Embed Size (px)
Citation preview
Paediatric Palliative Care Manual for Home Bases Carers 89
Module 9: Skin Problems Module Objectives
To review the most common types of skin problem experienced by children with HIV
To equip trainees with an understanding of potential complications of skin
problems in children with HIV
To review the treatment and management of skin problems To demonstrate that trainees have a vital role to play in preventing and
managing skin problems through education, assessment, management and referral
Slide Presentation: Skin Problems
Skin Problems
Paediatric Palliative CareFor Home Based Carers
Funded by
British High Commission, Pretoria
Small Grant Scheme
1. Welcome trainees and introduce yourself. Give a brief background in to your area of practice, role and experience. Ask the trainees for their experiences of caring for children with skin problems, how they have managed them and what they would hope to learn from this session. Encourage trainees to ask questions and share their thoughts throughout.
Skin ProblemsCommon in children with HIV
Often conditions common in all children but more severe
Often first sign of HIV infection / HIV disease progressing
Include: Rashes Slow HealingItchy skin Boils or abscessesPainful sores Drug reactionsDry skin
2. Skin problems are common in children with HIV, many of which are conditions seen in uninfected children. Yet in HIV-positive children, these are usually more severe, more prolonged and more difficult to treat. The risk of developing skin problems increases as disease progresses and the immune system weakens. They are therefore a sign that disease may be advancing. They may often be the first indication of HIV disease. Signs and symptoms vary greatly.
Paediatric Palliative Care Manual for Home Base Carers 90
Issues for a Child Hygiene dependent on carer
‘Pick up’ infections
Distressing symptoms
Secondary infections (scratching, picking)
May infect others
Increased risk of skin infections as HIV disease progresses
3. Children are more susceptible to skin infections than adults – they are dependent on the carer for ensuring good hygiene (e.g. bathing, hand washing). As children develop, they explore and are unaware of unhygienic practices – they will play with anything! The symptoms of skin infections can be particularly distressing, particularly for children. They do not understand the risks of scratching and picking sores and children’s skin problems tend to become secondarily infected, particularly as children’s nails may not be clean. In the case of contagious skin problems, play mates or carers may also be infected. The risk of children acquiring skin problems increases with disease progression.
Preventing Skin ProblemsDaily washing with soap and water
Dry skin well
Moisturise skin
Wash nappies and clothes regularly
Keep Nails short and clean
Expose skin to sun and air when possible
©TALC
4. Prevention is better than cure. All children, but particularly those with HIV, should be washed daily with soap and water to remove germs from the body which may lead to skin infection. Dry skin may crack and breakdown which allows germs to enter. This may be prevented through thorough drying and the use of moisturisers. Nappies and clothes need to be washed regularly otherwise these will harbour infection. Nails are a perfect breeding site for germs and nails should be kept short and clean. Sunlight and fresh air is extremely important for the maintenance of healthy skin and can help to prevent infections thrive on damp, dirty conditions.
ThrushExtremely common in children with HIV
Caused by Candida infection
Commonly found in nappy area or skin folds
May be painful for a child
May lead to secondary infection
©TALC
5. Ask trainees to describe what they see in the picture and what they think is the cause. The bright pink skin in the fold of this baby’s neck is due to candidiasis or thrush. It is extremely common in children with HIV. It is caused by the same fungus which causes oral thrush, Candida albicans. It is most commonly found in the nappy area or skin folds, is a vivid pink/red rash with a clearly demarcated border. It may be painful for the child and may become secondarily infected.
Paediatric Palliative Care Manual for Home Bases Carers 91
Managing ThrushExpose skin to sun and air
Clean area with water
Gentian Violet or Nystatin
Pain relief (Paracetamol)
Wash nappies and clothes well
Refer for medication if no improvement
©TALC
6. Ask trainees how they would manage thrush. The skin must be kept clean and dry and ideally exposed to the sun and air. Covering the thrush with nappies and clothes will not help and may even make the thrush worse. Gentian Violet or Clotrimazole ointment should be applied until the rash resolves. Nappies and clothes must be washed and dried well to prevent re-infection. If the thrush does not improve, the child should be referred for oral medication. Pain may be helped with regular Paracetamol.
Seborrhoeic dermatitis
Infection/ Inflammation of the skin
Highly suggestive of HIV infection
Thick, yellow scales on scalp, face, nappy area, behind ears
May be itchy and sore
May become secondarily infected ©TALC
7. Ask trainees to describe what they see in the picture. The child has seborrhoeic dermatitis which occurs frequently in children with HIV. It is usually more severe than seen in uninfected children and is highly suggestive of HIV infection. Thick, yellow scales occur on the scalp, face, nappy area and behind the ears. It may be very distressing for children and scratching may lead to secondary infection of the dermatitis.
Managing SeborrhoeicDermatitis
Ensure child has clean, short nails
Wash skin using aqueous cream
Moisturise skin
Pain relief (Paracetamol)
Refer for Chlorpheniraminemaleate
Refer as antibiotics or steroids may be required
8. Management involves hydrating the skin, symptom relief and preventing secondary infections. Parents/carers should be taught and encouraged to moisturise the child as often as possible which helps the skin to heal and prevents breakdown. Short, clean nails are essential to minimise the chance of secondary infection and skin damage during scratching. Paracetamol and Chlorpheniramine maleate can be very effective at relieving symptoms. Parents should be warned that Chlorpheniramine maleate may make the child sleepy. The child should be referred where skin is infected or there is no improvement with the above measures.
Paediatric Palliative Care Manual for Home Base Carers 92
Tinea InfectionsKnown as Ringworm
Flat, round, scaly, dry patches
Commonly found on face, trunk, extremities and head (with loss of hair)
May become severe, large, pus-filled patches
Common and highly infectious
©TALC
CDC/Dr Georg
9. Ask trainees to describe what they see in the picture and how they would manage it in the community. Tinea (also known as Ringworm) are fungal infections, most of which grow in the form of a ring. They may appear on any part of the body but most commonly on the face, scalp, between the fingers and toes and the trunk. They usually itch and may become secondarily infected. Ringworm is seen in ALL children but is more common and more severe in HIV-infected children. It is highly infectious, and will be passed amongst groups of children in close contact with one another.
Management of Ring WormWash infected area with soap and water
Ensure thorough hand washing
Apply Whitfield’s Ointment
Refer for oral Griseofulvin treatment
(1-3 months!)
10. Washing the infected area with soap and water daily may help but children with HIV will probably need more than this. Clotrimazole cream should be used if available. Whitfield’s ointment is cheaper, although less effective. Parents must be informed that the ointment will need to be applied for some time before the ringworm will improve. Oral Griseofulvin is the ideal but needs to be taken for 2-3 months! Thorough hand washing is essential to prevent ringworm from spreading.
Dry Skin and ItchingExtremely common in children with HIV
May be very distressing to child
May lead to skin infections
Avoid use of soaps
Bath child in bath oils
Moisturise skin with emulsifying ointments in stead
Keep child’s nails clean and short
11. Children with HIV commonly get dry, itchy skin. This is not fully understood but may be due to an inflammatory reaction to HIV itself. Symptoms of pruritis (itching) are not only distressing to the child but result in scratching. Dry skin easily becomes cracked. Both result in infections. The child needs regular moisturising and bathing in bath oils. Avoidance of soaps can help to prevent drying out the skin. Local creams may have been found to be effective in alleviating symptoms. As discussed earlier, the child’s nails should be short and clean to prevent infections whilst scratching.

Paediatric Palliative Care Manual for Home Bases Carers 93
Chicken PoxCaused by Varicella Zoster virus
Rash, developing to crusts
Found all over body, particularly on trunk
Commonly itchy and painful
Highly contagious (spread by contact with sores and secretions)
Much more severe than usual chicken poxCDC/J.D. Millar
12. Ask trainees to describe what they see in the picture. Like all children, HIV-infected children can get chicken pox. Caused by the Varicella Zoster Virus, it is characterised by a vesicular rash all over the body. The vesicles then develop in to crusts. It is commonly extremely itchy and painful. Chickenpox can be very severe indeed in HIV infected children and has dangerous complications which will be discussed. Both the sores themselves and secretions (e.g. coughing, saliva) are highly contagious and this poses a great risk to other vulnerable people in the household (e.g. young babies, elderly, pregnant women and HIV positive people.
Managing ChickenpoxPain relief
Thorough hand washing
Keep child away from young, sick, or elderly people
Acyclovir treatment
Symptom relief with Chlorpheniraminemaleate, Calamine
Wash clothes well
Antibiotic treatment if infected
13. Symptom relief and infection control are central to managing a child with chickenpox. Paracetamol, Chlorpheniramine maleate and Calamine are usually effective although stronger analgesia and sedation may be required in severe cases. Local topical remedies may also have been shown to have soothing effects. Infection control must be taught to parents/carers, particularly where vulnerable people are in contact with the child. Ideally, the child should not be in contact with these people. HIV-negative children are not usually treated for chickenpox but HIV-positive children require Acyclovir due to their immune suppression and the severity of the chickenpox. Children with secondary infections will require antibiotics.
Complications of Chicken poxComplications may occur
Secondary bacterial infectionsHaemorrhagic chickenpoxPneumoniaEncephalitis
Refer to Clinic/Hospital depending
on presence of danger signs
14. In extremely severe cases of chickenpox, complications of chickenpox may occur. Any child with Danger Signs as discussed in Module 15: Danger Signs, must be referred to a clinic or hospital immediately.

Paediatric Palliative Care Manual for Home Base Carers 94
Shingles (Herpes Zoster)Child has had chicken pox before
If immune system weakens, the chicken pox virus returns a s shingles
Extremely painful blisters, in clusteror line along the line of a nerve
Usually down leg, arm, neck, chest, face, may involve eye
Suggestive of HIV in a child
©TALC
©TALC
15. Ask trainees to describe what they see in the picture and what causes it. Both pictures show children with shingles, having vesicular rashes across the arm (top picture) and chest (bottom picture). Infection with the Varicella Zoster virus most commonly causes chicken pox in children. When the child recovers, the virus stays in the body, remaining dormant in the nerves. If the virus is reactivated at a later date, it can cause shingles which is characterised by painful ulcers along the ‘line’ of a nerve and do not cross the midline. The virus may be reactivated when the immune system is weakened. Therefore, whilst shingles is not usually seen in HIV-negative children, HIV-positive children who have had chickenpox before can get shingles. Shingles in a child is strongly indicative of HIV.
