Embed Size (px)
Citation preview
~~ ~~ ~~ ~~ ~~ ~
Case Finding in Elderly, Gerson el al. 729
Northeastern Ohio Universities College of Medicine. Akron OH
Division of Community Health Sciences (LWG)
University of Arizona Health Sciences Center. Tucson A 2
Arizona Center on Aging. Long Term Care (EWR)
Resurrection Medical Center. Chicago. IL
( M H ) Department of Emergency Medicinc
Boston City Hospital. Boston. MA Department of Emergency Medicine (EB)
Orcgon Health Sciences University, Ponltind. OR
Department of Emergency .Medicine (SK)
Reccived: May 13. 1994 Revision received: August 12. 1994 Accepted: August 20. 1994
Prior presentation: SAEM annual meeting. Washington. DC. .May 1994.
Acknowled-ments: Supported in part by a grant from the John A. Hartford Foundation. Contributors at study sites: Akron City Hospita!. Summa Health System, Sortheasiern Ohio Lnivcrsities College of Medicine: Carol Bojanowski. .MSS. RS. CHS. Steven R. Counsell. MD. Phil B. Fontanarosa. MD. and William D. Smucker. MD. Boston City Hospital: Donna Dicenso. RSP. Eric Hardt. MD, Sharon Levine. MD. and Barbara Ryan. RS. Oregon Health Sciences University. University Hospital: Jerris Hedges. .MD. M S . St. Francis Hospital: Glenn Aldinger. MD. University of Arizona Health Sciences Center: Ar:hur B. Sanders. MD. and Mark Tibbitts. BA. Address for correspondence and reprints:
Lowell W. Gerson. PhD Northeastern Ohio Universities College of Medicine PO Box 95 Roo:stow. OH 31272-0095
Key words: aged; emergency medical senices: E.MS; emergency depanment; geriatric care: social services
I EDUCATION AND PRACTICE
Multicenter Study of Case Finding in Elderly Emergency Department Patients
Lowell W. Gerson, PhD, Elaine W. Rousseau, PhD, Teresita M . Hogan, MD, Edward Bemstein, MD, Norman Kalbfleisch, MD
1 ABSTRACT
Objectives: To assess the feasibility of a brief comprehensive case- finding program for detecting functional, cognitive, and social im- pairments among elderly ED patients and to estimate the prevalence of unknown, undetected, or untreated impairments elderly patients may have.
Methods: A multicenter prospective study conducted at five private and public hospital EDs in five different communities across the country. Patients aged 60 years and older released to their homes during 52 randomly selected evening and weekend shifts between February 1 and April 30, 1993, were eligible for the case-finding program. They were evaluated by medical students who received special training (instructional videotape, supervised examinations, and conference calls) in the administration of a standardized 17-item protocol that included an interview and simple tests of function. The patients' physicians were notified of the screening results and were asked to return a one-month follow-up questionnaire. The physicians answered whether the presumed problem had been confirmed and whether a treatment plan for a new problem had been developed.
Results: Patient acceptance of the case-finding program was good; 252 of 338 eligible patients (75%) agreed to participate, and 281 conditions were detected for 242 screened patients (96%). The most frequently reported problems were with: performing the activities of daily living (79%); vision (55%); lack of influenza vaccination (54%); home environment (49%); mental status (46%); general health (41%); falls (40%); and depression (36%). The physicians returned ques- tionnaires for 153 patients (63%); 76 patients (50%) were evaluated at follow-up visits, during which 47 newly identified problems (62%) were confirmed and treatment plans were developed for 25 problems (53%) among 21 patients. A mean time of 17.7 ? 10.2 minutes was required to complete the screen.
Conclusions: A brief comprehensive case-finding program for func- tional, cognitive, and social impairment among elderly ED patients is feasible. The screening uncovered a significant amount of morbidity among older patients visiting EDs.
Acad. Emerg. Med. 1995; 2:729-734.
