Embed Size (px)
Citation preview

Moving Beyond Content Validation of Nursing Diagnoses
Laurence Parker, PhD, and Margaret Lunney, PhD, RN, CS
TOPIC. Studies to establish construct and
criterion-related validity of nursing diagnoses.
PURPOSE. The overwhelming majority of previous
studies addressed content validation by nurse
experts. This paper describes strategies to move
beyond content validation research to construct
and criterion-related validation.
SOURCES. The range of studies that should be
conducted for development of nursing diagnoses
are reviewed with examples drawn from the field
of psychology. Existing studies on the diagnoses
of in effective breathing pat tern, in effective
airway clearance and impaired gas exchange are
used as examples.
CONCLUSIONS. Many types of studies are needed for
each nursing diagnosis. Increased funding and
support for nursing diagnosis research will be
facilitated by attention to the accuracy of nurses’
diagnoses and outcomes of the diagnostic process.
Key words: Construct validity, nursing
diagnosis, resea rch met hod 01 ogy
This urticle was uduptedfrorn a puperpresented at the 13th Conference of the North American Nursing Diagnosis Association in St. Louis, MO, April 1998.
144
Laurence Parker, PhD, is Research Assistant Professor and Director of Health Services and Outcome Research, Thomas Jefferson Medical College, Department of Radiology, Philadelphia; Margaret Lunney, PhD, RN, CS, is Professor, Department of Nursing, College of Staten Island, Staten Island, NY.
T h e 25th anniversary of the North American Nursing Diagnosis Association (NANDA) is an appropriate time to consider the work done to develop and refine the NANDA taxonomy and the work that still needs to be done. The NANDA taxonomy was created and refined over the past 25 years through motivation, scholarly efforts, and commitment to name the phenomena of nursing’s concern. The NANDA taxonomy is advancing, albeit slowly, in the direction of other, more sophisticated classifications, such as the International Classification of Diseases (ICD-9). The purpose of this paper is to review briefly the state of the art of validation research for ongo- ing development of the NANDA taxonomy, to suggest that we may be stuck at the stage of nurse validation sur- veys, and to prompt nurses to move beyond this stage to other types of validation studies.
Background and Significance
The motivation and commitment to develop the NANDA taxonomy will continue into the 21st century because identification of human responses to health problems and life processes is the basis for nurses’ deci- sions on how to help people. Nurses cannot know what interventions to select or which outcomes to project unless they have accurate representations of what patients are experiencing. Accuracy of interpreting the human responses of patients is facilitated by the naming of responses (Lunney, 1998). In a theory of linguistics, Hayakawa & Hayakawa (1990) explained that naming improves thinking, which improves actions. Thus, the naming of responses to health problems and life pro- cesses helps nurses think more clearly, cooperate more effectively with patients and others, and communicate
Nursing Diagnosis Volume 9, No. 4, October-December, 1998

patient experiences to self and others as the basis for selection of interventions and outcomes.
Development of the NANDA taxonomy through the naming of human responses spearheaded the development of two other important taxonomies, the Nursing Interventions Classification (NIC) (McCloskey & Bulechek, 1996) and the Nursing Outcomes Classification (NOC) (Johnson & Maas, 1997). The use- fulness of these other two taxonomies in the provision of quality nursing care depends, however, on the accu- racy of nurses’ interpretations of the experiences of patients (Lunney, 1998). Nurses interpret the experi- ences of patients whether or not these interpretations are named as nursing diagnoses. If their interpretations are inaccurate, the most effective interventions and outcomes will not be selected. Accuracy of interpreta- tions of human responses is supported by a research- based taxonomy of diagnostic labels with signs and symptoms.
Standardized languages such as NANDA, NIC, and NOC are important for the Computer-Based Patient Record (CPR), which was projected to be in place by the year 2000 (American Nurses Association, 1995). Nursing care may not be represented in the CPR if the nursing classification systems are not valid and reliable. If nursing wants to be represented in the CPR of the future, there must be studies to establish the construct validity, criterion-related validity, and reliability of standardized nursing languages such as NANDA.
