-
7/27/2019 Musculoskeletal Chapter 31
1/124
C H A P T E R 3 1
Musculoskeletal
-
7/27/2019 Musculoskeletal Chapter 31
2/124
Pediatric Differences
Ossification nearly complete at birth Posterior fontanel closes
2-3 months of age Anterior fontanel closes approx. 18-24 months of
age Most skull growth by 2 years of age
Long bones of children porous and less dense than adults Muscles
increase in length and circumference, not in
number Until puberty, ligaments & tendons are stronger
than
bone Cartilage replaced by bone & skeletal
maturation by approximately 20 yearsof age
-
7/27/2019 Musculoskeletal Chapter 31
3/124
Who am I?
-
7/27/2019 Musculoskeletal Chapter 31
4/124
Immobilized Child
Once thought to be restorative for patients withillness and
injury
We now know that immobilization has serious
consequences Especially on growth & development of the
child
Inactivity leads to decrease in functional capacity of the
entirebody
Can delay age appropriate milestones
Decreased muscle mass & strength
Decreased metabolism
Decreased bone mineralization
-
7/27/2019 Musculoskeletal Chapter 31
5/124
Immobilization
Muscular system Decreased muscle strength and endurance
Disuse atrophy
Loss of joint mobility
Skeletal system Bone demineralization
Daily stresses on bone by motion & weight
bearing maintain balance between bone
formation (osteoblastic activity) and bone
resorption (osteoclastic activity).During immobil-
ization INCREASED calcium leaves the bone
causing osteopenia (demineralization)
Negative calcium balance
-
7/27/2019 Musculoskeletal Chapter 31
6/124
Immobilizationpsychologically
Movement is critical : immobility deprives child ofnatural
outlet for feelings
Physical growth and development depend onmovement
instrument of communication, expression andlearning
Respond to anxiety with
increased activity
-
7/27/2019 Musculoskeletal Chapter 31
7/124
Not Happy!
-
7/27/2019 Musculoskeletal Chapter 31
8/124
Traumatic Injury
Soft Tissue Injury
Muscles
LigamentsTendons
Sports injuries
Mishaps during play
-
7/27/2019 Musculoskeletal Chapter 31
9/124
Contusions
Damage to soft tissue, subcutaneous tissue andmuscle
Escape of blood into tissue-ecchymosis-black and
blue Swelling, pain disability
Crush injuries
-
7/27/2019 Musculoskeletal Chapter 31
10/124
Contusions
-
7/27/2019 Musculoskeletal Chapter 31
11/124
Dislocations
Occur when force of stress on ligament is sufficient todisplace
normal position of opposing bone ends or boneends to socket Pain
increased with active or passive movement of extremity May be an
obvious deformity & inability to move joint
Most common type : Phalanges elbow
Hip dislocation: (< 5 yrs old) potential loss of bloodsupply
to head of femur
Shoulder dislocation: (adolescents) sports related Reduce ASAP
Unreduced dislocations: increased swelling, reduction is
difficult,
increased risk neurovascular problems
-
7/27/2019 Musculoskeletal Chapter 31
12/124
Dislocations
-
7/27/2019 Musculoskeletal Chapter 31
13/124
Sprains
Trauma to a joint fromligament partially orcompletely torn
orstretched byforce
May have associated
damage tobloodvessels, muscles,tendons, and nerves
Presence of joint laxity
is indicator of severity Rapid onset of diffuse
swelling withdisability
-
7/27/2019 Musculoskeletal Chapter 31
14/124
Strains
Microscopic tear tomusculotendinousunit
Similar to sprain Swollen, painful to
touch
Generally incurredover time
-
7/27/2019 Musculoskeletal Chapter 31
15/124
Soft Tissue Injury
TherapeuticManagement RICES and ICESRest the injured partIce
immediately (max
30 min at a time)Compression with
elastic bandagesElevation of extremity
Immobilize andsupportCrutches (proper
size and height)
f
-
7/27/2019 Musculoskeletal Chapter 31
16/124
Soft Tissue Injurytreatment
-
7/27/2019 Musculoskeletal Chapter 31
17/124
Fractures
Common injury in children (rare in infants, except with
aMVA)
Clavicle the most frequently broken bone, especiallyunder 10
years. (Neonates if they are too large for moms
small pelvis) School aged: bicycle/vehicle or skate board
injuries
Adolescents: bicycles, ATVs, skateboards, motorcyclesports
Patterns of fractures, problems of diagnosis& methods
oftreatment are different in pediatrics than in adultpopulation
-
7/27/2019 Musculoskeletal Chapter 31
18/124
