Embed Size (px)
Citation preview
ELSEVIER Journal of the Neurological Sciences 126 (1994) 232-236
JOURNAL OF THE
NEUROLOGICAL SCIENCES
Shor t r e p o r t
Multifactorial obstructive sleep apnea in a patient with Chiari malformation
E. W e s l e y Ely a,*, W. V a u g h n M c C a l l b, E d w a r d F. H a p o n i k c
a Section on Pulmonary and Critical Care Medicine, Winston-Salem, NC 27157-1054, USA b Department of Psychiatry and Behavioral Medicine, Winston-Salem, NC 27157-1054, USA
c Department of Medicine, Section on Pulmonary and Critical Care Medicine, Bowman Gray School of Medicine of Wake Forest University, Medical Center Boulevard, Winston-Salem, NC 27157-1054, USA
Received 21 April 1994; revised 29 June 1994; accepted 11 July 1994
Abstract
We report a pat ient with severe obstructive sleep apnea (OSA) associated with a unique combination of syringobulbia-myelia, Chiari malformation type I (CM), absent hypoxic ventilatory drive, vocal cord paralysis, post -menopausal status, obesity, and acute respiratory failure necessitating mechanical ventilation. The remote onset of OSA five years after surgery underscores the need for long-term follow-up of pat ients with syringobulbia-myelia and CM and the importance of addressing multiple interacting neurologic, metabolic, and mechanical predisposit ions to s leep-disordered breathing.
Keywords: Chiari malformation; Obstructive sleep apnea; Syringobulbia-myelia
I. Introduction
Sleep apnea is an under-diagnosed, serious cause of morbidity and mortality estimated to occur in 2% of middle-aged women and 4% of men (Young et al. 1993). We present a patient with severe obstructive sleep apnea (OSA), surgically corrected syringobulbia- myelia with residual Chiari malformation type I (CM), permanent cranial nerve (CN) dysfunction with absent hypoxic ventilatory drive, vocal cord paralysis and mul- tiple other sites of anatomic upper airway obstruction, postmenopausal state, obesity, and periodic leg move- ments (PLM). This patient's unique, interacting predis- positions to sleep-disordered breathing resulted in near-fatal respiratory failure and cor pulmonale. Her evaluation and clinical course underscore the many pathophysiologic and management issues that must be addressed in patients with OSA.
* Corresponding author. Tel.: (910) 716-4649; Fax: (910) 716-7277. Abbreviations: ABG, arterial blood gas; CM, Chiari malformation
type I; CN, cranial nerve; CPAP, continuous positive airway pres- sure; ICP, intracranial pressure; OSA, obstructive sleep apnea; PLM, periodic leg movements.
0022-510X/94/$07.00 © 1994 Elsevier Science B.V. All rights reserved SSDI 0022-510X(94)00174-X
2. Case report
A 48-year-old woman with history of syringobulbia-myelia and CM (decompressed surgically 4 years earlier), obesity, cigarette smoking, hypertension, diabetes and previous hysterectomy and bi- lateral salpingo-oophorectomy presented to the emergency depart- ment with a 2-3-month history of daytime hypersomnolence, inter- mittent headaches, insomnia, memory loss, progressive dyspnea, and dependent edema. Her family reported loud snoring and had wit- nessed multiple apneic episodes. Admission arterial blood gas (ABG) on 2 liters nasal cannula oxygen showed a pH of 7.35, PaCO 2 61 mm Hg, PaO 2 34 mm Hg. On physical examination, vital signs included a pulse of 90 beats/min, respiratory rate of 16-18 breaths/min, weight of 233 pounds, and height of 64 inches. The patient was dyspneic and in obvious respiratory distress. Her oropharynx was markedly nar- rowed posteriorly with edematous oropharyngeal mucosa. Breath sounds were reduced bilaterally, with few bibasilar crackles; heart sounds were distant with a grade I I / IV apical systolic murmur. Lower extremities showed 2 + / 4 edema. The patient was lethargic but awake and oriented to person, place and time. CN exam revealed an absent gag reflex on the right-side only with an intact gag on the left and fasciculation of the right side of her tongue. There was no heart rate response to prolonged right-sided carotid massage but an intact heart rate response to left carotid massage. Slight weakness of the right arm and leg and diminished sensation in her right hand and leg (which had been persistent for years) were also present. The chest roentgenogram showed pulmonary edema, and the electrocar- diogram showed right atrial hypertrophy, low voltage, and inferior T-wave inversions. Follow-up ABG (on 35% O 2 via Venturi mask) showed a pH of 7.31, PaCO 2 92 mm Hg, PaO 2 73 mm Hg. The
E.W.. Ely et al. /Journal of the Neurological Sciences 126 (1994) 232-236 233
2 0 .