The need for research of NANDA labels and the tax- onomy of labels has been explained in a number of sources (Alexander, 1989; Dougherty, Jankins, Lunney, & Whitley, 1993; Gordon, 1994; Guzzetta, Kinney, & Grant, 1994; Hoskins et al., 1992; Kerr, 1991, 1994; Kerr et al., 1992,1993; Whitley, 1995, in press. The information from these sources can be used to plan a research program to refine specific diagnoses and the overall taxonomy. This paper reminds nurses that much of this work remains to be done. It gives examples using the diagnoses ineffective brea thing pattern (IBP), ineffective airway clearance (IAC), and impaired gas exchange (ICE).
State of the Ark Validation Research
The human responses on the NANDA list need to be validated for ongoing knowledge development of these concepts. Some of the concepts have been studied exten- sively in other fields, e.g., anxiety and fear. Other diag- nostic concepts (e.g., IBP, IAC, IGE) were developed for the NANDA taxonomy based on knowledge of physiol- ogy. Regardless of the source of concepts, however, incorporation in a nursing taxonomy with signs and symptoms requires validation research.
In the early days of validation research, nurse researchers studied the content validity of diagnoses by doing retrospective chart reviews, that is, studying which diagnoses were being used in clinical practice and what were the signs and symptoms that prompted use of the diagnoses. Examples of such studies are York (1985) and McDonald (1985). Later studies focused on nurse sur- veys. With the respiratory diagnoses, the studies of Boisvert (1995); Brukwitzki, Holmgren, and Maibusch (1996); Capuano, Hitchings, and Johnson (1990); Clark (1994); Matsuki and Otani (1995); and Wake, Fehring, and Fadden (1991) were nurse validation studies. Some of the findings from these studies were similar, but others were inconsistent, indicating a need for clinical validation with data from patients rather than nurses.
For all diagnoses on the NANDA list, there have been few clinical validation studies as described by Hoskins (1989) and Carlson-Catalano and Lunney (1995). A study by Carlson-Catalan0 et al. (1995, 1998) was the first reported clinical validation of the three respiratory nurs- ing diagnoses. Studies of the frequencies of diagnoses used in clinical settings (Gordon & Hiltunen, 1995; Hoskins et al., 1986; Lutjens, 1993), however, showed that one or more of these three diagnoses are used frequently by nurses. Many patients in many types of settings (criti- cal care, acute medical and surgical care, long-term care, home care) are at risk of these diagnoses, yet the research to guide use of these diagnoses is insufficient.
There have been few construct validation studies and criterion-related studies of any diagnoses, and none is available for knowledge development of IBP, IAC, and
Nursing Diagnosis Volume 9, No. 4, OctobepDecember, 1998 145

Moving Beyond Content Validation of Nursing Diagnoses
IGE. Examples of construct validation are studies by Chang (1989) and Whitley (Whitley & Tousman, 1996). The case control method used by Wooldridge et al. (1998) is an example of criterion-related validation, the criterion being patients with similar characteristics who did not experience the problem.
Knowledge Development
Steps in the process of knowledge development. Knowledge development of diagnoses in the NANDA taxonomy means a series of studies needs to be done for each individual diagnosis as well as groups of diagnoses. The steps in the process are: to conduct concept analysis (Whitley, 1995); develop operational definitions for DCs; develop hypotheses; obtain empirical data; use varied settings; examine reliability, incidence, and outcome; aggregate and compare findings; reformulate hypotheses for further testing; and reformulate diagnostic categories. Most of these steps were applied in a clinical validation study of the three respiratory diagnoses-IBP, IAC, and IGE (Carlson-Catalan0 et al., 1995,1998).
