Embed Size (px)
Citation preview

Nursing Forum Volume 43, No. 2, April-June 2008 103
Blackwell Publishing IncMalden, USANUFNursing Forum0029-64731744-6198XXX
ORIGINAL ARTICLES
Musculoskeletal Problems Experienced by Older Nurses in Hospital Settings
Musculoskeletal Problems Experienced by Older Nurses in Hospital Settings
Sheila J. Cameron, RN, EdD, Marjorie Armstrong-Stassen, PhD, Debbie Kane, RN, PhD, and Francisco B. P. Moro, PhD
The effects of musculoskeletal problems on older
nurses working in hospital settings was
examined, including what contributed to the
problems, and preferred treatments selected.
Inadequate sleep was significantly related to
musculoskeletal symptoms in all regions of the
body. Most frequent problems were in lower and
upper back, neck, and shoulder areas. Rotating
and/or 12-hr shifts, inadequate sleep, frequent
patient handling, and nurses who felt little
control over their work reported more lower back
symptoms. Surprisingly, nurses relied on
over-the-counter medications to treat their
problems. Implications for supporting the nursing
workforce and minimizing musculoskeletal
problems are discussed.
Search terms:
Job conditions, musculoskeletal
problems, older nurses
Sheila J. Cameron, RN, EdD, is University Professor, Faculty of Nursing, University of Windsor; Marjorie Armstrong-Stassen, PhD, is Professor, Odette School of Business, University of Windsor; Debbie Kane, RN, PhD, is Associate Professor, Faculty of Nursing, University of Windsor; and Francisco B. P. Moro, PhD, is Assistant Professor, Odette School of Business, University of Windsor, Windsor, ON, Canada
.
T
he prevalence of back injuries among nurses iswell documented. In a review of over 80 studies,Hignett (1996) concluded that nursing is among thehigh-risk occupations with respect to lower backinjury. Nelson, Fragala, and Menzel (2003) claimedthat the prevalence of work-related back injuries innursing is among the highest of any profession inter-nationally. Far less is known about the other types ofmusculoskeletal symptoms nurses may experienceand very little of the research conducted to date hasfocused specifically on older nurses.
The changing demographics of the nursing work-force in Canada and the projected shortage of nursesindicate that older nurses will play an increasinglysignificant role in meeting hospitals’ staffing require-ments. The average age of nurses in Canada is 45 yearsand one in five nurses is over the age of 55. The largestage group, accounting for 17% of the entire regulatednursing workforce in Canada, is nurses aged 50–54years (Canadian Institute for Health Information,2006b). One way of addressing the nursing shortage isto encourage older nurses to remain in the workforce.Musculoskeletal problems are a major factor in thedecision of nurses to change jobs or to leave the nurs-ing profession altogether (Owen, 2000); therefore, theretention of older nurses will depend at least to somedegree on ensuring that they are protected frommusculoskeletal problems. Given the lack of research inthis area, we know little about the types of musculo-skeletal problems older nurses experience and thefactors that are associated with them.

104 Nursing Forum Volume 43, No. 2, April-June 2008
Musculoskeletal Problems Experienced by Older Nurses in Hospital Settings
We know little about the types of
musculoskeletal problems older nurses
experience and the factors that are
associated with them.
Incidence of Musculoskeletal Problems and Contributing Factors
Healthcare workers in Canada experience moreworkplace musculoskeletal injuries than any othermajor occupational group (Kerr et al., 2002). In a studyexamining time-loss claims of healthcare workersacross Canada between 1992 and 2002, Yassi, Gilbert,and Cvitkovich (2005) found that musculoskeletalinjuries, primarily occurring during direct patient careactivities, accounted for the majority of time-loss claims.Yassi et al. also noted that even though prevention andsafety programs had been implemented across pro-vinces, factors associated with risk of injury such asthe increased workload in an aging workforce mayhave undermined the impact of these programs. There issubstantial empirical evidence that nurses are particu-larly at risk with respect to musculoskeletal injuries,and especially lower back injuries (Lagerström,Wenemark, Hagberg, & Wigaeus Hjelmi, 1995; Maul,Läubli, Klipstein, & Krueger, 2003; Menzel, 2004;Trinkoff, Lipscomb, Geiger-Brown, & Brady, 2002).Relatively few studies have investigated the incidenceof other types of musculoskeletal injuries among nurses.Smith and Leggat (2003) reported prevalence rates of30% for neck injuries, 40% for shoulder injuries, and upto 30% for injuries to the upper back, arms, legs, andknees. Trinkoff et al. reported prevalence rates of 46%for neck problems, 35% for shoulder problems, and47% for back problems.