E
~ 15,
~ 10,
5
%
Hypoxlc Ventilatory Response 8 L/Sec
~ "m~:lRl'~' 6 4
-2-
0 I I I I I I I
350 300 250 200 150 100 50 0
PaO2 (mm HO)
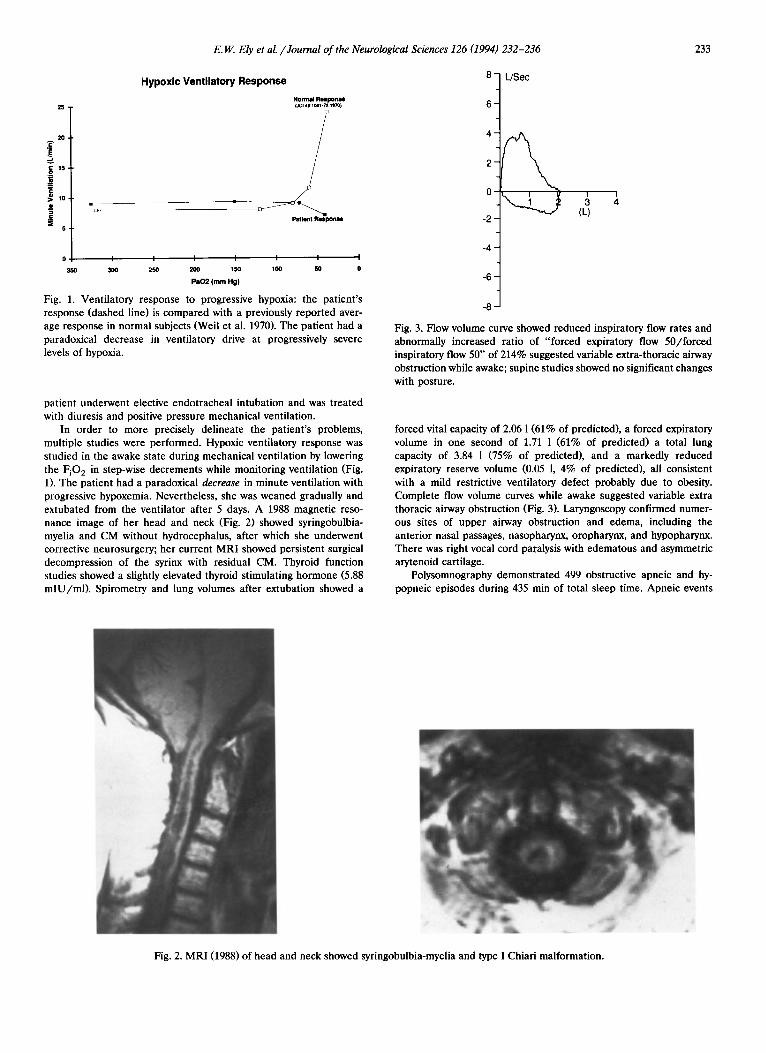
Fig. 1. Ventilatory response to progressive hypoxia: the patient's response (dashed line) is compared with a previously reported aver- age response in normal subjects (Weil et al. 1970). The patient had a paradoxical decrease in ventilatory drive at progressively severe levels of hypoxia.
patient underwent elective endotracheal intubation and was treated with diuresis and positive pressure mechanical ventilation.
