Embed Size (px)
Citation preview

MY JOURNEY TO SUDAN
Author: Sue Witt, RN, BN, Pieri, South Sudan, and Calgary, Alberta, CanadaSection Editors: Pat Clutter, RN, MEd, CEN, FAEN, and Carole Rush, RN, MEd, CEN, FAEN
I am sitting by my fireplace at home in Canada, listen-ing to the trucks go by outside, wondering if I reallydid survive 9 months living in a mud hut. So much
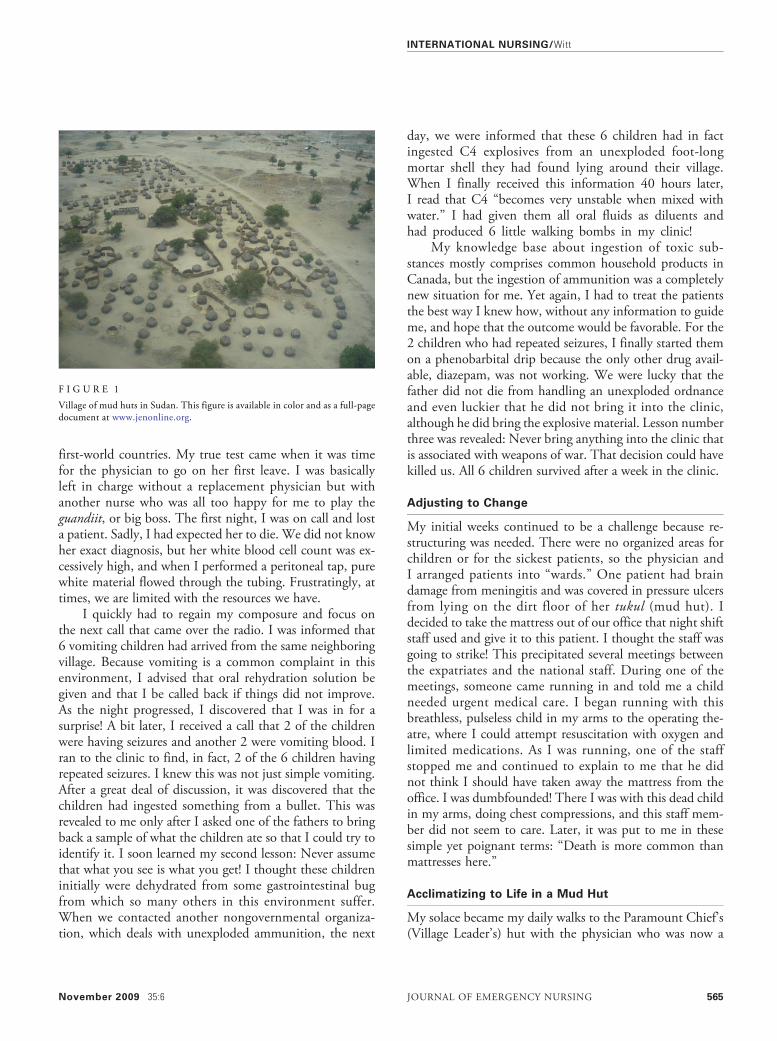
happened during that time; I close my eyes, and it is likeI am there—the smell of acacia trees burning to ward off arival tribe, the sound of donkeys baying, and the hundredsof birds that would flock to the tree above our shower andsquawk all night. People are singing somewhere. I close myeyes again, and even now I hear the gunfire. So much ofthese sounds had become my lullaby at night. I had trav-eled back a thousand years in time to a little place on thisearth that was unknown to many and forgotten by most(Figure 1) but not by Médecins Sans Frontières (MSF), asecular humanitarian-aid, nongovernmental organizationbest known for its projects in war-torn regions and devel-oping countries facing endemic disease.1 The organizationis known in most of the world by its French name orsimply as MSF, but in the United States and Canada thename Doctors Without Borders is often used instead.
When I graduated high school, I did not know what Iwanted to do with my life until I saw a nurse during somenews footage covering the Rwandan Genocide. She was onthe frontlines working with MSF in a refugee camp. I couldnot believe that nurses could do such great work in theircareers; I knew then that I wanted to continue these efforts.
Preparation for Work With MSF
To gain more professional and volunteer experience beforeapplying to MSF, I spent the 6 years after nursing schoolgraduation in a variety of environments. I had discoveredthat it was advantageous to have overseas experience andthat taking an offered course in London, though not man-datory, would be an asset in achieving an appointment.Table 1 outlines these experiences to make my curriculumvitae more attractive for any prospective field placements.