Types of validity studies. Methodology texts distin- guish between three types of validation studies: content, criterion-related, and construct validity. Content validity is the agreement of a construct or measuring instrument with expert judgment, or common senseso-called face validity. Most academic or personnel tests are con- structed in this way. Criterion-related validity lies in demonstrating there is a predictive relationship with another variable. The relationship between the Scholastic Aptitude Test (SAT) and college grade point average (GPA) often is cited as an example of criterion-related validity. Construct validity lies in developing a body of scienhfic theory related to the construct, and demonstrat- ing that the theoretical relations are appropriate. As with any scientific argument, the theoretical relations are sup- ported by the weight of empirical evidence. One of the first great studies of modern social psychology, The Authoritarian Personality (Adorno, Frenkel-Brunswick, Levinson, & Sanford, 1950), is a set of numerous types of empirical studies about this construct derived from psy-
choanalytic theory. Since content validity requires only expert judgment, it is less elaborate and expensive to establish than criterion-related or construct validity, which require the study of an appropriate group of sub- jects and the measurement of other criteria or constructs. For a personnel test, appropriate use of expert opinion produces a content valid test. In contrast, establishing cri- terion-related validity involves developing an appropri- ate measure of job performance and following a group of tested subjects over time. Criterion-related and construct validity are more convincing than content validity, which is, after all, just a systematic process of exploring the assumptions of experts. This is codified in federal regula- tions about personnel testing, which require criterion- related or construct validity studies if a personnel test differentially selects protected minorities. An example from Foucault (1970) illustrates why it is necessary to go beyond content validity in nursing diagnoses. He quoted a medieval taxonomy in which animals are divided into “(a) belonging to the Emperor, (b) embalmed, (c) tame, (d) sucking pigs, (el sirens, (f) fabulous, (g) stray dogs, (h) included in the present classification, (I) frenzied, (j) innumerable, (k) drawn with a very fine camel hair brush, (1) et cetera, (m) having just broken the water pitcher, (n) that from a long way off look like flies” (p. xv). It may seem impossible that such a classification would be developed, but this classification illustrates what can happen when classification depends only on content validity. Content validation only establishes that a group of experts think a certain way; there is no assur- ance that their judgments match real-world phenomena.
Construct validity, on the other hand, moves beyond assumptions. Cronbach (1990) stresses the similarity between construct validation and traditional scientific research. It involves developing plausible, rival hypotheses and testing them in empirical studies. Validation lies in the weight of evidence developed for a particular construct. A criterion-related validity study may be a piece of evidence in a construct-validation argument, but generally, criterion- related studies are concerned only with demonstrating pre- dictive relationships and not with developing a body of scientific theory about the construct. From the perspective
146 Nursing Diagnosis Volume 9, No. 4, Odober-December, 1998
of criterion-related validity, it is sufficient to demonstrate the relationship of the SAT with college GPA; from the per- spechve of construct validity, a deeper understanding of the causal p'ocesses involved in this relationship is demon- strated. Construct validity studies explain that the SAT measures cognitive aptitude, as its developers have a p e d ; or it measures the educational experiences or cul- tural backgrounds appropriate to college success.
Future Studies
Cronbach (1990) noted that construct validation is a fluid, creative process that cannot be reduced to rules.
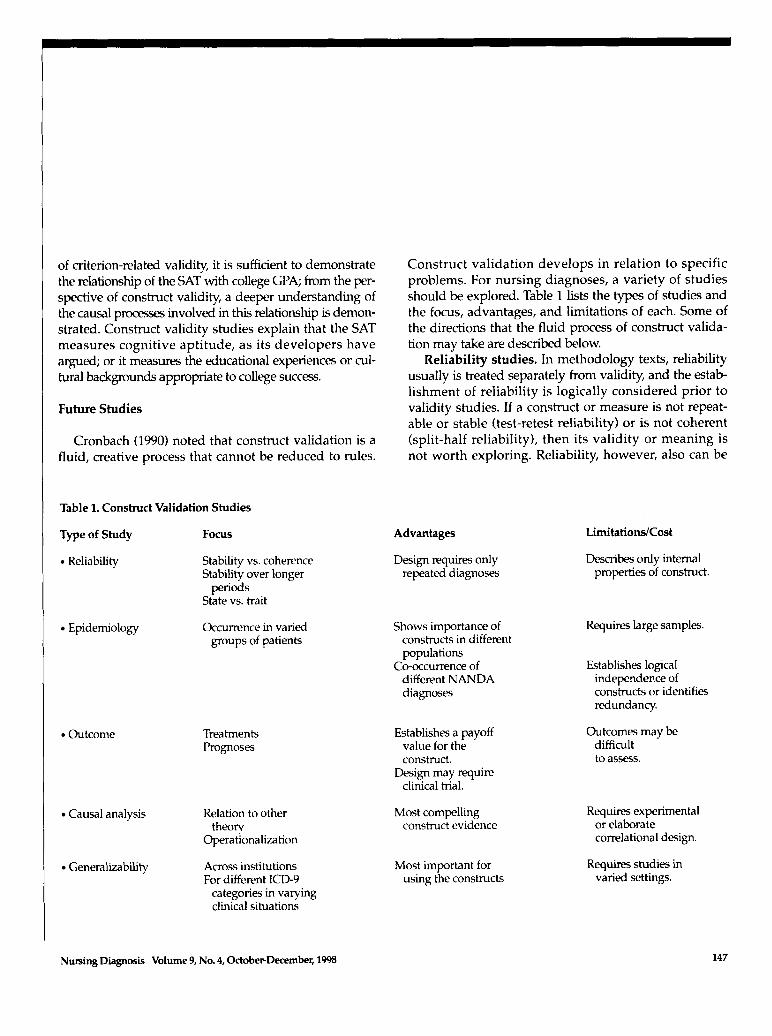
Table 1. Construct Validation Studies
Type of Study Focus
Keliability Stability vs. coherence Stability over longer
State vs. trait periods
Epidemiology Occumnce in varied groups of patients
Outcome Treatments Prognoses