In a review of published studies on the relationshipof risk factors and musculoskeletal injuries in thenursing profession, Sherehiy, Karwowski, and Marek(2004) found that most of the studies examined riskfactors related to the lower back, about half as manyconcerned shoulder or neck problems, and only threestudies examined risk factors associated with musculo-skeletal problems in other parts of the body. Daraischet al. (2003) argued that the association between work-related risk factors and musculoskeletal injury may bedifferent for each body region. Various factors havebeen identified in the literature as contributing to therisk of musculoskeletal injury. The factors we focusedon were those associated with the job; that is, aspectsof shift work, patient-handling tasks, and control overone’s work. We examined the association of reportedincidence of musculoskeletal problems with lengthof shift (8 or 12 hr), type of shift (rotating or fixed), andinadequate sleep. Few studies have examined theimpact of working long hours on workers’ risk foroccupational injuries (Dembe, Erickson, Delbos, &Banks, 2005). Dembe et al. found that working at least12 hr per day was associated with increased risk foroccupational injuries. Smith, Colligan, Frockt, andTasto (1979) found that nurses on a rotating shiftschedule had significantly more injuries than nurseson a fixed shift schedule. These researchers suggestedthat the greater fatigue experienced by rotating shiftnurses may put these nurses at more risk of experienc-ing injuries. Gold et al. (1992) found that nurses on arotating shift reported fewer hours of sleep and experi-enced more accidents than nurses on fixed shifts.Trinkoff et al. (2002) also found a significant relationshipbetween inadequate sleep and musculoskeletal injuries.
Smith and Leggat (2003) contended that manualhandling of patients is the most important risk factorin the development of musculoskeletal injury amongnurses. Repositioning a patient in bed is the mostcommonly reported activity associated with musculo-skeletal injury (Fragala & Pontani Bailey, 2003;Harber et al., 1985; Leighton & Reilly, 1995) althoughhelping patients out of bed is also commonly reported

Nursing Forum Volume 43, No. 2, April-June 2008 105
(Harber et al.; Smedley, Egger, Cooper, & Coggon, 1997;Yassi et al., 1995). Smith and Leggat noted that thefrequency of performing these patient-handling tasksis important. Nurses who perform these tasks morefrequently are at greater risk of musculoskeletal injury.
Dembe et al. found that working at least
12 hr per day was associated with increased
risk for occupational injuries.
There is some empirical evidence that low jobcontrol is associated with increased risk of experiencinga musculoskeletal injury (Bongers, de Winter, Kompier,& Hildebrandt, 1993; Hollmann, Heuer, & Schmidt,2001; Lagerström et al., 1995). In their review, Sherehiyet al. (2004) noted that the findings for job control as arisk factor are “somewhat ambiguous” (p. 260) becausenot all studies have shown a significant relationshipbetween job control and musculoskeletal injury. Someresearchers have found job control related to some typesof musculoskeletal injuries but not to others. Lagerströmet al. found low job control related to shoulder symptomsbut not to neck, low back, hand, or knee symptoms.
We found only two studies that have investigatedthe relationship between musculoskeletal injuryand nurses’ ability to perform their job. Leighton andReilly (1995) reported that over half of the nursesexperiencing back pain indicated that the back painmade performing their work slightly more difficultbut they could still continue performing all of theirduties. Trinkoff et al. (2002) found that nurses withmore severe musculoskeletal injuries were signifi-cantly more likely to modify their job duties than nurseswith less severe symptoms. Another area that has beenlargely unexplored is the treatment nurses seek whenthey do experience a musculoskeletal injury. Harber
et al. (1985) suggested that nurses as healthcare profes-sionals may “treat themselves” or seek informalphysician consultation. Trinkoff et al. found that nurseswith more severe musculoskeletal injuries weresignificantly more likely to report seeing a doctor orother health provider than nurses with less seriousinjuries.
Age may or may not be a contributing factor tomusculoskeletal injury. Age has been found to beassociated with neck, shoulder, hand, or knee symp-toms (Lagerström et al., 1995), arm or leg complaints(Engels, van der Gulden, Senden, & van’t Hoff, 1996),and back pain (Leighton & Reilly, 1995). Other researchers(Ando et al., 2000; Menzel, Brooks, Bernard, & Nelson,2004; Smedley et al., 1997; Venning, Walter, & Stitt, 1987)have found no significant relationship between ageand musculoskeletal injuries. There is, however, theassumption that the aging of the nursing workforcewill be a risk factor for musculoskeletal injury (Smith& Leggat, 2003). Kerr et al. (2002) noted that musculo-skeletal injuries like back pain and neck or shoulderpain are age related, particularly in relation to theduration of time off work to recuperate from such aninjury. Using Statistics Canada Labour Force Surveydata, the Canadian Nurses Association (2006) foundthat the illness and injury-related absenteeism rateamong nurses under 45 years of age declined between2002 and 2005, whereas there was an increase in theabsenteeism rate among nurses 55 and over duringthis same period. Fragala and Pontani Bailey (2003)argued that patient-handling tasks provide even greaterrisks to the aging healthcare workforce and older nurseswill not be equipped, from a physical perspective, toperform these tasks.
Research Questions
The purpose of the present study was to addressthe following research questions:
1. What types of musculoskeletal problems are oldernurses most likely to experience?

106 Nursing Forum Volume 43, No. 2, April-June 2008
Musculoskeletal Problems Experienced by Older Nurses in Hospital Settings
2. How are the job-related factors associated with theoccurrence of musculoskeletal problems amongolder nurses?
3. How do musculoskeletal problems impact theability of older nurses to perform their jobs?
4. What are older nurses’ treatments of choice formusculoskeletal problems?
What types of musculoskeletal problems
are older nurses most likely to experience?
