Embed Size (px)
Citation preview

J Occup Rehabil (2007) 17:327–352DOI 10.1007/s10926-007-9071-6
ORIGINAL PAPER
Models of Return to Work for Musculoskeletal Disorders
Izabela Z. Schultz · Anna W. Stowell ·Michael Feuerstein · Robert J. Gatchel
Published online: 8 February 2007C© Springer Science+Business Media, LLC 2007
Abstract Background: Musculoskeletal pain disorders are the most prevalent, costly, disabling,and commonly researched conditions in the workplace, yet the development of overarching con-ceptual models of return to work (RTW) in these conditions has been lagging. Method: A criticalreview of the literature was performed using multiple medical and health search engines inorder to provide an evaluation of the evolution and the state of the art of health and disabilitymodels with a focus on specific models of RTW. Results: The main tenets, implications fordiagnosis, treatment, and disability compensation, are the key perspectives analyzed for thefollowing specific models of RTW: biomedical, psychosocial, forensic, ecological/case manage-ment, biopsychosocial, and two more recent models developed by the Institute of Medicine andthe World Health Organization, respectively. Conclusions: Future development of models that
I. Z. Schultz (�)Deparment of Educational and Counselling Psychology, and Special Education,Scarfe Library Annex, Room 297, The University of British Columbia, 2125 Main Mall, Vancouver,British Colmbia, Canada V6T 1Z2e-mail: [email protected]
A. W. StowellDepartments of Anesthesiology and Pain Management, Psychiatry,and Rehabilitation Counseling, The Eugene McDermott Center for Pain Management,The University of TexasSouthwestern Medical Center, Dallas, TX, USA
M. FeuersteinDepartment of Medical and Clinical Psychology, Department of Preventive Medicine and Biometrics,Uniformed Services University of the Health Sciences, Bethesda, MD
R. J. GatchelDepartment of Psychology, College of Science, The University of Texas at Arlington, Arlington, TX, USA
R. J. GatchelDepartment of Anesthesiology and Pain Management and Rehabilitation Counseling,The Eugene McDermott Center for Pain Management, The University of Texas SouthwesternMedical Center, Dallas, TX, USA
Springer

328 J Occup Rehabil (2007) 17:327–352
are truly transdisciplinary, and address temporal and multidimensional aspects of occupationaldisability, remains a goal.
Keywords Occupational disability . Biomedical . Biopsychosocial . Return-to-work .
Disability models
Introduction
Musculoskeletal pain diseases involve an injury or disorder of the muscles, tendons, ligaments,joints, cartilage and spinal discs [1, 2] and constitute the most prevalent, costly, disabling, andcommonly researched conditions in the workplace. Yet, the development of comprehensiveconceptual models of return to work (RTW) in these pain-related conditions has been lagging.Over the past three decades, researchers and clinicians across many fields (i.e., occupationalmedicine, nursing, rehabilitation medicine, physical therapy, exercise physiology, physical andoccupational therapy, ergonomics, engineering, psychology, vocational counseling, economics,and public health) have contributed significantly to the accumulation of knowledge related tosecondary and tertiary prevention and management of work-related musculoskeletal disordersand associated disability. Despite this, there is no single theoretical framework driving this workor helping to integrate it to impact clinical management and policy.
While much more is empirically known about occupational disability than even a decadeago, the field continues to search for the most heuristic unifying models or theories of healthand disability that have a bearing on conceptualization of return to work. To facilitate thedevelopment of return to work models in musculoskeletal disorders, this paper will criticallyanalyze and integrate evolving theoretical approaches and empirical trends in health, disabilityand occupational rehabilitation literature. Our review will identify and update the key newdirections and emerging features of the evolution of return to work models, and associatedresearch challenges. It will further draw conceptual and methodological implications for futureconstruction of return to work models.
Historical perspectives on health and pain
In order to understand where we are today and the features of the recent evolution of RTWmodels, it is important to have a clear understanding of the conceptual foundations upon whichthis work has been built. Therefore, the following historical perspectives will be addressed: [1]the evolution of understanding of general health and disability; [2] the definition of RTW; and[3] evolution and application of major theories of disability to occupational disability with anemphasis on RTW.
Evolution of understanding of health and pain disability
To our knowledge, Hippocrates was the first to describe a mind-body connection. He proposedthat pain was felt when there is a disturbance of the four bodily humors [3]. He concluded thatpain and disability were symptoms of imbalance and had a rational, physical explanation contraryto others before him who attributed such defects in physical perfection to curses of punishmentby the gods [4]. Later, in the seventeenth century, Descartes described a dualistic theory of themind and body [5, 6], which postulated that anything that was not directly identifiable to anorganic origin was consequently of a psychological origin. Unfortunately, for the subsequent
Springer
J Occup Rehabil (2007) 17:327–352 329
three hundred years, this Cartesian view has served to hamper the development of integrativemodels of health. Melzack and Wall [7] ultimately defied the prevalent Cartesian dualistic mind-body paradigm of the time and built upon Hippocrates’ idea in the area of pain, one of the keyand least understood factors in health and disability. The proposed gate control theory of painplaced emphasis for pain regulation and the impact of function in both the peripheral and centralnervous systems. Melzack and Wall also proposed that the pain experience is comprised ofsensory, affective/emotional, and cognitive dimensions. The combination of these factors servesto impact an individual’s emotional and behavioral reaction to pain. This model has evolvedover the years to include a number of physiological processes that are proposed to explain manypain disorders, including the musculoskeletal pain disorders that are commonly associated withoccupational disability.
In the early 1970s, Brody [8] furthered our understanding of health by applying systemstheory to health. Brody argued that the health of an individual was best conceptualized withina hierarchy of natural systems ranging from subatomic particles at the lowest level through theperson, family, community, subculture, culture, society-nation, species, and lastly, biosphere. Heemphasized the importance of the interrelatedness of many factors that can impact health andhighlighted the importance of clarifying the relationships between these biological and socialprocesses.
Engel [9] built upon these earlier ideas with the development of the biopsychosocial approachin medicine. In his seminal paper in Science, Engel proposed that, to truly understand a patient’sillness, it was not sufficient to simply focus on the pathophysiology of the disorder. Social contextand psychosocial factors that might have contributed to the illness, or influenced the exacerbationand maintenance of the clinical problem, are important for any healthcare provider to consider.Engel’s arguments in favor of a biopsychosocial approach to medicine have proven influential,albeit with delay, in subsequent theory development, as well as in research and practice in health,healthcare, and disability.
In the 1990s, Melzack further refined the original gate control theory of pain. Melzack’s [10]updated model, the neuromatrix model of pain, grew out of work with patients who continuedto experience pain following spinal cord resection (e.g., as in phantom limb pain). By proposinga complex interaction of neural inputs from within and outside of the brain and the role of theimmune system in this process, the neuromatrix model helps account for the potential geneticinfluence on pain, as well as an individual’s response to the environment and its biologicalconcomitants.
Currently, the biopsychosocial approach has been modified in many different forms andis generally the most commonly considered and consensual framework for understanding themultidimensional aspects of many health problems. Unfortunately, in reality, this conceptual-ization, while critical to the area of psychosomatic medicine and behavioral medicine, has neverreached the level of specificity required for its systematic empirical validation within the fieldof occupational disability [11].
Definition of return to work
A great deal of research has been undertaken in the field of occupational disability; however, ithas been largely hampered by lack of a clear definition of RTW and remains fragmented [12].A review of the occupational disability literature identifies differences in the way researchersunderstand and operationalize the terms “disability” and “RTW.” Whereas occupational or workdisability is usually operationally defined as time off of work, reduced productivity, or workingwith functional limitations as a result (outcome), of either traumatic or non-traumatic clinicalconditions, the term “return to work” is utilized as both a process and outcome measure. RTW
Springer
330 J Occup Rehabil (2007) 17:327–352
can be conceptualized as the “process” of returning an injured worker to work (e.g., graduatedRTW or job accommodation), or being the measurable final common outcome of disability: thestatus of working or not working [13]. The term “RTW” can also reflect a range of definitionsof vocational outcomes, including duration or extent of an inability to work secondary tofunctional limitations [14]. The definitions of duration of occupational disability range fromcumulative, as in the duration of all days lost from work starting with the date of injury; throughcategorical (RTW status: yes/no); to continuous, such as time to RTW [13]. In addition, RTW asan outcome may involve return to the pre-injury employer or the pre-injury job, with or withoutaccommodation. Consequently, the perspectives on, and measurements of, RTW in research andpractice vary widely and depend upon the disability stakeholder [14–17].
Moreover, the recurrent nature of many musculoskeletal conditions that we know exist clin-ically was recently highlighted as something that should be seriously considered in disabilityprediction research [18]. While this was documented years ago by Baldwin, Butler, and John-son [19], the identification of patterns of RTW, with gaps in disability, involuntary termina-tion, unemployment, and retirement need to be considered in our comprehensive definitionsof occupational disability as the related research moves forward. Finally, when consideringmodels of disability and measurement of RTW, while it can be measured using both self-reported and administrative data, it is important to recognize that each one has its strengths andlimitations.
Much of the literature on prediction of occupational outcomes following injury focuses onthe identification of those at risk for disability rather than on those who do RTW. However, theaccumulation of evidence on factors predictive of occupational disability may not lead to thedevelopment of an empirically supported model of RTW as predictors of disability and predictorsof RTW often differ [20, 21]. More research on how these models actually differ would helpfurther clarify this issue.
Evolution of application of major theories of disability to occupational disability
Failure to RTW following illness or injury is often, both theoretically and operationally, equatedwith occupational disability. Historically, three major theoretical schools influenced the modelsand definitions of occupational disability: biomedical, biopsychosocial, and social construction[22–25, 26, as cited in, Imrie, 2004, 27, 28, as cited in, Imrie, 2004, 29, as cited in, Imrie,2004, 30, 31]. These theories contributed to the creation of both conceptual and specific modelsof disability within the context of RTW, as well as to more recent comprehensive models thathave attempted to integrate aspects of all the models. The following is, therefore, an attempt tosynthesize the literature from many disparate sources, to provide a comprehensive overview ofthe evolution and state of the art in regards to RTW models.
Method
A critical review of the literature was performed using multiple medical and health search enginesin order to provide an evaluation of the evolution and the state of the art of health and disabilitymodels with a focus on specific models of RTW. Search engines included Medline OVID,Medline Pubmed, CINAHL, Cochrane Database of Systematic Reviews, Academic SearchPremier, Health and Psychosocial Instruments (HAPI), Health Reference Center, IEEE Xplore,Natural Medicines Database, NCBI Databases, PsycINFO, Scopus, and Web of Science. Despitethe use of all of the above databases, due to the multidisciplinary and methodologically diverse
Springer
J Occup Rehabil (2007) 17:327–352 331
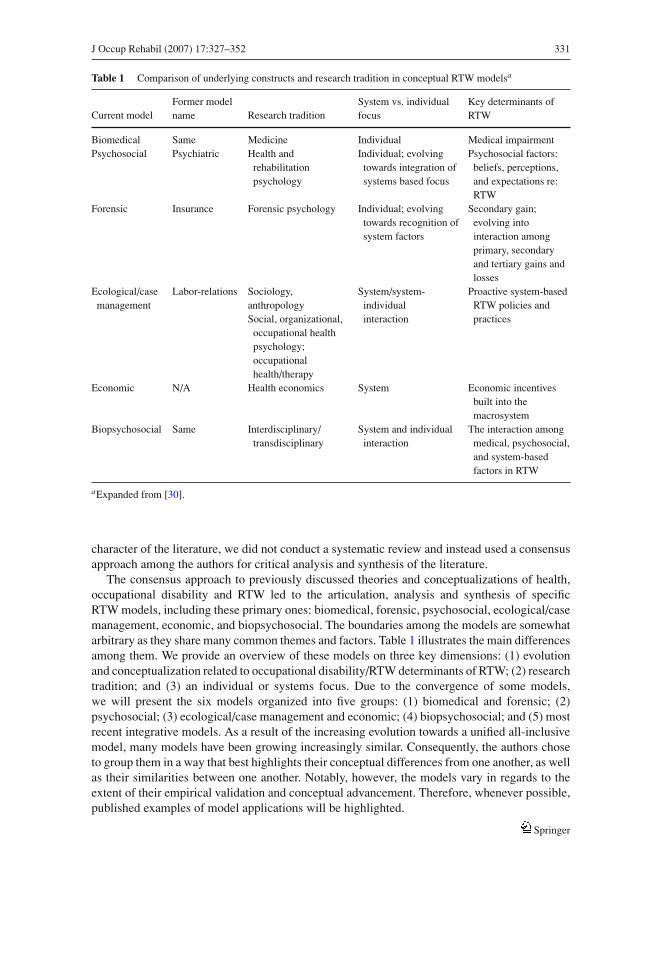
Table 1 Comparison of underlying constructs and research tradition in conceptual RTW modelsa
Current modelFormer modelname Research tradition
System vs. individualfocus
Key determinants ofRTW
Biomedical Same Medicine Individual Medical impairmentPsychosocial Psychiatric Health and
rehabilitationpsychology
Individual; evolvingtowards integration ofsystems based focus
Psychosocial factors:beliefs, perceptions,and expectations re:RTW
Forensic Insurance Forensic psychology Individual; evolvingtowards recognition ofsystem factors
Secondary gain;evolving intointeraction amongprimary, secondaryand tertiary gains andlosses
Ecological/casemanagement
Labor-relations Sociology,anthropologySocial, organizational,
occupational healthpsychology;occupationalhealth/therapy
System/system-individualinteraction
Proactive system-basedRTW policies andpractices
Economic N/A Health economics System Economic incentivesbuilt into themacrosystem
Biopsychosocial Same Interdisciplinary/transdisciplinary
System and individualinteraction
The interaction amongmedical, psychosocial,and system-basedfactors in RTW
aExpanded from [30].
character of the literature, we did not conduct a systematic review and instead used a consensusapproach among the authors for critical analysis and synthesis of the literature.
