Embed Size (px)
Citation preview

Mobility Training for theYoung AthleteToby Brooks, PhD, ATC, CSCS1 and Eric Cressey, MA, CSCS2
1Texas Tech University Health Sciences Center, Amarillo, Texas; and 2Cressey Performance, Hudson, Massachusetts
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are providedin the HTML and PDF versions of this article on the journal’s Web site (http://journals.lww.com/nsca-scj).
A B S T R A C T
CONTEMPORARY CORRECTIVE
EXERCISE TECHNIQUES EMPHA-
SIZING THE IMPORTANCE OF
ADEQUATE MOVEMENT ABILITY
AND SOFT TISSUE EXTENSIBILITY
ARE NOW RELATIVELY COMMON
IN MOST STRENGTH AND CONDI-
TIONING PROGRAMS. DESPITE
DEMONSTRATED POTENTIAL FOR
PERFORMANCE DEFICIT, PREAC-
TIVITY FLEXIBILITY TRAINING HAS
BEEN EMPLOYED ANDCONTINUES
TO BE USED BY MANY SPORT
COACHES. PARTICULARLY, IN THE
DEVELOPING ATHLETE, THE DIF-
FERENCES BETWEEN MOBILITY
AND FLEXIBILITY TRAINING ARE
SIGNIFICANT. THE PURPOSE OF
THIS ARTICLE IS TO DEFINE
MOBILITY AND DISCUSS THE
PRACTICAL IMPLICATIONS OF
INCORPORATING MOBILITY
MOVEMENTS, DRILLS, AND EXER-
CISES INTO PROGRAMMING FOR
YOUNG ATHLETES TO REDUCE
THE RISKOF INJURY ANDMAXIMIZE
PERFORMANCE.
INTRODUCTION
In recent years, mobility trainingand corrective exercise techniquesemphasizing the importance of
adequate soft tissue extensibility havebecome increasingly popular in thefield of strength and conditioning (3).More specifically, the application ofmobility concepts to young athletesin the prevention and treatment of
movement impairment syndromes hasalso grown increasingly popular. Manystrength and conditioning professionalshave recognized the importance ofappropriate functional movement abilityin athletic enhancement programmingand have altered more traditional pro-gramming to accommodate the needs oftheir athletes.
Conversely, flexibility training has oftenbeen loosely defined in a variety of ways,including in reference to the actuallength of muscle and soft tissue (i.e.,“inflexible” hamstrings), the amount ofmovement possible at a joint or seriesof joints (i.e., inflexible ankles), or theposition the athlete is capable of achiev-ing during an athletic or conditioningmovement (i.e., “too inflexible to performa deep squat”). Most commonly, flexibil-ity refers to the absolute range of motionpossible within a joint or series of jointsand may be either static or dynamic (2).
Although flexibility certainly influencessystemic movement, the construct offlexibility does not sufficiently addressall aspects of movement-specific func-tional activity. For example, flexibilityis usually assessed in a non–weight-bearing position, whereas the majorityof athletic movements occur with theathlete in standing or otherwise in anupright position. Because of the rela-tively isolated nature of flexibility exam-ination, the influence of systemicrestrictions such as fascia may not bereadily apparent. As a result, flexibilityis usually considered a clinical constructwith respect to a joint-specific defi-ciency or excess in movement.
