Embed Size (px)
Citation preview
1 Triage Specification – September 2018 – MSk Pathways
Musculoskeletal Services Supporting Self-management Pharmacological Management Triage Specification Pathway Referral Criteria September 2018 Clinical Lead [email protected]
2 Triage Specification – September 2018 - Contents
Contents
Contents .................................................................................................................................................. 2
References .............................................................................................................................................. 2
1. Context ............................................................................................................................................ 3
1.1. Challenges ................................................................................................................................ 3
1.2. Reviewing of MSk Clinical Pathways ....................................................................................... 3
1.3. General Notes .......................................................................................................................... 3
2. Supporting Self-Management and Prevention ............................................................................... 5
3. Pharmacological Management ....................................................................................................... 6
3.1. Pharmacological Management of Low Back Pain (without sciatica) ....................................... 6
3.2. Pharmacological Management of Sciatica .............................................................................. 7
4. Triage .............................................................................................................................................. 9
4.1. Specification for Triage ............................................................................................................ 9
4.2. Competencies of Triage Staff .................................................................................................. 9
4.3. Training and Education ............................................................................................................ 9
5. Musculoskeletal Pathways ............................................................................................................ 10
5.1. Generic Musculoskeletal Pathway Template ........................................................................ 10
5.2. Carpal Tunnel Syndrome ....................................................................................................... 12
5.3. Connective Tissue Disease and Vasculitis .............................................................................. 17
5.4. Hip osteoarthritis ................................................................................................................... 22
5.5. Inflammation of multiple joints ............................................................................................. 27
5.6. Inflammation of one joint...................................................................................................... 33
5.7. Inflammation of the spine ..................................................................................................... 40
5.8. Knee Pain ............................................................................................................................... 46
5.9. Low Back Pain and Sciatica .................................................................................................... 52
5.10. Metabolic Bone Disease - Osteoporosis ................................................................................ 62
5.11. Polymyalgia Rheumatica and Giant Cell Arteritis .................................................................. 67
5.12. Shoulder Pain ......................................................................................................................... 72
5.13. Chronic widespread pain (Fibromyalgia, Chronic primary pain) ........................................... 78
6. Appendix 1 – Interventions supporting key design principles ...................................................... 85
7. Appendix 2 – Process Maps .......................................................................................................... 86
References NICE Guidelines and Quality Standards ............................................ https://www.nice.org.uk/guidance NICE Clinical Knowledge Summaries .....................................................................https://cks.nice.org.uk BOA Commissioning Guidance .................. https://www.boa.ac.uk/pro-practice/commissioning-guides BSR Guidelines ....... https://www.rheumatology.org.uk/Knowledge/Excellence/Guidelines#guidelines Cochrane Musculoskeletal Decision Aids............... https://musculoskeletal.cochrane.org/decision-aids Ottawa Hospital Research Institute Decision Aids ...................... https://decisionaid.ohri.ca/AZlist.html NHS Right Care .................................. https://www.england.nhs.uk/rightcare/shared-decision-making/ Patient. (Information and decision aids accredited by the Information Standard) ... https://patient.info Expert clinical advice, NW London Musculoskeletal Clinical Network and Policy Development Group. ........... https://www.hounslowccg.nhs.uk/news,-publications-and-policies/publications.aspx?n=2136
3 Triage Specification – September 2018 - Context
1. Context
People live with painful musculoskeletal disorders for more years of their lives than any other condition; it is the third highest cause of NHS expenditure after mental health and ‘other’ illnesses and the second highest cause of loss of productivity in the workforce after minor illness (Ealing MSk JSNA 2017). 1.1. Challenges
Unwarranted variations in referral thresholds for surgery, consultant opinion and imaging, along with increased costs as well as no benefit to patient outcomes (NHS London DSU 2011, subsequent modelling: Ealing MSk JSNA 2017) remains a constant challenge.
• This is not helped by GPs bypassing planned pathways to circumvent waiting lists or achieve a consultant opinion even when this may not be necessary (MSk Clinical Network 2018).
• Increasing waiting times for consultant opinion and surgery is also a challenge.
1.2. Reviewing of MSk Clinical Pathways
To address the above challenges, the following MSK pathways have been reviewed against the North West London Outpatient Transformation Programme design principles:
Specialty Pathways
Upper Limb
Carpal Tunnel Shoulder Pain
Lower Limb Knee Pain Osteoarthritis Hip
Spinal Low Back Pain and Sciatica Inflammation of the Spine
Rheumatology Inflammation of one joint (e.g. gout) Inflammation of multiple joints (e.g. rheumatoid) Connective Tissue Disease and Vasculitis Polymyalgia Rheumatica and Giant Cell Arteritis Metabolic Bone Disease (e.g. osteoporosis)
Chronic Primary Pain Chronic widespread pain
As well as the following three cross cutting themes:
Cross cutting themes Supporting self-management Pharmacological treatments for pain Triage: standards and monitoring
This document is intended to be used by Referrers to ensure the specifications for good triage are clear, referral criteria are adhered to, as well as capturing the key points in relation to supporting self-management, pharmacological treatments for pain, and the standards for triage and how these will be monitored. 1.3. General Notes
Investigations in community (interface) clinics may be available where these have been commissioned. In general, community services have not been commissioned to urgently investigate
4 Triage Specification – September 2018 - Context
serious underlying pathology but are geared towards identifying and working up patients who are on surgical pathways. If such services are not available in community settings, then referrals to secondary care for investigation, discussion about the results and management planning may be required, depending on the urgency, resources and clinical expertise available in primary care. Thresholds for referrals are presented from the perspective of the recipient service because referrals can come from a variety of sources. Referrers should ask the following three questions and provide the information in the referral: What treatments has the patient had for this condition before?
How much improvement did the patient have with any previous treatments?
How long did the improvements last?
Consider if any treatments have had a significant meaningful clinical benefit on pain or function, lasting well beyond the end of the treatment. As a guide, for non-invasive treatments, this means at least a 30% improvement in pain or function, lasting at least 3-6 months beyond the end of treatment. A greater and more sustained improvement would be needed for invasive treatments in view of their higher clinical risks and costs. Referrers should also check the last discharge letter as this may give: Suggestions for further management
The conditions for re-referral
The most appropriate pathway or recipient (including primary care)
This information will be useful in deciding with patients whether similar treatment is likely to be helpful, whether other options should be considered, or whether the patient should be supported to self-manage in primary care.
5 Triage Specification – September 2018 – Supporting Self-Management and Prevention
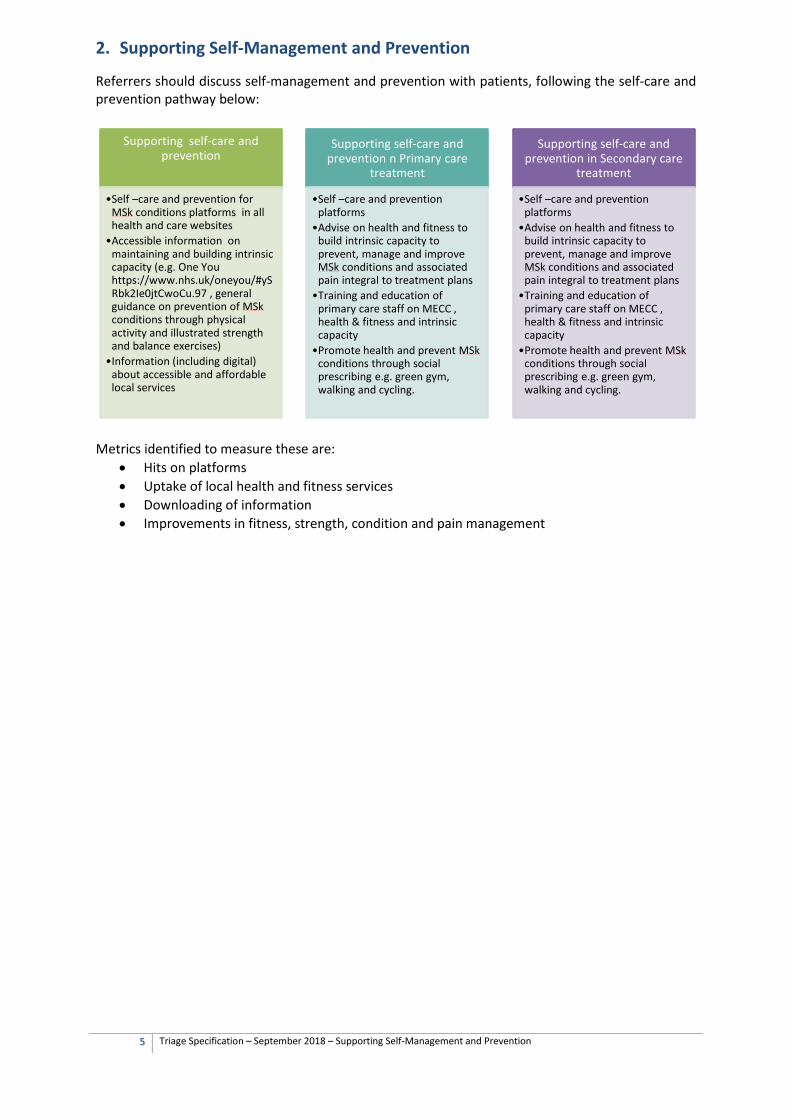
2. Supporting Self-Management and Prevention
Referrers should discuss self-management and prevention with patients, following the self-care and prevention pathway below:
Metrics identified to measure these are:
• Hits on platforms • Uptake of local health and fitness services • Downloading of information • Improvements in fitness, strength, condition and pain management
Supporting self-care and prevention
•Self –care and prevention for MSk conditions platforms in all health and care websites
•Accessible information on maintaining and building intrinsic capacity (e.g. One You https://www.nhs.uk/oneyou/#ySRbk2Ie0jtCwoCu.97 , general guidance on prevention of MSk conditions through physical activity and illustrated strength and balance exercises)
•Information (including digital) about accessible and affordable local services
Supporting self-care and prevention n Primary care
treatment
•Self –care and prevention platforms
•Advise on health and fitness to build intrinsic capacity to prevent, manage and improve MSk conditions and associated pain integral to treatment plans
•Training and education of primary care staff on MECC , health & fitness and intrinsic capacity
•Promote health and prevent MSk conditions through social prescribing e.g. green gym, walking and cycling.
Supporting self-care and prevention in Secondary care
treatment
•Self –care and prevention platforms
•Advise on health and fitness to build intrinsic capacity to prevent, manage and improve MSk conditions and associated pain integral to treatment plans
•Training and education of primary care staff on MECC , health & fitness and intrinsic capacity
•Promote health and prevent MSk conditions through social prescribing e.g. green gym, walking and cycling.
6 Triage Specification – September 2018 – Pharmacological Management – Low Back Pain (without Sciatica)
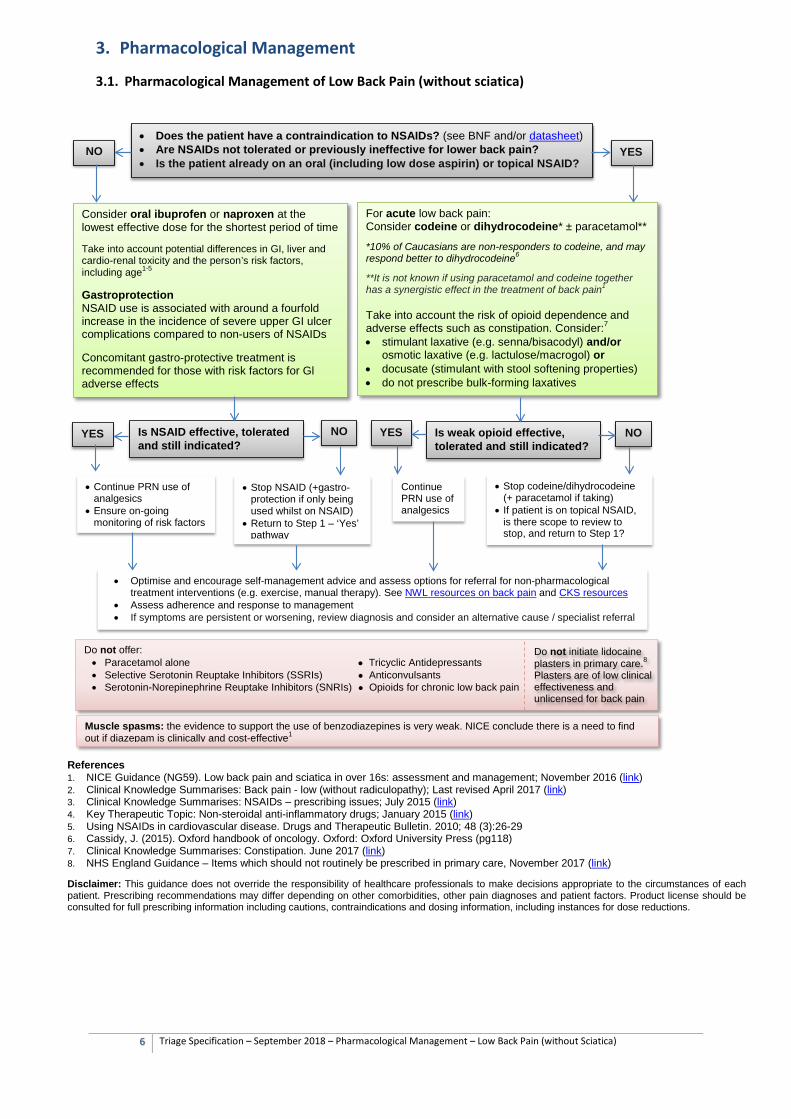
3. Pharmacological Management
3.1. Pharmacological Management of Low Back Pain (without sciatica)
References 1. NICE Guidance (NG59). Low back pain and sciatica in over 16s: assessment and management; November 2016 (link) 2. Clinical Knowledge Summarises: Back pain - low (without radiculopathy); Last revised April 2017 (link) 3. Clinical Knowledge Summarises: NSAIDs – prescribing issues; July 2015 (link) 4. Key Therapeutic Topic: Non-steroidal anti-inflammatory drugs; January 2015 (link) 5. Using NSAIDs in cardiovascular disease. Drugs and Therapeutic Bulletin. 2010; 48 (3):26-29 6. Cassidy, J. (2015). Oxford handbook of oncology. Oxford: Oxford University Press (pg118) 7. Clinical Knowledge Summarises: Constipation. June 2017 (link) 8. NHS England Guidance – Items which should not routinely be prescribed in primary care, November 2017 (link) Disclaimer: This guidance does not override the responsibility of healthcare professionals to make decisions appropriate to the circumstances of each patient. Prescribing recommendations may differ depending on other comorbidities, other pain diagnoses and patient factors. Product license should be consulted for full prescribing information including cautions, contraindications and dosing information, including instances for dose reductions.
Consider oral ibuprofen or naproxen at the lowest effective dose for the shortest period of time Take into account potential differences in GI, liver and cardio-renal toxicity and the person’s risk factors, including age1-5
Gastroprotection NSAID use is associated with around a fourfold increase in the incidence of severe upper GI ulcer complications compared to non-users of NSAIDs Concomitant gastro-protective treatment is recommended for those with risk factors for Gl adverse effects
• Does the patient have a contraindication to NSAIDs? (see BNF and/or datasheet) • Are NSAIDs not tolerated or previously ineffective for lower back pain? • Is the patient already on an oral (including low dose aspirin) or topical NSAID?
For acute low back pain: Consider codeine or dihydrocodeine* ± paracetamol** *10% of Caucasians are non-responders to codeine, and may respond better to dihydrocodeine6
**It is not known if using paracetamol and codeine together has a synergistic effect in the treatment of back pain1
Take into account the risk of opioid dependence and adverse effects such as constipation. Consider:7 • stimulant laxative (e.g. senna/bisacodyl) and/or
osmotic laxative (e.g. lactulose/macrogol) or • docusate (stimulant with stool softening properties) • do not prescribe bulk-forming laxatives
Is NSAID effective, tolerated and still indicated?
NO
YES
NO
YES Is weak opioid effective, tolerated and still indicated?
NO
YES
• Continue PRN use of analgesics
• Ensure on-going monitoring of risk factors
• Stop NSAID (+gastro-protection if only being used whilst on NSAID)
• Return to Step 1 – ‘Yes’ pathway
Continue PRN use of analgesics
• Stop codeine/dihydrocodeine (+ paracetamol if taking)
• If patient is on topical NSAID, is there scope to review to stop, and return to Step 1?
Do not offer: • Paracetamol alone ● Tricyclic Antidepressants • Selective Serotonin Reuptake Inhibitors (SSRIs) ● Anticonvulsants • Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs) ● Opioids for chronic low back pain
• Optimise and encourage self-management advice and assess options for referral for non-pharmacological treatment interventions (e.g. exercise, manual therapy). See NWL resources on back pain and CKS resources
• Assess adherence and response to management • If symptoms are persistent or worsening, review diagnosis and consider an alternative cause / specialist referral
Muscle spasms: the evidence to support the use of benzodiazepines is very weak. NICE conclude there is a need to find out if diazepam is clinically and cost-effective1
Do not initiate lidocaine plasters in primary care.8
Plasters are of low clinical effectiveness and unlicensed for back pain
7 Triage Specification – September 2018 – Pharmacological Management of Sciatica
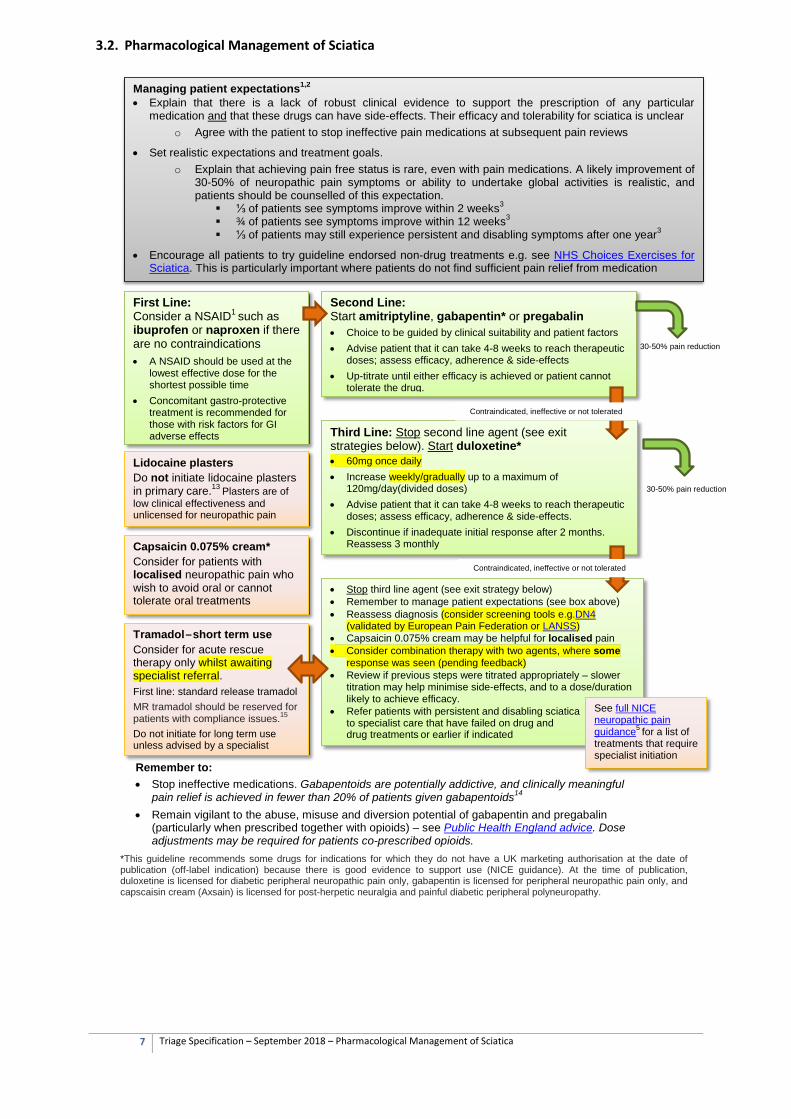
3.2. Pharmacological Management of Sciatica
Managing patient expectations1,2 • Explain that there is a lack of robust clinical evidence to support the prescription of any particular
medication and that these drugs can have side-effects. Their efficacy and tolerability for sciatica is unclear o Agree with the patient to stop ineffective pain medications at subsequent pain reviews
• Set realistic expectations and treatment goals. o Explain that achieving pain free status is rare, even with pain medications. A likely improvement of
30-50% of neuropathic pain symptoms or ability to undertake global activities is realistic, and patients should be counselled of this expectation.
⅓ of patients see symptoms improve within 2 weeks3 ¾ of patients see symptoms improve within 12 weeks3 ⅓ of patients may still experience persistent and disabling symptoms after one year3
• Encourage all patients to try guideline endorsed non-drug treatments e.g. see NHS Choices Exercises for Sciatica. This is particularly important where patients do not find sufficient pain relief from medication
First Line:
Consider a NSAID1 such as ibuprofen or naproxen if there are no contraindications
• A NSAID should be used at the lowest effective dose for the shortest possible time
• Concomitant gastro-protective treatment is recommended for those with risk factors for GI adverse effects
Second Line: Start amitriptyline, gabapentin* or pregabalin
• Choice to be guided by clinical suitability and patient factors • Advise patient that it can take 4-8 weeks to reach therapeutic
doses; assess efficacy, adherence & side-effects • Up-titrate until either efficacy is achieved or patient cannot
tolerate the drug.
• Stop third line agent (see exit strategy below) • Remember to manage patient expectations (see box above) • Reassess diagnosis (consider screening tools e.g.DN4
(validated by European Pain Federation or LANSS) • Capsaicin 0.075% cream may be helpful for localised pain • Consider combination therapy with two agents, where some
response was seen (pending feedback) • Review if previous steps were titrated appropriately – slower
titration may help minimise side-effects, and to a dose/duration likely to achieve efficacy.
