach provides a for-mula for specific volume enhancement based oneach individual anatomic territory.Rather thandelveinto the esoteric minutiae related to each anatomiczone, the clinical significance of each area isemphasized with attention to the clinically relevantpearls to guide the optimal surgical strategy.The middle third of the face is perhaps the most
important area for facial rejuvenation with autolo-gous fat and is anatomically the most complex interms of fully understanding each subunit. By ourdefinition, the middle facial third includes the lowereyelid, malar, and submalar area. A youthful face ischaracterized by a confluence of the lower eyelidand cheek regions, which become separated intovisually distinct regions with the aging process.With aging, the orbital rim becomes a separate en-tity from the cheek because of orbital fat bulgingsuperiorly and the cheek fat receding, which re-veals the bony orbital rim.3,8 The voluminouslateral cheek mound of youth dissipates to un-cover a smaller, flatter contour of the malar bonyeminence that lacks any notable soft tissuecoverage. The anterior cheek begins to separate,often with a linear depression that courses fromthe nasojugal depression down inferolaterally tothe buccal recess, which corresponds with theligamentous attachment known as the malarseptum (Fig. 3).9 The buccal region can showmarked atrophy and should be reconstituted alongwith the discussed anterior and lateral malar re-gions to achieve better confluence and to avoidexaggeration of buccal hollowing following malaraugmentation. As an extension of the midface,the nasolabial fold should be deemed part of mid-facial volume enhancement.
PREOPERATIVE PLANNING ANDPREPARATION
The facial fat transfer consultation is differentthan the discussion of lifting style procedures. Inorder to have a rewarding consultation, thesurgeon and patient must be in concordance.Thus, it is imperative to encourage review of older
photographs as an instrument to discuss restora-tion of youth because a patient may not initiallyentirely understand the benefits of autologousfat. Reviewing each decade of change andshowing the gradual dissipation of soft tissue vol-ume as seen in prior photographs, a patient canbegin to truly appreciate the aesthetic objectives.7
In addition, showing before-and-after photo-graphs of other patients who have similar anatomyand who have benefited from autologous facialfat transfer can also be illuminating to a prospec-tive patient. In addition, after establishing realisticaesthetic objectives, the surgeon must ensurethat the patient fully comprehends the benefitsand limitations of the procedure.
PROCEDURAL APPROACHMarking the Recipient Sites
The patient should be in an upright position so thatall the folds and depressions can be easily visual-ized. Rather than a standard gentian violet markingpen, a permanent marker is advocated owing tothe ease of removing the marks shortly after theprocedure is completed. The planned areas to beaugmented with fat are outlined. Often this in-cludes the temple, superior and inferior orbitalrim, anterior and lateral cheek, buccal hollow, pre-canine fossa, nasolabial groove, prejowl sulcus,and anterior chin (Fig. 4).

Fig. 4. Theplannedareas tobeaugmentedwith fat areoutlined. (From Lam SM, Glasgold MJ, Glasgold RA.Complementary fat grafting. Philadelphia: LippincottWilliams & Wilkins, 2007; with permission.)
Midface Fat Sculpting 225
Selection of Donor Site
Donor-site selection is based on where there isavailable fat for harvesting and on fat viability.10
It also depends on the level of anesthesia andthe ease of harvesting relative to patient posi-tioning. Asking the individual where the mostabundant adipose reserves are located is theeasiest method for selecting the favored donorsite for fat harvesting. Although men typically carrytheir extra fat in the truncal distribution, women’sfat storage can be either truncal or extremity domi-nant. The lower abdomen serves as a good sourcein both men and women and is a site easily ac-cessed without patient repositioning. When evalu-ating the lower abdomen as a potential donor site,patients should be examined to rule out the pres-ence of abdominal hernias. In women the outerthigh often provides an excellent and abundantsource of fat; alternatively the inner thigh can beused, which offers the benefit of not requiring in-traoperative repositioning. In men, the hip is agood alternative for fat harvest but requires intrao-perative patient repositioning.
Anesthesia and General Considerations
Fat graftingcanbeundertakenwith almost any levelof anesthesia, from straight local anesthesia to
general anesthesia. Intravenous conscious seda-tion is our preferred anesthesia, because it providesthe best balance of patient comfort and sedation,and facilitates intraoperative patient repositioningasnecessary. In instancesof small-volumesecond-ary fat transfers, the procedure is generally per-formed with an oral benzodiazepine and localanesthetic. The patient’s donor and recipient sitesare prepared in a sterile fashion using povidone-iodine solution and sterile drapes. If other concur-rent procedures are being performed, facial fattransfer shouldbeperformed first because, theoret-ically, the longer the tissue is outside thepatient, theless viable the fat graft becomes.