~~ ~
ACADEMIC EMERGENCY MEDICINE AUG 1995 VOL 2/NO 8 730
I One in eight Americans is over the age of 65 years, and by the year 2030, the proportion will be almost one in four.' People in this country who reach age 65 can expect to live another 17 years.2 A Department of Health and Human Services publication has stated that the nation's health goals for the aged must focus on the quality of life in those additional 17 years.3 Illnesshnjury prevention, particularly secondary prevention (the early detection of impairment), has been recommended by numerous national groups3-' and teams of clinician/ investigator^^^^ as an effective strategy for achieving the goal of healthy older Americans. These reports em- phasize the importance of the role of patients' personal physicians in primary and secondary illnesdinjury pre- vention. In doing so they overlook the frequency of the elderly's use of the ED as a source of medical care.1° The ED is an excellent place to introduce secondary prevention. It is a place where elderly persons who have functional, cognitive, and social impairments may be identified and linked to appropriate services for further evaluation and treatment.
While the ED may be a strategic location for case finding, we found no English-language article about broad-based screening programs for the aged in the ED, upon searching the MEDLINE files for 1983 forward. Gerson and colleagues" have recently reported a suc- cessful out-of-hospital screening program in which par-
amedics attending the elderly in their homes identified patients who were subsequently linked with needed ser- vices. We developed a multicenter pilot study to assess the possible merit of a comprehensive, but brief, case- finding program for detecting functional, cognitive, and social impairments among elderly emergency pa- tients.
I METHODS .......................................................................... ....... .... ...... ............ .........
Study Design This was a multicenter prospective study of elderly
patients presenting to five hospital EDs. The case-find- ing program was conducted from February 1, 1993, through April 30, 1993. Research assistants conducted a brief but extensive evaluation designed to detect the possible presence of functional, cognitive, and social impairments. The patients' physicians were informed of the results and were asked to return a questionnaire that asked in part whether the problem had been con- firmed and whether a treatment plan for a new problem had been developed. Hospital social services were in- formed of cases in which there was a positive response to the screening question regarding abuse, but no data were obtained for these referrals.
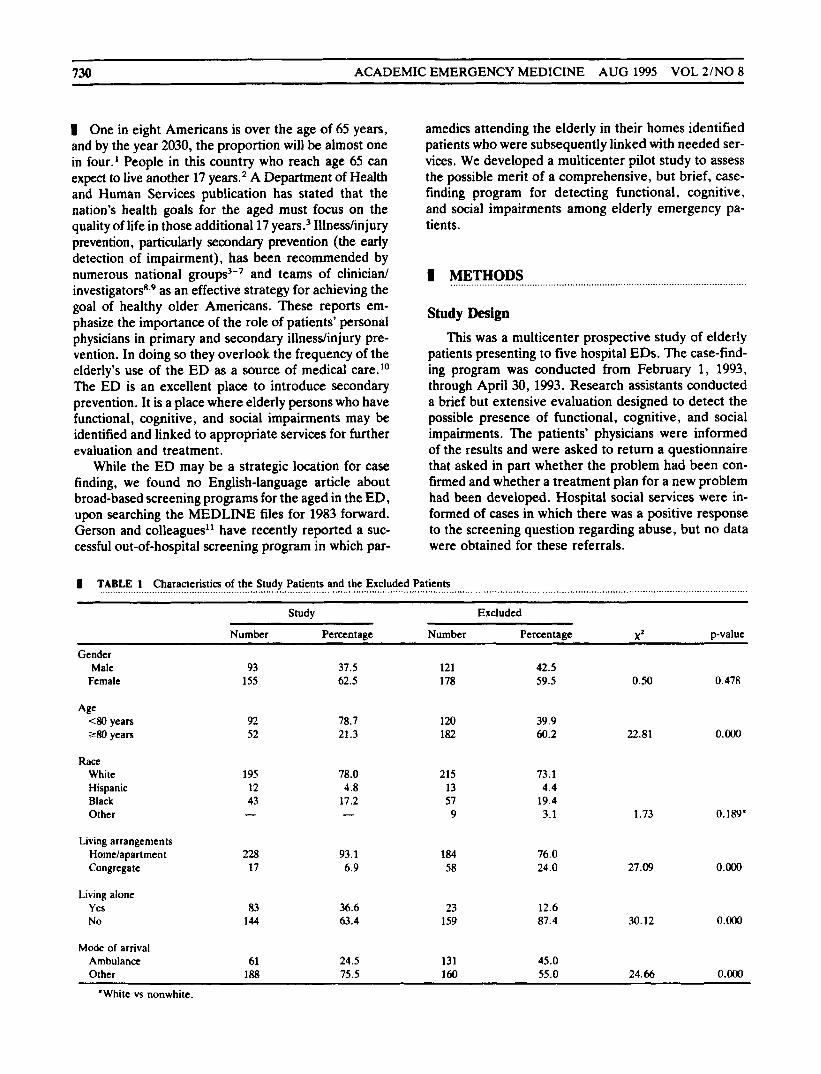
I TABLE 1 Characteristics of the Study Patients and the Excluded Patients
Study Excluded
Number Percentage Number Percentage X 2 p-value
Gender Male
Female 93
155 37.5 62.5
121 178
42.5 59.5 0.50 0.478
92 52
78.7 21.3
120 182
39.9 60.2 22.81 O.OO0
Race White Hispanic Black Other
195 12 43
78.0 4.8
17.2
215 13 57 9
73.1 4.4
19.4 3.1 1.73 0.189.
Living arrangements Homc/apartment Congregate
228 17
93.1 6.9
184 58
76.0 24.0 27.09 O.OO0