The consensus approach to previously discussed theories and conceptualizations of health,occupational disability and RTW led to the articulation, analysis and synthesis of specificRTW models, including these primary ones: biomedical, forensic, psychosocial, ecological/casemanagement, economic, and biopsychosocial. The boundaries among the models are somewhatarbitrary as they share many common themes and factors. Table 1 illustrates the main differencesamong them. We provide an overview of these models on three key dimensions: (1) evolutionand conceptualization related to occupational disability/RTW determinants of RTW; (2) researchtradition; and (3) an individual or systems focus. Due to the convergence of some models,we will present the six models organized into five groups: (1) biomedical and forensic; (2)psychosocial; (3) ecological/case management and economic; (4) biopsychosocial; and (5) mostrecent integrative models. As a result of the increasing evolution towards a unified all-inclusivemodel, many models have been growing increasingly similar. Consequently, the authors choseto group them in a way that best highlights their conceptual differences from one another, as wellas their similarities between one another. Notably, however, the models vary in regards to theextent of their empirical validation and conceptual advancement. Therefore, whenever possible,published examples of model applications will be highlighted.
Springer
332 J Occup Rehabil (2007) 17:327–352
Results
Biomedical and forensic models
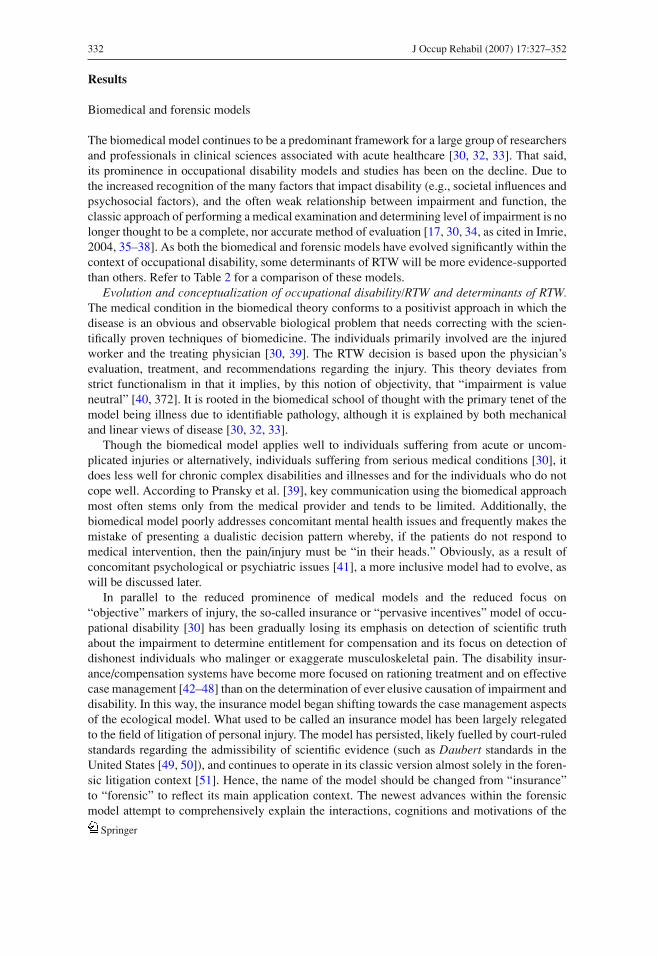
The biomedical model continues to be a predominant framework for a large group of researchersand professionals in clinical sciences associated with acute healthcare [30, 32, 33]. That said,its prominence in occupational disability models and studies has been on the decline. Due tothe increased recognition of the many factors that impact disability (e.g., societal influences andpsychosocial factors), and the often weak relationship between impairment and function, theclassic approach of performing a medical examination and determining level of impairment is nolonger thought to be a complete, nor accurate method of evaluation [17, 30, 34, as cited in Imrie,2004, 35–38]. As both the biomedical and forensic models have evolved significantly within thecontext of occupational disability, some determinants of RTW will be more evidence-supportedthan others. Refer to Table 2 for a comparison of these models.
Evolution and conceptualization of occupational disability/RTW and determinants of RTW.The medical condition in the biomedical theory conforms to a positivist approach in which thedisease is an obvious and observable biological problem that needs correcting with the scien-tifically proven techniques of biomedicine. The individuals primarily involved are the injuredworker and the treating physician [30, 39]. The RTW decision is based upon the physician’sevaluation, treatment, and recommendations regarding the injury. This theory deviates fromstrict functionalism in that it implies, by this notion of objectivity, that “impairment is valueneutral” [40, 372]. It is rooted in the biomedical school of thought with the primary tenet of themodel being illness due to identifiable pathology, although it is explained by both mechanicaland linear views of disease [30, 32, 33].
Though the biomedical model applies well to individuals suffering from acute or uncom-plicated injuries or alternatively, individuals suffering from serious medical conditions [30], itdoes less well for chronic complex disabilities and illnesses and for the individuals who do notcope well. According to Pransky et al. [39], key communication using the biomedical approachmost often stems only from the medical provider and tends to be limited. Additionally, thebiomedical model poorly addresses concomitant mental health issues and frequently makes themistake of presenting a dualistic decision pattern whereby, if the patients do not respond tomedical intervention, then the pain/injury must be “in their heads.” Obviously, as a result ofconcomitant psychological or psychiatric issues [41], a more inclusive model had to evolve, aswill be discussed later.
In parallel to the reduced prominence of medical models and the reduced focus on“objective” markers of injury, the so-called insurance or “pervasive incentives” model of occu-pational disability [30] has been gradually losing its emphasis on detection of scientific truthabout the impairment to determine entitlement for compensation and its focus on detection ofdishonest individuals who malinger or exaggerate musculoskeletal pain. The disability insur-ance/compensation systems have become more focused on rationing treatment and on effectivecase management [42–48] than on the determination of ever elusive causation of impairment anddisability. In this way, the insurance model began shifting towards the case management aspectsof the ecological model. What used to be called an insurance model has been largely relegatedto the field of litigation of personal injury. The model has persisted, likely fuelled by court-ruledstandards regarding the admissibility of scientific evidence (such as Daubert standards in theUnited States [49, 50]), and continues to operate in its classic version almost solely in the foren-sic litigation context [51]. Hence, the name of the model should be changed from “insurance”to “forensic” to reflect its main application context. The newest advances within the forensicmodel attempt to comprehensively explain the interactions, cognitions and motivations of the
Springer
J Occup Rehabil (2007) 17:327–352 333
Table 2 Comparison of the biomedical model and the forensic modela
Biomedical model Forensic model
Main tenets • Illness is due to physicalpathology
• People who anticipate secondary gains arelikely to be dishonest about their symptoms
• Symptoms and disability aredirectly proportionate tophysical pathology
• Mind and body are separate• Physicians in control of
diagnosis and treatmentdirection
• Objective proof of impairment and disabilitymust be provided
• It is paramount to clearly discriminate between“honest” and “dishonest” clients
• Interactions among primary, secondary andtertiary gains and losses should be considered
Underlying values • Scientific evidence andobjectivity
• Scientific truth• Protection of the system from abuse and
dishonesty• Cost limitation
Implications fordiagnosis
• Focus on uncovering organicpathology
• Sequential diagnostic approach
• Thorough and exhaustive assessment usingspecial forensic methods aimed at detection ofinconsistencies and deception
• Interdisciplinary model may be utilized• Individuals showing inconsistencies in testing
identified as “illegitimate”, “malingerers”,“symptom magnifiers,” and/or motivated bysecondary gain
• Adversarial service climateImplications fortreatment
• Cure-orientation rather thancoping-orientation
• Wide range of treatment options for clientsidentified as “honest” only
• Need to relate physicaltreatment to underlyingpathology
• No treatment for clients identified as“dishonest”
• Focus on physical treatmentmodalities
Implications forcompensation
• Compensation for impairmentswith clearly identified medicalcauses
• Lack of specific built-infinancial incentives for coping
• Compensation for “honest” clients only• Appears an attractive option due to simplicity• Long term costs due to chronicity in incorrectly
identified clients• Multiple systemic safeguards necessary to
detect malingering may cause serviceinefficiencies
aAdapted from [30], where updated information is italicized.
injured person within the disability system to better inform the RTW decision and behavior thusbringing it closer to the biopsychosocial approach [52, 53]. Within this expanded forensic model,Dersh, Polatin, and Gatchel also describe primary, secondary and tertiary gains and losses thatmay serve to impact the interaction between the injured worker and the larger disability system[54].
Research tradition. The biomedical model relies heavily on objective findings, identified bya systematic, scientific approach to the injury complaint [30]. On the other hand, the forensicmodel has evolved out of forensic psychology and neuropsychology research to explain themotivations an individual may have that could influence the RTW decision (i.e., malingering,secondary gain and primary gain).
Springer
334 J Occup Rehabil (2007) 17:327–352
Individual versus systems focus. Both the biomedical model and the classic forensic modelrely primarily on an individual focus on the patient. Though this is a strength in understandingand predicting outcome with acutely injured individuals, it does not readily apply to the morecomplex chronic patients who often account for much of the disability statistics.
Psychosocial models
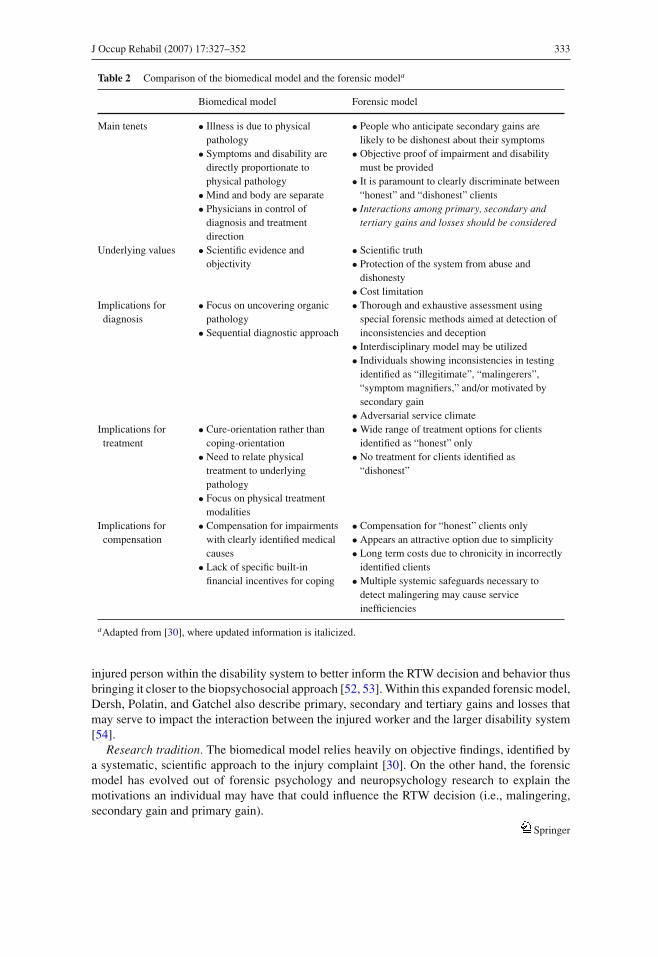
The psychiatric perspective [30] of disability has gradually been shifting away from the tra-ditional focus on psychopathology to a broader psychosocial adaptation perspective. Refer toTable 3 for a summary of the major features of this model.