Management of ShinglesAnalgesia (Paracetamol, Codeine)
Oral/IV acyclovir
Isolate child from sick, young, elderly
Hand washing
For itch: Calamine, Chlorpheniramine maleate
If infected: Antibiotic treatment (Amoxycillin / Flucloxacillin
16. Shingles can be extremely painful and analgesia must be central to its management. Paracetamol should be given regularly and the child may need Codeine in addition. The pain is due to nerve involvement and can therefore be very severe and difficult to treat. The pain can continue after the vesicles have disappeared. Sometimes the child will need medicine called carbamazepine to help this pain. Treatment for shingles is with oral Acyclovir or with IV Acyclovir for children with severe cases or who are unable to take medication by mouth. Infection control is essential as although contact with the vesicles will not cause shingles, it may result in chickenpox. Antibiotics may be required for secondary infections.
ScabiesCommon in all children
Very itchy bumps all over body
Caused by tiny mites which tunnel under the skin
Commonly between fingers and toes, in wrist-folds, around waist, on genitals, palms & soles of feet
Scratching causes infection, producing sores with pus
Symptom relief with Calamine, Chlorpheniramine maleate
17. Scabies is common in all children but occurs often in children with HIV. It is caused by a tiny mite (Sarcoptes scabei). The female burrows under the skin to lay her eggs which hatch into larvae within a few days. A few weeks later, intense itching occurs when the mites are plenty in number! Itchy papules occur, never above the neck. Scabies is passed through close personal contact with infected people. Where a child is itching, trainees should ask whether others in the house are also itching as this usually suggests scabies. Parents/carers must be encouraged to complete the child’s medication which is topical benzyl benzoate lotion. Ideally, the whole family should be treated. All clothes and bedding should be washed thoroughly.
Paediatric Palliative Care Manual for Home Bases Carers 95
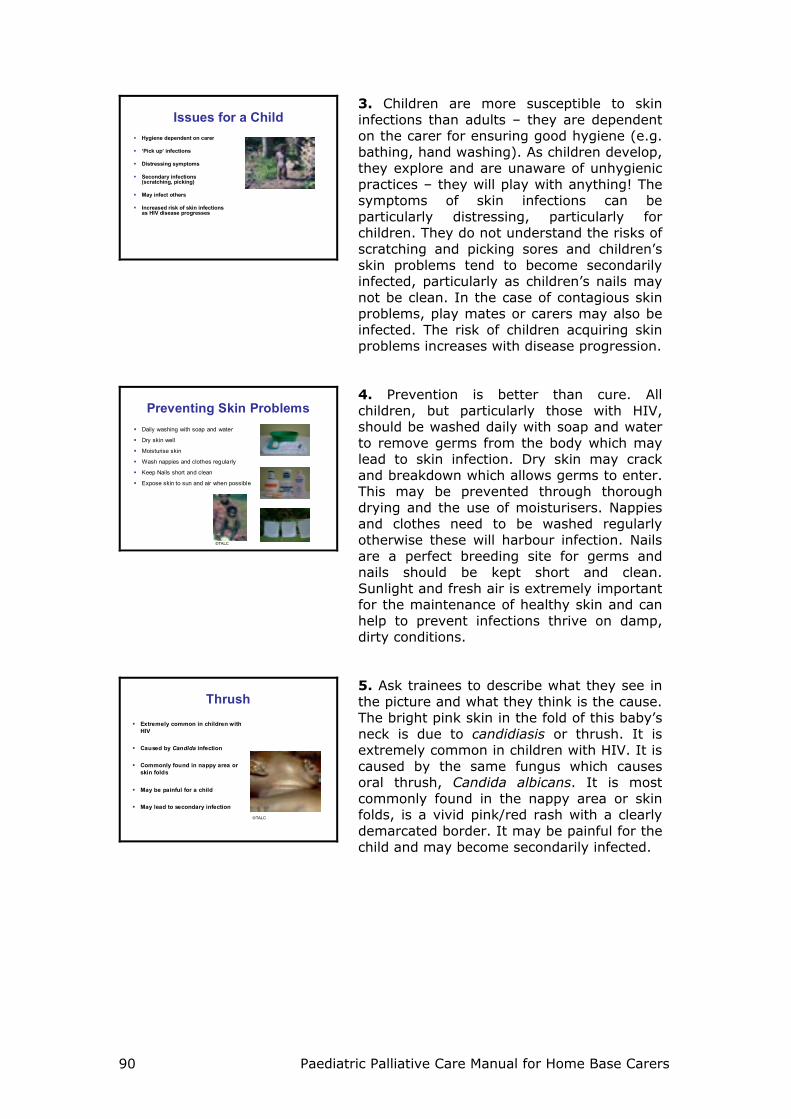
AbscessesChildren with HIV commonly get absce sses
Any child with an abscess must be referredfor inve stigation and treatment
©TALC©TALC
18. Ask trainees what they notice about the children in the pictures. Both have large abscesses on the neck (left) and scalp (right). Children with HIV may suffer from recurrent or multiple abscesses and these are suggestive of HIV infection. The abscesses are usually very painful. Children should be referred to the clinic or hospital for further investigation and correct management which may involve antibiotics and/or incision and drainage. This should only ever be done by those trained to do it and use of strict infection control measures is vital.
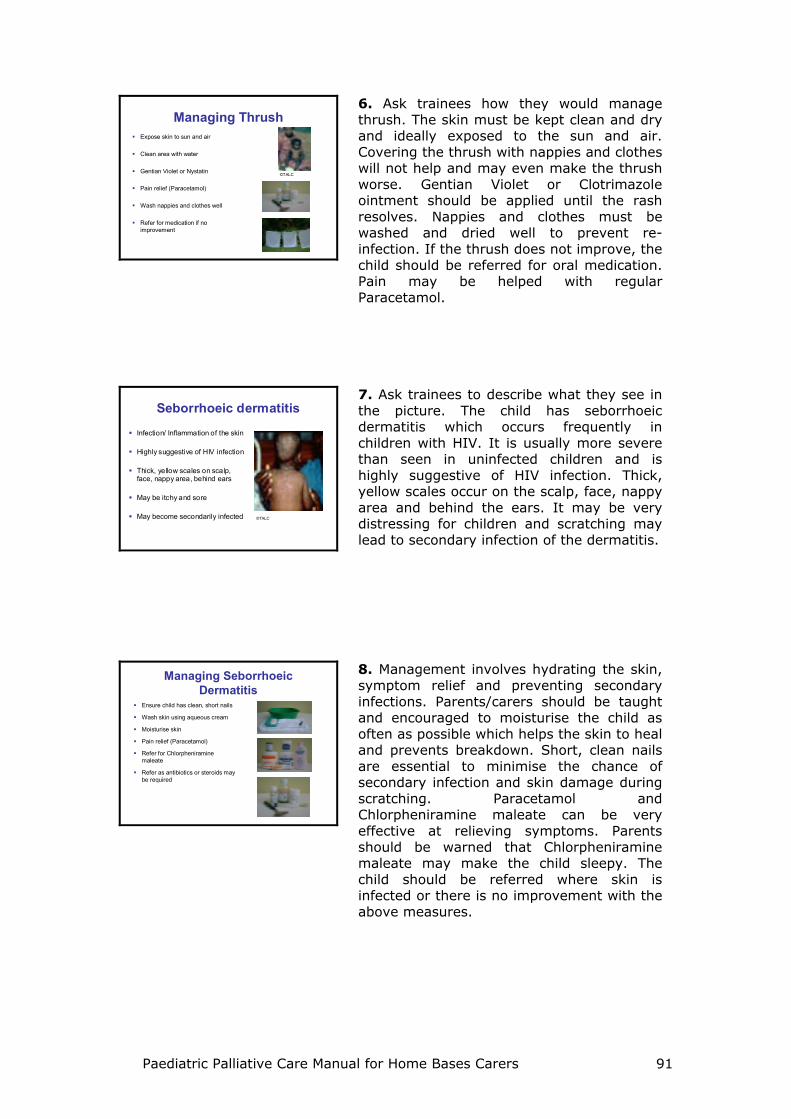
MolluscumFlesh-coloured, dome-shaped growths
Vary in size from 3mm – 1cm
Often indicate advanced HIV disease
Commonly occur on the face and can be extremely disfiguring
Refer child
19. Molluscum contagiosum is a viral infection. Flesh-coloured or ‘pearly’ growths occur in different sizes. Whilst these may sometimes itch, children are not usually disturbed by them. However, the growths may become widespread, large in size and extremely disfiguring. Children may be stigmatised against as a result. Molluscum is usually associated with a weak immune system and advancing disease. The child should be referred for appropriate treatment .
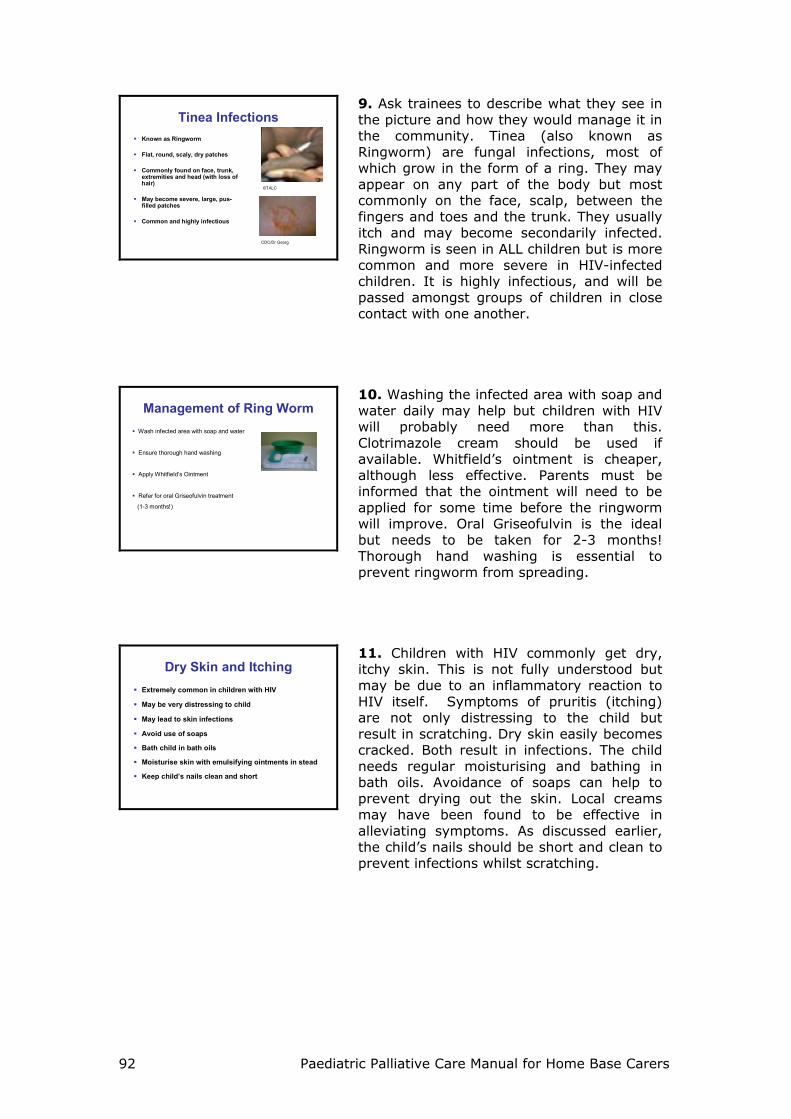
Drug ReactionsChildren with HIV take lots of drugs
A child may react to these drugs:Exfoliating skin rash FeverSevere painRisk of dehydration and malnutrition
More common in infected children:Taking Co-trimoxazleTaking anti-TB therapyStarting ARVs (eg Nevirapine, Abacavir)
Refer immediately
©TALC
20. Ask trainees to describe what they see in the picture. This child has Stevens-Johnson Syndrome, a severe drug reaction characterised by exfoliating skin and fever. It is extremely painful and the child is at great risk of dehydration. This child had taken medication for TB although other drugs may cause it too. The child needs immediate referral. Drug reactions may not always be this severe but children with any drug reaction need referring for management of the rash and a decision as to whether to stop or continue the drug. This should never be decided in the home but by professionals in the clinic/hospital. Most children can be referred to paediatric out-patients but a child with a rash like that in the picture needs to be referred urgently to hospital as they are seriously ill.