Donor-site Harvesting
The donor site is anesthetized once the patientachieves an appropriate level of sedation. Aninjection of 20 mL of 0.25% lidocaine with1:400,000 epinephrine is infiltrated with a 17.8-mm(7-inch) 22-gauge spinal needle placing half in thesuperficial aspect of the fat pad (the immediate sub-cutaneous plane) and the other half in the deepaspect of the fat pad (above the fascia in the deepsubcutaneous plane). The 20-mL mixture of anes-thetic solution can be constituted by mixing 15 mLof normal saline with 5 mL of 1% lidocaine with1:100,000 epinephrine. For individuals who are un-der lighter sedation or straight local anesthesia, a50:50 mix of 10 mL of normal saline and 10 mL of1% lidocaine with 1:100,000 epinephrine is usedinstead. A total of 20 mL of anesthetic mixture canbe used for the entire lower abdomen, whereas 20mL per extremity donor site is preferred.
After an appropriate time for anesthesia haselapsed, a 16-gauge Nokor� needle is used tocreate a stab incision through which the harvestingcannula can be inserted. Fat harvesting is under-taken with a blunt bullet-tip cannula (Tulip MedicalInc, San Diego, CA) attached to a Luer-Lok� 10-mL syringe. Harvesting is performed with handsuction, retracting the plunger with approximately2 mL of negative pressure to minimize trauma tothe adipocytes: a retaining device, such as a John-nie Lok� (Tulip Medical Inc) is useful for maintain-ing negative pressure and reduces unnecessaryforearm strain. As the cannula traverses the fatpad, dimpling of the overlying skin, which indi-cates being too superficial, should not be seen.Harvesting should be focused on getting fat fromthe mid to deeper levels of the fat pad. Thenondominant hand can be used to stabilize thefat pad but should not pinch or tent the skin, whichcan lead to uneven fat harvesting. In general, sur-geons should ensure that the same area of the fatpad is not being over harvested. After the cannula

Rabach et al226
is passed back and forth in a prescribed area, thecannula should be retracted back almost to theentry site before redirecting the cannula into afresh adjacent site. This maneuver ensures thatthe cannula does not remain in the same harvest-ing site, thereby allowing uniform harvestingacross the donor site and preventing iatrogeniccontour irregularities. Estimation of the amount offat needed for harvest should be based on theassumption that about half of the collected volumewill be fat, with the remainder consisting of blood,lysed fat cells, and lidocaine, which will be sepa-rated out during fat purification.
Fat Processing
After the fat has been harvested into the 10-mLLuer-Lok� syringes, the fat is prepared by centrifu-gation or by Puregraft� (Puregraft, San Diego, Ca).Fat processing is performed on a sterile field.Although the centrifuge is off the sterile field, sterilesleeves, within which the 10-mL syringes sit, areused to maintain sterility. A dedicated plug andcap (TulipMedical Inc)must beattached toeachsy-ringe to avoid spillage of contents during the centri-fugationprocess.Manycentrifugemodelsexist thatcan accommodate sterile sleeves or insertable ro-tary trays to maintain the sterility of the syringes.The syringes are inserted into the centrifuge in abalanced distribution and spun at approximately3000 revolutions per minute for 3 minutes. Onremoval, the supernatant (on the non–Luer-Lok�side) containing the lysed fatty acids is poured offfirst into a gauze or waste basin. Only after thesupranatant is pouredoff should thebloody infrana-tant be drained from the Luer-Lok� side. Inadver-tently draining the infranatant first predisposes thecolumn of fat to slide out of the other side of the sy-ringewhenpouringoff thesupranatant. Thesyringe,which now contains only a column of purified fat, isplaced into a test tube rack or cup so that it standsupright. A noncut 4 � 4 cotton gauze or neuropad-die is inserted into the syringe in contact with the fatin order to wick away the excess supranatant for aperiod of 5 to 10minutes. Thecontents fromseveral10-mLsyringesare then transferred toanempty20-mL syringe from the open non-Luer-Lok_ to theopen Luer-Lokside. The plunger is then insertedinto the back of the 20-mL syringe.Puregraft� is a membrane filtration system for
processing fat developed by Cytori therapeuticsas part of the technology for isolating adipose-derived stem cells. Puregraft� uses dual filtrationto purify fat. After fat is removed using the processearlier, the Puregraft� system (50-mL or 250-mLbags) is set up and fat is injected into the fat portof the Puregraft� bag. Lactated Ringer solution
is infiltrated into the bag (2 times the volume offat), the Puregraft� bag is agitated for a specifiedamount of time, placed flat for 1 minute, and thenthe wash fluid is drained through the drain port.This process is performed 2 times until fat is puri-fied of free lipids and other contaminants. Purifiedfat is then removed with a 20-mL Luer-Lok syringethrough the tissue port for reinjection.Regardless of the chosen processing technique,
the fat is then transferred from the 20-mL Luer-Loksyringe, using a Luer-Lok hub, into individual1-mL Luer-Lok syringes. Fat injections are per-formed using the 1-mL syringes attached to a0.9-mm or 1.2-mm blunt spoon-tip cannula (TulipMedical Inc).