Evolution and conceptualization of occupational disability/RTW and determinants of RTW.From a psychological viewpoint, RTW is a behavior. Additionally, occupational disability isnot viewed as an individual attribute, but as a complex set of conditions, activities, and rela-tionships, which have been created by a person’s social environment, including the workplace,healthcare, compensation systems, family, and other societal institutions [23, 24, 55, 56]. As aresult, RTW can be conceptualized using cognitive-behavioral and organizational psychologyperspectives [13, 14, 20, 30, 33, 41, 57]. Each of these perspectives has different implica-tions for the study of RTW behavior. Where musculoskeletal pain and disability are concerned,the cognitive-behavioral perspective is the most commonly used, and benefits from the mostconsistent empirical support [58].
Table 3 Summary of the psychosocial model
Psychosocial model
Main tenets • Psychosocial factors play predominant role in disability and readiness toRTW
• Psychosocial factors are both individual-related and system-related• Perceptions, beliefs, and expectations of recovery and disability,
self-efficacy, and ways of coping are more important than objective factorsin disability formation
• Motivational factors mediate between impairment and disabilityUnderlying values • Scientific truth
• Understanding subjective drivers of disabilityImplications for diagnosis • Psychosocial factors must be assessed and identified at any stage of
disability• Cognitions about disability must be particularly investigated• Stage of readiness for RTW including self-efficacy and decisional balance
should be identified• Psychological diagnosis is of secondary importance
Implications for treatment • Modifiable psychosocial factors must be targeted in treatment on a prioritybasis
• Cognitive-behavioral approaches constitute psychological treatment ofchoice
• Prevention targeting psychosocial factors can be undertaken in theinterdisciplinary intervention context, not only in psychological therapycontext
Implications for compensation • Though many psychosocial factors are not compensable they must beaccounted for in treatment
• Potential increase in health care benefits, but expedited RTW
Springer
J Occup Rehabil (2007) 17:327–352 335
Research tradition. Bandura’s social learning theory [59, 60] does appear to hold significantconceptual promise for understanding the motivation to RTW. Specifically, the significance ofexpectations of outcome (i.e., recovery and RTW), in combination with expectations of efficacy,in predicting an individual’s ability to achieve desired outcomes (i.e., RTW) has been gainingempirical research support [57, 61–63].
Individual versus system focus. This perspective focuses on beliefs, perceptions, expectations,locus of control, self-efficacy, and coping of the individual [64–68] as mechanisms underlyingdisability. As a transition from an exclusive focus on the individual [69], these models considerboth the individual and the workplace by looking at the perception of the workplace and its rolein occupational disability. More recently, the role of both individual cognitive-behavioral factorsand systems has been broadened to cover several psychosocial dimensions of systems, such asworkplace, unions, healthcare, and disability insurers [17, 70, 71].
Ecological/case management and the economic models
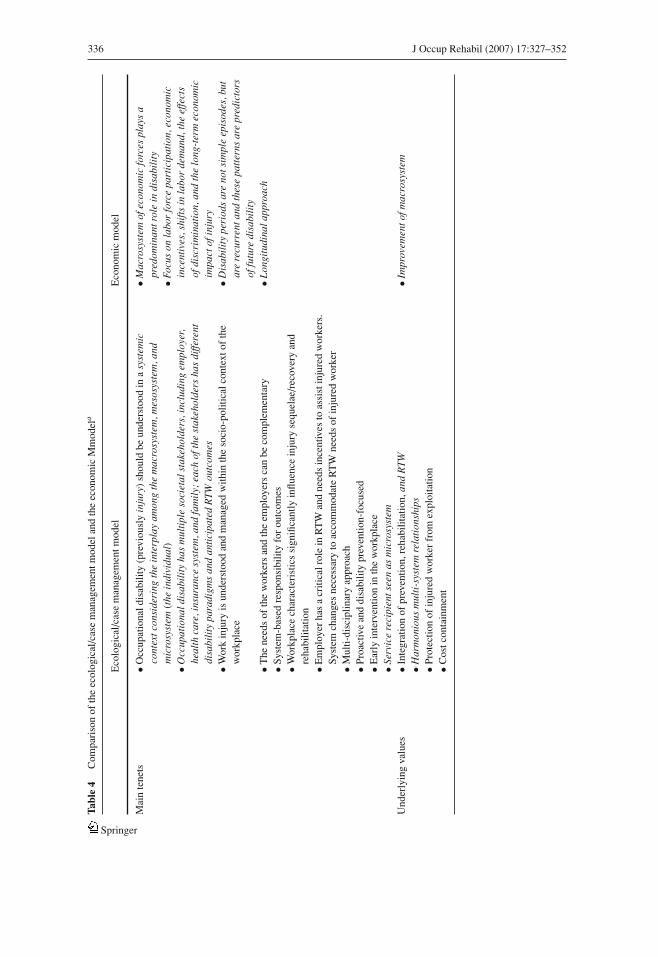
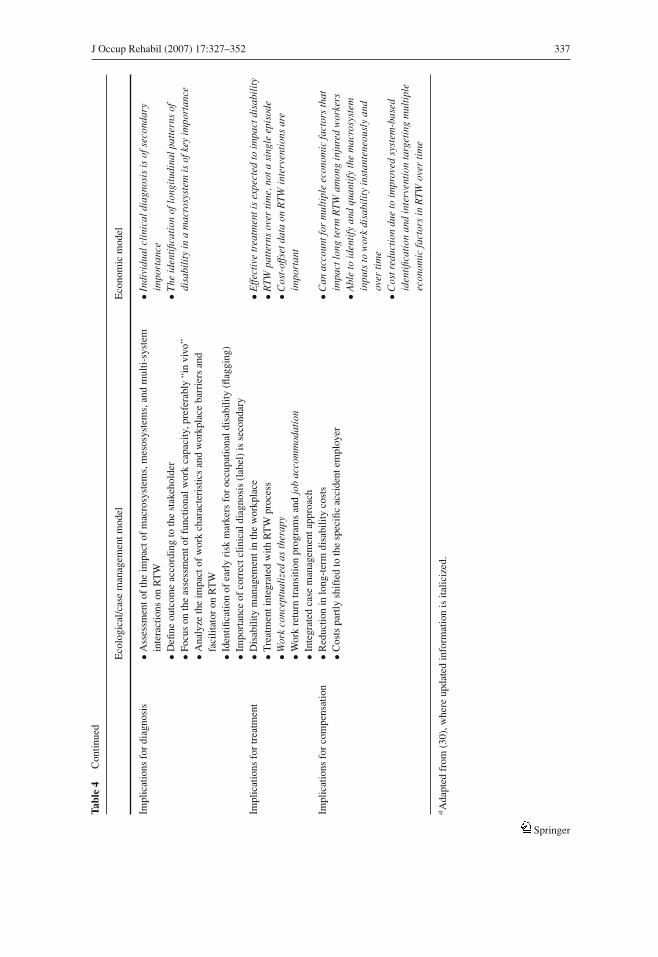
Over time, the ecological/case management and economic models expanded and converged inmany areas; consequently, they will be discussed together. Refer to Table 4 for a summarizedcomparison of the major features of these models.
Evolution and conceptualization of occupational disability/RTW and determinants of RTW.The primary focus of these models is on the decision and determinants of RTW from a stakeholderposition in which the interests of the complex interaction of the social environment are assessed;that is, the workplace and impact of RTW on employers, disability payors, insurance carriers,and healthcare utilization. Though the individual injured worker is also at the center of thismodel, the overwhelming societal implications of the RTW process and decision are paramount.The complexity and the multidimensional, dynamic nature of the ecological/case managementmodel constitute both this model’s strength and limitation. On one hand, it attempts to capturethe complex phenomenon of RTW from a social perspective as arising from the interaction ofmultiple societal systems, and aptly identifies the stakeholders in disability and relationshipsamong them that facilitate or hinder RTW. This model has been successfully validated andreplicated in multi-system RTW interventions in different legal, social and economic contextssuch as in Canada and in The Netherlands [72–74]. On the other hand, the model continuesto require further construct validation and development to better understand the respectivecontributions of its key system components and their interactions with characteristics of theinjured worker in various disability prevention contexts.
Research tradition. The ecological/case management model is founded upon a multitudeof disciplines, such as sociology, anthropology, social work, industrial/organizational, healthpsychology, nursing, and occupational health and therapy. In contrast, the economic model ismore narrowly based in the field of economics.
Individual versus systems focus. The ecological/case management model of RTW is, in part,based on Bronfenbrenner’s Systems Theory [75], which assumes the interaction of microsystems(the worker factors) with mesosystems (workplace, healthcare, and insurance system factors) andmacrosystems (economic, social, and legislative factors) [56, 72, 73, 76, 77]. The labor-relationsmodel, a specific application of the ecological/case management model, focuses on the mesosys-tem of work (workplace characteristics such as climate, culture, organization, job demand andaccommodation, policies, procedures, and practices) and effective disability/case managementof the injured worker as the key RTW intervention [30, 78–83]. The most recent advancesin the RTW interventions in musculoskeletal pain (focused on upper extremity disorders) ledtoward the integration of the ecological/labor-relations model with the biopsychosocial model.This newly integrated approach positions case management in the occupational environment
Springer
336 J Occup Rehabil (2007) 17:327–352
Tabl
e4
Com
pari
son
ofth
eec
olog
ical
/cas
em
anag
emen
tmod
elan
dth
eec
onom
icM
mod
ela
Eco
logi
cal/c
ase
man
agem
entm
odel
Eco
nom
icm
odel
Mai
nte
nets
•Occ
upat
iona
ldis
abili
ty(p
revi
ousl
yin
jury
)sh
ould
beun
ders
tood
ina
syst
emic
cont
extc
onsi
deri
ngth
ein
terp
lay
amon
gth
em
acro
syst
em,m
esos
yste
m,a
ndm
icro
syst
em(t
hein
divi
dual
)•O
ccup
atio
nald
isab
ilit
yha
sm
ulti
ple
soci
etal
stak
ehol
ders
,inc
ludi
ngem
ploy
er,
heal
thca
re,i
nsur
ance
syst
em,a
ndfa
mil
y;ea
chof
the
stak
ehol
ders
has
diffe
rent
disa
bili
typa
radi
gms
and
anti
cipa
ted
RT
Wou
tcom
es
•Mac
rosy
stem
ofec
onom
icfo
rces
play
sa
pred
omin
antr
ole
indi
sabi
lity
•Foc
uson
labo
rfo
rce
part
icip
atio
n,ec
onom
icin
cent
ives
,shi
fts
inla
bor
dem
and,
the
effe
cts
ofdi
scri
min
atio
n,an
dth
elo
ng-t
erm
econ
omic
impa
ctof
inju
ry•W
ork
inju
ryis
unde
rsto
odan
dm
anag
edw
ithin
the
soci
o-po
litic
alco
ntex
tof
the
wor
kpla
ce•D
isab
ilit
ype
riod
sar
eno
tsim
ple
epis
odes
,but
are
recu
rren
tand
thes
epa
tter
nsar
epr
edic
tors
offu
ture
disa
bili
ty•T
hene
eds
ofth
ew
orke
rsan
dth
eem
ploy
ers
can
beco
mpl
emen
tary
•Lon
gitu
dina
lapp
roac
h•S
yste
m-b
ased
resp
onsi
bilit
yfo
rou
tcom
es•W
orkp
lace
char
acte
rist
ics
sign
ifica
ntly
influ
ence
inju
ryse
quel
ae/r
ecov
ery
and
reha
bilit
atio
n•E
mpl
oyer
has
acr
itica
lrol
ein
RT
Wan
dne
eds
ince
ntiv
esto
assi
stin
jure
dw
orke
rs.