Living alone Yes No
83 144
36.6 63.4
23 159
12.6 87.4 30.12 O.OO0
Mode of arrival Ambulance Other
61 188
24.5 75.5
131 160
45.0 55.0 24.66 O.OO0
~
'White vs nonwhite.

Case Finding in Elderly, Gerson et al. 731
Pa tien t Population Five hospital EDs located in various parts of the
country participated in the study. Both private and pub- lic hospitals serving a variety of patients were included. In each ED, the research assistants were to approach all potentially eligible patients during 52 randomly se- lected evening and weekend shifts. Each shift was four hours long. Eligible patients were those who had reached their 60th birthdays, were being released to an inde- pendent community living arrangement, were able to understand the questions, and had given their consent to participate. Mental competence to participate was assessed on a gross level; the patients were able to engage in routine conversation and appeared to answer questions appropriately. Patients who had known de- mentia, whose physical conditions prevented them from being interviewed, or who were unable to communicate were excluded.
The study was approved by the human subjects re- view committees at all participating institutions. Writ- ten informed consent was obtained from all patients. Patients were aware that while their answers were con- fidential, their responses would be shared with ED per- sonnel, their physicians, and the research staff.
Research Assistants The research assistants were primarily medical stu-
dents who completed the patient interview portion of the curriculum. One center used ED research assistants as patient interviewers. To ensure standardization among interviewers, a training videotape was produced. All interviewers read the operations manual and viewed the videotape. After the initial training session the research assistants performed practice evaluations under super- vision. Interviewers also were trained to recognize cog- nitive impairment from various causes (e.g., dementia or other chronic conditions, acute illness, or substance abuse.)
Measurements The case-finding instrument used for this program
was a modified version of a short, easily administered battery of questions and tests of function for ambulatory patients in primary care settings that had been devel- oped by a team from Yale University.8 We added ques- tions about general health,12 polypharmacy, influenza vaccination, alcohol abuse,I3 and elder abuse" to those originally recommended. (The case-finding question- naire is available from the authors on request.) Patients were informed that the results would be sent to their personal physicians and that they were to call the phy- sician for the results and any follow-up that the phy- sician recommended.
Because this was a pilot study to test the potential of an extensive but brief impairment screening program for elderly E D patients, we focused on whether patients benefited from the screening and how well the process operated. Patients were considered to have benefited from the program when impairments were uncovered and confirmed by the patient's personal physician after the ED visit and a treatment plan was developed.