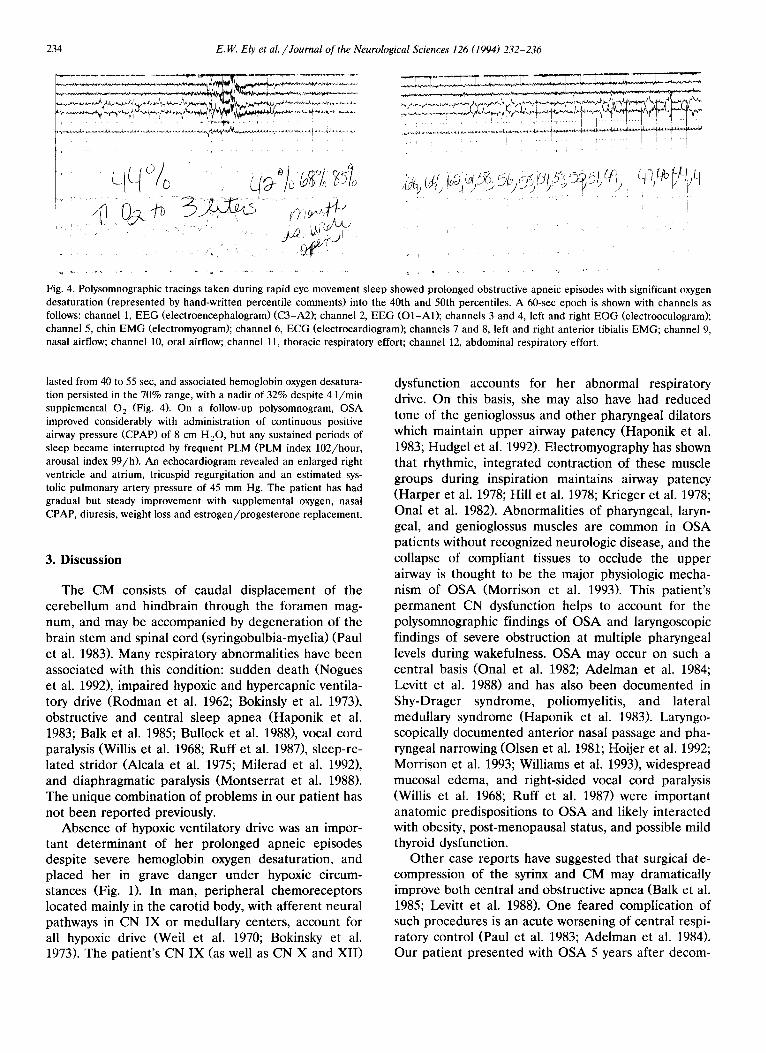
In order to more precisely delineate the patient's problems, multiple studies were performed. Hypoxic ventilatory response was studied in the awake state during mechanical ventilation by lowering the FiO 2 in step-wise decrements while monitoring ventilation (Fig. 1). The patient had a paradoxical decrease in minute ventilation with progressive hypoxemia. Nevertheless, she was weaned gradually and extubated from the ventilator after 5 days. A 1988 magnetic reso- nance image of her head and neck (Fig. 2) showed syringobulbia- myelia and CM without hydrocephalus, after which she underwent corrective neurosurgery; her current MRI showed persistent surgical decompression of the syrinx with residual CM. Thyroid function studies showed a slightly elevated thyroid stimulating hormone (5.88 mlU/ml) . Spirometry and lung volumes after extubation showed a
-4-
- 6 -
-8
(L)
Fig. 3. Flow volume curve showed reduced inspiratory flow rates and abnormally increased ratio of "forced expiratory flow 50/forced inspiratory flow 50" of 214% suggested variable extra-thoracic airway obstruction while awake; supine studies showed no significant changes with posture.
forced vital capacity of 2.06 1 (61% of predicted), a forced expiratory volume in one second of 1.71 1 (61% of predicted) a total lung capacity of 3.84 1 (75% of predicted), and a markedly reduced expiratory reserve volume (0.05 1, 4% of predicted), all consistent with a mild restrictive ventilatory defect probably due to obesity. Complete flow volume curves while awake suggested variable extra thoracic airway obstruction (Fig. 3). Laryngoscopy confirmed numer- ous sites of upper airway obstruction and edema, including the anterior nasal passages, nasopharynx, oropharynx, and hypopharynx. There was right vocal cord paralysis with edematous and asymmetric arytenoid cartilage.
Polysomnography demonstrated 499 obstructive apneic and hy- popneic episodes during 435 min of total sleep time. Apneic events
Fig. 2. MRI (1988) of head and neck showed syringobulbia-myelia and type I Chiari malformation.