Syst
emch
ange
sne
cess
ary
toac
com
mod
ate
RT
Wne
eds
ofin
jure
dw
orke
r•M
ulti-
disc
iplin
ary
appr
oach
•Pro
activ
ean
ddi
sabi
lity
prev
entio
n-fo
cuse
d•E
arly
inte
rven
tion
inth
ew
orkp
lace
•Ser
vice
reci
pien
tsee
nas
mic
rosy
stem
Und
erly
ing
valu
es•I
nteg
ratio
nof
prev
entio
n,re
habi
litat
ion,
and
RT
W•I
mpr
ovem
ento
fmac
rosy
stem
•Har
mon
ious
mul
ti-s
yste
mre
lati
onsh
ips
•Pro
tect
ion
ofin
jure
dw
orke
rfr
omex
ploi
tatio
n•C
ostc
onta
inm
ent
Springer
J Occup Rehabil (2007) 17:327–352 337
Tabl
e4
Con
tinue
d
Eco
logi
cal/c
ase
man
agem
entm
odel
Eco
nom
icm
odel
Impl
icat
ions
for
diag
nosi
s•A
sses
smen
tof
the
impa
ctof
mac
rosy
stem
s,m
esos
yste
ms,
and
mul
ti-sy
stem
inte
ract
ions
onR
TW
•Ind
ivid
ualc
lini
cald
iagn
osis
isof
seco
ndar
yim
port
ance
•Defi
neou
tcom
eac
cord
ing
toth
est
akeh
olde
r•F
ocus
onth
eas
sess
men
tof
func
tiona
lwor
kca
paci
ty,p
refe
rabl
y“i
nvi
vo”
•The
iden
tific
atio
nof
long
itud
inal
patt
erns
ofdi
sabi
lity
ina
mac
rosy
stem
isof
key
impo
rtan
ce•A
naly
zeth
eim
pact
ofw
ork
char
acte
rist
ics
and
wor
kpla
ceba
rrie
rsan
dfa
cilit
ator
onR
TW
•Ide
ntifi
catio
nof
earl
yri
skm
arke
rsfo
roc
cupa
tiona
ldis
abili
ty(fl
aggi
ng)
•Im
port
ance
ofco
rrec
tclin
ical
diag
nosi
s(l
abel
)is
seco
ndar
yIm
plic
atio
nsfo
rtr
eatm
ent
•Dis
abili
tym
anag
emen
tin
the
wor
kpla
ce•E
ffect
ive
trea
tmen
tis
expe
cted
toim
pact
disa
bili
ty•T
reat
men
tint
egra
ted
with
RT
Wpr
oces
s•R
TW
patt
erns
over
tim
e,no
tasi
ngle
epis
ode
•Wor
kco
ncep
tual
ized
asth
erap
y•W
ork
retu
rntr
ansi
tion
prog
ram
san
djo
bac
com
mod
atio
n•C
ost-
offs
etda
taon
RT
Win
terv
enti
ons
are
impo
rtan
t•I
nteg
rate
dca
sem
anag
emen
tapp
roac
hIm
plic
atio
nsfo
rco
mpe
nsat
ion
•Red
uctio
nin
long
-ter
mdi
sabi
lity
cost
s•C
osts
part
lysh
ifte
dto
the
spec
ific
acci
dent
empl
oyer
•Can
acco
untf
orm
ulti
ple
econ
omic
fact
ors
that
impa
ctlo
ngte
rmR
TW
amon
gin
jure
dw
orke
rs•A
ble
toid
enti
fyan
dqu
anti
fyth
em
acro
syst
emin
puts
tow
ork
disa
bili
tyin
stan
tene
ousl
yan
dov
erti
me
•Cos
tred
ucti
ondu
eto
impr
oved
syst
em-b
ased
iden
tific
atio
nan
din
terv
enti
onta
rget
ing
mul
tipl
eec
onom
icfa
ctor
sin
RT
Wov
erti
me
aA
dapt
edfr
om(3
0),w
here
upda
ted
info
rmat
ion
isita
liciz
ed.
Springer

338 J Occup Rehabil (2007) 17:327–352
involving systems and medical management, ergonomic accommodations, and problem-solvingas central to the RTW process [84–86].
Examples of ecological/case management and economic models. The most comprehensiveecological/case management model of RTW to date has been provided by Loisel [72, 73]. Accord-ing to this model, the actions and attitudes of key stakeholders in the occupational disablementprocess, together with interactions among the stakeholders, are critical in conceptualizing RTW.The workplace, the healthcare system, and the compensation system are the most importantstakeholders.
Loisel’s conceptual model of RTW and secondary prevention is illustrated in Fig. 1. Thecomponents of the model include the personal system at social, affective, cognitive, and phys-ical levels; and various organizational levels of the healthcare system, the workplace, and thecompensation system [73]. In this updated model, from Loisel’s previous 2001 model [72], thecultural and political context has been added to address the more global and societal contextwithin which occupational disability occurs.
In addition, the relatively newly articulated economic model is also system-based and eco-logical in its origin. This model focuses on macrosystem factors such as the impact of poorhealth on labor force participation, economic incentives and shifts in labor demand, the effectsof discrimination on the labor force, and the long-term economic impact of injury consideringintermittent episodes of disability [19, 87–90]. The aspects of this model should in the futurebe included in the development of comprehensive interdisciplinary research of occupationaldisability and RTW models. This model is much less known in the clinical and occupationalrehabilitation field which consequently may be a reason for a paucity of specific examples in thecommon RTW literature.
Fig. 1 The arena in occupational disability prevention [73, p. 509)
Springer

J Occup Rehabil (2007) 17:327–352 339
Other researchers have specifically looked at the role that rehabilitation professionals play inthe RTW process. Hergenrather et al. [91] systematically surveyed the attitudes and beliefs ofthese professionals surrounding their ability to help return a disabled worker to work based onthe theory of planned behavior (TPB), arising out of cognitive-behavioral theory. Their findingssuggest that job placement rehabilitation experts are altruistically motivated to help an injuredperson RTW. In summary, they found that the attitudes and beliefs of the professional, not justthe worker (as discussed in the impairment model), are an important factor within the system ofinfluences surrounding the RTW process.
Biopsychosocial models
Empirical support for a purely biomedical model of occupational disability and RTW is lacking,but the evidentiary basis for psychosocial determinants of disability has been rapidly growing[18, 20, 21, 35, 92, 93]. Indeed, there appears to be a trend to omit medical factors as likelynon-contributory in occupational disability studies. This is of concern because this assumptionis a priori and still continues to require verification. The biopsychosocial theory advocates theintegration of individual characteristics, including biological impairment, i.e., medical factorsinto a systems-based approach. It focuses on conceptualizing disability as a consequence ofthe interaction among biological, physical, behavioral/psychological, and social phenomena.A comprehensive biopsychosocial model incorporates medical/biological factors, as well aspsychosocial, environmental, and ergonomic factors, within a systems based approach. Thedevelopment of this model was primarily guided by empirically derived risk factors, whichconstitutes its strength, but also by cumulative clinical experience with patients with chronicmusculoskeletal pain, which some consider to be the model’s limitation.
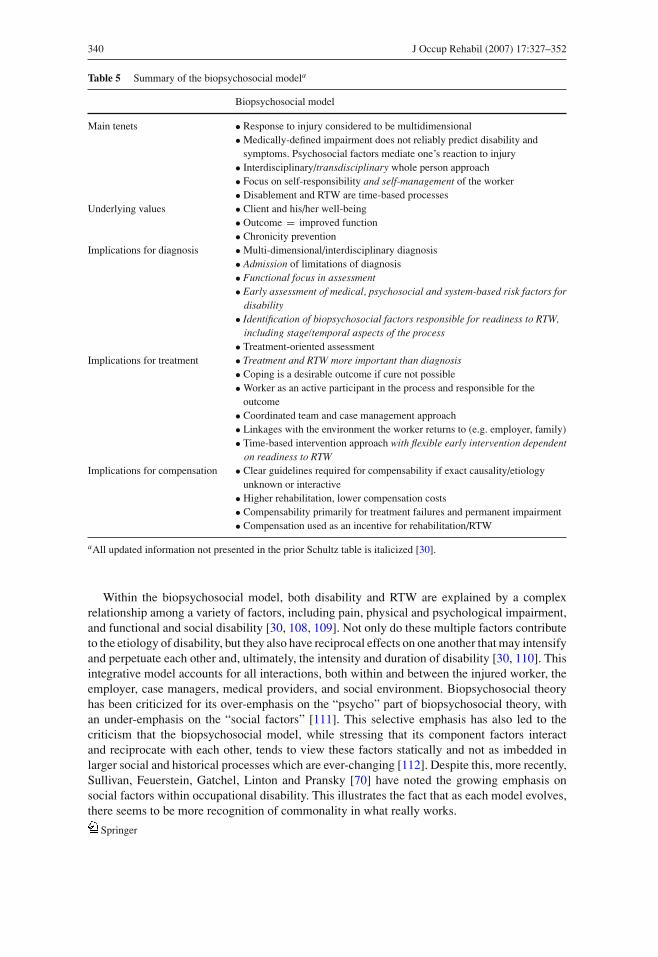
The difficulty in application of a not quite yet ready transdisciplinary paradigm and method-ology to conceptualize and measure the interaction between the physical and the psychosocialmay be the root cause of a lack of a universally agreed upon “best” model for understanding thecomplex issue of occupational disability and RTW – yet, development of such a model is whatmany continue to strive towards. Refer to Table 5 for a summary of the biopsychosocial model.
Evolution and conceptualization of occupational disability/RTW and determinants of RTW.The gate control theory by Melzack [7], has influenced research and practice in biopsychosocialaspects of pain and disability, and further helped to stimulate an interdisciplinary approach topain and disability research. Consequently, during the 1980s, there was an increased emphasis onthe role of psychosocial variables in pain disorders, [94–96]. Specifically, in regards to the workenvironment, Mayer and Gatchel [97] developed an innovative functional restoration approachto managing pain and reducing functional disability in work-related back pain that impacted howthese disorders were managed. The 1980s also saw the development of new multidisciplinarymodels that helped to explain work-related musculoskeletal disorders and occupational disabilitydeveloped for the purpose of guiding research and practice [98, 99].
Subsequently, the next decade was characterized by modifications and expansions of the newbiopsychosocially-oriented approaches to occupational disability. This included refinement ofinterdisciplinary conceptualizations of disability [100–102], the phase model of occupationaldisability [77], the focus on the role of organizational factors [82, 83], and the patterns ofoccupational disability and costs [19]. Since these developments, many studies have attemptedto identify predictors of occupational disability. These studies began to identify a wide rangeof predictors of exacerbation and/or maintenance of occupational disability [57, 63, 65, 69, 95,103–107]. As a result, evolving models of work-related musculoskeletal disorders have becomemore integrative.
Springer
340 J Occup Rehabil (2007) 17:327–352
Table 5 Summary of the biopsychosocial modela
Biopsychosocial model
Main tenets • Response to injury considered to be multidimensional• Medically-defined impairment does not reliably predict disability and
symptoms. Psychosocial factors mediate one’s reaction to injury• Interdisciplinary/transdisciplinary whole person approach• Focus on self-responsibility and self-management of the worker• Disablement and RTW are time-based processes
Underlying values • Client and his/her well-being• Outcome = improved function• Chronicity prevention
Implications for diagnosis • Multi-dimensional/interdisciplinary diagnosis• Admission of limitations of diagnosis• Functional focus in assessment• Early assessment of medical, psychosocial and system-based risk factors for
disability• Identification of biopsychosocial factors responsible for readiness to RTW,
including stage/temporal aspects of the process• Treatment-oriented assessment
Implications for treatment • Treatment and RTW more important than diagnosis• Coping is a desirable outcome if cure not possible• Worker as an active participant in the process and responsible for the
outcome• Coordinated team and case management approach• Linkages with the environment the worker returns to (e.g. employer, family)• Time-based intervention approach with flexible early intervention dependent
on readiness to RTWImplications for compensation • Clear guidelines required for compensability if exact causality/etiology
unknown or interactive• Higher rehabilitation, lower compensation costs• Compensability primarily for treatment failures and permanent impairment• Compensation used as an incentive for rehabilitation/RTW
aAll updated information not presented in the prior Schultz table is italicized [30].
Within the biopsychosocial model, both disability and RTW are explained by a complexrelationship among a variety of factors, including pain, physical and psychological impairment,and functional and social disability [30, 108, 109]. Not only do these multiple factors contributeto the etiology of disability, but they also have reciprocal effects on one another that may intensifyand perpetuate each other and, ultimately, the intensity and duration of disability [30, 110]. Thisintegrative model accounts for all interactions, both within and between the injured worker, theemployer, case managers, medical providers, and social environment. Biopsychosocial theoryhas been criticized for its over-emphasis on the “psycho” part of biopsychosocial theory, withan under-emphasis on the “social factors” [111]. This selective emphasis has also led to thecriticism that the biopsychosocial model, while stressing that its component factors interactand reciprocate with each other, tends to view these factors statically and not as imbedded inlarger social and historical processes which are ever-changing [112]. Despite this, more recently,Sullivan, Feuerstein, Gatchel, Linton and Pransky [70] have noted the growing emphasis onsocial factors within occupational disability. This illustrates the fact that as each model evolves,there seems to be more recognition of commonality in what really works.
Springer
J Occup Rehabil (2007) 17:327–352 341
Research tradition. As a result of the multiple sources of influence on the disability and RTWprocess, research is interdisciplinary and transdisciplinary in nature. That is to say, the researchderives from medical, social, anthropological, physical therapy, psychological, and occupationalspheres.