Conversely, mobility is considered amore functional construct describing
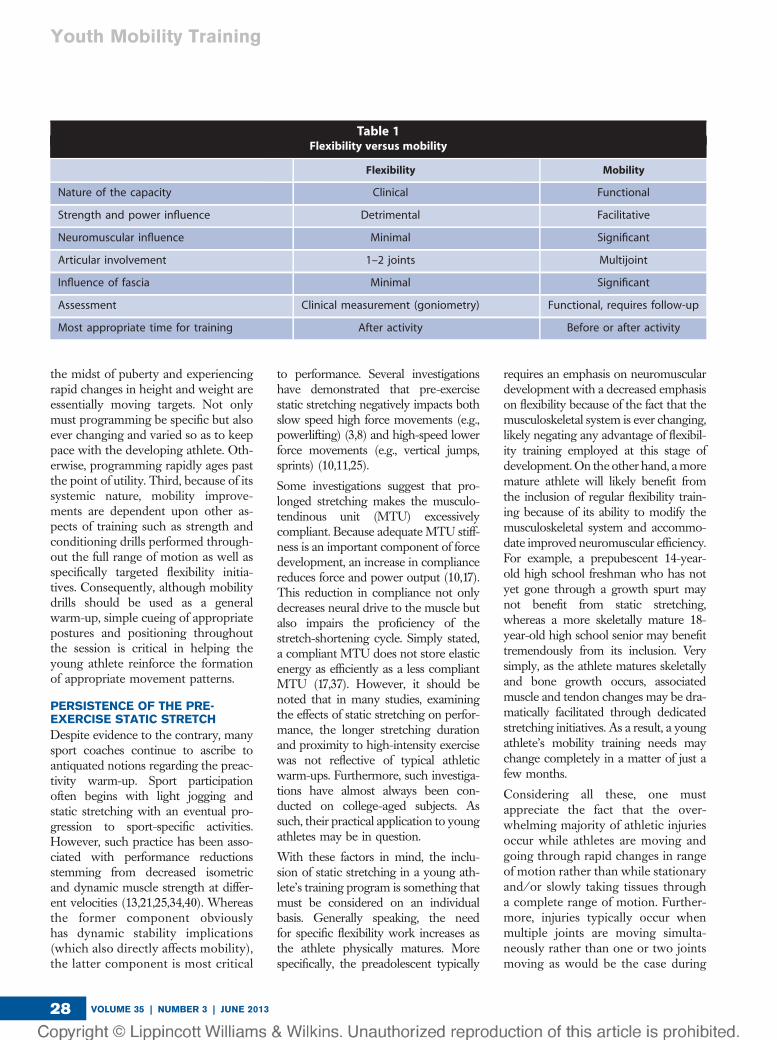
the athlete’s ability (or inability) toreach an intended posture or position.Although flexibility assessment gener-ally involves only 1 or 2 joints at a time,mobility assessment is typically multi-joint and as a result more systemic innature. Mobility is more global inscope and includes the athlete’s abilityto function and reach desired positionsduring activity and is heavily depen-dent upon stability and proper coordi-nation of multiple joints functioningsimultaneously. Although mobility isrelatively easy to assess in a generalsense, follow-up screening is typicallynecessary to identify the source of anyidentified restriction or inhibition.Table 1 further depicts the principaldifferences between the constructs offlexibility and mobility.
In appreciating these differences, 3critical distinctions emerge that shouldserve as the foundation for any efforttoward mobility training in the adoles-cent and high school athlete. First, nosingle method of mobility training iseffective for all athletes. The vast dis-parities and unique differences inyoung athletes make nonspecific pro-gramming impractical and largely inef-fective. As such, programming must betailored, at least to some degree, to beof maximum benefit to the developingathlete. Second, adolescent athletes in
KEY WORDS :
mobility; flexibility; training; youthathlete
Copyright � National Strength and Conditioning Association Strength and Conditioning Journal | www.nsca-scj.com 27
the midst of puberty and experiencingrapid changes in height and weight areessentially moving targets. Not onlymust programming be specific but alsoever changing and varied so as to keeppace with the developing athlete. Oth-erwise, programming rapidly ages pastthe point of utility. Third, because of itssystemic nature, mobility improve-ments are dependent upon other as-pects of training such as strength andconditioning drills performed through-out the full range of motion as well asspecifically targeted flexibility initia-tives. Consequently, although mobilitydrills should be used as a generalwarm-up, simple cueing of appropriatepostures and positioning throughoutthe session is critical in helping theyoung athlete reinforce the formationof appropriate movement patterns.
PERSISTENCE OF THE PRE-EXERCISE STATIC STRETCH
Despite evidence to the contrary, manysport coaches continue to ascribe toantiquated notions regarding the preac-tivity warm-up. Sport participationoften begins with light jogging andstatic stretching with an eventual pro-gression to sport-specific activities.However, such practice has been asso-ciated with performance reductionsstemming from decreased isometricand dynamic muscle strength at differ-ent velocities (13,21,25,34,40). Whereasthe former component obviouslyhas dynamic stability implications(which also directly affects mobility),the latter component is most critical
to performance. Several investigationshave demonstrated that pre-exercisestatic stretching negatively impacts bothslow speed high force movements (e.g.,powerlifting) (3,8) and high-speed lowerforce movements (e.g., vertical jumps,sprints) (10,11,25).
Some investigations suggest that pro-longed stretching makes the musculo-tendinous unit (MTU) excessivelycompliant. Because adequate MTU stiff-ness is an important component of forcedevelopment, an increase in compliancereduces force and power output (10,17).This reduction in compliance not onlydecreases neural drive to the muscle butalso impairs the proficiency of thestretch-shortening cycle. Simply stated,a compliant MTU does not store elasticenergy as efficiently as a less compliantMTU (17,37). However, it should benoted that in many studies, examiningthe effects of static stretching on perfor-mance, the longer stretching durationand proximity to high-intensity exercisewas not reflective of typical athleticwarm-ups. Furthermore, such investiga-tions have almost always been con-ducted on college-aged subjects. Assuch, their practical application to youngathletes may be in question.
