Embed Size (px)
Citation preview
Multiple SclerosisMultiple Sclerosis
Jaimie Lynn Maines, MS-IV
SYB #3
5 March 2008
Jaimie Lynn Maines, MS-IV
SYB #3
5 March 2008
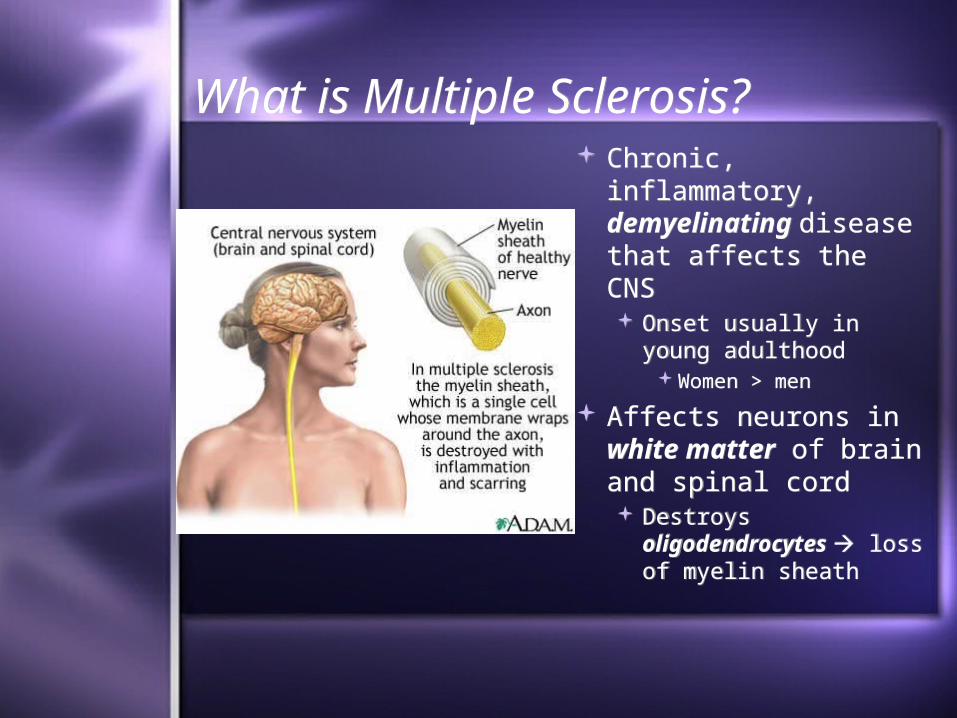
What is Multiple Sclerosis?What is Multiple Sclerosis? Chronic, inflammatory,
demyelinating disease that affects the CNS Onset usually in young
adulthood Women > men
Affects neurons in white matter of brain and spinal cord Destroys
oligodendrocytes loss of myelin sheath
Chronic, inflammatory, demyelinating disease that affects the CNS Onset usually in young
adulthood Women > men
Affects neurons in white matter of brain and spinal cord Destroys
oligodendrocytes loss of myelin sheath
Signs and SymptomsSigns and Symptoms Changes in sensation
(hypoesthesia) Muscle weakness Abnormal muscle
spasms Difficulty with
movement Ataxia Dysarthria Dysphagia
Changes in sensation (hypoesthesia)
Muscle weakness Abnormal muscle
spasms Difficulty with
movement Ataxia Dysarthria Dysphagia
Nystagmus, optic neuritis, diplopia
Fatigue and acute or chronic pain syndromes
Bladder and bowel difficulties
Cognitive impairment, depression
Lhermitte’s Sign Classic finding in MS
Nystagmus, optic neuritis, diplopia
Fatigue and acute or chronic pain syndromes
Bladder and bowel difficulties
Cognitive impairment, depression
Lhermitte’s Sign Classic finding in MS
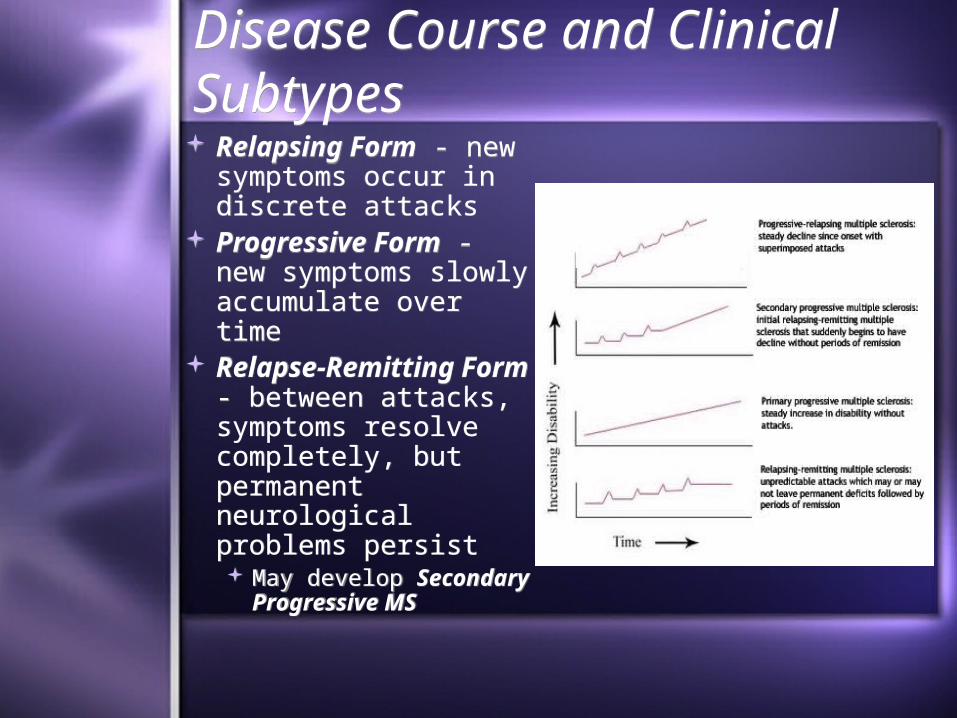
Disease Course and Clinical SubtypesDisease Course and Clinical Subtypes Relapsing Form - new