234 E. IV.. Ely et al. /Journal of the Neurological Sciences 126 (1994) 232-236
. . . . . . . , T
i i
i • ]
, ' a ,
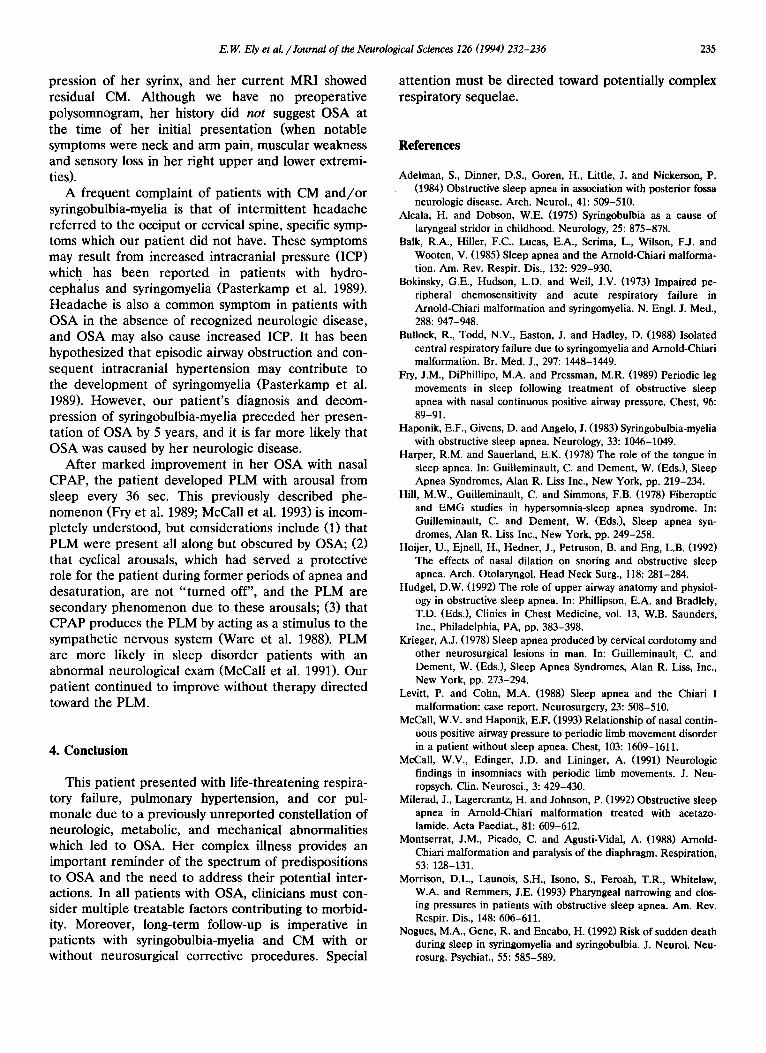
Fig. 4. Polysomnographic tracings taken during rapid eye movement sleep showed prolonged obstructive apneic episodes with significant oxygen desaturation (represented by hand-written percentile comments) into the 40th and 50th percentiles. A 60-sec epoch is shown with channels as follows: channel 1, EEG (electroencephalogram) (C3-A2); channel 2, EEG (O1-AI); channels 3 and 4, left and right EOG (electrooculogram); channel 5, chin EMG (electromyogram); channel 6, ECG (electrocardiogram); channels 7 and 8, left and right anterior tibialis EMG; channel 9, nasal airflow; channel 10, oral airflow; channel 11, thoracic respiratory effort; channel 12, abdominal respiratory effort.
lasted from 40 to 55 sec, and associated hemoglobin oxygen desatura- tion persisted in the 70% range, with a nadir of 32% despite 4 l /min supplemental 0 2 (Fig. 4). On a follow-up polysomnogram, OSA improved considerably with administration of continuous positive airway pressure (CPAP) of 8 cm H20, but any sustained periods of sleep became interrupted by frequent PLM (PLM index 102/hour, arousal index 99/h). An echocardiogram revealed an enlarged right ventricle and atrium, tricuspid regurgitation and an estimated sys- tolic pulmonary artery pressure of 45 mm Hg. The patient has had gradual but steady improvement with supplemental oxygen, nasal CPAP, diuresis, weight loss and estrogen/progesterone replacement.