With these factors in mind, the inclu-sion of static stretching in a young ath-lete’s training program is something thatmust be considered on an individualbasis. Generally speaking, the needfor specific flexibility work increases asthe athlete physically matures. Morespecifically, the preadolescent typically
requires an emphasis on neuromusculardevelopment with a decreased emphasison flexibility because of the fact that themusculoskeletal system is ever changing,likely negating any advantage of flexibil-ity training employed at this stage ofdevelopment. On the other hand, amoremature athlete will likely benefit fromthe inclusion of regular flexibility train-ing because of its ability to modify themusculoskeletal system and accommo-date improved neuromuscular efficiency.For example, a prepubescent 14-year-old high school freshman who has notyet gone through a growth spurt maynot benefit from static stretching,whereas a more skeletally mature 18-year-old high school senior may benefittremendously from its inclusion. Verysimply, as the athlete matures skeletallyand bone growth occurs, associatedmuscle and tendon changes may be dra-matically facilitated through dedicatedstretching initiatives. As a result, a youngathlete’s mobility training needs maychange completely in a matter of just afew months.
Considering all these, one mustappreciate the fact that the over-whelming majority of athletic injuriesoccur while athletes are moving andgoing through rapid changes in rangeof motion rather than while stationaryand/or slowly taking tissues througha complete range of motion. Further-more, injuries typically occur whenmultiple joints are moving simulta-neously rather than one or two jointsmoving as would be the case during
Table 1Flexibility versus mobility
Flexibility Mobility
Nature of the capacity Clinical Functional
Strength and power influence Detrimental Facilitative
Neuromuscular influence Minimal Significant
Articular involvement 1–2 joints Multijoint
Influence of fascia Minimal Significant
Assessment Clinical measurement (goniometry) Functional, requires follow-up
Most appropriate time for training After activity Before or after activity
Youth Mobility Training
VOLUME 35 | NUMBER 3 | JUNE 201328

most static stretches. Moreover, inju-ries generally occur when athletes arein weight bearing rather than seated,supine, or prone (although a compre-hensive mobility program appreciatesthat most upper-body movements areopen chain in nature).
Accordingly, with few exceptions, anoptimal pre-exercise warm-up shouldfocus on weight-bearing multijointmovements that take athletes throughfull range of motion in a progressivelymore dynamic context. With the youngathlete, such times are excellent oppor-tunities for the acquisition and refine-ment of gross motor skills, as fatigue isnot a factor and systemic movementsshould predominate. As a result, thewarm-up can serve as the most oppor-tune time to improve and ingrainmobility (18). When selected appropri-ately, mobility drills, frequently referredto as “dynamic flexibility” or “dynamicstretching,” can be used to achieve all ofthese pre-exercise goals (10).
Mobility drills categorized as “generalwarm-up” effectively bridge the gapbetween the pre-exercise rest stateand specific exercise by incorporatinghigh-intensity movements through fullrange of motion. At the same time,adequate warm-up should progressfrom general to specific.
Research has shown that dynamic flex-ibility drills improve performance ina number of specific measures of per-formance including 20-m sprints (10),jumping tasks (43), and agility tests(11); increase dynamic range of motion(20); and reduce injury rates when com-pared with static stretching (20). Addi-tionally, mobility drills can help torecruit or “activate” key muscles thatmay not contribute sufficiently as primemovers or stabilizers. For example, poorgluteus maximus function has repeat-edly been associated with low back pain(14,16), whereas insufficient strengthandmotor control of the gluteus mediusand lateral hip rotators has been associ-ated with an increased risk of iliotibialband friction syndrome (27) and ante-rior knee pain (5,19). In the upper body,insufficient recruitment of the lower and
middle trapezius (7) and serratus ante-rior (9) has been implicated in scapulardysfunction leading to shoulder pain.
Additionally, mobility training beforeexercise is an effective motor learningstrategy for a young athlete. All toooften, the athlete is instructed to com-plete rehabilitation and prehabilitationwork as sessions separate from “nor-mal” training and competition. Thisgap between corrective exercise andactual performance may impede theathlete’s ability to integrate the moreefficient strategies in performance.Incorporating this corrective work inthe warm-up period may make it easierfor the athlete to more quickly applyand ingrain the new movement strate-gies in higher intensity exercise.