Injection Techniques
In order to increase the likelihoodof fat survival, onlysmall parcels of fat (0.03–0.1 mL) are infiltrated perpass of the cannula across multiple tissue planes.The 3 tissue planes (referred to later) are deep,mid-dle, and superficial, corresponding respectivelywith a supraperiosteal plane, a midfascial to deepsubcutaneous plane, and a superficial subcutane-ousplane.Although these arenot distinct visualizedplanes, their importance is for guiding fatplacementin such away that fat survival can bemaximized andcontour problems minimized.The amount of fat injected per pass of the can-
nula varies from 0.03 to 0.1 mL depending on thearea treated. There are generally 4 major sites ofentry for the cannula, referred to earlier as entrysites A, B, C, and D. Additional entry sites shouldbe used as needed to address the desired areasof augmentation. Entry site A is located at the mid-cheek approximately at the base of the malarseptal depression. Entry site B resides about2 cm lateral to the lateral canthus, C is situatedimmediately behind the prejowl sulcus at the ante-rior border of the jowl, and D is located just abovethe brow to address the superior orbital rim(Fig. 5). Each entry site is made with a standard20-gauge needle through which the blunt infiltra-tion cannula can be inserted.Before fat infiltration, the entry and recipient
sites need to be anesthetized with 1% lidocainewith 1:100,000 epinephrine. The entry sites andfield blocks are done with a 30-gauge and 27-gauge needle respectively. The recipient sites arealso infiltrated diffusely with the same anestheticusing a blunt infiltration cannula. Use of the sameblunt infiltration cannula for fat infiltration for localanesthetic can minimize the likelihood of ecchy-mosis. In general, 5 to 10 mL of lidocaine are suf-ficient to achieve adequate anesthesia each sideof the face.

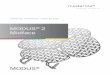
Fig. 5. Entry site A is located at the midcheek approx-imately at the base of the malar septal depression. En-try site B resides about 2 cm lateral to the lateralcanthus, C is situated immediately behind the prejowlsulcus at the anterior border of the jowl, and D islocated just above the brow to address the superiororbital rim. (From Glasgold RA, Glasgold MJ, LamSA. In: Papel I, editor. Facial plastic and reconstructivesurgery, 4th edition. New York: Thieme; in press.)