The physicians to whom referrals were made were sent a personal letter that explained the program and listed the abnormalities detected by the screening, along with a questionnaire identifying the 17 conditions from the case-finding instrument. Each referral physician was asked to complete the questionnaire and to return it within 30 days after the patient's ED visit. The physician was asked to report whether the patient followed up, to confirm that the problem was real (true-positive), and to indicate whether the screening had missed any problem of which he or she was aware (false-negative). The physician was asked to report whether the problem had been previously observed and to indicate what treatment was planned or being given. A stamped re- turn envelope was included. The exact date of each patient's ED visit was included in the body of the letter. Physicians who did not respond were recontacted and, if necessary, were sent duplicate letters and return forms.
I RESULTS
Of 562 patients who met the age criterion and were treated in the EDs during the study period, 86 (15.3%) refused to participate. Also excluded were 45 patients (8.0%) who were not approached, 39 (6.9%) who did not speak English, 35 (6.2%) who had known dementia, 31 (5 .5%) who were unable to communicate, 13 (2.3%) who were physically unable to participate, and 61 (10.9%) for a variety of logistic reasons (e.g., patients who were interviewed with an expectation that they would be re- leased home who were subsequently admitted to the hospital or who were with someone who might influence their responses). A total of 252 (44.8%) patients met the inclusion criteria and composed the study group.
The characteristics of the patients who were in- cluded in the study, as well as of those not included, are summarized in Table 1. The patients who were not screened were more likely than those who were screened to be older, to be living in a nursing home or similar facility, and to have arrived at the E D by ambulance. There was no race or gender difference between the screened and unscreened groups.
The study group comprised predominantly women (62.5%) less than 80 years of age (78.7%). The average age of the screened patients was 72.2 k 8.5 years. All of these patients lived in private homes or apartments;
. . . . . . . . . . . . , . . . . . . . . . , , . . , , . . . . . . . . , , . . . . , , . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . , , . . . . . . . . . . . . . . . . , , , . . . . . . , . , , , , . . .
732 ACADEMIC EMERGENCY MEDICINE AUG 1995 VOL 2/NO 8
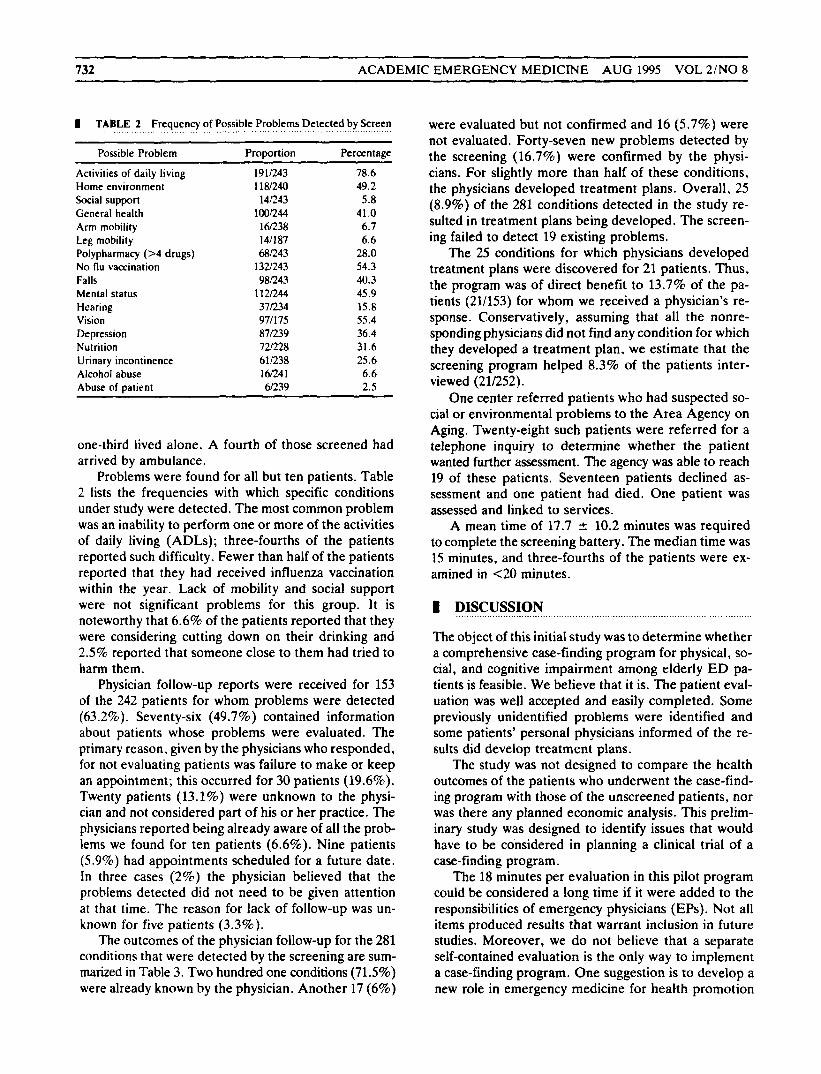
I TABLE 2 Frequency of Possible Problems Detected by Screen