Causal analysis Kelation to other
Operationalim tion
Generalizability Across institutions For differmt ICD9
categories in varying clinical situations
theory
Construct validation develops in relation to specific problems. For nursing diagnoses, a variety of studies should be explored. Table 1 lists the types of studies and the focus, advantages, and limitations of each. Some of the directions that the fluid process of construct valida- tion may take are described below.
Reliability studies. In methodology texts, reliability usually is treated separately from validity, and the estab- lishment of reliability is logically considered prior to validity studies. If a construct or measure is not repeat- able or stable (test-retest reliability) or is not coherent (split-half reliability), then its validity or meaning is not worth exploring. Reliability, however, also can be
Advantages Limitations/Cost
Design requires only repeated diagnoses
Describes only internal properties of construct.
Shows importance of Requires large samples. constructs in different populations
Co-occumnce of Establishes logical different NANDA independence of diagnoses constructs or identifies
redundancy.
Establishes a payoff value for the construct.
clinical trial. Design may require
Most compelling construct evidence
Outcomes may be difficult to assess.
Requires experimental or elaborate correlational design.
Most important for Requires studies in using the conshucts varied settings.
Nwsing Diagnosis Volume 9, No. 4, OdoberDecember, 1998 147
Moving Beyond Content Validation of Nursing Diagnoses
considered a component of construct validation. While it may be desirable, in general, to have repeatable, inter- nally consistent measures, the nature of the construct often influences which type of reliability is more impor- tant. Measurement of certain types of reliability may be important to demonstrate the correctness of a theory sur- rounding the construct. A scale that measures mood will not demonstrate test-retest reliability as will a scale that measures enduring characteristics of the person. A con- struct such as authoritarianism, which involves many dif- ferent types of behavior and underlying processes, will not exhibit the same internal consistency as a factor ana- lytic scale of introversion-extroversion. Finding the types of reliability one should find, and not finding the types one shouldn’t find, is evidence of the correctness of the theory, which defines the construct. In respect to the res- piratory diagnoses, internal consistency studies and long- term test-retest studies were not conducted, which would have considerable theoretical importance. The former requires more subjects to permit factor analyses and the latter is a longitudinal study. Conducting these types of studies would address such theoretically important ques- tions as whether these three diagnoses overlap, and whether one or more of the diagnoses are states or traits.
Epidemiological studies. It is important to explore the empirical occurrence of the diagnostic categories in the fashion of traditional epidemiological research (Alexander, 1989). These types of studies identify whether diagnostic categories are common or rare. They answer questions such as: What is the occurrence in dif- ferent patients of different ages, gender, and race? What is the occurrence in relation to other relevant demo- graphics, such as educational level or socioeconomic sta- tus? What are the interrelations of the NANDA cate- gories? The respiratory studies that are cited found that IBP and IAC are common and that the three diagnoses co-occur. Much broader studies are required, however, to answer questions such as: Is IGE so rare that it is not very useful, or is it so intertwined with the other two cat- egories that the three diagnoses should be redefined?
Outcome studies. The value of a diagnostic system lies in its ability to organize a set of understandings
about the phenomena it treats, to make differential pre- dictions about the categories, and to choose appropri- ate interventions for them. Studies of prognosis and outcomes require longer time frames and a variety of data sources. Such studies might lead to descriptions of better nursing practices or might take the form of full clinical trials of differential interventions. The stud- ies of respiratory diagnoses cited earlier have only touched on these issues by looking at expert opinion about interventions.