Epiphyseal(physeal) Injuries
Weakest point of long bones: cartilage growth plate(epiphyseal
plate)
Frequent site of damage during trauma
May affect future bone growth Treatment may include ORIF to
prevent growth
disturbances
-
7/27/2019 Musculoskeletal Chapter 31
19/124
Epiphyseal plate
-
7/27/2019 Musculoskeletal Chapter 31
20/124
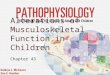
Types of Fractures
Simple or closed (no breakin the skin) Compound or open:
fractured bone protrudesthrough the skin
Complicated: bonefragments have damagedother organs or tissue
(lungor bladder)
Comminuted: smallfragments of bone are
broken from fracturedshaft and lie insurrounding tissue (rare
inchildren)
-
7/27/2019 Musculoskeletal Chapter 31
21/124
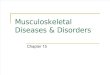
Types of fractures in children
Bend: Bone is bent but notbroken Buckle or torus:
Compression of porousbone, bulging projection atfracture site
(more
common in young children) Greenstick: compressed
side of bone bends, buttension side of bone
breaks, causing incomplete
fracture Complete: divides the bone
fragments
-
7/27/2019 Musculoskeletal Chapter 31
22/124
-
7/27/2019 Musculoskeletal Chapter 31
23/124
-
7/27/2019 Musculoskeletal Chapter 31
24/124
Clinical Manifestations of Fractures
Generalized swelling
Pain or tenderness
Deformity
Diminished functional use May have bruising, severe muscular
rigidity, crepitus
-
7/27/2019 Musculoskeletal Chapter 31
25/124
Bone healing and remodeling
Typically rapid healing inchildren (femoral shaft)
Neonatal period:2-3weeks
Early childhood:4 weeks Later childhood: 6-8
weeks
Adolescence: 8-12 weeks
-
7/27/2019 Musculoskeletal Chapter 31
26/124
Remember..
-
7/27/2019 Musculoskeletal Chapter 31
27/124
Fractures
Diagnostic evaluation: x-rayis most useful tool
Therapeutic managementgoals
Nursing considerations
Nurses make initialevaluation (calm quiet voice)
Calm the child and the parent tobetter assess
Good history of what occurredto see if abuse is possible
Spiral fx in young child mayindicate abuse
Multidisciplinary team tofurther assess
Assess Extent of Fractures
-
7/27/2019 Musculoskeletal Chapter 31
28/124
Assess Extent of FracturesThe 5 Ps
Pain and point oftenderness
Pulse distal to fracturesite
Pallor: capillary refill Paresthesia: sensation
distal to fracture site
Paralysis: movement
distal to the fracture site
-
7/27/2019 Musculoskeletal Chapter 31
29/124
Neurovascular Assessment
PULSES COLOR
MOVEMENT ANDSENSATION
TEMPERATURE
SWELLING
PAIN
-
7/27/2019 Musculoskeletal Chapter 31
30/124
The Child in a Cast
Cast application techniques Plaster of paris: drying
fiberglass
Nursing Care management First few hours after application:
Elevate extremity
assess sizing and monitor for degree of swelling Assess for hot
spots Casts of open fracture has window over wound for assessment
First few hours after surgical reduction (casted as closed
fracture)
bleeding may soak through the cast. Outline area to monitor
Educate parent on time to dry of plaster cast S/S that cast too
tight If cast too loose Home environment
Car seats Protecting the cast transparent dressing or diaper
-
7/27/2019 Musculoskeletal Chapter 31
31/124
Nursing Considerations
Swelling may continue thus cast becomes atourniquet, circulation
diminished, neurovascularcomplications
Elevate extremity If swelling is severe: casts are bivalved
Permanent tissue damage can occur within 6 to 8 hrs
COMPARTMENT SYNDROME
-
7/27/2019 Musculoskeletal Chapter 31
32/124
Compartment Syndrome
Pain
Swelling
Discoloration
Decreased pulses Decreased temperature
Inability to move distal exposed part
CALL PHYSICIAN IMMEDIETLY
-
7/27/2019 Musculoskeletal Chapter 31
33/124
Compartment Syndrome
-
7/27/2019 Musculoskeletal Chapter 31
34/124
Casting
-
7/27/2019 Musculoskeletal Chapter 31
35/124
Child in Traction
Traction: Extended pulling force
Purposes:
Fatigue muscle involved and reduce muscle spasm so bonescan be
realigned
Position distal and proximal bone ends in desired alignment
Immobilize until healing has taken place to permit casting
orsplinting
Help prevent or improve contracture deformity
Promote immobilization
Reduce muscle spasms
-
7/27/2019 Musculoskeletal Chapter 31
36/124
Traction: Essential Components
Traction: Forward force Attaching weight to distal bone