• Refer patients with persistent and disabling sciatica to specialist care that have failed on drug and non-drug treatments or earlier if indicated
Third Line: Stop second line agent (see exit strategies below). Start duloxetine*
• 60mg once daily • Increase weekly/gradually up to a maximum of
120mg/day(divided doses) • Advise patient that it can take 4-8 weeks to reach therapeutic
doses; assess efficacy, adherence & side-effects. • Discontinue if inadequate initial response after 2 months.
Reassess 3 monthly
Remember to: • Stop ineffective medications. Gabapentoids are potentially addictive, and clinically meaningful
pain relief is achieved in fewer than 20% of patients given gabapentoids14 • Remain vigilant to the abuse, misuse and diversion potential of gabapentin and pregabalin
(particularly when prescribed together with opioids) – see Public Health England advice. Dose adjustments may be required for patients co-prescribed opioids.
Tramadol – short term use Consider for acute rescue therapy only whilst awaiting specialist referral. First line: standard release tramadol MR tramadol should be reserved for patients with compliance issues.15
Do not initiate for long term use unless advised by a specialist
Capsaicin 0.075% cream* Consider for patients with localised neuropathic pain who wish to avoid oral or cannot tolerate oral treatments
Lidocaine plasters Do not initiate lidocaine plasters in primary care.13 Plasters are of low clinical effectiveness and unlicensed for neuropathic pain
30-50% pain reduction
Contraindicated, ineffective or not tolerated
30-50% pain reduction
Contraindicated, ineffective or not tolerated
See full NICE neuropathic pain guidance5 for a list of treatments that require specialist initiation
*This guideline recommends some drugs for indications for which they do not have a UK marketing authorisation at the date of publication (off-label indication) because there is good evidence to support use (NICE guidance). At the time of publication, duloxetine is licensed for diabetic peripheral neuropathic pain only, gabapentin is licensed for peripheral neuropathic pain only, and capscaisin cream (Axsain) is licensed for post-herpetic neuralgia and painful diabetic peripheral polyneuropathy.
8 Triage Specification – September 2018 – Pharmacological Management of Sciatica
Amitriptyline: • Starting dose of 10-25mg in the evening
• Increase by 10-25mg every 3 days as tolerated up to a maximum dose of 75mg daily (higher doses on specialist recommendation)
Gabapentin: • Starting dose of 300mg once daily (consider lower dose of 100mg once daily in elderly patients,
patients with low body weight or patients sensitive to gabapentin) • Increase by 300mg/day increments every 2-3 days, in divided doses, until effective, limited by
side-effects or a maximum dose of 3.6g daily is reached (consider slower titration by 100mg increments every 2-3 days, in divided doses, for elderly patients, patients with low body weight or patients sensitive to gabapentin but showing adequate response).
• Example Patient information Leaflet LINK Pregabalin: • Starting dose of 75mg daily (consider lower dose of 25mg/day in the elderly or patients with low
body weight) • Increase by 75mg every 3 days, in divided doses, until effective, limited by side-effects or a
maximum dose of 600mg daily is reached (consider slower titration by 25mg increments every 3 day, in divided doses, for elderly patients, patients with low body weight or patients sensitive to pregabalin but showing adequate response).
• Example Patient information Leaflet LINK Duloxetine • Example Patient information Leaflet LINK Discontinuing of therapy: If treatment has been ineffective, you may need to take into account withdrawal symptoms and consider gradual withdrawal of treatment:
Amitriptyline: The risk of withdrawal symptoms is increased if stopped suddenly after regular administration for 8 weeks or more, although withdrawal effects can occur within 5 days of stopping treatment. The dose should preferably be reduced gradually over about 4 weeks, or longer if withdrawal symptoms emerge. Gabapentin, pregabalin and duloxetine: Discontinuation should be gradual over a minimum of 1– 2 weeks.
References 1. NICE Guidance (NG59). Low back pain and sciatica in over 16s: assessment and management; November 2016 (link) 2. BMJ 2012; 344 doi: https://doi.org/10.1136/bmj.e497 (Published 13 February 2012) 3. BMJ 2013; 346 doi: https://doi.org/10.1136/bmj.f2690 (Published 03 May 2013) 4. BMJ 2017; 359 doi: https://doi.org/10.1136/bmj.j4248 (Published 12 October 2017) 5. NICE Clinical Guidelines (CG173): Neuropathic pain in adults: pharmacological management in non-specialist settings. November 2013 (link) 6. NICE Clinical Knowledge Summaries, Sciatica (lumbar radiculopathy), last updated February 2017 (link) 7. Summary of Product Characteristics, amitriptyline 10mg tablets (Activas UK). Date of revision of text: 16/10/17 (link) 8. Summary of Product Characteristics, Cymbalta (duloxetine) 30mg capsules (Eli Lilly and Company Limited). Date of revision of text: 26/1/17 (link) 9. Summary of Product Characteristics, Neurotin (gabapentin) 300mg capsules (Pfizer Limited). Date of revision of text: 9/17 (link) 10. Summary of Product Characteristics, Lyrica capsules (Pfizer Limited). Date of revision of text: 11/17 (link) 11. BNF online – amitriptyline monograph, accessed 04/10/17 12. Neuropathic pain – pharmacological management of neuropathic pain in adults in non-specialist settings, Updated February 2017 (link) 13. NHS England Guidance – Items which should not routinely be prescribed in primary care, November 2017 (link) 14. Department of Health. Drug misuse and dependence, July 2017 (link) 15. Openprescribing.net – Prescribing of high cost tramadol preparations by all CCGs (link)
Disclaimer: This guidance does not override the responsibility of healthcare professionals to make decisions appropriate to the circumstances of each patient. Prescribing recommendations may differ depending on other comorbidities, other pain diagnoses and patient factors. Product license should be consulted for full prescribing information including cautions, contraindications and dosing information, including instances for dose reductions. Recommended titration protocols may differ to the BNF/product datasheet but
9 Triage Specification – September 2018 – Triage
4. Triage
4.1. Specification for Triage
Effective triage is defined as Safe – triage is carried out in a timely manner (48 hours) by appropriately trained staff who
are triaging against evidence-based criteria which enables severity to be flagged early. Continuous audit of practitioners practice, highlighting repeat or re-referrals for same condition, as well as patient and clinician feedback and learning from complaints will ensure a safe service is being provided.
Effective – All referrals are triaged, including Consultant to Consultant referrals. Audit and reporting systems are in place to measure onward referral rates, clinical outcomes and final fate of patients.
Evidence based – One set of evidence-based published clinical pathways for adoption across North West London which are regularly audited.
4.2. Competencies of Triage Staff
It is important that staff clinically triaging referrals have the appropriate skills and experience to understand patients’ conditions and have access to a Multi-Disciplinary Team (MDT) for triage queries. Typically, orthopaedic and pain triage services should be staffed Extended Scope Practitioners (ESPs) or Advanced Practitioners with MSk experience who are experienced at working in community care. Rheumatology triage services should typically be triaged by GPs with Special Interest, rheumatologists or allied health professionals (AHPs) with further training and experience in rheumatology. 4.3. Training and Education
All Triage staff should be trained in the following skills: • Leadership • Communication • Management • Ability to delegate • Knowledge of scenarios and specialities available • Relationships with secondary care consultants
Primary Care clinicians should be trained in the following:
• Referral criteria • Triage clinician role • Adherence to clinical guidelines
It is important that there is consistency of approach and outcome across the Triage providers within North West London, and as such common standards have been developed that all CCGs have agreed to adhere to. These will be audited against regularly to provide feedback to triage staff, identify unwarranted variation, and inform future training requirements.
10 Triage Specification – September 2018 – MSk Pathways
5. Musculoskeletal Pathways
5.1. Generic Musculoskeletal Pathway Template
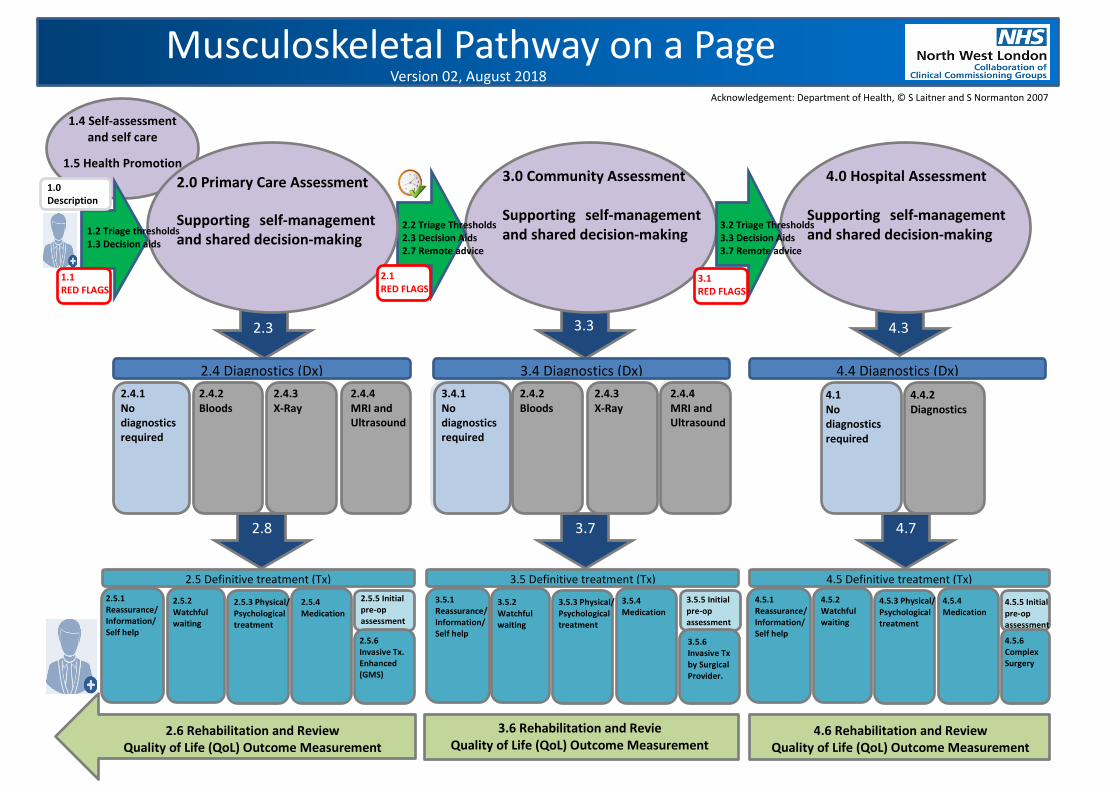
The high impact musculoskeletal pathways in NW London are based on the Department of Health 18 Week Commissioning Pathways (2007). Settings of care
The template uses a grid. Going from left to right, there are different settings of care: • Self-management
• Primary care
• Community care (musculoskeletal physiotherapy and interface services)
• Secondary care.
Assessment and Management
The columns contain the assessment and management in each setting of care. The transitions to each setting of care are shown by green arrows. Further information
• The generic musculoskeletal pathway template is shown below.
• The referral criteria for each transition (green arrows) are detailed in the pathway sections (further below).
• Process maps for all musculoskeletal services are shown in the following chapter.
• Assessment and management along specific musculoskeletal pathways in NW London are published separately.
Musculoskeletal Pathway on a Page
2.4 Diagnostics (Dx) 4.4 Diagnostics (Dx) 3.4 Diagnostics (Dx)
2.0 Primary Care Assessment Supporting self-management and shared decision-making
3.0 Community Assessment Supporting self-management and shared decision-making
4.0 Hospital Assessment Supporting self-management and shared decision-making
2.5 Definitive treatment (Tx) 3.5 Definitive treatment (Tx) 4.5 Definitive treatment (Tx)
1.4 Self-assessment and self care
1.5 Health Promotion
2.5.1 Reassurance/ Information/ Self help
2.5.2 Watchful waiting
2.5.3 Physical/ Psychological treatment
2.5.4 Medication
2.5.5 Initial pre-op assessment 2.5.6 Invasive Tx. Enhanced (GMS)
1.0 Description
2.8
2.3 3.3 4.3
4.7 3.7
1.2 Triage thresholds 1.3 Decision aids
2.2 Triage Thresholds 2.3 Decision Aids 2.7 Remote advice
3.2 Triage Thresholds 3.3 Decision Aids 3.7 Remote advice
Version 02, August 2018
2.4.1 No diagnostics required
2.4.2 Bloods
2.4.3 X-Ray
2.4.4 MRI and Ultrasound
4.1 No diagnostics required
4.4.2 Diagnostics
3.5.1 Reassurance/ Information/ Self help
4.5.1 Reassurance/ Information/ Self help
4.5.2 Watchful waiting
3.5.2 Watchful waiting
4.5.3 Physical/ Psychological treatment
3.5.3 Physical/ Psychological treatment
4.5.4 Medication
3.5.4 Medication 4.5.5 Initial
pre-op assessment
3.5.5 Initial pre-op assessment
4.5.6 Complex Surgery
3.5.6 Invasive Tx by Surgical Provider.
1.1 RED FLAGS
2.1 RED FLAGS 3.1
RED FLAGS
2.6 Rehabilitation and Review Quality of Life (QoL) Outcome Measurement
3.6 Rehabilitation and Revie Quality of Life (QoL) Outcome Measurement
4.6 Rehabilitation and Review Quality of Life (QoL) Outcome Measurement
3.4.1 No diagnostics required
2.4.2 Bloods
2.4.3 X-Ray
2.4.4 MRI and Ultrasound
Acknowledgement: Department of Health, © S Laitner and S Normanton 2007
12 Triage Specification – September 2018 – Carpal Tunnel Syndrome
5.2. Carpal Tunnel Syndrome
Background
Carpal tunnel syndrome present with non-traumatic tingling of the fingers due to compression of the median nerve at the wrist. Carpal tunnel syndrome is a common condition with a prevalence of between 7-16% in the UK. It is the commonest form of nerve entrapment. The differential diagnosis includes cubital tunnel syndrome (ulnar nerve entrapment at the elbow causing tingling in the lateral fingers), cervical nerve root irritation and adverse neural tension (loss of extensibility of the nerves arm with movement). Typical symptoms of carpal tunnel syndrome include:
• Intermittent tingling, numbness or altered sensation and burning or pain in the distribution of the median nerve (the thumb, index finger, middle finger, and radial half of the ring finger).
• Symptoms are often worse at night and can disrupt sleep.
• Symptoms may affect one or both hands.
• Pain in the hand may radiate up the arm into the wrist or as far as the shoulder.
• The person may complain of loss of grip strength, clumsiness and reduced manual dexterity for example when doing up buttons.
• Some people may present atypically, for example, they may have sensory changes in all digits.
• Severe disease may cause unremitting sensory symptoms, weakness or thenar muscle wasting.
Investigations
• Blood tests are only needed if the history and examination suggest an (undiagnosed) secondary cause or association such as inflammatory arthritis, hypothyroidism, acromegaly or diabetes.
• Imaging may be required if suspected trauma, fracture or ganglion.
• Electrophysiological testing should only be carried out in specialist settings of care, and reserved for situations where there is diagnostic doubt, complex cases, or if symptoms recur after initial surgery.
If referral is not indicated, manage carpal tunnel syndrome in primary care by
• Optimising treatment of any underlying condition, such as osteoarthritis, rheumatoid arthritis or hypothyroidism.
• Advise the person that lifestyle modifications (such as avoidance of repetitive movements or breaks from tasks that precipitate symptoms) may help.
• Wrist splinting in a neutral position - this can help with night time symptoms in particular. Splints can be purchased by the person from a pharmacy.
• Corticosteroid injection - this can be carried out in primary care if appropriate expertise is available.
13 Triage Specification – September 2018 – Carpal Tunnel Syndrome
Referral to General Practitioner
(Referral from triage, community or hospital services specifically for primary care medical review)
Inclusions
Assessment and management of multi-morbidity e.g. diabetes, hypothyroidism, osteoarthritis, and psychiatric co-morbidity.
If high suspicion of possible inflammatory arthritis, do not delay referral to a rheumatologist by waiting for investigations.
Medication reviews and non-urgent prescriptions.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Discussion about fitness for work and sickness certification.
Management following discharge from community or secondary care where no further intervention planned.
Patients referred back from community services with known or suspected serious underlying pathology where non-urgent (for re-evaluation and possible referral to secondary care).
Exclusions
Patients seen in community or secondary care settings who need emergency or urgent assessment e.g. suspicion of inflammatory joint disease, peripheral vascular disease or fracture.
14 Triage Specification – September 2018 – Carpal Tunnel Syndrome
Referral to Community Physiotherapy or First Contact Physiotherapist in Primary Care
Inclusions
Requires provision of splint if unable to purchase. (Patients can purchase wrist splints from pharmacy or online).
Requires advice on splint fitting and usage (in non-routine circumstances).
Requires advice on activity modification if causing symptoms.
Requires stretching and strengthening and joint mobilisation.
If post-operative hand therapy commissioned:
Post-operative hand therapy
Exclusions
Patients who need urgent rheumatology assessment e.g. suspicion of inflammatory joint disease.
Patients who need emergency orthopaedic assessment e.g. suspected fracture.
Patients with muscle weakness or wasting (refer to interface service).
15 Triage Specification – September 2018 – Carpal Tunnel Syndrome
Referral to Musculoskeletal Interface Service
Inclusions
Unsuccessful conservative treatment, including a trial of splinting, for mild carpal tunnel syndrome after 8 weeks.
Steroid injection if GP has not already administered.
Moderate symptoms, defined as:
o Intermittent paraesthesia in a median nerve distribution o Regular night waking o NO persistent hypoesthesia o Vibration sense may be reduced o Objective but mild weakness of the thenar muscles.
Diagnostic uncertainty
Interface service to ensure PPwT thresholds met and authorisation obtained prior to referral to secondary care for consideration of surgery.
Exclusions
Patients who need urgent rheumatology assessment e.g. suspicion of inflammatory joint disease.
Patients who need emergency orthopaedic assessment e.g. suspected fracture.
Anticoagulated, if requiring injection (ESPs may not be able to inject joint under patient group direction) (Consider GP minor surgery scheme if available).
16 Triage Specification – September 2018 – Carpal Tunnel Syndrome
Referral to Secondary Care Orthopaedics
Inclusions
Severe or deteriorating symptoms including:
o Persistent paraesthesia in a median nerve distribution o Regular night-waking and day time symptoms o Persistent hypoesthesia or numbness in a median nerve distribution o Vibration sense may be reduced o Moderate or severe weakness, or wasting of the thenar muscles.
Moderate to severe symptoms that persist after conservative therapy with either local corticosteroid injection (if appropriate) and/or nocturnal splinting (used for at least 8 weeks):
o Intermittent paraesthesia in a median nerve distribution o Regular night waking o NO persistent hypoesthesia o Vibration sense may be reduced o Objective but mild weakness of the thenar muscles.
Patient prepared to have surgical intervention following a shared decision-making discussion guided by a decision aid tool:
o All treatment options: https://patient.azureedge.net/treatment-options/carpal-tunnel-syndrome.pdf
o Surgery: https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=aa5319
Thresholds for carpal tunnel surgery (NWL PPwT version 4) https://www.hounslowccg.nhs.uk/news,-publications-and-policies/publications.aspx?n=2010:
o Patient has severe symptoms (see above), interfering with activities of daily living that persist after conservative therapy with either local corticosteroid injection and/or nocturnal splinting.
o Neurological deficit e.g. sensory blunting, muscle wasting or weakness of thenar abduction.
o Patients who smoke should have attempted to stop smoking 8 to 12 weeks before referral to reduce the risk of surgery and the risk of post-surgery complications. Patients should be routinely offered referral to smoking cessation services to reduce these surgical risks.
Exclusions
Suspected fracture or septic arthritis. (Refer to on-call orthopaedic team or A&E).
Suspicion of inflammatory joint disease, peripheral vascular disease. (Discuss with on-call specialist, or refer to medical, rheumatology or vascular team, depending on clinical presentation and urgency).
Patients who have not been triaged or referred from a community musculoskeletal service (including non-urgent internally generated referrals (consultant to consultant referrals).
PPwT form has not been completed by referrer where request is for a procedure covered by the policy.
Referral is not accompanied by any pre-requisite imaging or investigations required by the consultant or unit.