Method
The research design of this study was a cross-sectional descriptive field study employing bothquestionnaires and interviews.
Sample
The names and mailing addresses of registerednurses were obtained from the College of Nurses ofOntario. After limiting the database to registered nursesaged 45 and over who were employed in hospitalsin southwestern Ontario, the College of Nursesrandomly selected the names of 500 registered nurses.A total of 303 registered nurses participated in thisstudy. Their ages ranged from 45 to 63 years with anaverage age of 51.55 years (
SD
= 3.95). They had beenemployed in their current job positions an average of15.97 years (
SD
= 9.86) and in their current workplacean average of 20.84 years (
SD
= 8.83). Most were women(96%) and married (75%). The majority (97%) wereemployed in permanent full-time positions on a widevariety of units, including medical/surgical (20%), psy-chiatry (13%), obstetrics/neonatal (11%), intensive care/coronary care (11%), operating room/recovery (8%),oncology (3%), and continuing care/geriatrics (2%), and
32% were on other units such as emergency room andpediatrics. Thirty-five nurses participated in the inter-views designed to further explore issues raised in theresponses to the questionnaires. Twenty-five of thenurses interviewed were between the ages of 45 and55, and 10 of those interviewed were between the agesof 56 and 63. These numbers were representative ofthe age distribution of the nurses who had completedthe questionnaire, with 84% being between 45 and 55,and 16% being 56 and older.
Data Collection Procedures
The protocol for this study was approved by theuniversity’s research ethics board. Questionnairepackets containing a cover letter from the researchers,a letter of information for consent to participate inresearch, a questionnaire booklet, and a business replyenvelope for the return of the completed questionnairewere mailed to the randomly selected sample of 500registered nurses. The packets also contained a requestform and a separate envelope for those who wishedto participate in an interview. Three weeks later weconducted a follow-up mail out to those nurses who hadnot yet responded. An identification number was includedon the business reply envelope but the questionnaireitself was anonymous. We received 303 completed ques-tionnaires, 2 incomplete questionnaires which werediscarded, and 4 questionnaire packets which couldnot be delivered. The response rate was 61.5%. Thetelephone interviews were conducted by the project’sresearch coordinator who is also a registered nurse.
Instruments
Most of the questionnaire measures were developedspecifically for this study. To assess the level and typeof work-related musculoskeletal symptom nurses wereexperiencing, we asked “How often have you experiencedjob-related pain or discomfort in the following parts ofyour body in the past 12 months?” There were 11 partsof the body listed: neck, shoulder, upper back, lower

Nursing Forum Volume 43, No. 2, April-June 2008 107
back, upper arm, forearm/elbow, wrists, hands/fingers,thigh/knee, lower leg, and ankle/foot. The responsecategories were
almost never
(two times a year at most),
rarely
(every 2–3 months),
sometimes
(once a month),
frequently
(once a week), and
almost always
(daily).To assess whether and how much those work-relatedproblems nurses were experiencing more than rarelyinterfered with their job performance, we asked “Foreach of the musculoskeletal symptoms that you areexperiencing more than rarely, please indicate theextent to which this interferes with your ability toperform your job.” The same 11 parts of the body werelisted and the response categories ranged from 1 (Notat all) to 5 (A great deal). Respondents were thenasked to indicate what type of treatment they hadsought for each of the musculoskeletal symptoms thatthey were experiencing more than rarely. The types oftreatment were over-the-counter medications, physician,chiropractor, physiotherapist, and other (here a spacewas left and they were asked to specify the treatment).Respondents were instructed to check all that applied.
Respondents were asked to provide informationabout themselves (age, gender, marital status), abouttheir job (full-time or part-time status, unit wherespend most of their working time, and length of timeemployed in their current position), and about theirorganization (size, location, and number of yearsemployed in the hospital). They were also asked toidentify the shift they generally worked (8 or 12 hr)and the type of shift (rotating or fixed). We developeda two-item scale to assess sleep adequacy. One itemasked “How would you describe the quality of yoursleep?” The responses ranged from 1 (Very poor) to 5(Very good). The second item asked them approximatelyhow many hours of sleep they got daily. The responsesranged from 1 (Less than 5 hr) to 5 (More than 7 hr).The reliability coefficient (Cronbach alpha) was .79.Frequency of patient-handling tasks was assessed withfour items: “Repositioning patients in bed [turningand lifting patients up in bed],” “Transferring patientsbetween beds and chairs or stretchers,” “Making beds,”and “Pushing beds, stretchers or wheelchairs.” Respond-
ents were asked to indicate how much time in a daythey spent on these activities. The response categoriesranged from 1 (Not part of daily activities) to 5 (4 hr ormore). The Cronbach alpha was .90. We assessed jobcontrol with the 11-item job control measure developedby Greenberger (1982). Sample items are “How muchinfluence do you have over how you do your work?”and “How much influence do you have over the physicalconditions of your work stations (e.g., lighting, tem-perature)?” The response categories ranged from 1 (Noinfluence at all) to 5 (A great deal of influence). Cronbachalpha was .94.