Seven months after MSF training in Amsterdam, I finallyreceived the important phone call for a placement matchand found out that I would be leaving within the week!This one moment would change the course of my life for-ever…. It was the beginning of my journey to Sudan….
Preparing to leave was a flurry of paperwork andappointments. Before I knew it, with tears in my eyes, Iwas walking through the departure gate at the airport,waving to my younger sister and mother. I did not knowwhether this would be our last goodbye. Although thevillage I was going to was in the post-conflict stage, therewas still active fighting between different clans; MSF isoften caught in the middle of violence.
Arrival at MSF Headquarters in Kenya
After a small briefing in Amsterdam, I was flown toLokichoggio (Loki), Kenya, to the MSF compound head-quarters for South Sudan for more briefings. During mytime with the Medical Coordinator (Medco), I learned thatI would not be getting the handover in the field from theexiting nurse as planned. Because of rains and mud, wecould not reach each other! The implications of this situa-tion were very worrisome; I would not be receiving anorientation to my role in the field and would have to relyon the other medics and the national staff, whom I wouldsupervise, for my introduction. I was told that I would bein charge of running the inpatient department, which cur-rently had 88 patients admitted! The cases included chil-dren with measles, severe pneumonia, and snakebites, aswell as other severe medical cases in patients of all ages.
Arrival in the Field and Lessons Learned
As I arrived on the airstrip, I quickly learned the commongreeting male (hello), pronounced mall-eh. Walking to thecompound, I saw a young boy with an AK-47 firearm;I knew at that moment I was in for the challenge of mylife! My first lesson in the field was quickly learning thedifference between “happy” and “angry” gunfire. Happygunfire occurs during celebrations, when people shoot upinto the air and nobody retaliates. During angry gunfire,people shoot back at each other! When it is too close forcomfort, it sounds like a snap and you take cover.
The first month I had a reality check with the death ofmany children, most of whom I felt could have survived in
Sue Witt is Staff Nurse, Foothills Emergency Department, Expat SupervisorBase Nurse, Pieri, South Sudan, and Calgary, AB, Canada.
For correspondence, write: SueWitt, RN, BN; E-mail: [email protected].
J Emerg Nurs 2009;35:564-8.
Available online 12 September 2009.
0099-1767/$36.00
Copyright © 2009 Emergency Nurses Association. Published by Elsevier Inc.All rights reserved.
doi: 10.1016/j.jen.2009.08.006
I N T E R N A T I O N A L N U R S I N G
564 JOURNAL OF EMERGENCY NURSING 35:6 November 2009
first-world countries. My true test came when it was timefor the physician to go on her first leave. I was basicallyleft in charge without a replacement physician but withanother nurse who was all too happy for me to play theguandiit, or big boss. The first night, I was on call and losta patient. Sadly, I had expected her to die. We did not knowher exact diagnosis, but her white blood cell count was ex-cessively high, and when I performed a peritoneal tap, purewhite material flowed through the tubing. Frustratingly, attimes, we are limited with the resources we have.
I quickly had to regain my composure and focus onthe next call that came over the radio. I was informed that6 vomiting children had arrived from the same neighboringvillage. Because vomiting is a common complaint in thisenvironment, I advised that oral rehydration solution begiven and that I be called back if things did not improve.As the night progressed, I discovered that I was in for asurprise! A bit later, I received a call that 2 of the childrenwere having seizures and another 2 were vomiting blood. Iran to the clinic to find, in fact, 2 of the 6 children havingrepeated seizures. I knew this was not just simple vomiting.After a great deal of discussion, it was discovered that thechildren had ingested something from a bullet. This wasrevealed to me only after I asked one of the fathers to bringback a sample of what the children ate so that I could try toidentify it. I soon learned my second lesson: Never assumethat what you see is what you get! I thought these childreninitially were dehydrated from some gastrointestinal bugfrom which so many others in this environment suffer.When we contacted another nongovernmental organiza-tion, which deals with unexploded ammunition, the next
day, we were informed that these 6 children had in factingested C4 explosives from an unexploded foot-longmortar shell they had found lying around their village.When I finally received this information 40 hours later,I read that C4 “becomes very unstable when mixed withwater.” I had given them all oral fluids as diluents andhad produced 6 little walking bombs in my clinic!