fragment
Counter traction: backward force
Body weight provides this ( for free)
Frictional force: provided by patients contact withthe bed
-
7/27/2019 Musculoskeletal Chapter 31
37/124
Types of Traction
Manual Traction: applied by the hand distal tofracture site
Skin Traction: Directly to skin surface and indirectly
to skeletal structures Skeletal traction: directly to skeletal
structure with a
pin (ouch)
-
7/27/2019 Musculoskeletal Chapter 31
38/124
Skeletal Traction Pins
-
7/27/2019 Musculoskeletal Chapter 31
39/124
Types of Traction
Upper Extremity Traction: Humerus
Overhead suspension: arm bent at elbow andsuspended vertically
& traction applied to distal
end of the humerus.Dunlop traction: Lower arm is flexed and
suspended vertically with traction, while upperarm maintains
longitudinal direction and pull
-
7/27/2019 Musculoskeletal Chapter 31
40/124
Lower Extremity Traction
Bryant: running traction, pull in 1 direction
Bucks Extension: legs in an extended position
Russell Traction: skin traction with a padded sling
90-90 traction: most common skeletal traction Steinmann pin or
Kirschner wire distal in femur at 90 angle
both at hip and knee
Balance suspension traction with
Thomas splint
-
7/27/2019 Musculoskeletal Chapter 31
41/124
Types of Traction
-
7/27/2019 Musculoskeletal Chapter 31
42/124
Cervical Traction
Halo Brace (vest) attached to head with 4 screws inouter skull:
bars connected to vest> greater mobilityof rest of the body
-
7/27/2019 Musculoskeletal Chapter 31
43/124
Cervical Traction
Crutchfield tongs (Barton, Gardner-Wells) burr holesin the skull
& weights attached to the head
-
7/27/2019 Musculoskeletal Chapter 31
44/124
Nursing Care Management
Know the reason WHY traction is applied Assess patient
Assess pulses bilaterally
Alteration in sensation or increased pain
Assess any change in color of skin or nail bed
Skin breakdown/ massage pressure areas to stimulate
circulation
Position changes
Wash and dry skin daily
Any neurovascular changes: record and call MD
Assess traction apparatus
Check line of pull/ weights
Bandages in place/ excessive tightness
Do not remove unless under supervision of physician
Diet
Balanced diet with fruits and vegetables (fiber)
calcium
Encouraging fluids
Offering laxatives
Encourage deep breathing and Incentive Spirometry
Prevent foot drop
Encourage socialization/ discourage isolation
-
7/27/2019 Musculoskeletal Chapter 31
45/124
Nursing Care Management
Pain management: increased initially as traction pullis
fatiguing the muscle
Analgesics
Muscle relaxants
Pin care: according to hospital policy or physicianorder
Frequently assessed and cleaned to prevent infection
After first 48 to 72 hours assessment needed less frequently
-
7/27/2019 Musculoskeletal Chapter 31
46/124
Developmental Dysplasia of Hip
-
7/27/2019 Musculoskeletal Chapter 31
47/124
Developmental Dysplasia of HipDDH
Spectrum of disorders describing abnormaldevelopment of hip that
can occur
Infancy
childhood
Fetal life
Cause unknown
Gender, birth order, family history,
positioning, delivery type, joint laxity
& post natal positioning
Developmental Dysplasia of Hip
-
7/27/2019 Musculoskeletal Chapter 31
48/124
Developmental Dysplasia of HipDDH
Diagnostic Evaluation Not detected at initial exam after
birth Most often found in pediatrician
office for well baby check up Exhibits as hip joint laxity
and
NOT out right dislocation
Shortening of the limb on affectedside
Asymmetric thigh and gluteal fold Broadening of the perineum
Ortolani and Barlow tests most
reliable from birth to 3 months Barlow: thighs are adducted
Ortolani: abducting the thighs totest for hip subluxation
ordislocation
-
7/27/2019 Musculoskeletal Chapter 31
49/124
DDH
Ortolani Test
-
7/27/2019 Musculoskeletal Chapter 31
50/124
limited hip abduction in flexion
Barlow Test
-
7/27/2019 Musculoskeletal Chapter 31
51/124
thighs adducted
Signs of DDH
-
7/27/2019 Musculoskeletal Chapter 31
52/124
gasymmetry of gluteal and thigh folds
-
7/27/2019 Musculoskeletal Chapter 31
53/124
Therapeutic Management
Treatment initiated as soon as recognized
GOAL: obtain and maintain a safe and congruentposition of hip
joint to promote normal development
Early intervention more favorable in restoration of normalbony
architecture and function.