Paediatric Palliative Care Manual for Home Base Carers 96
Skin BreakdownChildren with HIV are are morelikely to get skin breakdown
Due to:MalnutritionImmobilitySkin infections
This can be prevented through:Good nutri tionRegular turning and good skin care for immobile, bed ridden childrenTreatment of skin infections
Picture of Skin Breakdown
©TALC
21. Malnutrition, immobility and skin infections place children with HIV at great risk of skin breakdown which results in pain and/or further infection. Good nutrition plays a major role in keeping skin healthy and preventing breakdown. Parents/carers need teaching about the importance of turning immobile, bed ridden children and preventing pressure sores. Skin infections need treating appropriately as early as possible to prevent further breakdown.
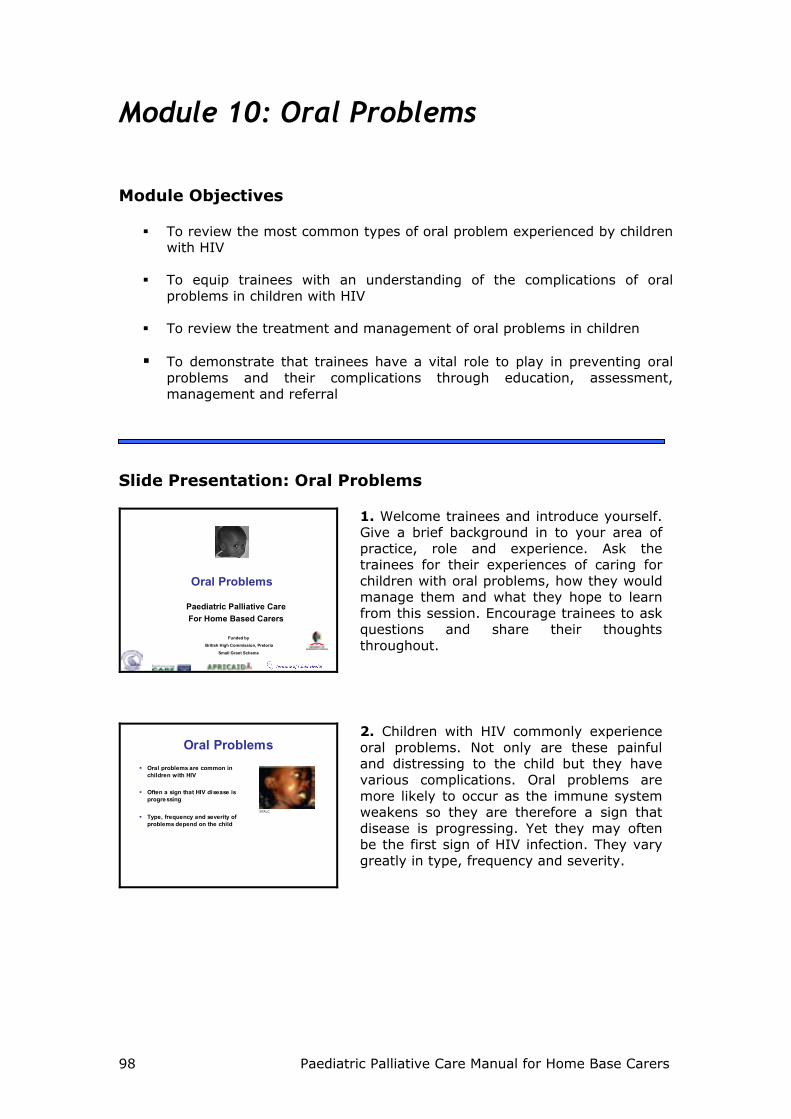
Kaposi’s SarcomaMost common type of cancer affecting people with HIV
Less common in children than adults but still seen
Pink, red, purple or brown/black, painless, lesions
May start on face, mouth, gums, palate or penis
©TALC
22. Ask trainees to describe what they see in the picture. This 4 year old boy has Kaposi’s sarcoma. He is very thin and ill, with a widespread rash with purple plaques and spots. He also has a swollen abdomen. Although not as common as seen in adults, children with HIV can get Kaposi’s sarcoma. It is a malignancy, characterised by red/purple/brown plaques and spots, often all over the body.
Kaposi’s sarcomaMay lead to skin infections and painful ulcers
May spread to:GI tract ( assess for blood in stool or abdominal pain)Lungs (assess for dry, productive cough)
Care is usually palliative
ARVs may be of benefitt
23. Kaposi’s sarcoma plaques may become infected or develop as painful ulcers. It may also affect the internal organs. It has a poor prognosis. Care is usually palliative although there is some evidence that ARVs can be of benefit. A child with Kaposi’s sarcoma is at risk of discrimination due to its association with HIV/AIDS. Plaques are usually less obvious on dark skin.
Management of Skin Problems
Good Hygiene
Symptom Relief (Paracetamol, Calamine, Chlorpheniramine maleate)
Antibiotic and Antifungal treatment
Prevent secondary infections (short nails, Gentian Violet)
Treatment for secondary infections
24. Ask trainees to describe the general management of skin problems in children, drawing on the issues raised in this module. Discussion points should include Infection control, Symptom relief, Treatment for the infection itself and Prevention/Management of secondary infections. Trainees are in a position to teach parents/carers how to prevent skin problems, refer children with for appropriate management and support parents/carers, assessing whether symptoms are controlled and the condition improves.

Paediatric Palliative Care Manual for Home Bases Carers 97
SummaryChildren with HIV commonly get a wide range of skin problems
These can cause intense itching, pain and distress
Preventing skin problems through good hygiene and care is extremely important
Delaying treatment for skin problems makes treatment more difficult and complications may occur
25. Children with HIV are susceptible to a wide variety of skin problems. Many of these are seen in uninfected children but occur with greater severity and prolonged duration in infected children. Prevention is essential through good nutrition and good hygiene. Parents/carers need to be taught how to ensure this within their home. Symptoms of skin problems may be very distressing to the child and effective symptom control is essential not only for alleviating suffering but for preventing further infections through scratching. Skin problems must be dealt with as soon as possible with appropriate treatment as they may be difficult to treat, damage the immune system further and complications may occur.
Paediatric Palliative Care Manual for Home Base Carers 98
Module 10: Oral Problems Module Objectives
To review the most common types of oral problem experienced by children with HIV
To equip trainees with an understanding of the complications of oral
problems in children with HIV
To review the treatment and management of oral problems in children To demonstrate that trainees have a vital role to play in preventing oral
problems and their complications through education, assessment, management and referral
Slide Presentation: Oral Problems
Oral Problems
Paediatric Palliative CareFor Home Based Carers
Funded by
British High Commission, Pretoria
Small Grant Scheme
1. Welcome trainees and introduce yourself. Give a brief background in to your area of practice, role and experience. Ask the trainees for their experiences of caring for children with oral problems, how they would manage them and what they hope to learn from this session. Encourage trainees to ask questions and share their thoughts throughout.
Oral ProblemsOral problems are common in children with HIV
Often a sign that HIV disease is progressing
Type, frequency and severity of problems depend on the child
©TALC
2. Children with HIV commonly experience oral problems. Not only are these painful and distressing to the child but they have various complications. Oral problems are more likely to occur as the immune system weakens so they are therefore a sign that disease is progressing. Yet they may often be the first sign of HIV infection. They vary greatly in type, frequency and severity.
Paediatric Palliative Care Manual for Home Bases Carers 99
IssuesOral problems are commonly painful and distressing for a child
A child may refuse to drink or eat
Children are therefore at risk of dehydration and/or malnutrition
Early diagnosis and treatment is essential to prevent complications
©TALC
©TALC
3. Oral problems in children with HIV are a great concern for a number of reasons. They are commonly painful and cause distress. Eating or drinking may be extremely sore or cause a burning sensation. As discussed in Modules 6 & 13, children with HIV are already at risk of malnutrition and dehydration and oral problems further increase this risk. The key to managing oral problems and preventing suffering or complications is early diagnosis and treatment. If trainees are familiar with some of the signs and symptoms of common oral problems and possible complications, they may play a vital role in referring and managing children.
Oral ThrushCommon in children
Caused by candida infection
White patches on roof of mouth, inside cheeks, back of tongue or throat
May be very painful
May be in corners of mouth or in throat
©TALC
4. Ask trainees what they see in this picture, if they can name this condition, how often they see it and how they would manage it in the home. The child in the picture has a white coating on her tongue and the mucosa of her mouth. She has severe oral thrush (candidiasis). Oral thrush is common in all young babies but less common after 6 months of age. It is very common in HIV infected children and is usually more severe and more difficult to treat than in uninfected babies. It is often associated with severe immune suppression and symptomatic HIV disease. It can sometimes be confused with milk in the mouth but thrush cannot be easily scraped off like milk and there may be bleeding when trying this. Thrush may also be in the oesophagus (the tube from the mouth to the stomach). In this case the child may complain of difficulty swallowing.
Oral ThrushPain is distressing for child
May be difficult to swallow
Child may not want/ be unable to eat or drink
May lead to dehydration and/or malnutrition
If severe, recurrent or in throat, suggestive of HIV
©TALC
5. The picture shows another child with severe oral thrush. Oral thrush can be extremely painful and distressing for the child. The child may find it painful and difficult to swallow and is therefore at risk of becoming dehydrated and malnourished. Children can die quickly from dehydration. A child with HIV may already be malnourished and thrush may make this more severe. Malnutrition will make the child even more susceptible to infections which he may not be able to fight. Severe, recurrent cases of oral thrush or oesophageal thrush are highly suggestive that the child has HIV.