Individual versus systems focus. The biopsychosocial approach is best classified as relyingon both a systems and individual focus. Again, the rationale is that this model, more than anyother (save perhaps the ecological/case management model), best strives to explain the disabil-ity/RTW continuum by understanding both the individual and the systems involved, and theirinteractions.
Examples of biopsychosocial models. There is clearly not a single biopsychosocial model ofoccupational disability but the convergence of their various characteristics has become apparent.Recent models that can be characterized as biopsychosocial constitute a synthesis of the biomed-ical and social construction models of disability, and assume some type of interaction amonginjured or affected workers, their medical condition, and the multitude of systems in whichthey function. Such syntheses place responsibility for recovery and RTW on the worker andclinicians, and advocate self-management approaches [30, 99], together with both clinical andoccupational interventions. They emphasize early identification of various “flags” for disability,including medical, psychosocial, and system-based secondary prevention.
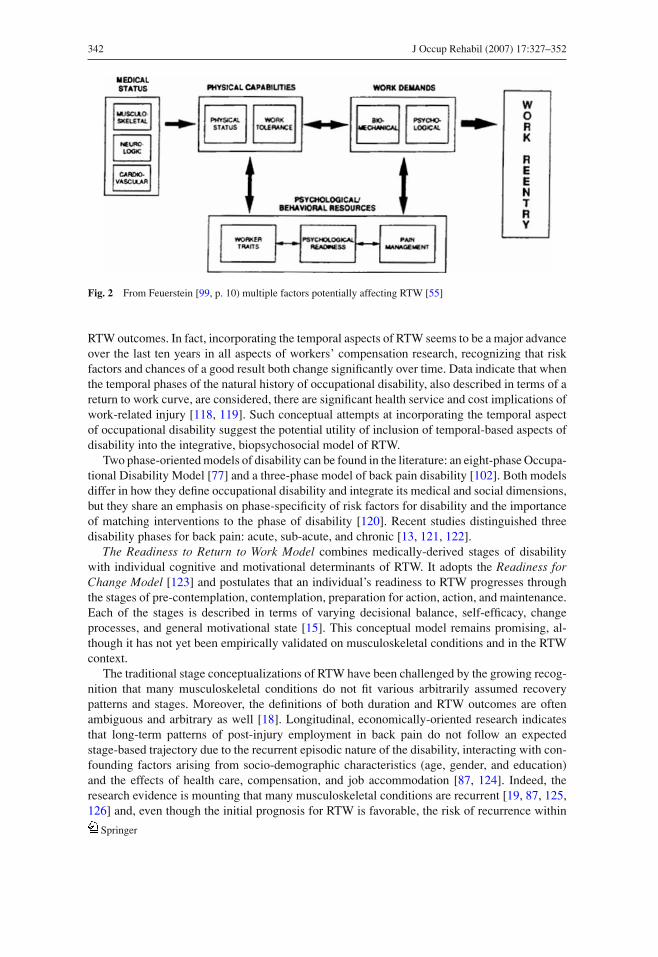
The occupational disability model articulated by Feuerstein [99] is an example of an earlybiopsychosocial approach. That model proposed that RTW was a function of the worker’s currentphysical condition in relation to work demands required on the job. The discrepancy betweenthe physical capabilities of work and work demands was further influenced by: the workers’ability to manage pain; their psychological readiness to work, which could include their fearof reinjury, expectation to RTW, and their ability to manage pain through medication; someother medical or physical therapy approach; and/or the use of behavioral pain managementstrategies. This model was used to construct an evaluation of a worker with a musculoskeletaldisorder, followed by the development of an integrated rehabilitation program that reflectedidentified areas requiring intervention. The model was used as the basis for a comprehensivemultidisciplinary rehabilitation program at the Center for Occupational Rehabilitation at theUniversity of Rochester [98, 113]. While ergonomic factors were addressed in the work demandcomponent of the model, the overall system was not reflected in the model. The rehabilitationprogram did address systems level concerns through the involvement of all members of theteam-nurse case manager, psychologist, occupational physician, physical therapist, ergonomist,and vocational counselor [99] (Fig. 2).
The biopsychosocial model of pain and disability recognizes that the relationships amongpain, physical, psychological, and contextual factors in disability are complex and interactivephenomena [33, 69, 108, 109, 114]. The generically understood biopsychosocial model of RTWhas obtained the best empirical support to date, particularly in the context of non-specific backpain [18, 21, 65, 115, 116] and upper extremity disorders [84, 117]. Moreover, the utility of thebiopsychosocial model for prediction of RTW over the biomedical model in musculoskeletalconditions, such as back pain, has been empirically demonstrated (e.g. [20, 21, 35]). However,systematic research on comparisons of the biopsychosocial model to other models of RTW (suchas ecological/case management or forensic) has not yet been undertaken.
One of the most significant recent contributions to the biopsychosocial models arises fromthe recognition of dynamic, time-based dimensions of the RTW process. There is emergingconceptual, clinical, and empirical consensus that RTW and occupational disability should notbe considered as static employment outcomes [18]. Rather, consideration should be given to thetemporal (time-based) aspects of RTW, patterns of work/disability, and how these factors interactwith the dynamic relationship between an individual and the workplace over time in producing
Springer
342 J Occup Rehabil (2007) 17:327–352
Fig. 2 From Feuerstein [99, p. 10) multiple factors potentially affecting RTW [55]
RTW outcomes. In fact, incorporating the temporal aspects of RTW seems to be a major advanceover the last ten years in all aspects of workers’ compensation research, recognizing that riskfactors and chances of a good result both change significantly over time. Data indicate that whenthe temporal phases of the natural history of occupational disability, also described in terms of areturn to work curve, are considered, there are significant health service and cost implications ofwork-related injury [118, 119]. Such conceptual attempts at incorporating the temporal aspectof occupational disability suggest the potential utility of inclusion of temporal-based aspects ofdisability into the integrative, biopsychosocial model of RTW.
Two phase-oriented models of disability can be found in the literature: an eight-phase Occupa-tional Disability Model [77] and a three-phase model of back pain disability [102]. Both modelsdiffer in how they define occupational disability and integrate its medical and social dimensions,but they share an emphasis on phase-specificity of risk factors for disability and the importanceof matching interventions to the phase of disability [120]. Recent studies distinguished threedisability phases for back pain: acute, sub-acute, and chronic [13, 121, 122].
The Readiness to Return to Work Model combines medically-derived stages of disabilitywith individual cognitive and motivational determinants of RTW. It adopts the Readiness forChange Model [123] and postulates that an individual’s readiness to RTW progresses throughthe stages of pre-contemplation, contemplation, preparation for action, action, and maintenance.Each of the stages is described in terms of varying decisional balance, self-efficacy, changeprocesses, and general motivational state [15]. This conceptual model remains promising, al-though it has not yet been empirically validated on musculoskeletal conditions and in the RTWcontext.
The traditional stage conceptualizations of RTW have been challenged by the growing recog-nition that many musculoskeletal conditions do not fit various arbitrarily assumed recoverypatterns and stages. Moreover, the definitions of both duration and RTW outcomes are oftenambiguous and arbitrary as well [18]. Longitudinal, economically-oriented research indicatesthat long-term patterns of post-injury employment in back pain do not follow an expectedstage-based trajectory due to the recurrent episodic nature of the disability, interacting with con-founding factors arising from socio-demographic characteristics (age, gender, and education)and the effects of health care, compensation, and job accommodation [87, 124]. Indeed, theresearch evidence is mounting that many musculoskeletal conditions are recurrent [19, 87, 125,126] and, even though the initial prognosis for RTW is favorable, the risk of recurrence within
Springer
J Occup Rehabil (2007) 17:327–352 343
the year is high [18, 104]. Therefore, stage or phase-based concepts of RTW need to accountfor the complex and interactive effects of individual demographic and psychosocial factors, incombination with a natural history of the condition (including recurrences), and systemic factorssuch as job accommodation, clinical and occupational interventions, and various benefit supportsystems.
It is important to note that, at present, there is no single unifying biopsychosocial model thatis used in research or clinical application. The inherent problem with biopsychosocial theory isits generic nature and lack of specificity [11]. In fact, this lack of specificity and the fact that themodel is largely based upon many of the strongest features of other prior models, such as thepsychosocial and ecological/ case management models, makes it at times difficult to distinguishas a stand alone, distinct model. Further, this issue is apparent in the current multiplicity ofconceptual and empirical biopsychosocial models of RTW. Nevertheless, based on the currentstate of theory and research in the field, future developments towards a unified and specificmodel, with respect to an underpinning of a biopsychosocial RTW basis, are likely to benefitfrom the inclusion of the following common six components:
1. Personal characteristics. Identification of the modifiable and non-modifiable personal char-acteristics of the individual who sustained injury; and modifiable and non-modifiable char-acteristics of the environment/ social system context in which recovery and RTW occur andtheir interactions;
2. Reciprocal interactions. Reciprocal interaction among multiple key macro-(socio-political,economic, legal, and cultural) and meso-system (workplace, healthcare, compensation, family,peers, and community) factors involved in RTW;
3. Microsystem inter-relationships. Inter-relationships among individual microsystem factors:medical/physical, demographic, and psychosocial interacting with work demands;
4. Expectation factors. Consideration of factors contributing both to expectations of functionaland RTW efficacy such as resiliency, coping and perception of personal and system barriers(RTW perceived by the worker as probable), and facilitators of RTW and expectations ofoutcome including perceived value of work and decisional balance of personal gains andlosses (RTW perceived as beneficial); both resulting in motivation (intent) to RTW;
5. Environmental variables. Inclusion of environmental variables including ergonomic factorsthat are related to work and RTW, and their interactions with both social systems-related andindividual variables;
6. Time factors. Time- or phase-based RTW factor interactions resulting in changing relation-ships among key components of the relationship between the individual and the system toproduce various dimensions of readiness to RTW and patterns of RTW.
Most recent integrative models
Two recent attempts have been made to devise models that integrate many of the most salientfeatures of the above models in order to more comprehensively understand RTW. Both theInstitute of Medicine and the World Health Organization have put fourth such examples that aredescribed below.
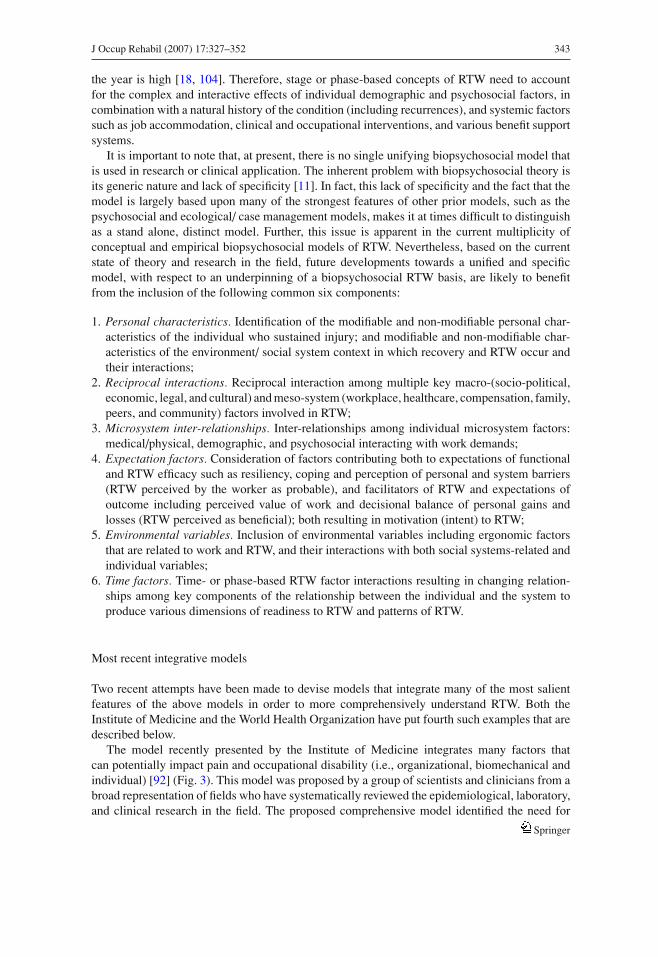
The model recently presented by the Institute of Medicine integrates many factors thatcan potentially impact pain and occupational disability (i.e., organizational, biomechanical andindividual) [92] (Fig. 3). This model was proposed by a group of scientists and clinicians from abroad representation of fields who have systematically reviewed the epidemiological, laboratory,and clinical research in the field. The proposed comprehensive model identified the need for
Springer
344 J Occup Rehabil (2007) 17:327–352
Fig. 3 Institute of Medicine model of disability [131]
understanding each of these factors in order to obtain a comprehensive view of work-relatedmusculoskeletal problems [93].