-
7/27/2019 Musculoskeletal Chapter 31
54/124
Therapeutic Management
Newborn to 6 months Pavlik Harnace
Hip joint in dynamic splint
Proximal femur centered in acetabulum
Worn continuously until proven
stable on exam and with x-ray
-
7/27/2019 Musculoskeletal Chapter 31
55/124
-
7/27/2019 Musculoskeletal Chapter 31
56/124
Therapeutic Management
Ages 6 to 18 monthsGradual reduction by traction for 3 weeks
Closed reduction of hip under general
anesthesia
If not successful then open reduction
Then placed in hip spica cast for 2 to 4
monthsOnce hip is stable a flexion abduction brace
is applied
-
7/27/2019 Musculoskeletal Chapter 31
57/124
Hip Spica cast
-
7/27/2019 Musculoskeletal Chapter 31
58/124
Therapeutic Management
Older Child Increasingly difficult after age 4
Impossible or inadvisable > 6 yrs
Contractures of muscles Deformity of femoral and acetabular
structures
Correction is challenging as most likely is secondary
toarthritis or CP
Operative reduction with or without presurgical traction
Contracted muscles
Osteotomy procedures
-
7/27/2019 Musculoskeletal Chapter 31
59/124
Nursing Management
Nurses can detect DDH on initial assessment
Ambulatory child who displays limp or unusual gateis
referred
Primary Nursing Goal: Teaching ParentWHY DEVICE BEING USED!!
Application of device
Maintenance of device
Keep in mind rapid growth of the infant/child(check
straps)/check for rubbing/ red marks
-
7/27/2019 Musculoskeletal Chapter 31
60/124
Nursing Management
Normalcy is the goal Involve the child in all activities of any
other child in
same age group
Maintain active role in family and activities
-
7/27/2019 Musculoskeletal Chapter 31
61/124
Congenital Clubfoot
Deformity of ankle and foot which includesforefoot adduction
Midfoot supination
Hindfoot varusAnkle equinus
Most common talipes equinovarus
Foot is pointed downward and inward invarying degrees
-
7/27/2019 Musculoskeletal Chapter 31
62/124
-
7/27/2019 Musculoskeletal Chapter 31
63/124
Congenital Clubfoot
Cause unknown Some attribute to abnormal positioning and
restricted movement in utero
Arrested or abnormal embryonic development Increased risk of hip
dysplasia
l l bf
-
7/27/2019 Musculoskeletal Chapter 31
64/124
Congenital Clubfoot
Classification Positional: intrauterine crowding
Responds to simple stretching and casting
Syndromic (teratologic): associated with other congenital
anomalies More severe form/ often resistant to tx
Surgical intervention may or may not be effective
Congenital/idiopathic: can occur in otherwise normal child
Always requires surgical intervention because there is a
bonyabnormality
i i l i
-
7/27/2019 Musculoskeletal Chapter 31
65/124
Diagnostic Evaluation
Detectable prenatally through U/S Noted at birth
h i
-
7/27/2019 Musculoskeletal Chapter 31
66/124
Therapeutic Management
Goal: achieve a painless, plantigrade and stable foot Serial
casting before discharge
Successive casts encourage gradual stretching and accommodate
rapidgrowth
Maximum correction achieved within 8 to 12 weeks
If no positive result after 3 months= surgical intervention
Three stages
Correction of deformity
Maintenance of correction until normal muscle balance is
regained
Follow up observation to prevent possible recurrence
P i
-
7/27/2019 Musculoskeletal Chapter 31
67/124
Ponseti
N i C M
-
7/27/2019 Musculoskeletal Chapter 31
68/124
Nursing Care Management
Casted child:observation of skin and circulation
Rapid growth
Educate the parentSigns of skin breakdown
Signs new cast needed
Help the child to live as normally as possible
M Add (V )
-
7/27/2019 Musculoskeletal Chapter 31
69/124
Metatarsus Adductus (Varus)
Most common congenital foot deformity Result of abnormal
intrauterine positioning
Type I: foot flexible and corrects easily
Type II: partial flexibility in forefoot Type III: foot rigid
and will not stretch
T t t
-
7/27/2019 Musculoskeletal Chapter 31
70/124