Last, mobility training coupled withresistance training assists the athletein developing functional stability. Thisis particularly important in the youngathlete, where insufficient stability isoftentimes confused with inadequate“flexibility.” By performing mobilitydrills before resistance training, the ath-lete first establishes range of motionand then subsequently applies stabilitywithin that range.
The need for supplemental static stretch-ing is markedly reduced once appro-priate mobility is established, and theathlete continues on a resistance trainingprogram through full range of motionwith frequent variation in exercise selec-tion and dynamic flexibility warm-ups.Simply stated, mobility maintenance ismuch easier than mobility creation. Tothat end, preparatory/warm-up, training,and flexibility sessions should be craftedwith the goal of both maintaining andimproving systemic mobility.
THE MODES OF MOBILITY INYOUNG ATHLETES
Having established that the warm-upperiod is an opportune time at whichto train mobility, it is crucial to selectdrills and other training stimuli thatprovide the most benefit in the leastamount of time. Most athletes, partic-ularly young athletes, often overlookthe importance of an adequate warm-up. As a result, warm-up is often
completed haphazardly and inatten-tively or simply skipped altogether.Accordingly, an appropriate warm-upshould be engaging for the athlete andits importance consistently reinforced.
Some young athletes may need to ded-icate extra time to some drills to effec-tively address identified limitations.Most frequently, athletes whose growthand maturation has outpaced theirpeers generally benefit the most fromadditional drills performed as separatesessions throughout the week. Whileincreased height and weight may pro-vide such athletes with a competitiveadvantage, it also likely increases thepredisposition to injury because ofintrinsic (e.g., insufficient eccentric con-trol, higher center of gravity) andextrinsic (e.g., overuse) factors (29).
Potential modes of mobility trainingfor young athletes vary considerablyand may include ground-based orstanding stimuli; open- or closed-chain movements; unilateral or bilat-eral patterns; upper-body, lower-body,or full-body movements; and isolatedor integrated skills. Although funda-mentally different, all modes still haveone goal in common: to teach theyoung athlete to move more efficiently.When performing these drills, the pointis not merely to increase core tempera-ture and circulation, but also to developand refine motor patterns that will beuseful in the training session to follow.As a result, if a young athlete performsthe prescribed drills with poor posture,then the same poor posture will mostlikely be evident once the training ses-sion (or competition) begins.
HIP FLEXION MOBILITY
It may seem counterintuitive toactively train hip flexion mobility(HFM) because so many young ath-letes spend countless hours sitting atdesks at school and at computers inthe home. However, in these seatedpositions, athletes rarely achieve themagnitude of hip flexion required dur-ing sprinting. Because this HFM isoften lacking, lumbar flexion is com-monly substituted as a means of attain-ing the required movement.
Strength and Conditioning Journal | www.nsca-scj.com 29

Effectively, in this compensated sce-nario, the athlete lacks sufficient lum-bar stability to prevent motion fromoccurring at that region (35). Addition-ally, inadequate hip flexion strengthhas been correlated with both kneeand low back pain (28,31).
Frequently, coaches often attempt toremedy this problem by simplystretching the muscles of the posteriorhip to improve range of motion; how-ever, such an approach ignores thestrong case for added strengtheningof the hip flexors in conjunction withan effective core stabilization program(and stretching of the posterior hipmusculature). By adding full range-of-motion exercises for hip flexion cou-pled with core stabilization training,this frequently observed compensatorypattern may be combated.
HIP EXTENSION MOBILITY
Just as inadequate hip flexion can leadto inefficient and potentially injuriousmovement patterns, poor hip exten-sion mobility (HEM) can be equallyproblematic, including a strong corre-lation between decreased HEM andboth anterior knee pain (31) and lowback pain (39). Exercises to addressthis deficiency and thereby preventsuch pain target hip flexor length tocreate hip extension range. Concur-rently, the addition of gluteal activation(GA) drills may be used to improvestrength in hip extension and positivelyimpact HEM.
HIP ABDUCTION MOBILITY
Hip abduction mobility (HAM),dependent upon length of the hip ad-ductors and strength of the hip abduc-tors, is an important yet commonlyoverlooked component of lowerextremity function. Limited HAM hasbeen associated with increased risk ofgroin strain (1). Whether the adductorsare, in fact, hypomobile is only oneissue of concern. The strength of theantagonist hip abductors is equallyimportant, as athletes tend to overuseadductor magnus as a hip extensor tocompensate for poor gluteus maximusand hamstring strength. Not surpris-ingly, abduction weakness is associated
with patellofemoral pain and mayresult in increased likelihood of kneevalgus collapse, a frequently observedmechanism of noncontact knee injury,especially among female athletes(15,31). In consideration of these fac-tors, a comprehensive approach toHAM should include a focus on bothadductor length and abductor strength.