Most recently, The World Health Organization’s newest model of disability is the InternationalClassification Functioning, Disability, and Health (ICF) Model of Disability [127–129]. It isbiopsychosocial in its intent, though the social elements are ultimately emphasized despite themedical condition residing at the core of the model. Medical and social factors are integratedby proposing disability as a relational phenomenon in which the functional limitations arisingfrom impairment become disabling in the context of broader social and attitudinal factors.Unfortunately, this model is very difficult to examine and operationalize, as many authors havenoted [11, 129], despite early promise and others’ attempts at application [127, 130].
The ICF model has been criticized for failure to specify the content of biopsychosocial theoryunderlying the model, for its atheoretical definition of impairment (e.g., lack of specificity inits underlying biopsychosocial theoretical constructs: and for excessive focus on non-discreteconstructs such as “system harmony” and “universalism”) [11]. The model appears to havebeen based on a social consensus approach to model building rather than on any specifictheory construction method [129]. As such, it may be susceptible to changes arising fromthe evolution of social, economic, and political perspectives, rather than from accumulationof new knowledge through empirical research. The model’s generic nature and problematictheory-building methodology likely limit its direct translation to occupational disability researchand practice. However, attempts to apply it in the development of a general model of physicalactivity [130], and as a clinical problem-solving tool in physical therapy, sports, and rehabilitationmedicine, have emerged [127].
Springer
J Occup Rehabil (2007) 17:327–352 345
The development of a conceptual model of occupational disability that would stimulate in-novative research and practice appears to require a more precise definition of function (i.e.,RTW) than the general theories of disability described thus far. Also, because different oc-cupational outcomes have different predictive models, a theoretical model of RTW does notnecessarily constitute simply the reverse side of the disability model. It is anticipated tohave its own unique features, though sharing some variance with the model of occupationaldisability.
Features of the recent evolution of RTW models
Current RTW conceptualizations have been evolving from generic health and disability theoriesand empirical research in occupational health and rehabilitation into increasingly comprehensive,multidimensional and converging models. The following are six of the key features of the changestoward increased understanding of RTW:
1. Evolution of the psychosocial model. Replacement of the traditional psychopathology-focusedpsychiatric model of disability by the broad-based psychosocial adaptation model, empha-sizing importance of both individual cognitions about disability and its system-based socialcontext, with the emergence of emphasis on cognitively-mediated motivational factors inRTW;
2. Addition and articulation of stage-based models of RTW. Focus on temporal aspects andpatterns of the disablement process by including medical recovery and psychosocial factorsinteracting with the time since injury and readiness to RTW;
3. Expansion of the ecological/case management model. Beyond a traditional sole focus onworkplace disability management to now include interaction among the worker and manykey disability stakeholders including workplace, healthcare, insurance systems, and societyat large;
4. Macrosystem approach to economic factors. Increased focus on the macrosystem of economicfactors in the development and perpetuation of occupational disability;
5. Diminished role of insurance and biomedical models. Greater perspective on the limitationsof the traditional biomedical and insurance models of disability, with many insurance sys-tems shifting away from the question of compensability (proving or disproving disability)to efficiencies in health-care cost management thus bringing the insurance model closer tothe ecological/case management model; the traditional insurance model focusing on medico-legal evidence has been largely relegated to forensic applications in the court system andshould, therefore, be best termed “forensic”; the newest expansions of the forensic modelsunderscore the complex interactions among individual factors such as motivations and cog-nitions, and social system factors thus bringing this approach closer to the biopsychosocialmodel;
6. Increased support and reliance upon the biopsychosocial model. The increase stems fromtwo main forces: (i) evidentiary support in healthcare and RTW literature, and (ii) increasedrecognition of, and efforts made towards, operationalization of both the depth of the multidi-mensional systems involved and the individuals, and the breadth of the interactions betweenthe systems and the individuals.
Springer
346 J Occup Rehabil (2007) 17:327–352
Research challenges and conclusions for future construction of RTW models
Based upon our review, we have concluded that a model of occupational disability and RTWshould possess certain qualities for it to be useful to researchers, clinicians, and affected workers.There are many stakeholders interested in the outcomes of studies on etiological factors affectingoccupational disability and approaches to prevent and manage it.
Future models that add to our understanding of occupational disability and return towork as they relate to musculoskeletal disorders should aspire to possess the following sixfeatures:
1. Multivariable. The model should include independent variables that have been empiri-cally shown to play some type of role in occupational disability and RTW. Future re-search does need to identify independent risk factors and their interactions in prospectivestudies.
2. Parsimonious. For scientific and clinical purposes, the model should help delineate potentialrelations among risk factors, yet not be so complex as to prevent research that tests the model’stheoretical and clinical validity using valid measures of variables.
3. Valid. The model should hold up to scientific rigor in terms of empirical tests of whether thefactors in combination predict or explain occupational disability and RTW.
4. Generalizable. The model should apply to a diverse group of workers with musculoskeletaldisorders. While there may be variations for different types of musculoskeletal disorders andcertain features of the legal, healthcare and compensation systems, the explanatory power ofa model should be applicable to a diverse group of workers and countries.
5. Reliable. The relationships among variables in the model should be repeatedly observed whenstudied by different research groups in different countries and within a given country.
6. Ecologically Valid. The number of variables, their measurement, and inter-relationships shouldinvolve measures that are of importance for understanding and modifying occupational dis-ability and facilitating RTW in real life, as per a number of stakeholders, so that the infor-mation collected and the interventions that evolve will actually be used to improve the stateof the art related to evaluation, prevention, and rehabilitation of occupational disability, andRTW.
The existing and newly developing models need to be evaluated against these above criteria.Notably, each model has served to improve our understanding of RTW, guide interventionand research approaches, and/or to help stimulate reform at a systems/societal level. Out ofour current evaluation of the past and present state of RTW models, the above criteria weredeveloped. Future model evaluation will benefit from use of these criteria to determine whichmodels will survive the test of time and evidentiary support.
The emerging conceptual models of RTW represent more comprehensive approaches thanwhat has been proposed in the past. The new models are transdisciplinary, integrative, interactive,and multidimensional. They focus on the interaction between the individual and the multiplesystems within which an individual functions and the interactions among these systems. All ofthese models propose dynamic interactions and some incorporate a temporal dimension. Bothclinical and occupational perspectives on disability are typically incorporated. Furthermore,both physical and psychological capacity dimensions of occupational disability are consideredimportant in RTW. The empirical validation of these models is an emerging trend and futureresearch will serve to refine them.
There are a number of challenges for research and practice that these models need to address.First of all, the models themselves are “emerging” and are not yet constructed well enough
Springer
J Occup Rehabil (2007) 17:327–352 347
to allow for consistent research validation. Research on the models’ generalizability, efficiency,internal consistency, and utility remains to be completed. Definitions of RTW need to be clarifiedand consistently operationalized so that they not only constitute a socially and contextuallyconstructed target, but are dependent on the system and stakeholders in question [14]. Researchersalso need to have some type of standard operational definitions of various work outcomes [16].We have known that RTW definitions based on a single RTW episode need to be replaced bythe identification of patterns of RTW, and supplemented by other sources of data includingduration of disability and cost; yet, this continues to be a future goal of research and is rarelyan aspect of a model of occupational disability and RTW [18]. Despite the absence of an agreedupon RTW taxonomy, researchers across several disciplines related to RTW recognized theimportance of both safe and sustained return to work. However, there is still no consensus basedon evidence for which dimensions provide us with the most valid measures of outcome. Notably,a multi-method, multi-perspective approach in measurement of RTW outcomes, ranging fromself-report through behavioral to economic measures, is likely the best one to use to apply to thiscomplex, multi-dimensional, and time-dependent construct. Relatedly, while the importance ofmulti-system interaction in RTW has been recognized in the new models, the methodology ofresearch on multi-system interactions is new and not well articulated. Both qualitative [76] andquantitative approaches appear to be helpful, using path analysis and other statistical modelingapproaches.
Several models of RTW have emerged over the past two decades. These have evolved fromconceptual understandings of pain, physical functioning, biopsychosocial research, and theirimpact on function. Newer models have been more expansive in their focus on potential factorsthat can impact occupational disability and RTW. While there is a role for many of thesemodels, at this point in time there is a need for a parsimonious multi-variable model withmajor explanatory qualities for enhancing our understanding of occupational disability and,consequently, improving prevention and management.
Acknowledgements The authors wish to express appreciation for thoughts on the economic perspective providedby Dr. William Johnson and for initial comments on this paper provided by Dr.Glenn Pransky. We also thank bothanonymous reviewers of our paper for their helpful suggestions. Supported in part by Grant Nos. K05 MH01107,3R01 MH46402, and 2R01 DE10713 from the National Institutes of Health, and in part by the Research Secretariatof Worksafe BC.
References
1. U.S. Department of Labor. Lost-worktime injuries and illnesses: Characteristics and resulting time awayfrom work, 1998, Publication USDL 00–115. Washington, D.C.: U.S. Department of Labor; 2000.
2. ICD9.chrisendres.com. 2006 ICD-9-CM: Medical Dictionary. 2006. Accessed 01/08/2007 [Available from:http://medical.webends.com/kw/musculoskeletal%20system]
3. Noy D. Department of Classics – Masters degree in ancient philosophy and mythology ancient medicine: Mythand practice. 2002 [cited 2006 August 15]; Available from: http://www.lamp.ac.uk/ ∼ noy/Medicine1.htm
4. McKee B. Disability culture timeline: A brief history. 2003 [cited 2006 August 15]; Available from:http://www.chairgrrl.com/DisabilityTimeline/index.htm
5. Descartes R. Treatise of Man; 1629.6. Descartes R. Discourse on method and the meditations. Translated by John Veitch. Amherst, NY: Prometheus
Books; 1989.7. Melzack R, Wall PD. Pain mechanisms: A new theory. Science 1965;50:971–9.8. Brody H. The systems view of man: Implications for medicine, science, and ethics. Perspect Biol Med
1973;17(1):71–92.9. Engel GL. The need for a new medical model: A challenge for biomedicine. Science 1977;196(4286):129–
36.10. Melzack R. Pain and stress: A new perspective. In: Gatchel RJ, Turk DC (eds). Psychosocial factors in pain:
Critical perspectives. New York: Guilford Publications, Inc.; 1999.
Springer
348 J Occup Rehabil (2007) 17:327–352
11. Imrie R. Demystifying disability: A review of the international classification of functioning, disability andhealth. Sociol Health Illn 2004;26(3):287–305.
12. Young AE, Roessler RT, Wasiak R, McPherson KM, Poppel MNM, Anema JR. A developmental conceptu-alization of return to work. J Occup Rehabil 2005;15(4):557–68.
13. Krause N, Dasinger LK, Deegan LJ, Rudolph L, Brand RJ. Psychosocial job factors and return-to-workafter compensated low back injury: A disability phase-specific analysis. Am J Ind Med 2001;40(4):374–92.
14. Krause N, Frank JW, Dasinger LK, Sullivan T, Sinclair SJ. Determinants of duration of disability and returnto work after work-related injury and illness: Challenges for future research. Am J Ind Med 2001;40:464–84.
15. Franche RL, Krause N. Readiness for return to work following injury or illness: Conceptualizing the inter-personal impact of health care, workplace, and insurance factors. J Occup Rehabil 2002;12(4):233–56.
16. Young A, Wasiak R, Roessler R, McPherson K, Anema J, van Poppel M. Return-to-work outcomes followingwork disability: Stakeholder motivations, interests and concerns. J Occup Rehabil 2005;15(4):543–56.
17. Stowell AW, McGeary DD. Musculoskeletal injury: A three-stage continuum from cause to disability todecision. In: Schultz IZ, Gatchel RJ (eds). Handbook of complex occupational disability claims: Early risk,identification, intervention, and prevention. New York: Springer; 2005. p. 117–39.
18. Linton S, Gross D, Schultz I, Main C, Cote P, Pransky G, Johnson W. Prognosis and the identification of work-ers risking disability: Research issues and directions for future research. J Occup Rehabil 2005;15(4):469–74.
19. Baldwin ML, Johnson WG, Butler RJ. The error of using returns-to-work to measure the outcomes of healthcare. Am J Ind Med 1996;29(632–641).
20. Crook J, Milner R, Schultz IZ, Stringer B. Determinants of occupational disability following a low backinjury: A critical review of the literature. J Occup Rehabil 2002;12(4):277–94.
21. Schultz IZ, Crook JM, Berkowitz J, Meloche GR, Milner R, Zuberbier OA. Biopsychosocial multivariatepredictive model of occupational low back disability. Spine 2002;27(23):2720–5.