symptoms occur in discrete attacks
Progressive Form - new symptoms slowly accumulate over time
Relapse-Remitting Form - between attacks, symptoms resolve completely, but permanent neurological problems persist May develop Secondary
Progressive MS
Relapsing Form - new symptoms occur in discrete attacks
Progressive Form - new symptoms slowly accumulate over time
Relapse-Remitting Form - between attacks, symptoms resolve completely, but permanent neurological problems persist May develop Secondary
Progressive MS
DiagnosisDiagnosisDifficult to diagnose in early stages
Definitive diagnosis cannot be made until other possible causes for symptoms have been ruled out
In Relapsing-Remitting: there must be evidence of at least 2 anatomically separate demyelinating events separated by at least 30 days
In Primary Progressive: there must be slow progression of si/sx over at least 6 months
Difficult to diagnose in early stagesDefinitive diagnosis cannot be made until
other possible causes for symptoms have been ruled out
In Relapsing-Remitting: there must be evidence of at least 2 anatomically separate demyelinating events separated by at least 30 days
In Primary Progressive: there must be slow progression of si/sx over at least 6 months
McDonald CriteriaMcDonald CriteriaClinical data alone - 2 separate episodes of
neurologic symptoms characteristic of MS, consistent PE
MRI - areas of demyelination appear as bright spots (active plaques enhance with Gad)
CSF - evidence of chronic inflammationOligoclonal bands combined with MRI and PE can
make definitive diagnosisVisual or Somatosensory Evoked Potentials -
brain with MS responds less actively to stimulation
Clinical data alone - 2 separate episodes of neurologic symptoms characteristic of MS, consistent PE
MRI - areas of demyelination appear as bright spots (active plaques enhance with Gad)
CSF - evidence of chronic inflammationOligoclonal bands combined with MRI and PE can
make definitive diagnosisVisual or Somatosensory Evoked Potentials -
brain with MS responds less actively to stimulation
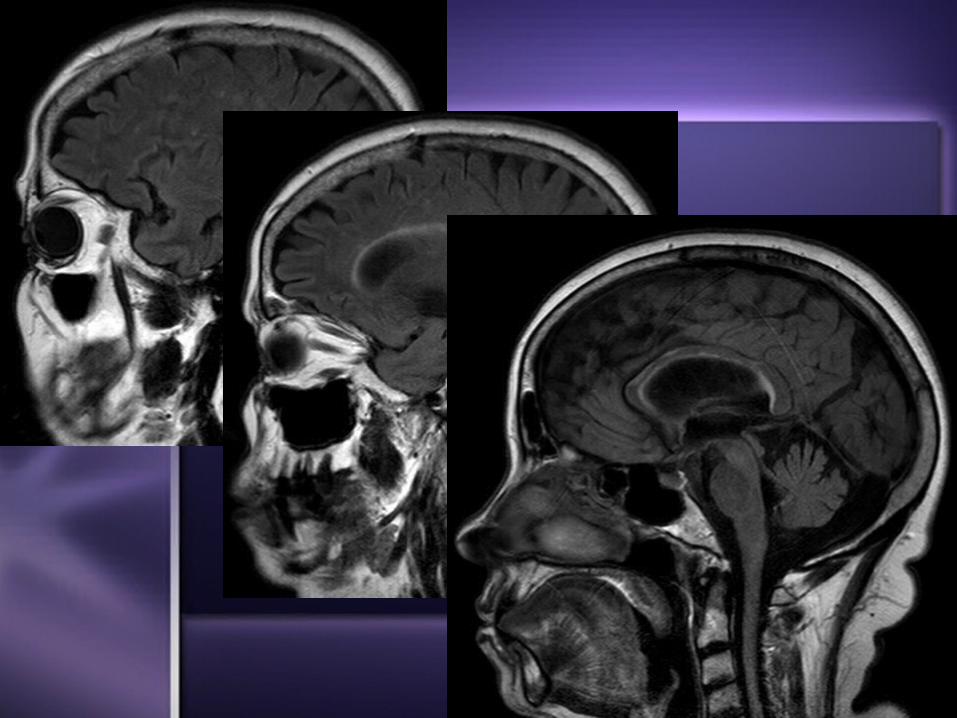
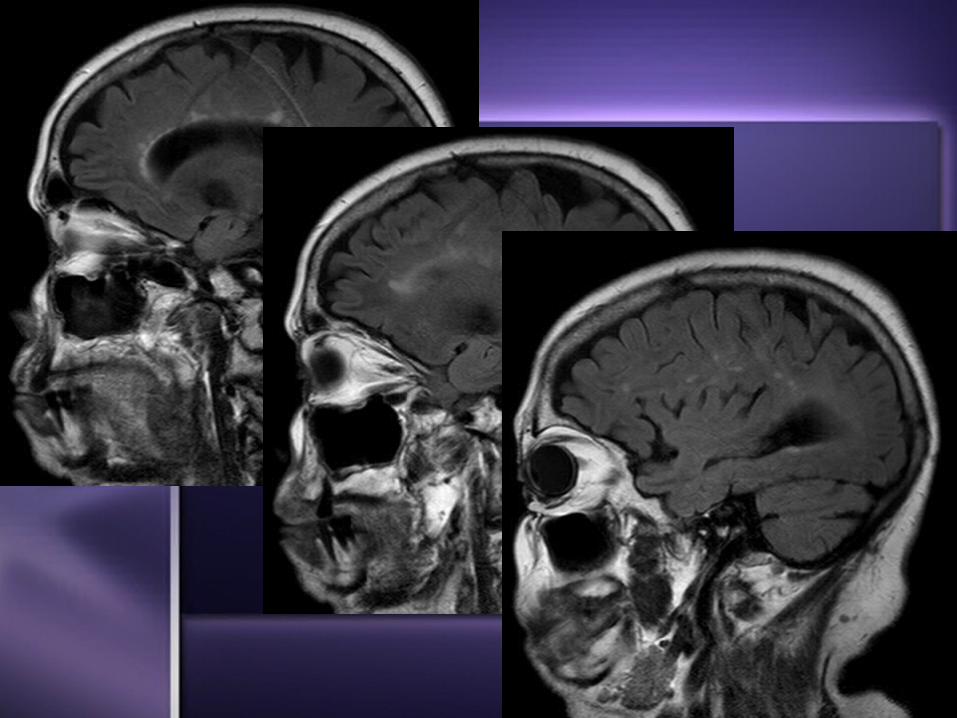
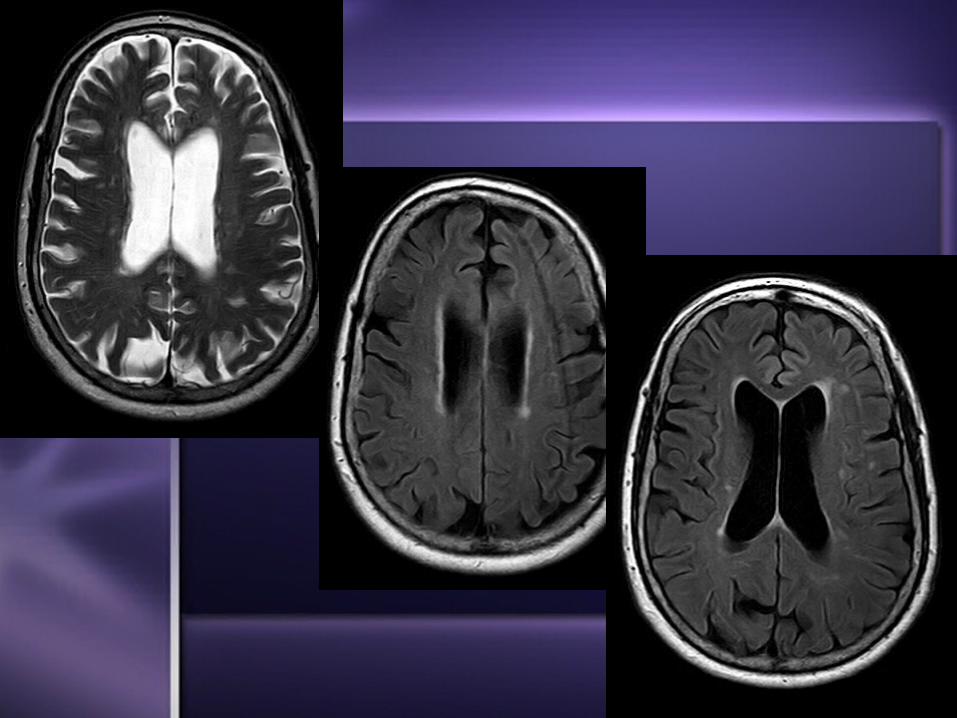
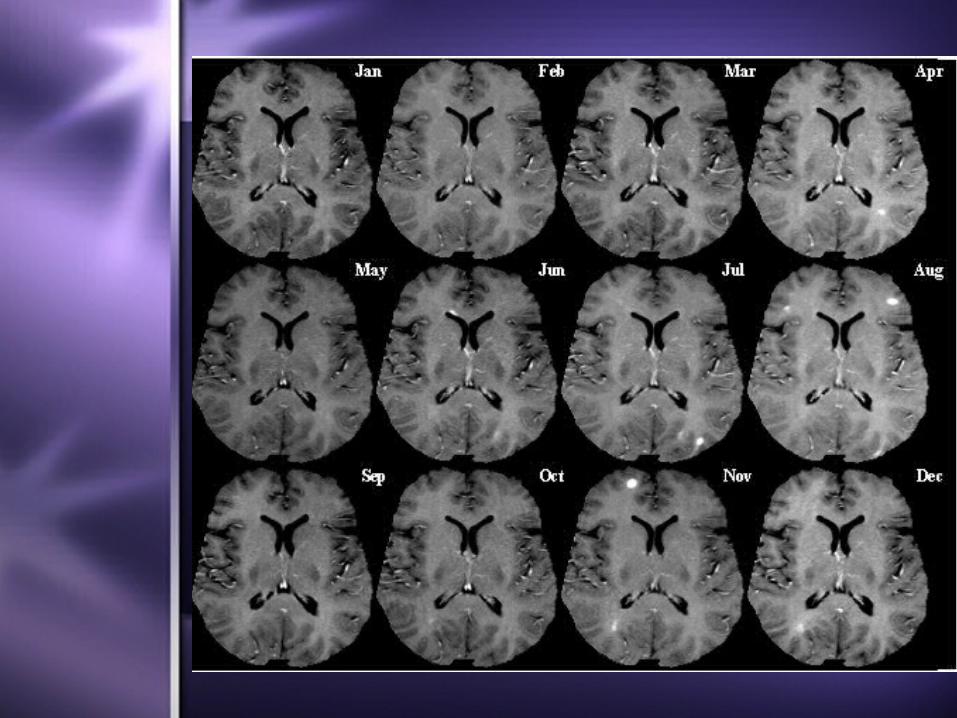
Imaging StudiesImaging StudiesMRI
Test of choice to support clinical diagnosisCharactertistic lesion - cerebral or spinal plaque;
periventricular region, corpus callosum, centrum semiovale, deep white matter structures, basal ganglia
Typically ovoid in appearance, arranged at right angles to corpus callosum
Hyperintense on T2 MRI, hypointense on T1 Diffusion imaging may identify plaques better Gad-enhancing plaques active lesions
Discrete region of demyelination
MRITest of choice to support clinical diagnosisCharactertistic lesion - cerebral or spinal plaque;