Paediatric Palliative Care Manual for Home Base Carers 100
Management of Oral ThrushWash hands
Wet a clean soft cloth with salt water and use to wash child’s mouth
Refer for:Daktarin oral gel (4-6 hourly x 7-14 days) and /orNystatin 6 hourly
Try both if severe/persistent
If N/A, paint with Gentian Violet
Avoid feeding for 20 minutes after medication
6. Ask trainees how they are managing oral thrush in their communities. Local remedies are commonly used (e.g. paw paw). Early, appropriate management of thrush is essential if it is to be treated effectively and complications are to be prevented. Hands must be washed before and after contact with the child’s mouth as thrush is highly infectious. Salt or bicarbonate of soda solutions help to keep the mouth clean and prevent further infection. Miconazole gel and Clotrimazole suspension is effective but may not be available locally. Gentian Violet is less effective but much cheaper. It should be painted on to the lesions twice daily. It is important that parent/carers are taught to avoid feeding for 20 minutes after medication otherwise the medication will be washed down and be of little help.
Management of Oral ThrushIf breast fed, check mother’s breasts for thrush
If thrush present, treat breasts with nystatin or Gentian Violet
Advise mother to wash breasts after feeds
If bottle fed, change to cup and spoon
©TALC
7. If a child is breast fed, it is extremely important to check whether the mother has thrush on her breasts. Otherwise, a child who has been treated for thrush may be re-infected during breastfeeding. The thrush may also be painful for the mother and sores may become secondarily infected. Stress to trainees that this is a potential route of HIV transmission too - children whose HIV status is unknown have an increased chance of being infected through breastfeeding if the breasts are infected with thrush. The mother must be treated as soon as possible and be advised to wash breasts after feeds. If only one breast is infected, the other breast should be used for breastfeeding (she should continue to empty the other breast). Feeding bottles may well be harbouring candida so these should be changed to a cup and spoon.
Management of Oral ThrushEnsure regular pain relief to relieve discomfort and encourage drinking/eating
Encourage small, frequent drinks and food to prevent dehydration & malnutrition
8. As stated earlier, thrush can be extremely painful and regular pain relief should be given not only to reduce suffering but in order to make it easier for the child to eat and drink. Dehydration and malnutrition may be prevented in this way. Pain relief should be given regularly (Paracetamol every 4-6 hours with a maximum of 4 doses in 24 hours), preferably timing doses to be given half an hour before feeds/meals. This can make eating and drinking much less painful for a child. Small frequent sips of drinks and soft food should be encouraged.
Paediatric Palliative Care Manual for Home Bases Carers 101
Management of Oral ThrushIf thrush is no better / worseor swallowing is painful:
refer child to clinic for investigations & medication
9. If the child’s condition does not improve and/or the child is finding it difficult to eat and drink, the child must be referred for further treatment and investigation. Relapses of severe thrush are common and may need more intensive treatment. It is extremely important that the child gets this. Delaying referral may make the thrush even harder to treat. One major concern with local remedies is that they may not always be sufficient and lead to a delay in seeking drug treatment. If the child finds it difficult to swallow, there may be oesophageal candidiasis although it cannot be seen. The child MUST be referred. Oral fluconazole may be required.
Preventing Oral ThrushThorough washing of bottles, teats, cups, spoons
Daily Tooth brushing
Breastfeeding
Nutritious foods
Vitamins
©TALC
10. Prevention is better than cure. Thrush is very common in children with HIV and there are important steps to preventing it. Trainees have a vital role to play in teaching parents/carers how to prevent thrush occurring in the first place. Feeding bottles are ideal breeding grounds for thrush and MUST be sterilised. In reality, families may not have access to sterilisation fluids and local policies must be encouraged. If sterilisation cannot be guaranteed, feeding with cups should be encouraged instead of bottles and teats, even for young babies. Tooth brushing helps to remove germs which may otherwise cause infection, while nutritious foods, vitamins and breastfeeding all encourage good immune responses. Breastfeeding also avoids use of non-sterile feeding implements.
Herpes SimplexPainful, small blisters or open sores on lips or in mouth
May also be around nose
May be accompanied by fever
Herpes >1 month = AIDS defining condition CDC/J.D.Milar
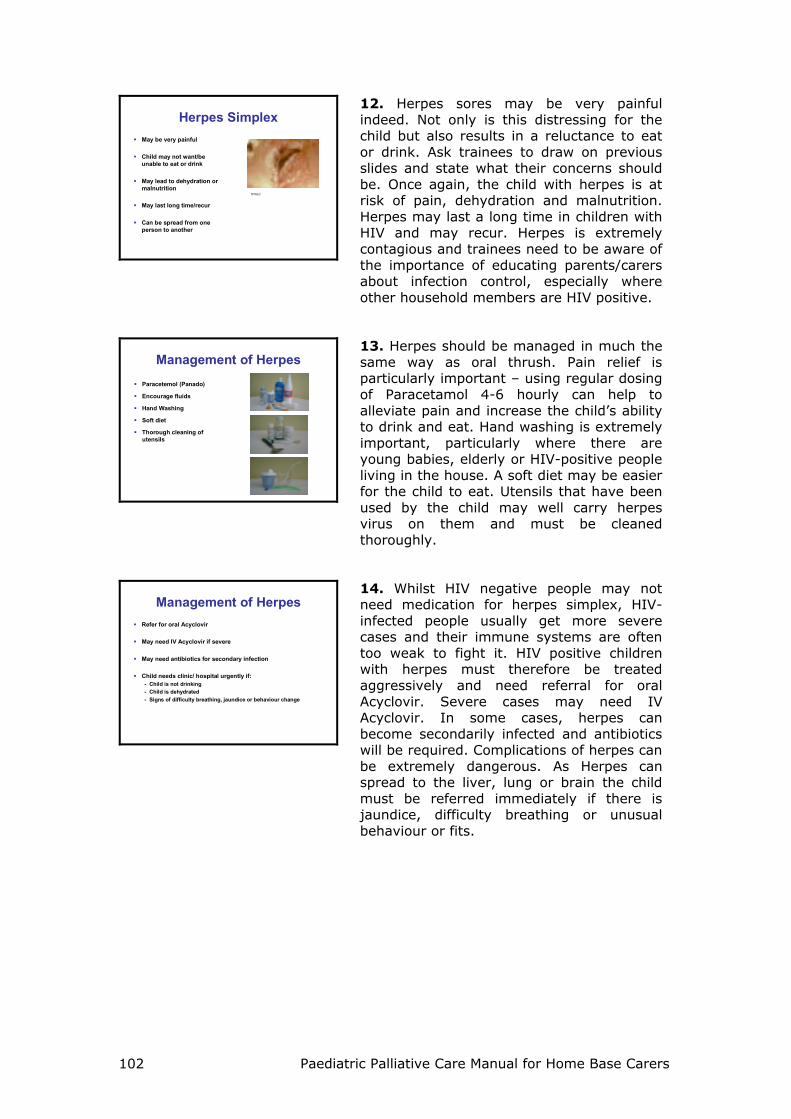
11. Ask trainees to describe what they see and name the condition. Herpes simplex is a virus which causes small blisters or open sores on the lips or in the mouth. Any child may have herpes simplex but it is much more common in HIV-infected children and cases are much more severe and more difficult to treat, as in this picture. In severe cases, the sores may also spread to around the nose. Sores may be accompanied by fever. The sores or blisters are very obvious to others and the child may be stigmatised against. If a child has herpes simplex for longer than one month, this is classed as an AIDS-defining condition.
Paediatric Palliative Care Manual for Home Base Carers 102
Herpes SimplexMay be very painful
Child may not want/be unable to eat or drink
May lead to dehydration or malnutrition
May last long time/recur
Can be spread from one person to another
©TALC
12. Herpes sores may be very painful indeed. Not only is this distressing for the child but also results in a reluctance to eat or drink. Ask trainees to draw on previous slides and state what their concerns should be. Once again, the child with herpes is at risk of pain, dehydration and malnutrition. Herpes may last a long time in children with HIV and may recur. Herpes is extremely contagious and trainees need to be aware of the importance of educating parents/carers about infection control, especially where other household members are HIV positive.
Management of HerpesParacetemol (Panado)
Encourage fluids
Hand Washing
Soft diet
Thorough cleaning of utensils
13. Herpes should be managed in much the same way as oral thrush. Pain relief is particularly important – using regular dosing of Paracetamol 4-6 hourly can help to alleviate pain and increase the child’s ability to drink and eat. Hand washing is extremely important, particularly where there are young babies, elderly or HIV-positive people living in the house. A soft diet may be easier for the child to eat. Utensils that have been used by the child may well carry herpes virus on them and must be cleaned thoroughly.
Management of HerpesRefer for oral Acyclovir
May need IV Acyclovir if severe
May need antibiotics for secondary infection
Child needs clinic/ hospital urgently if:- Child is not drinking- Child is dehydrated- Signs of difficulty breathing, jaundice or behaviour change
14. Whilst HIV negative people may not need medication for herpes simplex, HIV-infected people usually get more severe cases and their immune systems are often too weak to fight it. HIV positive children with herpes must therefore be treated aggressively and need referral for oral Acyclovir. Severe cases may need IV Acyclovir. In some cases, herpes can become secondarily infected and antibiotics will be required. Complications of herpes can be extremely dangerous. As Herpes can spread to the liver, lung or brain the child must be referred immediately if there is jaundice, difficulty breathing or unusual behaviour or fits.
Paediatric Palliative Care Manual for Home Bases Carers 103
Preventing HerpesNutritious Foods
Vitamins
Hand Washing
Avoid touching mouth
Avoid kissing if herpes present
Thorough cleaning of feeding implements and utensils
15. Like all the infections being discussed, strengthening the immune system can help to prevent cases of herpes and good nutrition and vitamins are extremely important in this. Hand washing is vital if herpes is not to be passed from one person to another. Parents/carers need to be taught this. Touching sores should be avoided although this is difficult to enforce in children. Kissing should certainly be avoided when blisters/sores are present. Again, feeding implements must cleaned thoroughly as they may be harbouring herpes virus.