17 Triage Specification – September 2018 – MSk Pathways – Connective Tissue Disease and Vasculitis
5.3. Connective Tissue Disease and Vasculitis
Background
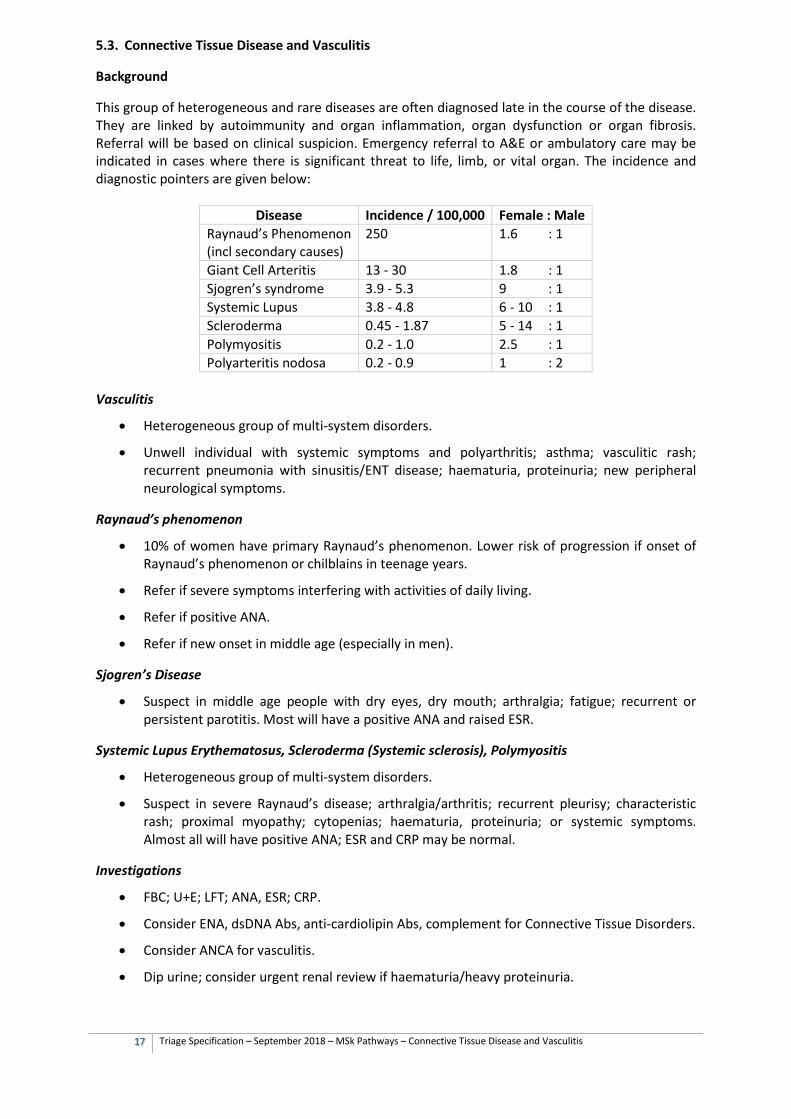
This group of heterogeneous and rare diseases are often diagnosed late in the course of the disease. They are linked by autoimmunity and organ inflammation, organ dysfunction or organ fibrosis. Referral will be based on clinical suspicion. Emergency referral to A&E or ambulatory care may be indicated in cases where there is significant threat to life, limb, or vital organ. The incidence and diagnostic pointers are given below:
Disease Incidence / 100,000 Female : Male Raynaud’s Phenomenon (incl secondary causes)
250 1.6 : 1
Giant Cell Arteritis 13 - 30 1.8 : 1 Sjogren’s syndrome 3.9 - 5.3 9 : 1 Systemic Lupus 3.8 - 4.8 6 - 10 : 1 Scleroderma 0.45 - 1.87 5 - 14 : 1 Polymyositis 0.2 - 1.0 2.5 : 1 Polyarteritis nodosa 0.2 - 0.9 1 : 2
Vasculitis
• Heterogeneous group of multi-system disorders.
• Unwell individual with systemic symptoms and polyarthritis; asthma; vasculitic rash; recurrent pneumonia with sinusitis/ENT disease; haematuria, proteinuria; new peripheral neurological symptoms.
Raynaud’s phenomenon
• 10% of women have primary Raynaud’s phenomenon. Lower risk of progression if onset of Raynaud’s phenomenon or chilblains in teenage years.
• Refer if severe symptoms interfering with activities of daily living.
• Refer if positive ANA.
• Refer if new onset in middle age (especially in men).
Sjogren’s Disease
• Suspect in middle age people with dry eyes, dry mouth; arthralgia; fatigue; recurrent or persistent parotitis. Most will have a positive ANA and raised ESR.
Systemic Lupus Erythematosus, Scleroderma (Systemic sclerosis), Polymyositis
• Heterogeneous group of multi-system disorders.
• Suspect in severe Raynaud’s disease; arthralgia/arthritis; recurrent pleurisy; characteristic rash; proximal myopathy; cytopenias; haematuria, proteinuria; or systemic symptoms. Almost all will have positive ANA; ESR and CRP may be normal.
Investigations
• FBC; U+E; LFT; ANA, ESR; CRP.
• Consider ENA, dsDNA Abs, anti-cardiolipin Abs, complement for Connective Tissue Disorders.
• Consider ANCA for vasculitis.
• Dip urine; consider urgent renal review if haematuria/heavy proteinuria.
18 Triage Specification – September 2018 – MSk Pathways – Connective Tissue Disease and Vasculitis
Referral to General Practitioner
(Referral from triage, community or hospital services specifically for primary care medical review)
Inclusions
Assessment and management of multi-morbidity and psychiatric co-morbidity.
Medication reviews and non-urgent prescriptions. Note, for disease-modifying drugs and immunosuppressants initiated in secondary care, there must be an shared care protocol that has been agreed and accepted by both the primary and secondary care clinician responsible for an individual patient.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Discussion about fitness for work and sickness certification.
Management following discharge from community or secondary care where no further intervention planned.
Patients referred back from community services with known or suspected serious underlying pathology where non-urgent (for re-evaluation and possible referral to secondary care).
Exclusions
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Patients seen in community or secondary care settings who need emergency or urgent assessment e.g. suspicion of inflammatory joint disease, peripheral vascular disease or fracture.
19 Triage Specification – September 2018 – MSk Pathways – Connective Tissue Disease and Vasculitis
Referral to Community Physiotherapy or First Contact Physiotherapist in Primary Care
Inclusions
Assessment and treatment of functional impairment.
Assessment of falls and provision of walking aids.
Improve general fitness and participation in regular physical activity.
Exercises for enhancing flexibility and muscle strength.
Exclusions
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Severe acute pain or inflammation.
Patient needs medical opinion.

20 Triage Specification – September 2018 – MSk Pathways – Connective Tissue Disease and Vasculitis
Referral to Rheumatology Interface Service
(May not be available in every CCG)
Inclusions
If rheumatological physiotherapy, hand therapy, occupational therapy, podiatry and psychology available:
Assessment and treatment of functional impairment.
Assessment of gait and stability, provision of orthotics.
Assessment and provision of splints and braces.
Advice and assessment about aids and adaptations to assist activities of daily living and promote independence.
Psychological interventions (for example, relaxation, stress management) and cognitive coping skills.
If rheumatology nurse or therapist with rheumatology training available:
Symptom and medication monitoring under shared care arrangement with primary and secondary care.
If rheumatologist or GP with a special interest available:
Diagnostic assessment and management advice. Patients particularly suited to community assessment are those with vague and undifferentiated symptoms where clinically there is a lower index of suspicion of inflammatory disease. (Patients clinically with a high index of suspicion should be referred to secondary care, unless a community service is specifically commissioned for this group of patients.)
Exclusions
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Severe acute pain or inflammation, unless service commissioned for acute assessment.
Patient needs medical opinion, unless a medical opinion commissioned.
21 Triage Specification – September 2018 – MSk Pathways – Connective Tissue Disease and Vasculitis
Referral to Secondary Care Rheumatology
Inclusions
Suspected connective tissue disease or vasculitis. (See history and supporting tests in ‘Background’ above). Negative or absent blood tests should not delay referrals made on clinical grounds.
Flare-up of connective tissue disease or vasculitis.
Any imaging performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral. Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
Exclusions
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Patient unable to manage at home due to severe symptoms. Discuss with rheumatology service in working hours; out of hours consider intermediate care assessment or other admission avoidance scheme, emergency admission or ambulatory care if critically unwell.
22 Triage Specification – September 2018 – MSk Pathways – Hip osteoarthritis
5.4. Hip osteoarthritis
Background
Osteoarthritis of the hip describes a clinical syndrome of joint pain accompanied by varying degrees of functional limitation and reduced quality of life. Approximately 450 patients per 100,000 will present to primary care with hip pain yearly. A quarter of these will have sustained improvement within three months and one third at a year. Osteoarthritis may not be progressive and most patients will not need surgery, with their symptoms adequately controlled by non-surgical measures. Symptoms progress in 15% of patients within 3 years and 28% within 6 years. Typically osteoarthritis presents in only one or a few joints at any one time, and pain develops over months or year Differential diagnosis
Degenerative hip disease is the most common diagnosis in the adult and is the long-term consequence of predisposing conditions. Inflammatory joint disease of the hip may develop at any age, alone or with other joint involvement and may be due to auto-immune disease. Tendinopathies affecting the adductors, psoas, hamstrings, or most commonly the abductors can occur. Trochanteric pain with local tenderness, is often due to trochanteric bursitis or abductor tendinopathy. Isolated trochanteric pain due to bursitis or tendinopathy settles in 64% after one year and 71% after five years.
Pain felt around and attributed to the hip can also be due to spinal or abdominal disorders which should be excluded. Hip pathology may cause pain felt only at the knee. In the young adult, Femoroacetabular Impingement Syndrome (FAI), labral tears and hip dysplasia may cause hip pain, usually felt in the groin Clinical history
Diagnose osteoarthritis clinically without investigations, after excluding alternative diagnoses (above) if a person:
1. Is aged 45 years or over, and
2. Activity-related joint pains, and
3. Has either no morning joint-related stiffness or morning stiffness that lasts no longer than 30 minutes.
• Functional impairment such as difficulty walking, climbing stairs, dressing, driving, or making sex painful.
• Psychosocial impact: may affect self-confidence, self-esteem, sleep quality, relationships and ability to self-care and care for others; may cause anxiety and depression
Examination
• Deep pain in the anterior groin on walking or climbing stairs, with possible referred pain to the lateral thigh and buttock, anterior thigh, knee, and ankle.
• Pain which may occur at rest and may disturb sleep.
• Painful restriction of internal rotation with the hip flexed.
• An antalgic gait — a lurch towards the affected hip with less time spent weight-bearing on that side; the pelvis is held normally.
• In advanced disease, there may be: o A Trendelenburg gait — a lurch towards the affected hip with less time spent
weight-bearing on that side and the pelvis tilting down on the unaffected side. o A fixed flexion external rotation deformity, with compensatory increased lumbar
lordosis and pelvic tilt. The lower limb can be significantly shortened.
23 Triage Specification – September 2018 – MSk Pathways – Hip osteoarthritis
Referral to General Practitioner
(Referral from triage, community or hospital services specifically for primary care medical review)
Inclusions
Assessment and management of multi-morbidity and psychiatric co-morbidity.
Medication reviews and non-urgent prescriptions.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Discussion about fitness for work and sickness certification
Management following discharge from community or secondary care where no further intervention planned
Patients referred back from community services with known or suspected serious underlying pathology where non-urgent (for re-evaluation and possible referral to secondary care).
Exclusions
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to bear any weight, history of a fall, suspected fracture or dislocation.
Patients seen in community or secondary care settings who need urgent specialist assessment e.g. severe pain unresponsive to analgesia and persistent loss of function.
24 Triage Specification – September 2018 – MSk Pathways – Hip osteoarthritis
Referral to Community Physiotherapy or First Contact Physiotherapy in Primary Care
Inclusions
Assessment and advice about the condition to aid shared decision-making, taking account of health literacy and patient beliefs.
o Acute or chronic groin, medial thigh, lateral hip or buttock pain; which may radiate to thigh or knee. Hip problems can present as isolated knee pain.
o Suspected or known osteoarthritis of the hip.
o Clicking or clunking hips with associated pain.
o Limited hip range causing loss of function.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Assessment and treatment of functional impairment.
Assessment of falls and provision of walking aids.
Advice and assessment about aids and adaptations to assist activities of daily living and promote independence.
Improve general fitness and participation in regular physical activity.
Exercises for enhancing flexibility and muscle strength.
If post-operative physiotherapy commissioned:
Post-operative physiotherapy
Exclusions
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to bear any weight, history of a fall, suspected fracture or dislocation.
Suspected inflammatory arthritis, unless rheumatological assessment commissioned.
Patients who need urgent specialist assessment e.g. severe pain unresponsive to analgesia and persistent loss of function.
Community physiotherapy only exclusions
Presented with same condition within previous 12 months, and there was no substantive improvement with treatment previously, and if no other community treatment options are appropriate (e.g. pain service, where commissioned).
Patients with frailty and high risk of falls, where a falls service is commissioned.
Co-morbidities that significantly impair a particular patient’s ability to exercise. For example neurological (e.g. stroke), severe cardiac, renal, liver or respiratory failure, recurrent disabling hypoglycaemia or poorly controlled epilepsy.
25 Triage Specification – September 2018 – MSk Pathways – Hip osteoarthritis
Referral to Musculoskeletal Interface Service
(May not be available in every CCG)
Inclusions
Unsuccessful conservative treatment (exercises, self-management strategies, physiotherapy and analgesia)
o Including suspected labral tears, ligament/capsular pathology and tendinopathies.
Diagnostic uncertainty
Interface service to ensure PPwT thresholds met and authorisation obtained prior to referral to secondary care for consideration of surgery.
Interface service to ensure onward referral to secondary care is accompanied by any imaging required by the receiving consultant or unit.
In very elderly patients and those assessed to be unsuitable for surgery, consider referral for image-guided intra-articular steroids - beneficial for between 3 weeks and 3 months.
Exclusions
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to bear any weight, history of a fall, suspected fracture or dislocation. These patients will be referred back to GP for urgent assessment (same day), or to A&E as clinically appropriate.
Suspected inflammatory arthritis, unless rheumatological assessment commissioned.
Patients who need urgent specialist assessment e.g. severe pain unresponsive to analgesia and persistent loss of function
Patients with frailty and high risk of falls, where a falls service is commissioned.
26 Triage Specification – September 2018 – MSk Pathways – Hip osteoarthritis
Referral to Secondary Care Orthopaedics
Inclusions
Unsuccessful conservative management.
Diagnostic uncertainty.
Patient prepared to have surgical intervention following a shared decision making discussion guided by a decision aid tool:
o All treatment options: http://www.decisionbox.ulaval.ca/fileadmin/documents/decisionbox/document/dbox.hip_knee_osteoarthritis.pdf
o Surgery: https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=uh1515
Thresholds for total hip replacement (NWL PPwT version 4) https://www.hounslowccg.nhs.uk/news,-publications-and-policies/publications.aspx?n=2010:
o Patient complains of severe joint pain AND functional limitation, despite the use of non- surgical treatments such as adequate doses of NSAID analgesia, weight control treatments and physical therapies OR
o Patient complains of mild to moderate joint pain AND has severe functional limitation, despite the use of non-surgical treatments such as adequate doses of NSAID analgesia, weight control treatments and physical therapies.
o Patients who smoke should have attempted to stop smoking 8 to 12 weeks before referral to reduce the risk of surgery and the risk of post-surgery complications. Patients should be routinely offered referral to smoking cessation services to reduce these surgical risks.
Any imaging (including X-ray hip) performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral. Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
Exclusions
Suspected fracture, dislocation, malignancy or septic arthritis. (Refer to on-call orthopaedic team or A&E).
Suspicion of inflammatory joint disease, peripheral vascular disease. (Discuss with on-call specialist, or refer to medical, rheumatology or vascular team, depending on clinical presentation and urgency).
Patients who have not been triaged or referred from a community musculoskeletal service (including non-urgent internally generated referrals (consultant to consultant referrals).
Conservative management and self-management strategies are clinically appropriate but have not been tried.
PPwT form has not been completed by referrer where request is for a procedure covered by the policy.
Referral is not accompanied by any pre-requisite imaging or investigations required by the consultant or unit.
27 Triage Specification – September 2018 – MSk Pathways – Inflammation of Multiple Joints
5.5. Inflammation of multiple joints
Background
Inflammatory polyarthritis (arthritis of multiple joints) should be suspected in patients with morning stiffness lasting greater than 30 minutes, positive MCP or MTP squeeze tests, or swollen joints (synovitis) on palpation. Other features that may support the diagnosis of polyarthritis include a personal or family history of psoriasis, inflammatory bowel disease or anterior uveitis or personal history of recent genitourinary infection or bowel infection. Fewer than half of all patients referred as suspected inflammatory polyarthritis have a diagnosis of inflammatory polyarthritis. Other common diagnoses include nodal osteoarthritis, carpal tunnel syndrome, and chronic pain syndromes. Symptoms and signs of persistent synovitis include persistent (not resolving within 3 or 4 weeks) pain, swelling, heat, early morning stiffness lasting more than 30 minutes and often recurring after longer periods of rest, and loss of function of the affected joint. Rheumatoid Arthritis
Rheumatoid arthritis is an inflammatory disease largely affecting synovial joints. It typically affects the small joints of the hands and the feet, and usually both sides equally and symmetrically, although any synovial joint can be affected. It is a systemic disease and so can affect the whole body, including the heart, lungs and eyes. The incidence of the condition is low, with around 1.5 men and 3.6 women developing rheumatoid arthritis per 10,000 people per year. The overall occurrence of rheumatoid arthritis is 2 to 4 times greater in women than men. The peak age of incidence in the UK for both men and women is the 70s, but people of all ages can develop the disease. An average GP with a list of 2000 patients will see one person newly diagnosed with rheumatoid arthritis approximately every 2 years. About 70 per cent of people with rheumatoid arthritis are seropositive. Seronegative rheumatoid arthritis may have a better outlook. Peripheral spondyloarthritis
Peripheral spondyloarthritis presents with multiple joint inflammation, tendinitis and enthesitis. Consider additional risk factors such as pain in the finger or toe joints, enthesitis (inflammation where tendons or ligaments insert into the bone), dactylitis (inflammation of the whole finger or toe – ‘sausage digits’), uveitis, psoriasis including nail disease, recent genitourinary infection, or a family history of spondyloarthritis or psoriasis. The prevalence of spondyloarthritis is 0.8-1.7%. Psoriatic arthritis may manifest in a number of different patterns. These include
predominant involvement of small joints in the hands and feet, predominant large joint involvement, particularly in the knees, or combinations of these. Psoriatic arthritis may also involve the axial joints, and inflammation of the entheses and/or finger and toe joints. Skin and nail involvement may not be present at diagnosis and in its absence, a family history of psoriasis is required to meet the diagnostic criteria.
Enteropathic spondyloarthritis is associated with inflammatory bowel disease (Crohn's disease and ulcerative colitis)
Reactive arthritis, which can occur in people after gastrointestinal or genitourinary infections, including Campylobacter, Chlamydia, Salmonella, Shigella, or Yersinia.
Undifferentiated spondyloarthritis presents with an asymmetrical oligoarticular (fewer than 5 involved joints) arthritis, often involving the knees.

28 Triage Specification – September 2018 – MSk Pathways – Inflammation of Multiple Joints
Investigations from primary care
Antibody testing, and testing of inflammatory markers do not make or exclude the diagnosis. NICE recommends blood tests for rheumatoid factor in adults with suspected rheumatoid arthritis, and anti-CCP antibodies if negative for rheumatoid factor. X-rays of hands and feet recommended for suspected rheumatoid arthritis. Referrals
Inflammatory polyarthritis or suspected persistent synovitis of recent onset (see definition above) should be referred on clinical grounds within three working days of presentation. Referrals should not be delayed pending results. and NICE recommend assessment in a rheumatology service or early arthritis clinic within three weeks. Early diagnosis and treatment of rheumatoid arthritis prevents significant morbidity, and significantly reduces treatment costs. The evidence for early treatment of patients with symptoms of greater than two years is weaker. Patients with symptoms for more than two years should therefore be referred into general rheumatology clinics.
29 Triage Specification – September 2018 – MSk Pathways – Inflammation of Multiple Joints
Referral to General Practitioner
(Referral from triage, community or hospital services specifically for primary care medical review)
Inclusions
Assessment and management of multi-morbidity and psychiatric co-morbidity.
Medication reviews and non-urgent prescriptions. Note, for disease-modifying drugs and immunosuppressants initiated in secondary care, there must be an shared care protocol that has been agreed and accepted by both the primary and secondary care clinician responsible for an individual patient.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Discussion about fitness for work and sickness certification.
Management following discharge from community or secondary care where no further intervention planned.
Patients referred back from community services with known or suspected serious underlying pathology where non-urgent (for re-evaluation and possible referral to secondary care).
Exclusions
Patients seen in community or secondary care settings who need emergency or urgent assessment e.g. suspicion of inflammatory joint disease, peripheral vascular disease or fracture.
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
30 Triage Specification – September 2018 – MSk Pathways – Inflammation of Multiple Joints
Referral to Community Physiotherapy or First Contact Physiotherapy in Primary Care
Inclusions
Assessment and treatment of functional impairment.
Assessment of falls and provision of walking aids.
Improve general fitness and participation in regular physical activity.
Exercises for enhancing flexibility and muscle strength.
Exclusions
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Severe acute pain or inflammation.
Patient needs medical opinion.
31 Triage Specification – September 2018 – MSk Pathways – Inflammation of Multiple Joints
Referral to Rheumatology Interface Service
(May not be available in every CCG)
Inclusions
If rheumatological physiotherapy, hand therapy, occupational therapy, podiatry and psychology available:
Assessment and treatment of functional impairment.
Assessment of gait and stability, provision of orthotics.
Assessment and provision of splints and braces.
Advice and assessment about aids and adaptations to assist activities of daily living and promote independence.
Psychological interventions (for example, relaxation, stress management) and cognitive coping skills.
If rheumatology nurse or therapist with rheumatology training available:
Symptom and medication monitoring under shared care arrangement with primary and secondary care.
If rheumatologist or GP with a special interest available:
Diagnostic assessment and management advice. Patients particularly suited to community assessment are those with vague and undifferentiated symptoms where clinically there is a lower index of suspicion of inflammatory disease. (Patients clinically with a high index of suspicion should be referred to secondary care, unless a community service is specifically commissioned for this group of patients.).
Exclusions
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Severe acute pain or inflammation, unless service commissioned for acute assessment.
Patient needs medical opinion, unless a medical opinion commissioned.
32 Triage Specification – September 2018 – MSk Pathways – Inflammation of Multiple Joints
Referral to Secondary Care Rheumatology
Inclusions
Suspected inflammatory arthritis on clinical grounds. (See history and supporting tests in ‘background’ above). Negative or absent blood tests or X-rays should not delay referrals made on clinical grounds.
Flare-up of inflammatory arthritis. (See exclusions below where very urgent treatment may be needed).
(Decision aids for discussing disease modifying anti-rheumatic drugs and biologics are not required for referral into secondary care. A variety of decision aids may be used in secondary care):
o https://www.england.nhs.uk/rightcare/shared-decision-making/
o https://decisionaid.ohri.ca/AZsearch.php?criteria=arthritis
o https://musculoskeletal.cochrane.org/decision-aids
Any imaging performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral. Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
Do not delay referral on the grounds of normal blood tests.