My knowledge base about ingestion of toxic sub-stances mostly comprises common household products inCanada, but the ingestion of ammunition was a completelynew situation for me. Yet again, I had to treat the patientsthe best way I knew how, without any information to guideme, and hope that the outcome would be favorable. For the2 children who had repeated seizures, I finally started themon a phenobarbital drip because the only other drug avail-able, diazepam, was not working. We were lucky that thefather did not die from handling an unexploded ordnanceand even luckier that he did not bring it into the clinic,although he did bring the explosive material. Lesson numberthree was revealed: Never bring anything into the clinic thatis associated with weapons of war. That decision could havekilled us. All 6 children survived after a week in the clinic.
Adjusting to Change
My initial weeks continued to be a challenge because re-structuring was needed. There were no organized areas forchildren or for the sickest patients, so the physician andI arranged patients into “wards.” One patient had braindamage from meningitis and was covered in pressure ulcersfrom lying on the dirt floor of her tukul (mud hut). Idecided to take the mattress out of our office that night shiftstaff used and give it to this patient. I thought the staff wasgoing to strike! This precipitated several meetings betweenthe expatriates and the national staff. During one of themeetings, someone came running in and told me a childneeded urgent medical care. I began running with thisbreathless, pulseless child in my arms to the operating the-atre, where I could attempt resuscitation with oxygen andlimited medications. As I was running, one of the staffstopped me and continued to explain to me that he didnot think I should have taken away the mattress from theoffice. I was dumbfounded! There I was with this dead childin my arms, doing chest compressions, and this staff mem-ber did not seem to care. Later, it was put to me in thesesimple yet poignant terms: “Death is more common thanmattresses here.”
Acclimatizing to Life in a Mud Hut
My solace became my daily walks to the Paramount Chief’s(Village Leader’s) hut with the physician who was now a
F I G U R E 1
Village of mud huts in Sudan. This figure is available in color and as a full-pagedocument at www.jenonline.org.
INTERNATIONAL NURSING/Witt
November 2009 35:6 JOURNAL OF EMERGENCY NURSING 565

very dear friend. I swear this small little piece of landheld the only palm tree in all of South Sudan … a littlepiece of paradise amid the dry cracked brown earth. Inpreparation for going to Sudan, I had said goodbye tomy life in Canada by selling my home and saying goodbyeto friends and family. I was focused to start a new life thatwould consist primarily of a mud hut (Figure 2). Living inthe field can be loosely related to flying an airplane withouta great deal of experience but with the hope that you canstay calm enough to learn how to keep yourself and asmany of your passengers alive as possible.
The days slipped away to months. Sunsets came andwent like the many faces of children I saved (Figure 3)and those who died (Figure 4). The sunset always did seemmore glorious after a child had died, because it remindedme of the impermanence of life. It became a ritual to watchthe colors of the evening sky change as the sun would setover the tops of the mud huts while wondering if I wouldlose any patients that night. I was finally beginning to trulyunderstand the concept of suffering. Without suffering,one could not recognize real joy. When I first arrived, therewas often dancing and singing mixed with the sounds ofgunfire; I did not comprehend the reason for a celebration.I started to see that life was precious here, and it could betaken at any moment because of illness or violence. Peoplelived in the moment because they did not know what thefuture would bring.
With the passing of time, the rains returned, remind-ing me of when I first arrived in the field, and I realizedthat my time was nearing the end. There were many obsta-cles I had survived such as being evacuated to our head-quarters in Kenya because of increased insecurities when
we felt our safety could not be guaranteed at the time. Ihad also been evacuated because of an intestinal illness re-sulting in a 10-pound weight loss in 4 days! The 2 mainchallenges were monotonous days cleaning the samewounds and the sudden presentation of very sick patientswith snakebites, severe pneumonia, dehydration, malaria,and gunshot wounds. After 9 months, my time in the fieldwas drawing to an end. I was both mentally and physicallyexhausted, but I had mixed emotions about returning toCanada. Where would I live and work? I worried about re-lating to friends and family because of how much this
TABLE 1Preparation for work with MSF
Experience Length of time Information on organization/experience gained
Work in Ecuador 1 mo The Mary A. Tidlund Charitable Foundation (www.tidlundfoundation.com)Work in Ghana 2 mo Cross-Cultural Solutions work at a regional hospital and outreach
focusing on maternal/child healthWork in NorthwestTerritories (Fort Smith)
1 mo Multi Options Nursing: charge nurse, ED nursing care of long-term patients
Diploma in tropical nursing 5 mo London School of Hygiene & Tropical Medicine (www.lshtm.ac.uk):Learned the pathophysiology and diagnosis (both clinically andmicroscopically) of various tropical diseases
MSF training in Amsterdam 1 wk www.doctorswithoutborders.org (United States)www.doctorswithoutborders.ca (Canada)
Work in Kenya 5 mo Lived with a family and worked at a small clinic without a doctor; learnedto be resourceful and work with the local population
F I G U R E 2
My home for 9 months. This figure is available in color and as a full-pagedocument at www.jenonline.org.