Mouth UlcersPainful blisters on tongue or in mouth
Size 2-3mm to 2-3 cm
Occur as single blister or in ‘clusters’
Occur on roof of mouth, tongue, inner cheek, tonsils
Child may be reluctant to eat or drink
©TALC
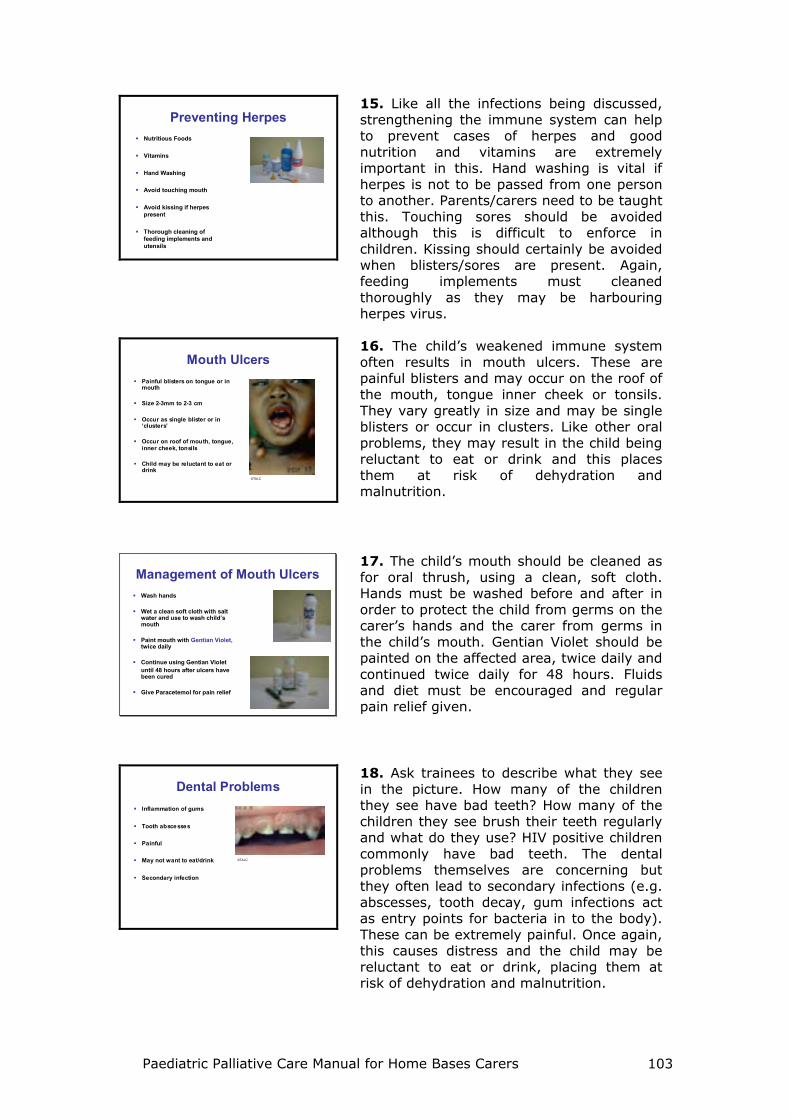
16. The child’s weakened immune system often results in mouth ulcers. These are painful blisters and may occur on the roof of the mouth, tongue inner cheek or tonsils. They vary greatly in size and may be single blisters or occur in clusters. Like other oral problems, they may result in the child being reluctant to eat or drink and this places them at risk of dehydration and malnutrition.
Management of Mouth UlcersWash hands
Wet a clean soft cloth with salt water and use to wash child’s mouth
Paint mouth with Gentian Violet,twice daily
Continue using Gentian Violetuntil 48 hours after ulcers have been cured
Give Paracetemol for pain relief
17. The child’s mouth should be cleaned as for oral thrush, using a clean, soft cloth. Hands must be washed before and after in order to protect the child from germs on the carer’s hands and the carer from germs in the child’s mouth. Gentian Violet should be painted on the affected area, twice daily and continued twice daily for 48 hours. Fluids and diet must be encouraged and regular pain relief given.
Dental ProblemsInflammation of gums
Tooth abscesses
Painful
May not want to eat/drink
Secondary infection
©TALC
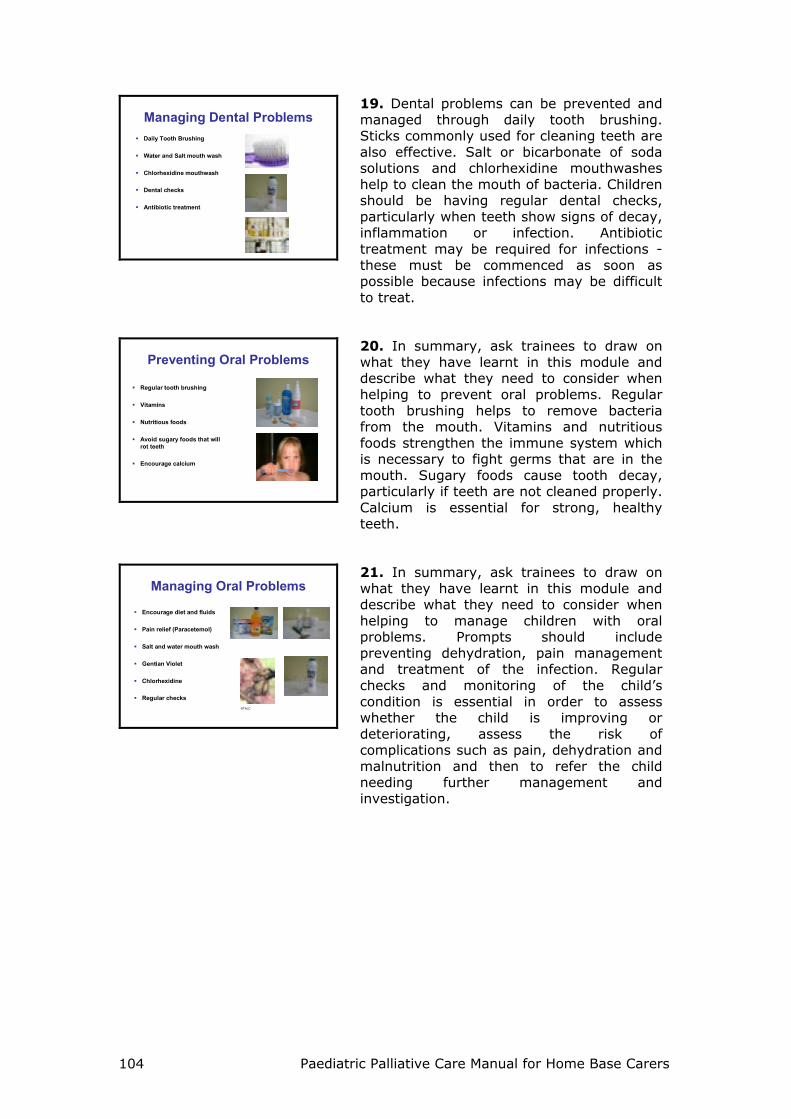
18. Ask trainees to describe what they see in the picture. How many of the children they see have bad teeth? How many of the children they see brush their teeth regularly and what do they use? HIV positive children commonly have bad teeth. The dental problems themselves are concerning but they often lead to secondary infections (e.g. abscesses, tooth decay, gum infections act as entry points for bacteria in to the body). These can be extremely painful. Once again, this causes distress and the child may be reluctant to eat or drink, placing them at risk of dehydration and malnutrition.
Paediatric Palliative Care Manual for Home Base Carers 104
Managing Dental ProblemsDaily Tooth Brushing
Water and Salt mouth wash
Chlorhexidine mouthwash
Dental checks
Antibiotic treatment
19. Dental problems can be prevented and managed through daily tooth brushing. Sticks commonly used for cleaning teeth are also effective. Salt or bicarbonate of soda solutions and chlorhexidine mouthwashes help to clean the mouth of bacteria. Children should be having regular dental checks, particularly when teeth show signs of decay, inflammation or infection. Antibiotic treatment may be required for infections - these must be commenced as soon as possible because infections may be difficult to treat.
Preventing Oral Problems
Regular tooth brushing
Vitamins
Nutritious foods
Avoid sugary foods that will rot teeth
Encourage calcium
20. In summary, ask trainees to draw on what they have learnt in this module and describe what they need to consider when helping to prevent oral problems. Regular tooth brushing helps to remove bacteria from the mouth. Vitamins and nutritious foods strengthen the immune system which is necessary to fight germs that are in the mouth. Sugary foods cause tooth decay, particularly if teeth are not cleaned properly. Calcium is essential for strong, healthy teeth.
Managing Oral Problems
Encourage diet and fluids
Pain relief (Paracetemol)
Salt and water mouth wash
Gentian Violet
Chlorhexidine
Regular checks©TALC
21. In summary, ask trainees to draw on what they have learnt in this module and describe what they need to consider when helping to manage children with oral problems. Prompts should include preventing dehydration, pain management and treatment of the infection. Regular checks and monitoring of the child’s condition is essential in order to assess whether the child is improving or deteriorating, assess the risk of complications such as pain, dehydration and malnutrition and then to refer the child needing further management and investigation.
Paediatric Palliative Care Manual for Home Bases Carers 105
Module 11: Fever Module Objectives
To demonstrate why children with HIV are likely to experience fevers To review the complications of fever in a child
To equip trainees with the knowledge and skills required to assess a child
with fever To review the management of a child with fever and when to refer
To demonstrate the importance of the role trainees have to play in
educating parents/carers in the prevention and management of fevers.
Slide Presentation: Fever
Fever
Paediatric Palliative CareFor Home Based Carers
Funded by
British High Commission, Pretoria
Small Grant Scheme
1. Welcome trainees and introduce yourself. Give a brief background in to your area of practice, role and experience. Ask the trainees for their experiences of caring for children with fever, how they manage it and what they hope to learn from this session. Encourage trainees to ask questions and share their thoughts throughout.
What is Fever? A raise in body temperatureabove 37.5oC (IMCI 2002)
During infections, the body is able to raise its temperature which helps to fight germs
So fever is one of the most common signs of infection in ALL children
2. Ask trainees to explain what they understand by ‘fever’. Fever is a body temperature of 37.5oC or above (IMCI, 2002). This fever or raise in body temperature is the body’s own way of trying to fight the infection. Fever is therefore not an infection itself but a SIGN of underlying infection. All children can get fevers when they are sick. The slide shows the soldiers (white blood cells or immune system) trying to fight the germs and a raise in body temperature helps this process.
Paediatric Palliative Care Manual for Home Base Carers 106
Children with HIVMore infections than mostchildren
More fevers than most children
Fever may be a sign of: Chest infectionsEar infectionsSkin infectionsDiarrhoeaMeningitisOral infectionsHIV Infection
©TALC
3. Due to their weakened immune system (or damaged, destroyed soldiers), children with HIV get more infections than HIV negative children. They therefore get more fevers. If a child has a fever, this could be a sign of a number of different infections, the majority of which may be normal childhood illnesses as listed in the slide. HIV itself can also cause a fever.