Treatment
Type I & IIOften times corrected with gentlemanipulation
Passive stretching of foot
Parent teaching performed
Continue for 6 weeks
Type III
Serial manipulation and casting
N i M t
-
7/27/2019 Musculoskeletal Chapter 31
71/124
Nursing Management
Teaching the parent
hold heal firmly and to stretch ONLY theforefoot
Cast teaching
Signs of skin breakdown
Signs new cast needed
Help the child to live as normally aspossible
Sk l t l Li b D fi i
-
7/27/2019 Musculoskeletal Chapter 31
72/124
Skeletal Limb Deficiency
Underdevelopment of skeletal elements ofextremities
Can range from minor defects (missing digit) toserious
abnormalities
Amelia: loss of entire extremity
Meromelia: partial absence of an extremity
Phocomelia: seal limbs
Most are primary defects of development of limb Prenatal
destruction can occur due to constriction of
amniotic band
-
7/27/2019 Musculoskeletal Chapter 31
73/124
Meromeliati l b f t it
-
7/27/2019 Musculoskeletal Chapter 31
74/124
partial absence of extremity
Sk l t l Li b D fi i
-
7/27/2019 Musculoskeletal Chapter 31
75/124
Skeletal Limb Deficiency
Therapeutic Management Prosthetic devices
Applied at earliest possible stage
Nursing Care Management
Teaching parent about prosthetic application
Occupational therapist
Encourage parent to assist the child in making age
appropriateadvancements
Do not OVERPROTECT child
L C l P th Di
-
7/27/2019 Musculoskeletal Chapter 31
76/124
Legg- Calve-Perthes Disease
Self limiting disorder withfemoral head aseptic
necrosis
Affects ages 2 to 12
Most commonly in boysages 4 to 8
Cause unknown
Can take place over 18
monthsor as long as several years
-
7/27/2019 Musculoskeletal Chapter 31
77/124
Camerons Personal Story
Legg Calve Perthes Disease
-
7/27/2019 Musculoskeletal Chapter 31
78/124
Legg- Calve-Perthes Disease
Insidious onset History may reveal intermittent limp or
persistent
ache or stiffness
Diagnosed with x-ray and confirmed with MRI Revealing
osteonecrosis
Legg Calve Perthes Disease
-
7/27/2019 Musculoskeletal Chapter 31
79/124
Legg- Calve-Perthes Disease
Therapeutic Management Goal: Keep head of femur in acetabulum
Treatment varies based on: Age
Appearance of femoral head vasculature and position within
acetabulum Rest and non weight bearing
At times traction applied to stretch tight adductor muscles
Non weight bearing devices:
Abduction brace Leg casts
Leather harness sling
Surgery in some cases
-
7/27/2019 Musculoskeletal Chapter 31
80/124
Legg Calve Perthes Disease
-
7/27/2019 Musculoskeletal Chapter 31
81/124
Legg- Calve-Perthes Disease
Self limiting Younger children have better prognosis for
complete
recovery Epiphysis are more cartilaginous
Children 10 and older have high risk for
degenerativearthritis
The later the diagnosis, the more damage to femoral
head
Legg Calve Perthes Disease
-
7/27/2019 Musculoskeletal Chapter 31
82/124
Legg- Calve-Perthes Disease
Nursing Care Management Identify the affected child and
refer
Educate the parent
Why device being orderedManagement and application of
corrective
device
Signs of skin breakdownSigns that a new size needed
Help the child to live as normally as possible
-
7/27/2019 Musculoskeletal Chapter 31
83/124
Skeletal deformity
-
7/27/2019 Musculoskeletal Chapter 31
84/124
Skeletal deformity
Kyphosis: increased convex angulation in curvatureof the
thoracic spine
Secondary to
TB
Arthritis Osteodystrophy
Compression fractures of thoracic spine
Lordosis: accentuation of cervical or lumbar
curvature Trauma
idiopathic
Idiopathic Scoliosis
-
7/27/2019 Musculoskeletal Chapter 31
85/124
Idiopathic Scoliosis
Complex spinal deformity in three plains Lateral curve
Spinal rotation causing rib asymmetry
Thoracic kyphosis
Most common spinal deformity Classified according to age of
onset Infantile: birth to 3 yrs
Juvenile: develops during childhood
Adolescent: develops during the growthspurt of early
adolescents.