3. D i s c u s s i o n
The CM consists of caudal displacement of the cerebellum and hindbrain through the foramen mag- num, and may be accompanied by degeneration of the brain stem and spinal cord (syringobulbia-myelia) (Paul et al. 1983). Many respiratory abnormalities have been associated with this condition: sudden death (Nogues et al. 1992), impaired hypoxic and hypercapnic ventila- tory drive (Rodman et al. 1962; Bokinsly et al. 1973), obstructive and central sleep apnea (Haponik et al. 1983; Balk et al. 1985; Bullock et al. 1988), vocal cord paralysis (Willis et al. 1968; Ruff et al. 1987), sleep-re- lated stridor (Alcala et al. 1975; Milerad et al. 1992), and diaphragmatic paralysis (Montserrat et al. 1988). The unique combination of problems in our patient has not been reported previously.
Absence of hypoxic ventilatory drive was an impor- tant determinant of her prolonged apneic episodes despite severe hemoglobin oxygen desaturation, and placed her in grave danger under hypoxic circum- stances (Fig. 1). In man, peripheral chemoreceptors located mainly in the carotid body, with afferent neural pathways in CN IX or medullary centers, account for all hypoxic drive (Weil et al. 1970; Bokinsky et al. 1973). The patient's CN IX (as well as CN X and XII)
dysfunction accounts for her abnormal respiratory drive. On this basis, she may also have had reduced tone of the genioglossus and other pharyngeal dilators which maintain upper airway patency (Haponik et al. 1983; Hudgel et al. 1992). Electromyography has shown that rhythmic, integrated contraction of these muscle groups during inspiration maintains airway patency (Harper et al. 1978; Hill et al. 1978; Krieger et al. 1978; Onal et al. 1982). Abnormalities of pharyngeal, laryn- geal, and genioglossus muscles are common in OSA patients without recognized neurologic disease, and the collapse of compliant tissues to occlude the upper airway is thought to be the major physiologic mecha- nism of OSA (Morrison et al. 1993). This patient's permanent CN dysfunction helps to account for the polysomnographic findings of OSA and laryngoscopic findings of severe obstruction at multiple pharyngeal levels during wakefulness. OSA may occur on such a central basis (Onal et al. 1982; Adelman et al. 1984; Levitt et al. 1988) and has also been documented in Shy-Drager syndrome, poliomyelitis, and lateral medullary syndrome (Haponik et al. 1983). Laryngo- scopically documented anterior nasal passage and pha- ryngeal narrowing (Olsen et al. 1981; Hoijer et al. 1992; Morrison et al. 1993; Williams et al. 1993), widespread mucosal edema, and right-sided vocal cord paralysis (Willis et al. 1968; Ruff et al. 1987) were important anatomic predispositions to OSA and likely interacted with obesity, post-menopausal status, and possible mild thyroid dysfunction.
Other case reports have suggested that surgical de- compression of the syrinx and CM may dramatically improve both central and obstructive apnea (Balk et al. 1985; Levitt et al. 1988). One feared complication of such procedures is an acute worsening of central respi- ratory control (Paul et al. 1983; Adelman et al. 1984). Our patient presented with OSA 5 years after decom-
E.W. Ely et al. /Journal of the Neurological Sciences 126 (1994) 232-236 235
pression of her syrinx, and her cur rent M R I showed residual CM. Al though we have no preopera t ive polysomnogram, her history did no t suggest O S A at the t ime of her initial presenta t ion (when notable symptoms were neck and a rm pain, muscular weakness and sensory loss in her right uppe r and lower extremi- ties).
A f requent complaint o f pat ients with CM a n d / o r syringobulbia-myelia is that of intermit tent headache referred to the occiput or cervical spine, specific symp- toms which our pat ient did not have. These symptoms may result f rom increased intracranial pressure (ICP) which has been repor ted in pat ients with hydro- cephalus and syringomyelia (Pas te rkamp et al. 1989). H e a d a c h e is also a c o m m o n symptom in patients with O S A in the absence of recognized neurologic disease, and O S A may also cause increased ICP. It has been hypothesized that episodic airway obstruct ion and con- sequent intracranial hyper tension may contr ibute to the development of syringomyelia (Pas te rkamp et al. 1989). However , our pat ient ' s diagnosis and decom- pression of syringobulbia-myelia p receded her presen- ta t ion of O S A by 5 years, and it is far more likely that O S A was caused by her neurologic disease.