Possible Problem Proportion Percentage
Activities of daily living 191043 78.6 Home environment 118/240 49.2
General health 100044 41 .O Arm mobility 16/238 6.1 Leg mobility 141187 6.6
N o flu vaccination 132/243 54.3 Falls 98043 40.3 Mental status 112044 45.9 Hearing 37034 15.8 Vision 971175 55.4 Depression 871239 36.4 Nutrition 7m2a 31.6 Urinary incontinence 611238 25.6 Alcohol abuse 16/24] 6.6 Abuse of patient 6/239 2.5
Social support 14Q43 5.8
Polypharmacy (>4 drugs) 68043 28.0
one-third lived alone. A fourth of those screened had arrived by ambulance.
Problems were found for all but ten patients. Table 2 lists the frequencies with which specific conditions under study were detected. The most common problem was an inability to perform one or more of the activities of daily living (ADLs); three-fourths of the patients reported such difficulty. Fewer than half of the patients reported that they had received influenza vaccination within the year. Lack of mobility and social support were not significant problems for this group. It is noteworthy that 6.6% of the patients reported that they were considering cutting down on their drinking and 2.5% reported that someone close to them had tried to harm them.
Physician follow-up reports were received for 153 of the 242 patients for whom problems were detected (63.2%). Seventy-six (49.7%) contained information about patients whose problems were evaluated. The primary reason, given by the physicians who responded, for not evaluating patients was failure to make or keep an appointment; this occurred for 30 patients (19.6%). Twenty patients (13.1%) were unknown to the physi- cian and not considered part of his or her practice. The physicians reported being already aware of all the prob- lems we found for ten patients (6.6%). Nine patients (5.9%) had appointments scheduled for a future date. In three cases (2%) the physician believed that the problems detected did not need to be given attention at that time. The reason for lack of follow-up was un- known for five patients (3.3%).
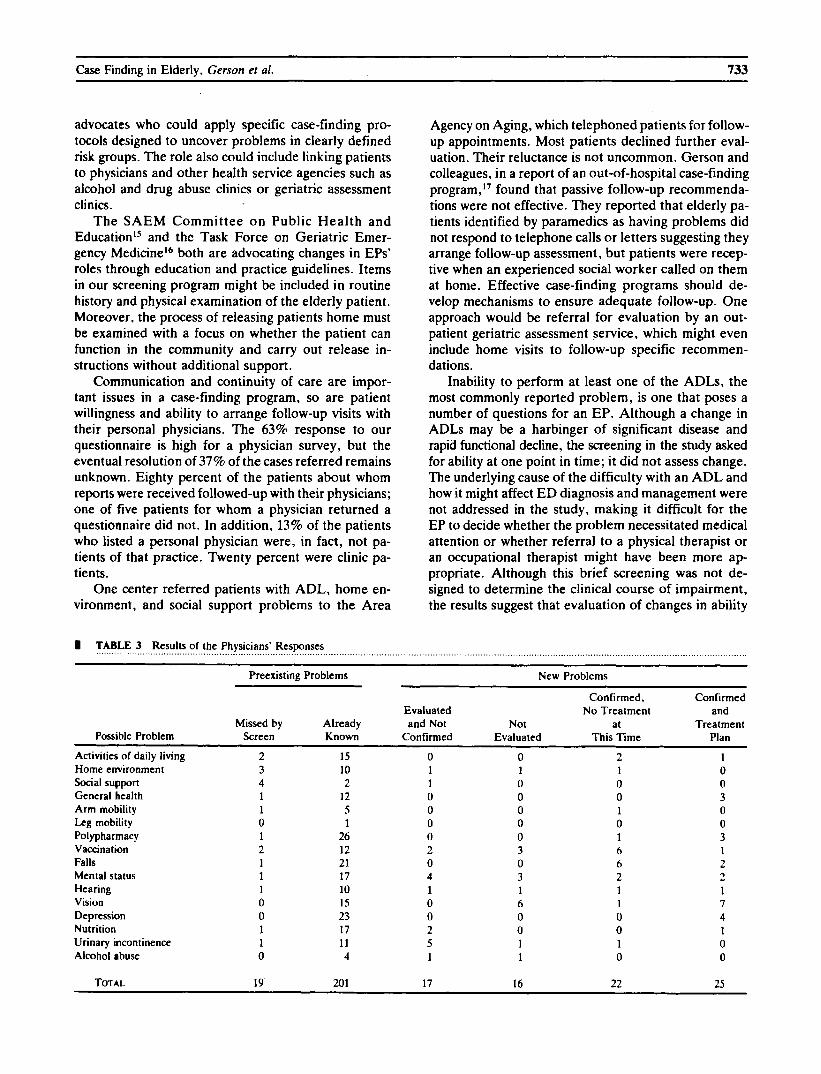
The outcomes of the physician follow-up for the 281 conditions that were detected by the screening are sum- marized in Table 3. Two hundred one conditions (71.5%) were already known by the physician. Another 17 (6%)
were evaluated but not confirmed and 16 (5.7%) were not evaluated. Forty-seven new problems detected by the screening (16.7%) were confirmed by the physi- cians. For slightly more than half of these conditions, the physicians developed treatment plans. Overall, 25 (8.9%) of the 281 conditions detected in the study re- sulted in treatment plans being developed. The screen- ing failed to detect 19 existing problems.