Most noticeable during the pre adolescent growth spurt
Idiopathic Scoliosisdiagnostic evaluation
-
7/27/2019 Musculoskeletal Chapter 31
86/124
diagnostic evaluation
Observation: behind standing child Symmetry of shoulder
height
Scapular or flank shape
Hip height and alignment
As child bends forward at the waist (Adams test)with hanging
arms
Assymetry of ribs and flanks may be noted
Scoliometer used to measure truncal rotation
Definitive diagnosis made by radiograph
of child in standing position
Idiopathic ScoliosisTherapeutic Management
-
7/27/2019 Musculoskeletal Chapter 31
87/124
Therapeutic Management
Observation with clinical and radiographic evaluation Curve <
10 degrees is postural variation
Curve < 20 degrees is mild
Orthotic intervention (bracing) Boston, Wilmington, TLSO
(thoracolumbosacral
orthosis),Milwaukee, Charleston Nighttime Bending Brace
Surgical spinal fusion: realignment and straighteningwith
internal fixation and instrumentation combinedwith bony fusion of
the realigned spine.
Curve >40 degrees Paralytic and Congenital curves
generally
-progress
Idiopathic ScoliosisNursing Care Management
-
7/27/2019 Musculoskeletal Chapter 31
88/124
Nursing Care Management
Treatments extends over years Childs identity (physical and
psychological) is
formed in adolescents
Nursing care must take into consideration the
adolescents perspective Positive reinforcement
Encouragement
Independence
Selection of clothing Participation of activities
Socialization with peers
Idiopathic ScoliosisNursing Care Management
-
7/27/2019 Musculoskeletal Chapter 31
89/124
Nursing Care Management
Preoperative Care Educate on complexity of surgery
Teach patient to manage own PCA
How to Log Roll
Prepare for foley catheter Possibility of a chest tube
Possibility of NG tube
Have a favorite toy, stuffed animal, iPad
Meeting with a peer who has undergone similar surgery as
well
-
7/27/2019 Musculoskeletal Chapter 31
90/124
Idiopathic ScoliosisNursing Care Management
-
7/27/2019 Musculoskeletal Chapter 31
91/124
Nursing Care Management
Postoperative care Monitored in an acute care setting
Neurological assessments of extremities critical
Delayed paralysis may develop
Most common post op issues Neurological injury
Spinal cord injury
Hypotension from blood loss
Wound infection
Log rolled
Skin care Risk for pressure ulcers
Pain management
Scoliosis
-
7/27/2019 Musculoskeletal Chapter 31
92/124
Scoliosis
Ambulation begins 2 or 3 P.O.D. Discharged after 1 week Adequate
urine output Fluid and electrolyte balance ileus
Skin integrity Start PT as soon as patient able Self care always
encouraged Teaching of family Body image
Refer family to resources American Association Orthopedic
Surgeons Scoliosis Research Society
Osteomyelitis
-
7/27/2019 Musculoskeletal Chapter 31
93/124
Osteomyelitis
Inflammation and infection of bony tissue May be caused by
exogenous reasons ( trauma/
puncture wound/ or surgery)
Or hematogenous sources (pre existing infection/tonsillitis/
impetigo where the organism travels)
Osteomyelitis
-
7/27/2019 Musculoskeletal Chapter 31
94/124
Osteomyelitis
Exogenous: infectious agent invades the bone following
penetrating
wound, open fracture, contamination in surgery or
secondaryextension from abscess or burn.