Fever in ChildrenFevers may cause discomfort to the child
Fevers increases loss of water through the skin
This increases the chance of dehydration in children
High fevers may lead to febrile convulsion(seizures or ‘fits’)
©TALC
©TALC
4. Ask trainees “What are the consequences of fever in children?”, “Why should they concern us?” Whilst fever is part of the body’s way of fighting off infection, fever can also be very dangerous, particularly for a young baby or small child. Firstly, fever may cause discomfort to a child. Secondly, a child with fever can quickly become dehydrated - like adults, when children get hot, they sweat and lose a lot of water. However, children become dehydrated more quickly due to their relatively greater body surface area. Thirdly, a high fever can lead to febrile convulsions and even severe, permanent brain damage.
Signs and Symptoms
How would you knowwhether Sofiso has
a fever?
©TALC
5. Ask trainees to describe how they would assess whether Sofiso has a fever whilst visiting him in the home. Take particular note of whether trainees have access to or are using thermometers in the home. Ideally, Home Based Carers require thermometers if they are to be assessing children with fever yet this will be depend on local resources and practicalities. The next three slides discuss three methods of assessing fever.
Has Sofiso got a fever?Touch the Child
Forehead, stomach or other parts of body may feel hot to the touch
He may or may not be sweating
Is his heart rate (pulse) fast?
©TALC
6. The first of three methods which trainees should be using to assess whether Sofiso has a fever is through touch. Ask trainees exactly where they should touch to feel for a fever. It must be stressed fever should be assessed by touching central parts of the child’s body (e.g. forehead, stomach) rather than peripheral parts (e.g. hands and feet). The peripheries actually become cooler during fever.
Paediatric Palliative Care Manual for Home Bases Carers 107
Has Sofiso got a fever?
Look at the Child
Is he withdrawn and/or reluctant to move?
Is he irritable?
Is he breathing fast?
©TALC
7. Secondly, trainees should be looking at the child. Fever commonly causes discomfort and a child with fever may well be quiet, withdrawn and/or reluctant to move. Parents may report that the child is ‘not himself’. Conversely, the child may be irritable and difficult to console. During fever, breathing rate increases. Fast breathing (or tachypnea) may also indicate the child is distressed.
Has Sofiso got a fever?Take the temperature
Our eyes and hands are very helpful inassessing fever
But, thermometers are more accurate and may be used to answer:
How high is the child’s temperature?Has the treatment effectively lowered the temperature?Has the fever risen?
©TALC
8. Thirdly, a thermometer should be used. Touching and observing the child does give an indication that the child is ‘hot’, yet a thermometer is the only way to accurately measure fever. This is not only extremely important for telling us exactly how high the temperature is but also for assessing whether the interventions used for reducing the temperature have been effective or whether the fever has risen even further. This is vital for effective management of fever and ensuring the child’s safety.
Using ThermometersTry to keep the child calm before taking temperature
Wash thermometer with cold soapy water and/or alcohol
Shake thermometer hard until reading is below 36 degrees
Place bulb end of thermometer well up in to armpit, holding arm down over it and elbow in to baby’s side
Hold position for 4-5 minutes, whilst singing songs/telling story
NEVER leave the child with the thermometer – he WILL move!
9. If thermometers are to be relied upon as a measure of fever, they must be used properly. Have one or more available as teaching aids. Trainees need to be confident in the use of thermometers. Although different varieties now exist (e.g. mercury, digital), mercury thermometers have been shown to be the most reliable and accurate. Digital ones also require batteries. Disposable plastic strips exist but these commonly spoil in hot conditions, making them useless.
Remember!!Mercury is poisonous
If a thermometer is broken, this is extremely dangerous
ALWAYS store a thermometer in a safe place where it will not be broken
10. Mercury thermometers are supplied with a plastic case. The thermometer must always be kept within this, in order to protect it from breaking and leaking mercury. The case must then be stored in a safe place where it is unlikely to get knocked around and broken. Mercury thermometers should never be left where children may find them. Trainees need a safe method of transporting thermometers when visiting the communities.
Paediatric Palliative Care Manual for Home Base Carers 108
Reading ThermometersHold thermometer in a good lightRotate until you see a silver line of mercuryLine up mercury with numbers, marked in full degrees (36,37,38) and every two-tenths degree (.1,.2,.3,.4)Point where mercury ends indicates the temperatureWrite it down straight away with time taken
34 35 36 37 38 39 405 5 5 5 5 5
11. If the thermometer has been used as described in slide 9, an accurate measurement of fever will have been recorded and this must now be read. This can be a little tricky initially until the individual has seen the mercury and knows what to be looking for. Either now or at the end of this session, ask trainees to practice with the thermometers to ensure they are confident in reading them. Remember, thermometers should be cleaned between use.
What to Do? Fever is usually a sign of infection in the child
So you need to:
Manage the feverIdentify what may be causing the fever
Any underlying infections can thenbe treated and managed appropriately
12. As discussed earlier, fever is not an infection itself but a sign of infection. Due to the potential dangers of fever in children, the fever must be managed immediately. In addition, the fever is a sign that the child needs assessment for any underlying infection. If trainees identify a child with fever, they have a vital role to play in a) helping to manage the fever and b) helping to ensure any underlying infection is treated and managed appropriately.
Does the Child have Fever?If carer reports history of feveror temperature is 37.5oC orabove:
Ask:
For how long?
If more than 7 days, has fever been present every day?
(IMCI, 2002)
13. The IMCI guidelines (2002) recommend this procedure for any child with fever. Having confirmed a fever, trainees should ask the parent/carer for how long the child has had the fever. If they report that the fever has been there for 7 days, it is important to ask whether it has been there every day or intermittently. The answers to these questions are extremely important in order to help the doctor or professional nurse to whom they refer the child.
Risk of Meningitis Look and Feel for:
Stiff neckBulging fontanelle
Suspected Meningitis if:
Any general danger signORStiff neckORBulging Fontanelle
(IMCI, 2002)
14. One of the greatest concerns for any child with fever is to exclude the risk of meningitis. This is not easy but the presence of a stiff neck and/or bulging fontanelle are associated with meningitis and need excluding. Teaching trainees to do this well is much more effective with a real child and should be included in any ward teaching. According to IMCI (2002), the child should be considered to be at risk of meningitis if there are ANY general danger signs (as discussed in Module 15: Danger Signs), OR the child has a stiff neck OR a bulging fontanelle.
Paediatric Palliative Care Manual for Home Bases Carers 109
Suspected MeningitisHome Based Carers
Administer one dose of paracetamol (Panado) for fever 38oC or above
Refer urgently!
Professional Nurses
Child needs dose of IM Ceftriaxone
Test blood sugar
Give one dose of paracetamol (Panado) for fever 38oC or above
(IMCI, 2002)
15. The management of a child with suspected meningitis will depend on the qualification of the Home Based Carer. IMCI recommendations are that the child needs Paracetamol, IM Ceftriaxone and a blood sugar test. This training programme assumes that most trainees are not professional nurses and their role should be to advise the parent to administer a dose of paracetamol (if the child is able to take it) and to then refer urgently. If professional nurses have been trained to do so, they should administer IM Ceftriaxone, Paracetamol and measure blood sugar and ensure the child gets to a clinic immediately.
If No Suspected MeningitisAssess the child - Look, Listen, Feel for the following:
Sore ThroatEar ache, pus from earDifficulty breathing, noisy breathingCough (+/- sputum)DiarrhoeaPain on passing urineSevere headache, neck stiffness, bulging fontanelleSkin Inflammation, sores, rashesPain in joints
Then give Paracetamol (Panado) and discuss with Professional Nurse
16. If the child has fever but no general danger signs, no stiff neck and no bulging fontanelle, other infections are likely. If trainees are able to identify any signs and symptoms, these may give an indication of the underlying infection. This information can be of great benefit to the doctor or professional nurse to whom they are referring the child. The child should be given Paracetamol to help bring the fever down. NB Stress to trainees they must always ask whether the parent/carer has already given a dose of Paracetamol as it may be less than 4 hours since the previous one.
Managing FeversRegular administration of medication to:
bring temperature down
keep temperature down
reduce discomfort
encourage drinking and eating
17. Paracetamol can be extremely effective at managing fevers yet the key to successful management is to give it regularly. Whilst a one-off dose may be sufficient for some cases of mild fever, the majority of cases of fever will persist and as soon as the first dose of paracetamol has worn off, the child’s body temperature will increase once more. Regular dosing helps to bring down the fever AND keep it down. It also makes the fever easier to keep under control rather than waiting for the fever to get high again. Paracetamol not only brings down the fever but also helps to alleviate discomfort. Regular fluids and diet are also essential.
Paediatric Palliative Care Manual for Home Base Carers 110
Giving Paracetamol for Fever
6-12 Years
1 Year up to 5Years
2 months up to 1 Year
Age or Weight
-5 – 10 ml
Half to 1 tablet10 – 20 ml
-2.5 - 5 ml
Tablet (500mg)Syrup (120mg/5ml)
Every 4-6 Hours AND No more than 4 Times a Day!