Af te r marked improvement in her O S A with nasal CPAP, the pat ient developed P L M with arousal f rom sleep every 36 sec. This previously described phe- n o m e n o n (Fry et al. 1989; McCall et al. 1993) is incom- pletely unders tood, but considerat ions include (1) that P L M were present all along but obscured by OSA; (2) that cyclical arousals, which had served a protective role for the pat ient during former periods o f apnea and desaturat ion, are not " t u rne d off", and the P L M are secondary p h e n o m e n o n due to these arousals; (3) that C P A P produces the P L M by acting as a stimulus to the sympathet ic nervous system (Ware et al. 1988). P L M are more likely in sleep disorder pat ients with an abnormal neurological exam (McCall et al. 1991). Our pat ient cont inued to improve without therapy directed toward the PLM.
4. Conclusion
This pat ient p resented with l i fe- threatening respira- tory failure, pu lmonary hypertension, and cor pul- monale due to a previously un repor t ed constellat ion o f neurologic, metabolic, and mechanical abnormali t ies which led to OSA. Her complex illness provides an impor tant reminder of the spect rum of predisposit ions to O S A and the need to address their potent ial inter- actions. In all pat ients with OSA, clinicians must con- sider multiple t reatable factors contr ibut ing to morbid- ity. Moreover , long- term follow-up is imperative in pat ients with syringobulbia-myelia and CM with or wi thout neurosurgical corrective procedures . Special
a t tent ion must be directed toward potential ly complex respiratory sequelae.
References
Adeiman, S., Dinner, D.S., Goren, H., Little, J. and Nickerson, P. (1984) Obstructive sleep apnea in association with posterior fossa neurologic disease. Arch. Neurol., 41: 509-510.
Alcala, H. and Dobson, W.E. (1975) Syringobulbia as a cause of laryngeal stridor in childhood. Neurology, 25: 875-878.
Balk, R.A., Hiller, F.C., Lucas, E.A., Scrima, L., Wilson, F.J. and Wooten, V. (1985) Sleep apnea and the Arnold-Chiari malforma- tion. Am. Rev. Respir. Dis., 132: 929-930.
Bokinsky, G.E., Hudson, L.D. and Weil, J.V. (1973) Impaired pe- ripheral chemosensitivity and acute respiratory failure in Arnold-Chiari malformation and syringomyelia. N. Engl. J. Med., 288: 947-948.
Bullock, R., Todd, N.V., Easton, J. and Hadley, D. (1988) Isolated central respiratory failure due to syringomyelia and Arnold-Chiari malformation. Br. Med. J., 297: 1448-1449.
Fry, J.M., DiPhillipo, M.A. and Pressman, M.R. (1989) Periodic leg movements in sleep following treatment of obstructive sleep apnea with nasal continuous positive airway pressure. Chest, 96: 89-91.
Haponik, E.F., Givens, D. and Angelo, J. (1983) Syringobulbia-myelia with obstructive sleep apnea. Neurology, 33: 1046-1049.
Harper, R.M. and Sauerland, E.K. (1978) The role of the tongue in sleep apnea. In: Guilleminault, C. and Dement, W. (Eds.), Sleep Apnea Syndromes, Alan R. Liss Inc., New York, pp. 219-234.
Hill, M.W., Guilleminault, C. and Simmons, F.B. (1978) Fiberoptic and EMG studies in hypersomnia-sleep apnea syndrome. In: Guilleminault, C. and Dement, W. (Eds.), Sleep apnea syn- dromes, Alan R. Liss Inc., New York, pp. 249-258.
Hoijer, U., Ejnell, H., Hedner, J., Petruson, B. and Eng, L.B. (1992) The effects of nasal dilation on snoring and obstructive sleep apnea. Arch. Otolaryngol. Head Neck Surg., 118: 281-284.
Hudgel, D.W. (1992) The role of upper airway anatomy and physiol- ogy in obstructive sleep apnea. In: Phillipson, E.A. and Bradlely, T.D. (Eds.), Clinics in Chest Medicine, vol. 13, W.B. Saunders, Inc., Philadelphia, PA, pp. 383-398.
Krieger, A.J. (1978) Sleep apnea produced by cervical cordotomy and other neurosurgical lesions in man. In: Guilleminault, C. and Dement, W. (Eds.), Sleep Apnea Syndromes, Alan R. Liss, Inc., New York, pp. 273-294.