Hematogenous: Existing infection spreads to bone
Sources may be furuncles, skin infection, URI, abscessed
teeth,pyelonephritis
Any organism can cause osteomyelitis
Infective emboli travel to arteries in bone metaphysis,
causingabscess formation and bone destruction
Anna
-
7/27/2019 Musculoskeletal Chapter 31
95/124
Anna
Osteomyelitis
-
7/27/2019 Musculoskeletal Chapter 31
96/124
Osteomyelitis
Staphylococcus aureus is most common causativeorganism
Signs and symptoms begin abruptly, resemblesymptoms of arthritis
and leukemia
Marked leukocytosis and elevated Sed rate
Early x-ray may appear normal
CT, Bone scan , MRI
Bone culture obtained from biopsy
or aspirate
Osteomyelitistherapeutic management
-
7/27/2019 Musculoskeletal Chapter 31
97/124
therapeutic management
May have sub-acute presentation with walled offabscess rather
than spreading infection
Prompt, vigorous IV ABT for extended period (3-4weeks or up to
several months)
Monitor hematologic, renal, hepatic
responses to treatment
OsteomyelitisNursing Considerations
-
7/27/2019 Musculoskeletal Chapter 31
98/124
Nursing Considerations
Complete bed rest and immobility of limb Casting at time
necessary
Pain management: position and medicate Surgery may be necessary
Long term IV access (for ABT administration) Nutritional
considerations Child may have vomiting and poor appetite As
infection controlled appetite returns
Long term hospitalization/ Physical Therapy to
ensure restoration of optimum functioning Psychosocial needs
Diversional and constructive activities
Juvenile Idiopathic Arthritis(juvenile rheumatoid arthritis)
-
7/27/2019 Musculoskeletal Chapter 31
99/124
(juvenile rheumatoid arthritis)
Chronic Autoimmune inflammatory disease causinginflammation of
joints and other tissue
Starts before age 16 with peak onset between ages 1 and 3
years
Twice as many girls are affected
13.9 per 100,000 children per year in caucasian children 113 per
100,000 children overall
Unknown cause
Immunogenic susceptibility
Environmental or external trigger such as a virus
Pathophysiology of JIA
-
7/27/2019 Musculoskeletal Chapter 31
100/124
Pathophysiology of JIA
Chronic inflammation of synovium with joint effusioneventual
erosion
destruction
fibrosis of the articular cartilageIf inflammatory process
continues
adhesions between joint surfaces
ankylosis of joints
-
7/27/2019 Musculoskeletal Chapter 31
101/124
JIA
-
7/27/2019 Musculoskeletal Chapter 31
102/124
Clinical Manifestations
-
7/27/2019 Musculoskeletal Chapter 31
103/124
Variable and unpredictable Not life threatening but can
cause significant disability 70% of cases eventually
becomes inactive However child may have severe
or minimal joint damage bytime disease process abates
30% have progressive diseaseinto adulthood Significant joint
deformity and
functional disability Medical evaluations PT
Possible joint replacements Chronic or acute uveitis may
occur
Diagnosis
-
7/27/2019 Musculoskeletal Chapter 31
104/124
g
Diagnosis of exclusion Clinical criteria at age of onset before
16 years
Swelling and pain
Lab tests may or may not provide evidence
Sedimentation rate may or may not be elevated
Leukocytosis usually present with acute exacerbationAntinuclear
antibodies common but not specific
Radiology studies
Show soft tissue swelling and joint space widening with
increasedsynovial fluid
Uveitis Inflammation of anterior chamber of the eye
Can be sight threatening
Therapeutic Management
-
7/27/2019 Musculoskeletal Chapter 31
105/124
p g
Control pain NSAIDS
Preserve Joint ROM and function
PT: active range of motion
Minimize effects of inflammation/ Joint deformity
NSAIDs/PT/OT
Promote normal growth and development
Pool therapy Nighttime splinting reduce flexion deformity
Medications
-
7/27/2019 Musculoskeletal Chapter 31
106/124
NSAIDS
Naproxen, ibuprofen and tolmetin
Take with food
Hydrate
bruising
Methotrexate
Second line tx for children who have failed NSAIDs alone
Used in combination with NSAID
CBC and LFTs
Corticosteroids
Potent immunosuppressives
Incapacitating arthritis/ uveitis/life threatening
complications
Etanercept (TNFI) (Enbrel)
Tumor necrosis factor receptor blocker SAARDS
Slow acting anti rheumatic drugs
Work in combination with NSAIDS
Sulfasalazine
Hydroxychloraquine, gold, D-penicillamine.