Exclusions
Suspected clinical emergency e.g. sepsis, endocarditis. Refer to accident and emergency.
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Patient unable to manage at home due to severe symptoms. Discuss with rheumatology service in working hours; out of hours consider intermediate care assessment or other admission avoidance scheme, emergency admission or ambulatory care if critically unwell.
33 Triage Specification – September 2018 – MSk Pathways – Inflammation of One Joint
5.6. Inflammation of one joint
Background
The commonest new presentation of mild or moderate inflammation in a single joint in primary care is osteoarthritis. Differential diagnoses and incidence (new diagnoses or presentations) in primary care
• Osteoarthritis (Age >40 yrs: 1,290/100,000 men, 1,860/100,000 women)
• Gout, pseudogout (302/100,000 men, 72/100,000 women)
• Peripheral spondyloarthritis (60/100,000 men, 10/100,000 women)
• Septic arthritis (6/100,000 people)
• Bursitis, cellulitis, tenosynovitis
• Trauma
• Haemochromatosis
• Bony metastases
Osteoarthritis
Diagnose osteoarthritis clinically without investigations, after excluding alternative diagnoses (above) if a person:
1. Is aged 45 years or over, and
2. Activity-related joint pains, and
3. Has either no morning joint-related stiffness or morning stiffness that lasts no longer than 30 minutes.
Osteoarthritis of large joints may be associated with some warmth and an effusion in the joint. Be aware that atypical features, such as a history of trauma, prolonged morning joint-related stiffness, rapid worsening of symptoms or the presence of a hot swollen joint, may indicate alternative or additional diagnoses. Gout
Gout commonly initially presents with podagra (acute inflammation of the great toe MTP joint). Inflammation at this site is almost always caused by gout and can be diagnosed on clinical grounds. Patients who have her preceding history of episodes of podagra may later develop episodic or more persistent inflammation in other joints. Septic arthritis
Rarely infections can present with subacute pain and swelling in the joint (e.g. tuberculosis). Where diagnostic uncertainty exists aspiration and possibly a synovial biopsy are indicated. Such patients should be referred to secondary care. Patients with a short history of a hot, swollen and tender joint (or joints) with restriction of
movement and loss of function should be regarded as having septic arthritis until proven otherwise.
34 Triage Specification – September 2018 – MSk Pathways – Inflammation of One Joint
Referral to General Practitioner
(Referral from triage, community or hospital services specifically for primary care medical review)
Inclusions
Assessment and management of multi-morbidity and psychiatric co-morbidity.
Medication reviews and non-urgent prescriptions. Note, for disease-modifying drugs and immunosuppressants initiated in secondary care, there must be an shared care protocol that has been agreed and accepted by both the primary and secondary care clinician responsible for an individual patient.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Discussion about fitness for work and sickness certification
Management following discharge from community or secondary care where no further intervention planned.
Patients referred back from community services with known or suspected serious underlying pathology where non-urgent (for re-evaluation and possible referral to secondary care).
Exclusions
Patients seen in community or secondary care settings who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary malignancy, sudden inability to bear any weight, history of a fall, suspected fracture or dislocation.
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Patients seen in community or secondary care settings who need urgent specialist assessment e.g. severe pain unresponsive to analgesia and persistent loss of function.
35 Triage Specification – September 2018 – MSk Pathways – Inflammation of One Joint
Referral to Community Physiotherapy or First Contact Physiotherapy in Primary Care
Inclusions
Advice about the condition to aid shared decision-making, taking account of health literacy and patient beliefs.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Assessment and treatment of functional impairment.
Assessment of falls and provision of walking aids.
Assessment and provision of splints, orthotics and braces.
Advice and assessment about aids and adaptations to assist activities of daily living and promote independence.
Improve general fitness and participation in regular physical activity.
Exercises for enhancing flexibility and muscle strength.
Exclusions
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary malignancy, sudden inability to bear any weight, history of a fall, suspected fracture or dislocation.
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Patients who need urgent specialist assessment e.g. severe pain unresponsive to analgesia and persistent loss of function.
36 Triage Specification – September 2018 – MSk Pathways – Inflammation of One Joint
Referral to Musculoskeletal or Rheumatology Interface Service
(May not be available in every CCG)
Inclusions
Unsuccessful conservative treatment
Diagnostic uncertainty
Complex multidisciplinary assessments of function and activities of daily living.
Interface service to ensure PPwT thresholds met and authorisation obtained prior to referral to secondary care for consideration of surgery.
Interface service to ensure onward referral to secondary care is accompanied by any imaging required by the receiving consultant or unit.
Request for corticosteroid injection in patients with confirmed diagnosis.
If rheumatology nurse or therapist with rheumatology training available:
Symptom and medication monitoring under shared care arrangement with primary and secondary care.
If rheumatologist or GP with a special interest available:
Diagnostic assessment and management advice. Patients particularly suited to community rheumatology assessment are those with vague and undifferentiated symptoms where clinically there is a lower index of suspicion of inflammatory disease. (Patients clinically with a high index of suspicion should be referred to secondary care, unless a community service is specifically commissioned for this group of patients.)
If medical staff available:
Corticosteroid injection in anticoagulated patients with confirmed diagnosis.
Exclusions
Suspected septic arthritis; other emergency condition suspected.
Severe acute pain or inflammation, unless service commissioned for acute assessment.
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Patient needs medical opinion, unless a medical opinion commissioned.
Anticoagulated, if requiring injection (ESPs may not be able to inject joint under patient group direction) (Consider GP minor surgery scheme if available, or medical staff in interface service if commissioned).
37 Triage Specification – September 2018 – MSk Pathways – Inflammation of One Joint
Referral to Secondary Care Rheumatology
Inclusions
Suspected inflammatory arthritis on clinical grounds. (See history and supporting tests in ‘background’ above). Negative or absent blood tests or X-rays should not delay referrals made on clinical grounds.
Flare-up of inflammatory arthritis. (See exclusions below where very urgent treatment may be needed).
(Decision aids for discussing disease modifying anti-rheumatic drugs and biologics are not required for referral into secondary care. A variety of decision aids may be used in secondary care):
o https://www.england.nhs.uk/rightcare/shared-decision-making/
o https://decisionaid.ohri.ca/AZsearch.php?criteria=arthritis
o https://musculoskeletal.cochrane.org/decision-aids
Any imaging performed in primary or community care should be available on IEP/receiving
unit, and the reports forwarded with the referral. Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
Exclusions
Suspected clinical emergency e.g. sepsis, endocarditis. Refer to accident and emergency.
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Patient unable to manage at home due to severe symptoms. Discuss with rheumatology service in working hours; out of hours consider intermediate care assessment or other admission avoidance scheme, emergency admission or ambulatory care if critically unwell.
38 Triage Specification – September 2018 – MSk Pathways – Inflammation of One Joint
Referral to Secondary Care Orthopaedics
Inclusions
Unsuccessful conservative management.
Opinion regarding synovial biopsy (e.g. for diagnosis of pigmented villonodular synovitis, or following recommendation from consultant rheumatologist).
Patient prepared to have surgical intervention for joint replacement surgery or knee arthroscopy following a shared decision-making discussion guided by a decision aid tool:
o Osteoarthritis treatment options: http://www.decisionbox.ulaval.ca/fileadmin/documents/decisionbox/document/dbox.hip_knee_osteoarthritis.pdf
o Gout: https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=hw69011#aa25495
o Hip Replacement Surgery: https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=uh1515
o Knee arthroscopy: https://www.bmj.com/content/357/bmj.j1982
o Knee Replacement Surgery: https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=uh1514
Thresholds for surgery (NWL PPwT):
o Hip replacement https://www.hounslowccg.nhs.uk/media/70177/Hip-Replacement-v4.pdf
o Knee arthroscopy, not funded for osteoarthritis or as a primary diagnostic tool: https://www.hounslowccg.nhs.uk/media/70192/Knee-Arthroscopy-v4.pdf
o Knee replacement: https://www.hounslowccg.nhs.uk/media/70195/Knee-Replacement-v4.pdf
Any imaging (see hip and knee sections for prerequisites for surgery) performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral. Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
Exclusions
Suspected fracture, dislocation or septic arthritis. (Refer to on-call orthopaedic team or A&E).
Suspicion of inflammatory joint disease, peripheral vascular disease. (Discuss with on-call specialist, or refer to medical, rheumatology or vascular team, depending on clinical presentation and urgency).
Patients who have not been triaged or referred from a community musculoskeletal service (including non-urgent internally generated referrals (consultant to consultant referrals).
PPwT form has not been completed by referrer where request is for a procedure covered by the policy.
Referral is not accompanied by any pre-requisite imaging or investigations required by the consultant or unit.
39 Triage Specification – September 2018 – MSk Pathways – Inflammation of One Joint
Referral to Accident and Emergency/Ambulatory Care
Inclusions
Suspected infective or septic arthritis.
Imminent threat to life, limb or internal organ.
Other emergency condition suspected.
Exclusions
Non-emergency cases.
40 Triage Specification – September 2018 – MSk Pathways – Inflammation of the Spine
5.7. Inflammation of the spine
Background
Ankylosing spondylitis and axial spondyloarthropathy are found in around 0.3-1.2% of the population. Spondyloarthritis encompasses a group of inflammatory conditions with some shared features, including extra-articular manifestations. Both peripheral and axial joints can be affected. The spondyloarthritides are distinct from rheumatoid arthritis but are as important to recognise and manage early in their presentation to improve health outcomes. Most people with these conditions have either psoriatic arthritis or axial spondyloarthritis, which includes ankylosing spondylitis. Ankylosing spondylitis and non-radiographic axial spondyloarthritis primarily affect the spine, in particular the sacroiliac joint. Both conditions present in similar ways; the primary classification difference is whether sacroiliitis is detectable on X-ray. Contrary to common misconceptions, axial spondyloarthritis affects similar numbers of women and men, is not always apparent on plain X-ray, and occurs in people who are seronegative for human leucocyte antigen B27 (HLA-B27). No single test has been shown to have sufficient sensitivity or specificity to diagnose or rule out spondyloarthritis. HLA-B27 is found in 75% of people with axial spondyloarthritis and up to 20% of asymptomatic people, and varies with ethnicity. Imaging is only recommended in specialist (community or hospital) settings. Do not delay referral on the grounds of normal blood tests.
Diagnosis: history and examination
The diagnosis is frequently made late. Suspect in a person who has had low back pain that started before the age of 45 years and has lasted for longer than 3 months, with:
• 4 or more of the additional criteria below or
• Exactly 3 of the additional criteria below and a positive HLA-B27 test (performed from primary or community care).
Consider additional risk factors such as pain in the finger or toe joints, enthesitis (inflammation where tendons or ligaments insert into the bone), dactylitis (inflammation of the whole finger or toe – ‘sausage digits’), uveitis, psoriasis including nail disease, recent genitourinary infection, or a family history of spondyloarthritis or psoriasis. If two or fewer criteria are present, then the GP should reassess if new symptoms, signs or risk factors emerge.
Additional criteria are: • Low back pain that started before the age of 35 years (this further increases the likelihood
that back pain is due to spondyloarthritis compared with low back pain that started between 35 and 44 years)
• Waking during the second half of the night because of symptoms • Buttock pain • Improvement with movement • Improvement within 48 hours of taking non-steroidal anti-inflammatory drugs (NSAIDs) • A first-degree relative with spondyloarthritis • Current or past arthritis • Current or past enthesitis • Current or past psoriasis.
Complete an examination, particularly looking for loss of spinal movements in at least two planes and a positive Schober’s test (a test for restricted lumbar flexion) that might support a diagnosis of axial spondyloarthritis.
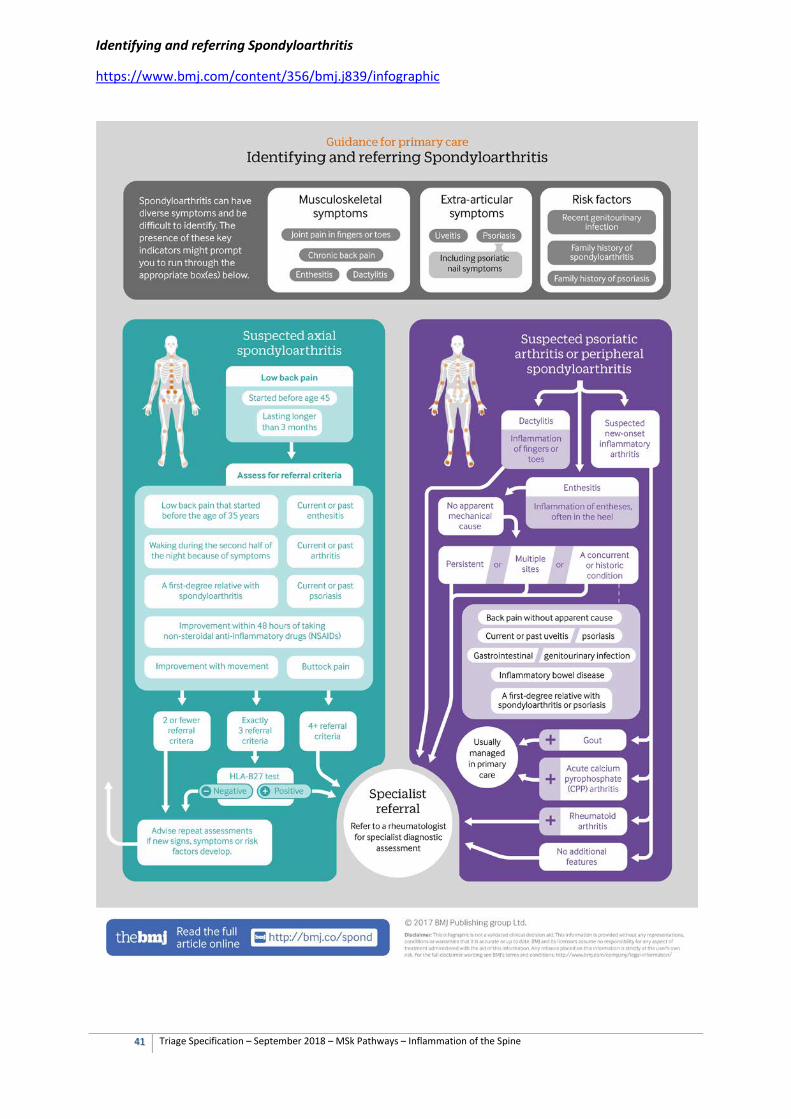
41 Triage Specification – September 2018 – MSk Pathways – Inflammation of the Spine
Identifying and referring Spondyloarthritis
https://www.bmj.com/content/356/bmj.j839/infographic
42 Triage Specification – September 2018 – MSk Pathways – Inflammation of the Spine
Referral to the General Practitioner
(Referral from triage, community, or hospital services specifically for primary care medical review)
Inclusions
Assessment and management of multi-morbidity and psychiatric co-morbidity.
Medication reviews and non-urgent prescriptions. Note, for disease-modifying drugs and immunosuppressants initiated in secondary care, there must be an shared care protocol that has been agreed and accepted by both the primary and secondary care clinician responsible for an individual patient.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Discussion about fitness for work and sickness certification.
Management following discharge from community or secondary care where no further intervention planned.
Patients referred back from community services with known or suspected serious underlying pathology where non-urgent (for re-evaluation and possible referral to secondary care).
Exclusions
Patients seen in community or secondary care settings who need emergency or urgent assessment e.g. suspicion of inflammatory joint disease, peripheral vascular disease or fracture.
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Neurological involvement, where investigations, injections or surgery are planned.
43 Triage Specification – September 2018 – MSk Pathways – Inflammation of the Spine
Referral to Community Physiotherapy or First Contact Physiotherapist in Primary Care
Inclusions
Assessment and treatment of functional impairment.
Assessment for exercises for people with axial spondyloarthritis:
o Stretching, strengthening and postural exercises.
o deep breathing exercises.
o Spinal extension exercises
o Range of motion exercises for the lumbar, thoracic and cervical sections of the spine
o Aerobic exercise.
If hydrotherapy available:
Consider hydrotherapy as an adjunctive therapy to manage pain and maintain or improve function for people with axial spondyloarthritis.
Exclusions
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Severe acute pain or inflammation.
Patient needs medical opinion.
Diagnostic uncertainty about spondyloarthritis
44 Triage Specification – September 2018 – MSk Pathways – Inflammation of the Spine
Referral to Musculoskeletal or Rheumatology Interface
(May not be available in every CCG)
Inclusions
If rheumatological physiotherapy, hand therapy, occupational therapy, podiatry and psychology available for people with spondyloarthritis:
Assessment and treatment of functional impairment.
Assessment of gait and stability, provision of orthotics.
Assessment of activities of daily living
Advice to assist activities of daily living and promote independence.
Psychological interventions (for example, relaxation, stress management) and cognitive coping skills.
If rheumatology nurse or therapist with rheumatology training available:
Symptom and medication monitoring under shared care arrangement with primary and secondary care.
If rheumatologist or GP with a special interest available:
Diagnostic assessment and management advice. Patients particularly suited to community assessment are those with vague and undifferentiated symptoms where clinically there is a lower index of suspicion of inflammatory disease. (Patients clinically with a high index of suspicion should be referred to secondary care, unless a community service is specifically commissioned for this group of patients.).
Exclusions
Suspected infective or neoplastic pathology.
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Severe acute pain or inflammation, unless service commissioned for acute assessment.
Patient needs medical opinion, unless a medical opinion commissioned.
45 Triage Specification – September 2018 – MSk Pathways – Inflammation of the Spine
Referral to Secondary Care Rheumatology
Inclusions
Investigation and management of spinal inflammation. Suspect spondyloarthritis in a person who has had low back pain that started before the age of 45 years and has lasted for longer than 3 months, with:
o Four or more of the additional criteria below or o Exactly three of the additional criteria below and a positive HLA-B27 test (performed
from primary or community care).
Consider additional risk factors: small joint pains, enthesitis, dactylitis, uveitis, psoriasis including nail disease, recent genitourinary infection, or a family history of spondyloarthritis or psoriasis. If two or fewer criteria are present, then the GP should reassess if new symptoms, signs or risk factors emerge.
Additional criteria are: o Low back pain that started before the age of 35 years (this further increases the
likelihood that back pain is due to spondyloarthritis compared with low back pain that started between 35 and 44 years)
o Waking during the second half of the night because of symptoms o Buttock pain o Improvement with movement o Improvement within 48 hours of taking non-steroidal anti-inflammatory drugs
(NSAIDs) o A first-degree relative with spondyloarthritis o Current or past arthritis o Current or past enthesitis o Current or past psoriasis.
Diagnostic uncertainty, particularly in patients clinically with a high index of suspicion, unless a community service is specifically commissioned for this group of patients.
Flare-up of inflammatory arthritis. (See exclusions below where very urgent treatment may be needed).
Any imaging performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral. Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
Do not delay referral on the grounds of normal blood tests.
(Decision aids for discussing disease modifying anti-rheumatic drugs and biologics are not required for referral into secondary care. A variety of decision aids may be used in secondary care):
o https://www.england.nhs.uk/rightcare/shared-decision-making/ o https://decisionaid.ohri.ca/AZsearch.php?criteria=arthritis o https://musculoskeletal.cochrane.org/decision-aids
Exclusions
Suspected infective or neoplastic pathology.
Patient unable to manage at home due to severe symptoms. Discuss with rheumatology service in working hours; out of hours consider intermediate care assessment or other admission avoidance scheme, emergency admission or ambulatory care if critically unwell.
Neurological involvement (Refer to musculoskeletal interface clinic unless requires urgent surgical decompression. See low back pain and sciatica pathway.)
46 Triage Specification – September 2018 – MSk Pathways – Knee pain
5.8. Knee Pain
Background
The prevalence of knee pain with disability in primary care is 6%, and the prevalence of moderate or severe knee pain is 12%. The rates are higher in older people, and higher in women than men, at all ages. 3% of patients consult their GPs annually for knee pain. In older people, knee problems are most commonly due to osteoarthritis, with a prevalence in women over 75 yrs of 36% and men over 75 yrs of 27%. Risk factors for knee pain include: increasing age, overweight and obesity, social deprivation, South Asian ethnicity, previous knee injury, knee-straining work and participation in sport involving torsion or high level of impact. Causes of knee pain by age group (n.b. can overlap)
<18 years Patellofemoral pain, Osgood-Schlatter's disease, referred pain from hip (e.g.. slipped capital femoral epiphysis), joint hypermobility syndrome, growing pains, patellar subluxation/instability, osteochondritis dissecans, septic arthritis, tumours, patellar tendonitis, bipartite patella, Henoch-Schonlein purpura
18-50 years Patellofemoral pain (usually young adults), trauma (cruciate and collateral ligament sprains, meniscal tears), joint hypermobility syndrome, bursitis, inflammatory arthritis, septic arthritis, early osteoarthritis (previous injury), plicae, iliotibial band syndrome
>50 years Osteoarthritis, gout and pseudogout, Baker's cyst, referred pain from osteoarthritis of hip and lumbosacral spine, degenerative meniscal tear, septic arthritis, secondary tumours
Clinical history
Mechanism of trauma, uni- or bilateral involvement, night or rest pain, swelling (time course), locking, gelling, giving way, previous injuries, surgery or medical conditions, extra-articular features. Diagnose osteoarthritis clinically without investigations, after excluding alternative diagnoses (above) if a person:
1. Is aged 45 years or over, and
2. Activity-related joint pains, and
3. Has either no morning joint-related stiffness or morning stiffness that lasts no longer than 30 minutes.
• Functional impairment such as difficulty walking, climbing stairs, dressing or driving.