HIP EXTERNAL ROTATIONMOBILITY
Hip external rotation mobility(HERM) is intimately linked with hipextension and abduction as well asGA. Hip external rotation weaknesshas been linked to patellofemoral pain(31,33). While working to improveHERM, the athlete should work inboth hip flexion and extension. Forexample, a cradle walk (Figure 1 andVideo, Supplemental Digital Content 1,http://links.lww.com/SCJ/A105) canprovide HERM in flexion, whereasa walking spiderman lunge providesHERM in extension (Figure 2 andVideo, Supplemental Digital Content 2,http://links.lww.com/SCJ/A106).
GLUTEAL ACTIVATION
Gluteus maximus actions includeabduction, external rotation, andextension. Although abduction andexternal rotation components ofmovement are important, GA drillsthat use the gluteal muscles in the sag-ittal plane to achieve terminal hipextension and some posterior pelvic
tilt are frequently overlooked. Insuffi-cient gluteus maximus function andhip extension strength has been fre-quently implicated in cases of low backand knee pain (14,16,31). The singleleg supine bridge (Figure 3 and Video,Supplemental Digital Content 3,http://links.lww.com/SCJ/A107) andother similar exercises can be helpfulin triggering GA.
HIP ADDUCTION AND INTERNALROTATION MOBILITY
Deficits of hip adduction and internalrotation are often overlooked because
Figure 1. Cradle walk.
Figure 2. Walking spiderman lunge.
Figure 3. Single leg supine bridge.
Youth Mobility Training
VOLUME 35 | NUMBER 3 | JUNE 201330

of the tremendous focus on strength-ening the hip abductors and externalrotators to prevent or rehabilitatefrom injury. However, loss of hipadduction or internal rotation mobility(HIRM) is not uncommon and canlead to a host of other related issuesif left unchecked. Such complicationshave been identified with far greaterfrequency in men than women (6).This typical increase in HIRM cansubsequently predispose the femaleathlete to an increased risk of trau-matic noncontact knee injury (mostnotably, anterior cruciate ligamentand medial collateral ligament prob-lems). Therefore, unless a female ath-lete has been specifically identified aslacking hip internal rotation and/oradduction, it is generally best to avoidexercises that increase mobility inthese planes/directions.
ANKLE MOBILITY
Ankle mobility (AM), particularly dor-siflexion, is critical to normal gait. Ath-letes require substantially moredorsiflexion range for sprinting, squat-ting, lunging, jumping, throwing, anda host of other athletic activities. Anathlete who lacks AM may substitutelumbar flexion to achieve adequate“depth,” thereby putting the spine atrisk. Specific to young athletes, limitedAM contributes to the development ofOsgood-Schlatter disease (33).
One simple way to progressivelyimprove AM and develop strengthand proprioception at the feet is tosimply perform various exercises with-out shoes (4,26). Infants typicallydevelop tremendous dexterity withthe feet in the initial years of life, a timeduring which footwear is the exceptionrather than the rule. Years later, thoseindividuals may develop planus feet,plantar fasciitis, and immobile anklesdespite the use of modern athletic foot-wear (30). Barefoot training can helpreactivate muscles long underusedbecause of the added support and pro-tection of shoes (26).
THORACIC SPINE MOBILITY
Although excessive mobility in the lum-bar spine is generally considered
problematic (core instability), adequatethoracic spine mobility (TSM) is imper-ative for both upper extremity andlumbar spine health. Limited TSMand shoulder impingement have beenassociated with chronic low back painin obese individuals (23,41). While ad-dressing TSM, chief concerns includethoracic extension and rotation, as themajority of the population uses far toomuch thoracic flexion in the course ofdaily living as a result of excessive sit-ting. With most drills in this mode,humeral horizontal abduction, externalrotation, and flexion, all of which posi-tively influence scapular positioninginto posterior tilt and retraction, shouldbe used extensively. For the young ath-lete, a drill such as the quadruped exten-sion-rotation movement (Figure 4 andVideo, Supplemental Digital Content 4,http://links.lww.com/SCJ/A108) canbe beneficial in promoting stabilitythrough the hips while promoting TSM.