The 25 conditions for which physicians developed treatment plans were discovered for 21 patients. Thus, the program was of direct benefit to 13.7% of the pa- tients (21/153) for whom we received a physician’s re- sponse. Conservatively, assuming that all the nonre- sponding physicians did not find any condition for which they developed a treatment plan, we estimate that the screening program helped 8.3% of the patients inter- viewed (21/252).
One center referred patients who had suspected so- cial or environmental problems to the Area Agency on Aging. Twenty-eight such patients were referred for a telephone inquiry to determine whether the patient wanted further assessment. The agency was able to reach 19 of these patients. Seventeen patients declined as- sessment and one patient had died. One patient was assessed and linked to services.
A mean time of 17.7 2 10.2 minutes was required to complete the screening battery. The median time was 15 minutes, and three-fourths of the patients were ex- amined in <20 minutes.
m DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . , . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
The object of this initial study was to determine whether a comprehensive case-finding program for physical, so- cial, and cognitive impairment among elderly ED pa- tients is feasible. We believe that it is. The patient eval- uation was well accepted and easily completed. Some previously unidentified problems were identified and some patients’ personal physicians informed of the re- sults did develop treatment plans.
The study was not designed to compare the health outcomes of the patients who underwent the case-find- ing program with those of the unscreened patients, nor was there any planned economic analysis. This prelim- inary study was designed to identify issues that would have to be considered in planning a clinical trial of a case-finding program.
The 18 minutes per evaluation in this pilot program could be considered a long time if it were added to the responsibilities of emergency physicians (EPs). Not all items produced results that warrant inclusion in future studies. Moreover, we do not believe that a separate self-contained evaluation is the only way to implement a case-finding program. One suggestion is to develop a new role in emergency medicine for heahh promotion
advocates who could apply specific case-finding pro- tocols designed to uncover problems in clearly defined risk groups. The role also could include linking patients to physicians and other health service agencies such as alcohol and drug abuse clinics or geriatric assessment clinics.