We also developed the interview questions specifi-cally for this study. The interview began with a filteringquestion asking if the interviewees had experienced orsustained any work-related musculoskeletal problemsduring their nursing career. If the interviewees answeredyes to this question, they were asked to describe thenature of the problems and the circumstances. Thiswas followed up with questions about how they hadbeen affected by the problems and if age had contributedin any way to their symptoms. If interviewees had notexperienced a work-related problem, they were askedif they were aware of any staff in their work area or ontheir unit who had experienced a work-related musculo-skeletal problem. If yes, they were asked to describethe nature of the problem and the circumstances. Wealso inquired if they could identify any factors theyfelt had contributed to their own lack of problems.
Data Analysis
The questionnaire data were analyzed using fre-quencies and Pearson product–moment correlationanalysis. Content analysis was used to identify the majorthemes/trends in the interview data.
Findings
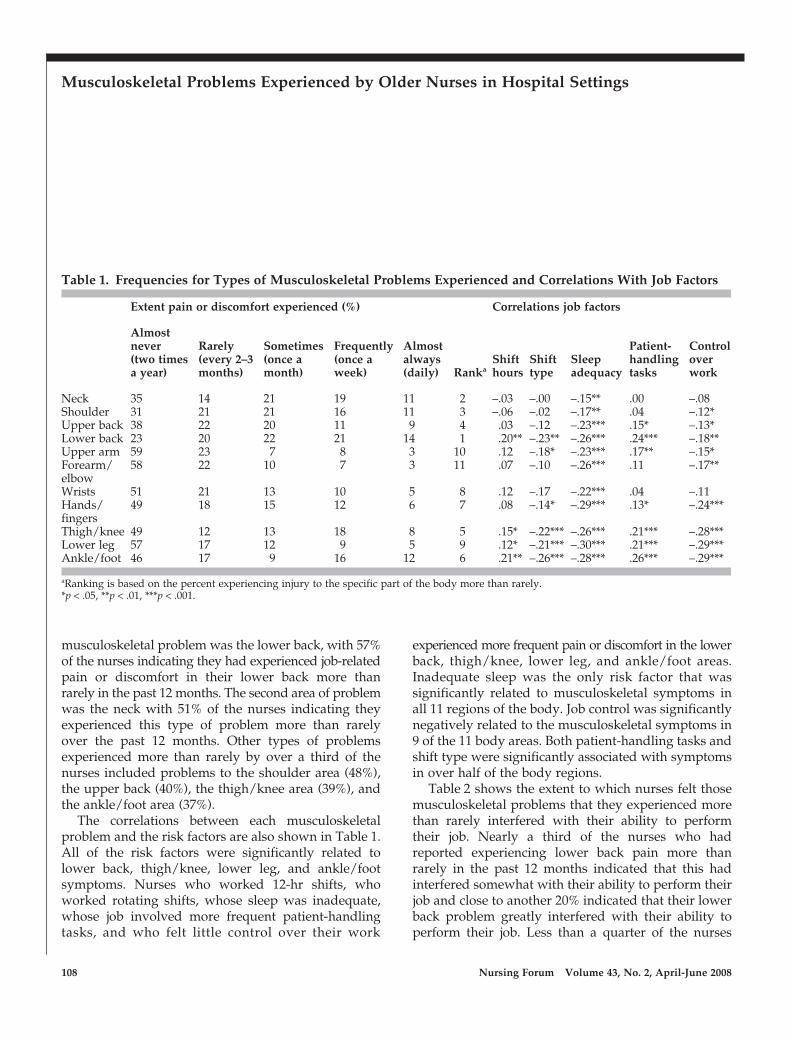
The frequencies for the types of work-relatedmusculoskeletal problems nurses experienced are pre-sented in Table 1. The most frequently experienced
108 Nursing Forum Volume 43, No. 2, April-June 2008
Musculoskeletal Problems Experienced by Older Nurses in Hospital Settings
musculoskeletal problem was the lower back, with 57%of the nurses indicating they had experienced job-relatedpain or discomfort in their lower back more thanrarely in the past 12 months. The second area of problemwas the neck with 51% of the nurses indicating theyexperienced this type of problem more than rarelyover the past 12 months. Other types of problemsexperienced more than rarely by over a third of thenurses included problems to the shoulder area (48%),the upper back (40%), the thigh/knee area (39%), andthe ankle/foot area (37%).
The correlations between each musculoskeletalproblem and the risk factors are also shown in Table 1.All of the risk factors were significantly related tolower back, thigh/knee, lower leg, and ankle/footsymptoms. Nurses who worked 12-hr shifts, whoworked rotating shifts, whose sleep was inadequate,whose job involved more frequent patient-handlingtasks, and who felt little control over their work
experienced more frequent pain or discomfort in the lowerback, thigh/knee, lower leg, and ankle/foot areas.Inadequate sleep was the only risk factor that wassignificantly related to musculoskeletal symptoms inall 11 regions of the body. Job control was significantlynegatively related to the musculoskeletal symptoms in9 of the 11 body areas. Both patient-handling tasks andshift type were significantly associated with symptomsin over half of the body regions.