SCAPULAR STABILITY
Poor periscapular muscle function isa near-universal finding in those withshoulder pain (7,9). Typically, athletespresent with poor recruitment of themiddle and lower trapezius and serratusanterior, along with shortness andinflexibility of the pectoralis minor. Col-lectively, these deficits contribute to
faulty posture, most notably, scapularprotraction. This faulty positioning isusually apparent both statically anddynamically. Scapular protraction im-pairs ideal movement at the glenohum-eral and acromioclavicular joints (32),and a simple drill such as thescapular wall slide (Figure 5 and Video,Supplemental Digital Content 5,http://links.lww.com/SCJ/A109) canbe an effective means of promot-ing dynamic scapular retraction.
CERVICAL MOBILITY
Another commonly overlooked com-ponent of upper extremity health iscervical spine mobility, which is oftremendous importance. Forwardhead posture (FHP) is significantlygreater in patients with overuse shoul-der injuries compared with healthycontrols (12). Likewise, FHP with con-current rounded shoulders increasesscapular protraction and anterior tiltduring shoulder flexion (overheadreaching) independent of the presenceof symptoms (38). Although it may beeffective to integrate various “chin tuck”drills into the warm-up for those ath-letes who present with a pronouncedFHP, successful interventions to correctFHP have often centered on addressingimpairments further down the kineticchain, including the glenohumeral joint,scapulae, and thoracic spine and simply
Figure 4. Quadruped extension-rotation. Figure 5. Scapular wall slide.
Strength and Conditioning Journal | www.nsca-scj.com 31

cueing a neutral cervical spine postureduring all training drills. In other words,athletes should look forward rather thanup when squatting, deadlifting, or per-forming mobility drills.
SHOULDER INTERNAL ROTATIONMOBILITY
Maintaining shoulder internal rota-tion mobility (SIRM) is an importantcomponent in the successful man-agement of overhead athletes suchas baseball players, swimmers, tennisplayers, and track and field throw-ers. Reinold et al. (32) noted thatin response to the eccentric stressimposed during arm deceleration,pitchers tend to lose shoulder internalrotation after a pitching outing.Although this loss can be preventedwith appropriate mobility efforts, ifleft unchecked over the course of mul-tiple outings and competitive seasons,it can ultimately lead to a host of is-sues, including glenohumeral internalrotation deficit and global shoulderpain (24).
Overhead athletes often present withsignificantly more external rotationand less internal rotation in the dom-inant shoulder than the nondominantshoulder; however, if the arc of motion(internal rotation plus external rotation)is equal bilaterally, this asymmetry maybe considered normal (42). Therefore,best practice for overhead athletesinvolves normalizing total motionbilaterally, even if the specific limits ofmotion are dissimilar. Performed cor-rectly, the side-lying sleeper stretch forinternal rotation (Figure 6 and Video,Supplemental Digital Content 6,
http://links.lww.com/SCJ/A114) isa preferred means of gaining SIRM.
SHOULDER EXTERNAL ROTATIONMOBILITY
Although shoulder external rotationmobility (SERM) is rarely a problemin overhead throwing athletes, it isa common deficit in athletes whospend long periods of time sittingand those who regularly performnumerous pressing movements(bench press, etc) with little or nopulling movements to ensure muscu-lar balance. Not surprisingly, insuffi-cient external rotation is associatedwith shoulder impingement, whereasimprovement of external rotationmobility can reduce impingementsymptoms (22,36). The “no money”drill (dynamic shoulder external rota-tion with the upper arms at the sidesand the elbows flexed to 908, move-ment into end range shoulder externalrotation before movement back to thetorso and repeating, alternating “top”hand position with each repetition)can be used either singly or witha lower extremity movement such asa skip to help promote SERM alongwith global motor control.
CONCLUSIONS
Although related, mobility and flexibil-ity are unique constructs that are bestapproached as independent abilities tobe addressed specifically. Developingmobility in the young athlete involvesmaximizing the effectiveness and effi-ciency of the warm-up through tar-geted dynamic flexibility drills andspecific positioning cues. Additionally,this affords the strength and condition-ing specialist an excellent opportunityto enhance motor learning in thedeveloping athlete. In addition, devel-oping a comprehensive and specifictraining program to improve strength,stability, and tissue quality to accountfor differences in gender, physicalmaturity, age, training experience, andsport participation is a critical skill.Although static stretching definitelyhas a place in many athletes’ programs,its overall utility is largely specific toeach individual athlete.
Conflicts of Interest and Source of Funding:The authors report no conflicts of interestand no source of funding.
Toby Brooks isan assistant pro-fessor in theDepartment ofRehabilitationSciences, TexasTech UniversityHealth SciencesCenter, Lubbock.
He also serves as director of Research andEducation for the International YouthConditioning Association.
Eric Cressey isthe president andcofounder ofCressey SportsPerformance inHudson.