INTERNATIONAL NURSING/Witt
566 JOURNAL OF EMERGENCY NURSING 35:6 November 2009

experience had inevitably changed me. The last week in thefield, I struggled to work. I could not get thoughts of homeout of my head. I dreamed about owning a little place onthis earth I could call my own. I longed for the smell offresh-cut grass. I envisioned an easy life at home, sittingby the fire sipping wine and enjoying the silence. My wholelife in the last 14 years had revolved around achieving workwith MSF. It was such a huge dream to have achieved,what would I do now? Had this one goal become solelyhow I defined myself? I was not sure I could handle a“normal” life because I had trained myself to live with acertain amount of stress and adrenalin.
Going Home and Culture Shock
My departure from Sudan occurred with as much frenzyas leaving Canada. The rains resulted in unpredictablelanding strip access; to catch the plane, I had 10 minutesto say goodbye to everyone who had become my family in
the last 9 months. The trip home was a blur because ofexhaustion and the beginning of some serious culture shock.I was surprised at seeing so many other white people in theairport and how fast everyone moved. My brain had tospeed up again to start processing all the stimuli aroundme. I felt numb and slept for nearly a week. During my firstwalk outside, I was actually nervous to cross the street be-cause I had lived without roads and vehicles for the last9 months. Once walking on the street, I heard a car back-fire; I hit the ground instinctively thinking it was a gunshot.I felt I was too materialistic, so I gave away the majority ofmy clothes; of course, sometime later, I realized that havingwarm clothes in Canada would be beneficial.
Those who did ask about my trip did not really wantto hear the details because they are simply too grotesque ortoo foreign a concept to comprehend. Most of my friendsand family did not even ask. I had stories to tell, but thosestories fell onto deaf ears or none at all; I was surrounded bypeople, but I felt completely alone. The only way I couldcope was to put on a “happy face” for everyone. I did notbelong here, and I did not belong there. I was not preparedfor the length of time it took to adjust to living back inCanada again. I learned how to cry in silence so that nobodywould know the struggle I was going through.
Final Thoughts
There were times in the field when supplies were limitedand choices had to be made. I felt intense guilt thinkingI had played God with peoples’ lives. Those who have
F I G U R E 3
Me and a patient who survived malnutrition and malaria. This figure is available incolor and as a full-page document at www.jenonline.org.
F I G U R E 4
The first little one I lost. This figure is available in color and as a full-pagedocument at www.jenonline.org.
INTERNATIONAL NURSING/Witt
November 2009 35:6 JOURNAL OF EMERGENCY NURSING 567

never done this work can have misconceptions about ac-tually saving lives versus the real feelings of frustrationand wanting to do more. I did what I had to do, workingwell beyond my scope of practice in Canada. The mostdisturbing comment I received was about liability. Peoplewould say, “Well, at least nobody will sue you over there.”My patients were not guinea pigs; I did what I could withthe resources I had and hoped that it was enough. Life isvaluable whether you live in a mansion or a mud hut.Through my stories, I hope to close the gap between thedeveloped and the still-developing world.
My time in Sudan has given me strength. Eventually,the tears lessoned, and the pain of acknowledging every-thing I had experienced started to subside. Every once inawhile, I smell a wood-burning fireplace and can smile
now, thinking back to where it all began … my journeyto Sudan.
REFERENCE1. Doctors Without Borders. Available at: http://en.wikipedia.org/
wiki/Doctors_Without_Borders. Accessed June 30, 2009.
Submissions to this column are encouraged and may be sent toPat Clutter, RN, MEd, CEN, [email protected] Rush, RN, MEd, CEN, [email protected]
INTERNATIONAL NURSING/Witt
568 JOURNAL OF EMERGENCY NURSING 35:6 November 2009