Table 2 shows the extent to which nurses felt thosemusculoskeletal problems that they experienced morethan rarely interfered with their ability to performtheir job. Nearly a third of the nurses who hadreported experiencing lower back pain more thanrarely in the past 12 months indicated that this hadinterfered somewhat with their ability to perform theirjob and close to another 20% indicated that their lowerback problem greatly interfered with their ability toperform their job. Less than a quarter of the nurses
Table 1. Frequencies for Types of Musculoskeletal Problems Experienced and Correlations With Job Factors
Extent pain or discomfort experienced (%)
Ranka
Correlations job factors
Almost never (two times a year)
Rarely (every 2–3 months)
Sometimes (once a month)
Frequently (once a week)
Almost always (daily)
Shift hours
Shift type
Sleep adequacy
Patient-handling tasks
Control over work
Neck 35 14 21 19 11 2 –.03 –.00 –.15** .00 –.08Shoulder 31 21 21 16 11 3 –.06 –.02 –.17** .04 –.12*Upper back 38 22 20 11 9 4 .03 –.12 –.23*** .15* –.13*Lower back 23 20 22 21 14 1 .20** –.23** –.26*** .24*** –.18**Upper arm 59 23 7 8 3 10 .12 –.18* –.23*** .17** –.15*Forearm/elbow
58 22 10 7 3 11 .07 –.10 –.26*** .11 –.17**
Wrists 51 21 13 10 5 8 .12 –.17 –.22*** .04 –.11Hands/fingers
49 18 15 12 6 7 .08 –.14* –.29*** .13* –.24***
Thigh/knee 49 12 13 18 8 5 .15* –.22*** –.26*** .21*** –.28***Lower leg 57 17 12 9 5 9 .12* –.21*** –.30*** .21*** –.29***Ankle/foot 46 17 9 16 12 6 .21** –.26*** –.28*** .26*** –.29***
aRanking is based on the percent experiencing injury to the specific part of the body more than rarely.*p < .05, **p < .01, ***p < .001.

Nursing Forum Volume 43, No. 2, April-June 2008 109
who reported experiencing a lower back problemindicated that their pain did not interfere with theirability to perform their job. Almost half of the nurseswho reported experiencing problems to their thigh/knee and ankle/foot areas indicated that theseproblems interfered at least somewhat with theirability to perform their job. Other types of injuries thathad more than a minimal effect on nurses’ ability toperform their job were injuries to the hands/fingers(40%), lower leg (40%), forearm/elbow (38%), wrists(37%), and shoulder (34%). Even for the problemhaving the least effect on performance, neck injury,over a quarter of the nurses indicated that this hadinterfered at least somewhat with their ability toperform their job.
Table 3 presents the types of treatment nurses soughtfor their problems. The majority of nurses relied onover-the-counter medications to treat these problems.In addition to using over-the-counter medications,they were most likely to seek treatment from a physicianwhen the problem involved the ankle/foot, lower back,and shoulder areas. About a third also sought treatmentfrom a physiotherapist for problems with the neck,shoulder, and lower back.
The most frequently experienced
musculoskeletal problem was the lower
back, with 57% of the nurses indicating they
had experienced job-related pain or
discomfort in their lower back more than
rarely in the past 12 months.
Interview Findings
Almost two thirds (63%) of nurses in the 45–55 agegroup and 70% of nurses in the 56 and over age groupreported having personally experienced a muscu-loskeletal problem at work. All nurses who had notpersonally experienced a work-related problem knewof colleagues who had experienced musculoskeletal
Table 2. Extent Frequently Experienced Musculoskeletal Problems Interfere With Ability to Perform the Job
Interference with job performance (%)
Not at all A little Somewhat Quite a lot A great deal
Neck 37 35 22 5 1Shoulder 37 29 23 10 1Upper back 37 31 24 7 1Lower back 22 27 32 15 4Upper arm 48 19 23 6 4Forearm/elbow 31 31 28 6 4Wrists 33 30 24 8 5Hands/fingers 23 36 23 13 4Thigh/knee 24 30 32 10 4Lower leg 33 27 36 3 1Ankle/Foot 28 25 33 10 4

110 Nursing Forum Volume 43, No. 2, April-June 2008
Musculoskeletal Problems Experienced by Older Nurses in Hospital Settings
problems at work. The most frequent type of problemmirrored those found for the questionnaire data withback, neck, and shoulders followed by hips, ankles,and feet being most prevalent. When discussing howthe problems occurred, two main themes emerged:those caused by lifting, moving, and transferring patients,and those caused by patients who were either men-tally ill or who were experiencing agitation and/orconfusion related to their condition. Increased patientage and morbidity combined with people with mentaldisturbance meant it was increasingly likely thatnurses would experience a problem in the workplace.
Physical demands . . . they’re increasingly heavy . . .with our aging population . . . obesity . . . and staffinglevels [not] what they should be . . . the shift work isdraining . . . in an emergency department it is emo-tionally demanding especially with the workload.
I had a twisting injury to my right arm by a patientbecause of their electrolyte imbalance . . . then he laterattacked two nurses and tried throwing us out of awindow . . . I ended up with lacerations and abrasions.
Most nurses were off work from a few weeks to1–2 months, although one nurse reported returning towork after a 2-year absence. Approximately 15% hadnot returned to work and cited chronic pain and ensuingtreatment as reasons they did not return.