periventricular region, corpus callosum, centrum semiovale, deep white matter structures, basal ganglia
Typically ovoid in appearance, arranged at right angles to corpus callosum
Hyperintense on T2 MRI, hypointense on T1 Diffusion imaging may identify plaques better Gad-enhancing plaques active lesions
Discrete region of demyelination
Differential DiagnosisDifferential DiagnosisNeuromyelitis Optica
Autoimmune disease - attack of optic nerves and spinal cord
StrokeAcute Disseminated Encephalomyelitis
Immune mediated disease of brain following viral infection or vaccination; multiple inflammatory cell deposits found in white matter
Lyme DiseaseTumorsLupus
Neuromyelitis OpticaAutoimmune disease - attack of optic nerves and
spinal cordStrokeAcute Disseminated Encephalomyelitis
Immune mediated disease of brain following viral infection or vaccination; multiple inflammatory cell deposits found in white matter
Lyme DiseaseTumorsLupus
Medical TreatmentMedical TreatmentThere is NO cureTreatments aimed at returning function
following an attack, preventing new attacks, and preventing disability IV steroids for acute attacksInterferon - disease modifying treatmentNeurorehabilitation to ease burden of
progressive impairment
There is NO cureTreatments aimed at returning function
following an attack, preventing new attacks, and preventing disability IV steroids for acute attacksInterferon - disease modifying treatmentNeurorehabilitation to ease burden of
progressive impairment