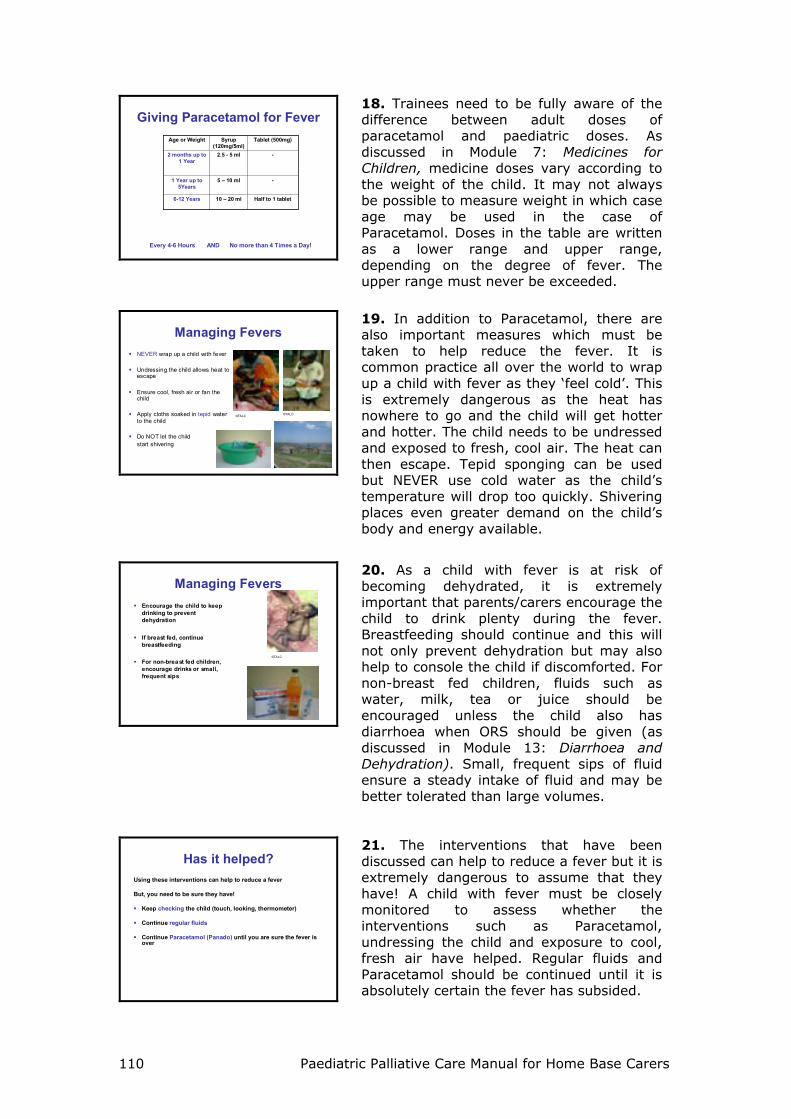
18. Trainees need to be fully aware of the difference between adult doses of paracetamol and paediatric doses. As discussed in Module 7: Medicines for Children, medicine doses vary according to the weight of the child. It may not always be possible to measure weight in which case age may be used in the case of Paracetamol. Doses in the table are written as a lower range and upper range, depending on the degree of fever. The upper range must never be exceeded.
Managing FeversNEVER wrap up a child with fever
Undressing the child allows heat to escape
Ensure cool, fresh air or fan the child
Apply cloths soaked in tepid water to the child
Do NOT let the child start shivering
©TALC
©TALC©TALC
19. In addition to Paracetamol, there are also important measures which must be taken to help reduce the fever. It is common practice all over the world to wrap up a child with fever as they ‘feel cold’. This is extremely dangerous as the heat has nowhere to go and the child will get hotter and hotter. The child needs to be undressed and exposed to fresh, cool air. The heat can then escape. Tepid sponging can be used but NEVER use cold water as the child’s temperature will drop too quickly. Shivering places even greater demand on the child’s body and energy available.
Managing FeversEncourage the child to keep drinking to prevent dehydration
If breast fed, continue breastfeeding
For non-breast fed children, encourage drinks or small, frequent sips
©TALC
20. As a child with fever is at risk of becoming dehydrated, it is extremely important that parents/carers encourage the child to drink plenty during the fever. Breastfeeding should continue and this will not only prevent dehydration but may also help to console the child if discomforted. For non-breast fed children, fluids such as water, milk, tea or juice should be encouraged unless the child also has diarrhoea when ORS should be given (as discussed in Module 13: Diarrhoea and Dehydration). Small, frequent sips of fluid ensure a steady intake of fluid and may be better tolerated than large volumes.
Has it helped?Using these interventions can help to reduce a fever
But, you need to be sure they have!
Keep checking the child (touch, looking, thermometer)
Continue regular fluids
Continue Paracetamol (Panado) until you are sure the fever is over
21. The interventions that have been discussed can help to reduce a fever but it is extremely dangerous to assume that they have! A child with fever must be closely monitored to assess whether the interventions such as Paracetamol, undressing the child and exposure to cool, fresh air have helped. Regular fluids and Paracetamol should be continued until it is absolutely certain the fever has subsided.
Paediatric Palliative Care Manual for Home Bases Carers 111
Febrile ConvulsionsChildren adjust less quickly to high body temperatures
Temperature above 38.5 C or a rapid change in temperature may lead to febrile convulsion
Most common in children 6 months to 5 years
Usually only last 1-2 minutes
Signs and Symptoms:CollapseEyes rolling upwardFoaming at mouthStiffening of the bodyUncontrolled jerking movementsBreathing difficulty in severe cases
22. The body of a child cannot adjust to high temperatures in the same way that an adult can. One of the greatest concerns with high fevers in a child is that it may cause the child to have a febrile convulsion or ‘fit’. These can sometimes leave the child with severe neurological damage. The most common period during which febrile convulsions may occur is between 6 months and 5 years, usually lasting 1-2 minutes. Ask trainees if they have witnessed a child having a febrile convulsion and to describe what they saw. Not all children will look the same during a fit but common signs and symptoms are listed here.
Handling Febrile ConvulsionsKeep calm
Reassure care giver
Ensure area around child is clear and safeNever restrain the child or place anything in mouthLoosen clothing around neck and bodyPosition child with head lower than body if possibleChild may lose consciousness but will usually ‘come round’without helpIf the convulsion lasts longer than 5 minutes, the child needs emergency help
23. Ask the same trainees how they felt during the child’s convulsion, what happened and how they managed it. Trainees need to feel confident in knowing what to do for a child having a seizure. Children should be managed in much the same ways as adults. The primary focus is on ensuring the child does not harm himself during the seizure. Ask trainees about local practices which sometimes involve putting objects in the mouth during a seizure. Stress this should never be done. If the seizure does not resolve within 5 minutes, the child must be taken to a clinic as quickly as possible.
After a Febrile ConvulsionThe child may sleep
Ensure child is on his side
Give Paracetamol (Panado) if the child is conscious/ able to swallow
Apply cool cloths to body
NEVER put child in a bath
Take child to a clinic for further investigation and treatment of cause
24. Children commonly sleep after a fit or convulsion. Parents/carers need reassurance that their child is safe and only sleeping. The child should be on his side to help him breathe well and to prevent him from aspirating (inhaling) if he vomits. The fever must be brought down and paracetamol should be given if the child is awake. Rectal paracetamol is quicker and more effective if there is someone trained to give it and suppositories are available. Tepid cloths can be applied to help bring down the fever but never cold cloths as this will bring the temperature down too quickly. In addition, the cold cloths cause the blood vessels to constrict (close) which pushes the hot blood back in towards the internal organs. Putting the child in the bath would be extremely dangerous for the same reasons and it could lead to more fits. Furthermore, it is extremely hard to protect a child if fitting in a bath and the child could drown. A child that has had a febrile convulsion needs professional assessment and treatment for the underlying cause of the fever.

Paediatric Palliative Care Manual for Home Base Carers 112
Note!
If a child has a seizure and is not between 6 months and 5 years,
this is likely to be caused by something other than fever
25. A fever is by no means the only cause of convulsion in children. As stated earlier, the most common period for febrile convulsions is between the ages of 6 months and 5 years. Trainees should be aware that if a child younger than 6 months or older than 5 years has had a convulsion, it is less likely to be a febrile convulsion but a neurological problem. The child must be assessed and managed appropriately in a clinic or hospital.
EducationCare Givers need to be taught how to recognise and managetemperatures in order to:
Alleviate the child’s discomfort
Prevent dangerously hightemperatures
Ensure infections are treated as early as possible
26. Education for parents and carers is vital if children with fever are to be managed appropriately and protected from the potential dangers of high fever. Trainees are in a very important position in that they can help parents/carers to understand the possible consequences of fever, how to alleviate discomfort and prevent dangerously high temperatures. Importantly, trainees can ensure children with fever are followed up for appropriate management of underlying infection.
Remember!!Fever is a very useful sign of infection
Fevers must be managed properlyto prevent distress and complications
BUT, the child’s behaviour is the bestsign of how sick a child is :-
A child may have:
NO fever with infection eg pneumonia, meningitis (especially in malnutrition)
HIGH fever with a mild cold
27. It has been shown that fever is a very useful indicator that the child has an underlying infection which must be treated appropriately. However, fever can be misleading as not all children will have fever with infection. Some children may be extremely sick yet have no fever (e.g. a child with malnutrition does not have sufficient energy in the body to raise its body temperature). Conversely, some children may get a very high fever with only a mild cold. So fever is a good indicator of infection but it should not be the sole indicator and the child’s behaviour is the best sign of how well/unwell a child is, as will be discussed further in Module 16: Danger Signs.
Paediatric Palliative Care Manual for Home Bases Carers 113
Module 12: Acute Respiratory Infections Module Objectives
To review the importance of Acute Respiratory Infection in childhood To equip the trainee to recognise the symptoms and signs of Acute
Respiratory Tract Infections in children To teach the trainees how to appropriately manage children with Acute
Respiratory Infections within the trainees scope of practice
Slide Presentation: Acute Respiratory Infections
Acute Respiratory Infections
Paediatric Palliative CareFor Home Based Carers
Funded by
British High Commission, Pretoria
Small Grant Scheme
1. Welcome trainees and introduce yourself. Give a brief background in to your area of practice, role and experience of caring for children with Acute Respiratory Infections. Ask the trainees for their experiences of Acute Respiratory Infections (ARIs) in children, challenges they have faced, how they have managed them and what they would hope to learn from this session. Encourage trainees to ask questions and share their thoughts throughout.
Causes of Death in Children World-Wide
024
68
1012
1416
1820
Perc
enta
ge o
f Dea
ths
RespiratoryInfections
Diarrhoea Measles Malaria HIV
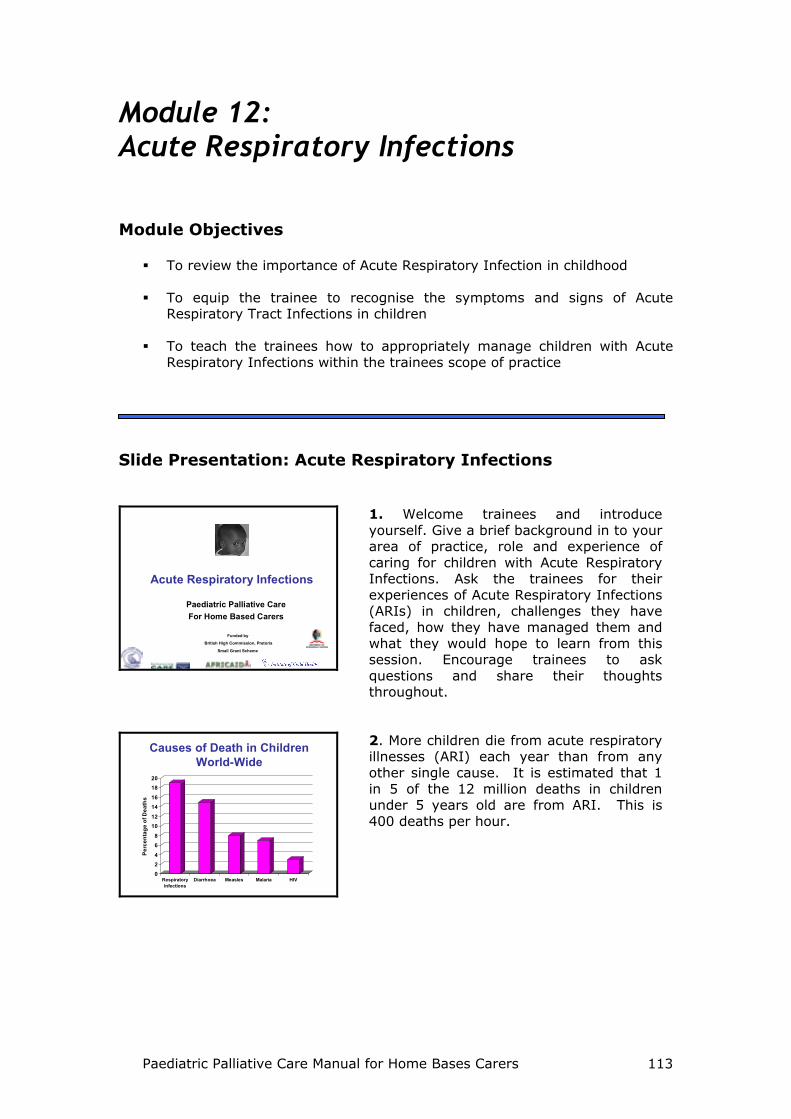
2. More children die from acute respiratory illnesses (ARI) each year than from any other single cause. It is estimated that 1 in 5 of the 12 million deaths in children under 5 years old are from ARI. This is 400 deaths per hour.