Nurses talked of the impact that musculoskeletalproblems had had on their lives. Over 50% reportedbeing financially affected when they were receivingworkers’ compensation while on disability, althoughothers were paid full sick leave. When nurses returnedto work following a problem, many returned initiallyto modified assignments. Those who returned to theirregular duties stated that their unit colleagues wereoften accommodating to ensure they were not undulystressed by their work duties. Some felt guilty whenthis meant their colleagues were taking on additionalduties.
Nurses were also concerned about 12-hr shifts,having to work too many shifts “back-to-back” as wellas increasing difficulty sleeping when shift rotationswere frequent. One nurse when talking about “younger”nurses felt that younger nurses took better care ofthemselves than many of the older nurses.
Table 3. Type of Treatment Sought for Musculoskeletal Problems Experienced More Than Rarely
Type of treatment (%)
OTC medications Physician Chiropractor Physiotherapist Othera
Neck 65 34 23 34 24Shoulder 57 36 21 33 22Upper back 53 31 24 24 21Lower back 64 37 27 32 19Upper arm 46 19 8 23 8Forearm/elbow 50 34 4 20 20Wrists 45 28 5 16 21Hands/fingers 43 30 3 8 11Thigh/knee 62 36 12 23 19Lower leg 50 22 3 5 12Ankle/Foot 54 40 6 16 23
aThe written responses to this category covered a wide variety of treatments including acupuncture, rest, meditation/relaxation/yoga, exercise such as swimming and Pilates, wearing support hose/splint/wrist support, and changing nursing assignments.The percentages exceed 100% because respondents were instructed to check all the treatments that they sought for the specific injury.

Nursing Forum Volume 43, No. 2, April-June 2008 111
It’s interesting how they prefer to work reducedtime because they find it so physically demandingand if asked to do overtime they’ll say “no, I’m tootired and I’ll make myself sick.” We can learn fromthat generation. They take better care of themselvesthan we do.
Nurses who had not experienced a problem them-selves attributed this to several factors. Their hospitalshad in place Health and Safety committees, offeredWellness Programs for staff, and provided goodorientation programs with emphasis on good bodymechanics. Several nurses noted their hospitals werebecoming more proactive rather than reactive regard-ing workplace health and safety. On a personal level,many in this group reported “good” work habits withadequate rest, good body mechanics, and appropriatefootwear as well as having a supportive spouse asimportant factors in their personal health.
I think it’s more important to have . . . the balancebetween family and friends. It sounds so basic . . .but you have to have a good . . . you know happy . . .stable life to be able to do your job . . . get enoughsleep . . . and stay healthy.
One nurse when talking about “younger”
nurses felt that younger nurses took better
care of themselves than many of the older
nurses.
Discussion and Implications
This study contributes to our existing knowledge ofthe nursing profession and work-related musculoskeletal
problems in several respects. The study focuses onolder nurses, an important consideration given theaging of the nursing workforce in Canada and othercountries. Unlike many studies, we did not limit ourstudy to back-related problems but instead examinedthe frequency of occurrence of musculoskeletal symp-toms for 11 different regions of the body. We alsolooked at the job-related risk factors that may contributeto musculoskeletal problems. Some of these, such asjob control, have not been widely studied in this con-text and few, if any, studies have included all of thesejob-related risk factors in the same study. Our studygoes beyond determining the extent older nursesexperience workplace musculoskeletal problems byexamining the impact they have on nurses’ ability toperform their job and the type of treatment sought bynurses.
The most recent report from the Canadian Institutefor Health Information (2006a), released in December2006, found that 33.8% of female nurses reported atleast one musculoskeletal condition and that one thirdof nurses working in hospitals and long-term carefacilities reported health difficulties. This percentage ishigher than statistics from the general population offemale workers and also higher than other nurses incommunity and clinic settings. Our findings furtherillustrate that the problem is significant in oldernurses.
The older age of nurses in our study represented45- to 65-year-old women, and in this random samplethe drop off of subjects over age 55 was significant.Only one third of the sample continued working pastthe age of 55 years and after 60 years of age only 5%remained in the workforce. This has obvious implica-tions for us in Canada where the nursing shortage isprojected to be over 113,000 by 2016 (Oulton, 2006).The Canadian Institute for Health Information (2006b)also reported that if nurses continue to retire at 55rather than 65 years of age, then projected losses indi-cate we will lose 64,258 nurses or a quarter of the 2001nursing workforce by the end of 2006. If ways can befound to support the older nurse to remain at work,

112 Nursing Forum Volume 43, No. 2, April-June 2008
Musculoskeletal Problems Experienced by Older Nurses in Hospital Settings
this has the potential to impact positively on the work-force. Consequently, all efforts to retain and supportnurses can significantly impact on the supply ofnurses available in Canada over the next decade.