Causal analyses. Ultimately, construct validation involves establishing the meaning of constructs. There are large bodies of theory and research that are relevant to the NANDA categories. These include research about patient behaviors, such as self-care and locus of control; patient states, such as anxiety and fatigue; and underly- ing patient physiological states. The process of construct validation involves defining the relation of new cate- gories to well-established categories. The convergent- discriminant validity paradigm of Campbell and Fiske (1959) is a well-known model for assessing convergences and divergences in constructs across measurement domains. As research mounts, it becomes possible to move away from expert judgment of the categories to the development of diagnostic checklists and scales. No such studies were done of IBP, IAC, and IGE.
Generalizability. The ability to extend knowledge to other populations, generalizability, was termed external validity by Cook and Campbell (1979). In the past, respira- tory diagnostic studies used convenience samples of patients, rather than sampling from the wide variety of patient domains, and, where they have been multi-institu- tional, sample size has not permitted comparison of institu- tions. The diagnostic categories need to be examined a m s institutions, for different ICD-9 categories, and for diffemt clinical situations such as changes in body position (Robichaud, 1990). The question here is not just occurrence in different p u p s , but whether the same underlying causal and predictive relationships hold in different settings.
Controversies. One controversy to consider is the best type of research design, e.g., experimental/clinical trials, field studies, and quasi-experiments. Cook and
148 Nursing Diagnosis Volume 9, No. 4, OctoberDecember, 1998

Campbell (1 979) emphasized causal analysis and leaned toward the experimental model; Cronbach (1982) emphasized generalizability. There is always a trade-off between precise causal analysis and the use of generaliz- able natural settings. To study a number of issues out- lined above, more complex and larger designs are neces- sary. Construct validation can be conducted, however, by aggregation of a large number of small incremental stud- ies using similar designs as described by Carlson- Catalan0 and Lunney (1995).
Another controversy is whether constructs should be homogeneous or heterogeneous. The opposing traditions in construct development are factor analysis, which emphasizes coherence of constructs, and the theory- based or rational approach, which emphasizes the scope of underlying theory. The variety of studies necessary for ongoing development of a classification system probably involves both sides of each of these controversies.
Conclusions
Nurses who are testing the validity of diagnostic concepts for the NANDA taxonomy need to move beyond content validation studies so the signs and symptoms of nursing diagnoses approved by NANDA are supported by a series of studies. Moving beyond nurse validation surveys to studies of construct and cri- terion-related validity increases the possibility, but does not guarantee, that nurses who use these concepts will make useful diagnoses as the basis for interventions and outcomes.
A systematic call for nursing diagnosis research by other organizations besides NANDA will help advance this agenda. To set nursing diagnosis research as a high priority for the next 25 years, nurses need to influence the reviewers of the National Institute of Nursing Research, National Institutes of Health, and private foun- dations who support nursing research. The construct and criterion-related validity of diagnoses on the NANDA list, and other diagnoses not yet on the list, need to be studied to improve the overall validity of the taxonomy.
To accomplish these goals, research funds are needed. The importance of these issues needs to be addressed in many forums so that funding sources will value the development of a valid and reliable taxonomy of human responses. Larger studies, involving more nurses, more patients, more settings, and more modalities of data col- lection need to be designed if a full program of construct validation is to be achieved.
One way this can be done is to attend to the accuracy of nurses' diagnoses (Lunney 1998; Lunney Karlik, Kiss, & Murphy, 1997; Lunney & Paradiso, 1995). Taking credit for high levels of accuracy that are occurring and taking responsibility for lower levels of accuracy may prompt funding agencies and agency administrators to focus on the NANDA taxonomy as a tool to facilitate continuous quality improvement. Even more important, perhaps, is a focus on outcomes. If nurses can demon- strate that the classification system leads to interventions that improve therapeutic outcomes, arguments for fund- ing will be compelling.
References
Adorno, T.W., Frenkel-Brunswick, E., Levinson, D.J., & Sanford, R.N. (1950). The authoritarian personality. New York Harper.
Alexander, C. (1989). Epidemiological approaches to validation of nurs- ing diagnoses. In Monograph of the Invitational Conference on Research Methods for Validation of Nurs ing Diagnoses (pp. 121 -136). Philadelphia: NANDA.