REFERENCES1. Arnason A, Sigurdsson S, Gudmundsson A,
Holme I, Engebretsen L, and Bahr R. Risk
factors for injuries in football. Am J Sports
Med 31: 5S–16S, 2004.
2. Bachele T and Earle R, eds. Essentials of
Strength Training and Conditioning.
Champaign, IL: Human Kinetics, 2008.
3. Behm D, Bambury A, Cahill F, and
Power K. Effect of acute static stretching
on force, balance, reaction time, and
movement time.Med Sci Sports Exerc 36:
397–402, 2004.
4. Biscontini L. Barefoot but not footloose.
Am Fitness 26: 49–50, 2008.
5. Brindle T, Mattacola C, and McCrory J.
Electromyographic changes in the gluteus
medius during stair ascent and descent in
subjects with anterior knee pain. Knee Surg
Sports Traumatol Arthrosc 11: 244–251,
2003.
6. Brophy R, Chiaia T, Maschi R, Dodson C,
Oh L, Lyman S, Allen A, and Williams R.
The core and hip in soccer athletes
compared by gender. Int J Sports Med 30:
663–667, 2009.
7. Cools A, Witvrouw E, Declercq G,
Danneels L, and Cambier D. Scapular
muscle recruitment patterns: trapeziusFigure 6. Side-lying sleeper stretch.
Youth Mobility Training
VOLUME 35 | NUMBER 3 | JUNE 201332
muscle latency with and without
impingement symptoms. Am J Sports Med
31: 542–549, 2003.
8. Cramer J, Housh T, Johnson G, Miller J,
Coburn J, and Beck T. Acute effects of
static stretching on peak torque in women.
J Strength Cond Res 18: 236–241, 2004.
9. Diederichsen L, Nørregaard J, Dyhre-
Poulsen P, Winther A, Tufekovic G,
Bandholm T, Rasmussen L, and
Krogsgaard M. The activity pattern of
shoulder muscles in subjects with and
without subacromial impingement.
J Electromyogr Kinesiol 19: 789–799, 2009.
10. Fletcher I and Jones B. The effect of
different warm-up stretch protocols on 20
meter sprint performance in trained rugby
union players. J Strength Cond Res 18:
885–888, 2004.
11. Fletcher I and Monte-Colombo M. An
investigation into the effects of different
warm-up modalities on specific motor skills
related to soccer performance. J Strength
Cond Res 24: 2096–2101, 2010.
12. Greenfield B, Catlin P, Coats P, Green E,
McDonald J, and North C. Posture in
patients with shoulder overuse injuries and
healthy individuals. J Orthop Sports Phys
Ther 21: 287–295, 1995.
13. Haag S, Wright G, Gillette C, and
Greany J. Effects of acute static stretching
of the throwing shoulder on pitching
performance of national collegiate athletic
association division III baseball players.
J Strength Cond Res 24: 452–457, 2010.
14. Hungerford B, Gilleard W, and Hodges P.
Evidence of altered lumbopelvic muscle
recruitment in the presence of sacroiliac
joint pain. Spine 28: 1593–1600, 2003.
15. Imwalle L, Myer G, Ford K, and Hewett T.
Relationship between hip and knee kinematics
in athletic women during cutting maneuvers:
A possible link to noncontact anterior cruciate
ligament injury and prevention. J Strength
Cond Res 23: 2223–2230, 2009.
16. Kankaanpaa M, Taimela S, Laaksonen D,
Hanninen O, and Airaksinen O. Back and
hip extensor fatigability in chronic low back
pain patients and controls. Arch Phys Med
Rehabil 79: 412–417, 1998.
17. Kubo K, Kanehisa H, Kawakami Y, and
Fukunaga T. Influence of static stretching
on viscoelastic properties of human tendon
structures in vivo. J Appl Physiol 90: 520–
527, 2001.
18. Kurz T. Science of Sports Training: How to
Plan and Control Training for Peak
Performance. Island Pond, VT: Stadion, 2001.
19. Long-Rossi F and Salsich G. Pain and hip
lateral rotator muscle strength contribute to
functional status in females with
patellofemoral pain. Physiotherapy Res Int
15: 57–64, 2010.
20. Mann D and Jones M. Guidelines to the
implementation of a dynamic stretching
program. Strength Cond J 21: 53–55,
1999.
21. McBride JM, Deane R, and Nimphius S.
Effect of stretching on agonist-antagonist
muscle activity and muscle force output
during single and multiple joint isometric
contractions. Scand J Med Sci Sports 17:
54–60, 2007.