Midface Fat Sculpting 227
Volume loss in the midface results in visiblebreakpoints along the malar septum and betweenthe lower lid and cheek, imparting an aged andtired appearance. Often, the midface is the mostimportant region of the face to augment with fat.Reestablishing a uniform and seamless contourbetween the lower eyelid and cheek should bethe principal objective in many cases. As previ-ously mentioned, although infiltration of fat intothe canine fossa and nasolabial fold is unlikely toefface a deep nasolabial fold, it is important forthe purpose of creating a better transition betweenthe newly augmented cheek and the upper lip.9
The inferior orbital rim is one of the most difficultareas of the face to enhance with fat and consti-tutes a region where the most complications arise.Injection of too large a fat bolus (>0.03–0.05mL percannula pass) or placement of fat too superficiallyincreases the chance of a noticeable irregularitypostoperatively. The most important change intechnique, which has reduced complicationsdramatically, is an inferiorly based entry site so
the cannula passes perpendicularly to the inferiororbital rim. This maneuver should be performedwith the index finger of the surgeon’s nondominanthand placed on the superior aspect of the inferiororbital rim to protect the globe. As the surgeon be-gins incorporating fat transfer, it is recommendedthat a conservative amount of fat be placed alongthe inferior orbital rim (a total of 2 mL per side)in the immediately supraperiosteal plane so asto minimize contour problems. As surgeons gainexperience with the technique they will find thatlarger volumes of fat can be used with additionalplacement in a more superficial plane to allow foroptimal results, particularly in the most volume-deficient patients. The lateral and anterior cheeksare easy areas to augment with fat, allowing moresuperficial passage of the cannula with the moregenerousamount of 0.1mLperpasswithout riskingcontour irregularities. The skeletonized lateralcheek should be augmented to restore a youthful,full, rounded contour that blends well with a fullanterior cheek. The anterior cheek is typicallydivided by a linear depression running from thesuperomedial nasojugal groove to the inferolateralbuccal region. Placement of fat into the anteriorcheek should principally be situated into the great-est areas of tissue loss: the depression at themalarseptum and the region inferomedial to the malarseptum. Passage of the cannula to reach the ante-rior cheek can be made from a lateral cheek entrysite, and the cannula often must be forcefullypushed through the fibrousmalar septum tobreachit. At times, the malar septum does not pose muchresistance and can easily be traversed. Patientsshould be evaluated for the presence of a malarbag, which appears as a protuberance at the junc-tion of the anterior and lateral cheek lying just lateralto the upper portion of the malar septum. Whenpresent, surgeons should attempt to avoid place-ment of excessive fat under the already prominentmalar bag. Gentle contouring around the malarbag can help soften the appearance of the malarprotuberance while at the same time rebuildingthe lost volume of the cheek. If patients note a his-tory of fluctuating, cyclical edema of themalar bag,placement of fat immediately below this structuremay only worsen the condition and lead to a pro-tracted swelling in this area for several months. Inthin patients, the buccal and submalar regions areoften hollow and can tolerate a generous amountof fat with minimal concern of contour irregularity.Placement of fat into the subcutaneous tissue andmore deeply softens a gaunt appearance and pro-vides a better transition between the malar andsubmalar regions. In addition, the canine fossaand the nasolabial fold are augmented with fat,not with the expectation of effacement of the

Rabach et al228
fold but again to achieve an improved transition be-tween the newly augmented anterior cheek and theupper lip. A generous amount of fat can be placedinto the canine fossa (the triangular depression cir-cumscribed by the nasal alamedially and the upperextent of the nasolabial fold laterally) deeply into thesupraperiosteal plane to improve the hollowness inthis area. The entire nasolabial fold, including thecanine fossa, can then be augmented from aperpendicular direction into amore superficial sub-cutaneous plane.
POTENTIAL COMPLICATIONS ANDMANAGEMENT
The complications that arise after fat grafting aremore distinctive than those that arise after tradi-tional lifting procedures. Injuries to nerves orvascular structures are extremely rare and arebeyond the scope of this article. A classificationof complications following fat grafting, includinglumps, bulges, overcorrection, under-correction,and entry-site divot, is presented here.
Lumps
Lumps are small, discrete areas of excessive fat,and are most likely to occur in the periorbital regionbecause of the thin soft tissue covering in theregion. Technically it is caused by either too largea bolus of fat with a single pass or too muchfat placed in one spot, instead of appropriatelydispersing the small parcels throughout the region.Conservative placement of fat in the periorbital re-gions is an important step in avoiding this problem.When a lump does occur, treatment begins withsteroid injections into the area of concern. If thisfails to correct the problem, and there appears tobe a discrete lump of fat, directly excising this canalleviate the contour deformity. If this proves inef-fective the definitive remedy is excision of thelump through a discrete incision situated alongthe inferior orbital rim at the junction of the thinlower lid skin and the thicker cheek skin (Fig. 6).
Bulges
A bulge is a wide contour irregularity, character-ized by palpable persistent edema or thickening.A bulge generally manifests as an oval-shapedelevation with palpable induration oriented parallelto the inferior orbital rim.Injection with conservative amounts of triam-
cinolone acetonide in increasing strengths from5mg/mL to 40 mg/mL repeated over 1 to 2 monthshave been shown to be beneficial in most circum-stances. In our experience, direct liposuction ofthese areas has not been successful.