22. Bickenbach JE, Chatterji S, Badley EM, Ustun TB. Models of disablement, universalism and the internationalclassification of impairments, disabilities and handicaps. Soc Sci Med 1999;48:1173–87.
23. Tate D, Pledger C. An integrative conceptual framework of disability. Am Psychol 2003;58:289–95.24. Olkin R, Pledger C. Can disability studies and psychology join hands? A new model of disability. Am Psychol
2003;58:296–304.25. Verbrugge LM, Jette AM. The disablement process. Soc Sci Med 1994;38(1):1–14.26. Abberley P. The concept of oppression and the development of a social theory of disability. Disabil Handicap
Soc 1987;2(1):5–19.27. Meyerson L. The social psychology of the physical disability: 1948 and 1988. J Soc Issues 1988;44(1):173–
88.28. Hughes B, Paterson K. The social model of disability and the disappearing body: Towards a sociology of
impairment. Disabil Handicap Soc 1997;12(3):325–40.29. Fougeyrollas P, Bouregard L. Disability: An interactive person-environment social creation. Handbook of
disability studies. London: Sage; 2001.30. Schultz IZ, Crook J, Fraser K, Joy PW. Models of diagnosis and rehabilitation in musculoskeletal pain-related
occupational disability. J Occup Rehabil 2000;10(4):271–93.31. Fine M, Asch A. Disability beyond stigma: Social interaction, discrimination, and activism. J Soc Issues
1988;44(1):3–21.32. Leibowitz G. Organic and biophysical theories of behavior. J Dev Phys Disabil 1991;3:201–43.33. Turk DC. Biopsychosocial perspective on chronic pain. In: Gatchel RJ, Turk DC (eds). Psychological
approaches to pain management. New York: Guilford Press; 1996. p. 3–32.34. Kelly M, Field D. Comments on the rejection of the biomedical model in sociological discourse. Med Sociol
News 1994;19(3):34–7.35. Hunt D, Zuberbier OA, Kozlowski A, Berkowitz J, Schultz IZ, Milner RA, Crook JM, Turk DC. Are
components of a comprehensive medical assessment predictive of work disability following an episode ofoccupational low back trouble? Spine 2002;27(23):2715–9.
36. Robinson JP, Turk DC, Loeser JD. Pain, impairment, and disability in the AMA guidelines. J Law MedEthics 2004;32(2):315–26.
37. Cocchiarella L, Andersoon GBJ (eds). Guides to the evaluation of permanent impairment. 5th ed. Chicago,Illinois: AMA Press; 2001.
38. Cocchiarella L, Turk MA, Andersson G. Improving the evaluation of permanent impairment. J Am MedAssoc 2000;283:532–3.
39. Pransky G, Shaw WS, Franche R, Clarke A. Disability prevention and communication among workers,physicians, employers, and insurers: Current models and opportunities for improvement. Disabil Rehabil2004;26(11):625–34.
Springer
J Occup Rehabil (2007) 17:327–352 349
40. Boorse C. Concepts of health. In: Van de Veer D, Regan T (eds.), Health care ethics: An introduction.Philadelphia: Temple University Press; 1987. p. 359–93.
41. Polatin PB, Kinney RK, Gatchel RJ, Lillo E, Mayer TG. Psychiatric illness and chronic low-back pain. Themind and the spine – Which goes first? Spine 1993;18(1):66–71.
42. Shaw WS, Feuerstein M, Lincoln AE, Miller VI, Wood PM. Case management services for work-related upperextremity disorders: Integrating workplace accommodation and problem-solving. AAOHN J 2001;49:378–89.
43. Pergola T, Salazar MK, Graham KY, Brines J. Case management services for injured workers: Providers’perspectives. AAOHN J 1999;47(9):397–404.
44. Salazar MK, Graham KY. Evaluation of a case management program. AAOHN J 1999;47(9):416–23.45. Tsai JH, Salazar MK, Graham KY, Brines J. Case management for injured workers: A descriptive study
using a record review. AAOHN J 1999;47(9):405–15.46. Brines J, Salazar MK, Graham KY, Pergola T. Return to work experience of injured workers in a case
management program. AAOHN J 1999;47(8):365–72.47. Green-McKenzie J, Parkerson J, Bernacki E. Comparison of workers’ compensation costs for two cohorts
of injured workers before and after the introduction of managed care. J Occup Environ Med 1998;40:568–72.
48. Bernacki EJ, Tsai SP. Ten years’ experience using workers’ compensation case management system to controlworkers’ compensation costs. J Occup Environ Med 2003;45(5):508–19.
49. Daubert v. Merrell Dow Pharmaceuticals. 61 U.S.L.W. 4805; 1993.50. Wikipedia. Daubert Standard. 2006 [cited 2006 August 13]; Available from: http://en.wikipedia.org/
wiki/Daubert Standard51. Schultz IZ, Brady DO. Psychological injuries at trial: American Bar Association: Tort trial and insurance
practice section; 2003.52. Hadjistavropoulos T, Bieling P. File review consultation in the adjudication of mental health and chronic
pain disability claims. Consult Psychol J: Pract Res 2001;52(1):53–63.53. Sherman JF, Ohrback R. Objective and subjective measurement of pain: Current approaches to forensic
applications. In: Young G, Kane AW, Nicholson K (eds.), Psychological knowledge in court: PTSD, pain,and TBI. New York: Springer; 2006. p. 193–214.
54. Dersh J, Polatin PB, Leeman G, Gatchel RJ. The management of secondary gain and loss in medicolegalsettings: Strengths and weaknesses. J Occup Rehabil 2004;14(4):267–79.
55. Schultz IZ, Gatchel R (eds.). Handbook of complex occupational disability claims: Early risk identification,intervention, and prevention. New York: Springer; 2005.
56. Baril R, Berthelette D. Les composantes et les determinants organisationnels des interventions de maintiendu lien d’emploi en enterprise. Montreal: Institut de recherche en sante et en securite du travail du Quebec;2000; Rapport No. R-238.
57. Schultz IZ, Crook J, Meloche GR, Berkowitz J, Milner R, Zuberbier OA, Meloche W. Psychosocial fac-tors predictive of occupational low back disability: Towards development of a return-to-work model. Pain2004;107:77–85.
58. Karjalainen K, Malmivaara A, van Tulder M, Roine R, Jauhiainen M, Hurri H, Koes B. Multidisciplinarybiopsychosocial rehabilitation for subacute low back pain among working age adults (Review): The CochraneDatabase of Systematic Reviews; 2003.
59. Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol Rev 1977;84:191–215.
60. Bandura A. The social foundations of thought and action. Englewood Cliffs: Prentice-Hall; 1986.61. Sandstrom J, Esbjornsson E. Return to work after rehabilitation. The significance of the patient’s own
prediction. Scand J Rehabil Med 1986;18:29–33.62. Cole DC, Mondloch MV, Group EPM. Listening to workers: How recovery expectations predict outcomes.
Can Med Assoc J 2002;166:749–54.63. Turner J, Franklin G, Fulton-Kehoe D, Sheppard L, Wickizer T, Wu R, Gluck J, Egan K. Worker recovery
expectations and fear-avoidance predict work disability in a population-based workers’ compensation backpain sample. Spine 2006;31(6):682–9.
64. Burton AK, Tilloston KM, Main CJ, Hollis S. Psychosocial predictors of outcome in acute and subchroniclow back trouble. Spine 1995;20:722–8.
65. Linton S. A review of psychological risk factors in back and neck pain. Spine 2000;25:1148–56.66. Turk DC, Gatchel RJ. Psychosocial assessment of chronic occupational musculoskeletal disorders. In: Mayer
TM, Gatchel RJ, Polatin PB, (eds.), Occupational musculoskeletal disorders: Function, outcomes & evidence.Philadelphia: Lippincott, Williams & Wilkins; 2000. p. 587–608.
67. Jensen M, Romano J, Turner J, Good A, Wald L. Patient beliefs predict patient functioning: Further supportfor a cognitive-behavioral model of chronic pain. Pain 1999;81:95–104.
Springer
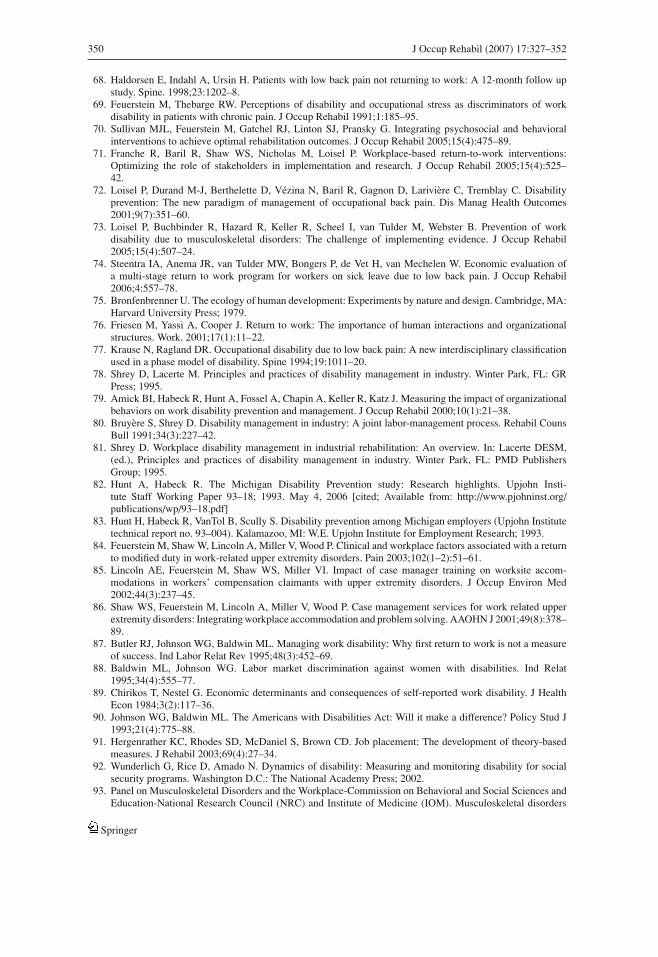
350 J Occup Rehabil (2007) 17:327–352
68. Haldorsen E, Indahl A, Ursin H. Patients with low back pain not returning to work: A 12-month follow upstudy. Spine. 1998;23:1202–8.
69. Feuerstein M, Thebarge RW. Perceptions of disability and occupational stress as discriminators of workdisability in patients with chronic pain. J Occup Rehabil 1991;1:185–95.
70. Sullivan MJL, Feuerstein M, Gatchel RJ, Linton SJ, Pransky G. Integrating psychosocial and behavioralinterventions to achieve optimal rehabilitation outcomes. J Occup Rehabil 2005;15(4):475–89.
71. Franche R, Baril R, Shaw WS, Nicholas M, Loisel P. Workplace-based return-to-work interventions:Optimizing the role of stakeholders in implementation and research. J Occup Rehabil 2005;15(4):525–42.
72. Loisel P, Durand M-J, Berthelette D, Vezina N, Baril R, Gagnon D, Lariviere C, Tremblay C. Disabilityprevention: The new paradigm of management of occupational back pain. Dis Manag Health Outcomes2001;9(7):351–60.
73. Loisel P, Buchbinder R, Hazard R, Keller R, Scheel I, van Tulder M, Webster B. Prevention of workdisability due to musculoskeletal disorders: The challenge of implementing evidence. J Occup Rehabil2005;15(4):507–24.
74. Steentra IA, Anema JR, van Tulder MW, Bongers P, de Vet H, van Mechelen W. Economic evaluation ofa multi-stage return to work program for workers on sick leave due to low back pain. J Occup Rehabil2006;4:557–78.
75. Bronfenbrenner U. The ecology of human development: Experiments by nature and design. Cambridge, MA:Harvard University Press; 1979.
76. Friesen M, Yassi A, Cooper J. Return to work: The importance of human interactions and organizationalstructures. Work. 2001;17(1):11–22.
77. Krause N, Ragland DR. Occupational disability due to low back pain: A new interdisciplinary classificationused in a phase model of disability. Spine 1994;19:1011–20.
78. Shrey D, Lacerte M. Principles and practices of disability management in industry. Winter Park, FL: GRPress; 1995.
79. Amick BI, Habeck R, Hunt A, Fossel A, Chapin A, Keller R, Katz J. Measuring the impact of organizationalbehaviors on work disability prevention and management. J Occup Rehabil 2000;10(1):21–38.
80. Bruyere S, Shrey D. Disability management in industry: A joint labor-management process. Rehabil CounsBull 1991;34(3):227–42.