Nursing Care Management
-
7/27/2019 Musculoskeletal Chapter 31
107/124
g g
Assessment of all aspects of the child General health
Status of involved joints
Emotional response
Support of the parents Parental concerns of prognosis
Financial concerns
Spouse and sibling relationships
Job and schedule conflicts
Referral to social worker, counselors and support groups
Nursing Care Management
-
7/27/2019 Musculoskeletal Chapter 31
108/124
g g
Relieve Pain Provide as much relief as possible Medications
Opioids avoided Non pharmacologic
Behavior therapy
Relaxation techniques Promote general health Well balanced diet
with sufficient caloric intake Sufficient rest Communication
between family/PCP/rheumatology team is critical
Normalcy Encourage independence!!! Attending school
important
Communicate with school and school nurse
Nursing Care Management
-
7/27/2019 Musculoskeletal Chapter 31
109/124
g g
Educate the patient and family on Medications Therapeutic levels
r/t schedules Signs and symptoms of toxicity
splints and appliances Proper placement and reason for
device
available resources
Benefits of heat application Moist heat Bathtub Electric
blankets
Exercise Pools : range of motion
Prevent isolation and foster independence Encourage child to
perform ADLs independently Encourage family to pursue normal
activities
Osteosarcoma
-
7/27/2019 Musculoskeletal Chapter 31
110/124
Most common bonecancer in children
Peak incidence between10 and 25 years of age
Primary tumor sites inmetaphysis of long bones(most likely in
lowerextremities)
>50% femur
Humerus, tibia pelvis, jawand phalanges
Therapeutic Management
-
7/27/2019 Musculoskeletal Chapter 31
111/124
Surgery and chemotherapy Biopsy followed by limb salvage or
amputation
Nursing Care Management
-
7/27/2019 Musculoskeletal Chapter 31
112/124
Education for family and child Salvage vs amputation
Prosthesis fitting promotes early functioning
Chemotherapy and side effects
Anger and depression are normal and expected
Honesty and straightforward answers Be in the room when
physician explains
Everyone grieves and learns differently
Phantom limb pain Sensations such as tingling itching and pain
in amputated limb
Elavil
Nursing Care Management
-
7/27/2019 Musculoskeletal Chapter 31
113/124
Promote normalcy and resumption of preamputation activities
Pick clothing that does not draw attention to amputation
Body image critical to adolescents
Ewing Sarcoma
-
7/27/2019 Musculoskeletal Chapter 31
114/124
Primitive neuroectodermal tumor Second most common malignant
bone tumor in
childhood
Under age 30 majority being between ages 4 and 25
Originates in the shaft of long and trunk bones
Femur tibia fibula humerus ulna vertebrae scapula ribs
pelvicbone and skull
-
7/27/2019 Musculoskeletal Chapter 31
115/124
Therapeutic Management
-
7/27/2019 Musculoskeletal Chapter 31
116/124
Intensive irradiation of the bone combined withchemotherapy
Amputation last resort
Nursing Care Management
-
7/27/2019 Musculoskeletal Chapter 31
117/124
Less traumatic for family related to likelihood that
noamputation will be necessary Need education r/t Diagnostic
testing (BMT, biopsy) Radiation and chemotherapy
Intense radiotherapy causes skin reaction Dry or moist
desquamation then hyperpigmentation
Increased sensitivity of area Child should wear loose fitted
clothing over the area to minimize
additional skin irritation
Chemotherapy
Hair loss, n/v, peripheral neuropathy and possible
cardiotoxicity
Encourage resumption of normal lifestyle and activities
-
7/27/2019 Musculoskeletal Chapter 31
118/124
Systemic Lupus Erythematosus(SLE)
-
7/27/2019 Musculoskeletal Chapter 31
119/124
Autoimmune disease of connective tissues and bloodvessels
Chronic
Multisystem Result of genetics as well as a trigger
Exposure to ultraviolet light
Estrogen/pregnancy
Infections
drugs
Multisystem
-
7/27/2019 Musculoskeletal Chapter 31
120/124
SLE
-
7/27/2019 Musculoskeletal Chapter 31
121/124
Clinical Manifestations
Malar rash
Discoid rash
Photosensitivity
Oro nasal ulcers
Arthritis
Serositis
Renal disorder
Neurological disorders
Hematologic disorders
Therapeutic Management
-
7/27/2019 Musculoskeletal Chapter 31
122/124
Balance medications needed to avoid exacerbation
andcomplications
While preventing or minimizing treatment associatedmorbidity
Corticosteroids
Antimalarial: rash and arthritis
NSAIDS
Immunosuppressive: cyclophosphamide
Nutrition
Sleep Exercise
Limited exposure to sun & UV light
Nursing Care Management
-
7/27/2019 Musculoskeletal Chapter 31
123/124
Goal: assist family to positively adjust to disease &
therapy Recognize exacerbation Recognize complications of
medications Discuss with health care provider
Body Image Problems Rash/hair loss/ steroid therapy
Support Groups Lupus Foundation of America Arthritis
Foundation
Teaching Regular medical supervision Seek attention QUICKLY
during illness or prior to elective surgical procedures
Avoid sun and AVB exposure Wear sunscreen and sun resistant
clothing Limiting outdoor activities
-
7/27/2019 Musculoskeletal Chapter 31
124/124