The SAEM Committee on Public Health and Educationls and the Task Force on Geriatric Emer- gency Medicinet6 both are advocating changes in EPs’ roles through education and practice guidelines. Items in our screening program might be included in routine history and physical examination of the elderly patient. Moreover. the process of releasing patients home must be examined with a focus on whether the patient can function in the community and carry out release in- structions without additional support.
Communication and continuity of care are impor- tant issues in a case-finding program, so are patient willingness and ability to arrange follow-up visits with their personal physicians. The 63% response to our questionnaire is high for a physician survey, but the eventual resolution of 37% of the cases referred remains unknown. Eighty percent of the patients about whom reports were received followed-up with their physicians; one of five patients for whom a physician returned a questionnaire did not. In addition, 13% of the patients who listed a personal physician were, in fact, not pa- tients of that practice. Twenty percent were clinic pa- tients.
One center referred patients with ADL, home en- vironment, and social support problems to the Area
TABLE 3 Results of the Physicians’ Responses ........ .. .. .................................................... ....... ..__.... . . . . . . . . . . . . .
Agency on Aging, which telephoned patients for follow- up appointments. Most patients declined further eval- uation. Their reluctance is not uncommon. Gerson and colleagues, in a report of an out-of-hospital case-finding program,” found that passive follow-up recommenda- tions were not effective. They reported that elderly pa- tients identified by paramedics as having problems did not respond to telephone calls or letters suggesting they arrange follow-up assessment, but patients were recep tive when an experienced social worker called on them at home. Effective case-finding programs should de- velop mechanisms to ensure adequate follow-up. One approach would be referral for evaluation by an out- patient geriatric assessment service, which might even include home visits to follow-up specific recommen- dations.
Inability to perform at least one of the ADLs, the most commonly reported problem, is one that poses a number of questions for an EP. Although a change in ADLs may be a harbinger of significant disease and rapid functional decline, the screening in the study asked for ability at one point in time; it did not assess change. The underlying cause of the difficulty with an ADL and how it might affect ED diagnosis and management were not addressed in the study, making it difficult for the EP to decide whether the problem necessitated medical attention or whether referral to a physical therapist or an occupational therapist might have been more ap- propriate. Although this brief screening was not de- signed to determine the clinical course of impairment, the results suggest that evaluation of changes in ability
Preexisting Problems New Problems
Confirmed, Confirmed
Missed by A 1 re ad y and Not Not at Treatment Evaluated N o Treatment and
Possible Problem Screen Known Confirmed Evaluated This Time Plan ~~ ~~
Activities of daily living 2 15 0 0 2 1 Home environment Social support General health Arm mobility Leg mobility Polypharmacy Vaccination Falls Mental status Hearing Vision Depression Nutrition Urinary incontinence Alcohol abuse
3 4 1 1 0 1 2 1 1 1 0 0 1 1 0
10 2
12 5 1
26 12 21 17 10 15 23 17 11 4
1 1 0 0 0 0 2 0 4 1 0 0 2 5 1
1 0 0 0 0 0 3 0 3 1 6 0 0 1 1
1 0 0 1 0 1 6 6 2 1 1 0 0 1 0
0 0 3 0 0 3 1 2 2 1 7 4 1 0 0
TOTAL 19 201 17 16 22 25

734 ACADEMIC EMERGENCY MEDICINE AUG 1995 VOL 21NO 8
to perform ADLs deserves more attention in the ED, since such changes are often associated with significant health problems. Similar arguments may be made for examining changes in mental status, including depres- sion.
More than 54% of the patients studied did not have a current influenza vaccination, not significantly differ- ent from the 63% reported by Rodriguez and Baraff.18 These researchers offered pneumococcal and influenza vaccination to unvaccinated elderly patients, and more than half accepted. Thus, ED vaccination of these older patients could be highly appropriate.
Problems with social support, arm and leg mobility, and alcohol abuse were, when compared with other problems, infrequently reported or observed. Never- theless, they occurred with sufficient frequency to war- rant questioning elderly patients and observing their mobility.