Overcorrection
Overcorrection is a difficult condition to correctand should be avoided at all cost. As previouslydiscussed, a conservative strategy for autologousfat transfer should be instituted to prevent thisproblem from arising. It is common in the earlypostoperative period for patients to be concernedthat too much fat was placed. Patients areinformed of significant tissue edema and thustime must pass for resorption of nonviable adipo-cytes before results can truly be appreciated. Forthis reason we recommend waiting 6 monthsbefore considering any surgical intervention toaddress overcorrection. Correction of this entityinvolves microliposuction of the areas perceivedto be overcorrected using an 18-gauge Klein-Capistrano microliposuction cannula in a cross-hatched pattern.
Undercorrection
Undercorrection is the best complication toencounter, because it is the most easily correct-able condition. Because of the variable survivalof transferred adipocytes, we counsel all patientspreoperatively of the possible need for a touch-up procedure to achieve the desired end point.Additional fat harvesting and infiltration canbe accomplished quickly and without difficultyunder local anesthesia or limited intravenoussedation.
Entry-site Divot
Tethering or divoting at the entry site is a rareoccurrence and usually manifests as a dimple atthe entry site during facial animation. This compli-cation can easily be rectified by limited subcisionusing a Nokor� or standard needle across thescar band.
POSTPROCEDURAL CARE
At the end of the procedure, the patient has no su-tures, bandages, or drains of any kind unless aconcurrent lifting procedure was performed thatrequires use of these ancillary measures. Thepatient is discharged after appropriate postanes-thesia observance. Although some surgeons whoperform fat transfer do not advocate immediatepostoperative icing of transplanted regions giventhe risk of reducing fat-cell viability, we think thatthere is no compromise to the aesthetic resultand recovery is expedited. We advocate intermit-tent icing for the first 48 to 72 hours postopera-tively, which can be continued if the patientdesires. Head elevation also reduces the extentof postoperative edema, but a restful night’s sleep

Fig. 6. (A) Preoperative view. (B) Excision of the lump through a discrete incision along the inferior orbital rim atthe junction of the thin lower lid skin and the thicker cheek skin. (C) Postoperative view. (From Lam SM, GlasgoldMJ, Glasgold RA. Complementary fat grafting. Philadelphia: Lippincott Williams & Wilkins, 2007; with permission.)
Midface Fat Sculpting 229
is of paramount importance and thus this isonly stressed for the first several nights after sur-gery. Although heavy exercise, especially withincreased intra-abdominal pressure and bendingover, should be avoided, a light isometric weight-lifting regimen with one-half to one-third the typicalweight and lighter cardiovascular exercise can be
undertaken, typically by the fourth or fifth postop-erative day. In addition, salt intake should belimited because this assists in the resolution ofpostoperative edema.
Although postoperative care is simple andstraightforward, management of postoperativeexpectations may be more involved. Patients

Rabach et al230
may perceive that their faces appear too inflatedfor their liking in the first several postoperativeweeks and regard this outcome as an unintendedresult. Although the expected course of recoverywill have been explained in detail preoperatively,constant reassurance must be offered, with pa-tients returning as often as necessary for en-couragement and counsel. In addition, theecchymosis and edema are often more pro-nounced in conjunction with a brow or face-liftand can be a social and professional encum-brance for a longer period of time. In addition,the fat harvesting sites are generally sore for thefirst several days to weeks after surgery.
CLINICAL RESULTS IN THE LITERATURE ANDEVIDENCE
Improving the predictability and reliability of autol-ogous fat grafting has been one of the primary in-terests. We assessed long-term (>1 year) volumechanges after autologous fat grafting to the mid-face using three-dimensional photography (Vec-tra; Canfield) and found our average take to be32% with an average injection volume of 10 mLin 1 side of the midface. The range of take was10% to 88%.11 With an average take of only about3 mL and volume that was highly unpredictableonly 20% of the patients thought that they neededa second procedure. This finding supports theidea that smaller volumes over larger areas withtransitions into surrounding areas are desirableand produces an overall result that is better thanusing any individual site. It also made us reflecton our understanding of end points. Based onthe aging theory of shadow patterns, the youthfuleffect is achieved by adding enough volume to ahollow to fill it and create a highlight, which impliesthat for any given hollow on the face there is a largerange of volumes that will fill it. For example, fillinga midface depression may be acceptable with vol-ume takes of between 2 and 5 mL.Hoping to improve the take of our autologous fat
grafting we assessed different techniques of pro-cessing the fat.12 Puregraft� is a membrane filtra-tion system for processing fat developed by CytoriTherapeutics as part of the technology for isolatingadipose-derived stem cells. We studied long-termtake of midface fat transfers using this systemand found an average take of 49% at 7 months.This percentage is a significant improvementcompared with centrifuge processing. The Pure-graft� processed fat has less free lipid contentand contaminant blood and a higher volume ofpotentially viable fat.13
We also studied the effect of harvesting cannuladesign on the fat graft. We originally used a 4-mm
keel–type cannula for harvesting. Recently, cheesegrater–type cannulas were introduced. Using thePuregraft� system we were able to compare thefat obtained with each cannula type. The yield ofinjectable potentially viable fat from the cheesegrater cannulas was significantly lower than fromthe keel, with a greater amount of free lipid content.For this reason we currently only recommend keel-type cannulas for harvesting.