81. Shrey D. Workplace disability management in industrial rehabilitation: An overview. In: Lacerte DESM,(ed.), Principles and practices of disability management in industry. Winter Park, FL: PMD PublishersGroup; 1995.
82. Hunt A, Habeck R. The Michigan Disability Prevention study: Research highlights. Upjohn Insti-tute Staff Working Paper 93–18; 1993. May 4, 2006 [cited; Available from: http://www.pjohninst.org/publications/wp/93–18.pdf]
83. Hunt H, Habeck R, VanTol B, Scully S. Disability prevention among Michigan employers (Upjohn Institutetechnical report no. 93–004). Kalamazoo, MI: W.E. Upjohn Institute for Employment Research; 1993.
84. Feuerstein M, Shaw W, Lincoln A, Miller V, Wood P. Clinical and workplace factors associated with a returnto modified duty in work-related upper extremity disorders. Pain 2003;102(1–2):51–61.
85. Lincoln AE, Feuerstein M, Shaw WS, Miller VI. Impact of case manager training on worksite accom-modations in workers’ compensation claimants with upper extremity disorders. J Occup Environ Med2002;44(3):237–45.
86. Shaw WS, Feuerstein M, Lincoln A, Miller V, Wood P. Case management services for work related upperextremity disorders: Integrating workplace accommodation and problem solving. AAOHN J 2001;49(8):378–89.
87. Butler RJ, Johnson WG, Baldwin ML. Managing work disability: Why first return to work is not a measureof success. Ind Labor Relat Rev 1995;48(3):452–69.
88. Baldwin ML, Johnson WG. Labor market discrimination against women with disabilities. Ind Relat1995;34(4):555–77.
89. Chirikos T, Nestel G. Economic determinants and consequences of self-reported work disability. J HealthEcon 1984;3(2):117–36.
90. Johnson WG, Baldwin ML. The Americans with Disabilities Act: Will it make a difference? Policy Stud J1993;21(4):775–88.
91. Hergenrather KC, Rhodes SD, McDaniel S, Brown CD. Job placement: The development of theory-basedmeasures. J Rehabil 2003;69(4):27–34.
92. Wunderlich G, Rice D, Amado N. Dynamics of disability: Measuring and monitoring disability for socialsecurity programs. Washington D.C.: The National Academy Press; 2002.
93. Panel on Musculoskeletal Disorders and the Workplace-Commission on Behavioral and Social Sciences andEducation-National Research Council (NRC) and Institute of Medicine (IOM). Musculoskeletal disorders
Springer
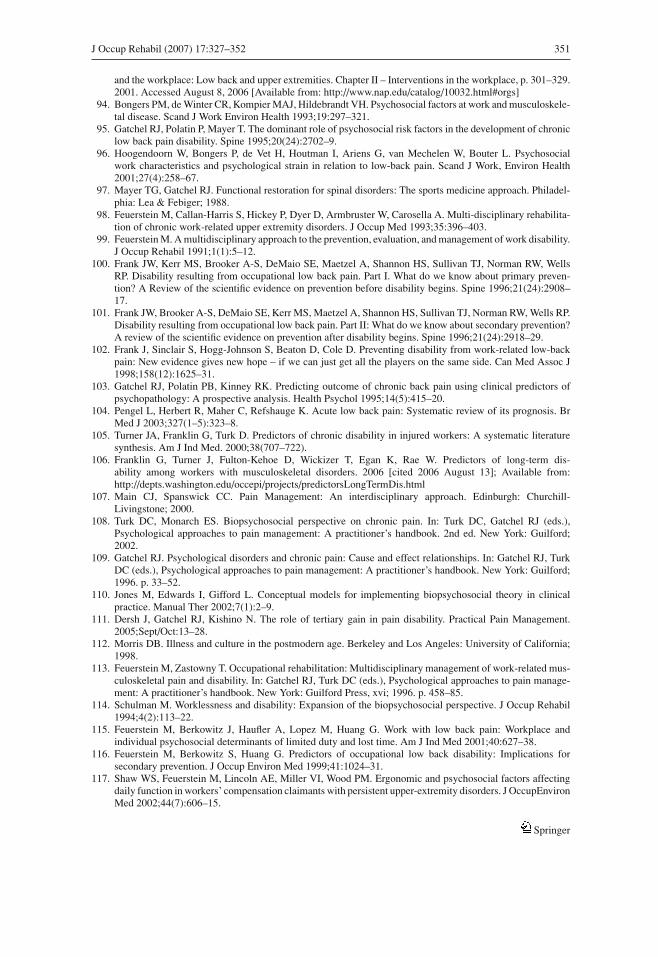
J Occup Rehabil (2007) 17:327–352 351
and the workplace: Low back and upper extremities. Chapter II – Interventions in the workplace, p. 301–329.2001. Accessed August 8, 2006 [Available from: http://www.nap.edu/catalog/10032.html#orgs]
94. Bongers PM, de Winter CR, Kompier MAJ, Hildebrandt VH. Psychosocial factors at work and musculoskele-tal disease. Scand J Work Environ Health 1993;19:297–321.
95. Gatchel RJ, Polatin P, Mayer T. The dominant role of psychosocial risk factors in the development of chroniclow back pain disability. Spine 1995;20(24):2702–9.
96. Hoogendoorn W, Bongers P, de Vet H, Houtman I, Ariens G, van Mechelen W, Bouter L. Psychosocialwork characteristics and psychological strain in relation to low-back pain. Scand J Work, Environ Health2001;27(4):258–67.
97. Mayer TG, Gatchel RJ. Functional restoration for spinal disorders: The sports medicine approach. Philadel-phia: Lea & Febiger; 1988.
98. Feuerstein M, Callan-Harris S, Hickey P, Dyer D, Armbruster W, Carosella A. Multi-disciplinary rehabilita-tion of chronic work-related upper extremity disorders. J Occup Med 1993;35:396–403.
99. Feuerstein M. A multidisciplinary approach to the prevention, evaluation, and management of work disability.J Occup Rehabil 1991;1(1):5–12.
100. Frank JW, Kerr MS, Brooker A-S, DeMaio SE, Maetzel A, Shannon HS, Sullivan TJ, Norman RW, WellsRP. Disability resulting from occupational low back pain. Part I. What do we know about primary preven-tion? A Review of the scientific evidence on prevention before disability begins. Spine 1996;21(24):2908–17.
101. Frank JW, Brooker A-S, DeMaio SE, Kerr MS, Maetzel A, Shannon HS, Sullivan TJ, Norman RW, Wells RP.Disability resulting from occupational low back pain. Part II: What do we know about secondary prevention?A review of the scientific evidence on prevention after disability begins. Spine 1996;21(24):2918–29.
102. Frank J, Sinclair S, Hogg-Johnson S, Beaton D, Cole D. Preventing disability from work-related low-backpain: New evidence gives new hope – if we can just get all the players on the same side. Can Med Assoc J1998;158(12):1625–31.
103. Gatchel RJ, Polatin PB, Kinney RK. Predicting outcome of chronic back pain using clinical predictors ofpsychopathology: A prospective analysis. Health Psychol 1995;14(5):415–20.
104. Pengel L, Herbert R, Maher C, Refshauge K. Acute low back pain: Systematic review of its prognosis. BrMed J 2003;327(1–5):323–8.
105. Turner JA, Franklin G, Turk D. Predictors of chronic disability in injured workers: A systematic literaturesynthesis. Am J Ind Med. 2000;38(707–722).
106. Franklin G, Turner J, Fulton-Kehoe D, Wickizer T, Egan K, Rae W. Predictors of long-term dis-ability among workers with musculoskeletal disorders. 2006 [cited 2006 August 13]; Available from:http://depts.washington.edu/occepi/projects/predictorsLongTermDis.html
107. Main CJ, Spanswick CC. Pain Management: An interdisciplinary approach. Edinburgh: Churchill-Livingstone; 2000.
108. Turk DC, Monarch ES. Biopsychosocial perspective on chronic pain. In: Turk DC, Gatchel RJ (eds.),Psychological approaches to pain management: A practitioner’s handbook. 2nd ed. New York: Guilford;2002.
109. Gatchel RJ. Psychological disorders and chronic pain: Cause and effect relationships. In: Gatchel RJ, TurkDC (eds.), Psychological approaches to pain management: A practitioner’s handbook. New York: Guilford;1996. p. 33–52.
110. Jones M, Edwards I, Gifford L. Conceptual models for implementing biopsychosocial theory in clinicalpractice. Manual Ther 2002;7(1):2–9.
111. Dersh J, Gatchel RJ, Kishino N. The role of tertiary gain in pain disability. Practical Pain Management.2005;Sept/Oct:13–28.
112. Morris DB. Illness and culture in the postmodern age. Berkeley and Los Angeles: University of California;1998.
113. Feuerstein M, Zastowny T. Occupational rehabilitation: Multidisciplinary management of work-related mus-culoskeletal pain and disability. In: Gatchel RJ, Turk DC (eds.), Psychological approaches to pain manage-ment: A practitioner’s handbook. New York: Guilford Press, xvi; 1996. p. 458–85.
114. Schulman M. Worklessness and disability: Expansion of the biopsychosocial perspective. J Occup Rehabil1994;4(2):113–22.
115. Feuerstein M, Berkowitz J, Haufler A, Lopez M, Huang G. Work with low back pain: Workplace andindividual psychosocial determinants of limited duty and lost time. Am J Ind Med 2001;40:627–38.
116. Feuerstein M, Berkowitz S, Huang G. Predictors of occupational low back disability: Implications forsecondary prevention. J Occup Environ Med 1999;41:1024–31.
117. Shaw WS, Feuerstein M, Lincoln AE, Miller VI, Wood PM. Ergonomic and psychosocial factors affectingdaily function in workers’ compensation claimants with persistent upper-extremity disorders. J OccupEnvironMed 2002;44(7):606–15.
Springer

352 J Occup Rehabil (2007) 17:327–352
118. Hagen K, Thune O. Work incapacity from low back pain in the general population [Epidemiology]. Spine1998;23(19):2091–5.
119. Williams DA, Feuerstein M, Durbin D, Pezzullo J. Costs across the natural history of disability in occupationallow back pain. Spine 1998;23(21):2329–36.
120. Franche R, Krause N. Readiness for return to work following injury or illness. In: Schultz I, Gatchel R (eds.),Handbook of complex occupational disability claims: Early risk identification, intervention, and prevention.New York: Springer; 2005. p. 67–92.
121. Dasinger LK, Krause N, Thompson PJ, Brand RJ, Rudolph L. Doctor proactive communication, return towork recommendation, and duration of disability after a workers’ compensation low back injury. J OccupEnviron Med 2001;43(6):515–25.
122. McIntosh G, Frank J, Hogg-Johnson S, Bombardier C. Prognostic factors for time receiving workers’compensation benefits in a cohort of patients with low back pain. Spine 2000;25(2):147–57.
123. Prochaska JO, DiClemente CC. Stages and processes of self-change in smoking: Toward an integrativemodel. J Consult Clin Psychol 1983;51:390–5.
124. Johnson WG, Baldwin ML, Butler RJ. Back pain and work disability: The need for a new paradigm. IndRelat 1998;37(1):9–34.
125. Pransky G, Benjamin K, Hill-Fotouhi C, Fletcher KE, Himmelstein J, Katy JN. Work-related outcomes inoccupational low back pain: A multidimensional analysis. Spine 2002;27:864–70.
126. Wasiak R, Pransky G, Verma S, Webster B. Recurrence of low back pain: Definition-sensitivity analysisusing administrative data. Spine 2003;28:2283–91.
127. Steiner WA, Ryser L, Huber E, Uebelhart D, Aeschlimann A, Stucki G. Use of the ICF model as a clinicalproblem-solving tool in physical therapy and rehabilitation medicine. Phys Ther 2002;82(11):1098–107.
128. World Health Organization. International Classification of Functioning, Disability, and Health (ICF): ICFfull report. Geneva, Switzerland: World Health Organization; 2001.
129. Dahl T. International classification of functioning, disability and health: An introduction and discussion ofits potential impact on rehabilitation services and research. J Rehabil Med 2002;34:201–4.
130. van der Ploeg HP, van der Beek AJ, van der Woude LH, van Mechelen W. Physical activity for people witha disability: A conceptual model. Sports Med 2004;34(10):639–49.
131. Panel on Musculoskeletal Disorders and the Workplace-Commission on Behavioral and Social Sciences andEducation-National Research Council (NRC) and Institute of Medicine (IOM). Musculoskeletal disordersand the workplace: Low back and upper extremities. Executive Summary, p 3, figure. ES.1. 2001. AccessedOctober 12, 2006 [Available from: http://newton.nap.edu/books/0309072840/html/3.html]
Springer