• Psychosocial impact: may affect self-confidence, self-esteem, sleep quality, relationships and ability to self-care and care for others; may cause anxiety and depression
Examination
• Inspection, Palpation, Range of motion
• Ligament and meniscal tests, Gait and stability
• Adjacent joints and spine
• Systemic examination
47 Triage Specification – September 2018 – MSk Pathways – Knee pain
Referral to General Practitioner
(Referral from triage, community or hospital services specifically for primary care medical review)
Inclusions
Assessment and management of multi-morbidity and psychiatric co-morbidity.
Medication reviews and non-urgent prescriptions.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Discussion about fitness for work and sickness certification
Management following discharge from community or secondary care where no further intervention planned
Patients referred back from community services with known or suspected serious underlying pathology where non-urgent (for re-evaluation and possible referral to secondary care).
Exclusions
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to bear any weight, suspected fracture or dislocation, suspected quadriceps or patella tendon rupture, severe soft tissue injury with gross instability, neurovascular damage following trauma, compartment syndrome, acute (<2 wks) and persistently ‘true’ locked knee (defined as loss of normal extension only).
Patients seen in community or secondary care settings who need urgent specialist assessment e.g. severe pain unresponsive to analgesia and persistent loss of function.
48 Triage Specification – September 2018 – MSk Pathways – Knee pain
Referral to Community Physiotherapy or First Contact Physiotherapy in Primary Care
Inclusions
Advice about the knee pain to aid shared decision-making, taking account of health literacy and patient beliefs.
o Acute or chronic knee pain.
o Suspected or known osteoarthritis.
o Anterior knee pain, including where suspected arising from the patellofemoral joint.
o Soft tissue injuries including suspicion of meniscal tears, ligament injuries or tendinopathies.
o History or clinical examination of knee instability.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Assessment and treatment of functional impairment.
Assessment of falls and provision of walking aids.
Assessment of gait and stability, and provision of orthotics and braces.
Advice and assessment about aids and adaptations to assist activities of daily living and promote independence.
Improve general fitness and participation in regular physical activity.
• Exercises for enhancing flexibility and muscle strength.
If post-operative physiotherapy commissioned:
Post-operative physiotherapy
Exclusions
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to bear any weight, suspected fracture or dislocation, suspected quadriceps or patella tendon rupture, severe soft tissue injury with gross instability, neurovascular damage following trauma, compartment syndrome, acute (<2 wks) and persistently ‘true’ locked knee (defined as loss of normal extension only).
Suspected inflammatory arthritis, unless rheumatological assessment commissioned.
Patients who need urgent specialist assessment e.g. severe pain unresponsive to analgesia and persistent loss of function.
Community physiotherapy only exclusions
Presented with same condition within previous 12 months, and there was no substantive improvement with treatment previously, and if no other community treatment options are appropriate (e.g. pain service, where commissioned).
Patients with frailty and high risk of falls, where a falls service is commissioned.
Co-morbidities that significantly impair a particular patient’s ability to exercise. For example neurological (e.g. stroke), severe cardiac, renal, liver or respiratory failure, recurrent disabling hypoglycaemia or poorly controlled epilepsy.
49 Triage Specification – September 2018 – MSk Pathways – Knee pain
Referral to Musculoskeletal Interface Service
(May not be available in every CCG)
Inclusions
• Unsuccessful conservative treatment (exercises, self-management strategies, physiotherapy, analgesia and steroid injection – if available.)
o Including suspected meniscal tears, intermittent locking, ligament pathologies, instability, tendinopathies and anterior knee pain
• Steroid injection, where clinically indicated (e.g. acute flare of osteoarthritis, non-septic effusion, bursitis), if GP has not already administered.
• Diagnostic uncertainty.
• Interface service to ensure PPwT thresholds met and authorisation obtained prior to referral to secondary care for consideration of surgery.
• Interface service to ensure onward referral to secondary care is accompanied by any imaging required by the receiving consultant or unit.
If medical staff available:
• Corticosteroid injection in anticoagulated patients with confirmed diagnosis.
Exclusions
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to bear any weight, suspected fracture or dislocation, suspected quadriceps or patella tendon rupture, severe soft tissue injury with gross instability, neurovascular damage following trauma, compartment syndrome, acute (<2 wks) and persistently ‘true’ locked knee (defined as loss of normal extension only). These patients will be referred back to GP for urgent assessment (same day), or to A&E as clinically appropriate.
Suspected inflammatory arthritis, unless rheumatological assessment commissioned.
Patients who need urgent specialist assessment e.g. severe pain unresponsive to analgesia and persistent loss of function.
Anticoagulated, if requiring injection (ESPs may not be able to inject joint under patient group direction) (Consider GP minor surgery scheme if available, or medical staff in interface service if commissioned).
50 Triage Specification – September 2018 – MSk Pathways – Knee pain
Referral to Secondary Care Orthopaedics
Inclusions
Unsuccessful conservative management.
Diagnostic uncertainty.
Patient prepared to have surgical intervention following a shared decision making discussion guided by a decision aid tool:
o All treatment options: http://www.decisionbox.ulaval.ca/fileadmin/documents/decisionbox/document/dbox.hip_knee_osteoarthritis.pdf http://www.valeofyorkccg.nhs.uk/rss/data/uploads/shared-decision-making/sdm-osteoarthritis-of-the-knee.pdf
o Surgery: Knee Replacement https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=uh1514
o Surgery: Meniscal Tear https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=te7366
o Surgery: Degenerative Meniscal Tear https://www.bmj.com/content/357/bmj.j1982
o Surgery: ACL Injury https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=aa54360
Thresholds for knee arthroscopy (NWL PPwT version 4) https://www.hounslowccg.nhs.uk/news,-publications-and-policies/publications.aspx?n=2010:
o Referral for knee arthroscopy should be considered only in the following situations: Removal of loose body A clear history of mechanical locking in a patient with osteoarthritis. Meniscal surgery (repair or resection) Ligament reconstruction/ repair (including lateral release) Synovectomy or synovial biopsy Suspected chondral lesion
o Use of knee arthroscopy as a diagnostic tool will only be funded in the following situations: Patients with medial knee pain where the Plica syndrome is suspected. When Chondromalacia patellae is suspected
o Arthroscopy will not be funded for the following indications: As part of treatment for osteoarthritis. Use of knee arthroscopy as a primary diagnostic tool
o Patients who smoke should have attempted to stop smoking 8 to 12 weeks before referral to reduce the risk of surgery and the risk of post-surgery complications. Patients should be routinely offered referral to smoking cessation services to reduce these surgical risks.
51 Triage Specification – September 2018 – MSk Pathways – Knee pain
Thresholds for knee replacement (NWL PPwT version 4) https://www.hounslowccg.nhs.uk/news,-publications-and-policies/publications.aspx?n=2010:
o Funding for total or partial knee replacement surgery is available if the following criteria are met: 1. Patient complains of moderate joint pain AND moderate to severe functional
limitations that has a substantial impact on quality of life, despite the use of non-surgical treatments such as adequate doses of NSAID analgesia, weight control treatments and physical therapies AND
2a. Has radiological features of severe disease OR 2b. Has radiological features of moderate disease with limited mobility or instability
of the knee joint o Patients not meeting the above criteria can be referred via the IFR route where
there are exceptional circumstances present. o Patients who smoke should have attempted to stop smoking 8 to 12 weeks before
referral to reduce the risk of surgery and the risk of post-surgery complications. Patients should be routinely offered referral to smoking cessation services to reduce these surgical risks.
Any imaging performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral:
o Knee anteroposterior (AP), lateral views, Rosenberg weight bearing and skyline views for consideration of joint replacement surgery.
o Knee MRI for consideration of meniscal or ligament injury.
Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
Exclusions
Suspected fracture, dislocation, septic arthritis, severe acute trauma, compartment syndrome, acute neurovascular trauma, malignancy, acute (<2 wks) and persistently ‘true’ locked knee (defined as loss of normal extension only). (Refer to on-call orthopaedic team or A&E).
Suspicion of inflammatory joint disease, peripheral vascular disease. (Discuss with on-call specialist, or refer to medical, rheumatology or vascular team, depending on clinical presentation and urgency).
Patients who have not been triaged or referred from a community musculoskeletal service (including non-urgent internally generated referrals (consultant to consultant referrals).
Conservative management and self-management strategies are clinically appropriate but have not been tried.
PPwT form has not been completed by referrer where request is for a procedure covered by the policy.
Referral is not accompanied by any pre-requisite imaging or investigations required by the PPwT policy, consultant or unit.
52 Triage Specification – September 2018 – MSk Pathways – Low Back Pain and Sciatica
5.9. Low Back Pain and Sciatica
Background
Low back pain and sciatica are recurrent conditions. 11% of men and 16% of women have chronic low back pain, and 30% of people still have clinically significant symptoms after a year after onset of sciatica. Back pain accounts for 7% of GP consultations and results in the loss of 4.1 million working days a year. Most patients seen in primary care do not have serious underlying pathology. The NICE guideline (NG59, 2016) advises clinicians to assess the clinical likelihood of serious underlying pathology at every review, and refer for appropriate investigation and management (see infographic https://www.bmj.com/content/356/bmj.i6748/infographic). In some cases it may be appropriate to investigate and manage in primary care e.g. patients in last phase of life. Causes of Low Back Pain in Primary Care
Low back pain without serious underlying pathology 85% Compression fractures 4% Tumour 1% Prolapsed intervertebral disc 1-3% Ankylosing spondylitis, Spinal infections, Intra-abdominal pathology < 1% each
Less than 1% of patients presenting in primary care will require surgery or injections. NICE does not recommend surgery or injections for back pain in the absence of structural pathology or nerve root involvement. Acupuncture is decommissioned in community and hospital care in NW London. Definitions
Low back pain that is not associated with serious or potentially serious causes has been described in the literature as 'non-specific', 'mechanical', 'musculoskeletal' or 'simple' low back pain. For consistency, NICE used the term 'low back pain' throughout the guideline. Specific causes of low back pain include sciatica, vertebral fracture, intra-abdominal pathologies, and more rarely, ankylosing spondylitis, cancer, and infection. NICE used 'sciatica' to describe leg pain secondary to lumbosacral nerve root pathology rather than the terms 'radicular pain' or 'radiculopathy', although they are more accurate. This is because 'sciatica' is a term that patients and clinicians understand, and it is widely used in the literature to describe neuropathic leg pain secondary to compressive spinal pathology. Serious underlying pathology
• Most single features in the history have poor predictive accuracy for serious underlying pathology.
• Single features that should raise suspicion o Cancer that can metastasise to bone (lung, breast, thyroid, kidney, prostate,
myeloma). o Trauma that could cause a fracture. o Sphincter disturbance or perianal loss of sensation.
• Look at the whole clinical picture, considering additional past history and examination findings.
• Further investigation and referral are indicated if strong suspicion of serious underlying pathology.
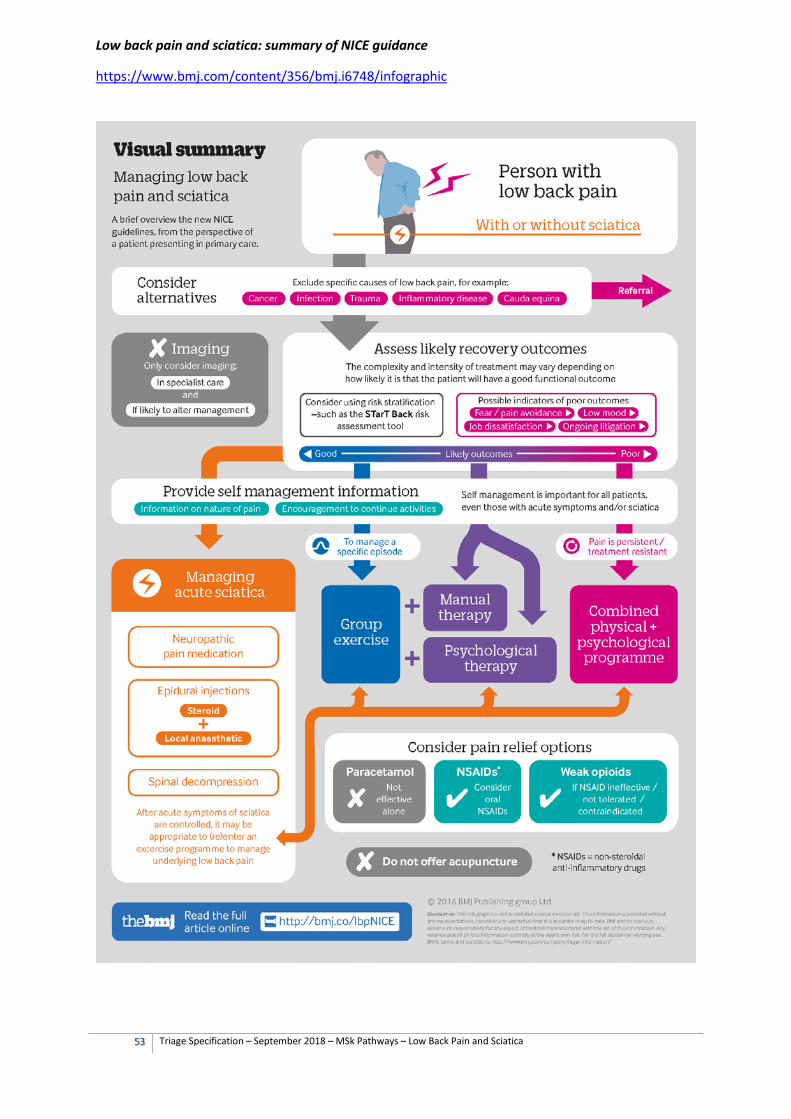
53 Triage Specification – September 2018 – MSk Pathways – Low Back Pain and Sciatica
Low back pain and sciatica: summary of NICE guidance
https://www.bmj.com/content/356/bmj.i6748/infographic
54 Triage Specification – September 2018 – MSk Pathways – Low Back Pain and Sciatica
Referral to General Practitioner
(Referral from triage, community or hospital services specifically for primary care medical review)
Inclusions
Assessment and management of multi-morbidity and psychiatric co-morbidity.
Medication reviews and non-urgent prescriptions. Note, for disease-modifying drugs and immunosuppressants initiated in secondary care for spondyloarthritis, there must be an shared care protocol that has been agreed and accepted by both the primary and secondary care clinician responsible for an individual patient.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Discussion about fitness for work and sickness certification.
Management following discharge from community or secondary care where no further intervention planned.
Patients referred back from community services with known or suspected serious underlying pathology where non-urgent (for re-evaluation and possible referral to secondary care).
Exclusions
Patients seen in community or secondary care settings who need emergency or urgent assessment e.g. suspected cauda equina syndrome, metastatic spinal cord compression, serious trauma
Imaging for low back pain and sciatica except where there is no community musculoskeletal service commissioned or for investigation of serious underlying pathology where hospital assessment is not clinically indicated (e.g. X-ray for suspected osteoporotic vertebral fractures)
55 Triage Specification – September 2018 – MSk Pathways – Low Back Pain and Sciatica
Referral to Community Physiotherapy or First Contact Physiotherapy in Primary Care
Inclusions
Acute episode of low back pain or acute exacerbation (less than 3 months) of chronic low back pain. As a guide, consider a threshold for referral of less than 70% recovery after 2wks of supported self-management
Recurrent low back pain where onset of less than 3 months for this episode AND the patient improved by more than 50% following previous physiotherapy AND where the improvement lasted more than 6 months
Exclusions
Reasonable clinical suspicion of serious underlying pathology (red flags) including cancer, infection, trauma, severe and progressive neurology e.g. cauda equina syndrome. These patients will be referred back to GP for urgent assessment (same day).
Very severe nerve root pain (e.g. where may need epidural for pain control and patient willing to consider a spinal injection, refer to interface service) unless in rehab phase (see NICE pathway https://www.bmj.com/content/356/bmj.i6748/infographic).
Not been offered self-management advice, where clinically appropriate.
A validated decision tool (e.g. STarT Back) or clinical assessment suggests the person is at high risk of poor functional outcome due to psychological and social factors, and a musculoskeletal interface service or community pain service has been commissioned. Psychosocial risk factors for poor functional outcome:
o Psychological factors low mood and anxiety. strong belief that pain is harmful coupled with a fear of movement. presenting with physical manifestations of psychological distress and life-
trauma.
o Social factors financial uncertainty. ongoing litigation and compensation claims.
Community physiotherapy only exclusions
Presented with same condition within previous 12 months, and there was no substantive improvement with treatment previously, and if no other community treatment options are appropriate (e.g. pain service, where commissioned).
Chronic widespread pain or inflammatory disorder (refer to rheumatology interface service if commissioned), unless a specialist service has identified a specific functional goal for physiotherapy (e.g. improving gait, improving balance and reducing falls, occupational rehabilitation).
Patients with neurological problems including Stroke, MND, Parkinson’s disease and multiple sclerosis, where a neurological rehabilitation service is commissioned.
Patients with frailty and high risk of falls, where a falls service is commissioned.
Co-morbidities that significantly impair a particular patient’s ability to exercise. For example neurological (e.g. stroke), severe cardiac, renal, liver or respiratory failure, recurrent disabling hypoglycaemia or poorly controlled epilepsy.
56 Triage Specification – September 2018 – MSk Pathways – Low Back Pain and Sciatica
Referral to Musculoskeletal Interface Service
(May not be available in every CCG)
Inclusions
Low back pain and sciatica with lack of persistent benefit from exercise and manual therapies.
Patients at high risk of poor functional outcome e.g. due to psychological and social factors (unless a community pain service offering a combined physical and psychological approach has been commissioned for these patients).
Severe nerve root pain where the person is prepared to consider injections or surgery (check previous discharge letters for suitability).
Structural pathology suspected or known, not requiring urgent evaluation (e.g. spondylolisthesis with back or leg pain, symptomatic scoliosis).
Patient prepared to have an MRI (only where clinically indicated) following a shared decision making discussion guided by a decision aid tool:
o MRI for low back pain: https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=aa6410
Evaluation for referral for consideration of diagnostic blocks for radio frequency denervation (as per NICE NG59 https://pathways.nice.org.uk/pathways/low-back-pain-and-sciatica):
o Non-surgical treatment has not worked for them (including pain management programmes) and
o The main source of pain is thought to come from structures supplied by the medial branch nerve(s) and
o They have moderate or severe levels of localised back pain (rated as 5 or more on a visual analogue scale, or equivalent) at the time of referral.
If musculoskeletal physician services commissioned
Acute sciatica of less than 3 months duration for consideration of an epidural (where patient prepared to consider spinal injections), where covered by the NW London CCGs Low Back Pain and Sciatica Policy (https://www.hounslowccg.nhs.uk/news,-publications-and-policies/publications.aspx?n=2010)
Assessment of undiagnosed pain, multi-morbidity and psychiatric co-morbidity.
Advice on pharmacological management.
Advice on diagnosis and management of osteoporosis and fragility fractures.
Exclusions
Reasonable clinical suspicion of serious underlying pathology (red flags) including cancer, infection, trauma, severe and progressive neurology e.g. cauda equina syndrome. These patients will be referred back to GP for urgent assessment (same day), or to A&E as clinically appropriate.
Fractures, including osteoporotic fractures, unless the patient has been reviewed by a doctor (e.g. orthopaedic surgeon, musculoskeletal physician) and cleared for community treatment – see above.

57 Triage Specification – September 2018 – MSk Pathways – Low Back Pain and Sciatica
Spondyloarthritis (refer to rheumatology interface service if commissioned), unless a specialist service has identified a specific functional goal for physiotherapy (e.g. improving gait, improving balance and reducing falls, occupational rehabilitation).
Patients with neurological problems including Stroke, MND, Parkinson’s disease and multiple sclerosis, where a neurological rehabilitation service is commissioned.
Patients with frailty and high risk of falls, where a falls service is commissioned.
58 Triage Specification – September 2018 – MSk Pathways – Low Back Pain and Sciatica
Referral to Secondary Care Spinal Orthopaedic or Neurosurgery Service
Inclusions
Investigation and management where reasonable clinical suspicion of serious underlying pathology requiring urgent assessment (within 2 weeks).
Diagnostic uncertainty (particularly in the presence of structural pathology, and where a trial of conservative management has been unsuccessful or is not clinically indicated).
Consideration of spinal decompression for nerve root pain, canal stenosis, benign and malignant tumours.
Consideration of other procedures covered by NICE Interventional Procedures guidance where appropriate and cost-effective for use within the NHS for this person. (Review the old notes first).
Consideration of vertebroplasty (n.b. limited evidence).
Consideration of surgery for symptomatic structural pathology (e.g. spondylolisthesis).
Patient prepared to have surgical intervention following a shared decision making discussion guided by a decision aid tool:
o Surgery: Prolapsed Lumbar Disc https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=aa6282
o Surgery: Lumbar Spinal Stenosis: https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=aa121240
Any imaging (including MRI spine) performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral. Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
Exclusions
Suspected metastatic cord compression, cauda equina syndrome, fracture or septic arthritis. (Refer to on-call neurosurgical or orthopaedic teams, or A&E).
Suspicion of peripheral vascular disease (e.g. aortic aneurysm, limb ischaemia). (Discuss with on-call vascular team).
Acute sciatica where conservative management, neuropathic agents or steroid epidurals are clinically appropriate but have not been tried. (Refer to MSk Interface service, where commissioned, or pain service for consideration of epidural).
Suspected spondyloarthritis. (See ‘Inflammation of the Spine’ above).
Patients who have not been triaged or referred from a community musculoskeletal service (including non-urgent internally generated referrals (consultant to consultant referrals).
Exercise and manual therapies have not been tried where clinically appropriate.
PPwT form has not been completed by referrer where request is for a procedure covered by the policy.
Referral is not accompanied by any pre-requisite imaging or investigations required by the PPwT policy, consultant or unit.