Paediatric Palliative Care Manual for Home Base Carers 114
30-40% admissions
77% deaths in HIV infected infants
CFR=34%
CFR=22%
HIV infected children are at increased risk of respiratory disease
70 000 HIV Infected children born annually in S. Africa
2.8 million HIV infected children worldwide
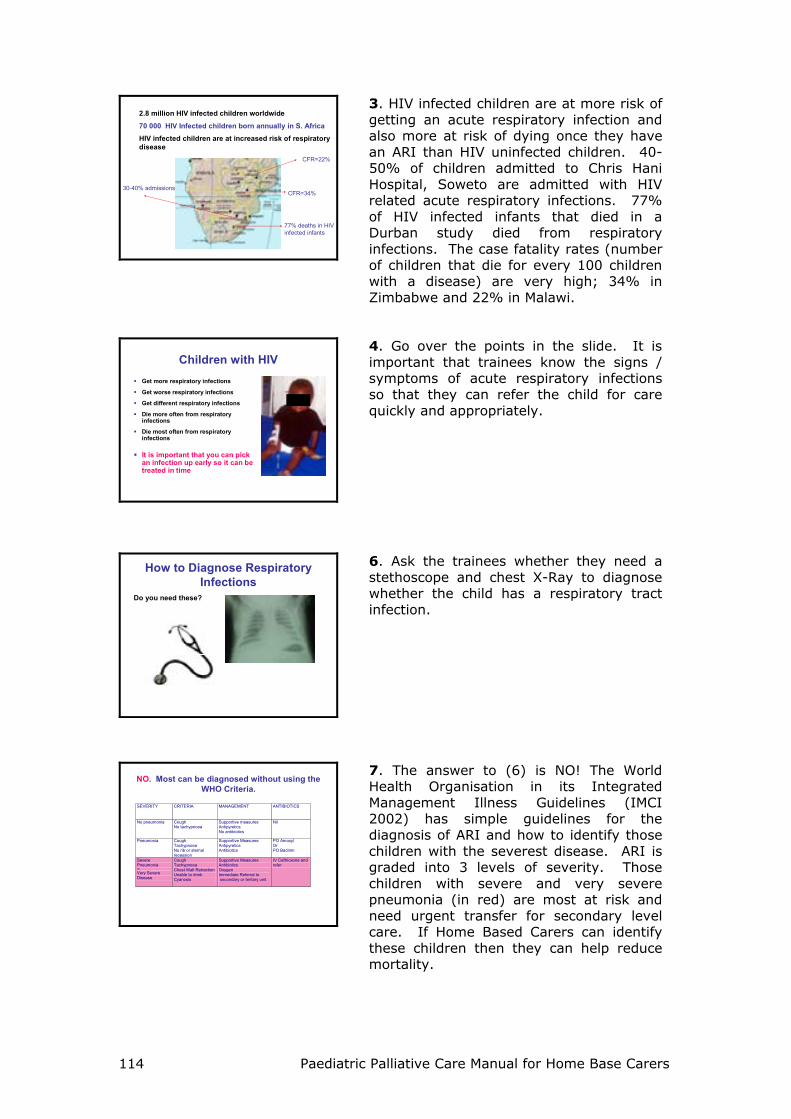
3. HIV infected children are at more risk of getting an acute respiratory infection and also more at risk of dying once they have an ARI than HIV uninfected children. 40-50% of children admitted to Chris Hani Hospital, Soweto are admitted with HIV related acute respiratory infections. 77% of HIV infected infants that died in a Durban study died from respiratory infections. The case fatality rates (number of children that die for every 100 children with a disease) are very high; 34% in Zimbabwe and 22% in Malawi.
Children with HIVGet more respiratory infections
Get worse respiratory infections
Get different respiratory infections
Die more often from respiratory infections
Die most often from respiratory infections
It is important that you can pick an infection up early so it can be treated in time
4. Go over the points in the slide. It is important that trainees know the signs / symptoms of acute respiratory infections so that they can refer the child for care quickly and appropriately.
How to Diagnose Respiratory Infections
Do you need these?
6. Ask the trainees whether they need a stethoscope and chest X-Ray to diagnose whether the child has a respiratory tract infection.
NO. Most can be diagnosed without using the WHO Criteria.
IIMC
SEVERITY CRITERIA MANAGEMENT ANTIBIOTICS
No pneumonia Cough No tachypnoea
Supportive measures Antipyretics No antibiotics
Nil
Pneumonia Cough Tachypnoea No rib or sternal recession
Supportive Measures Antipyretics Antibiotics
PO Amoxyl Or PO Bactrim
Severe Pneumonia Or
Very Severe Disease
Cough Tachypnoea Chest Wall Retraction Unable to drink Cyanosis
Supportive Measures Antibiotics Oxygen Immediate Referral to secondary or tertiary unit
IV Ceftrioxone and refer
7. The answer to (6) is NO! The World Health Organisation in its Integrated Management Illness Guidelines (IMCI 2002) has simple guidelines for the diagnosis of ARI and how to identify those children with the severest disease. ARI is graded into 3 levels of severity. Those children with severe and very severe pneumonia (in red) are most at risk and need urgent transfer for secondary level care. If Home Based Carers can identify these children then they can help reduce mortality.
Paediatric Palliative Care Manual for Home Bases Carers 115
What is tachypnea?Breathing fast
Under 2 months: 60/minute
2 months – 1 year: 50/minute
Over 1 year: 40/minute
©TALC
8. The term “tachypnea” means “to breath fast”. Sick children can breathe fast for many reasons. Children will breathe fast if they have a fever, are septic or if they have a respiratory infection. All of these are serious and so IMCI has criteria to define what is fast breathing and when to refer to hospital. Go over the criteria in the slide for tachypnea. (IMCI 2002)
What to askIs the child able to drink or breastfeed?
Does the child vomit everything?
Has the child had convulsions?
Does the child have a fever?
Does the child have a cough?
Has there been difficulty in breathing?
9. To identify whether the child has an ARI or danger symptoms requiring transfer to hospital the trainees should learn to ask the questions in the slide. IMCI defines any child with a cough and fever as having an acute respiratory tract infection.
What To DoLook at the child generally:
LethargyUnconscious
Look, listen, feelLook for cyanosisLook for chest indrawingLook & listen for stridor and wheezeCount the respiratory rate
Decide which sort of acute respiratoryinfection the child has
10. After asking the questions, the carer needs to examine the child for signs which suggest an acute respiratory infection or any signs that would require urgent transfer. The WHO video on how to identify ARI should be shown as part of this module.
No PneumoniaWhat you find:
CoughFever
No fast breathingNo chest indrawing
What to do:
Reassure the motherGive panadoEncourage fluids
If in doubt referEnsure child is reviewed within 48 hrs.
11. Children who have a cough and fever but no other symptoms / signs are defined as having “no pneumonia”. The carer should educate the mother to:
1. Give regular anti-pyretics (Paracetamol)
2. Encourage regular oral fluids If the HBC is in any doubt they should refer up to a higher level of care. They should arrange for any child not referred onwards to be reviewed again within 48 hours either by themselves or at the clinic. This is important as children can deteriorate very quickly. It is important that the home
Paediatric Palliative Care Manual for Home Base Carers 116
based carer advices the child’s guardian what danger signs to look for and to encourage them to seek further health care advice if they are concerned that the child is deteriorating at any time. The “Danger Signs” to look for are covered in Module 15: Danger Signs.
PneumoniaWhat you find:
Cough Fever
Fast breathing
NO CHEST INDRAWING
What to do:
Reassure motherGive PanadoRefer to clinicChild will receive oral antibiotics. Ensure mum knows how to give them
Follow-up in 48 hrsEnsure mum is giving medicationIf worse, refer hospital
12. Any child with a cough and fever who also has fast breathing is defined as having “pneumonia”. These children will need oral antibiotics and therefore the Home Based Carer needs to either refer the child to clinic or discuss the child with a professional nurse depending on local policy .
Severe or Very Severe Pneumonia
What you find:
CoughFever
Fast BreathingChest Indrawing
Cyanosis (very severe)
If able:– Give oxygen and IV
ceftriaxone and refer to hospital.
– Under 6 months, add in oral bactrim.
– Test blood sugar and treat if low
If not able:– refer to nearest available
health centre for stabilisation and transfer.
13. Children who have chest in-drawing and / or are cyanosed are seriously ill and need urgent referral to secondary level care. This should be done in accordance with local Home Based Care policy and local IMCI guidelines. If within the Home based Carer’s scope of practice, the child should receive intravenous ceftriaxone before referral. Children under 6 months old are at particularly high risk of PCP and should also therefore receive oral bactrim. All children should have their blood glucose checked and rectified if low.
TuberculosisTB is common in both adults and children
Children present with:Chronic cough (more than 2 weeks)Weight loss or Failure to thriveNight sweats
TB is difficult to diagnose so if you suspect – refer to clinic
14. South Africa has very high levels of Tuberculosis. It is one of 22 countries that the WHO has designated as “TB Hot Spots”. The diagnosis of TB is often difficult to make, especially in children. If the child has any of the three symptoms on the slide then TB must be ruled out. The child should therefore be referred according to local policies.