This study was designed to avoid interference with normal ED operations. Interviewing was done largely by medical students and was restricted to evenings and weekends-when normal social services would not be available. It is possible that elderly patients who present at these times may have different levels of impairment than do patients who visit the ED at other times. Ad- ditional research is required to assess the value of a case-finding program where assessment is performed by ED personnel as part of their normal activities. On the other hand, there may be merit in hiring and training a cohort of individuals who can perform a brief com- prehensive screening. Patients for whom problems are suspected might be evaluated by a trained geriatric nurse in the ED, referred to an outpatient geriatric assessment service, or referred to a personal physician.
I CONCLUSION
A brief comprehensive case-finding program for func- tional, cognitive, and social impairment among elderly ED patients is feasible. The screening approach we used uncovered a significant amount of morbidity, and 14% of the patients for whom follow-up was available ben- efited from the program.
I REFERENCES
1. U.S. Senate Special Committee on Aging. Aging America: Trends and Projections. Washington, DC: U.S. Department of Health and Human Services, 1988.
2. National Center for Health Statistics. Vital Statistics of the United States, 1988; vol 2. sec 6, life tables. DHHS Publication No. (PHS) 91-1 104. Washington, DC: U.S. Government Printing Of- fice, 1991.
3. Department of Health and Human Services. Healthy People 2OOO: National Health Promotion and Disease Prevention Objectives. DHHS Publication No. (PHS) 91-50212. Washington, DC: U.S. Government Printing Office, 1991.
4. US. Preventive Services Task Force. Guide to Clinical Preven- tive SeMces: An Assessment of the Effectiveness of 169 Inter- ventions. Baltimore: Williams & Wilkins. 1989.
5. Rubenstein LV. Calkins DR, Greenfield S . et al. Health status assessment for elderly patients: report of the Society of General Internal Medicine Task Force on Health Assessment. J Am Ger- iatr Soc. 1989; 37562-9.
6. National Cancer Institute. Working Guidelines for Early Cancer Detection: Rationale and Supporting Evidence to Decrease Mor- tality. Bethesda, MD: National Cancer Institute, 1987.
7. Medical Practice Committee, American College of Physicians. Periodic health examination: a guide for designing individualized preventive health care in the asymptomatic patient. Ann Intern
8. Lachs MS. Feinstein AR, Cooney LM, et al. A simple procedure for general screening for functional disability in elderly patients. Ann Intern Med. 1990; 112599-706.
9. Klinkman MS, Zazove P. Mehr DR, Ruffin MT. A criterion- based review of preventive health care in the elderly: part 1. Theoretical framework and development of criteria. J Fam Pract
10. Strange GR, Chen EH. Sanders AB. Use of emergency depart- ments by elderly patients: projections from a multicenter data base. Ann Emerg Med. 1992; 21:819-24.
11. Gerson LW. Schelble DT, Wilson JE. Using paramedics to iden- tify at-risk elderly. Ann Emerg Med. 1992; 21:688-91.
12. Rackowski W, Mor V, Hiris J. The association of self-rated health with two year mortality in a sample of well elderly. J Aging Health. 1991; 3527-43.
13. Ewing JA. Detecting alcoholism: the CAGE questionnaire. JAMA.
14. Neale AV, Hwalek MA, Scott RO, et al. Validation of the Hwa- lek-Sengstock elder abuse screening test. J Appl Gerontol. 1991;
15. Bernstein E, Goldfrank LR, Kellerman AL. et al. A public health approach to emergency medicine: preparing for the twenty-first century. Acad Emerg Med. 1994; 13277-86.
16. Sanders AB. Care of the elderly in emergency departments: con- clusions and recommendations. Ann Emerg Med. 1992; 21:830- 4.
17. Gerson LW, Hoover R, McCoy S, Palmisano B. Linking the elderly tocommunity services. J Emerg Med Sew. 1991; 16:45-8.
18. Rodriguez RM, Baraff LJ. Emergency department immunization of the elderly with pneumococcal and influenza vaccines. Ann Emerg Med. 1993; 21:1729-32.
Med 1981; 95:729-32.
1992; 34205-24.
1984; 252:1905-7.
10:406- 18.





