Whereas the literature on back problems for nursesis relatively well known, knowledge about other typesof musculoskeletal problems are not. In our sample,over 40% of the nurses experienced symptoms fromneck/shoulder, and upper and lower back problems,with 38% reporting ankle/foot and knee injuries oncea month. Hospital wellness programs designed to sup-port good ergonomic practices to alleviate stress andstrain on these regions of the body will be of particularbenefit to this workforce. At times lifting equipmentmay be of value to minimize injury; however, makingnurses aware of how vulnerable certain joints are toinjury and how they may be protected through goodergonomic practices may be of particular value whenpreserving health. O’Brien-Pallas, Duffield, and Alksnis(2004) also suggested that providing bonus money forthe gym may have particular value for older nurseswho may no longer need child-care services or educa-tional incentives but who may benefit themselves andtheir institution by having additional health supportsuch as a regular exercise program.
Hospital nurses in our sample also reported moreproblems managing their workload due to patientmental health issues. This finding was reported to usduring the interview phase of our research whennurses talked of the “stresses” of their jobs, and thatin recent years stress had been compounded by theincreasing acuity of hospitalized patients, as well asthe increased age of patients requiring care. In a reviewof studies exploring the link between psychosocialfactors and musculoskeletal injury, Bongers et al. (1993)found that high perceived workload, time pressures,as well as stress symptoms were all positively linkedwith musculoskeletal disease. It is apparent that anyprograms developed for nurses to work towardsminimizing musculoskeletal problems at work need toalso consider psychosocial issues and stressors beingexperienced.
The job-related factors associated with these prob-lems are clearly evident in this investigation. Sleepadequacy was highly related to problems experienced;less sleep was positively correlated with every type ofproblem examined. Rotating shift type and 12-hr shiftswere both correlated with lower back, ankle/foot, lowerleg, and thigh/knee problems. These findings haveparticular significance for mid-career to older nurses.The work of Gold et al. (1992) clearly indicated theimpact of sleep loss of nurses who worked rotatingshifts. Nurses who worked days/afternoons and nightswere classified as working rotating shifts and hadtwice the odds of almost falling asleep while driving,and twice the odds of a reported accident or perform-ance error related to sleepiness. It appears likely thatlapsed attention such as that described could alsoresult in personal injury and although it was notexamined in our study it should be considered infuture research of this type. Dembe et al. (2005) alsoreported that injury rates were higher with overtimeand increased with 12-hr workdays, and the CanadianNurses Association report (2006) on trends in illnessand injury-related absenteeism found that both increasedin Canadian nurses over 45 years of age and in thoseworking overtime at their place of employment. It isapparent that closer examination of shift rotations,overtime, and illness may enable employers to assisttheir staff to avert illness and injury especially as nursesage. While the difficulties of maintaining any workforce 24/7 is challenging, exploring alternate staffingmodels and providing a range of options for full- andpart-time work need ongoing testing and study.
Hospital nurses in our sample also reported
more problems managing their workload
due to patient mental health issues.

Nursing Forum Volume 43, No. 2, April-June 2008 113
The issue of treating oneself with over-the-countermedications suggests that these drugs may make thepain manageable; however, this will do little to pre-vent or avert further problems. Workplace wellnessprograms and opportunities for further assessment bypractitioners such as physiotherapists, chiropractors,and physicians could all help to minimize the effectsof the musculoskeletal problems in the future.
The findings in this study illustrate some of thecritical issues relating to musculoskeletal problemsthat need to be addressed in the hospital workplace,particularly as we are witnessing that as nurses increasein age they tend to leave their employment at least adecade before other workers normally leave. Futureresearch to determine if there is a link betweenmusculoskeletal problems and age of retirement wouldbe useful.
Author contact: [email protected], with a copy to theEditor: [email protected]
References
Ando, S., Ono, Y., Shimaoka, M., Hiruta, S., Hattari, Y., Hori, F.,et al. (2000). Associations of self estimated workloads withmusculoskeletal symptoms among hospital nurses.
Occupationaland Environmental Medicine
,
57
, 211–216.Bongers, P. M., de Winter, C. R., Kompier, M. A. J., & Hildebrandt,
V. H. (1993). Psychosocial factors at work and musculoskeletaldisease.
Scandinavian Journal of Work and Environmental Health
,
19
,297–312.
Canadian Institute for Health Information. (2006a).
Findings from the2005 national survey of the work and health of nurses
. Ottawa:Author.
Canadian Institute for Health Information. (2006b).
Highlights fromthe regulated nursing workforce in Canada
,
2005: Preliminary report
.Ottawa: Author.
Canadian Nurses Association. (2006).
Trends in illness and injury-relatedabsenteeism and overtime among publicly employed registered nurses
.Ottawa: Author.
Daraisch, N., Genaidy, A. M., Karwowski, W., Davis, L. S., Stam-bough, J., & Huston, R. L. (2003). Musculoskeletal outcomes inmultiple body regions and work effects among nurses: The effectsof stressful and stimulating working conditions.
Ergonomics
,
46
,1178–1199.
Dembe, A. E., Erickson, J. B., Delbos, R. G., & Banks, S. M. (2005).The impact of overtime and long work hours on occupationalinjuries and illnesses: New evidence from the United States.
Occupational and Environmental Medicine
,
62
, 588–597.
Engels, J. A., van der Gulden, J. W. J., Senden, T. F., & van’t Hoff, B.(1996). Work related risk factors for musculoskeletal complaintsin the nursing profession: Results of a questionnaire survey.