American Nurses Association. (1995). Nursing data systems: The emerging framework. Washington, DC: American Nurses Publishing.
Boisvert, C. (1995). Validation of four nursing diagnoses in France: A preliminary report. In M.J. Rantz & I? Lemone (Eds.), Classification of nursing diagnoses: Proceedings of the eleventh conference (pp. 182-188). Glendale, CA CINAHL.
Brukwitzki, G., Holmgren, C., & Maibusch, R. (1996). Validation of defining characteristics of the nursing diagnosis ineffective airway clearance. Nursing Diagnosis, 7,63 -69.
Campbell, D.T., & Fiske, D.W. (1959). Convergent and discriminant val- idation by the multitrait-multimethod matrix. Psychological Bulletin,
Capuano, T.A., Hitchings, K.S., & Johnson, S. (1990). Respiratory nurs- ing diagnoses: Practicing nurses' selection of defining characteris- tics. Nursing Diagnosis, 1,169-174.
Carhn-Catalano, J., & Lunnq, M. (1995). Quantitative methods for clini- cal validation of nursing diagnoses. Clinical Nurse Specialist, 9,306-311.
56,81-105.
Nursing Diagnosis Volume 9, No. 4, Odober-December, 1998 149

Moving Beyond Content Validation of Nursing Diagnoses
Carlson-Catalano, J., Lunney, M., Paradiso, C., Bruno, J., Luise, B.K., Martin, T., Massoni, M., & Pachter, S. (1995). Clinical validation of three respiratory nursing diagnoses (abstract). In M.J. Rantz & I? LeMone (Eds.), Classification of nursing diagnoses: Proceedings of the eleventh conference (pp. 214-215). Glendale, CA: CINAHL.
Carlson-Catalano, J., Lunney, M., Paradiso, C., Bruno, J., Luise, B.K., Martin, T., Massoni, M., & Pachter, S. (1998). Clinical validation of ineffective breathing pattern, ineffective airway clearance and impaired gas exchange. l m g e , 30,243-248.
Chang, B.L. (1989). Reliability and construct validity In Monograph of the Invitational Conference on Research Methods for Validation of Nursing Diagnoses (pp. 217-234). Philadelphia: NANDA.
Clark, C.M. (1994). Validation of the defining characteristics of ineffec- tive airway clearance. In R.M. Carroll-Johnson & M. Paquette (Eds.), Classification of nursing diagnoses: Proceedings of the tenth con- ference (p. 334). Philadelphia: Lippincott.
Cook, T.D., & Campbell, D.T. (1979). Quasi-experimentation: Design and analysis issues for field settings. Boston: Houghton Mifflin.
Cronbach, L.J. (1982). Designing evaluations of educational and social pro- grams. New York Jossey-Bass.
Cronbach, L.J. (1990). Essentials of psychological testing (5th ed.). New York HarperCollins
Dougherty, C.M., Jankins, J.K., Lunney, M., & Whitley, G. (1993). Conceptual and research-based validation of nursing diagnoses: 1950-1993. Nursing D&nosis, 4,156-165.
Foucault, M. (1970). The order of things. London: Tavistock. Gordon, M. (1994). Nursing diagnosis: Process and application (3rd ed.). St.
Louis: Mosby-YearBook. Gordon, M., & Hiltunen, E. (1995). High frequency treatment priority
nursing diagnoses in critical care. Nursing Diagnoses, 6,143- 154. Guzzetta, C., Kinney, M. & Grant, J., (1994). Symposium on validation
models (1994). In R.M. Carroll-Johnson & M. Paquette (Eds.), Classification of nursing diagnoses: Proceedings of the tenth conference (pp. 42-62). Philadelphia: Lippincott.
Hayakawa, S.I., & Hayakawa, A.R. (1990). Language in thought and action (5th ed). San Diego: Harcourt Brace.
Hoskins, L.M. (1989). Clinical validation methodologies for nursing diagnosis research. In R.M. Carroll-Johnson (Ed.), Classification of nursing diagnoses: Proceedings of the eighth conference (pp. 126- 131). Philadelphia: Lippincott.