22. McClure P, Bialker J, Neff N, Williams G,
and Karduna A. Shoulder function and 3-
dimensional kinematics in people with
shoulder impingement syndrome before
and after a 6-week exercise program. Phys
Ther 84: 832–848, 2004.
23. Meurer A, Grober J, Betz U, Decking J, and
Rompe J. BWS-mobility in patients with an
impingement syndrome compared to
healthy subjects: An inclinometric study
(German). Z Orthop Ihre Grenzgeb 142:
415–420, 2004.
24. Myers J, Laudner K, Pasquale M, Bradley J,
and Lephart S. Glenohumeral range of
motion deficits and posterior shoulder
tightness in throwers with pathologic
internal impingement. Am J Sports Med 34:
385–391, 2006.
25. Nelson A, Kokkonen J, and Arnall D. Acute
muscle stretching inhibits muscle strength
endurance performance. J Strength Cond
Res 19: 338–343, 2005.
26. Nigg B. Biomechanical considerations on
barefoot movement and barefoot shoe
concepts. Footwear Sci 1: 73–79, 2009.
27. NoehrenB, Davis I, and Hamill J. Prospective
study of the biomechanical factors
associated with iliotibial band syndrome.
Clin Biomech 22: 951–956, 2007.
28. Nourbakhsh M and Arab A. Relationship
between mechanical factors and incidence
of low back pain. J Orthop Sports Phys
Ther 32: 447–460, 2002.
29. Olsen S, Fleisig G, Dun S, Loftice J, and
Andrews J. Risk factors for shoulder and
elbow injuries in adolescent baseball
pitchers. Am J Sports Med 34: 905–912,
2006.
30. Orchard J. Plantar fasciitis. BMJ 345: 35–
40, 2012.
31. Prins M and van der Wurff P. Females with
patellofemoral pain syndrome have weak
hip muscles: A systematic review. Aust J
Physiother 55: 9–15, 2009.
32. Reinold M, Wilk K, Macrina L, Sheheane C,
Dun S, Fleisig G, Crenshaw K, and
Andrews J. Changes in shoulder and elbow
passive range of motion after pitching in
professional baseball players. Am J Sports
Med 36: 523–527, 2008.
33. Sarcevi�c Z. Limited ankle dorsiflexion: A
predisposing factor to Morbus Osgood
Schlatter? Knee Surg Sports Traumatol
Arthrosc 16: 726–728, 2008.
34. Simic L, Sarabon N, and Markovic G. Does
pre-exercise static stretching inhibit
maximal muscular performance? A meta-
analytical review. Scand J Med Sci Sports
Epub ahead of print on February 8, 2012.
doi: 10.1111/j.1600-0838.2012.01444.x.
35. Sjolie A. Low-back pain in adolescents is
associated with poor hip mobility and high
body mass index. Scand J Med Sci Sports
14: 168–175, 2004.
36. Skolimowski J, Demczuk-W1odarczyk E,
Barczyk K, Anwajler J, and Skolimowska B.
Analysis of three-dimensional motion of the
glenohumeral joint in impingement
syndrome. Orthop Traumatol Rehabil 10:
554–565, 2008.
37. Taylor K, Sheppard J, Lee H, and
Plummer N. Negative effect of static
stretching restored when combined
with a sport specific warm-up
component. J Sci Med Sport 12:
657–661, 2009.
38. Thigpen C, Padua D, Michener L,
Guskiewicz K, Giuliani C, Keener J, and
Stergiou N. Head and shoulder posture
affect scapular mechanics and muscle
activity in overhead tasks. J Electromyogr
Kinesiol 20: 701–709, 2010.
39. Van Dillen L, McDonnell M, Fleming D, and
Sahrmann S. Effect of knee and hip
position on hip extension range of motion in
individuals with and without low back pain.
J Orthop Sports Phys Ther 30: 307–316,
2000.
40. Vetter R. Effects of six warm-up protocols
on sprint and jump performance.
J Strength Cond Res 21: 1233–1237,
2007.
41. Vismara L, Menegoni F, Zaina F, Galli M,
Negrini S, and Capodaglio P. Effect of
obesity and low back pain on spinal
mobility: A cross sectional study in women.
J Neuroeng Rehabil 7: 3, 2010.
42. Wilk K, Meister K, and Andrews J. Current
concepts in the rehabilitation of the
overhead throwing athlete Am J Sports
Med 30: 136–151, 2002.
43. Young W and Behm D. Effects of running,
static stretching and practice jumps on
explosive force production and jumping
performance. J Sports Med Phys Fitness
43: 21–27, 2003.
Strength and Conditioning Journal | www.nsca-scj.com 33