Referral for acupuncture. (See NWL PPwT v4 https://www.hounslowccg.nhs.uk/news,-publications-and-policies/publications.aspx?n=2010)
59 Triage Specification – September 2018 – MSk Pathways – Low Back Pain and Sciatica
Referral to Community Pain Service offering a combined physical and psychological approach
(May not be available in every CCG)
Inclusions
High risk of poor functional outcome or high levels of distress e.g. due to psychological and social factors where single modality treatments have been ineffective or not clinically appropriate.
Low back pain, with or without sciatica, or widespread chronic pain where non-invasive treatments have not had at least a 30% improvement in pain or function, lasting at least 3-6 months beyond the end of treatment, and where previous assessment suggests that invasive treatments (injections, surgery) are not appropriate.
Any imaging performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral. Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
If medical support available
Step down from strong opioids and other pain medications in conjunction with support from a combined physical and psychological approach, where appropriate for a community setting.
Exclusions
Reasonable clinical suspicion of serious underlying pathology (red flags) including cancer, infection, trauma, severe and progressive neurology e.g. cauda equina syndrome. These patients will be referred back to GP for urgent assessment (same day), or to A&E as clinically appropriate.
Spondyloarthritis (refer to rheumatology interface service if commissioned), unless a specialist service has identified that a pain management approach should be considered.
Patient does not accept a combined approach including a psychological approach to pain management.
60 Triage Specification – September 2018 – MSk Pathways – Low Back Pain and Sciatica
Referral to Secondary Care Pain Service
Inclusions
Acute sciatica of less than 3 months duration for consideration of an epidural (where patient prepared to consider spinal injections), where covered by the NW London CCGs Low Back Pain and Sciatica Policy.
Assessment of undiagnosed pain, multi-morbidity and psychiatric co-morbidity, where a positive diagnosis has not been made in a primary or community care setting, or where the diagnosis is in doubt.
Low back pain, with or without sciatica, or widespread chronic pain where community-based non-invasive treatments have not had at least a 30% improvement in pain or function, lasting at least 3-6 months beyond the end of treatment, and where the person is prepared to consider either a hospital-based physical and psychological approach, or injections (where covered by the NW London CCGs Low Back Pain and Sciatica Policy, above.
Consideration of other procedures covered by NICE Interventional Procedures guidance where appropriate and cost-effective for use within the NHS for this person. (Review the old notes first).
Low back pain, with or without sciatica, or widespread chronic pain for advice on pharmacological management, including stepping down medication where this cannot be managed in primary care.
Patient prepared to have intervention following a shared decision making discussion guided by a decision aid tool:
o Epidural Injections: https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=abk1059
Thresholds for imaging, injections and surgery for low back pain and sciatica (NWL PPwT version 4) https://www.hounslowccg.nhs.uk/news,-publications-and-policies/publications.aspx?n=2010 and FAQ: https://www.hounslowccg.nhs.uk/news,-publications-and-policies/publications.aspx?n=6024
1. NWL CCGs do NOT commission the following for low back pain and non-radicular spinal pain: a. Facet joint injections b. Therapeutic medial branch blocks c. Intradiscal therapy d. Prolotherapy e. Trigger point injections with any agent, including botulinum toxin f. Epidural steroid injections for chronic low back pain or for neurogenic
claudication inpatients with central spinal canal stenosis g. Any other spinal injections not specifically covered above
2. NWL CCGs fund epidurals (local anaesthetic and steroid) only in patients who have less than three months history of acute and severe lumbar radiculopathy at time of referral.
3. NWL CCGs will NOT fund Spinal fusion or lumbar disc replacement for low back pain. Surgical procedures for specific causes of LBP e.g. spondylolisthesis, scoliosis or severe structural disease are routinely funded where clinical indicated.
4. NWL CCGs recommend that imaging should not routinely be offered in a non-specialist setting for people with low back pain with or without sciatica.
61 Triage Specification – September 2018 – MSk Pathways – Low Back Pain and Sciatica
Thresholds for radiofrequency denervation for low back pain (NWL PPwT version 4) https://www.hounslowccg.nhs.uk/news,-publications-and-policies/publications.aspx?n=2010 and FAQ: https://www.hounslowccg.nhs.uk/news,-publications-and-policies/publications.aspx?n=6024
o NWL CCGs fund radiofrequency denervation for chronic low back pain when:
1. The patient has tried and exhausted all the conservative treatments / non-surgical management of the chronic low back pain (see clinical pathway in NICE Clinical Guidance 59) AND
2. The patient has moderate or severe levels of localised back pain graded as 5 or more on a zero to 10 visual analogue scale, or equivalent at the time of assessment AND
3. A diagnostic medial branch block has provided at least 80% improvement in pain on a zero to 10 on a visual analogue pain scale or equivalent.
Any imaging (including MRI spine) performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral. Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
Exclusions
Reasonable clinical suspicion of undiagnosed serious underlying pathology (red flags) including cancer, infection, trauma, severe and progressive neurology e.g. cauda equina syndrome. These patients will be referred back to GP for urgent assessment (same day), or to A&E as clinically appropriate. (Patients with a confirmed diagnosis and who have been medically assessed as appropriate for hospital pain clinic may be referred).
Suspicion of peripheral vascular disease (e.g. aortic aneurysm, limb ischaemia). (Discuss with on-call vascular team).
Suspected spondyloarthritis. (See ‘Inflammation of the Spine’ above).
Patients who have not been triaged or referred from a community musculoskeletal service (including non-urgent internally generated referrals (consultant to consultant referrals).
Exercise and manual therapies have not been tried where clinically appropriate.
A previous discharge plan has advised that no further treatments would be helpful in the pain clinic, and there is no substantive change in the clinical presentation, and there are no medication issues that could be managed in primary care (e.g. where the GP and patient do not need specialist support to step down ineffective or harmful medication).
PPwT form has not been completed by referrer where request is for a procedure covered by the policy.
Referral is not accompanied by any pre-requisite imaging or investigations required by the PPwT policy, consultant or unit.
Referral for acupuncture. (See NWL PPwT v4 https://www.hounslowccg.nhs.uk/news,-publications-and-policies/publications.aspx?n=2010)

62 Triage Specification – September 2018 – MSk Pathways – Metabolic Bone Disease - Osteoporosis
5.10. Metabolic Bone Disease - Osteoporosis
Background
Osteoporosis is a common condition. NICE estimate more than 2 million women in England and Wales are living with osteoporosis, and 180,000 fragility fractures present to health care providers per annum. The majority of osteoporosis diagnosis and management is undertaken in the primary care or through hospital case-finding Fracture Liaison Services. 221 per 100,000 women consult GPs annually with a new diagnosis of osteoporosis, and 657 per 100,000 consult GPs annually for review.
• Osteoporosis is a disease characterized by low bone mass and structural deterioration of bone tissue, with a consequent increase in bone fragility and susceptibility to fracture. Osteoporosis itself is asymptomatic, and often remains undiagnosed until a fragility fracture occurs. An osteoporotic fracture is a fragility fracture occurring as a consequence of osteoporosis. Characteristically, fractures occur in the wrist, spine, and hip, but they can also occur in the arm, pelvis, ribs, and other bones.
• A fragility fracture is defined as a fracture following a fall from standing height or less, although vertebral fractures may occur spontaneously, or as a result of routine activities such as bending or lifting.
• Osteoporosis is defined by the World Health Organization as a bone mineral density (BMD) of 2.5 standard deviations below the mean peak mass (average of young healthy adults) as measured by dual-energy X-ray absorptiometry (DXA) applied to the femoral neck and reported as a T-score. However, BMD measurement does not assess the structural deterioration in bone and consequently, most osteoporotic fractures occur in women who do not have osteoporosis as defined by a T-score equal to or less than -2.5.
Risk factors for fragility fractures
Reduced bone mineral density Endocrine disease including diabetes mellitus, hyperthyroidism, and hyperparathyroidism, gastrointestinal malabsorption: Crohn's disease, ulcerative colitis, coeliac disease, and pancreatitis; chronic kidney disease, chronic liver disease, chronic obstructive pulmonary disease, menopause (esp. premature) immobility, body mass index of less than 18.5 kg/m²
Unaffected bone mineral density Age - risk increases with age and is at least partly independent of BMD, oral corticosteroids (dependent on the dose and duration of treatment), smoking, alcohol (3 or more units daily), previous fragility fracture (risk increases with increasing number of fractures), rheumatoid arthritis, and other inflammatory arthropathies, parental history of hip fracture, drugs: pioglitazone, carbamazepine, antipsychotics, SSRIs and proton pump inhibitors, aromatase inhibitors GNRH analogues
Risk factors for falls Impaired vision, neuromuscular weakness and incoordination, cognitive impairment, the use of alcohol and sedative drugs
Assessment
Assess risk factors above. Offer DEXA scan in those with a history of fragility fracture, or those in the region of intervention thresholds for bone sparing agents on FRAX or QFRACTURE risk scores. See NICE Pathway https://pathways.nice.org.uk/pathways/osteoporosis for specific guidance on assessment. Assess for vitamin D deficiency and calcium intake. Assess falls risk using a risk assessment tool in people with high degree of frailty or those who have suffered a fragility fracture. Bone-sparing treatments are of greater benefit for secondary prevention, i.e. those who have had a fragility fracture previously. Different medical specialties provide osteoporosis care in complex cases (very low bone mineral density, failure or intolerance of treatment, endocrine and bone metabolism disorders): rheumatology, endocrinology, metabolic bone physician and care of the elderly physicians. Consider referral to endocrinology for those in whom hypogonadism is suspected.
63 Triage Specification – September 2018 – MSk Pathways – Metabolic Bone Disease - Osteoporosis
Referral to General Practitioner
(Referral from triage, community or hospital services specifically for primary care medical review)
Inclusions
Medication reviews (bone sparing agents and drugs increasing risk of falls) and non-urgent prescriptions.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice, alcohol reduction, vitamin D status and calcium intake.
Assessment and management of multi-morbidity and psychiatric co-morbidity.
Discussion about fitness for work and sickness certification.
Management following discharge from community or secondary care where no further intervention planned.
Patients referred back from community services with known or suspected serious underlying pathology where non-urgent (for re-evaluation and possible referral to secondary care).
Patient prepared to have bone sparing agents following a shared decision making discussion guided by a decision aid tool:
o Bisphosphonates for Treating Osteoporosis: https://www.nice.org.uk/guidance/ta464/resources/decision-support-from-nice-information-to-help-people-with-osteoporosis-and-their-health-professionalsdiscuss-the-options-pdf-4608867565
Exclusions
Patients seen in community or secondary care settings who need emergency or urgent assessment e.g. acute fractures or suspected bony metastases.
64 Triage Specification – September 2018 – MSk Pathways – Metabolic Bone Disease - Osteoporosis
Referral to Falls Service, Community Physiotherapy or First Contact Physiotherapist in Primary Care
Inclusions
Advice about the condition to aid shared decision-making, taking account of health literacy and patient beliefs.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice, alcohol reduction, vitamin D status and calcium intake.
Assessment and treatment of functional impairment.
Assessment of falls and provision of walking aids.
Advice and assessment about aids and adaptations to assist activities of daily living and promote independence.
Improve general fitness and participation in regular physical activity.
Exercises for enhancing flexibility and muscle strength.
If post-operative physiotherapy commissioned (following fragility fracture):
Post-operative physiotherapy
Exclusions
Fractures, including osteoporotic fractures, unless the patient has been reviewed by a doctor (e.g. orthopaedic surgeon, musculoskeletal physician) and cleared for community treatment – see below.
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to bear any weight, history of a fall, suspected fracture or dislocation.
Suspected inflammatory arthritis, unless rheumatological assessment commissioned.
Patients who need urgent specialist assessment e.g. severe pain unresponsive to analgesia and persistent loss of function.
65 Triage Specification – September 2018 – MSk Pathways – Metabolic Bone Disease - Osteoporosis
Referral to Musculoskeletal Interface Service
(May not be available in every CCG)
Inclusions
If musculoskeletal physician services commissioned
Advice about the condition to aid shared decision-making, taking account of health literacy and patient beliefs.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice, alcohol reduction, vitamin D status and calcium intake.
Advice on diagnosis and management of osteoporosis and fragility fractures
Advice on pharmacological management
Any imaging (X-rays, MRI) performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral. Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Key blood tests include FBC, ESR, U&Es, Glc, LFTs, Ca and Vit D, TSH. Any previous relevant outpatient summary letters and imaging reports (including X-ray reports from A&E and primary/community care, all previous DEXA scan reports) should be forwarded with the referral
Exclusions
Fractures, including osteoporotic fractures, unless the patient has been reviewed by a doctor (e.g. orthopaedic surgeon, musculoskeletal physician) and cleared for community treatment – see above.
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to bear any weight, history of a fall, suspected fracture or dislocation.
Patients with frailty and high risk of falls where a falls service is commissioned.
Suspected inflammatory arthritis, unless rheumatological assessment commissioned.
66 Triage Specification – September 2018 – MSk Pathways – Metabolic Bone Disease - Osteoporosis
Referral to Metabolic Bone Clinic, Rheumatologist or Ortho-geriatrician
Inclusions
Oral bisphosphonate contraindicated or intolerant.
Further reduction in bone mineral density inspite of compliant oral bisphosphonate use.
Parenteral therapy is considered.
Premenopausal women and men aged less than 50 years, who take steroids and had osteoporotic fracture.
Men aged over 50 with an osteoporotic fracture; men with severe osteoporosis.
History of multiple low impact fractures or severe osteoporosis (T score < -3.0).
Osteoporosis due to secondary causes (glucocorticoids, inflammatory arthritis, inflammatory bowel disease, malabsorption, HIV, hyperparathyroidism, prolonged amenorrhoea, aromatase inhibitors, GNRH analogues).
Consider referral for people who have further fractures whilst on treatment, but take account that treatment only reduces fracture risk by 50%, so some people will have a further fracture in spite of adequate treatment.
Consider referral to endocrinology for those in whom hypogonadism is suspected.
Paget’s disease, osteomalacia, rare genetic bone diseases.
Patient prepared to have bone sparing agents following a shared decision making discussion guided by a decision aid tool:
o Bisphosphonates for Treating Osteoporosis: https://www.nice.org.uk/guidance/ta464/resources/decision-support-from-nice-information-to-help-people-with-osteoporosis-and-their-health-professionalsdiscuss-the-options-pdf-4608867565
Any imaging (X-rays, MRI) performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral.
Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Key blood tests include FBC, ESR, U&Es, Glc, LFTs, Ca and Vit D, TSH.
Any previous relevant outpatient summary letters and imaging reports (including X-ray reports from A&E and primary/community care, all previous DEXA scan reports) should be forwarded with the referral
Exclusions
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to bear any weight, suspected (unconfirmed) fracture or dislocation. (Refer to on-call orthopaedic team or A&E).
67 Triage Specification – September 2018 – MSk Pathways – Polymyalgia Rheumatica and Giant Cell Arteritis
5.11. Polymyalgia Rheumatica and Giant Cell Arteritis
Background
Polymyalgia Rheumatica
Polymyalgia rheumatica (PMR) is the most common cause of new inflammatory rheumatic disease in elderly people, and represents one of the most common indications for long-term corticosteroid therapy. The annual incidence of polymyalgia rheumatica is 84 per 100,000. Polymyalgia rheumatica (PMR) is usually diagnosed and treated in the community. The average age of onset is just over 70 years of age and is seldom diagnosed in people younger than 50 years of age. It occurs about two to three times as frequently in women vs men. The prevalence varies between different populations, with Scandinavian people having a higher rate than other white, black and Japanese people. Giant cell arteritis and its complications can occur, abruptly and without warning, early in the course of polymyalgia rheumatica in up to 10% of cases. Complications of long-term corticosteroid treatment are common, and may occur in up to 60% of people. Response to systemic corticosteroids is rapid and dramatic, with many symptoms resolving after a few days of treatment. Treatment for 1–3 years is often required. Relapse is common, but responds to restarting or increasing the dose of systemic corticosteroids. Refer people with atypical features of PMR who do not have a clear alternative cause for their symptoms including people who:
• Have diagnostic uncertainty, lack of response, or therapeutic difficulty.
• Are less than 60 years of age.
• Have red flags suggestive of a serious underlying condition such as weight loss, night pain, or neurological features.
• Do not have the core features of PMR including: o Bilateral shoulder or pelvic girdle aching. o Stiffness lasting for at least 45 minutes after waking or periods of rest.
• Have clinical features that are uncommon with PMR including people: o With normal inflammatory markers; or ESR of more than 100 mm/hour; or very high
CRP. o With a chronic onset of their symptoms.
Refer for specialist management if:
• It is not possible to reduce corticosteroids at reasonable intervals without causing relapse.
• Corticosteroids are required for more than 2 years.
Giant Cell Arteritis/Temporal Arteritis
The annual incidence of giant cell arteritis in the UK population is approximately 20 per 100,0000people. It is uncommon under the age of 60, and very rare under the age of 50. Consider in those over 50, with a new headache, temporal artery abnormality (tenderness, thickening, pulseless); jaw claudication; systemic symptoms; new onset of visual or neurological symptoms. It is rare to have normal inflammatory markers (ESR and CRP) with untreated active giant cell arteritis; however some patients will have active disease with only mildly raised inflammatory markers. About 30–50% of people have spontaneous exacerbations of disease, especially during the first 2 years, that are independent of the corticosteroid regimen. It is an sight-threatening emergency and if the diagnosis is suspected, an urgent referral
should be made to ambulatory care or accident and emergency. Patients with new neurological signs or visual loss may require admission.
68 Triage Specification – September 2018 – MSk Pathways – Polymyalgia Rheumatica and Giant Cell Arteritis
Referral to the General Practitioner
(Referral from triage, community or hospital services specifically for primary care medical review)
Inclusions
Patients referred back from community services with known or suspected serious underlying pathology where non-urgent (for re-evaluation and possible referral to secondary care).
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Screening for complications of corticosteroid therapy including glucose intolerance, raised blood pressure, fluid retention, weight gain, muscle weakness, osteoporosis and mood disturbances.
Assessment and management of multi-morbidity and psychiatric co-morbidity.
Medication reviews and non-urgent prescriptions. Note, for disease-modifying drugs and immunosuppressants initiated in secondary care, there must be an shared care protocol that has been agreed and accepted by both the primary and secondary care clinician responsible for an individual patient.
Discussion about fitness for work and sickness certification.
Management following discharge from community or secondary care where no further intervention planned.
See NICE Clinical Knowledge Summaries for differential diagnosis, investigations and management:
o https://cks.nice.org.uk/polymyalgia-rheumatica
o https://cks.nice.org.uk/giant-cell-arteritis
Exclusions
Suspected temporal arteritis. (Emergency referral to A&E or ambulatory care).
Patients seen in community or secondary care settings who need emergency or urgent assessment e.g. suspected temporal arteritis, acute angle closure glaucoma, myeloma, connective tissue disease or autoimmune disease. (Emergency referral to A&E or ambulatory care).
.
69 Triage Specification – September 2018 – MSk Pathways – Polymyalgia Rheumatica and Giant Cell Arteritis
Referral to Community Physiotherapy or First Contact Physiotherapy in Primary Care
Inclusions
Assessment and treatment of functional impairment.
Assessment of falls and provision of walking aids.
Improve general fitness and participation in regular physical activity.
Exercises for enhancing flexibility and muscle strength.
Exclusions
Suspected temporal arteritis. (Emergency referral to A&E or ambulatory care).
Cases where there is significant threat to life, limb, vision, or vital organ. (Emergency referral to A&E or ambulatory care).
Severe acute pain or inflammation.
Patient needs medical opinion.
70 Triage Specification – September 2018 – MSk Pathways – Polymyalgia Rheumatica and Giant Cell Arteritis
Referral to Rheumatology Interface Service
(May not be available in every CCG)
If rheumatological physiotherapy, occupational therapy and psychology available:
Assessment and treatment of functional impairment.
Assessment of gait and stability.
Advice and assessment about aids and adaptations to assist activities of daily living and promote independence.
Psychological interventions (for example, relaxation, stress management) and cognitive coping skills.
If rheumatology nurse or therapist with rheumatology training available:
Symptom and medication monitoring under shared care arrangement with primary and secondary care.
If rheumatologist or GP with a special interest available:
Diagnostic uncertainty, unusual presentation lack of response, or therapeutic difficulty.
Exclusions
Suspected temporal arteritis. (Emergency referral to A&E or ambulatory care).
Cases where there is significant threat to life, limb, vision, or vital organ. (Emergency referral to A&E or ambulatory care).
Severe acute pain or inflammation, unless service commissioned for acute assessment.
Patient needs medical opinion, unless a medical opinion commissioned.
71 Triage Specification – September 2018 – MSk Pathways – Polymyalgia Rheumatica and Giant Cell Arteritis
Referral to Secondary Care Rheumatology
Inclusions
Suspected polymyalgia rheumatica with diagnostic uncertainty. Negative or absent blood tests should not delay referrals made on clinical grounds.
Diagnosed polymyalgia rheumatica with therapeutic difficulty:
It is not possible to reduce corticosteroids at reasonable intervals without causing relapse.
Corticosteroids are required for more than 2 years.
Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral. Any imaging performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral.
Exclusions
Suspected temporal arteritis. (Emergency referral to A&E or ambulatory care).
Cases where there is significant threat to life, limb, vision, or vital organ. (Emergency referral to A&E or ambulatory care).