SUMMARY
There is currently a major paradigm shift fromexcision-based surgery to strictly volume en-hancement. As the perfect facial filler has not yetbeen found, development of synthetic facial inject-ables continues to advance at a remarkable pace.Just a few years ago, bovine collagen was the onlyUS Food and Drug Administration (FDA)–approvedsynthetic filler. As the FDA proceeds with theapproval process there are many choices. Eachtype of filler carries a specific characteristic thatmakes it more suited for a certain clinical applica-tion. The continuing changes in facial fillers offerthe possibility of volume augmentation procedureswith less downtime and without the need for har-vesting fat.A combined approach requiring judicious selec-
tion of lifting procedures and fat grafting tailoredto each individual is advocated.14 Whatever theoutcome, it seems that fat grafting and facialvolume enhancement represent the present andfuture of facial rejuvenation. We predict thatvolume enhancement will continue to play an in-creasing role as both a complementary proce-dure and as a stand-alone procedure in facialrejuvenation.
REFERENCES
1. Lam SM. A new paradigm for the aging face. Facial
Plast Surg Clin North Am 2010;18(1):1–6.
2. Lam SM, Glasgold RA, Glasgold MJ. Fat harvesting
techniques for facial fat transfer. Facial Plast Surg
2010;26(5):356–61.
3. Glasgold MJ, Lam SM, Glasgold RA. Complemen-
tary Fat Grafting. In: Papel I, editor. Facial Plastic
and Reconstructive Surgery. 3rd edition. New York:
Thieme; 2008.
4. Lam SM. Fat grafting: an alternative or adjunct to
facelift surgery? Facial Plast Surg Clin North Am
2013;21(2):253–64.
5. Coleman SR. Structural fat grafts: the ideal filler?
Clin Plast Surg 2001;28(1):111–9.
6. Lam S, Glasgold M, Glasgold R. Complementary Fat
Grafting. Philadelphia: Lippincott, Williams & Wil-
kins; 2007.

Midface Fat Sculpting 231
7. Mendelson B, Wong CH. Changes in the facial skel-
eton with aging: implications and clinical applica-
tions in facial rejuvenation. Aesthetic Plast Surg
2012;36(4):753–60.
8. Massry GG, Azizzadeh B. Periorbital fat grafting.
Facial Plast Surg 2013;29(1):46–57.
9. Mendelson BC, Muzaffar AR, Adams WP Jr. Surgical
anatomy of the midcheek and malar mounds. Plast
Reconstr Surg 2002;110(3):885–96 [discussion:
897–911].
10. Geissler PJ, Davis K, Roostaeian J, et al. Improving
fat transfer viability: the role of aging, body mass in-
dex, and harvest site. Plast Reconstr Surg 2014;
134(2):227–32.
11. Meier JD,GlasgoldRA,GlasgoldMJ. 3Dphotography
in the objective analysis of volume augmentation
including fat augmentation and dermal fillers. Facial
Plast Surg Clin North Am 2011;19(4):725–35, ix.
12. Botti G, Pascali M, Botti C, et al. A clinical trial
in facial fat grafting: filtered and washed versus
centrifuged fat. Plast Reconstr Surg 2011;127(6):
2464–73.
13. Gerth DJ, King B, Rabach L, et al. Long-term volu-
metric retention of autologous fat grafting processed
with closed-membrane filtration. Aesthet Surg J
2014;34(7):985–94.
14. Lamb J. Volume rejuvenation of the face. Mo Med
2010;107(3):198–202.








![[hal-00945905, v2] Crowd Sculpting: A space-time sculpting](https://img.pdfslide.net/doc/110x75/61d00833c69c8e549e339118/hal-00945905-v2-crowd-sculpting-a-space-time-sculpting-.jpg)