Hoskins, L.M., Kerr, M.E., Fitzpatrick, J.J., Warren, J.J., Avant, K., Carpenito, L.J., Hurley, M.E., Jakob, D.F., Lunney, M., Mills, W., & Rottcamp, B.C. (1992). Axes: Focus for Taxonomy 11. Nursing Dingnosis, 3,117-123.
Hoskins, L.M., McFarlane, E.A., Rubenfeld, M.G., Schreier, A.M., & Walsh, M.B. (1986). Nursing diagnosis in the chronically ill. In M.E. Hurley (Ed.), Classification of nursing diagnoses: Proceedings of the sixth conference (pp. 319-329). St. Louis: Mosby
Johnson, M., & Maas, M. (Eds.). (1997). Nursing outcomes classification (NOC). St. Louis: Mosby.
Ken; M. (1991). Validation of taxonomy In R.M. Carroll-Johnson (Ed.), Classification of nursing diagnoses: Proceedings of the ninth conference (pp. 37-63). St. Louis: Mosby.
Kerr, M. (1994). How reliable are your reliability measures? In R.M. Carroll-Johnson & M. Paquette (Eds.), Classification of nursing diag- nosis: Proceedings of the tenth conference (pp. 291 -293). Philadelphia: Lippincott.
Kerr, M.E., Hoskins, L.M., Fitzpatrick, J.J., Warren, J.J., Avant, K., Carpenito, L.J., Hurley, M.E., Jakob, D.F., Lunney, M., Mills, W., & Rottcamp, B.C. (1992). Development of definitions for Taxonomy 11. Nursing Diagnosis, 3,65-71.
Kerr, M.E., Hoskins, L.M., Fitzpatrick, J.J., Warren, J.J., Avant, K.C., Hurley, M.E., Lunney, M., Mills, W.C., & Rottkamp, B.C. (1993). Taxonomic validation: An overview. Nursing Diagnosis,
Lunney, M. (1998). Commentary: Accuracy of nurses' diagnoses- Foundation of NANDA, NIC, and NOC. Nursing Diagnosis, 9,
Lunney, M., Karlik, B., Kiss, M., & Murphy, P. (1997). Accuracy of nurses' diagnoses of psychosocial responses. Nursing Diagnosis, 8,
Lunney, M., & Paradiso, C. (1995). Accuracy of interpreting human responses. Nursing Management, 6(1), 48H-48K.
Lutjens, L. (1993). The nature and use of nursing diagnosis in hospitals. Nursing Diagnosis, 4,107-113.
Matsuki, M., & Otani, E. (1995). Diagnostic content validation for anxi- ety, hopelessness, and ineffective airway clearance. In M.J. Rantz & I? Lemone (Eds.), Classification of nursing diagnoses: Proceedings of the eleventh conference (pp. 275-276). Glendale, CA: CINAHL.
McCloskey, J.C., & Bulechek, G.M. (Eds.). (1996). Nursing interventions classification (NIC) (2nd ed.). St. Louis: Mosby-Yearbook.
McDonald, B.R. (1985). Validation of three respiratory nursing diag- noses. Nursing Clinics of North America, 20,697-710.
Robichaud, A.M. (1990). Alteration in gas exchange related to body position. Critical Care Nurse, 10(1), 56-59.
Wake, M.M., Fehring, R.J., & Fadden, T. (1991). Multinational valida- tion of anxiety, hopelessness and ineffective airway clearance. Nursing Diagnosis, 2,57-66.
Whitley, G.G. (1995). Concept analysis as foundation to nursing diag- nosis. Nursing Diagnosis, 6,91-92.
Whitley, G.G. (In press). Process and methodologies for research valida- tion of nursing diagnosis. Nursing Diagnosis.
Whitley, G.G., & Tousman, S.A. (1996). A multivariate approach for the validation of anxiety and fear. Nursing Diagnosis, 7,116- 127.
Wooldridge, J., Herman, J., Garrison, C., Haddock, S., Massey, J., & Tavakoli, A. (1998). A validation study using the case control method of the nursing diagnosis Risk for Aspiration. Nursing Diagnosis, 9,5-13.
York, K. (1985). Clinical validation of two respiratory nursing diagnoses and their defining characteristics. Nursing Clinics of North America,
4, 6-14.
83-85.
157- 166.
20,657-667.
Author contact: [email protected]
150 Nursing Diagnosis Volume 9, No. 4, October-December, 1998