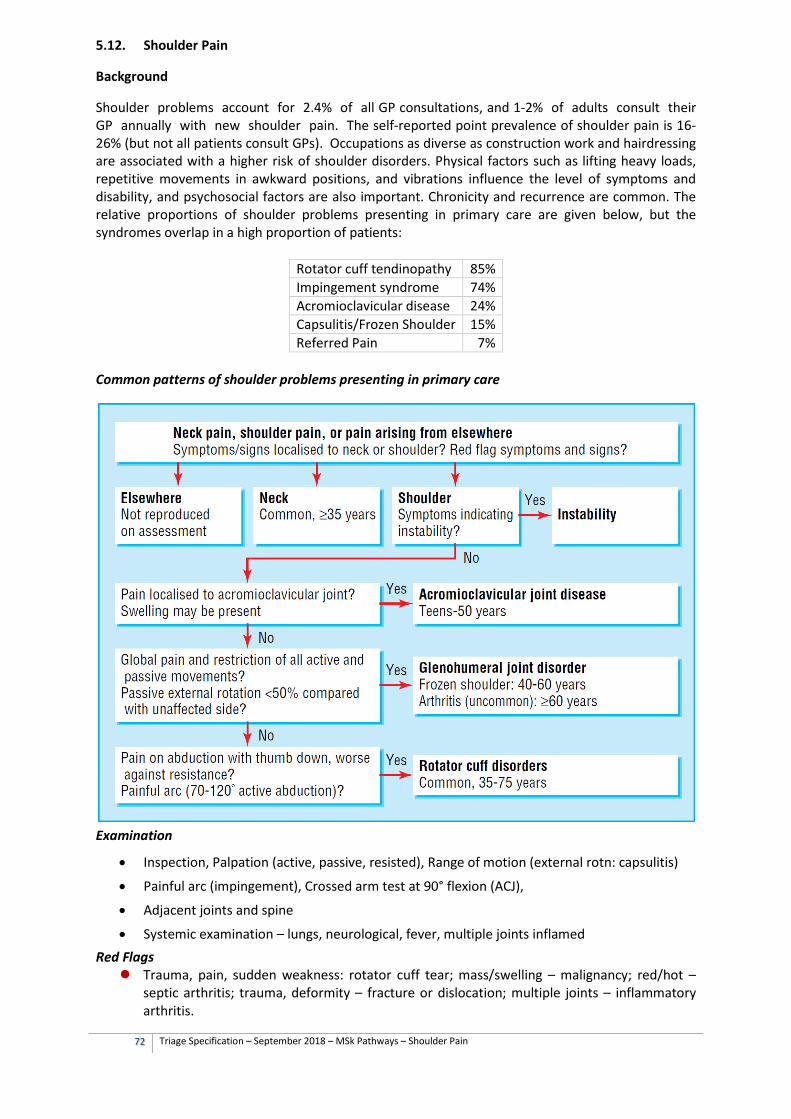
72 Triage Specification – September 2018 – MSk Pathways – Shoulder Pain
5.12. Shoulder Pain
Background
Shoulder problems account for 2.4% of all GP consultations, and 1-2% of adults consult their GP annually with new shoulder pain. The self-reported point prevalence of shoulder pain is 16-26% (but not all patients consult GPs). Occupations as diverse as construction work and hairdressing are associated with a higher risk of shoulder disorders. Physical factors such as lifting heavy loads, repetitive movements in awkward positions, and vibrations influence the level of symptoms and disability, and psychosocial factors are also important. Chronicity and recurrence are common. The relative proportions of shoulder problems presenting in primary care are given below, but the syndromes overlap in a high proportion of patients:
Rotator cuff tendinopathy 85% Impingement syndrome 74% Acromioclavicular disease 24% Capsulitis/Frozen Shoulder 15% Referred Pain 7%
Common patterns of shoulder problems presenting in primary care
Examination
• Inspection, Palpation (active, passive, resisted), Range of motion (external rotn: capsulitis)
• Painful arc (impingement), Crossed arm test at 90° flexion (ACJ),
• Adjacent joints and spine
• Systemic examination – lungs, neurological, fever, multiple joints inflamed Red Flags Trauma, pain, sudden weakness: rotator cuff tear; mass/swelling – malignancy; red/hot –
septic arthritis; trauma, deformity – fracture or dislocation; multiple joints – inflammatory arthritis.
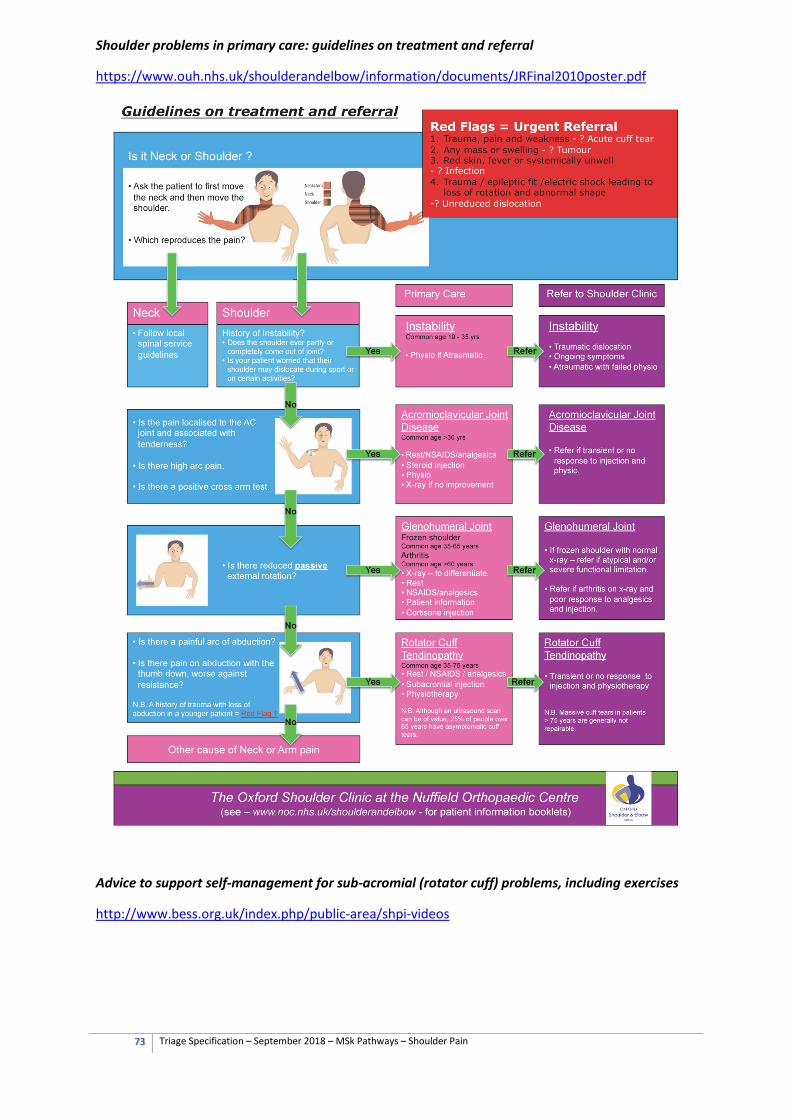
73 Triage Specification – September 2018 – MSk Pathways – Shoulder Pain
Shoulder problems in primary care: guidelines on treatment and referral
https://www.ouh.nhs.uk/shoulderandelbow/information/documents/JRFinal2010poster.pdf
Advice to support self-management for sub-acromial (rotator cuff) problems, including exercises
http://www.bess.org.uk/index.php/public-area/shpi-videos
74 Triage Specification – September 2018 – MSk Pathways – Shoulder Pain
Referral to General Practitioner
(Referral from triage, community or hospital services specifically for primary care medical review)
Inclusions
Assessment and management of multi-morbidity and psychiatric co-morbidity.
Medication reviews and non-urgent prescriptions.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Discussion about fitness for work and sickness certification
Management following discharge from community or secondary care where no further intervention planned
Patients referred back from community services with known or suspected serious underlying pathology where non-urgent (for re-evaluation and possible referral to secondary care).
Exclusions
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to abduct following trauma (acute rotator cuff tear), suspected fracture or dislocation, severe soft tissue injury with gross instability, neurovascular damage following trauma. (Refer to on-call orthopaedic team or A&E).
Patients seen in community or secondary care settings who need urgent specialist assessment e.g. severe pain unresponsive to analgesia and persistent loss of function.
75 Triage Specification – September 2018 – MSk Pathways – Shoulder Pain
Referral to Community Physiotherapy or First Contact Physiotherapy in Primary Care
Inclusions History or clinical examination suggestive of:
o Subacromial, rotator cuff and acromioclavicular syndromes. o Shoulder instability (if not caused by significant trauma). o Frozen shoulder, capsulitis – only during the ‘thawing phase’ (there is little evidence
that exercises are helpful during the painful and frozen phases, although a patient may benefit from reassurance and advice regarding activity modification).
o Neck problems presenting with shoulder pain.
Advice about the condition to aid shared decision-making, taking account of health literacy and patient beliefs.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Assessment and treatment of functional impairment.
Assessment of falls and provision of walking aids.
Advice and assessment about aids and adaptations to assist activities of daily living and promote independence.
Improve general fitness and participation in regular physical activity.
Exercises for enhancing flexibility and muscle strength.
If post-operative physiotherapy commissioned:
Post-operative physiotherapy
Exclusions
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to abduct following trauma (acute rotator cuff tear), suspected fracture or dislocation, severe soft tissue injury with gross instability, neurovascular damage following trauma. (Refer to on-call orthopaedic team or A&E).
Suspected inflammatory arthritis, unless rheumatological assessment commissioned.
Patients seen in community or secondary care settings who need urgent specialist assessment e.g. severe pain unresponsive to analgesia and persistent loss of function.
Community physiotherapy only exclusions
Presented with same condition within previous 12 months, and there was no substantive improvement with treatment previously, and if no other community treatment options are appropriate (e.g. pain service, where commissioned).
Co-morbidities that significantly impair a particular patient’s ability to exercise. For example neurological (e.g. stroke), severe cardiac, renal, liver or respiratory failure, recurrent disabling hypoglycaemia or poorly controlled epilepsy.
76 Triage Specification – September 2018 – MSk Pathways – Shoulder Pain
Referral to Musculoskeletal Interface Service
(May not be available in every CCG)
Inclusions
Unsuccessful conservative treatment, including physiotherapy, activity modification, NSAIDs and steroid injections (where clinically appropriate)
Steroid injection if GP has not already administered
Diagnostic uncertainty
Acute rotator cuff injuries where early surgical repair may be indicated (e.g. trauma in younger patients)
If medical staff available:
Corticosteroid injection in anticoagulated patients with confirmed diagnosis.
Exclusions
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to abduct following trauma (acute rotator cuff tear), suspected fracture or dislocation, severe soft tissue injury with gross instability, neurovascular damage following trauma. (Refer to on-call orthopaedic team or A&E).
Suspected inflammatory arthritis, unless rheumatological assessment commissioned.
Patients seen in community or secondary care settings who need urgent specialist assessment e.g. severe pain unresponsive to analgesia and persistent loss of function.
77 Triage Specification – September 2018 – MSk Pathways – Shoulder Pain
Referral to Secondary Care Orthopaedics
Inclusions
Unsuccessful conservative management.
Patient prepared to have surgical intervention following a shared decision making discussion guided by patient information leaflets and decision aid tools:
o Treatments for impingement, frozen shoulder and instability: https://www.ouh.nhs.uk/shoulderandelbow/information/patient-information.aspx
o Surgery: rotator cuff repair, shoulder replacement, anterior stabilisation, manipulation under anaesthetic (for frozen shoulder): https://www.ouh.nhs.uk/shoulderandelbow/information/patient-information.aspx
o Surgery: subacromial decompression: https://www.healthwise.net/cochranedecisionaid/Content/StdDocument.aspx?DOCHWID=aa54545 https://www.bmj.com/content/362/bmj.k2860
Thresholds for surgical referral: NHS England is currently consulting on proposals to only offer arthroscopic subacromial decompression for pure subacromial shoulder impingement, in appropriate cases. ‘Pure subacromial shoulder impingement’ means subacromial pain not caused by associated diagnoses such as rotator cuff tears, acromio-clavicular joint pain, or calcific tendinopathy. https://www.england.nhs.uk/evidence-based-interventions. Once the scope is finalised by NHS England, all CCGs will be expected to implement the recommendations.
Any imaging performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral:
o X-ray shoulder for frozen shoulder (to exclude arthritis). o X-ray of acromioclavicular joint (for severe osteoarthritis or instability). o Ultrasound shoulder (for rotator cuff or subacromial problems).
Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
Exclusions
Patients who need emergency or urgent assessment e.g. joint pain associated with systemic symptoms, signs of infection, known primary or suspected malignancy, sudden inability to abduct following trauma (acute rotator cuff tear), suspected fracture or dislocation, severe soft tissue injury with gross instability, neurovascular damage following trauma. (Refer to on-call orthopaedic team or A&E).
Suspicion of inflammatory joint disease, peripheral vascular disease. (Discuss with on-call specialist, or refer to medical, rheumatology or vascular team, depending on clinical presentation and urgency).
Patients who have not been triaged or referred from a community musculoskeletal service (including non-urgent internally generated referrals (consultant to consultant referrals).
Conservative management and self-management strategies are clinically appropriate but have not been tried.
PPwT form has not been completed by referrer where request is for a procedure covered by the policy.
Referral is not accompanied by any pre-requisite imaging or investigations required by the consultant or unit.
78 Triage Specification – September 2018 – MSk Pathways – Chronic widespread pain (Fibromyalgia, Chronic primary pain)
5.13. Chronic widespread pain (Fibromyalgia, Chronic primary pain)
Background
Chronic widespread pain (also known as fibromyalgia or chronic primary pain) is a common disorder. The incidence in primary care is 180-583 per 100,000 per year. The population prevalence is 1.2-5.4%. The aetiology is unknown, and the definition excludes specific rheumatological causes. It is 2-3 times more common in women than men, and the prevalence increases with age, reaching a peak around the seventh decade of life. Chronic primary pain is chronic pain in one or more anatomical regions, and is characterised by significant emotional distress (anxiety, anger, frustration, depressed mood) and functional disability (interference in daily life activities and reduced participation in social roles). Chronic primary pain is multifactorial: biological, psychological and social factors contribute to the pain syndrome. The diagnosis is appropriate independently of identified biological or psychological contributors unless a specific diagnosis would better account for the presenting symptoms. (ICD-11 2018). Chronic widespread pain commonly co-occurs with a number of physical conditions, including rheumatoid arthritis and systemic lupus erythematosus. It is also strongly associated with anxiety, depression, irritable bowel syndrome and post-traumatic stress disorder. The exact pathophysiology is not known. Hypotheses include: Peripheral and central sensitivity at spinal or brainstem level, altered pain perception and somatisation. The nociceptive system has links with the stress regulating, immune and sleep systems, which may explain some of the clinical features. Patients are commonly referred to musculoskeletal, pain and rheumatology services. Features in the history favouring chronic widespread pain include the distribution of pain (head trunk and four limbs; muscles as well as bone and joints); chronicity (greater than three months); symptoms of fatigue, non-refreshing sleep and cognitive ‘fogging’. The presence of tender myofascial trigger points and absence of synovitis on examination support the diagnosis. Screening tests for alternative diagnoses
• TSH, vitamin D, U+E, LFT, Calcium, Phosphate, Full Blood Count, ESR, urine dipstick.
• Consider ANA (note high risk of false positives, ANA tests of 1:80 are not usually clinically significant in adults).
• Consider screening for depression and anxiety.
• Consider sleep apnoea; Epworth score in obese patients at risk of sleep apnoea.
• Be aware of false positive results when screening for conditions of low prevalence in a primary care population.
Referrals
• Consider making the diagnosis and managing chronic widespread pain in primary care. EULAR revised recommendations for the management of fibromyalgia.
• Refer to a community or hospital pain service if diagnostic uncertainty. o Rheumatologists in North-West London do not supply pain management services.
Do not refer patients with known or suspected fibromyalgia to rheumatology unless additional clinical features suggest a rheumatological diagnosis.
79 Triage Specification – September 2018 – MSk Pathways – Chronic widespread pain (Fibromyalgia, Chronic primary pain)
• Consider referral under an alternative pathway for patients with any of the following symptoms, signs or investigations suggestive of a rheumatological condition, infection or malignancy:
o Abnormal neurological signs present (including muscle abnormalities) o Visual disturbance/change o Swollen joints (synovitis) o MTP/MCP joint tenderness (or pain on squeeze test) o Morning joint stiffness (lasting over 30 minutes) o Unexplained rise in erythrocyte sedimentation rate (ESR) o A positive ANA test with a titre of greater than 1:80. ANA tests of less than 1:80 are
not usually clinically significant in adults o Unexplained blood/protein on urine dipstick o Weight loss o Fever o Lymphadenopathy o Recent onset Raynaud’s phenomenon o Skin rashes (psoriasis, SLE, dermatomyositis)
80 Triage Specification – September 2018 – MSk Pathways – Chronic widespread pain (Fibromyalgia, Chronic primary pain)
Referral to the General Practitioner
(Referral from triage, community, or hospital services specifically for primary care medical review)
Inclusions
Consider history, examination and screening tests in primary care to rule out alternative diagnoses. Be aware of false positive results when screening for conditions of low prevalence in a primary care population.
Assessment and management of multi-morbidity and psychiatric co-morbidity.
Medication reviews and non-urgent prescriptions. Note, patients with opioid or gabapentinoids dependence are likely to need specialist support to reduce medication.
Advice regarding achieving and maintaining optimal weight, nutrition, physical activity and healthy lifestyle, including smoking cessation advice.
Discussion about fitness for work and sickness certification.
Management following discharge from community or secondary care where no further intervention planned.
Patients referred back from community services with known or suspected serious underlying pathology where non-urgent (for re-evaluation and possible referral to secondary care).
Exclusions
Cases where there is significant threat to life, limb, or vital organ. (Emergency referral to A&E or ambulatory care).
Patients seen in community or secondary care settings who need emergency or urgent assessment e.g. suspicion of inflammatory joint, multi-system or connective tissue disease, peripheral vascular disease or fracture. (Refer to a specialist as clinically appropriate).
81 Triage Specification – September 2018 – MSk Pathways – Chronic widespread pain (Fibromyalgia, Chronic primary pain)
Referral to Community Physiotherapy or First Contact Physiotherapy in Primary Care
Inclusions
Re-referral for the same condition only where the patient has demonstrated a significant (> 50%) improvement lasting beyond the end of previous treatment (> 6 months).
Assessment of unrelated musculoskeletal problem.
Assessment and treatment of functional impairment.
Assessment of falls and provision of walking aids.
Improve general fitness and participation in regular physical activity.
Advice regarding pacing.
Exercises for enhancing flexibility and muscle strength.
Exclusions
Reasonable clinical suspicion of serious underlying pathology (red flags) including cancer, infection, trauma, severe and progressive neurology, inflammatory joint disease, multi-system disease or connective tissue disease. These patients will be referred back to GP for urgent assessment (same day).
Not been offered self-management advice, where clinically appropriate.
Presented with same condition within previous 12 months, and there was no substantive improvement with treatment previously, and if no other community treatment options are appropriate (e.g. pain service, where commissioned).
Chronic widespread pain or inflammatory disorder (refer to rheumatology interface service if commissioned), unless a specialist service has identified a specific functional goal for physiotherapy (e.g. improving gait, improving balance and reducing falls, occupational rehabilitation).
82 Triage Specification – September 2018 – MSk Pathways – Chronic widespread pain (Fibromyalgia, Chronic primary pain)
Referral to Musculoskeletal Interface Service
(May not be available in every CCG)
Inclusions
Confirmation of diagnosis where uncertainty.
High risk of poor functional outcome or high levels of distress e.g. due to psychological and social factors where single modality treatments have been ineffective or not clinically appropriate.
Any imaging performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral. Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
Pain management advice.
Exclusions
Patients with features in the history, examination or screening tests suggesting serious underlying pathology. (Refer to a specialist as clinically appropriate).
Not been offered self-management advice, where clinically appropriate.
Presented with same condition within previous 12 months, and there was no substantive improvement with treatment previously, and if no other community treatment options are appropriate (e.g. pain service, where commissioned).
83 Triage Specification – September 2018 – MSk Pathways – Chronic widespread pain (Fibromyalgia, Chronic primary pain)
Referral to Community Pain Service offering a combined physical and psychological approach
(May not be available in every CCG)
Inclusions
High risk of poor functional outcome or high levels of distress e.g. due to psychological and social factors where single modality treatments have been ineffective or not clinically appropriate
Chronic widespread pain where non-invasive treatments have not had at least a 30% improvement in pain or function, lasting at least 3-6 months beyond the end of treatment, and where previous assessment suggests that invasive treatments (injections, surgery) are not appropriate
Any imaging performed in primary or community care should be available on IEP/receiving unit, and the reports forwarded with the referral. Any blood tests and pathology performed in primary or community care should be available on ICE/OpenNet and key results forwarded with the referral. Any previous relevant outpatient summary letters and imaging reports should be forwarded with the referral.
If medical support available
Step down from strong opioids and other pain medications in conjunction with support from a combined physical and psychological approach, where appropriate for a community setting
Exclusions
Reasonable clinical suspicion of serious underlying pathology (red flags) including cancer, infection, trauma, severe and progressive neurology, inflammatory joint disease, multi-system disease or connective tissue disease. These patients will be referred back to GP for urgent assessment (same day).
Patient does not accept a combined approach including a psychological approach to pain management.
84 Triage Specification – September 2018 – MSk Pathways – Chronic widespread pain (Fibromyalgia, Chronic primary pain)
Referral to Secondary Care Rheumatology or Pain Services
Inclusions
Assessment of undiagnosed pain, multi-morbidity and psychiatric co-morbidity, where a positive diagnosis has not been made in a primary or community care setting, or where the diagnosis is in doubt.
Rheumatology: exclusion of rheumatological disease in patients presenting with widespread pain
Pain Services: widespread chronic pain for advice on pharmacological management, including stepping down medication where this cannot be managed in primary or community care.
Pain Services: Consideration of other procedures covered by NICE Interventional Procedures guidance where appropriate and cost-effective for use within the NHS for this person. (Review the old notes first).