Levitt, P. and Cohn, M.A. (1988) Sleep apnea and the Chiari I malformation: case report. Neurosurgery, 23: 508-510.
McCall, W.V. and Haponik, E.F. (1993) Relationship of nasal contin- uous positive airway pressure to periodic limb movement disorder in a patient without sleep apnea. Chest, 103: 1609-1611.
McCall, W.V., Edinger, J.D. and Lininger, A. (1991) Neurologic findings in insomniacs with periodic limb movements. J. Neu- ropsych. Clin. Neurosci., 3: 429-430.
Milerad, J., Lagercrantz, H. and Johnson, P. (1992) Obstructive sleep apnea in Arnold-Chiari malformation treated with acetazo- lamide. Acta Paediat., 81: 609-612.
Montserrat, J.M., Picado, C. and Agusti-Vidal, A. (1988) Arnold- Chiari malformation and paralysis of the diaphragm. Respiration, 53: 128-131.
Morrison, D.L., Launois, S.H., Isono, S., Feroah, T.R., Whitelaw, W.A. and Remmers, J.E. (1993) Pharyngeal narrowing and clos- ing pressures in patients with obstructive sleep apnea. Am. Rev. Respir. Dis., 148: 606-611.
Nogues, M.A., Gene, R. and Encabo, H. (1992) Risk of sudden death during sleep in syringomyelia and syringobulbia. J. Neurol. Neu- rosurg. Psychiat., 55: 585-589.

236 E.W. Ely et al. /Journal of the Neurological Sciences 126 (1994) 232-236
Olsen, K., Kern, E. and Westbrook, P. (1981) Sleep and breathing disturbance secondary to.nasal obstruction. Otolaryngol. Head Neck Surg., 124: 158-160.
Onal, E., Lopata, M. and O'Connor, T. (1982) Pathogenesis of apneas in hypersomnia-sleep apnea syndrome. Am. Rev. Respir. Dis., 125: 167-174.
Pasterkamp, H., Sardoso, E.R. and Booth, F.A. (1989) Obstructive sleep apnea leading to increased intracranial pressure in a pa- tient with hydrocephalus and syringomyelia. Chest, 95: 1064-67.
Paul, K.S., Lye, R.H., Strang, F.A. and Dutton, J. (1983) Arnold- Chiari malformation: review of 71 cases. J. Neurosurg., 58: 183- 187.
Rodman, T., Resnick, M.E., Berkowitz, R.D. et al. (1962) Alveolar hypoventilation due to involvement of the respiratory center by obscure disease of the central nervous system. Am. J. Med., 32: 208-217.
Ruff, M.E., Oakes, W.J., Fisher, S.R. and Spock, A. (1987) Sleep apnea and vocal cord paralysis secondary to Type I Chiari malfor- mation. Pediatrics, 80: 231-234.
Ware, J.C., Blumoff, R. and Pittard, J.T. (1988) Peripheral vasocon- striction in patients with sleep related periodic leg movements. Sleep, 11: 182-187.
Weil, J.V., Byrne-Quinn, E., Sodel, I.E. et al. (1970) Hypoxic ventila- tory drive in normal man. J. Clin. Invest., 49: 1061-1072.
Williams, A.J. and Santiago, S., Jr. (1993) The nose and obstructive sleep apnea. Chest, 104: 993.
Willis, W.H. and Weaver, D.F. (1968) Syringomyelia with bilateral vocal cord paralysis. Arch. Otolaryngol., 87: 42-44.
Young, T., Palta, M., Dempsey, J., Skatrud, J., Weber, S. and Badr, S. (1993) The occurrence of sleep-disordered breathing among middle-aged adults. N. Engl. J. Med., 328: 1230-1235.









![Rx161 Arnold-Chiari Malformationfinalcopy0048502.netsolhost.com/.../pdfs/RXforms/Arnold_Chiari_Malformation.pdfArnold-Chiari malformation [Chiari malformation (CM)] is a congenital](https://img.pdfslide.net/doc/110x75/5ab9a8f17f8b9ac60e8e5491/rx161-arnold-chiari-malforma-malformation-chiari-malformation-cm-is-a-congenital.jpg)