Occupational and Environmental Medicine
,
53
, 636–641.Fragala, G., & Pontani Bailey, L. (2003). Addressing occupational
strains and sprains: Musculoskeletal injuries in hospitals.
AAOHNJournal
,
51
, 252–259.Gold, D. R., Rogacz, S., Bock, N., Tosteson, T. D., Baum, T. H.,
Speizer, F. E., et al. (1992). Rotating shift work, sleep, and acci-dents related to sleepiness in hospital nurses.
American Journal ofPublic Health
,
82
, 1011–1014.Greenberger, D. B. (1982).
Personal control at work: Its conceptualiza-tion and measurement
. Office of Naval Research Technical Report1-1-4-1982. Madison, WI: University of Wisconsin.
Harber, P., Billet, E., Gutowski, M., SooHoo, K., Lew, M., & Roman, A.(1985). Occupational low-back pain in hospital nurses.
Journal ofOccupational Medicine
,
27
, 518–524.Hignett, S. (1996). Work-related back pain in nurses.
Journal of AdvancedNursing
,
23
, 1238–1246.Hollmann, S., Heuer, H., & Schmidt, K.-H. (2001). Control at work: A
generalized resource factor for the prevention of musculoskeletalsymptoms?
Work and Stress
,
15
, 29–39.Kerr, M., Laschinger, H., Severin, C., Almost, J., Thomson, D.,
O’Brien-Pallas, L., et al. (2002).
Monitoring the health of nursesin Canada
. Ottawa: Canadian Health Services ResearchFoundation.
Lagerström, M., Wenemark, M., Hagberg, M., & Wigaeus Hjelmi, E.(1995). Occupational and individual factors related to musculo-skeletal symptoms in five body regions among Swedishnursing personnel.
International Archives Occupational EnvironmentalHealth
,
68
, 27–35.Leighton, D. J., & Reilly, T. (1995). Epidemiological aspects of back
pain: The incidence and prevalence of back pain in nursescompared to the general population.
Occupational Medicine
,
45
,263–267.
Maul, I., Läubli, T., Klipstein, A., & Krueger, H. (2003). Course oflow back pain among nurses: A longitudinal study across eightyears.
Occupational and Environmental Medicine
,
60
, 497–503.Menzel, N. N. (2004). Back pain prevalence in nursing personnel:
Measurement issues.
AAOHN Journal
,
52
, 54–65.Menzel, N. N., Brooks, S. M., Bernard, T. E., & Nelson, A. (2004).
The physical workload of nursing personnel: Association withmusculoskeletal discomfort.
International Journal of Nursing Studies
,
41
, 859–867.Nelson, A., Fragala, G., & Menzel, N. (2003). Myths and facts about
back injuries in nursing.
American Journal of Nursing
,
103
(2), 32–40.
O’Brien-Pallas, L., Duffield, C., & Alksnis, C. (2004). Who will therebe to nurse? Retention of nurses nearing retirement.
Journal ofNursing Administration
,
34
, 298–302.Oulton, J. A. (2006). The global nursing shortage: An overview of
issues and actions.
Policy, Politics, & Nursing Practice
,
7
(3 Suppl.),34S–39S.
Owen, B. D. (2000). Preventing injuries using an ergonomicapproach.
AORN Journal
,
72
, 1031–1036.Sherehiy, B., Karwowski, W., & Marek, T. (2004). Relationship between

114 Nursing Forum Volume 43, No. 2, April-June 2008
Musculoskeletal Problems Experienced by Older Nurses in Hospital Settings
risk factors and musculoskeletal disorders in the nursing profession:A systematic review.
Occupational Ergonomics
,
4
, 241–279.Smedley, J., Egger, P., Cooper, C., & Coggon, D. (1997). Prospective
cohort study of predictors of incident low back pain in nurses.
British Medical Journal
,
314
, 1225–1228.Smith, D., & Leggat, P. (2003). Musculoskeletal disorders in nursing.
Australian Nursing Journal
,
11
, CU1–CU3.Smith, M. J., Colligan, M. J., Frockt, I. J., & Tasto, D. L. (1979). Occu-
pational injury rates among nurses as a function of shift schedule.
Journal of Safety Research
,
11
, 181–187.Trinkoff, A. M., Lipscomb, J. A., Geiger-Brown, J., & Brady, B.
(2002). Musculoskeletal problems of the neck, shoulder, and back
and functional consequences in nurses.
American Journal ofIndustrial Medicine
,
41
, 170–178.Venning, P. J., Walter, S. D., & Stitt, L. W. (1987). Personal and job-related
factors as determinants of incidence of back injuries amongnursing personnel.
Journal of Occupational Medicine
,
29
, 820–825.Yassi, A., Gilbert, M., & Cvitkovich, Y. (2005). Trends in injuries,
illnesses, and policies in Canadian healthcare workplaces.
CanadianJournal of Public Health
,
96
, 333–339.Yassi, A., Khokhar, J., Tate, R., Cooper, J., Snow, C., & Vallentyne, S.
(1995). The epidemiology of back injuries in nurses at a largeCanadian tertiary care hospital: Implications for prevention.
Occupational Medicine
,
45
, 215–220.





