Pain management service offering a combined physical and psychological approach: High risk of poor functional outcome or high levels of distress e.g. due to psychological and social factors, and patient accepts a combined approach including a psychological approach to pain management
Exclusions
All services: Reasonable clinical suspicion of undiagnosed serious underlying pathology (red flags) including cancer, infection, trauma, severe and progressive neurology, inflammatory disorders where patient systemically unwell. These patients will be referred back to GP for urgent assessment (same day), or to A&E or on-call medical teams as clinically appropriate.
All services: Patients with chronic widespread pain who have not been triaged or referred from a community musculoskeletal service (including non-urgent internally generated referrals (consultant to consultant referrals).
All services: Patient has not been offered advice from primary or community services regarding achieving and maintaining optimal weight, nutrition, physical activity, pacing and healthy lifestyle.
All services: A previous discharge plan has advised that no further treatments would be helpful in secondary care or pain management service, and there is no substantive change in the clinical presentation, and there are no medication issues that could be managed in primary care (e.g. where the GP and patient do not need specialist support to step down ineffective or harmful medication)
Pain management services: Patient does not accept a combined approach including a psychological approach to pain management
Rheumatology: patients where there is no diagnostic dilemma, and where the patient should be assessed by pain management service.
Pain services: PPwT form has not been completed by referrer where request is for a procedure covered by the policy
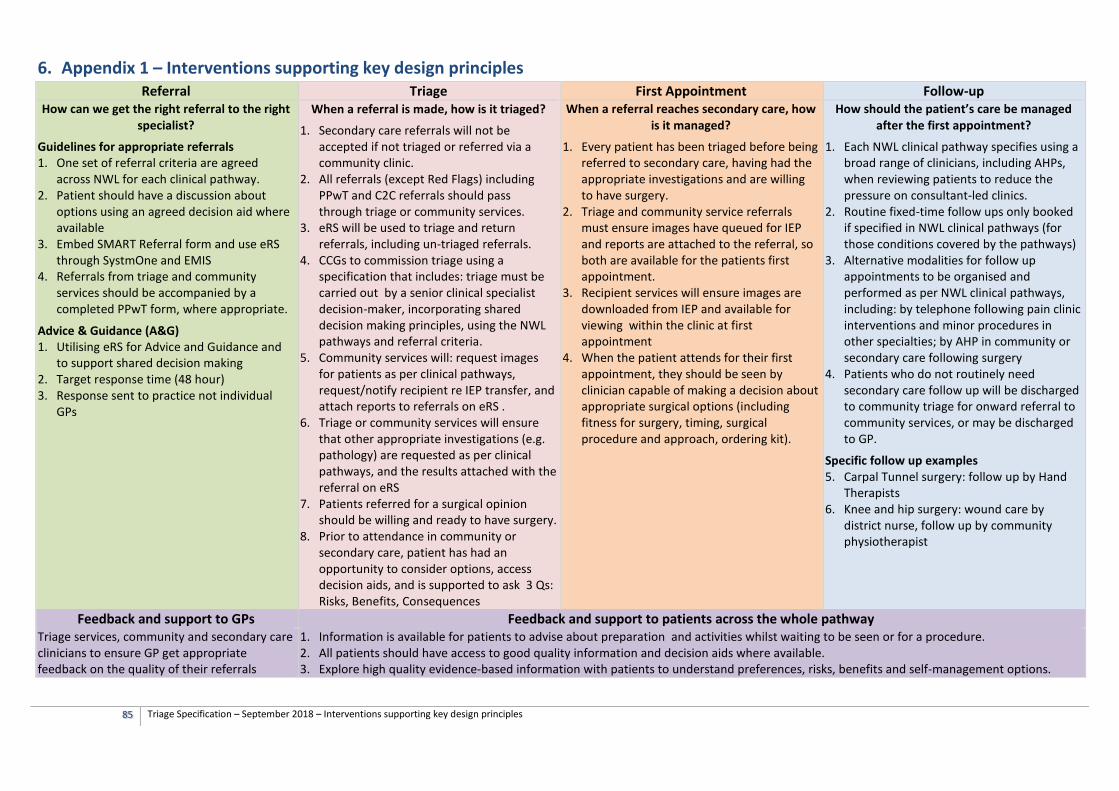
85 Triage Specification – September 2018 – Interventions supporting key design principles
6. Appendix 1 – Interventions supporting key design principles Referral Triage First Appointment Follow-up
How can we get the right referral to the right specialist?
Guidelines for appropriate referrals 1. One set of referral criteria are agreed
across NWL for each clinical pathway. 2. Patient should have a discussion about
options using an agreed decision aid where available
3. Embed SMART Referral form and use eRS through SystmOne and EMIS
4. Referrals from triage and community services should be accompanied by a completed PPwT form, where appropriate.
Advice & Guidance (A&G) 1. Utilising eRS for Advice and Guidance and
to support shared decision making 2. Target response time (48 hour) 3. Response sent to practice not individual
GPs
When a referral is made, how is it triaged?
1. Secondary care referrals will not be accepted if not triaged or referred via a community clinic.
2. All referrals (except Red Flags) including PPwT and C2C referrals should pass through triage or community services.
3. eRS will be used to triage and return referrals, including un-triaged referrals.
4. CCGs to commission triage using a specification that includes: triage must be carried out by a senior clinical specialist decision-maker, incorporating shared decision making principles, using the NWL pathways and referral criteria.
5. Community services will: request images for patients as per clinical pathways, request/notify recipient re IEP transfer, and attach reports to referrals on eRS .
6. Triage or community services will ensure that other appropriate investigations (e.g. pathology) are requested as per clinical pathways, and the results attached with the referral on eRS
7. Patients referred for a surgical opinion should be willing and ready to have surgery.
8. Prior to attendance in community or secondary care, patient has had an opportunity to consider options, access decision aids, and is supported to ask 3 Qs: Risks, Benefits, Consequences
When a referral reaches secondary care, how is it managed?
1. Every patient has been triaged before being referred to secondary care, having had the appropriate investigations and are willing to have surgery.
2. Triage and community service referrals must ensure images have queued for IEP and reports are attached to the referral, so both are available for the patients first appointment.
3. Recipient services will ensure images are downloaded from IEP and available for viewing within the clinic at first appointment
4. When the patient attends for their first appointment, they should be seen by clinician capable of making a decision about appropriate surgical options (including fitness for surgery, timing, surgical procedure and approach, ordering kit).
How should the patient’s care be managed after the first appointment?
1. Each NWL clinical pathway specifies using a broad range of clinicians, including AHPs, when reviewing patients to reduce the pressure on consultant-led clinics.
2. Routine fixed-time follow ups only booked if specified in NWL clinical pathways (for those conditions covered by the pathways)
3. Alternative modalities for follow up appointments to be organised and performed as per NWL clinical pathways, including: by telephone following pain clinic interventions and minor procedures in other specialties; by AHP in community or secondary care following surgery
4. Patients who do not routinely need secondary care follow up will be discharged to community triage for onward referral to community services, or may be discharged to GP.
Specific follow up examples 5. Carpal Tunnel surgery: follow up by Hand
Therapists 6. Knee and hip surgery: wound care by
district nurse, follow up by community physiotherapist
Feedback and support to GPs Feedback and support to patients across the whole pathway Triage services, community and secondary care clinicians to ensure GP get appropriate feedback on the quality of their referrals
1. Information is available for patients to advise about preparation and activities whilst waiting to be seen or for a procedure. 2. All patients should have access to good quality information and decision aids where available. 3. Explore high quality evidence-based information with patients to understand preferences, risks, benefits and self-management options.
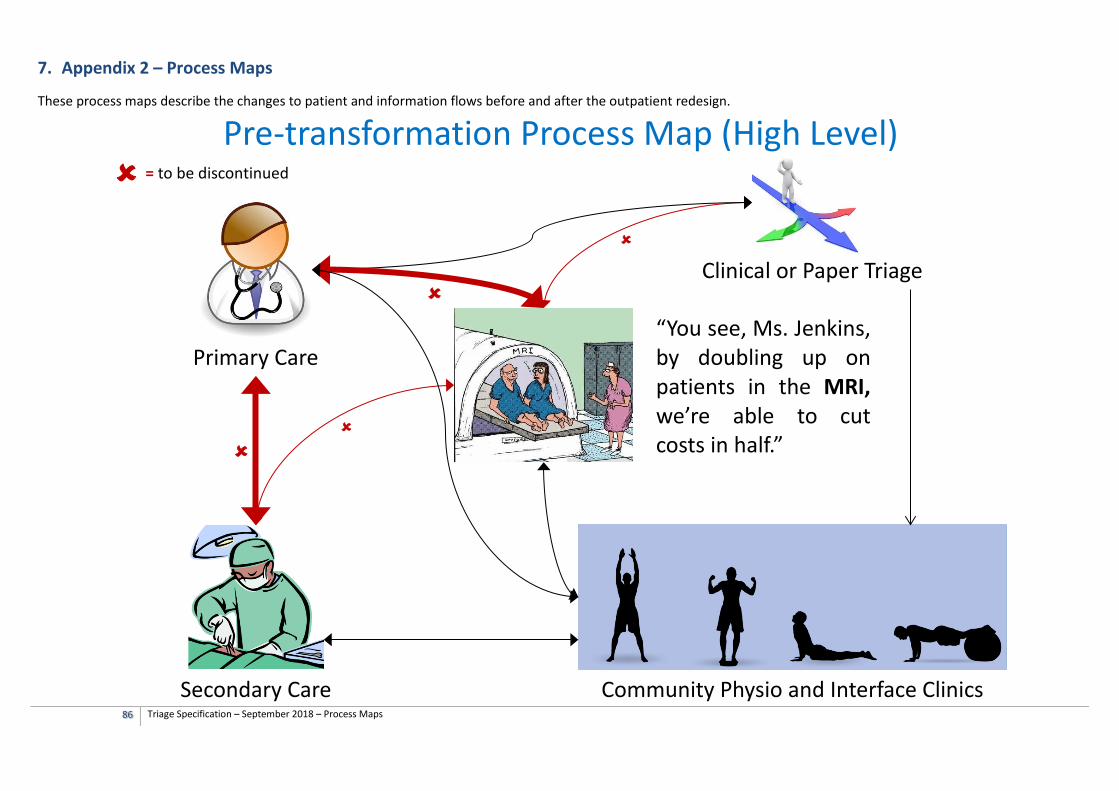
86 Triage Specification – September 2018 – Process Maps
7. Appendix 2 – Process Maps
These process maps describe the changes to patient and information flows before and after the outpatient redesign.
“You see, Ms. Jenkins, by doubling up on patients in the MRI, we’re able to cut costs in half.”
Primary Care
Secondary Care Community Physio and Interface Clinics
Clinical or Paper Triage
= to be discontinued Pre-transformation Process Map (High Level)
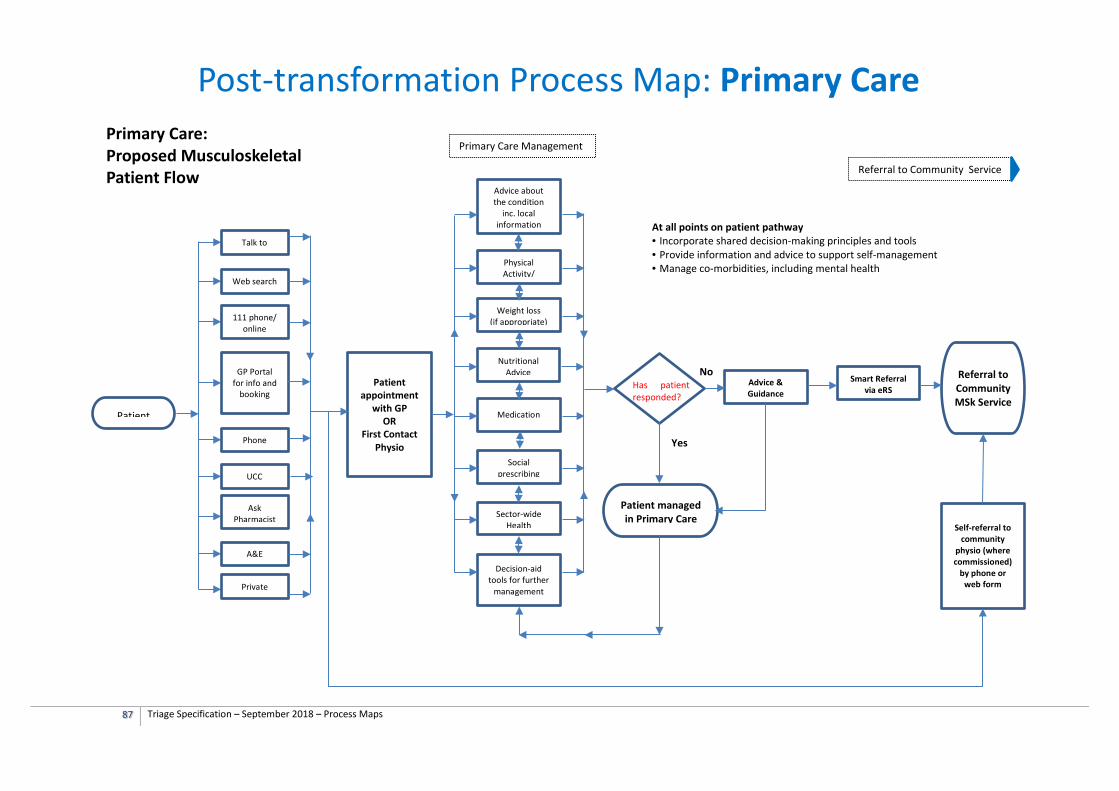
87 Triage Specification – September 2018 – Process Maps
Patient
Primary Care: Proposed Musculoskeletal Patient Flow
Patient managed in Primary Care
Talk to
Web search
111 phone/ online
GP Portal for info and
booking
Phone
A&E
Ask Pharmacist
UCC
Private
Patient appointment
with GP OR
First Contact Physio
Advice about the condition
inc. local information
Sector-wide Health
Social prescribing
Decision-aid tools for further
management
Medication
Physical Activity/
Nutritional Advice
Weight loss (if appropriate)
Primary Care Management
Has patient responded?
Advice & Guidance
Yes
No Smart Referral
via eRS Referral to Community MSk Service
Referral to Community Service
Post-transformation Process Map: Primary Care
Self-referral to community
physio (where commissioned)
by phone or web form
At all points on patient pathway • Incorporate shared decision-making principles and tools • Provide information and advice to support self-management • Manage co-morbidities, including mental health
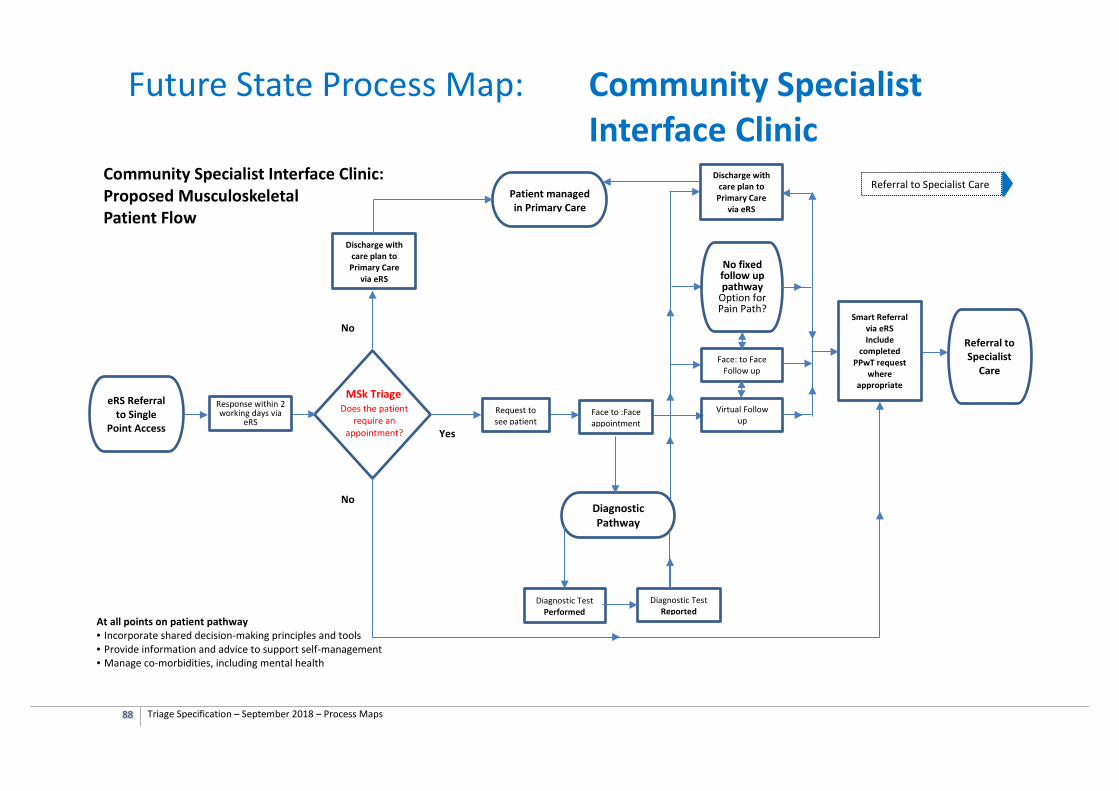
88 Triage Specification – September 2018 – Process Maps
Future State Process Map: Community Specialist
Interface Clinic Community Specialist Interface Clinic: Proposed Musculoskeletal Patient Flow
eRS Referral to Single
Point Access
Diagnostic Pathway
Discharge with care plan to Primary Care
via eRS
Diagnostic Test Reported
Face to :Face appointment
Diagnostic Test Performed
MSk Triage Request to see patient
Yes
Referral to Specialist Care
Response within 2 working days via
eRS Does the patient
require an appointment?
No
Discharge with care plan to
Primary Care via eRS
Virtual Follow up
Face: to Face Follow up
No fixed follow up pathway
Option for Pain Path?
Referral to Specialist
Care
Smart Referral via eRS Include
completed PPwT request
where appropriate
Patient managed in Primary Care
At all points on patient pathway • Incorporate shared decision-making principles and tools • Provide information and advice to support self-management • Manage co-morbidities, including mental health
No
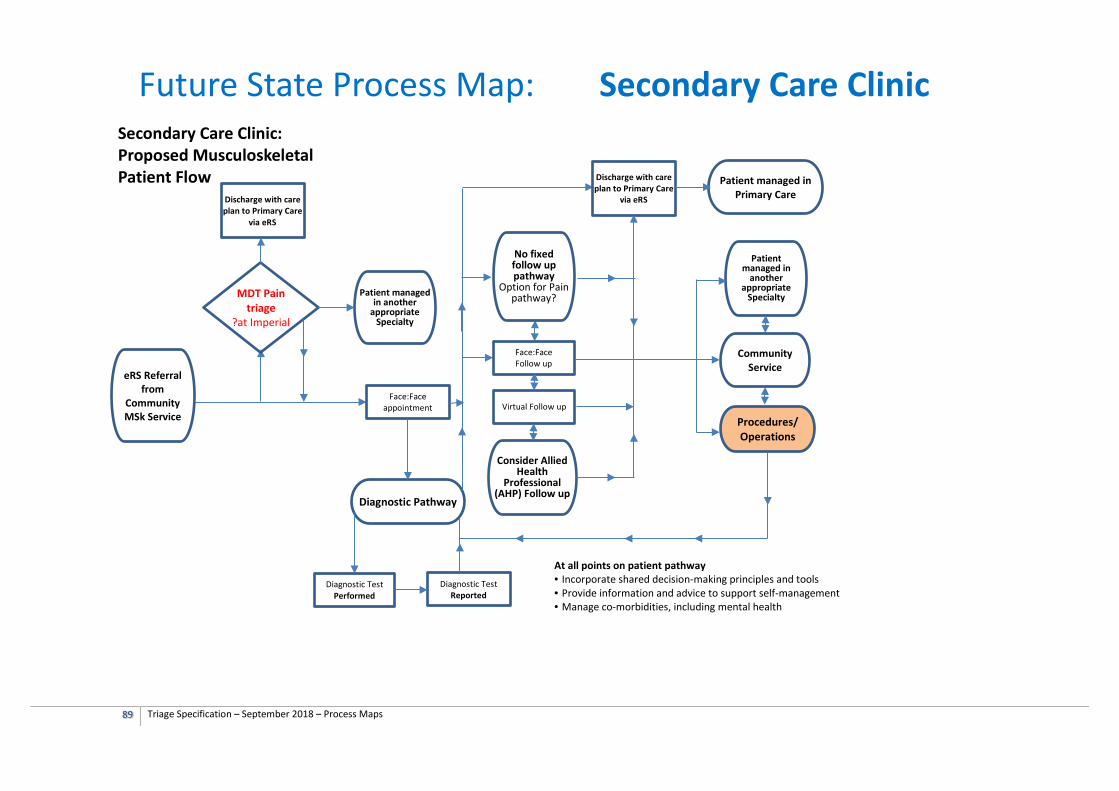
89 Triage Specification – September 2018 – Process Maps
Secondary Care Clinic: Proposed Musculoskeletal Patient Flow
Face:Face appointment
eRS Referral from
Community MSk Service
Diagnostic Pathway
Diagnostic Test Reported
Diagnostic Test Performed
Discharge with care plan to Primary Care
via eRS
Virtual Follow up
Face:Face Follow up
Patient managed in Primary Care
Procedures/ Operations
Consider Allied Health
Professional (AHP) Follow up
MDT Pain triage
?at Imperial
Patient managed in another
appropriate Specialty
No fixed follow up pathway
Option for Pain pathway?
Community Service
Patient managed in
another appropriate
Specialty
Discharge with care plan to Primary Care
via eRS
Future State Process Map: Secondary Care Clinic
At all points on patient pathway • Incorporate shared decision-making principles and tools • Provide information and advice to support self-management • Manage co-morbidities, including mental health





























